Embed Size (px)
Citation preview
NEONATAL INFECTIONS, NOENATAL SEPSIS,
OPTHALMIA NEONATRUM & CONGENITAL SYPHILLIS
Anti microbial selection1. E.Coli, Klebsiella, Shigella & Salmonella :
Amnioglycorides or 3’rd generation Cehalosponis.
2. Haemophilus Influenza : Ampicillin & 3’rd generation Cehalosponis. Sometimes ampicillin are resistant.
3. Pseudomonas : Amnioglycorides + anti pseudomonas pencillin.
4. Bacteroides Fragilis : Metronidazole, clindamycin, some beta lactomoses such as imipenum & ampicillin with sulbactim & chloramphenicol.
Group B Streptococcus
Group b streptococcus hemolytic streptococci
were unknown to the perinatal scene until there
early 1970’s where they replaced E.Coli as the
single most common agent associated with
bacterial meningitis during the 1’st 2 months of
life.
PathophysiologyIntensity of the maternal colonization is directly
Related to risk of invasive disease in the neonate
because of low & high density colonization
Risk of amniotic fluid contaminated with meconium
or vernix caseosa which promotes the growth of
the GBS & E.Coli
Conts…. Few organisms in the vaginal vault due to the
PMOM
Possibly contributing to the paradox.
Organisms usually reach the blood stream by fetal
aspiration or swallowing of the contaminated
amniotic fluid
Leading to bacteremia.
Escherichia Coli E.Coli is a gram negative, non
spore forming motile rod. It is a
normal inhabitant of the gastro
intestinal tract & most common
cause of the gram negative infection
in the new born.
Listeria Monocytogenes1. It is found in the birds & mammals, including
domestic and farm animals.
2. It is found in the unpasteurized milk, soil and
fecal matter.
3. The infection appears to be undiagnosed and an
underreported cause of the congenital infection.
Neonatal meningitis A neonatal bacterial
meningitis is the inflammation
of the meninges due to the
bacterial invasion. Meningitis
can be a sequence of the new
born infection.
Toxoplasmosis
The importance of the
parasite toxoplasma gondii
was discovered by health
care worker through the
perinatal death.
Management1. Prevention & early recognition.2. Mother at a risk should avoid soil digging,
handling or cooking under cooked meat.3.If the signs of infection exhibit then report
immediately.4.Congenital toxoplasmosis : Pyrimethamine +
Sulfonamides. 2mg/kg/day, orally for 2 days, followed by 1mg/kg/day for 2 or 6 months, then 1mg/kg/day every Monday, Wednesday and Friday for a year period.
Conts…5.Doses of 100mg/kg/day is divided into 2 doses for
1 year.
6.Levovorin 10 mg is given 3 times weekly & for 1
week after Pyrimethamine therapy.
7.Corticosteroids are given in the form of predinose
at 1 mg/kg/day in 2 divided doses until there is a
resolution of elevated protein in CSF.
RUBELLA
Congenital rubella is a viral
infection acquired from the
mother during pregnancy. It
has been established that
the rubella virus can be
responsible for other
abnormalities.
Management 1.Avoid pregnancy for atleast 2 months after
immunizations to decrease the risk of rubella syndrome.
2.If the women receives rubella or RHoGAIG (RhIG). The vaccine may not trigger an immune response because blood products & RHoGAIG have pooled sera that may contain antibodies against rubella. Thus the women does not produce antibodies.
3.Trites should be drawn between 6 weeks after the vaccination or at most after 3 weeks.
Conts….4.Vaccination is not recommended in
pregnancy but in case if they don’t wish
to continue the pregnancy they go for
the vaccination.
5.Avoid contacts with the patients.
6.Follow up for the children for the
cardiac problems & cataracts should be
done.
Cytomegalo virus Infection with cytomegalovirus, a member
of the herpes family, is common. CMV is a
DNA virus covered with a glycoprotein
coat that closely resembles the herpes &
varicella zoster virus. CMV infection is
more prevalent in lower economic group &
especially common in the developing
countries.
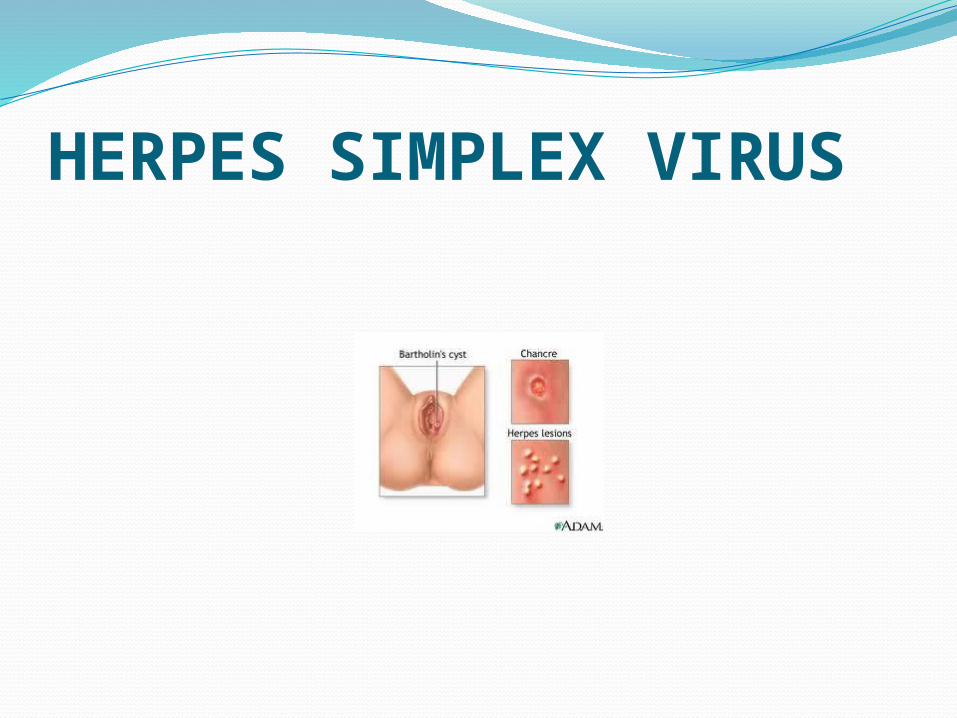
HERPES SIMPLEX VIRUS
Introduction Neonatal herpes simplex virus infection is
usually transmitted during delivery. HSV is a
member of a family of the large DNA virus.
They contain linear, double strands of DNA.
The herpes family also includes CMV,
Varicella-Zooster & Epstein-Barr Virus.
Management 1. Antiviral drug: Acyclavir & Vidarabine.
2. Vidarabine: 15-30mg/kg/day/IV, over a period of
10-14 days for 12 hours.
3. Acyclavir: 30mg/kg/day/IV divided over 8 hours
for 10 to 14 days. it helps in decreasing the
reactivation of the virus particularly in the
treatment of herpes simplex encephalitis.
4.Eye: Trifluridine, 1 drop every 2 hours, as well as
IV therapy.
Other’s1.Isolation : viral shedding provides
an reservoir for infecting others.
2.Family education & support.
3.Hand washing techniques.
4.Positive cultures at birth may just
reflect colonization, cultures should
be repeated at 24 to 48 hours.
Hepatitis virus It is a double stranded DNA
containing virus exposure to
infected blood & body fluids,
percutaneous introduction of blood
& administration of infected blood
products are the principal routes of
transmission.
Chlamydia Chlamydia trachomatis infection has
been identified as causing significant
increase in the incidence of PROM,
the number of low birth weight babies
and the rate of infant mortality.
Candida Albicans
It is the more prevalent form in the
neonates. Candida organisms are oval,
yeast like cells that can bud to reproduce
C-Albican producers endotoxican,
hemolysis, pyrogen & protrolytic enzymes
that are damaging to the tissues.


![[XLS] · Web view2015/01/30 · Haemophilus parainfluenzae, biotype V (organism) Haemophilus parainfluenzae, biotype VI - HAEPA6 HAEPA6 Haemophilus parainfluenzae, biotype VI (organism)](https://img.pdfslide.us/doc/110x75/5aebb4d37f8b9a585f8debf8/xls-view20150130haemophilus-parainfluenzae-biotype-v-organism-haemophilus.jpg)