Embed Size (px)
Citation preview

1Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Anti-Infective Drugs Anti-Infective Drugs Advisory Committee MeetingAdvisory Committee Meeting
Clinical Trial Designs for Clinical Trial Designs for Community Acquired PneumoniaCommunity Acquired Pneumonia
Anti-Infective Drugs Anti-Infective Drugs Advisory Committee MeetingAdvisory Committee Meeting
Clinical Trial Designs for Clinical Trial Designs for Community Acquired PneumoniaCommunity Acquired Pneumonia
April 1 & 2, 2008
Edward Cox, MD MPHDirector, Office of Antimicrobial Products
OND/CDER/FDA
April 1 & 2, 2008
Edward Cox, MD MPHDirector, Office of Antimicrobial Products
OND/CDER/FDA

2Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
WelcomeWelcomeWelcomeWelcome• Welcome• Topic for discussion
– Clinical trial designs for Community Acquired Pneumonia (CAP)
• Primary purpose of the meeting– To seek the Advisory Committee’s advice on
informative, safe, and ethical trial designs to evaluate the safety and efficacy of antibacterial drugs for the treatment of CAP
– Work through the key parameters in the design of a CAP trial
– Very interested to hear the scientific rationale, evidence relied upon and reasoning in arriving at recommendations for clinical trial designs for CAP
• Welcome• Topic for discussion
– Clinical trial designs for Community Acquired Pneumonia (CAP)
• Primary purpose of the meeting– To seek the Advisory Committee’s advice on
informative, safe, and ethical trial designs to evaluate the safety and efficacy of antibacterial drugs for the treatment of CAP
– Work through the key parameters in the design of a CAP trial
– Very interested to hear the scientific rationale, evidence relied upon and reasoning in arriving at recommendations for clinical trial designs for CAP

3Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Background - 1Background - 1Background - 1Background - 1
• Antibacterial drugs discovered many years ago• Represented a major advance in medicine• Antibacterial therapy incorporated into clinical
practice before sophisticated clinical trial designs• Standard of care for CAP for years• Some of the information that tells us about effect
of antibacterial drugs in CAP (compared to “no treatment”) is from literature from many years ago
• Antibacterial drugs discovered many years ago• Represented a major advance in medicine• Antibacterial therapy incorporated into clinical
practice before sophisticated clinical trial designs• Standard of care for CAP for years• Some of the information that tells us about effect
of antibacterial drugs in CAP (compared to “no treatment”) is from literature from many years ago

4Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Background - 2Background - 2Background - 2Background - 2
• Science of clinical trials in New Drug Applications (NDAs) has also advanced– Microbiologically focused label– Respiratory tract infections (RTI)
• composite data from a variety of RTIs– Lower respiratory tract infections (LRTI)
• composite data ABECB & CAP– Community acquired pneumonia (CAP)
• trials specific for CAP• noninferiority design w/ margin of 10 to 15%• margin choice based upon convention rather than
clear justification based upon evaluation of available data
• oral agents – mild to moderate severity
• Science of clinical trials in New Drug Applications (NDAs) has also advanced– Microbiologically focused label– Respiratory tract infections (RTI)
• composite data from a variety of RTIs– Lower respiratory tract infections (LRTI)
• composite data ABECB & CAP– Community acquired pneumonia (CAP)
• trials specific for CAP• noninferiority design w/ margin of 10 to 15%• margin choice based upon convention rather than
clear justification based upon evaluation of available data
• oral agents – mild to moderate severity

5Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
CAP IndicationCAP IndicationCAP IndicationCAP Indication
INDICATIONS AND USAGE• [Drug Name] is indicated in the treatment of
infections caused by susceptible strains of the designated microorganisms in the conditions listed below:
Community-acquired pneumonia caused by Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, Moraxella catarrhalis, Legionella pneumophila, Chlamydophila pneumoniae, or Mycoplasma pneumoniae
INDICATIONS AND USAGE• [Drug Name] is indicated in the treatment of
infections caused by susceptible strains of the designated microorganisms in the conditions listed below:
Community-acquired pneumonia caused by Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, Moraxella catarrhalis, Legionella pneumophila, Chlamydophila pneumoniae, or Mycoplasma pneumoniae

6Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Some Drugs with a CAP or Related IndicationSome Drugs with a CAP or Related IndicationSome Drugs with a CAP or Related IndicationSome Drugs with a CAP or Related Indication
• Microbiologically “focused”– penicillin G, penicillin V, tetracycline, oxytetracycline, doxycycline,
minocycline, demeclocycline, clindamycin, lincomycin, streptomycin
• Respiratory tract infections (past indication - composite)– ampicillin, cephalexin, cefazolin– amikacin, gentamicin
• Lower respiratory tract infections (past indication - AECB & CAP)– amoxicillin, amoxicillin/clavulanate, piperacillin,
piperacillin/tazobactam, ticarcillin/clavulanate – erythromycin– cefotaxime, cefoxitin, ceftazidime, ceftizoxime, ceftriaxone, cefaclor
cefuroxime injection, – imipenem/cilistatin, - aztreonam - tobramycin– ciprofloxacin - metronidazole (Bacteroides)
• Community-acquired pneumonia– amoxicillin/clavulanate– cefdinir, cefditoren pivoxil, cefpodoxime proxetil, loracarbef, – azithromycin, clarithromycin, telithromycin– ofloxacin, levofloxacin, moxifloxacin, gemifloxacin, – linezolid
• Microbiologically “focused”– penicillin G, penicillin V, tetracycline, oxytetracycline, doxycycline,
minocycline, demeclocycline, clindamycin, lincomycin, streptomycin
• Respiratory tract infections (past indication - composite)– ampicillin, cephalexin, cefazolin– amikacin, gentamicin
• Lower respiratory tract infections (past indication - AECB & CAP)– amoxicillin, amoxicillin/clavulanate, piperacillin,
piperacillin/tazobactam, ticarcillin/clavulanate – erythromycin– cefotaxime, cefoxitin, ceftazidime, ceftizoxime, ceftriaxone, cefaclor
cefuroxime injection, – imipenem/cilistatin, - aztreonam - tobramycin– ciprofloxacin - metronidazole (Bacteroides)
• Community-acquired pneumonia– amoxicillin/clavulanate– cefdinir, cefditoren pivoxil, cefpodoxime proxetil, loracarbef, – azithromycin, clarithromycin, telithromycin– ofloxacin, levofloxacin, moxifloxacin, gemifloxacin, – linezolid

7Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Importance & Challenges - 1Importance & Challenges - 1Importance & Challenges - 1Importance & Challenges - 1
• Public Health need for new therapeutic options– antimicrobial resistance
• Need informative trials to characterize safety and efficacy– weigh risks and benefits
• Importance of having new drugs in this area also supports the importance of adequately characterizing safety and efficacy
• Quality information to inform appropriate use
• Public Health need for new therapeutic options– antimicrobial resistance
• Need informative trials to characterize safety and efficacy– weigh risks and benefits
• Importance of having new drugs in this area also supports the importance of adequately characterizing safety and efficacy
• Quality information to inform appropriate use

8Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Importance & Challenges - 2Importance & Challenges - 2Importance & Challenges - 2Importance & Challenges - 2
• Community acquired pneumonia
– risk of progression or extension of infection
• Clinical Trials of CAP should
– not expose patients to significant risk
– be informative
– be ethical & acceptable
– strategies to minimize risk• provisions for “rescue therapy”
• patient selection
• DSMB
• Community acquired pneumonia
– risk of progression or extension of infection
• Clinical Trials of CAP should
– not expose patients to significant risk
– be informative
– be ethical & acceptable
– strategies to minimize risk• provisions for “rescue therapy”
• patient selection
• DSMB

9Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Drug Product ApprovalDrug Product ApprovalDrug Product ApprovalDrug Product Approval
• 1938: Federal Food, Drug and Cosmetic Act required pre-clearance of drugs for safety & pre-market notification but did not include evaluation of efficacy
• 1962: FDC Act amended to add requirement for demonstration of effectiveness based upon “substantial evidence”
• “Substantial evidence” defined in FDC Act 505(d) as:“evidence consisting of adequate and well-controlled investigations, including clinical investigations, by experts qualified by scientific training and experience to evaluate the effectiveness of the drug involved, on the basis of which it could fairly and responsibly be concluded by such experts that the drug will have the effect it purports or is represented to have under the conditions of use prescribed, recommended, or suggested in the labeling or proposed labeling thereof.”
• 1938: Federal Food, Drug and Cosmetic Act required pre-clearance of drugs for safety & pre-market notification but did not include evaluation of efficacy
• 1962: FDC Act amended to add requirement for demonstration of effectiveness based upon “substantial evidence”
• “Substantial evidence” defined in FDC Act 505(d) as:“evidence consisting of adequate and well-controlled investigations, including clinical investigations, by experts qualified by scientific training and experience to evaluate the effectiveness of the drug involved, on the basis of which it could fairly and responsibly be concluded by such experts that the drug will have the effect it purports or is represented to have under the conditions of use prescribed, recommended, or suggested in the labeling or proposed labeling thereof.”

10Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Adequate and well controlled Adequate and well controlled studiesstudies
Adequate and well controlled Adequate and well controlled studiesstudies
21 CFR § 314.126 Adequate and well-controlled studies. (a) The purpose of conducting clinical investigations of a drug is to distinguish the effect of a drug from other influences, such as spontaneous change in the course of the disease, placebo effect, or biased observation.
• Active treatment concurrent control…– The test drug is compared with known effective therapy; for
example, where the condition treated is such that administration of placebo or no treatment would be contrary to the interest of the patient.
– If the intent of the trial is to show similarity of the test and control drugs, the report of the study should assess the ability of the study to have detected a difference between treatments. Similarity of test drug and active control can mean either that both drugs were effective or that neither was effective. The analysis of the study should explain why the drugs should be considered effective in the study, for example, by reference to results in previous placebo-controlled studies of the active control drug.
21 CFR § 314.126 Adequate and well-controlled studies. (a) The purpose of conducting clinical investigations of a drug is to distinguish the effect of a drug from other influences, such as spontaneous change in the course of the disease, placebo effect, or biased observation.
• Active treatment concurrent control…– The test drug is compared with known effective therapy; for
example, where the condition treated is such that administration of placebo or no treatment would be contrary to the interest of the patient.
– If the intent of the trial is to show similarity of the test and control drugs, the report of the study should assess the ability of the study to have detected a difference between treatments. Similarity of test drug and active control can mean either that both drugs were effective or that neither was effective. The analysis of the study should explain why the drugs should be considered effective in the study, for example, by reference to results in previous placebo-controlled studies of the active control drug.

11Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Inactive(e.g. placebo)
Active Controls & Noninferiority - 1Active Controls & Noninferiority - 1Active Controls & Noninferiority - 1Active Controls & Noninferiority - 1
Test
Active Control
Response rate
Case# 1: Large treatment effect Low spontaneous
resolution rate

12Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Active Control
Test
Active Controls & Noninferiority - 2Active Controls & Noninferiority - 2Active Controls & Noninferiority - 2Active Controls & Noninferiority - 2
Inactive (e.g. placebo)
Case #2: Unclear treatment effect High spontaneous
resolution rate
Response rate

13Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Inactive(e.g. placebo)
Active Control
Test
Active Controls & Noninferiority - 3Active Controls & Noninferiority - 3Active Controls & Noninferiority - 3Active Controls & Noninferiority - 3
Inactive (e.g. placebo)
Test
Active Control
Response rate
Case# 1: Large treatment effect Low spontaneous
resolution rate
Case #2: Unclear treatment effect High spontaneous
resolution rate
Response rate

14Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
CAP TrialsCAP TrialsCAP TrialsCAP Trials• Quantitative estimate of the effect of the
active control drug over placebo in a current day study based upon what we know from previously conducted studies– treatment effect
• Treatment effect reflects the types of patients and how studied– severity of disease, type of disease– endpoint & timing of assessment– other factors
• Accounting for uncertainty – discounting, judgments, rationale
• Goal of informative trial designs
• Quantitative estimate of the effect of the active control drug over placebo in a current day study based upon what we know from previously conducted studies– treatment effect
• Treatment effect reflects the types of patients and how studied– severity of disease, type of disease– endpoint & timing of assessment– other factors
• Accounting for uncertainty – discounting, judgments, rationale
• Goal of informative trial designs

15Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
CAP Trials in NDAsCAP Trials in NDAsCAP Trials in NDAsCAP Trials in NDAs
• Inpatient studies of CAP– Intravenous antibacterial drugs with or without
an oral formulation (“step-down” therapy)• additional studies with the oral formulation typically
done– Indication
• CAP
• Outpatient studies of CAP– Oral antibacterial drugs– Indication
• mild to moderate CAP
• Inpatient studies of CAP– Intravenous antibacterial drugs with or without
an oral formulation (“step-down” therapy)• additional studies with the oral formulation typically
done– Indication
• CAP
• Outpatient studies of CAP– Oral antibacterial drugs– Indication
• mild to moderate CAP

16Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Key TopicsKey TopicsKey TopicsKey Topics- Review what we know and don’t know about CAP
and issues in clinical trial design- treatment effect based upon available data
- what population- what endpoint (when to assess)- other key parameters
- Address key issues in clinical trial design for CAP & describe possible informative CAP trial designs- studies of IV drugs - - studies of oral drugs- endpoints- what population- can noninferiority studies be done? - can superiority studies can be done?
- Review what we know and don’t know about CAP and issues in clinical trial design- treatment effect based upon available data
- what population- what endpoint (when to assess)- other key parameters
- Address key issues in clinical trial design for CAP & describe possible informative CAP trial designs- studies of IV drugs - - studies of oral drugs- endpoints- what population- can noninferiority studies be done? - can superiority studies can be done?

17Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Overview of the 2-Day MeetingOverview of the 2-Day MeetingOverview of the 2-Day MeetingOverview of the 2-Day Meeting
• Agenda – Day #1
– IDSA/FDA CAP workshop
– IDSA perspective
– ATS/ACCP statement
– Ethical considerations
– Noninferiority trials in CAP
• Agenda – Day #1
– IDSA/FDA CAP workshop
– IDSA perspective
– ATS/ACCP statement
– Ethical considerations
– Noninferiority trials in CAP

18Anti-Infective Drugs Advisory Committee Anti-Infective Drugs Advisory Committee April 1 & 2, 2008April 1 & 2, 2008
Overview of the 2-Day MeetingOverview of the 2-Day MeetingOverview of the 2-Day MeetingOverview of the 2-Day Meeting• Agenda – Day #1 (continued)
– Historical data on CAP
– Contemporary CAP trials
– Approaches to setting an NI margin
– Exposure-Response analysis for CAP
– Critical considerations in CAP trial design
• Day # 2
– A clinician’s scientific approach to pneumonia
– Considerations in design of CAP studies
– Questions and discussion
– Questions for the AC
• Agenda – Day #1 (continued)
– Historical data on CAP
– Contemporary CAP trials
– Approaches to setting an NI margin
– Exposure-Response analysis for CAP
– Critical considerations in CAP trial design
• Day # 2
– A clinician’s scientific approach to pneumonia
– Considerations in design of CAP studies
– Questions and discussion
– Questions for the AC

19
For questions 1 and 2:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
To rely on noninferiority studies for new drugs to treat CAP, we must be able to estimate the effect size a control drug would have on the primary endpoint used in the current trial. The Agency has presented information on the historical experience that suggest a reduction in mortality with point estimates ranging from 18 to 25% in the observational studies and from approximately 10 to 19% in controlled trials. These data are derived from patients with pneumococcal / lobar pneumonia.

20
Question 1a:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
1. Can these data be utilized to select a noninferiority margin for a contemporary CAP study for an IV drug in hospitalized patients?
a) To what severity of pneumonia or type of patients would it apply and how should severity be defined?

21
Question 1b-1c:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
b) Should a microbiological diagnosis be necessary for inclusion in the primary analysis population for the trial, and if
so, what organisms should be included (e.g., S. pneumoniae, other microbes)?
c) Should strategies be utilized to enrich the population for patients with a particular microbial etiology (e.g., S. pneumoniae, or other microbes)?

22
Question 1d:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
d) Please discuss whether the evidence which shows a treatment effect based on mortality can be linked to endpoints which are used in current non-inferiority CAP trials (i.e. clinical success/failure). If so, how? (Note: the possible components of the clinical failure endpoint might include some of the following mortality, receiving rescue therapy, lack of resolution of clinical signs and symptoms such that additional antibacterial therapy is administered, lack of resolution of signs and symptoms at the time the primary endpoint is assessed.)

23
Question 1e:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
e) The historical evidence for a treatment effect is based on studies which evaluated penicillin, sulfonamides, and tetracyclines. Given the need to preserve the treatment effect (the effect of the comparator agent over placebo or no treatment) in a future study, what are appropriate choices for comparator agents? Please explain the basis and information that supports the recommendation for comparator agents for a future study.

24
Question 1f:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
f) What is your best estimate of the treatment effect size (M1) that the historical data support for treatment of hospitalized CAP (based on severity selected in part a of this question, above) in a future CAP trial and what is your recommendation for a noninferiority margin that preserves a portion of the treatment effect (i.e., M2) for a CAP trial in this population with the endpoints discussed above?

25
Question 2:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
2. Given the information presented, mostly from historical data on the treatment effect of drugs for CAP in patients with pneumococcal / lobar pneumonia, please address the following questions on trials of outpatient CAP (studies using an oral drug).

26
Question 2a:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
a) Can a treatment effect be reliably quantified for a noninferiority study of outpatient CAP (i.e., for an oral drug)?
i. To which patient population would this information apply with regards to disease severity and microbiological etiology?
ii. What endpoint(s) should be utilized?
iii. What is the proposed noninferiority margin and what data support the proposed noninferiority margin?

27
Question 2b:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
b) Can placebo-controlled trials be carried out in less severely ill patients with CAP?
i. If yes, how can risk to patients be minimized? What patient population could be enrolled? What endpoints should be evaluated?

28
Question 2c:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
c) Can you suggest any alternative study designs that could be utilized which would allow for an informative trial of outpatient CAP (i.e., an oral drug) to be conducted? Please describe.

29
Question 3:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
3. In a setting of hospitalized CAP as described in question 1 (above), one could study therapy with an intravenous formulation administered initially with subsequent “step down” therapy to an oral formulation as a means to support the use of the oral and IV formulations for severe disease.

30
Question 3 continued:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
This leaves the question of whether the finding of efficacy for severe CAP would provide evidence of efficacy that could be used to support efficacy of the oral formulation for less severe (i.e., mild and moderate CAP). Do you believe the finding of efficacy in more severe CAP supports the drug’s effect in less severe CAP, even though the drug has not been directly studied in less severe CAP?

31
Question 4:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
4. If the available evidence for setting a noninferiority margin in current CAP trials is derived primarily from studies of patients with CAP due to S.pneumoniae, should noninferiority studies include patients with other etiologies of CAP?

32
Question 4 continued:
Anti-Infective Drugs Advisory Committee meetingAnti-Infective Drugs Advisory Committee meetingApril 1 & 2, 2008April 1 & 2, 2008
If not, what additional data/studies are needed to show that antibacterial drugs are effective for specific organisms? When addressing this question please consider the following organisms:
Chlamydophila pneumoniae
Haemophilus influenzae
Legionella pneumophila
Mycoplasma pneumoniae
Staphylococcus aureus
Klebsiella pneumoniae

33
Key Issues from Key Issues from the FDA-IDSA the FDA-IDSA
WorkshopWorkshopJohn Alexander, MD, MPHJohn Alexander, MD, MPH
Medical Team Leader,Medical Team Leader,Division of Anti-Infective and Division of Anti-Infective and
Ophthalmology Products, Ophthalmology Products, CDERCDER

34
FDA-IDSA WorkshopFDA-IDSA Workshop
Held January 17-18, 2008Held January 17-18, 2008 GoalsGoals
Examine critical issues in:Examine critical issues in: The design and conduct of trials of the safety The design and conduct of trials of the safety
and efficacy of antibacterial drugs in the and efficacy of antibacterial drugs in the treatment of CAPtreatment of CAP
The implications of emerging scientific tools The implications of emerging scientific tools that assist in the diagnosis of the etiology of that assist in the diagnosis of the etiology of CAPCAP
Discuss clinical trial design and statistical Discuss clinical trial design and statistical considerations in demonstrating efficacy considerations in demonstrating efficacy in clinical trials of CAP.in clinical trials of CAP.

35
CAP ScenariosCAP Scenarios Day 1 – CAP not requiring hospitalizationDay 1 – CAP not requiring hospitalization35 y/o male, 3 days of URI, purulent sputum, coughing35 y/o male, 3 days of URI, purulent sputum, coughing fever (38.3 C),fever (38.3 C), RR 18, “crackles” at R base RR 18, “crackles” at R baseCXR – bilateral LL infiltrates, R>LCXR – bilateral LL infiltrates, R>L Day 2 – Hospitalized CAP, not requiring ICUDay 2 – Hospitalized CAP, not requiring ICU65 y/o female, mild COPD, diabetes, HTN, smoker (35 65 y/o female, mild COPD, diabetes, HTN, smoker (35
PY)PY)
↑ ↑ sputum, ↑ dyspnea, fever (39.2 C), RR 24, Osputum, ↑ dyspnea, fever (39.2 C), RR 24, O22 sat= sat= 89% RA89% RA
definite L crackles, no rubs, PORT=IV, CURB-65=2definite L crackles, no rubs, PORT=IV, CURB-65=2CXR – LLL consolidation, air bronchogram, large heartCXR – LLL consolidation, air bronchogram, large heart

36
CAP Presentations – AC CAP Presentations – AC RepriseReprise
Criteria for NI Trials and Clinical ImportanceCriteria for NI Trials and Clinical Importance NI Trials Submitted in the Recent PastNI Trials Submitted in the Recent Past Historical Data on Treatment EffectHistorical Data on Treatment Effect PK/PD RelationshipPK/PD Relationship Clinician’s PerspectiveClinician’s Perspective Consultant’s PerspectiveConsultant’s Perspective IDSA PerspectiveIDSA Perspective Open Public Hearing – Industry PresentationsOpen Public Hearing – Industry Presentations
AC Presentations Informed by CAP Workshop AC Presentations Informed by CAP Workshop

37
CAP Presentations – CAP Presentations – DiagnosticsDiagnostics
Improved Detection of Improved Detection of S. S. pneumoniaepneumoniae
Molecular Diagnostics for Viral and Molecular Diagnostics for Viral and Bacterial PathogensBacterial Pathogens
Etiology of Outpatient CAPEtiology of Outpatient CAP Etiology of Hospitalized CAPEtiology of Hospitalized CAP Procalcitonin – Biomarker for CAPProcalcitonin – Biomarker for CAP

38
DiagnosticsDiagnostics
* Intensive Care Unit * Intensive Care Unit ††Influenza A/B, Adenovirus, RSV, parainfluenza Influenza A/B, Adenovirus, RSV, parainfluenza ## Gram-negative bacilli Gram-negative bacilli
Lancet 2003 (Dec. 13); 362:1991Lancet 2003 (Dec. 13); 362:1991
Outpatient Outpatient (Mild)(Mild)
Non-ICU Non-ICU inpatientsinpatients
ICU* (Severe)ICU* (Severe)
S pneumoniaeS pneumoniae S pneumoniaeS pneumoniae S pneumoniaeS pneumoniae
M pneumoniaeM pneumoniae M pneumoniaeM pneumoniae LegionellaLegionella spp. spp.
H influenzaeH influenzae C pneumoniaeC pneumoniae H influenzaeH influenzae
C pneumoniaeC pneumoniae H influenzaeH influenzae GNBGNB##
Resp. VirusesResp. Viruses†† LegionellaLegionella spp. spp. S aureusS aureus
AspirationAspiration
Resp. VirusesResp. Viruses††

39
DiagnosticsDiagnostics Conventional methods (CM) for bacterial Conventional methods (CM) for bacterial
diagnosis are limiteddiagnosis are limited Blood cultures have low yieldBlood cultures have low yield Sputum samples not available for all patientsSputum samples not available for all patients
Study of 109 patients with CAP (77 Study of 109 patients with CAP (77 hospitalized)*hospitalized)*
Pathogen identified by CM in 54/109Pathogen identified by CM in 54/109 Transthoracic aspirates identified Transthoracic aspirates identified S. S.
pneumoniae pneumoniae as etiologic agent in 33% as etiologic agent in 33% (18/55) of patients with unknown cause (18/55) of patients with unknown cause based on conventional methodsbased on conventional methods Not practical for clinical trialsNot practical for clinical trials
*Ruiz-Gonzalez et al. Am J Med 1999; 106:385-390*Ruiz-Gonzalez et al. Am J Med 1999; 106:385-390

40
DiagnosticsDiagnostics
Binax NowBinax Now®® S. pneumoniaeS. pneumoniae Urinary Ag Urinary Ag Approved – August 1999Approved – August 1999
Prospective study suspected Prospective study suspected S pneumoS pneumo (sepsis (sepsis or LRTI)or LRTI)
Sens 90%, Spec 75% vs. blood culture Sens 90%, Spec 75% vs. blood culture Spanish Study of CAP* Spanish Study of CAP*
Concentrated urine samplesConcentrated urine samples 10/13 (77%) bacteremic pneumococcal CAP10/13 (77%) bacteremic pneumococcal CAP 9/14 (64%) non-bacteremic pneumococcal CAP9/14 (64%) non-bacteremic pneumococcal CAP 69/300 (23%) CAP but no pathogen isolated69/300 (23%) CAP but no pathogen isolated
*CID 2003 (Feb 1); 36:286*CID 2003 (Feb 1); 36:286

41
DiagnosticsDiagnostics
Atypical PathogensAtypical Pathogens LegionellaLegionella
Urinary Ag has replaced other methods for Urinary Ag has replaced other methods for diagnosis (Sens 75-85%; Spec 99% for diagnosis (Sens 75-85%; Spec 99% for L. L. pneumophilapneumophila 1) 1)
MycoplasmaMycoplasma MIF - Serologic testing is current standardMIF - Serologic testing is current standard
Chlamydophila (Chlamydia)Chlamydophila (Chlamydia) MIF – Poor correlation with culture or PCR*MIF – Poor correlation with culture or PCR* PCR – Multiple in-house assays (need PCR – Multiple in-house assays (need
standardization) standardization) CID 2007 (Feb 15); 44:568CID 2007 (Feb 15); 44:568

42
DiagnosticsDiagnostics
xTAG™ Respiratory Virus PanelxTAG™ Respiratory Virus Panel Approved - Jan. 2008Approved - Jan. 2008 PCR system for viral DNA/RNA PCR system for viral DNA/RNA
detectiondetection Influenza A(H1 & H3)/B, RSV A/B, Influenza A(H1 & H3)/B, RSV A/B,
Adenovirus, Parainfluenzae (1, 2, 3), Adenovirus, Parainfluenzae (1, 2, 3), Human Metapneumovirus, RhinovirusHuman Metapneumovirus, Rhinovirus
Use for diagnosis of viral infectionsUse for diagnosis of viral infections ?Exclusion of patients from CAP trials??Exclusion of patients from CAP trials?

43
DiagnosticsDiagnostics
Procalcitonin (PCT)Procalcitonin (PCT) ““Hormokine” produced by parenchymal cellsHormokine” produced by parenchymal cells Increases in response to sepsisIncreases in response to sepsis Attenuated by viral infection-related cytokinesAttenuated by viral infection-related cytokines ““Promising” as biomarker for selecting patients Promising” as biomarker for selecting patients
more likely to have bacterial vs. viral pathogen more likely to have bacterial vs. viral pathogen Limited experience with PCT at a few centersLimited experience with PCT at a few centers Not yet used in trials for drug developmentNot yet used in trials for drug development

44
CAP PresentationsCAP Presentations
Pneumonia Severity - PORT Score Pneumonia Severity - PORT Score (a.k.a. PSI)(a.k.a. PSI) Developed as a prediction tool for short-Developed as a prediction tool for short-
term mortality in CAP patientsterm mortality in CAP patients

45
PORT ScorePORT Score
NEJM 1997; 336(4):243-250

46
PORT ScorePORT Score
DemographicsDemographics H & PH & P LaboratoryLaboratoryage = yrs (M)age = yrs (M) neoplasia (+30)neoplasia (+30) pH <7.35 (+30)pH <7.35 (+30)age = yrs – 10 (F)age = yrs – 10 (F) CHF (+10)CHF (+10) BUN >30 (+20)BUN >30 (+20)nursing home (+10)nursing home (+10) renal disease (+10)renal disease (+10) Na <130 Na <130
(+20)(+20)liver disease (+20)liver disease (+20) glucose >250 (+10)glucose >250 (+10)CVD (+10)CVD (+10) hct <30% (+10)hct <30% (+10)
pulse >125 (+10)pulse >125 (+10) p0p022 <60 (+10) <60 (+10)SBP <90 (+20) SBP <90 (+20) CXR - effusion (+10)CXR - effusion (+10)RR >30 (+20)RR >30 (+20)T >40 C or <35 C (+15)T >40 C or <35 C (+15)altered mental status (+20)altered mental status (+20)
NEJM 1997; 336(4):243-250

47
PORT ScorePORT Score
NEJM 1997; 336(4):243-250

48
PORT ScorePORT Score
Prognostic score for mortalityPrognostic score for mortality Includes elements related to severity, but Includes elements related to severity, but
not a true severity scorenot a true severity score Good tool for reducing unnecessary Good tool for reducing unnecessary
hospitalization hospitalization Intended to supplement, not override, Intended to supplement, not override,
physician judgmentphysician judgment Tool was studied in treated patientsTool was studied in treated patients Would it predict mortality in untreated Would it predict mortality in untreated
patients?patients?

49
Workshop DiscussionWorkshop Discussion
Many concerns about non-inferiority trialsMany concerns about non-inferiority trials Selection criteria, diagnostics, endpoints, Selection criteria, diagnostics, endpoints,
analysisanalysis But … non-inferiority could be supported But … non-inferiority could be supported
for some CAP patientsfor some CAP patients Need for clear guidance for CAP studiesNeed for clear guidance for CAP studies For mild pneumonia, more debate about For mild pneumonia, more debate about
use of NI trials though most still question use of NI trials though most still question ethics of placebo control trial or ethics of placebo control trial or practicality of superioritypracticality of superiority

50
Workshop DiscussionWorkshop Discussion Disease SeverityDisease Severity
PORT score and CURB-65 both discussedPORT score and CURB-65 both discussed Clinical EndpointsClinical Endpoints
Emphasis on PRO tool for mild pneumoniaEmphasis on PRO tool for mild pneumonia Objective, but how can PRO measure be related to Objective, but how can PRO measure be related to
historic evidence of treatment effect?historic evidence of treatment effect? Discussed use of mortality for severe Discussed use of mortality for severe
pneumoniapneumonia Advantage – objective, most related to historic Advantage – objective, most related to historic
datadata Disadvantage – uncommon, treatment alternatives Disadvantage – uncommon, treatment alternatives
Composite EndpointComposite Endpoint

51
AcknowledgementsAcknowledgements
Co-Chairs: Thomas R. Fleming, David Gilbert, Edward Co-Chairs: Thomas R. Fleming, David Gilbert, Edward CoxCox
Rapporteur: Brad SpellbergRapporteur: Brad SpellbergParticipants: Paul Ambrose, John G Bartlett, Helen Participants: Paul Ambrose, John G Bartlett, Helen
Boucher, John S Bradley, Dale Bratzler, Dennis Dixon, Boucher, John S Bradley, Dale Bratzler, Dennis Dixon, Roger M Echols, Thomas M File Jr, Michael Fine, Roger M Echols, Thomas M File Jr, Michael Fine, Karen Higgins, Keith P Klugman, Katherine A Karen Higgins, Keith P Klugman, Katherine A Laessig, Lionel A Mandell, Timothy F Murphy, Daniel Laessig, Lionel A Mandell, Timothy F Murphy, Daniel M Musher, Michael Niederman, Frederick Nolte, M Musher, Michael Niederman, Frederick Nolte, Robert O’Neill, Tatiana Oussova, John Powers III, Robert O’Neill, Tatiana Oussova, John Powers III, Bruce Psaty, Mary Singer, George H Talbot, Robert Bruce Psaty, Mary Singer, George H Talbot, Robert Temple, Glenn Tillotson, Richard WunderinkTemple, Glenn Tillotson, Richard Wunderink
http://www.fda.gov/cder/meeting/CAP.htmhttp://www.fda.gov/cder/meeting/CAP.htm

52
American Thoracic Society/American College of Chest Physicians Perspective
Richard G. Wunderink MDNorthwestern University Feinberg School of Medicine
Division of Pulmonary and Critical Care Medicine

53
ATS/ACCP Perspective
Applaud the Agency’s attempt to improve quality of clinical trials for CAP
Agree with concerns about the need for new antibiotics Especially new classes of antibiotics
Epidemic of resistant pathogens is incontrovertible, concerning, and unlikely to diminish in future

54
ATS/ACCP Themes/Emphasis
Clinically relevantConsistent with most recent
IDSA/ATS CAP guidelines

55
ATS/ACCP Themes/Emphasis
Clinically relevantStratification/definition

56
CAP CategoriesMild = outpatient Moderate = hospitalized
outside the ICU Severe = ICU admission

57
Etiology of Severe CAP
4323 13 18
19
86
11
13
38
1619
10 23
27
32
15 8
3820
0%
20%
40%
60%
80%
100%
OtherS.pneumoEnterobacNonfermS.aureus

58
Severe CAP and Pneumonia Severity Index
6 5.68.7
15.9
23.8
0
5
10
15
20
25
ICU
Adm
issi
on (
%)
I II III IV V
Pneumonia Severity Index Class
Angus, AJRCCM, 2002
27% of ICU Adm

59
Diagnostic Criteria for Severe CAP
60
17
33.3
26 2420
49
18.5 16.7
23.7
0
10
20
30
40
50
60
%
ATS Revised ATS BTS PSI IV-V PSI V
Met Criteria for SCAP
If met, admitted to ICU
Angus, AJRCCM, 2002

60
Mechanical Ventilation- NIV or ETT
SCAPICU
SCAPICU
Septic Shock
•Confusion Hypothermia•Uremia Leukopenia•RR > 30 Thrombocytopenia•Massive fluid resuscitation for BP•PaO2/FiO2 < 250 Multilobar
YES
YES
NO
NO
3/9 = SCAP/ICU

61
ATS/ACCP Themes/Emphasis
Clinically relevantStratification/definitionInclusion of severe CAP/ICU
patients

62
SCAP: IDSA/ATS Guideline-Recommended Therapy
Beta-lactam (cephalosporin)
PLUSMacrolide or Fluoroquinolone

63
Combination Therapy in SCAP
71.8
6370.7
60.5
0
10
20
30
40
50
60
70
80
Cli
nica
l Cur
e (%
)
Protocol mITT Protocol mITT
Cefotax/OfloxLevoflox
Overall Population Mechanical Ventilation
Leroy, Chest, 2005

64
ATS/ACCP Themes/Emphasis
Clinically relevantConsistent with IDSA/ATS
CAP guidelinesExclusion of healthcare-
associated pneumonia (HCAP)

65
Risk Factors for MDR Pathogens
Antimicrobial therapy in preceding 90 daysCurrent hospitalization > 5 daysHigh frequency of antibiotic resistance in
community or specific hospital unitPresence of risk factors for HCAP
> 2 days hospitalization in previous 90 days Nursing home or extended care facility residence Home infusion therapy or wound care Chronic dialysis for > 30 days Family member with MDR
Immunosuppressive disease or therapy

66
Risk Factors for MDR Pathogens
Antimicrobial therapy in preceding 90 daysPRSP but ? Pseudomonas, MRSA, Acinetobacter
High frequency of antibiotic resistance in community – MRSA but Pseudomonas, Acinetobacter
Presence of risk factors for HCAP > 2 days hospitalization in previous 90 days Nursing home or extended care facility residence
? Ambulatory vs. Trach/PEG/bedbound Home infusion therapy or wound care Chronic dialysis for > 30 days Family member with MDR
Immunosuppressive disease or therapy
MRSA but ? Pseudomonas,Acinetobacter

67
ATS/ACCP Themes/Emphasis
Clinically relevantConsistent with IDSA/ATS
CAP guidelinesExclusion of healthcare-
associated pneumonia (HCAP)Comparator drug

68
ATS/IDSA Guidelines: Hospitalized CAP
Newer fluoroquinoloneCephalosporin plus macrolide
For carefully selected patients, azithromycin alone
• Substitute doxycycline for macrolide

69
3rd Gen Cephalo
Aminoglycoside
B-lactam+Macro
Cephalo+MacroQuinolone
Treatment Outcomes Data
Gleason, Arch Intern Med, 1999

70
Clinically Relevant Need to parallel CMS/Joint Commission
standards to allow American physicians to participate
Easier IRB approval Easier to get participants to get agree to enrollment CAP process of care improvement projects have
consistently documented that increased adherence to IDSA/ATS guideline-recommended therapy is associated with lower mortality
Newer agents may demonstrate superiority to penicillin for CAP
would not be clinically relevant

71
Practical Implications Would not support placebo-controlled
trials Allow enrollment of patients who have
already received an initial dose of a once-a-day antibiotic such as ceftriaxone
Allow combination therapy for drugs which may not have atypical coverage
Shorter duration of therapy Disconnect approval for CAP from
linkage to nosocomial pneumonia

72
Mortality as an Endpoint
Unclear that antibiotics will differentially affect mortality

73
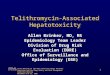
Unchanged CAP Fatality Rates
1
10
100
1000
Dea
ths
/100
,000
Pneumonia Tuberculosis Sepsis AIDS
www.cdc.gov/nchs/data
Clinical use of penicillin starts
Effective anti-TB drugs

74
Mortality as an Endpoint
Unclear that antibiotics will differentially affect mortalitySevere CAP – immunomodulationModerate CAP - ? cardiovascularMild CAP – ? bad luck

75
The Association between Pneumococcal Pneumonia and Acute Cardiac Events
0
5
10
15
20
MyoardialInfarct
CHF
Pat
ient
s
With CHFWith ArrhythmiaAlone
27.3
8.8
0
5
10
15
20
25
30
%
Mortality
Acute Cardiac None
p < 0.008OR 3.9
N=33 N=137
Musher et al, Clin Infect Dis, 2007
33/170 (19.4%) had at leastone major cardiac event

76
SCAP: Deaths Age < 5511,684 Admissions in Alberta
3
26.9 26.1
1.8
12.4
17.6
1.6
22.517.8
8.2
4743.1
0
5
10
15
20
25
30
35
40
45
50
%
ARF/RespArr MechVent Shock ICUAdm
Overall Death < 11 days All Deaths
Marrie, CID, 2003

77
Septic Shock and Respiratory Failure in CAP
PneumoniaPneumonia = 40% of septic
shock
Septic shock in approximately 15%
of CAP
RespFailure
Septic Shock
Lethal Pneumonia

78
Mortality as an Endpoint
Unclear that antibiotics will differentially affect mortality
Exception is inappropriate initial empirical antibiotics in severe CAPBut don’t know what antibiotic(s)
minimize inappropriate initial empirical since group has not been studied

79
But…

80
3rd Gen Cephalo
Aminoglycoside
B-lactam+Macro
Cephalo+MacroQuinolone
Treatment Outcomes Data
Gleason, Arch Intern Med, 1999

81
Atypical Coverage for Bacteremic CAP
• Quinolones most common monotherapy
• ? Quinolone in non-ICU, macrolide combination in critically ill 0
0.2
0.4
0.6
0.8
1
1.2
1.4
Mor
tali
ty O
dds
Rat
io
Mono Atyp Macro Quin Doxy
Hospital 30 day
* **† †
* p < 0.01, † p < 0.05Metersky, Chest, 2007

82
Combination Therapy of Bacteremic Pneumococcal CAP
0.220.3
0.4 0.42
0.29
1
0
0.2
0.4
0.6
0.8
1
Mor
talit
y O
dds
Rat
io
Waterer Mufson Martinez Baddour Weiss Harbarth

83
Combination Therapy for SCAP
No shock Shock
Hazard Ratio = 1.69 (95% CI 1.09-2.60)
p = 0.01
Difference remained if inappropriate initial therapy or deaths ininitial 48 hours are excluded
Rodriguez, Crit Care Med, 2007

84
Mortality as an Endpoint
Important endpoint Requires inclusion of severe, ICU-
admitted CAP patients Cannot be primary endpoint in
superiority trials For non-inferiority trials, margin
should be small

85
Other CAP EndpointsFor moderate CAP, clinically and financially
relevant endpoint is hospitalizationFavor use of objective criteria, such as time to
clinical stability, rather than subjective clinicalHospitalization is often used to correct other
medical issues not reliableFor intravenous-only study medication, helps
solve problem of oral continuationTools have been already been developed

86
Other CAP Endpoints• For mild CAP, clinically relevant
endpoint is return to normal activities• Favor use of Patient-Reported Outcomes
– Self limited disease, therefore assessment at a static endpoint time unlikely to demonstrate differences
– Margins suggested by IDSA committee appear reasonable and supported by prior literature

87
Biomarker Endpoints/ Entry Criteria
Procalcitonin is not FDA approved for this indicationProbably minimal impact on CAPNormal/drop in level may be supportive evidence of
“cure” but implications of persistently elevated are less obvious
FDA has been barrier to use of point-of-care tests which might improve quality of CAP trials

88
Implicit in these statements are several goals which the ATS/ACCP would strongly
support: Problem of increasing antibiotic resistance is
real and an anticipatory approach is needed Pharmaceutical industry needs clear guidelines
and the ability to be more nimble in recruiting patients
Majority of patients in these trials should be studied in healthcare systems that are similar to that of the US

89
Thank you

Antiinfective Drugs Advisory Committee, April 1, 2008Antiinfective Drugs Advisory Committee, April 1, 2008 9090
Ethical Considerations for Trials Ethical Considerations for Trials in Community Acquired in Community Acquired
PneumoniaPneumonia
Robert M. Nelson, M.D., Ph.D.Robert M. Nelson, M.D., Ph.D.Office of Pediatric TherapeuticsOffice of Pediatric Therapeutics
andandSara F. Goldkind, M.D., M.A.Sara F. Goldkind, M.D., M.A.
Good Clinical Practice ProgramGood Clinical Practice Program
Food and Drug AdministrationFood and Drug Administration

9191
Unmet Needs - AdultsUnmet Needs - Adults
66thth leading cause of death in USA leading cause of death in USA– #1 cause of death from an infectious disease in USA #1 cause of death from an infectious disease in USA
Approximately 5.6 million cases of CAP Approximately 5.6 million cases of CAP occur annually in USA, and 1.1 million occur annually in USA, and 1.1 million require hospitalizationrequire hospitalization– 80% of patients with CAP treated as outpatients: 80% of patients with CAP treated as outpatients:
mortality rate <1-5%mortality rate <1-5%– If hospitalization required: mortality rate 12% overallIf hospitalization required: mortality rate 12% overall– If ICU admission required: mortality rate 12-36%If ICU admission required: mortality rate 12-36%

UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006 9292
Unmet Needs - ChildrenUnmet Needs - Children
Over 2 million deaths per year

UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006 9393
Unmet Needs - ChildrenUnmet Needs - Children

9494
Outline of DiscussionOutline of Discussion
The Ethical Requirement of Scientific ValidityThe Ethical Requirement of Scientific Validity– Choice of Control Group; Assay Sensitivity; Non-Choice of Control Group; Assay Sensitivity; Non-
Inferiority and Superiority (Placebo) DesignsInferiority and Superiority (Placebo) Designs
Ethical Balance of Risk and BenefitEthical Balance of Risk and Benefit– Withholding Known Effective TreatmentWithholding Known Effective Treatment
Design Modification and other issues in Adult Design Modification and other issues in Adult and Pediatric Studies of Antibiotics for CAPand Pediatric Studies of Antibiotics for CAPConclusion: Ethical and Scientific StandardConclusion: Ethical and Scientific Standard

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 9595
Choice of Control GroupChoice of Control GroupA Critical Decision affecting…A Critical Decision affecting…– Possible Inferences; Ethical Acceptability; Possible Inferences; Ethical Acceptability;
Minimizing Bias; Subjects and Recruitment; Minimizing Bias; Subjects and Recruitment; Endpoints; Credibility of Results; Acceptability Endpoints; Credibility of Results; Acceptability to Regulatory Authorities; Other Features of to Regulatory Authorities; Other Features of Study, Conduct and Interpretation.Study, Conduct and Interpretation.
Key to Scientific Validity (Causal Inference)Key to Scientific Validity (Causal Inference)– Allows for discrimination of patient outcomes Allows for discrimination of patient outcomes
causedcaused by the test treatment from outcomes by the test treatment from outcomes caused by other factors, such as the natural caused by other factors, such as the natural progression of the disease, observer or patient progression of the disease, observer or patient expectations, or other treatment.expectations, or other treatment.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 9696
Types of Control GroupsTypes of Control Groups
Concurrent Control (control/test groups Concurrent Control (control/test groups chosen from same population, usually by chosen from same population, usually by randomization, and treated concurrently)randomization, and treated concurrently)– Placebo (two or three-arm study)Placebo (two or three-arm study)– Active (Positive)Active (Positive)– Dose-Response (different dose or regimen of study Dose-Response (different dose or regimen of study
treatment)treatment)– No treatment (not blinded)No treatment (not blinded)
External (including historical) Controls, External (including historical) Controls, regardless of comparator treatmentregardless of comparator treatment

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 9797
External or Non-concurrent External or Non-concurrent ControlsControls
There are serious concerns about the There are serious concerns about the ability of trials using external (including ability of trials using external (including historical) controls, regardless of historical) controls, regardless of comparator treatment, to ensure the comparator treatment, to ensure the comparability of test and control groups, comparability of test and control groups, and to minimize important biases.and to minimize important biases.
Thus, this is an unacceptable study design Thus, this is an unacceptable study design for antibiotic efficacy studies for CAP.for antibiotic efficacy studies for CAP.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 9898
Dose-Response DesignDose-Response DesignAntibiotic trials may compare two regimens Antibiotic trials may compare two regimens (e.g., short vs. long treatment course) using (e.g., short vs. long treatment course) using eithereither superiority or non-inferiority design superiority or non-inferiority design (thus, similar issues as (thus, similar issues as active control trialsactive control trials).).Choice of the lower dose (or shorter course) Choice of the lower dose (or shorter course) must be a fair comparison since trial must be a fair comparison since trial conditions should not favor one treatment conditions should not favor one treatment over the other. If not, cannot assure assay over the other. If not, cannot assure assay sensitivity, and may raise similar ethical sensitivity, and may raise similar ethical concerns as concerns as placebo controlsplacebo controls..

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 9999
Focus: Active/Placebo ControlsFocus: Active/Placebo Controls
Two Approaches to Establish EfficacyTwo Approaches to Establish EfficacySuperioritySuperiority of test treatment to control of test treatment to control (whether placebo or active control)(whether placebo or active control)
SimilaritySimilarity of test treatment to known of test treatment to known effective treatment (active control)effective treatment (active control)– Equivalence (i.e., equally effective)Equivalence (i.e., equally effective)– Non-inferiority (i.e., not less effective by NIM)Non-inferiority (i.e., not less effective by NIM)– Key assumptionKey assumption: active control is effective : active control is effective
under trial conditions (i.e., assay sensitivity)under trial conditions (i.e., assay sensitivity)

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 100100
Assay SensitivityAssay Sensitivity
Definition: the ability of a clinical trial Definition: the ability of a clinical trial to distinguish effective treatment from to distinguish effective treatment from less effective or ineffective treatment.less effective or ineffective treatment.
Lack of assay sensitivity has different Lack of assay sensitivity has different implications for superiority and non-implications for superiority and non-inferiority trials.inferiority trials.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 101101
Assay SensitivityAssay SensitivitySuperiority TrialSuperiority Trial– If superiority trial lacks assay sensitivity, it will fail If superiority trial lacks assay sensitivity, it will fail
to show that test treatment is superior and will to show that test treatment is superior and will fail to lead to conclusion of efficacy.fail to lead to conclusion of efficacy.
– When one treatment is shown to be superior, that When one treatment is shown to be superior, that finding itself establishes assay sensitivity.finding itself establishes assay sensitivity.
Non-Inferiority (NI) TrialNon-Inferiority (NI) Trial– If non-inferiority trial lacks assay sensitivity, trial If non-inferiority trial lacks assay sensitivity, trial
may find ineffective treatment to be non-inferior; may find ineffective treatment to be non-inferior; could lead to erroneous conclusion of efficacy.could lead to erroneous conclusion of efficacy.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 102102
Assay Sensitivity in NI TrialsAssay Sensitivity in NI Trials
Inferred from two determinations:Inferred from two determinations:1)1) Historical evidence of sensitivity to drug Historical evidence of sensitivity to drug
effects (HESDE)effects (HESDE), i.e., similarly designed past , i.e., similarly designed past trials regularly distinguish effective from less trials regularly distinguish effective from less effective or ineffective treatments; and,effective or ineffective treatments; and,
2)2) Appropriate trial conductAppropriate trial conduct, i.e., conduct of trial , i.e., conduct of trial did not undermine ability to distinguish did not undermine ability to distinguish effective from less effective or ineffective effective from less effective or ineffective treatments (IDSA: “constancy assumption”?).treatments (IDSA: “constancy assumption”?).

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 103103
(1) HESDE(1) HESDE
Evaluate Evaluate beforebefore beginning non-inferiority trial beginning non-inferiority trial
Appropriately designed and conducted trials using Appropriately designed and conducted trials using specific treatment (or other treatments with similar specific treatment (or other treatments with similar effects) to be used as the active control must show effects) to be used as the active control must show treatment effect (optimally, superior to placebo).treatment effect (optimally, superior to placebo).
Without well-supported historical evidence of Without well-supported historical evidence of sensitivity to drug effects, demonstration of efficacy sensitivity to drug effects, demonstration of efficacy using non-inferiority trial design is not possible and using non-inferiority trial design is not possible and should not be attempted.should not be attempted.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 104104
Choosing a Non-Inferiority Margin (NIM)Choosing a Non-Inferiority Margin (NIM)
NIM: degree of inferiority of test treatment to NIM: degree of inferiority of test treatment to control (delta) that trial will attempt to exclude control (delta) that trial will attempt to exclude statistically.statistically.
NIM NIM ≤≤ smallest effect size that active drug smallest effect size that active drug would reliably be expected to have compared would reliably be expected to have compared with placebo in the setting of the planned trial.with placebo in the setting of the planned trial.– onlyonly possible when there is historical evidence of sensitivity possible when there is historical evidence of sensitivity
to drug effects.to drug effects.– requires requires measure of superiority of active treatment to controlmeasure of superiority of active treatment to control, ,
not uncontrolled measures (e.g., change from baseline).not uncontrolled measures (e.g., change from baseline).

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 105105
(2) Appropriate Trial Design & Conduct(2) Appropriate Trial Design & Conduct
Can only be fully evaluated Can only be fully evaluated afterafter the non- the non-inferiority trial is completed. inferiority trial is completed.
Planned non-inferiority trial must share critical Planned non-inferiority trial must share critical design characteristics with the historical trials design characteristics with the historical trials used to determine that evidence of sensitivity to used to determine that evidence of sensitivity to drug effects exists.drug effects exists.
Trial conduct should adhere closely to that of Trial conduct should adhere closely to that of the historical trials and should be of high quality the historical trials and should be of high quality (e.g. good compliance, few losses to follow-up).(e.g. good compliance, few losses to follow-up).

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 106106
Scrupulous Trial Conduct may be Scrupulous Trial Conduct may be necessary for Assay Sensitivitynecessary for Assay Sensitivity
For non-inferiority trials, may be weaker For non-inferiority trials, may be weaker stimulus to engage in efforts to ensure study stimulus to engage in efforts to ensure study qualityquality– Errors that diminish observed treatment differences (e.g., Errors that diminish observed treatment differences (e.g.,
poor compliance, high placebo response, concomitant poor compliance, high placebo response, concomitant treatment, misclassification of outcomes) may undermine treatment, misclassification of outcomes) may undermine preservation of assay sensitivity. preservation of assay sensitivity.
– Some trial errors can increase variance, thus decreasing Some trial errors can increase variance, thus decreasing likelihood of showing non-inferiority by widening likelihood of showing non-inferiority by widening confidence interval (e.g., poor measurement technique).confidence interval (e.g., poor measurement technique).

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 107107
Non-Inferiority Trial Conduct?Non-Inferiority Trial Conduct?Review non-inferiority trial conduct for factors Review non-inferiority trial conduct for factors that that – might obscure differences between treatmentsmight obscure differences between treatments
E.g., observed differences in populations enrolled, use of E.g., observed differences in populations enrolled, use of concomitant therapies, compliance with therapy, and extent of, and concomitant therapies, compliance with therapy, and extent of, and reasons for, subjects dropping out?reasons for, subjects dropping out?
– might make the trial different from the trials that provided the might make the trial different from the trials that provided the basis for determining the NIM.basis for determining the NIM.
E.g., atypical outcomes with active control treatment (e.g., unusually E.g., atypical outcomes with active control treatment (e.g., unusually high or low antibiotic cure rate) can indicate important differences high or low antibiotic cure rate) can indicate important differences which undermined assay sensitivity.which undermined assay sensitivity.
Concurrent trial monitoring may be necessary to Concurrent trial monitoring may be necessary to minimize risk and assure adequate trial conductminimize risk and assure adequate trial conduct

108108
Given these problems with NI designs, Given these problems with NI designs, why not an AC superiority design?why not an AC superiority design?
Scientific and Policy ConcernsScientific and Policy Concerns– In spite of questions about specifying a reliable In spite of questions about specifying a reliable
treatment effect (i.e., NIM) based on past experience, treatment effect (i.e., NIM) based on past experience, antibiotics are generally highly effective. Thus, a antibiotics are generally highly effective. Thus, a superiority design may require a larger sample size superiority design may require a larger sample size than a non-inferiority trial (depending on the margin).than a non-inferiority trial (depending on the margin).
– There may be other advantages of new over existing There may be other advantages of new over existing antibiotics that may not be captured by an actively antibiotics that may not be captured by an actively controlled superiority study to establish efficacy (such controlled superiority study to establish efficacy (such as different resistance profiles, improved safety, ease of as different resistance profiles, improved safety, ease of administration, formulation advantages, cost, etc.)administration, formulation advantages, cost, etc.)

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 109109
Ethical preference for AC trial designs?Ethical preference for AC trial designs?
Active control trials may pose fewer ethical Active control trials may pose fewer ethical problems than placebo-controlled trials because all problems than placebo-controlled trials because all subjects receive active treatment. subjects receive active treatment. – But subjects receiving a new treatment are not receiving standard But subjects receiving a new treatment are not receiving standard
therapy and thus may be receiving an ineffective or harmful drug. therapy and thus may be receiving an ineffective or harmful drug.
If active control therapy improves survival or If active control therapy improves survival or decreases irreversible morbidity, withholding of decreases irreversible morbidity, withholding of such treatment from experimental group raise such treatment from experimental group raise same concerns that render placebo control same concerns that render placebo control unacceptable.unacceptable.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 110110
Placebo Control (or Superiority Design) may assure Placebo Control (or Superiority Design) may assure Assay Sensitivity, but can it meet ethical guidelines?Assay Sensitivity, but can it meet ethical guidelines?
Placebo-controlled trial for efficacy is as free of assumptions Placebo-controlled trial for efficacy is as free of assumptions and reliance on external information as possible.and reliance on external information as possible.
Most problems in design or conduct of placebo-controlled Most problems in design or conduct of placebo-controlled trial increase likelihood of failure to demonstrate treatment trial increase likelihood of failure to demonstrate treatment difference (and thereby establish efficacy), so trial contains difference (and thereby establish efficacy), so trial contains built-in incentives for excellence.built-in incentives for excellence.
When primary purpose of trial is comparison of two active When primary purpose of trial is comparison of two active agents, addition of placebo control provides an internal agents, addition of placebo control provides an internal standard that enhances inferences that can be drawn. standard that enhances inferences that can be drawn. However, ethical issues with use of placebo control remain a However, ethical issues with use of placebo control remain a concern with three-arm design.concern with three-arm design.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 111111
Ethical Issues with Placebo Ethical Issues with Placebo ControlsControls
Where an available treatment is known to prevent Where an available treatment is known to prevent serious harm, such as death or irreversible serious harm, such as death or irreversible morbidity, it is generally inappropriate to use a morbidity, it is generally inappropriate to use a placebo control. There are exceptions, however, placebo control. There are exceptions, however, such as when standard therapy has such severe such as when standard therapy has such severe toxicity that many patients refuse to receive it.toxicity that many patients refuse to receive it.
When a new treatment is tested for a condition for When a new treatment is tested for a condition for which no effective treatment is known, there is which no effective treatment is known, there is usually no ethical problem with a study comparing usually no ethical problem with a study comparing the new treatment to placebo. the new treatment to placebo.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 112112
Ethical Issues with Placebo Ethical Issues with Placebo ControlsControls
When there is no serious harm, it is generally When there is no serious harm, it is generally considered ethical to ask patients to considered ethical to ask patients to participate in a placebo-controlled trial, even participate in a placebo-controlled trial, even if they may experience discomfort, assuming if they may experience discomfort, assuming adequate informed and voluntary consent.adequate informed and voluntary consent.
Can a randomized placebo-controlled trial for Can a randomized placebo-controlled trial for community acquired pneumonia in adult and community acquired pneumonia in adult and pediatric patients meet this standard?pediatric patients meet this standard?

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 113113

http://www.wma.net/e/policy/b3.htmhttp://www.wma.net/e/policy/b3.htm 114114
Debate over Placebo Controls: Debate over Placebo Controls: Paragraph 29. WMA Declaration of Helsinki (2000)Paragraph 29. WMA Declaration of Helsinki (2000)
““The benefits, risks, burdens and The benefits, risks, burdens and effectiveness of a new method should be effectiveness of a new method should be tested against those of the best current tested against those of the best current prophylactic, diagnostic, and therapeutic prophylactic, diagnostic, and therapeutic methods. This does not exclude the use of methods. This does not exclude the use of placebo, or no treatment, in studies where no placebo, or no treatment, in studies where no proven prophylactic, diagnostic or therapeutic proven prophylactic, diagnostic or therapeutic method exists.”method exists.”

Added by the WMA General Assembly, Washington 2002 (http://www.wma.net/e/policy/b3.htm)Added by the WMA General Assembly, Washington 2002 (http://www.wma.net/e/policy/b3.htm) 115115
Note of Clarification on Paragraph 29Note of Clarification on Paragraph 29
““The WMA hereby reaffirms its position that The WMA hereby reaffirms its position that extreme care must be taken in making use of a extreme care must be taken in making use of a placebo-controlled trial and that in general this placebo-controlled trial and that in general this methodology should only be used in the methodology should only be used in the absence of existing proven therapy. However, a absence of existing proven therapy. However, a placebo-controlled trial may be ethically placebo-controlled trial may be ethically acceptable, even if proven therapy is available, acceptable, even if proven therapy is available, under the following circumstances…”under the following circumstances…”

Added by the WMA General Assembly, Washington 2002 (http://www.wma.net/e/policy/b3.htm)Added by the WMA General Assembly, Washington 2002 (http://www.wma.net/e/policy/b3.htm) 116116
Note of Clarification on Paragraph 29Note of Clarification on Paragraph 29
““However, a placebo-controlled trial may be However, a placebo-controlled trial may be ethically acceptable, even if proven therapy is ethically acceptable, even if proven therapy is available, under the following circumstances:available, under the following circumstances:– ““Where for compelling and scientifically sound Where for compelling and scientifically sound
methodological reasons its use is necessary to determine methodological reasons its use is necessary to determine the efficacy or safety of a prophylactic, diagnostic or the efficacy or safety of a prophylactic, diagnostic or therapeutic method; therapeutic method; oror
– ““Where a prophylactic, diagnostic or therapeutic method is Where a prophylactic, diagnostic or therapeutic method is being investigated for being investigated for a minor conditiona minor condition and the patients and the patients who receive placebo will who receive placebo will not be subject to any additional not be subject to any additional risk of serious or irreversible harmrisk of serious or irreversible harm.”.”

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 117117
Choice of control in clinical trialsChoice of control in clinical trials
““As a general rule, research subjects in As a general rule, research subjects in the control group of a trial of a diagnostic, the control group of a trial of a diagnostic, therapeutic, or preventive intervention therapeutic, or preventive intervention should receive an established effective should receive an established effective intervention. In some circumstances it may intervention. In some circumstances it may be ethically acceptable to use an be ethically acceptable to use an alternative comparator, such as placebo or alternative comparator, such as placebo or "no treatment"."no treatment".

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 118118
Choice of control in clinical trialsChoice of control in clinical trials““Placebo may be used:Placebo may be used:– ““When there is no established effective intervention;When there is no established effective intervention;– ““When withholding an established effective intervention would When withholding an established effective intervention would
expose subjects to, at most, temporary discomfort or delay in expose subjects to, at most, temporary discomfort or delay in relief of symptoms;relief of symptoms;
– ““When use of an established effective intervention as When use of an established effective intervention as comparator would not yield scientifically reliable results comparator would not yield scientifically reliable results andand use of placebo would not add any risk of serious or use of placebo would not add any risk of serious or irreversible harm to the subjects.”irreversible harm to the subjects.”
A placebo-controlled trial for CAP may be ethical A placebo-controlled trial for CAP may be ethical IFIF the use of placebo would not add the use of placebo would not add any riskany risk of of serious or irreversible harm to the subjects.serious or irreversible harm to the subjects.

E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001E-10 Choice of Control Group and Related Issues in Clinical Trials, May 2001 119119
Design Modifications and Using Other Controls Design Modifications and Using Other Controls That May Resolve Ethical (and Other) IssuesThat May Resolve Ethical (and Other) Issues
Additional Control GroupsAdditional Control Groups– Three-arm Trial; Placebo and Active ControlThree-arm Trial; Placebo and Active Control– Additional DosesAdditional Doses– Factorial DesignsFactorial Designs
Other Modifications of Study DesignOther Modifications of Study Design– Add on Study, Placebo-Controlled; Replacement Study.Add on Study, Placebo-Controlled; Replacement Study.– Early Escape; Rescue TreatmentEarly Escape; Rescue Treatment– Limited Placebo PeriodLimited Placebo Period– Randomized WithdrawalRandomized Withdrawal
Appear of limited application to antibiotic Appear of limited application to antibiotic trials.trials.

120120
Adult Studies of Adult Studies of Antibiotics for CAPAntibiotics for CAP

121121
Alter risks based upon choice of Alter risks based upon choice of study populationstudy population
An ethical study requires both:An ethical study requires both:– Minimization of risks to enrolled subjectsMinimization of risks to enrolled subjects– Maximization of scientific validity (assay Maximization of scientific validity (assay
sensitivity and study design)sensitivity and study design)Choice of study populationChoice of study population
How can these two goals best be achieved?How can these two goals best be achieved?– Tailoring study population with more rigorous Tailoring study population with more rigorous
entry criteria, butentry criteria, but– This may affect generalizability of resultsThis may affect generalizability of results

122122
CAP: study in adultsCAP: study in adultsHeterogeneous populationHeterogeneous populationSome factors that influence course, Some factors that influence course, response, and mortalityresponse, and mortality– Elderly (>65 y/o)Elderly (>65 y/o)– SmokersSmokers– Outpatient vs. inpatient (ward vs. ICU)Outpatient vs. inpatient (ward vs. ICU)– USA vs outside USAUSA vs outside USA– Co-morbiditiesCo-morbidities– Functional statusFunctional status– Virulence of the infectious organism and Virulence of the infectious organism and
antibiotic resistance profileantibiotic resistance profile

123123
Clinical diagnosis based upon symptoms Clinical diagnosis based upon symptoms and signs -- empiric therapyand signs -- empiric therapyCombination of clinical presentation and Combination of clinical presentation and radiographic findings -- empiric therapyradiographic findings -- empiric therapyEmpiric therapy is influenced by standard-Empiric therapy is influenced by standard-of-care for that regionof-care for that regionPathogen-directed therapyPathogen-directed therapy– Prevalence of resistant organisms (in a given Prevalence of resistant organisms (in a given
local)local)– Associated complexitiesAssociated complexities
CAP: study in adultsCAP: study in adults

124124
Minimization of RiskMinimization of Risk
Primary imperative is to minimize Primary imperative is to minimize research-related risks to subjects without research-related risks to subjects without compromising reliability of research results compromising reliability of research results upon which to base safety and efficacy upon which to base safety and efficacy claimsclaims– Enroll a less sick study populationEnroll a less sick study population– Enroll a study population with ease of access Enroll a study population with ease of access
to health care including on-going monitoring to health care including on-going monitoring (clinical improvement usually occurs by day 3) (clinical improvement usually occurs by day 3) and follow-up (at 6 wks)and follow-up (at 6 wks)

125125
Minimization of RiskMinimization of RiskIf a less sick study population is selected can onset of If a less sick study population is selected can onset of antibiotic treatment be delayed to mimic PCT?antibiotic treatment be delayed to mimic PCT?– Will this choice of study population provide useful information Will this choice of study population provide useful information
(meaningful endpoint) in light of PCT studies that have already (meaningful endpoint) in light of PCT studies that have already been done on young, low-risk, clinically stable outpatients with been done on young, low-risk, clinically stable outpatients with mild CAP? mild CAP?
– Some data demonstrate that antibiotic administration within 8 Some data demonstrate that antibiotic administration within 8 hours of hospital arrival was associated with a significantly lower hours of hospital arrival was associated with a significantly lower 30-day mortality and length of hospital stay in both unadjusted 30-day mortality and length of hospital stay in both unadjusted and adjusted (for patient risk status) analyses; for those who did and adjusted (for patient risk status) analyses; for those who did not receive pre-hospital antibiotics, 4 hours was associated with not receive pre-hospital antibiotics, 4 hours was associated with decreased mortality & length of hospital stay {Multi-center decreased mortality & length of hospital stay {Multi-center retrospective cohort study of 14,069 hospitalized elderly patients retrospective cohort study of 14,069 hospitalized elderly patients with pneumonia} Can a delay in treatment be justified?with pneumonia} Can a delay in treatment be justified?
– Although there are prognostic scoring systems (PSI, CURB, Although there are prognostic scoring systems (PSI, CURB, CURB-65) they do not account for all factors contributing to CURB-65) they do not account for all factors contributing to disease severity.disease severity.

126126
Scientific validityScientific validity
Enrich the study population with responders (e.g., Enrich the study population with responders (e.g., subjects who meet the criteria for a pathogen-directed subjects who meet the criteria for a pathogen-directed therapy)therapy)– The only randomized controlled trial of diagnostic strategy in CAP The only randomized controlled trial of diagnostic strategy in CAP
demonstrated no statistically significant differences in mortality demonstrated no statistically significant differences in mortality rate of length of hospital stay between patients receiving rate of length of hospital stay between patients receiving pathogen-directed therapy and patients receiving empirical pathogen-directed therapy and patients receiving empirical therapy [IDSA/ATS Guidelines for CAP in Adults, 2007]therapy [IDSA/ATS Guidelines for CAP in Adults, 2007]
– Even when extensive diagnostic testing is used, causative Even when extensive diagnostic testing is used, causative pathogen cannot be identified in up to 50% of cases [ATS pathogen cannot be identified in up to 50% of cases [ATS Guidelines for Management of Adults with CAP, 2001]Guidelines for Management of Adults with CAP, 2001]
Given low virulence of atypical and viral pathogens, and Given low virulence of atypical and viral pathogens, and effectiveness of approved antibiotics, will studying mild to effectiveness of approved antibiotics, will studying mild to moderate CAP give reliable results?moderate CAP give reliable results?

127127
Generalizability of ResultsGeneralizability of Results
Ability to generalize study results to the Ability to generalize study results to the projected use population projected use population – Variations in standard-of-care Variations in standard-of-care
Local vs. universal standardsLocal vs. universal standards
– Differing prevalence of bacterial pathogens Differing prevalence of bacterial pathogens (including resistant organisms)(including resistant organisms)
– Nuanced approaches to CAP (e.g., US Nuanced approaches to CAP (e.g., US outpatient therapy addresses broad outpatient therapy addresses broad antimicrobial coverage; European approach antimicrobial coverage; European approach focuses on empiric therapy for S. pneumoniafocuses on empiric therapy for S. pneumonia

128128
Additional Issues from Additional Issues from Pediatric Studies of Pediatric Studies of Antibiotics for CAPAntibiotics for CAP

World Health Organization, Pocket Book of Hospital care for children 2005World Health Organization, Pocket Book of Hospital care for children 2005 129129
WHO Classification of PneumoniaWHO Classification of Pneumonia

UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006 130130

Agarwal et al BMJ 2004Agarwal et al BMJ 2004 131131

Ashgar et al BMJ 2008Ashgar et al BMJ 2008 132132

UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006UNICEF/WHO, Pneumonia: The forgotten killer of children, 2006 133133

Hazir et al Lancet 2008Hazir et al Lancet 2008 134134

135135
Wide Agreement on Ethical Wide Agreement on Ethical PrinciplesPrinciples
Research involving children Research involving children eithereither must present a must present a balance of risks and potential benefits comparable balance of risks and potential benefits comparable to the available alternatives (21 CFR 50.52), to the available alternatives (21 CFR 50.52), oror be be restricted to “minimal (or low) risk” absent direct restricted to “minimal (or low) risk” absent direct benefit to child (21 CFR 50.51 or 53).benefit to child (21 CFR 50.51 or 53).Under 21 CFR 50, Subpart D, withholding known Under 21 CFR 50, Subpart D, withholding known effective treatment from children enrolled in a effective treatment from children enrolled in a control group must present no more than a “minor control group must present no more than a “minor increase over minimal risk.”increase over minimal risk.”

136136
Ethical Standard for Choice of Control Ethical Standard for Choice of Control Group in CAP Clinical TrialsGroup in CAP Clinical Trials
There are concerns that the use of an established effective There are concerns that the use of an established effective intervention as the comparator in a NIM design would not intervention as the comparator in a NIM design would not yield scientifically reliable results, lending credence to the yield scientifically reliable results, lending credence to the need for either active superiority or placebo controlled trial need for either active superiority or placebo controlled trial designs. The scientific ability to set a credible NIM is key to designs. The scientific ability to set a credible NIM is key to the resolution of this discussion.the resolution of this discussion.A placebo-controlled trial for CAP would only be ethical A placebo-controlled trial for CAP would only be ethical IFIF the use of a placebo would not add the use of a placebo would not add any riskany risk of serious or of serious or irreversible harm to the subjects. There are doubts that a irreversible harm to the subjects. There are doubts that a CAP trial could be designed to meet this standard.CAP trial could be designed to meet this standard.Cautionary note: “Where a placebo-controlled trial is Cautionary note: “Where a placebo-controlled trial is unethical and an active control trial would not be credible, it unethical and an active control trial would not be credible, it may be very difficult to study new drugs at all.” (ICH E-10) may be very difficult to study new drugs at all.” (ICH E-10)

137137
ChallengesChallengesActive Control TrialsActive Control Trials– Assure scientific validity with eitherAssure scientific validity with either
Selection of an appropriate NIM combined with meticulous trial Selection of an appropriate NIM combined with meticulous trial conduct using non-inferiority design, orconduct using non-inferiority design, or
Use of a superiority design.Use of a superiority design.
Placebo Control TrialsPlacebo Control Trials– Assure ethical treatment of subjects by avoiding any risk of Assure ethical treatment of subjects by avoiding any risk of
serious or irreversible harm.serious or irreversible harm.
All trials must meet the dual ethical All trials must meet the dual ethical requirements of (1) scientific validity and (2) an requirements of (1) scientific validity and (2) an appropriate balance of risk and potential appropriate balance of risk and potential benefit.benefit.

Odysseus vor Scilla und Charybdis, Johann Heinrich Füssli, 1794-1796Odysseus vor Scilla und Charybdis, Johann Heinrich Füssli, 1794-1796 138138
“Of these two rocks the one reaches heaven and its peak is lost in a dark cloud.… [There] Scylla sits…, a dreadful monster [that] no one - not even a god - could face…without being terror-struck.…No ship ever yet got past her without losing some men, for she shoots out all her heads at once, and carries off a man in each mouth.”
“[With] the other rocks [lies] the sucking whirlpool of Charybdis. Three times [a] day…she vomit[s] forth her waters, and three times she sucks them down again; see that you be not there when she is sucking, for if you are, Neptune himself could not save you; you must hug the Scylla side and drive ship by as fast as you can, for you had better lose six men than your whole crew.”
““Is there no way,”' said I, “of escaping Charybdis, and… keeping Scylla off when she is trying to harm my men?” “You dare-devil,” replied the goddess, …you will not let yourself be beaten even by the immortals.”

Issues in Non-Inferiority Trials
in CAP
April 1, 2008
Thomas R. Fleming, Ph.D. Professor of Biostatistics
University of Washington
Fleming TR. Statistics in Medicine, 2008, Vol 27, #3 Fleming TR, Powers JH. “Issues in NI Trials in CAP”, to appear
FDA Anti Infective Drugs Advisory Committee

Motivation for Non-Inferiority
~ Classic setting: Experimental (EXP) has favorable profile relative to Standard (STD) in
• side effects• convenience of administration• cost
~ Ethical approach
Eg : STD EXP SETTING Amphotericin B Voriconazole Invasive Aspergillosis
Penicillin New Quinolone CAP “076” ZDV Nevirapine MCT of HIV

Dual Goals of Non-Inferiority Trials
• To enable a direct evaluation of the clinical efficacy/safety
of EXP relative to STD
• To contribute evidence to the evaluation of efficacy/safety
of EXP relative to PLA

Non-Inferiority Trials… Some Requirements
ICH E9: STD should have clinical efficacy
• that is of substantial magnitude
• that is precisely estimated
• with estimates that are relevant to the setting in which the non-inferiority trial
is being conducted
e.g., EXP vs. Vancomycin in patients with VRE

Factors invalidating Constancy Assumption(EXP vs. STD NI Trial vs. Trials evaluating STD)
patient characteristicse.g., Disease caused by pathogens resistant to STD in NI Trial
use of supportive caree.g., Enhanced concomitant Rx attenuates effect of STD in NI Trial
dose, schedule, level of adherencee.g., Lower adherence to STD in NI trial
efficacy and safety endpoints ~ definition ~ validation process ~ missing data
…..as in maintaining conditions of a lab experiment…

Illustration CAP NI Trial: Choice of Margin
New Quinolone (EXP) vs. Penicillin (STD) in Community Acquired Pneumonia (Pneumococcal pneumonia)
NON-INFERIORITY TRIAL Failure
New Quinolone 38 / 150 ( 25% ) Penicillin 30 / 150 ( 20% )
(EXP ─ STD) 95% C. I. : ( ─5%, 15% )
PENICILLIN TRIAL Failure
Placebo 87 / 175 ( 50% ) Penicillin 35 / 175 ( 20% )
(PLA ─ STD) 95% C.I. : ( 20%, 40% )

Failure Probability
0% 10% 20% 30% 40%
EXP better
EXP compared with STD
STD better
% Failure
(EXP - STD)
EXP - STD

Factors Influencing the Choice of Marginand Interpretation of NI Trial Results
• Effect of the STD regimen
• Clinical Relevance of Reduction in Efficacy

Illustration CAP NI Trial: Choice of Margin
New Quinolone (EXP) vs. Penicillin (STD) in Community Acquired Pneumonia (Pneumococcal pneumonia)
NON-INFERIORITY TRIAL Failure
New Quinolone 38 / 150 ( 25% ) Penicillin 30 / 150 ( 20% )
(EXP ─ STD) 95% C. I. : ( ─5%, 15% )
PENICILLIN TRIAL Failure
Placebo 87 / 175 ( 50% ) Penicillin 35 / 175 ( 20% )
(PLA ─ STD) 95% C.I. : ( 20%, 40% )

Failure Probability
0% 10% 20% 30% 40%
Placebo better
Placebo compared with STD
STD better
% Failure
(Placebo - STD)
Placebo - STD meta-analysis
Margin of STD benefit
EXP - STD

Failure Probability
0% 10% 20% 30% 40%
Placebo better
Placebo compared with STD
STD better
% Failure
(Placebo - STD)
Placebo - STD meta-analysis
50% of STD benefit
Margin of STD benefit
EXP - STD

Factors Influencing the Choice of Marginand Interpretation of NI Trial Results
• Effect of the STD regimen
• Clinical Relevance of Reduction in Efficacy

Factors Influencing Choice of Margin
• Clinical importance of:
─ a reduction in efficacy
─ taking into consideration…
safety/tolerance profile resistance or drug/drug interactions convenience of administration

Failure Probability
0% 10% 20% 30% 40%
Placebo better
Placebo compared with STD
STD better
% Failure
(Placebo - STD)
Placebo - STD meta-analysis
50% of STD benefit
Margin of STD benefit
EXP - STD

Suppose a NI trial is positive…What is the Conclusion about Efficacy?
• The EXP regimen is “at least as good as” the STD regimen…
• The EXP regimen is“not worse than” the STD regimen…

Illustration CAP NI Trial: Choice of Margin
New Quinolone (EXP) vs. Penicillin (STD) in Community Acquired Pneumonia (Pneumococcal pneumonia)
NON-INFERIORITY TRIAL Failure
New Quinolone 375 / 1500 ( 25% ) Penicillin 300 / 1500 ( 20% )
(EXP ─ STD) 95% C. I. : ( 2%, 8% )
PENICILLIN TRIAL Failure
Placebo 87 / 175 ( 50% ) Penicillin 35 / 175 ( 20% )
(PLA ─ STD) 95% C.I. : ( 20%, 40% )

Failure Probability
0% 10% 20% 30% 40%
Placebo better
Placebo compared with STD
STD better
% Failure
(Placebo - STD)
Placebo - STD meta-analysis
50% of STD benefit
Margin of STD benefit
EXP - STD

Suppose a NI trial is positive…What is the Conclusion about Efficacy?
• The EXP regimen is “at least as good as” the STD regimen…
• The EXP regimen is“not worse than” the STD regimen…

Suppose a NI trial is positive…What is the Conclusion about Efficacy?
• The EXP regimen is “at least as good as” the STD regimen… NO!
• The EXP regimen is“not worse than” the STD regimen… NO!
• The EXP regimen is“not meaningfully worse than”
the STD regimen

Challenges in Non-Inferiority Trials in CAP
Not simply,
“Are STD antibiotics effective at all in CAP?
Rather: we need to determine…
what is the magnitude of effect of STD?
on what clinically important outcome measures?
in what population?
in what experimental conditions?

Issues in Design of Non-Inferiority Trials in CAP
• Choice of Endpoint
• Addressing Confounding due toLack of Randomized Trials evaluating STD
• Literature Review to Derive Margins for Non-Inferiority Trials in CAP
• Conclusions

160
Lack of Utility of Microbiological Endpoints
• “In a considerable number of bacteremic patients, death occurred in spite of repeatedly negative blood cultures following therapy, even including the heart’s blood in those who came to autopsy. Many of them died with purulent focal complications.”
Finland M et al, Ann Intern Med 1940

161
Lack of Utility of Defervescence as an Endpoint
“The temperature became normal in three days in about half of treated cases compared with about a quarter of controls...but a secondary pyrexia was fairly common and was considered quite usual… The average duration of pyrexia in hospital was little affected by the drug, the figures being 4.8 and 5.6 days for treated and control groups.”
Agranat A.L. et al., Lancet 1939.

162
Lack of Utility of Defervescence as an Endpoint
• Raising or lowering body temperature may not reflect overall benefits/risks in treatment of pneumonia
• Antipyretics (acetaminophen, non-steroidal anti-inflammatory drugs) can lower body temperature but do not affect
other aspects of pneumonia (mortality, symptoms)
• Serum therapy resulted in
febrile reactions in 26% to 44% of subjects but
decreased mortality compared to no specific treatment
Finland and Brown, Am J Med Sci 1939, p 151, p351, p389

What are Potential Endpoints?
• All-cause mortality
• Decrease in complications – empyema, meningitis, endocarditis
• Resolution of symptoms – cough, dyspnea, chest pain, fatigue
• Biomarkers – resolution of chest x-ray, physical findings such
as rales, body temperature, WBC, etc.

164
Outcomes Dependent on Measurement Methods
• Median time to resolution of cough 14 days– Metlay JP et al Respir Med 1998; 92:1137-42.
• 20% of patients report substantial fatigue at 3 months from time of initial diagnosis
– Metlay JP et al J Gen Intern Med 1997; 12:423-30.
• Not consistent with rapid resolution of fatigue in single trial (different form of measurement?)
– Kingston JR et al JAMA 1961; 176:118-123.

165
Outcomes
“Studies of patients with community-acquired pneumonia have established certain expected rates of outcomes, including mortality, clinical complications, and time to resolution of symptoms….However, there are no well-controlled studies that provide definitive estimates of the magnitude of the impact of antimicrobial therapy on these outcomes for patients with community-acquired pneumonia.”
Metlay JP and Singer DE Clin Micro Infect 2002

166
Impact of Age on Outcome
Dowling H.F. et al Am J Med Sci 1951.Dowling H.F. et al Am J Med Sci 1951.

Issues in Design of Non-Inferiority Trials in CAP
• Choice of Endpoint
• Addressing Confounding due to Lack of Randomized Trials evaluating STD
• Literature Review to Derive Margins for Non-Inferiority Trials in CAP
• Conclusions

168
Importance of Baseline Comparability
• “Any presentation concerning mortality from pneumonia is incomplete if it fails to consider the most important factors influencing prognosis in this disease, namely: bacteremia, age, and the presence of systemic complications.”
Finland and Brown Am J Med Sci 1939, p 151.

169
Impact of Age and Bacteremia on Mortality
Finland M. Conn State Med J 1943Finland M. Conn State Med J 1943

170
Importance of Baseline Comparability
Group 1Group 1
Group 2Group 2
Mortality (%)Mortality (%)
9/18 (50%)9/18 (50%)
1/18 (6%)1/18 (6%)
Difference 44%Difference 44%P= 0.003P= 0.003
sulfanilamidesulfanilamide
no specificno specifictreatmenttreatment
Group 1 (Group 1 (sulfanilamidesulfanilamide))10/18 (56%) bacteremic10/18 (56%) bacteremic11/18 (61% ) multi-lobar11/18 (61% ) multi-lobar13/18 (72%) > age 3013/18 (72%) > age 30
Group 2 (Group 2 (no specific rx.)no specific rx.)0/18 (0%) bacteremic0/18 (0%) bacteremic0/18 (0%) over age 300/18 (0%) over age 30
Data from Finland M and Brown JW, Am J Med Sci 1939, 151Data from Finland M and Brown JW, Am J Med Sci 1939, 151

Issues in Design of Non-Inferiority Trials in CAP
• Choice of Endpoint
• Addressing Confounding due toLack of Randomized Trials evaluating STD
• Literature Review to Derive Margins for Non-Inferiority Trials in CAP
• Conclusions

• Extensive review of original source articles (rather than reliance on review articles)
• Lack of use of randomization in pre-1940s
• Predominantly sulfonamide derivatives & penicillin (closer to current beta-lactams & quinolones) …inhibition of growth of pathogenic microorganisms
rather than serum therapy …augmentation of the host immune response
• Majority subjects with pneumococcal pneumonia only and with microbiological confirmation of disease …difficult to extrapolate to mycoplasma & chlamydophila
Literature Review in CAP

Among articles reviewed:
8 papers provide data by bacteremia and age 5 papers provide data by age alone 3 papers provide data by bacteremia alone
…Search by J. Powers & T. Fleming
Literature Review in CAP

By Age
Bacteremic Subjects
No Specific
Treatment Antibiotics
Non-Bacteremic
No Specific
Treatment Antibiotics
<30 # Deaths / # Patients
81 / 126 4 / 16
64.3% 25.0%
90 / 1036 5 / 63
8.68% 7.94% Treatment Difference
Proposed Margin
39% (16%, 62%)
10 %
1% (-6%, 8%)
NONE
30-49 # Deaths / # Patients
319 / 428 21 / 66
74.3% 31.8%
218 / 1222 12 / 112
17.8% 10.7% Treatment Difference
Proposed Margin
43% (31%, 55%)
10 %
7% (1%, 15%)
0.5 %
≥ 50 # Deaths / # Patients
368 / 395 32 / 70
93.2% 45.7%
353 / 715 20 / 117
49.4% 17.1% Treatment Difference
Proposed Margin
47% (35%, 59%) 10 %
32% (24%, 40%)
10 %

175
Important Baseline Risk Factors for Poor Outcomes in Pneumonia
1. Older age
2. Presence of bacteremia
3. Presence of multi-lobar disease
4. Bronchopneumonia (as opposed to lobar pneumonia)
5. Type of infecting pneumococcus (type III highest mortality)
6. Presence of co-morbid illness
7. Late initiation of treatment
Tilghman and Finland Arch Intern Med 1937 and others
Note: PORT scoring takes into account age and presence of co-morbid illness, not other factors

PORT Scores Do Not Account for Bacteremia
30 day mortality 13% 30 day mortality 21%
Musher D et al. Medicine 2000; 79(4):210-21.

By Age
Bacteremic Subjects
No Specific
Treatment Antibiotics
Non-Bacteremic
No Specific
Treatment Antibiotics
<30 # Deaths / # Patients
81 / 126 4 / 16
64.3% 25.0%
90 / 1036 5 / 63
8.68% 7.94% Treatment Difference
Proposed Margin
39% (16%, 62%)
10 %
1% (-6%, 8%)
NONE
30-49 # Deaths / # Patients
319 / 428 21 / 66
74.3% 31.8%
218 / 1222 12 / 112
17.8% 10.7% Treatment Difference
Proposed Margin
43% (31%, 55%)
10 %
7% (1%, 15%)
0.5 %
≥ 50 # Deaths / # Patients
368 / 395 32 / 70
93.2% 45.7%
353 / 715 20 / 117
49.4% 17.1% Treatment Difference
Proposed Margin
47% (35%, 59%) 10 %
32% (24%, 40%)
10 %

Issues in Design of Non-Inferiority Trials in CAP
• Choice of Endpoint
• Addressing Confounding due toLack of Randomized Trials evaluating STD
• Literature Review to Derive Margins for Non-Inferiority Trials in CAP
• Conclusions

Non-Inferiority Trials
• Do not establish EXP is “as effective as” STD; NI trial rules out EXP is “unacceptably worse”
• Margins should be smaller than differences in efficacy patients & caregivers consider to be clinically relevant
• Margins should not be based on what can be ruled out using a pre-specified sample size
(1993 FDA Anti-Infective Drugs Guidance Document)
• Margins should not be based on “consensus” in the absence of data on STD

Challenges in Non-Inferiority Trials in CAP
Not simply,
“Are STD antibiotics effective at all in CAP?
Rather: we need to determine…
what is the magnitude of effect of STD?
on what clinically important outcome measures?
in what population?
in what experimental conditions?

Non-Inferiority Trials in CAP
• NI trial designs should be avoided if possible……they share many of the inherent dangers
of historically controlled trials….
Garattine S, Bertele V. “NI trials are unethical because they disregard patients’ interests.” Lancet 2007; 370: 1875-77
• Valid NI Trials can be done in CAP… with an all-cause mortality endpoint in a pop. with ≥15% mortality, (Bacteremic or Port 4/5) with microbiological confirmation of
pneumococcal pneumonia-like disease with effective STD control regimens with setting-specific margins ≤ 10%

182
Treatment Effect of Antibacterial Treatment Effect of Antibacterial Drugs in Community-Acquired Drugs in Community-Acquired
Pneumonia: Pneumonia: A Historical PerspectiveA Historical Perspective
Mary Singer, M.D., Ph.D.Mary Singer, M.D., Ph.D.
Medical Officer, Office of Antimicrobial Medical Officer, Office of Antimicrobial Products, FDA/CDERProducts, FDA/CDER

183
ObjectivesObjectives
To review evidence for a treatment effect of To review evidence for a treatment effect of antibacterial drugs in Community Acquired antibacterial drugs in Community Acquired Pneumonia (CAP)Pneumonia (CAP)
To estimate the magnitude of the treatment To estimate the magnitude of the treatment effect in the context of non-inferiority trialseffect in the context of non-inferiority trials

184
Approach to Estimation of Approach to Estimation of Treatment Effect for Antibacterial Treatment Effect for Antibacterial
Drugs in CAPDrugs in CAP
1.1. Historical Data Historical Data • Natural History studiesNatural History studies• Published studies performed Published studies performed pre- and postpre- and post - -
introduction of antibacterial drugsintroduction of antibacterial drugs Most were studies of pneumococcal or lobar pneumoniaMost were studies of pneumococcal or lobar pneumonia Hospitalized patientsHospitalized patients Mortality EndpointMortality Endpoint
Observational studies (treated vs. untreated)Observational studies (treated vs. untreated) Controlled trials: antibacterial drugs vs. untreated Controlled trials: antibacterial drugs vs. untreated
controlscontrols Pneumococcal or lobar pneumonia Pneumococcal or lobar pneumonia MycoplasmaMycoplasma pneumonia controlled trials pneumonia controlled trials
2.2. Alternative ApproachesAlternative Approaches

185
History of Effective Treatment History of Effective Treatment for Pneumococcal Pneumoniafor Pneumococcal Pneumonia
18811881 Streptococcus (Diplococcus) Streptococcus (Diplococcus) pneumoniaepneumoniae identified as ‘the’ cause of identified as ‘the’ cause of pneumonia pneumonia
1913 - 19401913 - 1940 Serum Therapy Serum Therapy
1938-19391938-1939 SulfapyridineSulfapyridine
1940 - 19451940 - 1945 Penicillin and other antibioticsPenicillin and other antibiotics

186
Natural History of CAPNatural History of CAP
““Recovery followed the ‘crisis’ - an abrupt decrease Recovery followed the ‘crisis’ - an abrupt decrease in temperature over 12 hours, accompanied by in temperature over 12 hours, accompanied by passage ‘from a condition of extreme distress and passage ‘from a condition of extreme distress and anxiety to one of comparative comfort’ - and anxiety to one of comparative comfort’ - and occurred in a large proportion of cases. A fatal occurred in a large proportion of cases. A fatal outcome was noted in 20-35%. Worse prognosis outcome was noted in 20-35%. Worse prognosis was evident in ‘drunkards’ and the elderly, with was evident in ‘drunkards’ and the elderly, with fatality increasing to 50-65% in the elderly in those fatality increasing to 50-65% in the elderly in those in their 6th and 7th decades.”in their 6th and 7th decades.”
- Sir William Osler, 1894, who succumbed to - Sir William Osler, 1894, who succumbed to HaemophilusHaemophilus influenzae pneumonia in 1919influenzae pneumonia in 1919

187
Percentage of Untreated Patients "Terminating by Percentage of Untreated Patients "Terminating by Recovery" by each Day in Seven Different Pneumococcal Recovery" by each Day in Seven Different Pneumococcal
TypesTypes
(Bullowa, 1937)(Bullowa, 1937)

188
Pneumococcal Pneumonia (Untreated) in Pneumococcal Pneumonia (Untreated) in Infants and Children: Effect of Age and Infants and Children: Effect of Age and
Bacteremia on MortalityBacteremia on MortalityBullowa (1937)Bullowa (1937)
GroupGroup Percent MortalityPercent Mortality
< 2 years old*< 2 years old*
Percent MortalityPercent Mortality
> 2 years old**> 2 years old**
Positive BCPositive BC 30/38 (79%)30/38 (79%) 8/31 (26%)8/31 (26%)
Negative BCNegative BC 57/400 (14%)57/400 (14%) 13/454 (3%)13/454 (3%)
All CasesAll Cases 87/438 (20%)87/438 (20%) 21/485 (4%)21/485 (4%)
BC = blood culture *8.7% *8.7% bacteremicbacteremic
**6.4% bacteremic**6.4% bacteremic

189
OBSERVATIONAL STUDIESOBSERVATIONAL STUDIES

190

191
Mortality in Pneumococcal PneumoniaMortality in Pneumococcal Pneumonia Tilghman and Finland (1937)Tilghman and Finland (1937)
TreatmentTreatment Percent MortalityPercent Mortality
BacteremicBacteremic
N=582N=582
Percent MortalityPercent Mortality
Non-bacteremicNon-bacteremic
N=1004N=1004
Percent MortalityPercent Mortality
OverallOverall
N=1586N=1586
SerumSerum 46/10246/102
(45%)(45%)
21/176 21/176
(12%)(12%)
67/278 67/278
(24%)(24%)
No serumNo serum 405/480 405/480
(84%)(84%)
261/826 261/826
(32%)(32%)
666/1306 666/1306
(51%)(51%)

192
Pneumococcal Pneumonia: Duration of Acute Pneumococcal Pneumonia: Duration of Acute IllnessIllness
(Tilghman and Finland, 1937)(Tilghman and Finland, 1937)

193
Mortality in Pneumococcal PneumoniaMortality in Pneumococcal PneumoniaFinland (1943)Finland (1943)

194
Treatment of Pneumococcal Treatment of Pneumococcal Pneumonia with PenicillinPneumonia with Penicillin
Meads, et al. (1945)Meads, et al. (1945)
SeveritySeverity PenicillinPenicillin
N=37N=37
Penicillin after Penicillin after sulfa treatmentsulfa treatment
N=17N=17
Grade 2 Grade 2 (moderate)(moderate)
1515 11
Grade 3 (acutely Grade 3 (acutely ill/irrational)ill/irrational)
99 55
Grade 4 (shock Grade 4 (shock &/or CHF)&/or CHF)
1313 1111
Observational Study in patients with moderate-severe Observational Study in patients with moderate-severe pneumococcal pneumoniapneumococcal pneumonia

195
Treatment of Pneumococcal Treatment of Pneumococcal Pneumonia with Penicillin: Pneumonia with Penicillin:
OutcomesOutcomesMeads, et al. (1945)Meads, et al. (1945)
Outcome Outcome Penicillin Penicillin
(N=37)(N=37)
Penicillin after sulfa failure Penicillin after sulfa failure or intolerance (N=17)or intolerance (N=17)
DeathDeath 7 (19%)7 (19%) 3 (18%)3 (18%)
RelapseRelapse 22 11
ComplicationsComplications 00 00
Bacteremia after Bacteremia after penicillin treatmentpenicillin treatment
0/120/12 4/64/6
Duration of acute Duration of acute symptoms* < 48 symptoms* < 48 hourshours
27/30 (90%)27/30 (90%) 9/14 (64%)9/14 (64%)
Duration of fever < Duration of fever < 48 hours48 hours
24/30 (80%)24/30 (80%) 8/14 (57%)8/14 (57%)
*symptoms such as delirium, prostration, and dyspnea

196
Case Fatality Rate in Pneumococcal Pneumonia Case Fatality Rate in Pneumococcal Pneumonia treated with Serum, Sulfonamides or “Antibiotics”treated with Serum, Sulfonamides or “Antibiotics”
Dowling and Lepper (1951) Dowling and Lepper (1951)

197
Mortality in Pneumococcal Pneumonia Mortality in Pneumococcal Pneumonia with Bacteremiawith Bacteremia
Austrian and Gold (1964)Austrian and Gold (1964)
Prospective, observational study (1952-1962)Prospective, observational study (1952-1962) N= 455 with bacteremic pneumococcal N= 455 with bacteremic pneumococcal
pneumonia without extra-pulmonary pneumonia without extra-pulmonary complicationscomplications
50% < 50 years old; 55% had pre-existing co-50% < 50 years old; 55% had pre-existing co-morbiditiesmorbidities
Most treated with penicillin or other Most treated with penicillin or other antibacterial agents (96%); while 4% received antibacterial agents (96%); while 4% received no specific treatmentno specific treatment

198
Mortality in Pneumococcal Pneumonia Mortality in Pneumococcal Pneumonia with Bacteremiawith Bacteremia
Austrian and Gold (1964)Austrian and Gold (1964)
TreatmentTreatment Case Fatality RateCase Fatality Rate
n/N (%)n/N (%)
PenicillinPenicillin 57/338 (17%)57/338 (17%)
TetracyclinesTetracyclines 10/55 (18%)10/55 (18%)
Erythromycin, chloramphenicol, Erythromycin, chloramphenicol, streptomycinstreptomycin
2/14 (14%)2/14 (14%)
““Mixed”Mixed” 6/30 (20%)6/30 (20%)
Any antibacterial treatmentAny antibacterial treatment 75/437 (17%)75/437 (17%)
No treatmentNo treatment 14/17 (82%)14/17 (82%)

199
Survival in Bacteremic Pneumococcal Bacteremia Survival in Bacteremic Pneumococcal Bacteremia Treated with Penicillin or SerumTreated with Penicillin or Serum
Austrian and Gold (1964) Austrian and Gold (1964)

200
Observational Studies: MicrobiologyObservational Studies: Microbiology
StudyStudy PathogenPathogen
Finland (1943)Finland (1943) S. pneumoniaeS. pneumoniae
Dowling and Lepper (1951)Dowling and Lepper (1951) S. pneumoniaeS. pneumoniae
Austrian and Gold (1964)Austrian and Gold (1964) S. pneumoniaeS. pneumoniae

201
Treatment Effect:Observational Studies
41
78
31
82
17
30
135
17
0102030405060708090
Finland Finland(BC+)
Dowling Austrian(BC+)
Mo
rta
lity
%
Untreated Sulfa Penicillin

202
Summary of Antibacterial Drug Summary of Antibacterial Drug Treatment Effect in Pneumococcal Treatment Effect in Pneumococcal
PneumoniaPneumoniaObservational StudiesObservational Studies Treatment vs. Treatment vs.
Untreated controlsUntreated controlsMortality Difference Mortality Difference (95% confidence (95% confidence interval)interval)
Finland (1943)Finland (1943) SulfonamidesSulfonamides 24% (21, 27)24% (21, 27)
48% (bacteremic)48% (bacteremic)
Dowling and Lepper Dowling and Lepper (1951)(1951)
SulfonamidesSulfonamides
Penicillin, tetracyclinesPenicillin, tetracyclines
18.5% (15, 21)18.5% (15, 21)
25.4% (22, 28)25.4% (22, 28)
Austrian and Gold Austrian and Gold (1964)(1964)
Penicillin, Penicillin, tetracyclines, other tetracyclines, other antibacterial drugsantibacterial drugs
65% (47, 84)65% (47, 84)
(bacteremic)(bacteremic)

203
Observational Studies: Observational Studies:
Effect of Age on MortalityEffect of Age on Mortality
StudyStudy Treated < Treated < 50 years old50 years old
Untreated < Untreated < 50 years old50 years old
Treated ≥ 50 Treated ≥ 50 years oldyears old
Untreated Untreated
≥ ≥ 50 years 50 years oldold
Finland Finland (1943)(1943)
NRNR NRNR NRNR NRNR
Dowling and Dowling and Lepper Lepper (1951)(1951)
97/1672 97/1672
(6%)(6%)
139/715 139/715 (19%)(19%)
historicalhistorical
107/522 107/522 (20%)(20%)
192/362 192/362 (53%)(53%)
historicalhistorical
Austrian and Austrian and Gold (1964)Gold (1964)
(Bacteremic)(Bacteremic)
13/178 13/178
(7%)(7%)
371/693 371/693 (73%)(73%)
historicalhistorical
44/160 44/160
(28%)(28%)
322/345 322/345 (93%)(93%)
historicalhistorical

204
Controlled Clinical TrialsControlled Clinical Trials

205
Controlled Clinical Trial- SerotherapyControlled Clinical Trial- Serotherapy
Park, et al. (1928)Park, et al. (1928) Alternate patients with lobar pneumoniaAlternate patients with lobar pneumonia Treatment:Treatment:
Polyvalent antiserum:Polyvalent antiserum: pneumococcal types I, II, III pneumococcal types I, II, III
or:or: Standard treatment:Standard treatment: fluids, pain relief with elastic fluids, pain relief with elastic
adhesive plaster, restriction of opiates, no drastic adhesive plaster, restriction of opiates, no drastic catharsis, oxygen for cyanosis or rapid breathing, catharsis, oxygen for cyanosis or rapid breathing, digitalization for heart rate > 120digitalization for heart rate > 120

206
Case Fatality Rate in Patients with Type Case Fatality Rate in Patients with Type I Pneumococcal Pneumonia by Severity: I Pneumococcal Pneumonia by Severity:
(Park, et al., 1928)(Park, et al., 1928)Condition at Condition at baselinebaseline
Serum-treated Serum-treated Standard Standard treatment treatment
Treatment Treatment DifferenceDifference
Any conditionAny condition 20% (N=114)20% (N=114) 34% (N= 109)34% (N= 109) 14%14%
GoodGood
(> 70)(> 70)
9%9% 13%13% 4%4%
Fair (50-70)Fair (50-70) 29%29% 52%52% 23%23%
Poor (< 50)Poor (< 50) 64%64% 100%100% 36%36%

207
Controlled Clinical Trial of Treatment of Controlled Clinical Trial of Treatment of Lobar Pneumonia Lobar Pneumonia
Evans and Gaisford (1938)Evans and Gaisford (1938)
All patientsAll patients M & B 693M & B 693
(Sulfapyridine)(Sulfapyridine)
ControlControl
All patientsAll patients 8/100 (8%)8/100 (8%) 27/100 (27%)27/100 (27%)
Age > 50Age > 50 4/18 (22%)4/18 (22%) 7/10 (70%)7/10 (70%)
Treatment:Treatment: M&B 693: 2-(p-aminobenzenesulphonamide) pyridine M&B 693: 2-(p-aminobenzenesulphonamide) pyridineControl:Control: Non-specific treatment (presumed standard of care) Non-specific treatment (presumed standard of care)Population:Population: Hospitalized patients with lobar pneumonia (8 - 68 years old); 86% Hospitalized patients with lobar pneumonia (8 - 68 years old); 86% < 50 years old; proportion bacteremic not reported; specific pneumococcal < 50 years old; proportion bacteremic not reported; specific pneumococcal serotypes reported in 22%; 78% were not identified.serotypes reported in 22%; 78% were not identified.Treatment group:Treatment group: Determined by enrollment on alternate day Determined by enrollment on alternate day Excluded:Excluded: Patients who died within 24 hours Patients who died within 24 hours
Case Fatality Rate

208
Resolution of FeverResolution of Fever Evans and Gaisford (1938)Evans and Gaisford (1938)
Treatment Treatment GroupGroup
NN Cumulative Resolution of Cumulative Resolution of Fever within 48 hoursFever within 48 hours
N (%)N (%)
Treated Treated 100100 60 (60%)60 (60%)
ControlControl 100100 34 (34%)34 (34%)

209
Follow-up Case Series: Gaisford (1939)Follow-up Case Series: Gaisford (1939)
400 cases lobar pneumonia (hospitalized)400 cases lobar pneumonia (hospitalized) Includes 100 cases previously described in Includes 100 cases previously described in
Evans and Gaisford (1938)Evans and Gaisford (1938) Proportion of bacteremic patients not reportedProportion of bacteremic patients not reported Excluded deaths within 12 hours of admissionExcluded deaths within 12 hours of admission

210
Case Fatality Rates by Age in Lobar Case Fatality Rates by Age in Lobar PneumoniaPneumonia
(Gaisford, 1939) (Gaisford, 1939)
Age RangeAge Range
(years)(years)
UntreatedUntreated
19361936
n/N (%)n/N (%)
UntreatedUntreated
19371937
n/N (%)n/N (%)
SulfapyridineSulfapyridine
1938-19391938-1939
n/N (%)n/N (%)
5-195-19 5/127 (4)5/127 (4) 7/153 (5)7/153 (5) 0/115 (0)0/115 (0)
20-5020-50 53/216 (25)53/216 (25) 54/230 (23)54/230 (23) 5/199 (3)5/199 (3)
≥ ≥ 50 50 35/72 (49)35/72 (49) 39/78 (50)39/78 (50) 21/86 (24)21/86 (24)
All AgesAll Ages 93/415 (22)93/415 (22) 100/461 (22)100/461 (22) 26/400 (7)26/400 (7)

211
Controlled Clinical Trial: Treatment of Controlled Clinical Trial: Treatment of Pneumococcal Pneumonia with Pneumococcal Pneumonia with
SulfapyridineSulfapyridine Graham, et al. (1939)Graham, et al. (1939)
Dagenan (M&B 693)Dagenan (M&B 693) ControlsControls
3/50 (6%)3/50 (6%) 7/30 (23%)7/30 (23%)
3/17 (18%) bacteremic3/17 (18%) bacteremic 3/6 (50%) bacteremic3/6 (50%) bacteremic
Hospitalized patients with primarily pneumococcal pneumonia (14% had other unidentified pathogens)Alternate patientsAge < 50 years: 70% overall; bacteremia 29% overallControl: no specific therapy (20% bacteremic)Dagenan (M&B 693) = Sulfapyridine (34% bacteremic)
Case Fatality Rate

212
Controlled Clinical Trial: Treatment of Controlled Clinical Trial: Treatment of Lobar Pneumonia with SulfapyridineLobar Pneumonia with Sulfapyridine
Agranat, et al. (1939)Agranat, et al. (1939) Lobar pneumonia (microbiology not described)Lobar pneumonia (microbiology not described) Several study sites in South Africa: results reported Several study sites in South Africa: results reported
separatelyseparately Sulfapyridine vs. control (method of treatment allocation Sulfapyridine vs. control (method of treatment allocation
was by admission to separate ward with “no selection”)was by admission to separate ward with “no selection”) Site 1: Johannesburg Hospital Site 1: Johannesburg Hospital
Europeans (97% < 50 years old)Europeans (97% < 50 years old) Non-Europeans (81% < 50 years old)Non-Europeans (81% < 50 years old) Mild (+), Moderate (++), Severe (+++)Mild (+), Moderate (++), Severe (+++)
32-33% severe in treated groups32-33% severe in treated groups 17-26% severe in untreated groups17-26% severe in untreated groups
Proportion bacteremic patients not reportedProportion bacteremic patients not reported Results of other sites not reported here because of Results of other sites not reported here because of
differences in patient populations and disease severitydifferences in patient populations and disease severity

213
Case Fatality RatesCase Fatality RatesAgranat, et al. (1939)Agranat, et al. (1939)
SubsetSubset ControlControl SulfapyridineSulfapyridine
EuropeansEuropeans 6/27 (22%)6/27 (22%) 2/22 (7%)2/22 (7%)
Non-EuropeansNon-Europeans 16/86 (19%)16/86 (19%) 6/71 (9%)6/71 (9%)
Case Fatality Rate

214
Resolution of FeverResolution of FeverAgranat, et al. (1939)Agranat, et al. (1939)
Days Days hospitalized hospitalized with feverwith fever
Non-Non-EuropeanEuropean
ControlControl
N=86N=86
Non-Non-EuropeanEuropean
TreatedTreated
N=71N=71
EuropeanEuropean
ControlControl
N=23N=23
European European
TreatedTreated
N=22N=22
% patients% patients % patients% patients % patients% patients % patients% patients
11 1.41.4 12.312.3 00 26.126.1
22 8.68.6 21.521.5 00 34.834.8
33 17.117.1 18.518.5 1010 8.78.7
Cumulative % Cumulative % at 3 daysat 3 days
2727 5252 1010 70%70%

215
Controlled Trials :MicrobiologyControlled Trials :Microbiology
Observational Studies:Observational Studies: Pathogens ReportedPathogens Reported
Evans and Gaisford (1938)Evans and Gaisford (1938) Pneumococcal types I, II, III, and Pneumococcal types I, II, III, and IV in 44/200 (22%) cases; 78% not IV in 44/200 (22%) cases; 78% not reported reported
Graham, et al. (1939)Graham, et al. (1939) S. pneumoniaeS. pneumoniae in 69/80 (86%); in 69/80 (86%); 11/86 (14%) not pneumococcal11/86 (14%) not pneumococcal
Agranat et al. (1939)Agranat et al. (1939) Not reported except in 2 deaths: Not reported except in 2 deaths:
S. pneumoniaeS. pneumoniae, , StaphylococcusStaphylococcus

216
Treatment Effect:Controlled Trials
2723
1922
86
97
0
5
10
15
20
25
30
Evans Graham Agranat(1)
Agranat(2)
Ca
se
Fa
talit
y R
ate
Untreated Sulfa

217
Summary of Antibacterial Drug Summary of Antibacterial Drug Treatment Effect in Pneumococcal Treatment Effect in Pneumococcal
PneumoniaPneumonia
Controlled StudiesControlled Studies Treatment vs. Treatment vs. untreated controlsuntreated controls
Difference in Case Difference in Case Fatality Rate Fatality Rate
(95% confidence (95% confidence interval)interval)
Evans and Gaisford Evans and Gaisford (1938)(1938)
SulfapyridineSulfapyridine 19% (8.8, 29.2)19% (8.8, 29.2)
Graham, et al., (1939)Graham, et al., (1939) SulfapyridineSulfapyridine 17% (0.1, 36.4)17% (0.1, 36.4)
32% (bacteremic)32% (bacteremic)
Agranat, et al. (1939)Agranat, et al. (1939) SulfapyridineSulfapyridine 10% (-0.3, 20.6)10% (-0.3, 20.6)
15% (-6.2, 35.5)15% (-6.2, 35.5)

218
MycoplasmaMycoplasma Pneumonia: Randomized Pneumonia: Randomized Controlled TrialsControlled Trials
Kingston, et al. (1961)Kingston, et al. (1961)
Randomized, double-blind, placebo-controlled Randomized, double-blind, placebo-controlled trialtrial
Military recruits (age 17-22); Military recruits (age 17-22); Total N= 300; (subgroup of “Eaton-agent” Total N= 300; (subgroup of “Eaton-agent”
positive N=133)positive N=133) ““Eaton agent” (Eaton agent” (MycoplasmaMycoplasma) diagnosed ) diagnosed
serologically; and nose and throat cultures serologically; and nose and throat cultures were negative for pneumococcus and were negative for pneumococcus and streptococci.streptococci.
Treatment: Tetracycline (demeclocycline) vs. Treatment: Tetracycline (demeclocycline) vs. placeboplacebo

219
Duration of Fever in Duration of Fever in MycoplasmaMycoplasma Pneumonia: Pneumonia: Effect of TreatmentEffect of Treatment
(Kingston, et al. 1961)(Kingston, et al. 1961)

220
MycoplasmaMycoplasma Pneumonia: Outcomes Pneumonia: OutcomesKingston, et al., (1961)Kingston, et al., (1961)
ParameterParameter TreatedTreated
Mean Duration Mean Duration (days)(days)
PlaceboPlacebo
Mean Duration Mean Duration (days)(days)
Treatment Treatment Difference (days)Difference (days)
Temperature 100ºFTemperature 100ºF 2.12.1 8.18.1 6.06.0
Abnormal CXRAbnormal CXR 9.59.5 20.020.0 10.510.5
RalesRales 6.96.9 15.515.5 8.68.6
CoughCough 9.79.7 22.022.0 12.312.3
Bed restBed rest 5.85.8 9.29.2 3.43.4
Fatigue, malaiseFatigue, malaise 2.72.7 8.58.5 5.85.8
AnorexiaAnorexia 2.02.0 7.07.0 5.05.0

221
MycoplasmaMycoplasma Pneumonia: Randomized, Pneumonia: Randomized, Controlled TrialsControlled Trials (Smilack, et al., 1974)(Smilack, et al., 1974)
Randomized, placebo-controlled, double-blind Randomized, placebo-controlled, double-blind trialtrial
Population: hospitalized military personnel, Population: hospitalized military personnel, mostly male, 17 to 23 years old (n=130; mostly male, 17 to 23 years old (n=130; MycoplasmaMycoplasma confirmed in 32) confirmed in 32)
Diagnosis: serological; bacterial pathogen-Diagnosis: serological; bacterial pathogen-negative by culturenegative by culture
Treatment: clindamycin (n=9), tetracycline Treatment: clindamycin (n=9), tetracycline (n=15), or placebo (n=8)(n=15), or placebo (n=8)
Antipyretic use in 8 patients (clindamycin:1; Antipyretic use in 8 patients (clindamycin:1; tetracycline: 4; placebo: 3)tetracycline: 4; placebo: 3)

222
MycoplasmaMycoplasma Pneumonia: Outcomes Pneumonia: OutcomesSmilack, et al. (1974)Smilack, et al. (1974)
Duration of Fever > 99º F

223
Summary: Summary: MycoplasmaMycoplasma Pneumonia Pneumonia StudiesStudies
Treatment effect of antibacterial drugs shown in Treatment effect of antibacterial drugs shown in young, healthy patients on:young, healthy patients on: Decreased duration of fever (and other signs Decreased duration of fever (and other signs
and symptoms), hospitalization, CXR and symptoms), hospitalization, CXR abnormalitiesabnormalities
Caveats: Reporting of antipyretic use Caveats: Reporting of antipyretic use inconsistent among studies; and some inconsistent among studies; and some uncertainty in datauncertainty in data
Can these data be extrapolated to all Can these data be extrapolated to all outpatients with CAP?outpatients with CAP?
Can these data be used to determine a non-Can these data be used to determine a non-inferiority margin for outpatient CAP? inferiority margin for outpatient CAP?

224
Limitations of using the Historical Data Limitations of using the Historical Data to Estimate Treatment Effectto Estimate Treatment Effect
Differences in Patient Populations: Differences in Patient Populations: e.g. co-morbidities, immune status, pneumococcal e.g. co-morbidities, immune status, pneumococcal
vaccinationvaccination Differences in Organisms/Disease:Differences in Organisms/Disease:
Mostly hospitalized patients with pneumococcal Mostly hospitalized patients with pneumococcal pneumonia pneumonia
Severity was not well-characterizedSeverity was not well-characterized Most CAP now treated in outpatient settingMost CAP now treated in outpatient setting S. pneumoniaeS. pneumoniae isolated less frequently isolated less frequently Atypical organisms common in mild CAPAtypical organisms common in mild CAP
Differences in Standard of CareDifferences in Standard of Care Differences in Study Design:Differences in Study Design:
Observational dataObservational data Controlled trials were not randomized or blindedControlled trials were not randomized or blinded Endpoints: mortality vs. clinical responseEndpoints: mortality vs. clinical response Study drugs: penicillin, sulfonamides, tetracyclinesStudy drugs: penicillin, sulfonamides, tetracyclines

225
ConclusionsConclusions
Evidence for treatment effect of Evidence for treatment effect of antibacterial drugs in hospitalized patients antibacterial drugs in hospitalized patients with CAP (pneumococcal or lobar with CAP (pneumococcal or lobar pneumonia) based primarily on a mortality pneumonia) based primarily on a mortality benefit benefit Limited data on the treatment effect for other Limited data on the treatment effect for other
endpoints such as time to resolution of signs and endpoints such as time to resolution of signs and symptoms of CAPsymptoms of CAP
Evidence, albeit limited, for antibacterial Evidence, albeit limited, for antibacterial effect on resolution of signs and symptoms effect on resolution of signs and symptoms in atypical (in atypical (MycoplasmaMycoplasma) pneumonia) pneumonia

226
Contemporary CAP trials and determination of treatment effect
Sumati Nambiar MD MPHMedical Team Leader
Division of Anti-Infective
and Ophthalmology Products

227
Overview
Summary of recent CAP trials (oral and IV studies) Linking historical studies to contemporary CAP
trials Alternate approaches to determining
treatment effect

228
Study design
Inclusion criteria included presence of new infiltrate(s) on chest x-ray AND at least 2 of the following signs or symptoms: cough, sputum production, auscultatory findings, dyspnea,
tachypnea, fever, elevated WBC, hypoxemia Microbiologic evaluation was to be performed on each
patient isolation of a pathogen not required for overall evaluability
Primary endpoint was clinical cure at the test of cure visit, 7 – 21 days after completion of therapy
Primary analyses populations: ITT and per protocol

229
Outcomes
Clinical cure: Complete resolution or improvement of all signs and symptoms Improvement or lack of progression of all abnormalities on
chest radiograph No additional antibacterial therapy required
Microbiologic response: Eradication: Absence of original pathogen from TOC culture Persistence: Presence of original pathogen in TOC culture Presumed eradication: Clinical cure without specimen for
culture Presumed persistence: Clinical failure without culture of
specimen

230
Analysis Populations Intent to treat (ITT)
All randomized patients Per Protocol or Clinically Evaluable
ITT patients without any major protocol violations Modified/Microbiologic ITT (MITT):
ITT patients with baseline pathogen, including serologic diagnosis
Microbiologically Evaluable: MITT patients without any major protocol violations

231
Oral CAP studies
Seven comparative studies conducted from
2000-present Most were multinational Randomized, double-blind, non-inferiority trials
Pre-specified non-inferiority margin was 10 or 15%
300-500 randomized patients per study Active controls included clarithromycin,
amoxicillin/clavulanate and levofloxacin

232
Clinical Features
Cough: 97 - 100% Sputum Production: 75% - 100% Fever: 19% -33% (98% outlier) Chills: 1-6% (69% outlier) Shortness of Breath: 18% - 100% Chest Pain: 41% - 76% Multilobe involvement: 16-25%

233
Baseline pathogens
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7
S. pneumoniae

234
Clinical outcomes
-20
0
20
1 2 3 4 5 6 7
Study
Test
- C
ontr
ol
-15
-10
Intent to TreatPer Protocol

235
Summary of oral CAP studies Age
Mean 46 years (range 18 to 98 years) Middle 50% of the population ranged from 35 – 55 years
PORT scores Majority of patients had PORT scores II 5 to 10% of patients had PORT score of III
Microbiology: Baseline pathogens identified in 45%-75% 6-20% had S. pneumoniae 0-2% had S. pneumoniae bacteremia
Outcomes: Clinical cure, > 80% ITT and ≥90% PP Mortality <2%

236
IV CAP studies Similar design as the oral only studies Some were open label Endpoints and analysis populations similar to
oral CAP studies Study size ranged from about 300 – 700
patients

237
Summary of IV CAP studies Age:
Mean 56 years (range 13-97 years) Middle 50% 40-70 years
PORT scores: 55% PORT I and II 20% PORT III or PORT IV < 5% PORT V
Microbiology: Baseline pathogens identified in 30-55% 20% had S. pneumoniae 4-9 % had S. pneumoniae bacteremia
Outcomes: Clinical cure, 80% ITT and 90% PP Mortality, 2-4%

238
Bridging the gap

239
CAP Studies in early 1900’s
Hospitalized patients Severity of disease unclear
Reasonable to assume that most had moderate-severe disease
No standardized classification system Most studies were primarily in patients with
pneumococcal pneumonia Some studies included patients without
confirmed pneumococcal etiology

240
Current CAP Trials Majority have been oral CAP studies
NI trials with a pre-specified margin of 10-15%
Patient characteristics:
Otherwise healthy patients with mild-moderate CAP
Few patients had PORT scores ≥III
Proportion of patients with S. pneumoniae small
Number of patients with bacteremia small
Primary endpoint was clinical outcome
High success rates and small differences in efficacy
Mortality low in most studies

241
Linking Historical Data with Current CAP trials
Patient populations Difficult to define a patient population identical to those in
historical studies Can patients in current CAP trials be compared to
those in historical studies if matched for age? More than 75 % of patients in the controlled historical
studies and ~50-75% of patients in the observational studies were < 50 years of age
Is it acceptable to assign PORT scores for patients in the historical studies based on age alone? Only limited data are available on co-morbidities

242
Linking Historical Data with Current CAP trials
Microbiology Historical data, is primarily from patients with
pneumococcal pneumonia; in a few patients S. aureus, or hemolytic streptococci were identified, and some had no baseline pathogen In current studies, S. pneumoniae is isolated in only a
small fraction of cases and only a small proportion of patients have bacteremia
Can the treatment effect be extrapolated to organisms other than S. pneumoniae?

243
Linking Historical Data with Current CAP trials
Endpoints Treatment effect for mortality can be estimated
Treatment effect is larger in patients older than 50 years and in bacteremic patients
In current studies, mortality is low; rescue therapy is used in patients failing treatment
Clinical outcome is primary endpoint rather than mortality Based on limited data for other endpoints from historical studies,
is it reasonable to extrapolate from the treatment effect seen with mortality in historical data to clinical outcome in present trials?
As death is included in clinical failure, can we assume that the treatment effect for clinical outcome is likely to be greater than that seen for mortality?

244
Alternative approaches

245
Alternate approaches
Outcomes from studies of ‘discordant’ treatment Non-adherence to treatment guidelines In vitro susceptibility
Timing of antibiotic administration ‘Failed’ active comparator studies Superiority studies Dose-ranging studies

246
Discordant Therapy• Discordance based on guidelines
Retrospective studies that used varying definitions of discordant therapy
Endpoints varied;48-hour mortality, 30-day mortality, in-hospital mortality
Number of patients who received discordant therapy was small
Some studies did not adjust for severity of illness or other covariates
• Discordance based on in vitro susceptibility of S. pneumoniae to beta-lactams No difference in mortality/clinical success seen (Falagas 2006)
With the recent change in penicillin breakpoints, definitions used in some studies may not be applicable
(http://www.fda.gov/cder/foi/label/2008/050638s012lbl.pdf)

247
Other Supportive Data
• Active comparator studies Most studies have been NI studies, few have shown superiority (Finch et
al. AAC 2002, File et al. AAC 1997) All classes effective; summary reviews have not demonstrated
superiority of one class over another (Mills et al. 2005, Shefet et al. 2005) Estimate of treatment difference would be an underestimate Very few studies demonstrated superiority, likely by chance alone
• Timing of antibiotic administration Data from observational studies Time to first antibiotic dose (TFAD) of 4 hours associated with better
outcomes• Dose-response studies
No studies identified that showed superiority of one dosing regimen over another

248
‘Failed’ active comparator studies
• Phase 3 randomized, double-blind non-inferiority trials in hospitalized CAP patients (Pertel et al. CID 2008)
• Second study stopped early based on results of first study
• Studies were conducted from October 2000- February 2002
• 413 daptomycin and 421ceftriaxone-treated patients (pooled)
• PORT scores: ~42% class II, 30% class III, remainder class IV
• Microbiology:• MITT population: 132/467 (28.3%) daptomycin-treated and
116/469 (24.7%) ceftriaxone-treated
• Bacteremia: 30 (7.3%) daptomycin-treated and 29 (6.9%) in ceftriaxone-treated patients

249
Results
• Clinical Outcome (Daptomycin vs. Ceftriaxone, pooled data): ITT population: 70.9% vs.77.4%; -6.5%, (-12.4, -0.6) CE population: 79.4% vs. 87.9%; -8.5% , (-13.8, -3.2) MITT population: 74.2 % vs. 79.3%; -5.1%, (-15.6%, 5.4%)
• Mortality: 21 (4.6%) daptomycin-treated patients and 12 (2.6%) ceftriaxone-treated patients died during the study
• Post hoc analysis in the pooled CE population showed that daptomycin-treated patients who received prior effective therapy for < 24 hrs had higher success rates than those who did not receive such therapy
• Though daptomycin has been shown to interact with pulmonary surfactant, daptomycin effect likely larger than placebo

250
Other endpoints
Some studies have demonstrated superiority of one regimen over another in time to resolution of symptoms as a secondary endpoint or as a subgroup analysis (Anzueto et al. CID 2006, Finch et al. AAC 2002, Welte et al. CID 2005)
Some studies have used clinician reported outcomes, while some have used patient reported outcomes that were not validated
CAP-Sym, is a patient based outcome measure that has been evaluated in outpatients with CAP (Lamping et al. Chest 2002) Has not been used as a primary endpoint in registrational
trials

251
Summary of Supportive Data
Overall, studies support effectiveness of antibacterials in CAP
Choice of antibacterial and timing of administration appear to be important
Supportive information not contributory to determining magnitude of treatment effect
Alternate endpoints such as time to resolution of signs and symptoms may be an option

252
“Pneumonia kills more children than any other illness – more than AIDS, malaria and measles combined. Over 2 million children die from pneumonia each year, accounting for almost 1 in 5 underfive deaths worldwide”
http://www.unicef.org/publications/files/Pneumonia_The_Forgotten_Killer_of_Children.pdf

253
Pediatric CAP studies As in adults, historical studies in children showed
reduction in mortality after introduction of sulfonamides (Raycraft 1941, Ormiston 1942)
Most recent trials have been ‘equivalency trials’ (APPIS study, NO-SHOTS study) Studied children with severe or very severe pneumonia based
on WHO classification system Regimens varied: oral amoxicillin vs. iv ampicillin/ penicillin
chloramphenicol vs. ampicillin/gentamicin In most studies results similar in both treatment groups One recent study (SPEAR study) showed that ampicillin +
gentamicin was superior to chloramphenicol in children aged 2-59 months with very severe pneumonia (Asghar et al. BMJ 2008)

254
Summary
Overview of recent CAP trials (oral and IV) study design, endpoints, analysis populations,
microbiology and outcomes Although treatment effect was demonstrated
in historical studies, there are difficulties in linking historical data to current CAP trials
Overview of additional data that are supportive of antibacterial effect in CAP, though not directly contributory to estimating a treatment effect

255
Conclusions
Patient populations described in the historical studies differ from those seen in current CAP trials In current trials patients may be less ill A small proportion have S. pneumoniae as the baseline
pathogen Very few are bacteremic
Endpoints evaluated in historical studies are different from those used in current CAP trials
For non-inferiority trials in CAP we need to Define patient populations and endpoints that are best
supported by the treatment effect seen in historical studies

256
NI Margin for CAP StudiesIssues and Approaches
Thamban Valappil, Ph.D.Statistical Team Leader,
Office of Translational ScienceCenter for Drug Evaluation and Research
U.S. Food and Drug Administration
Anti-Infectives Drugs Advisory Committee April 1-2, 2008

257
Outline
• Critical Steps in Designing a NI trial • Statistical Uncertainties in NI Studies• Discounting and Preservation of Control
Treatment Effect• Historical Evidence in CAP studies• Magnitude of Treatment Benefit• Future Trial Design Considerations

258
Critical steps in designing a NI trial
• Determine whether historical evidence of sensitivity to drug effect (HESDE) exists.
• Determine the design features of the historical placebo-controlled trials from which HESDE has been established.
• Determine a scientifically justifiable non-inferiority margin.
• Assure the quality of the trial and its conduct. – Any kind of “subjectivity or imprecision” can be
rewarded in a non-inferiority trial and can artificially make the treatments look similar, when in fact, that they are not similar.

259
Statistical Uncertainties in NI StudiesWhat are the sources of uncertainties?• Magnitude and precision of the estimate of active
control treatment effect based on historical placebo-controlled studies.
• Lack of constancy assumption i.e. the potential lack of comparability of historical evidence to estimate the size of the treatment effect in the current NI study.
• The observed treatment effect from a single study or collection of studies may not be reproducible introducing bias.
• Control for the overall type I error rate in the estimate of the treatment difference between the test drug and active control in the current NI study.

260
“Untreated”
Active Control
Test Drug
Treatment Effect
Unclear treatment effect

261
Untreated Active Control
Test Drug
Treatment Effect
Substantial treatment benefit

262
How to account for statistical uncertainties in estimating an NI Margin?
1. Discounting (reduction) of the historical control effect size
AND
2. Preservation of the control effect

263
Discounting of the control effect size
Discounting of the historical control effect size is required to account for various sources of uncertainties, for example:
– Lack of constancy assumption– Lack of intra-trial variability– Differences in the patient population,
differences in dosing or duration of control drug

264
Preservation of the control effect
– Preservation of the discounted treatment effect size (M1) is based on the 95% CI around the difference in treatment effects.
– The proportion of the control effect preserved (M2) is based on good clinical judgment.
– Smaller NI margin should be chosen when treatment failures result in irreversible outcome such as mortality.

265
Why Smaller NI Margin?
Let us consider an example, using the endpoint “clinical success/failure”.
Clinical Success(%) Clinical Failures(%)* 95% 5%
85% 15%
3 times!
* Clinical failures include mortality

266
Non-Inferiority - Inference
Let us assume that we have established a NI margin based on “adequate and well-controlled” historical studies.
What would be the statistical inference?

267
Non-Inferiority - Inference
0Test Drug Better
Non-inferiority shown
Non-inferiority shown, but more variability
Non-inferiority not shown
Non-inferiority shown/Superiority is shown
NI Margin
Treatment Difference (Test Drug – Control)Treatment Difference (Test Drug – Control)95% Confidence Intervals95% Confidence Intervals
(1)
(2)
(3)
(4)

268
Historical Evidence in CAP StudiesReliability of the control effect;• The historical data for CAP would not be
considered adequate based on the current standard for “adequate and well controlled” studies. • There are several design issues which may have
introduced bias. • All-cause mortality rates were evaluated in these
historical studies. • There was limited information on the resolution of
clinical signs and symptoms as measured in the current CAP studies.

269
Historical Evidence in CAP Studies (cont…)
• No “true” placebo-controlled studies were conducted. However, studies which used no specific treatment (symptomatic therapy) were considered as “untreated/placebo”.
• There are major limitations in the historical studies including (but not limited to) the following:
• These studies were not blinded
• Some were observational studies, while some were controlled although not randomized per current standards.
• Majority of patients were hospitalized with pneumococcal/lobar pneumonia

270
Historical Evidence in CAP Studies (cont…)
• Subjects were assigned to antibacterial drugs including penicillin and sulfonamides in these studies.
• There was significant variability in mortality rates across studies.
• The difference in overall mortality based on point estimates in pneumococcal/lobar pneumonia from the controlled studies was in the range of 10-19%. However, there is significant variability in these estimates and therefore it lacks reliability.

271
Evans and Evans and
Gaisford Gaisford (1938)(1938)
Graham et. al (1938)
Agranat et. al (1939), Non Europeans
Agranat et. al (1939) Europeans
Controlled Clinical TrialsVariability in Mortality Rates
8.80%
0.10% -0.30%
-6.20%
19%17%
15%
29.20%
36.40%
20.60%
35.50%
10%
-10%
0%
10%
20%
30%
40%

272
Historical Evidence in CAP Studies (cont…)
Is the control effect reproducible? • There appears to be a mortality benefit in hospitalized
CAP patients assumed to have “moderate to severe” pneumococcal /lobar pneumonia.
• However, there is significant variability and associated uncertainties in the estimated historical mortality rates.
• The magnitude of effect may not be reliable or reproducible in all CAP patients who appear to have less severe disease.

273
Historical Evidence in CAP Studies (cont…)
Constancy of the Control effectConstancy of the Control effect
• Does the control effect remain constant over Does the control effect remain constant over time?time?
• How do historical trials compare to current How do historical trials compare to current trials?trials?• Patient population, disease definition, outcome Patient population, disease definition, outcome
criteria, dose, duration of control and, timing of criteria, dose, duration of control and, timing of the outcome assessment.the outcome assessment.
• What is the internal variability of the effect size What is the internal variability of the effect size in the historical trials?in the historical trials?

274
Historical Evidence CAP Studies (cont…)• The antibacterials used in these studies The antibacterials used in these studies included
sulfonamides, penicillin and tetracycline
• The mortality rates in current studies are not very high (~4%).
• The lack of comparability between historical CAP studies and the current studies raise concerns in determining a precise estimate of treatment effect.
– This can be due to any of a number of sources, including differences in patient population, advances in standard of care, differences in the endpoints (mortality or clinical outcomes) or emerging drug resistance issues.

275
Study Quality and Conduct • The historical CAP studies were not
randomized per current standards, blinded or controlled for potential biases. • In general, when using historical studies, the
following issues can undermine its ability to reliably estimate the treatment benefit.
– Subjective endpoint – Lack of specificity in the diagnosis of patients– Spontaneous resolution of signs and
symptoms– Treatment non-compliance– Contribution of adjunctive therapies – Misclassification of outcomes

276
Summary of Historical Evidence• Historical data may be primarily limited to
those with moderate-severe disease due to Streptococcus pneumoniae.
• Historical studies do not provide quantitative estimates of clinical benefit other than all-cause mortality.
• The microbiological etiology in historical studies differs from recent CAP studies.

277
Few Comments-1
• This presentation focused only on “controlled studies” while the IDSA position paper has also considered other studies.
• IDSA position paper reported absolute mortality rate in the controlled studies by pooling studies and did not take into consideration the lack of internal consistency in the mortality rates across studies.– Pooling studies makes several strong assumptions including
similarity in the patient population, disease characteristics, treatment duration and it may be difficult to meaningfully interpret the results.

278
Few Comments-2Kingston et al. JAMA 1961• Tetracycline (demeclocycline) vs. placebo was studied in 290
healthy marine recruits between age 17-22 years with mild CAP. • M. pneumoniae was the etiology in 133 (46%) – which is only a
subgroup of patients.• Several endpoints: mean time to defervescence (temperature <
99F), normalization of chest X-ray, resolution of cough and few other endpoints.
• There are potential multiple testing issues and the inflation of overall type I error rate.
• Duration of fever is based on cumulative percent and it is not clear how missing values were accounted and it has the potential for overestimating the treatment effect.
• Findings are based on a single study and subgroup analysis. It cannot be generalized.

279
Magnitude of Treatment Benefit• There appears to be a treatment benefit based on
all-cause mortality rate in historical studies (although the estimates lacks precision) in hospitalized CAP patients with pneumococcal /lobar pneumonia.
• However, mortality is lower in current studies due to availability of alternative therapies which could rescue patients and prevent death.
The question is, can we translate the mortality benefit observed in historical studies to a clinical benefit as measured in current studies or will it be misleading?

280
Magnitude of Treatment Benefit (cont…)
• The margin chosen for a non-inferiority trial cannot be greater than the smallest effect size that the active drug would be reliably expected to have compared with placebo in the setting of the planned trial (ICH E10).
• A non-inferiority trial design is possible if we use mortality as the endpoint or scientifically justify the extrapolation of the mortality benefit seen in historical trials to another clinically meaningful endpoint.

281
Clinical Failures (~15%) and Mortality Rates Differential Effects (Hypothetical Example)
Figure 1 Figure 2 Figure 3
Mortality Rate
T C T C CT
Rescue Rate*
* Patient who received alternative therapy for rescue; ** Failures other than mortality
T = Test C = Comparator
Clinical Failures in Test and Control Drug
Failure**
15%

282
Future Trial Design Considerations
Primary Endpoint(s):– All-cause mortality – Clinical failure including mortality – PRO Instrument (lacks historical data to link
and therefore at this time can only be used in superiority trials to establish effect)
• E.g. Time to resolution of clinical signs and symptoms

283
Future Trial Design Considerations (cont…)
Primary Hypothesis:– Superiority or Non-inferiority?
• Choice of NI margin (if non-inferiority)– What is the magnitude of antibacterial treatment
effect based on historical studies? – Did we control for variability in the historical data
and discount for the uncertainties?– If so, in what patient population and for which
endpoint?– Did we preserve some fraction of the control
effect?

284
Future Trial Design Considerations (cont…)
Patient Population:
• Identify patient populations that are comparable to those in historical studies to precisely estimate the treatment benefit.– Who should be enrolled?
• Should it based on PORT scores or some other criteria?
• Should only patients with confirmed bacterial etiology be enrolled?

285
Thank you!

286
Exposure-Response Analysis for
Community-Acquired Pneumonia
April 1st, 2008
Christoffer Wenzel Tornoe, Ph.D.Pharmacometrics, Office of Clinical Pharmacology
Center of Drug Evaluation and ResearchFood and Drug Administration

287
Question
Can exposure-response analysis contribute to the discussion of anon-inferiority margin for studies of CAP?

288
Y-intercept as “Untreated/Placebo” Response Estimate
Forrest A et al. Pharmacokinetics and pharmacodynamics of oral grepafloxacin in patients with acute bacterial exacerbations of chronic bronchitis. J Antimicrob Chemother. 1997;40 Suppl A:45-57.
Grepafloxacin against AECB
Treatment Effect
“Untreated/Placebo” Response
AUC/MIC

289
Bottom Line Up Front
• What is the exposure-response derived treatment effect against Streptococcus pneumoniae in patients with mild-moderate CAP?– 37% (95%CI -6;80%)
• Can exposure-response analysis support the choice of non-inferiority margin in CAP trials?– Very likely, but more data (with low free AUC/MIC
ratios) are needed to precisely quantify the treatment effect

290
Background
• Data available– Fluoroquinolone antibiotics have been widely
studied in the treatment of CAP– Reported to exhibit concentration-dependent
killing of pathogens responsible for CAP– Free AUC/MIC ratio is the PK/PD parameter that
correlates with therapeutic effectiveness

291
Pre-clinical Information
Craig WA, Andes DR. Correlation of the Magnitude of the AUC24/MIC for 6 Fluoroquinolones against Streptococcus pneumoniae
with survival and bactericidal activity in an animal model. In Abstracts of the 40th ICAAC, Toronto, Canada, Sept. 17-20, 2000. Abs-289.
Ciprofloxacin, gatifloxacin, gemifloxacin, levofloxacin, moxifloxacin, and sitafloxacin
Free AUC/MICFree AUC/MIC

292
Methodology
• Drug Class– Fluoroquinolone antibiotics
• Enrollment Criteria– Clinical signs and symptoms of CAP (e.g., fever,
cough, chest pain, sputum production) – Presence of a new or progressive infiltrate on
chest x-ray

293
Methodology (cont’)
• Patient Population– Mild-moderate (few severe) CAP– In- or outpatient based on clinical status– Most patients between 40 and 65 years
• Treatment and Administration– 7-14 days of treatment
• Oral therapy (mild-moderate disease)• IV/PO (moderate-severe disease)

294
Exposure-Response DataDrug
Dose
Location/Date/Protocol
Population(ITT / PK)
Admin. Route/Hospitalized/Duration
Primary Endpoint (TOC)
Clinical response (ITT/PP)
Garenoxacin
400 mg daily
Multinational1999-2000
AI464-004
Mild-severe
N=199/106
OralOut patients10 days
7-14 days post Rx
0.84/0.91
Gatifloxacin
Gati 400 mg dailyLevo 500 mg daily
US1997-1998
AI420-038 AI420-038
Mild-severe
N=203/12N=197/16
IVOral, OralIn/Out patients
7-14 days7-14 days
7-14 (5-28)days post Rx 0.89/0.90
0.95/0.93
Gemifloxacin
320 mg daily
Multinational1998-1999
049/061
Mild-moderate
N=290/46N=216/71
OralIn/Out patients
7-14 days7 days
14-21 days post Rx
0.88/0.940.83/0.92

295
Top 5 Pathogens in CAP Studies
N Free AUC MIC Free AUC/MICLevofloxacin
Streptococcus pneumoniae 16 40 (18-61) 0.72 (0.06-1) 97 (26-689)
Gemifloxacin
Streptococcus pneumoniae 30 3.8 (1.7-15) 0.01 (0.002-0.06) 353 (38-1938)
Haemophilus influenzae 16 4.4 (2.2-7.5) 0.003 (0.001-0.01) 2158 (212-6101)
Staphylococcus aureus 14 3.4 (2.0-5.8) 0.01 (0.004-0.01) 3996 (134-923)
Haemophilus parainfluenzae 9 3.4 (1.9-4.6) 0.01 (0.004-0.03) 401 (119-932)
Moraxella catarrhalis 5 3.0 (2.1-4.6) 0.02 (0.01-0.06) 316 (46-568)
GarenoxacinHaemophilus parainfluenzae 26 23 (13-51) 0.1 (0.01-2) 716 (26-2202)
Staphylococcus aureus 19 26 (14-54) 0.08 (0.01-1) 1302 (27-3823)
Streptococcus pneumoniae 16 23 (13-41) 0.05 (0.01-0.06) 595 (222-1337)
Haemophilus influenzae 16 23 (15-43) 0.03 (0.004-0.12) 1903 (206-5562)
Moraxella catarrhalis 7 20 (16-26) 0.03 (0.01-0.03) 877 (540-1710)
GatifloxacinStreptococcus pneumoniae 12 38 (27-53) 0.2 (0.03-0.25) 365 (107-1759)

296
Methodology• Drug Exposure
– AUC– Protein binding– MIC
• Clinical Response– Resolution of signs and symptoms of pneumonia at
test-of-cure visit
• Exposure-Response Analysis– Classification and Regression Tree (CART) Analysis– Logistic Regression
Free AUC/MIC

297
MethodologyDrug Exposure
Dose
Demographic Covariates
Observed PK
Patients with observed PK were used for the E-R analysis

298
Protein Binding was Taken into Account when Pooling Data Across Drugs
Craig WA, Andes DR. In Abstracts of the 40th ICAAC, Toronto, Canada, Sept. 17-20, 2000. Abs-289;

299
MethodologyMIC
All Pathogens
Pathogens with MIC
Pathogen with highest MIC
Patients with Strep. pneumoniae being the mostresistant pathogen were used for the E-R analysis
Strep. pneumoniae with MIC

300
Greater Variation in MIC than Free AUC
0.01
0.1
1
0 20 40 60 80 100
Percentile
MIC
(m
cg/m
L)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
10
0 20 40 60 80 100
Percentile
Fre
e A
UC
(m
cg h
r/m
L)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
+

301
Only Few Patients with Low Free AUC/MIC
100
1000
0 20 40 60 80 100
Percentile
Fre
e A
UC
/MIC
GarenoxacinGatifloxacinGemifloxacinLevofloxacin

302
CART AnalysisOnly 5 Patients with Free AUC/MIC<37
0.0
0.2
0.4
0.6
0.8
1.0
50 100 200 500 1000
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
Estimated Free AUC:MIC break-point = 37
0.0
0.2
0.4
0.6
0.8
1.0
50 100 200 500 1000
| | |N=5 N=69
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
CART Analysis: Select Optimal Free AUC/MIC Breakpoint that Maximally Distinguishes the Response

303
0.0
0.2
0.4
0.6
0.8
1.0
50 100 200 500 1000
| | |N=5 N=69
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
0.0
0.2
0.4
0.6
0.8
1.0
50 100 200 500 1000
| | |N=5 N=69
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
60%
97%
Estimated Treatment Effect of 37% (95%CI -6;80%) for Fluoroquinolones in CAP against S. Pneumoniae

304
Summary
• Relationship between free AUC/MIC and clinical response was established
• Exposure-response analysis limitations– Limited number of patients (5 out of 74) with
sub-therapeutic AUC/MIC ratios since most quinolones are dosed in a manner that result in significantly higher exposures than those associated with failure in animal infection models
– Only Levofloxacin treated patients with sub-therapeutic exposures
– Few clinical failures (4 out of 74)
• More exposure-response data with low AUC/MIC ratios needed to quantify the treatment effect

305
Conclusions
• What is the exposure-response derived treatment effect against Streptococcus pneumoniae in patients with mild-moderate CAP?– 37% (95%CI -6;80%)
• Can exposure-response analysis support the choice of non-inferiority margin in CAP trials?– Very likely, but more data (with low free AUC/MIC
ratios) are needed to precisely quantify the treatment effect

306

307
Clinical Failures
Mean 71 169 51 91 21.2 0.20 353
Drug Study Pathogen Weight Height Age CrCL SexFreeAUC
MICFree
AUC/MICMicro
Levo 038 Str. Pneu 93 168 54 152 F 26.1 1.0 26.1 Failure
Levo 038 Str. Pneu 79 180 32 100 M 33.7 1.0 33.7 Failure
Gareno
004 Str. Pneu 57 170 53 17 F 40.1 0.03 1337PresumedPersisted
Gareno
004 Str. Pneu 57 163 38 110 F 17.9 0.03 597Presumed persisted

308
Sub-therapeutic patients
Mean 71 169 51 91 21.2 0.20 353
Drug Study Pathogen Weight Height Age CrCL SexFreeAUC
MICFree
AUC/MICClinical
Levo 038 Str. Pneu 93 168 54 152 F 26.1 1.0 26.1 Failure
Levo 038 Str. Pneu 79 180 32 100 M 33.7 1.0 33.7 Failure
Levo 038 Str. Pneu 67 185 37 229 M 18.2 0.5 36.3 Success
Levo 038 Str. Pneu 87 160 54 132 F 27.0 1.0 27.0 Success
Levo 038 Str. Pneu 83 163 32 111 F 31.2 1.0 31.2 Success

309
AUC vs. Covariates
10
100
40 60 80 100 120
Body weight (kg)
AU
C (
mcg
hr/
mL)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
10
100
20 40 60 80
Age (years)
AU
C (
mcg
hr/
mL)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin
10
100
50 100 150 200
Creatinine clearance (mL/min)
AU
C (
mcg
hr/
mL)
GarenoxacinGatifloxacinLevofloxacin
Body weight Age
Creatinine Clearance

310
AUC percentiles
10
100
0 20 40 60 80 100
Percentile
AU
C (
mcg
hr/
mL)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin

311
Free AUC percentiles
10
0 20 40 60 80 100
Percentile
Fre
e A
UC
(m
cg h
r/m
L)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin

312
MIC percentiles
0.01
0.1
1
0 20 40 60 80 100
Percentile
MIC
(m
cg/m
L)
GarenoxacinGatifloxacinGemifloxacinLevofloxacin

313
Levofloxacin MIC percentiles
0.1
1
0 20 40 60 80 100
Percentile
Levo
floxa
cin
MIC
(m
cg/m
L)
GarenoxacinGemifloxacinLevofloxacin

314
Free AUC/MIC percentiles
100
1000
0 20 40 60 80 100
Percentile
Fre
e A
UC
/MIC
GarenoxacinGatifloxacinGemifloxacinLevofloxacin

315
No cut-point identified for Free AUC vs. Clinical Response Rate for Strep. Pneumoniae
0.0
0.2
0.4
0.6
0.8
1.0
0 10 20 30 40 50 60
||||||||||||||||||||||||||| || | ||| ||||
|
| | | |
|
|||| ||| | | ||
|
| | |||
|
||| ||| | | || | | |
N=74
Free AUC
Pro
babi
lity
of C
linic
al R
espo
nse
Streptococcus pneumoniae

316
67% (95% CI: 30-93%) Clinical Response Rate for Strep. Pneumoniae with MIC>0.75
Estimated MIC break-point = 0.75
0.0
0.2
0.4
0.6
0.8
1.0
0.01 0.1 1 2 4 8
| ||||||||| ||||||||||||||||||||||
||
|||||||| ||||||||||||||||
|
||||||||||||||||
|
||||| |||||||
||
||||||
|| | |
N=88 N=9
MIC
Pro
babi
lity
of C
linic
al R
espo
nse
Streptococcus pneumoniae

317
Exposure-Response Relationship for Haemophilus influenzae
0.0
0.2
0.4
0.6
0.8
1.0
500 1000 2000 4000
| || |
|
| || || | || || || | |||| || || || ||| |
N=32
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
Haemophilus influenzae

318
0.0
0.2
0.4
0.6
0.8
1.0
50 100 200 500 1000 2000
|
|
| ||
|
|| | || |
|
|| || || || || ||| ||
| |
||| ||
| | |N=8 N=27
Free AUC/MIC
Pro
ba
bili
ty o
f C
linic
al R
esp
on
seHaemophilus parainfluenzae
Exposure-Response Relationship for
Haemophilus parainfluenzae
Estimated fAUC:MIC break-point = 201

319
Exposure-Response Relationship for
Staphylococcus aureus
0.0
0.2
0.4
0.6
0.8
1.0
25 50 100 200 500 1000 2000
||| || | || | ||
|
| | || || || ||| | | || | |
| | |
|
N=33
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
Staphyloccocus aureus

320
Exposure-Response Relationship for
Moraxella catarrhalis
0.0
0.2
0.4
0.6
0.8
1.0
50 100 200 500 1000
|| || | || || ||
|
N=12
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
Moraxella catarrhalis

321
Levofloxacin (Pulmonary 001)
0.0
0.2
0.4
0.6
0.8
1.0
20 40 60 80 100 150
| | | | |
N=5N=5
N=5N=5
Free AUC/MIC
Pro
babi
lity
of C
linic
al R
espo
nse
Levofloxacin

322
Mean (range) Free AUC, MIC, and Free AUC/MIC by Pathogen in CAP Studies
N Free AUC MIC Free AUC/MIC
Streptococcus pneumoniae 74 21 (1.7-61) 0.2 (0.002-1) 352 (26-1938)
Haemophilus parainfluenzae 35 18 (1.9-51) 0.1 (0.004-2) 635 (26-2202)
Haemophilus influenzae 32 13 (2-43) 0.01 (0.001-0.12) 2031 (206-6101)
Staphylococcus aureus 33 17 (2-54) 0.05 (0.004-1) 918 (27-3823)
Moraxella catarrhalis 12 13 (2-26) 0.02 (0.01-0.06) 643 (46-1708)

323
Levofloxacin for Community-Acquired Infection
Preston SL et al. Pharmacodynamics of levofloxacin: a new paradigm for early clinical trials. JAMA. 1998;279:125-9.
Results were reproduced using data from LFOVIB-MULT-001 study in NDA 20634 but mainly driven by non-S. pneumoniae pathogens and not valid for determining M1

324
Clinical Response vs. Free AUC/MIC with “Placebo”
response of 70%Levo/Gati/Gemi* (N=36/12/31)Ambrose Analysis
*Ambrose PG, Bhavnani SM, Owens RC. PK-PD of antimicrobial therapy: It’s not just for mice anymore. Clin Infect Dis. 2007;44:79-86.
Estimated “breakpoint” = 33.8 hr

Critical Considerations in CAP Trial Design
A Consultant’s Perspective
FDA Advisory Committee Meeting1 April 2008
George H. Talbot, MD, FIDSA


3/31/08 Talbot
FDA’s Charge
Provide for the AC: • A “reality check regarding what is feasible
vis-à-vis trials conducted by industry, based on your discussions with industry colleagues, investigators, and other regulatory agencies.
• Your vision of what might be a reasonable path forward for future trials for CAP products ...”

3/31/08 Talbot
Discussion Points
• Why do we need new antibiotics for CAP?• Undertaking a CAP clinical trial program• Major trial design issues• Conclusions• Next steps

3/31/08 Talbot
Disclosures
• June 2006-Oct 2007: CMO of Cerexa, Inc.
• Consultancies to Actelion, Calixa, Cerexa, PTC, Shire, Theravance, ViroPharma, Wyeth; advise Cerexa on CAP program
• Equity option grants: Calixa, Mpex
• Diversified healthcare equity portfolio
• Member of IDSA’s AATF
• Self-supported to attend this meeting
Perspectives Presented are Mine

Why Do We Need New Antibiotics for CAP?

3/31/08 Talbot
Why Do We Need New Antibiotics for CAP?
• Emerging resistance in CAP pathogens– Streptococcus pneumoniae
• Macrolide• Cephalosporin (ceftriaxone)
– MRSA?
• Treatment options for other RTIs– Some patients with sinusitis, acute exacerbation of
chronic bronchitis, or acute otitis media DO require antibiotic therapy
– If new antibiotics can’t easily be studied in those indications, CAP becomes the last bastion for RTI drug development

3/31/08 Talbot
Why Do We Need New Antibiotics for CAP?
• Antibiotic pipeline in general is at risk– Decreasing investment by large pharma– “Deconstructed” basic R&D platforms– Increased clinical trials costs & uncertainty– Better opportunities elsewhere– New molecules often from Japanese innovators
• The “new” descriptor can be falsely reassuring– Many “new” compounds are recycled from older
innovators

3/31/08 Talbot
Why Do We Need New Antibiotics for CAP?
• The CAP pipeline has had problems– Telithromycin (oral)– Faropenem (oral)– Gemifloxacin (oral)– Gatifloxacin (oral)
• Oral, as well as IV, options are needed – Hospital admission/discharge pressures– Lots of outpatient CAP– Many hurdles for oral compounds
• New classes/ MOAs desirable

3/31/08 Talbot
Why Do We Need New Antibiotics for CAP?
• One day, some of us, or one of our family members, will need one….
• Decisions made in 2008 will determine what antibiotics are available in 2015.
“The lesson of history is that we need a pipeline.”
John Bartlett, MD

Undertaking a CAP Clinical Trial Program

3/31/08 Talbot
Thinking about “Industry”
• “Industry” is not a monolith– Large pharma vs. “Biotech”– Differing goals, assumptions, & constraints– However, there are….
• Common denominators for pharma R&D– Finding funding,– Fiduciary responsibility to shareholders, AND– Doing the right thing for patients and society
Decisions are Complex
R&D Scientists Believe in What They Do

3/31/08 Talbot
Context of a Starting a CAP Program
• The multiplicity of audiences, worldwide– Patients– Investigators– IRBs/ ECs– Regulatory agencies– Prescribing physicians (medical need)– Formularies and insurance companies
Varying Needs Add Risk & Uncertainty

3/31/08 Talbot
Will the Trial Program Prove to Be:
• Credible?
• Predictable?
• Feasible?

3/31/08 Talbot
Credibility
Scientific Considerations:• Are validated methods/ tools available to
design, conduct and analyze clinical trials? • Will the data/ conclusions withstand
rigorous scientific examination?• Will regulators worldwide find the results Will regulators worldwide find the results
acceptable?acceptable?• Will the results address an unmet need or
provide data relevant to current practice?

3/31/08 Talbot
Credibility
Ethical Considerations:• Is trial design acceptable to all audiences?• VERY difficult for pharmaceutical
companies to be innovators if doing so requires contravening established clinical practice guidelines/ investigational precedent.– Example: placebo-controlled trials when
audiences expect active controls
Examine Controversial Hypotheses in Non-pharma Sponsored Trials

3/31/08 Talbot
Predictability
• What predictability ISN’T: Stacking the deck to ensure the results you want!
• What it IS: Identifying the clinical, statistical, regulatory, & commercial variables that impact the trial results – and accounting for them carefully in design, conduct, & analysis
Predictability is an Essential Consideration -- Trial Timeframes are Measured in Years, and
Costs in Millions of $

3/31/08 Talbot
Why is Predictability So Important?
Direct Study Costs
Fully Loaded Costs
Patients Enrolled
Cost per Patient
Trial #1 $18.1 million $19.6 million ~550 $36,600
Trial #2 $18.5 million ~$19.0 million
~600 $31,700

3/31/08 Talbot
Why is Predictability So Important?
Direct Study Costs
Fully Loaded Costs
Patients Enrolled
Cost per Patient
Trial #3 $17.2 million $21.0 million ~430 $48,800
Trial #4 $9.2 million
$12.6 million 425 $29,600

3/31/08 Talbot
Why is Predictability So Important?
Direct Study Costs
Fully Loaded Costs
Patients Enrolled
Cost per Patient
Trial #5 $28.0 million $41.5 million ~600 $69,100
Trial #6 $19.0 million $31.6 million ~625 $50,500

3/31/08 Talbot
What’s at Stake: A Lot …
• For early stage development, venture capital interest is high now, but opinions can shift rapidly
• For Phase 3, smaller companies generally need a large pharma partner
• So, $$ currently targeted for CAP could go elsewhere – – Other indications, – Other therapeutic areas, – Even other industries

3/31/08 Talbot
Compounds at Risk on the Predictability Axis
• Recently completed or ongoing P3 trials– Cethromycin– Tigecycline– Ceftobiprole– Ceftaroline
• Potential for late-stage development– Nemonoxacin – Faropenem – EDP-420 – Rx-1741 – etc.….
Clinicaltrials.gov accessed 3/27/08

3/31/08 Talbot
Compounds at Risk on the Predictability Axis
• Overhanging issues:– NI design and acceptable NI margin– Outcome measures– Populations studied
• Example: Recent CAP studies– NI margin: 10%– Populations: PSI I-V, ~80% II-IV– Outcome measure: Clinical response, incl.
death, in Clinically Evaluable patients (i.e., regardless of whether pathogen isolated)
Poster L-1450, ICAAC 2007

3/31/08 Talbot
Compounds at Risk on the Predictability Axis
• CAP pathogens (% of enrolled)
Poster L-1450, ICAAC 2007
Pathogen n %
Atypicals 147 17.4
H. influenzae 33 3.9
M. catarrhalis 8 1.0
S. pneumoniae 190 22.5
Culture 109 12.9
Urine Ag 81 9.6
Culture + Patients are in the Minority

3/31/08 Talbot
Feasibility
• Are the scientific & regulatory requirements understood?
• Can the trials be completed within an acceptable time frame, especially:– Design– Enrollment– Regulatory review
• Will the costs of the trials make sense compared to other options?

3/31/08 Talbot
Clear Regulatory Guidance is Essential – Ideally, Without Jeopardizing Decisions
Already Made in Good Faith
Deciding to Start a CAP Trial: Summary

Major Design Issues in CAP Clinical Trials

3/31/08 Talbot
Specific Design Considerations
• Spectrum of Study Drug
• Dose Selection
• Choice of Comparator*Choice of Comparator*
• IV-Oral Switch
• Inclusion/Exclusion Criteria*Inclusion/Exclusion Criteria*
• Statistical Assumptions*Statistical Assumptions*
* Focus points* Focus points

3/31/08 Talbot
Spectrum of Study Drug
• Macrolides & FQs efficacious vs. the spectrum of CAP pathogens
• Conundrum for cephalosporins: – Some data showing improved outcome with
addition of macrolide in pneumococcal CAP– The spectrum of cephs does not include
atypical pathogens….
How to Provide Optimal Therapy, without an Overlap in Spectrum that Confounds
Efficacy Assessment?

3/31/08 Talbot
Issues in Dose Selection Rationale for CAP
• Potency (MIC) against target organisms• Activity in animal pneumonia models• Human Phase 1 PK• Known PK-PD relationships (plasma)• PK-PD modeling• Lung penetration • Consideration of active site in lung• Prior experience with class• Phase 2 data if available

3/31/08 Talbot
Dose Selection
• State of the art science allows prediction of efficacious dosing regimens
• However, we must beware the unexpected:– Different pathogens than anticipated– Higher than expected MICs of target pathogens– Drug inactivation at target site– PK variability– Drug-drug interactions

3/31/08 Talbot
Choice of Comparator
• There is a substantial, consistent antibiotic treatment effect in CAP (HESDE)– Mortality– Morbidity– Historical, discordant Rx, daptomycin data
• Effect size varies by severity of illness– Most pronounced in moderate to severe CAP, but
clinically meaningful in mild CAP
• Asking industry to conduct placebo-controlled studies in CAP would place them in an untenable position with many of their audiences
IDSA CAP position paper

3/31/08 Talbot
Choice of Comparator
• Exercise due care in comparator selection:– Spectrum of activity– Dosing regimen (which may have changed
since initial regulatory approval)– Tolerability
• What isn’t acceptable – Use of a comparator that is suboptimal re:
these parameters - in hopes of demonstrating superiority in an active-control study

3/31/08 Talbot
IV-Oral Switch
• Standard of care in many countries• Pressure from insurers, hospitals• Clinical trial design utilizing oral switch
– Relevant to clinical practice – Improves trial feasibility
• Conundrum: potential confounding of efficacy and safety assessments

3/31/08 Talbot
Inclusion/Exclusion: Patient Populations
• CAP severity can be defined– Well studied, validated prediction tools– Can be adapted as severity assessment– Meet constancy assumption– Feasible for patient trial enrollment– Relevant to clinical practice & product label
• Suggested approach– Pneumonia Severity Index as base– Adjust PSI for selected other variables that
reflect severity but are not in PSI
IDSA CAP position paper

3/31/08 Talbot
Inclusion/ Exclusion: Prior Antibiotic Therapy
• Artifactually improves response in CAP
• The “obvious” solution – avoid prior Rx – has major logistical consequences
• We need better approaches to this issue – At present, the most attractive is to allow a
single dose of a short-acting agent
– In the future, rapid diagnostics may facilitate inclusion of non-treated patients only
Clin Infect Dis, 2008; 46: 1142

3/31/08 Talbot
Inclusion/ Exclusion: Which Pathogens?
• Documentation of treatment effect– Data abundant for S. pneumoniae and, to a
lesser extent, “Atypicals” – Fewer data for H. influenzae, other “Typicals”
• However, – Diagnostic accuracy to allow timely triage for
trial entry is not yet feasible for typical or “atypical” pathogens
– In clinical practice, pathogen often not known
IDSA CAP position paper

3/31/08 Talbot
Inclusion/ Exclusion: Which Pathogens?
• Restricting primary trial analysis to – Typical pathogens only - will at least double clinical trial
sample size – S. pneumoniae only - will multiply 4-5-fold the required
sample size
• Such increased “N” will add time & cost – each a powerful deterrent
• Trial data based on clinically defined populations are useful and generalizable
• Logistically, retaining clinical criteria for primary evaluation is desirable

3/31/08 Talbot
Statistical assumptions: NI or Not NI?
• NI design justified- based on HESDA & constancy– Moderate to severe CAP with dichotomous
outcome: 10% delta– Mild CAP: 5% delta with dichotomous outcome– Mild CAP: ?10% delta for time-to-events
• Superiority design neither feasible nor justifiable for registration trials – patients would be enrolled: – Little chance of the trial meeting its endpoint– Potentially exposed to suboptimal comparator

3/31/08 Talbot
Statistical Assumptions: Outcome Measures
• Relevant outcome measures (endpoints) have been identified
• Moderate-severe CAP– Mortality & morbidity – Consider composites: Death, time to discharge,
etc.
• Mild CAP– Morbidity – Time-to analyses??
• Issue: instruments validated?• Needed now: studies of mild-mod CAP

3/31/08 Talbot
In Conclusion (1)
• Society will benefit from the availability of new antibiotics for treatment of CAP– NOT just for CAP– Resistance is increasing– Decisions now determine our options in 2015
• CAP trials must be – Credible, predictable, and feasible– Needed: updated, clear, & specific guidance

3/31/08 Talbot
In Conclusion (2)
• A substantial treatment effect of antibiotics in CAP has been established
• Superiority design?– Placebo-controlled: very problematic– Active control: difficult & unnecessary– Each could place patients at risk
• NI design?– Scientifically appropriate – Logistically feasible

3/31/08 Talbot
In Conclusion (3)
• Utilizing an NI design– Patient populations can be defined that satisfy
clinical & regulatory demands: “PSI-plus” for defining severity
– Outcome measures incorporating both morbidity and mortality are appropriate
• Pathogens– Technology does not yet allow identification at
entry to enrich study population– Restricting trial analysis to micro subsets will
add lots of time and cost to trials

3/31/08 Talbot
How the Advisory Committee Can Help
• Consider the proposals presented on both their scientific merits AND the ability of companies to implement them
• Make the best possible, balanced decisions today (maybe they won’t be perfect…)
• Help our FDA to give prompt, clear guidance for antibiotics in the wings
Facilitate the Development of Safe and Effective New CAP Therapies

3/31/08 Talbot
Acknowledgements
• FDA-IDSA CAP Workshop discussions
• IDSA’s AATF
• Advanced Life Sciences, Cerexa, Replidyne, and Wyeth for CAP trial cost data

Thank you for your attention!