Embed Size (px)
Citation preview


ANNUAL REPORT
A Report contributing to the betterUnderstanding of NLR supported program activities in Nepal
Year 2012
Editorial Offi ce:
Netherlands Leprosy Relief,Country Representative’s Offi ce,
Kathmandu, Nepal; Po. Box 25270
Email:
[email protected], [email protected]
[email protected], [email protected]
Telephone:
+977 4252115; +977 016227564; +977 021 526571
091-522499
Fax:
+977 1 4245882; +977 021 524640, +977 091 521927
This report is published annually by NLR Nepal. This report is provided free to
all institutions and individuals working with leprosy control & CBR in Nepal and NLR
Amsterdam, WHO, ILEP etc outside of the country. In addition to this free distribution
may possible as per demand of related others either institutions or individuals for those
who may have some value of this type of report.

Annual Report Office (APO)
Netherlands Leprosy Relief (NLR)
Nepal
2012

List of abbreviations
AHW Auxiliary Health WorkerBLC Biratnagar Leprosy ClinicDLC Dhangadhi Leprosy ClinicCLAPS Community Leprosy Affected Persons for Self-helpBPKIHS BP Koirala Institute of Health Sciences CM Community MemberDHO District Health Offi cerDTLA District Tuberculosis / Leprosy AssistantEDR Eastern Development RegionELCP Eastern Leprosy Control ProjectFWLCP Far Western Leprosy Control ProjectFCHV Female Community Health VolunteersFGD Focus Group DiscussionHA Health AssistantHE Health EducationGON Government of NepalHP Health PostHS Health Staff LCD Leprosy Control DivisionMB Multi bacillaryMDT Multi Drug TherapyMOH Ministry of HealthNGO Non Governmental OrganizationNLR Netherlands Leprosy ReliefPB Pauci bacillaryPHC Primary Health CenterPHO Public Health Offi cerPLD Person with Disability due to Leprosy POD Prevention of DisabilityPT PatientPWD Person with DisabilityRFT Released from TreatmentRTLA Regional Tuberculosis / Leprosy AssistantSHP Sub Health PostCR Country RepresentativePL Project LeaderFC Field Program Co-ordinatorTO Training Offi cerLS Leprosy SupervisorVDC Village Development CommitteeVHW Village Health WorkersWHO World Health OrganizationSA Statistical AssistantNFDN National Federation of Disabled Nepal NNSWA Nepal National Social Welfare Association

Annual Report Office (ARO), NLR Nepal for 2012
SummaryAfter 3 years of witnessing the declaration of leprosy elimination at country
level leprosy elimination has been achieved at regional level at regional levels.
Having its own understanding of the indicator for the elimination worldwide,
NLR has modified its supporting strategies to sustain leprosy control activities as
well as to alleviate the consequences of the disease. Now the national leprosy
control program also has expanded its activities to care after cure through CBR
approach. In this way the leprosy control program shows its dynamism and
proves to be one of the successful programs in Nepal. The numerical burden
of the disease is decreasing including new cases, under treatment cases, child
& cases with grade II disabilities. At the same time, we consider the leprosy
burden not only the number of cases who need MDT but also those affected people suffering from its
consequences. Major consequences of leprosy are social & environmental barriers associated with
physical impairments. Stigma, loss of dignity & prejudices are the results of such consequences. There are
still many challenges on further reducing the burden of this disease in the communities.
In the fiscal year 2012, 1214 new patients were detected in NLR supported two Regions including
51 cases with DG II. New case detection rate is in decreasing trend but fluctuating which is 13.2 in EDR &
FWDR per 100000 populations during this year. Some active case detection activities were introduced in
this reporting year such as active contact examination for family & neighbours, mobilization of DAG and
community awareness activities followed by home visits. New case detection rate (NCDR) still remains
high in some of the districts indicating that transmission of the disease is still high resulting heavy leprosy
burden in the community. MB proportion in Eastern & Far Western region is 50.4% & 56% respectively.
Skin smear examination is done for more than 80% of newly detected cases. The disability grade II among
new cases is 3.6% in Eastern & 6% in Far Western region where as the additional deformities developed
in the patients during their MDT as calculated by comparing the EHF scores at the beginning and end of
the treatment is 0.11% in EDR & 1.23 in FWDR, which is quite acceptable considering the nature of disease
to develop reactions. The treatment completion rate has been sustained to above 97% in EDR & 93% in
FWDR.
For all these achievements supportive activities such as training is very essential. In the past
reporting year a total of 190 health workers were trained in our project area on leprosy & disabilities
issues. Quarterly review meetings were continually held at various levels as monitoring tools of leprosy
control activities which were very effective opportunity for on the job training to BHS staffs. Similarly,
the combined technical supervision together with regional and district authorities was found to be more
effective in administrative as well as technical on the job training for health personnel. During the reporting
year more than 70% of leprosy treatment centres in high endemic districts & District Health Offices were
visited in the project area.
As community empowerment and involvement is crucial for the successful implementation of
program, the project has carried out various activities to enhance community participation. Apart from
regular activities like patient education in clinics, distribution of reading materials and other community
education materials, we continued the community health education through affected persons & leprosy

patients. The people affected by leprosy have formed self-care groups in many areas and are being
involved in disseminating messages about the suggestive signs of leprosy, availability of free treatment
and its curability, importance of full course and timely treatment. They also share their experiences about
the need of self-care for insensitive hands, feet and affected eyes. The world leprosy day & world disability
day were celebrated weeklong including different awareness raising activities in both the regions followed
by press conferences and advocacy meetings on final day. The Netherlands Leprosy Relief (NLR) also
participated in the celebrations at national level.
Activities aiming to prevention of secondary disabilities and deformities are prime importance and
more priorities are given by our projects. POID activities in the regional clinics with some minor surgeries
in Koshi Zonal & Seti Zonal hospitals as well as the functional peripheral POD clinics and SCGs in VDCs
have resulted in decrease of referrals to other hospitals. Early case detection and proper management of
reactions and neuritis are the main stay in prevention of primary disabilities. To enhance such activity at the
field level POID services (reaction management, ulcer care etc) have been provided through some PHCs
in the districts. We also provide the assistive and protective devices to the needy patients. Counselling
service has been found beneficial for patients who find difficulties to cope with the life because of stigma
due to leprosy and its consequences.
Rehabilitation activities for persons with disabilities including leprosy affected are continuing in
Morang & Kailali as pilots. District disability management & coordination committee (DDMC) chaired
by local development officer is quite active at district levels. Our program strategy of mainstreaming
disability due to leprosy to general disability and to general community development activities has started
to show positive results at different level. We have established very good partnership with other I/NGOs
& government agencies to enhance multi sector & multi dimensional approach on rehabilitation activities
especially in Morang & Kailali. Disability due to leprosy is being given high priority. At the same time
National strategy for leprosy 2011-2015 has been finalised & published by GON on the basis of WHO
global strategy that has clearly focused for the need of rehabilitation for PWDL along with treatment &
empowerment.
Lastly, we express our sincere thanks to everybody who encouraged, participated and supported us
in this struggle to reduce the burden of leprosy & management of disabilities. We would like to express
our sincere thanks especially to the director of the Leprosy Control Division for his valuable guidelines,
encouragements and support for the program. Beside this, our special thanks go to and directors of Eastern
& Far Western Regional Health Directorates, all D/PHOs, DEOs, LDOs, WDOs, RTLOs and DTLOs for their
remarkable contribution to the program. We cannot stay aside not saying few words of appreciation to the
NLR, NFDN, NELRA, NNSWA and NLF and the GoN staffs who were involved in the programme for their
contribution to the success of the program. We also would like to thank our colleagues I/NGOs, partners
and friends in our mutual quest for leprosy control who have been always supportive.
Finally, we would like to express our sincere thanks to the Netherlands Leprosy Relief, Amsterdam
for continuous technical and operational guidelines and generous financial support, which are the most
crucial inputs for the successful running of the program. We appeal to everybody “Let us continue our
efforts to create Nepal without leprosy”

Pg 1Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 1Annual RReportt
1. Introduction
1.1 Procedures for producing this ARO
Current report is developed on the basis of MAPA prepared on 2011 based on logical framework that
was developed during the preparation of five years NLR projects in Nepal and that of annual planning (AP)
& annual budget (AB) for 2012.
This report was prepared with the contribution from field and program coordinators and other senior
staff from NLR and implementing partners. Performances achievements of both CBR & leprosy projects of
past year 2012 were reviewed, analysed and merged to develop overall NLR progress report.
1.2 NLR support on leprosy control & rehabilitation programs in Nepal
The NLR support is provided through long-term project agreements. Since last few years, NLR has
replaced its strategy to support the national leprosy control projects and extended it to cover the disability
management and rehabilitation, through CBR approach. The emphasis is primarily given to capacity
building through training of local health workers and other implementing partners, program management,
supervision, logistics and activities related to the prevention of disabilities, health education and, where
necessary, investments in drugs, equipment, vehicle etc. NLR strives to work and coordinate activities
with other national and international organizations active in this field such as ILEP members, NGOs, DPOs
and CBR organizations.
NLR has its country representative office in Kathmandu and two field projects in Eastern and Far
Western regions of Nepal covering 25 districts (16 in EDR & 9 in FWDR). Ministry of Health and Population,
LCD, RHD, D/PHO are the partners for the leprosy control and financial support for this is provided
through government Red Book. Additional direct technical support on case management, capacity
building & supervision/monitoring is also provided from field projects of the respective areas. Support
on rehabilitation goes through NGO partners as well as related GON line ministries offices districts. For
rehabilitation services piloting is being done in two districts of Nepal (Morang – Eastern; Kailali – Far
western). As per project agreement with social welfare council (SWC) the following are the partners
mentioned in project document for NLR in Nepal;
• Ministry of Health and Population, Department of Health Services, Leprosy Control Division (LCD)
• Ministry of Health and Population, Department of Health Services, Leprosy Control Division (LCD)
and its offices in regions and distrits
• National Federation of Disabled Nepal (NFDN), Central Office Kathmandu, Regional offices
• SagarmathaApangaSangha (SAS), Saptari

Pg 2 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 2 AAnnuall Report
• Apang BikashSangha (ABS), Udayapur
• Apanga Sewa Sangha (ASS), Dhankuta, and Panchthar
• Nepal Leprosy Fellowship (NLF), Sunsari
• Community Based Rehabilitation (CBR), Biratnagar
• Nepal National Social Welfare Association (NNSWA), Mahendranagar, Kanchanpur
In addition to above mentioned partners; there are different networks (AIN, NLN, CBR group etc) and also
different likeminded I/NGO partners like Plan Nepal, HI, Action AID, Save the children, World Vision,
Karuna Foundation etc where NLR has established a good linkage & coordination in different activities
which contributed to the following achievements:
• Non-leprosy I/NGOs have started to include persons affected by leprosy and persons with disability
due to leprosy in their areas of support
• DPOs and their networks at districts, regional and national level have understood causes &
consequences of leprosy and started to give priority to leprosy affected persons in mainstream
disability movement.
• Persons with disability due to leprosy have started to entertain GON provisions on disability with
access to disability ID cards that was never done before
• Leprosy has been included in the definition of disability and included & incorporated in GON policy
papers
• Social stigma against leprosy is reducing, dignity, self respect & self reliance of individuals’ improved,
interactive participation is increasing.
• DPOs & other stakeholders are taking ownership of Self care groups in the communities
• Persons affected and with disabilities due to leprosy have formed district level committees in three
districts of eastern region viz, Morang, Jhapa & Sunsari
• DPOs have started to include persons affected by leprosy in their executive bodies
• Leprosy organizations & rehabilitation centers are opened up for general disabilities
• New National strategies for leprosy control has incorporated rehabilitation.

Pg 3Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 3Annual RReportt
1.3 Reporting on Indicators and targets
INDICATORS FOR ‘PROGRAMME SUPPORT’ (95)
Indicators Basic/ Optional Target (if set) Achievement
% of plans and reports received in time by HO B 2 time 100%
% of plans received in time and according to
standards by HOB 2 time 100%
% of planned RBM planning workshops
implemented according to (long-term) planningB 2 time 100%
% of planned monitoring visits by technical staff/
consultants executedB 1729 days 103% (1780)
% of monitoring visits about which a reports
has been produced, timely and according to
standards
B 1133 days 92% (1042)
% of planned NLR M&E meetings implemented B 9 time 100%
% of planned reviews and (mid-term and end)
evaluations implemented according to planning) B 6* 100%*
% of projects that were implemented successfully
(according to RO) B 2 type 100%
% of budget that has been used B 36729874 94.5%
% of counterpart funds that is released to projects
in time for useB 2** 100%**
% of staff positions in project teams filled
adequately B 31 person 100%
% of NLR programme budget covered by local
fundraising among private and/or institutional
donors
B 0 0
% of NLR programme budget covered by local
fundraising among private and/or institutional
donors
B 0 0
*These are the review meetings and mid term evaluation is planned in 2013.
**Inclusive Education is supported by Plan Nepal and DDCC Morang supported VDMC meetings
Because of some delay in budget approval we had to put more efforts on the remaining period for the
completion of targeted activities. Annual budget expenditure of 2012 is 94.5% including the expenditure
through Redbook for leprosy control support. About the reports of the monitoring visits we have developed
our own system of brief & detail reporting, reports of 1042 days out of 1133 meet that standard. Our
learning during this period is further usefulness of RBM, and we have developed & are using computerized

Pg 4 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 4 AAnnuall Report
software to support this system and this has helped us a lot for proper planning, timely monitoring of
implementations and achieving the results at the field projects.
INDICATORS FOR ‘CASE FINDING’ (10) Indicators Basic/ Optional Target (if set) Achievement
Number of new cases detected per year B 1214
% of new cases presenting with grade-2
disabilities/impairments B 4.2%
Proportion of child cases among new cases B 6.5%
The data presented here covers the period of 16 July 2011 to 15 July 2012 to match with GON
fiscal year to avoid errors and confusions. Number of new cases as well as new case detection rate is
fluctuating in Nepal. Grade-2 disability that is now 4.2% in NLR supported areas. Concentration of the
program need to be more on interruption of chain of transmission that may helps to bring down existing
high child proportion of 6.5%.
INDICATORS FOR ‘CASE MANAGEMENT’ (20)
Indicators Basic/ Optional Target (if set) Achievement
% of patients who develop new/additional
disability during multidrug therapyB <1%
0.16% EDR &
1.23 FWDR
Treatment completion rate among PB and MB B >95%
97% & 98% EDR
and 90% & 96%
FWDR
Number of patients who completed treatment
successfully B All 1148
Number of people trained in self-care B All needy 1187
Number of self care groups functioning with
NLR support/facilitation B
All endemic
VDCs163
Number of self care groups established through
NLR support/facilitation (during the year)B 74 43
Since last several years the patient compliance and regularity remain at the level of satisfaction in
both the regions. This became possible because of well managed CRS (cross referral system). Patients’
diagnosed at higher level are sent to their respective VDCs for regular MDT. Regular monitoring (review)
meetings are becoming quite helpful on situation analysis and solving the noted problems at any level.
Self-care activities through mixed self-care groups are found effective not only for ulcer healing &
physical wellbeing but also to empower the individuals and reducing stigma at community level. Most of

Pg 5Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 5Annual RReportt
these self care groups will be matured after a year and be the part of Disabled peoples’ organization –
DPO. Our strategies in this regard is mainstreaming of disability due to leprosy to general disability and
further mainstreaming of disability to general development programs keeping in priority that leprosy is not
excluded. Our vision is community based inclusive development with the focus on: equal opportunities for
all, equal rights and barrier free environment especially for leprosy affected & disability.
INDICATORS FOR ‘MEDICAL REHABILITATION’ (30)
Indicators Basic/ Optional Target (if set) Achievement
Total number of people that have been provided
with medical rehabilitation services (Total = paid
for by NLR + facilitated by NLR)
B 1671
Medical rehabilitation includes surgeries, assistive & protective devices, self-care & physiotherapy
services, treatment & referral services for complications & others related to health for PWD/PWDL. This
service can be enhanced to many more people if existing GON provisions are better implemented and
proper reporting system is established.
INDICATORS FOR ‘STIGMA’ (40
Indicators Basic/ Optional Target (if set) Achievement
% of People Affected by Leprosy with increased
self-esteem (e.g. measured with ISMI, Most
Signifi cant change or other qualitative methods)
O
Assessment
done for 115
persons this year
% decrease in stigma towards People Affected
by Leprosy in the community after intervention
to reduce stigma (e.g. measured with EMIC
scale)
O
Assessment
done for 115
persons this year
Number/% of discriminatory policies and laws
that have been repealed or amendedB 0
It has been found from a number of studies that stigma against persons affected by leprosy is
caused mainly due to ulcers & impairments. Because of self care activities through self care/help groups
& establishment of POID centres at peripheral level ulcers are healed easily. Disability due to leprosy has
been mainstreamed into general disability and disability issue is now started to be taken development
issue rather than individual problem so that perception as well as attitude of the community people has

Pg 6 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 6 AAnnuall Report
been changed. Our strategy of “change the system to fit the individuals but not to change the individuals
to fit the system” is found appropriate to reduce stigma and to increase dignity and self reliance of persons
affected by leprosy.
INDICATORS FOR ‘NON-MEDICAL REHABILITATION’ (50)
Indicators Basic/ Optional Target (if set) Achievement
Total number of people who received education
support (Total = paid for by NLR and facilitated
by NLR)
B 42
% of relevant meetings/workshops in which
People Affected by Leprosy participatedB
136 groups
(about 75%)
Total number of people that received services
aiming at economic production (Total = paid for
by NLR + facilitated by NLR)
B 52
For education support, we are supporting to promote inclusive education at all level to meet set target
of education for all. In Morang & Kailali projects out of 1149 (596 EDR & 553 FWDR) public schools 739
(380 EDR & 359 FWDR) have started to be transformed into inclusive schools. A total of 592 persons (47
DEO staff, 150 school management committee persons, 395 school head teachers) have been trained so
far on inclusive education. DEO reports from both piloting districts show that in both the districts around
5% of total school going age children are still out of schools in overall district and it comprises Dalit
(untouchable), marginalized groups & children with disabilities. Similarly, in Sunsari a total of 427 persons
(32 DEO staff, 30 school management committee persons, 365 school head teachers) have been trained
and all 365 public schools started to be transformed into inclusive schools. NLR, NFDN, DEO & Plan
Nepal has made the joint effort for these all achievements. We together with other partners also provide
individual support for really needy students and this year we provided such support to 42 persons with
leprosy and disability.
Apart from the two pilot districts, we also provide some technical & financial support through our
partners in other endemic districts also. Since, CBR is multi sector & multi dimensional strategy, although
overall achievement is tremendously high it is difficult to identify contribution of individual organization.
NLR role in this is that of facilitator to promote this concept. Here we have mentioned the achievements
depending on financial support of NLR. In the past fiscal year vocational training supports are provided to
84 places and IGP support to 55 groups so the numbers of individuals getting support aiming at economic
production is still higher than 96 persons that will be reported later by the partners.

Pg 7Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 7Annual RReportt
Other INDICATORS
Item: Information Details:
Number of health centre staff trained for leprosy 190 15 POID training & 175 BLT
Number of people under treatment for leprosy in
NLR supported areas
868 MB – 594 & PB – 274
Number of contacts of patients examined 2961 Including neighbours & relatives
Medical rehabilitation facilities established/
supported
69 centres POID centres supported
Number of people provided with orthopaedic
footwear
945 Protective footwear
Number of people provided with reconstructive
surgery
70 persons This year only
Number of people provided with prostheses 33 persons Through partners
Number of people provided with wheelchairs 62 Through partners
Number of people provided with vocational
training
86 groups Majorities of them are SCG
Number of people provided with microcredit’s/
loan
55 groups Groups to provide to individuals
Number of people financially supported for
education (primary school, high school or higher
education)
23 persons 21 children of leprosy affected
persons (by partners & others)
Cars/(motor)cycles bought 0
The national program has given high priority for contact examination. This includes the not only the
patients’families but also neighbours of index cases. The target given for health workers is surrounding
10 houses of index cases.
Achievement of prostheses seems quite low this is because of less service providing centres and also
the services are quite expensive. As mentioned earlier, rehabilitation requires multi sectoral cooperative
approach it is difficult to identify the percentage contribution of NLR. The lessons we learnt here are;
o Better results are achieved if the government system incorporates requirement of the people
o Advocacy & lobbying for the implementation of existing policies are important.

Pg 8 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 8 AAnnuall Report
2. Epidemiological situation
Our record shows that since the last eleven years (2002 to 2012) a total of 24229 new leprosy cases
detected in NLR supported regions. Out of detected new cases 2006 are children under 14 years, 1124
detected with DG II and 8550 are female. During this period 226 cases reported as relapsed, 25518
completed the prescribed treatment where as 593 defaulted from the treatment. The following table
shows the detail year wise statistics;
2002- 2009 2010 2011 2012 Total
New case 20650 1180 1185 1214 24229
Relapse 199 8 7 12 226
RFT 21864 1356 1150 1148 25518
Defaulter 452 12 22 7 593
Child 1762 93 72 79 2006
DG II 982 42 49 51 1124
Female 7326 453 384 387 8550
Table shows the fluctuating trend of relapse, defaulters, child and increasing trend of DG II cases over
the past three years. Number of RFT cases seems more than the new detected cases because treatment
restarted & transferred in cases are not included in this table. The major thing that we achieved during this
period is patient compliance and regularity, as we can see from the table that ignorable or few numbers
of cases are being defaulted from the treatment in recent years. This was possible when we started the
system of referring the detected cases to their own area for MDT.
The absolute number of new cases of leprosy are not decreasing, on the contrary slightly increasing
every year. Early diagnosis is promoted and very few cases are being reporting with grade II impairment
at the time of diagnosis. The main problem of leprosy is now reaction and disability management of the
new as well as old treated cases. The epidemiological trends over the last 11 years have been furnished
in the following diagrams;
2.1 Trend of annual new case detection rate (ANCDR)

Pg 9Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 9Annual RReportt
Figure shows decreasing trend in EDR & fluctuating trend in FWDR of new case detection rate over
the last eleven years. ANCDR was quite high in 2002 because leprosy elimination campaign – LEC was
conducted in high endemic Terai districts. It is gradually decreasing in following years but the value seems
still high that is 1.3 per 10000 populations in the year 2012. New cases are continually detected in the
communities and the rate is still higher in Terai districts. GON has given more emphasis on contact tracing
through index case approach for active case detection. According to this approach health workers &
community volunteers are instructed to identify the suspects in the families and 10 houses surrounding the
detected cases. In addition to this rapid surveys & skin camps are also being done in high endemic clusters.
2.2 Trend of MB proportion among new cases
Figure shows fluctuating trend of MB proportion among new cases over the past eleven years. In
2002, the year of LEC in leprosy endemic districts, more PB cases were detected so the MB proportion is
quite low. WHO criteria of classifying patients having either more than 5 skin patches and/or more than
one nerve involved and/or skin smear is positive as MB leprosy is followed in Nepal.
2.3 Trend of child proportion among new cases

Pg 10 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 10 AAnnuall Report
Figure shows fluctuating & decreasing trend of child (below 14 yrs of age) proportion among new
cases over the past eleven years. In 2003 this proportion seems quite high in EDR because of massive
school survey done in Saptari (one of the leprosy endemic) district. Child proportion is still high indicating
the recent transmission in those clusters. This might be one of the problematic areas where leprosy
control program in Nepal should focus more in future to interrupt the chain of leprosy transmission in high
endemic clusters.
2.4 Trend of DG II proportion among new cases
Figure shows the decreasing trend with some fluctuation of DG II proportion among new detected
cases over the past eleven years. No proper reporting system exists for the additional deformities from
all level but our finding from referral clinics, some of peripheral POID centres & PHC/HP shows that it is
less than 1% based on cohort report of the same cohort patients. There are some possibilities that when
the affected persons with anaesthetic hands and feet (DG I) stops coming to health centres can easily get
ulcers. If proper care for ulcer is not done there is possibility of further worsening of impairments. Hence,
there might be more persons in the communities with different impairments in covered in this data. New
attention need to be paid by LCP for the surveillance of leprosy affected persons even after RFT. From the
past year 2012 we have started to keep inventory of all affected persons from the low endemic districts,
until now records are updated in three of the districts.
2.5 Trend of female proportion among new cases

Pg 11Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 11Annual RReportt
Figure shows fluctuating trend of female proportion among new cases over the past eleven years.
It shows that around 32% of total leprosy affected persons are female. Gender discrimination & gender
violence still exists in Nepal. Leprosy is stigmatized disease (although the level of stigma is reducing).
Women with leprosy may have double discrimination; one being a women and the other women with
leprosy. Situation analysis of such issues need to be done and more focus need to be paid for gender
equity & social inclusion. LCP should incorporate women empowerment activities to ensure social dignity
& social justice of leprosy affected females.
2.6 Trend of treatment completion rate (TCR) for MB (Cohort report)
2.7 Trend of treatment completion rate (TCR) for PB (Cohort report)
Figures above show increasing trend of treatment completion rate among both MB and PB cases
over the past eleven years. It is obvious that patient compliances started to improve after MDT services
were made available at every VDC level after 2002. Here completion rate is calculated on the basis of
cohort reporting system.
Treatment completion rate of PB is almost 100% but we do not include those who were initially
classified as PB but changed to MB & transferred out as well so that this is only over 95% in past fiscal
year.

Pg 12 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 12 AAnnuall Report
3. Qualitative information
3.1 World Leprosy Day
Leprosy day, as initiated & started by Raul Folerau & his team at 1953, is celebrated on last Sunday
of January every year. For the celebration of 59th word leprosy day in Nepal (2012), LCD director formed
a team of GON & INGOs working in leprosy and visited all regions starting from eastern to far western
boarder of the country, attended the celebration functions and observed the rehabilitation models &
approaches practised by different organizations. It was expected that the findings will help to design a
common understanding of leprosy rehabilitation activities in Nepal. NLR was the part of the team. This
type of LWT exercise is not only for better coordination between the stakeholders but is also a good forum
on learning & correction of errors.
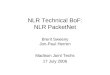
In addition to learning visits
different other activities were planned
and implemented in that week in
our regions for the celebration of
59th world leprosy day for example:
messages through e-media and print
media; interaction and coordination
meeting with DDC, DPHO, DEO,
WDO, DDC, DDMC & other CBR
organizations; orientation to various
groups on causes & consequences
of leprosy; articles & publications;
meeting with zonal hospitals to enhance ownership of RLRC; interaction with journalists; mass rally &
celebration by DPOs/SCG; celebration in RLRC (quiz contest among leprosy affected persons & drug
sellers; drawing (arts) competition among leprosy affected persons; fruits. t-shirts & blankets distribution
for admitted persons); new case detection activity by training and mobilizing of FCHV in leprosy endemic
areas.
3.2 Stigma reducing activities
Stigma against leprosy is associated with ulcers & other impairment rather than the disease itself.
Ignorance & negligence of ulcers & impairment by affected persons can cause the secondary problems
such as bad smell, looking ugly, pus, etc that is very difficult to tolerate by others. So the first preferences
is to teach the affected persons on self care activities for proper management of own impairments from

Pg 13Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 13Annual RReportt
getting further worsening. If such activities are done in a group peers get mutual help & encouragement
from each other. If these are only leprosy specific groups they will not get any more support from remaining
part of community peoples and again it is easy to be pointed out as “Leprosy affected” gatherings. If other
persons having the more or less same problems but causes may be different, such as persons with
disabilities due to other causes, diabetics, neuropathy etc also join the groups a pronounce part of the
communities are covered. Now such mixed groups owned by DPOs can work together to improve their
self-reliance and dignity. Second part is the environmental barriers & attitude of the community peoples
towards leprosy affected persons. They need to be oriented on causes, consequences, transmissions,
impairment treatment and cure about leprosy.
Following are the some of the major activities we did for stigma reduction at
community level:
• Community awareness activities by direct talks and discussions
• Messages through electronic & print media preferably in local languages
• Formation of mixed self care & self help (DPO) groups
• Community level activities enhancing more community ownership on the program
• Mainstreaming of leprosy related disabilities to general disabilities
• Comprehensive PIOD activities through POID centers
• Promotion of inclusive education to transform the existing societies to
inclusive societies
Case story of Aasha Kumari Choudhary (30 years old female)
Aasha Kumari Choudhary, a leprosy affected girl, is an inhabitant of Hariharpur
VDC of Saptari district who belongs to a very poor family. Her father is also a
leprosy-affected person. Four brothers of her father are living separately. At the
beginning her father did know about the disease, due to tingling sensation of his
hand and feet he has taken other medicines from district hospital. There was no
any improvement of that tingling sensation. Once when he was ploughing the
field, hard root of maize plant penetrated his feet making a wound but he was
unknown, even then he didn’t go anywhere for treatment.

Pg 14 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 14 AAnnuall Report
Aasha says that, she was 10 years old when she got leprosy. She felt tingling sensation in her hands
& feet and couldn’t walk around. Her feet were swollen. Her father took her to nearby treatment centre for
check up. It was not cured for long times so she was referred to a doctor in district headquarter of Saptari,
but again no any improvement was noticed, rather worsened. Her mother was taking care of her.
One-day a documentary film was shown in her village to aware community people about sign &
symptoms of leprosy & its consequences. When this was done her father and other neighbours suspected
her leprosy. She and her farther, after check up, were diagnosed leprosy. After listening that he got
leprosy, her father was so frightened that he could not speak any anything anymore just kept staring. Her
mother started crying, hardly distressed, that worsened her condition and became mental illness.
After knowing that she got leprosy she was worrying how to meet & talk with her friends and afraid
of her relatives if they visited to her house. She was feeling that her thinking capacity was abandoned.
Leprosy worker suggested her father to get MDT from nearby health post but denied because of fear that
other people could know about his disease. Her father was having a fear of exclusion from the society and
exclusion from the feast during festivals & celebrations.
Later on Aasha & her family came to know that not only them but other people in their communities
are also affected and taking medicine from health post, hence, they started MDT for 24 months. On getting
MDT from health post she wanted to accompany her aunt’s children but due to the fear of transmission
her aunt didn’t allow and further stopped her children to meet Aasha & her farther. Aasha was unable to
do any work, her mother was already disturbed & stopped working there was only her farther to look after
the household & other works. Her aunt used to call her as “leper” and due to fear of disease others didn’t
come near to her. Her survival was at stake.
After some time self care group & activities were started in her village. She joined the groups. SCG
with the assistance from local health worker she was referred to tertiary level referral centre for correction
of her impairments. She stayed there for 6 months & surgical operation was done. She also learnt about
taking care of her hands & feet. She was sent to that hospital the second time for correction of her hand
and stayed there 6 months more.
She was an adolescent now and people started on talking about her marriage but for a leprosy-
affected girl it was not easy. Her elder sister managed a boy for her & proposed for marriage. She was
thinking that, being leprosy affected girl there would be some problem later on in their relationship of
conjugal life so she didn’t accept to marry him. Her sister further insisted but her father suggested that
it was up to her so that she denied even she was interested. She said that her family condition was such
poor that she wanted to leave it & go somewhere. But, she didn’t know where to go, with hand operated

Pg 15Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 15Annual RReportt
twice and the problem in the feet resulting impossible to walk a long distance. Later some improvement
was seen in her hand & feet.
In 2010, during the reformation of self care group in her village, she & her father became the members
of that group. She is already trained and learnt about self-care activities from referral centres but now
joined the group to accompany her father. But, her father being the only her father for their household
activities didn’t have sufficient time for such activities she said. After her repeated pursuance, he started
soaking his feet for brief before going to work and during night he was over tired of work & went to bed
after meal, that is why her father’s wound recurs frequently.
Nowadays, she and her father are the active members of that self-care group in their village. They
are regularly attending the group meetings and assisting other members about such activities. Aasha is
now the member of micro credit and saving scheme and has started saving. Because of problem in her
feet, she can’t walk a long distance but feel comfortable to a short distance. She can go to nearby grocery
to buy and can help her father on cooking. Now she attends the wedding and other ceremonies in the
villages which she could not do before. Her aunt & others do not use discriminatory word to call her and
started to visit her family. She says, nowadays our neighbours’ attitude towards our family has been
changed as they know leprosy is curable, I am happy with this.
Due to poverty her father is compelled to do different household works even he needs the rest. That
is the reason why his wound is not healed. She said why this disease is common mainly for poor? They
are not facing with hand to mouth problems but also the burden due to disease!

Pg 16 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 16 AAnnuall Report
4. Research & study – Self care group assessment
NLR Nepal is being involved on different types of studies including international multi country
researches. In 2010, after getting approval from Nepal health research council (NHRC) we have started
a study that entitled “Assessment of self care group activities among persons with leprosy related
disabilities”. In this study the impact of self-care activities of persons who are participating in self care
groups (SCG) and those who are not involved in SCGs of leprosy-related disability will be compared. Not
only the impairment, but together with restrictions in participation, activity limitation influenced by stigma
cause disability. Since the several self care groups are well functioning in the field, clarity of what should
be measured as the impact of being a member of a SCG is needed. In this study, medically the level of
foot and ulcer will be assessed and socially self stigma and participation in the wider community is being
looked at.
The present study is being conducted in Eastern Region of Nepal in Morang (4 groups), Sunsari (2
groups) and Saptari (2 groups). 60 SCG members and 60 none-SCG members with disabilities due to leprosy
will be included, of which 60 non-SCG members will be assessed from Jhapa, Sunsari, Saptari & Siraha.
These 120 persons will complete the Feet assessment questionnaire, Wound assessment questionnaire,
The Participation scale (The P-scale) and the Explanatory Model Interview Catalogue (EMIC). The main
focus of the study is on providing evidence on impact of self care activities through self care groups in
order to give information to design and support appropriate interventions. In addition, what determinants
of disability are influencing participation restriction will also be looked into. First year data collection of
this study has been completed so far and we are about to complete the collection of data for 24-month,
the final month of this study.

Pg 17Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 17Annual RReportt
Some other major studies done through NLR in Nepal until now are as follows;
SN TitleDate &
duration
Principal
Investigator
1Assessment of Self-Care group activities: Among
persons with leprosy related disabilities2010-2013 Nandlal Banstola
2The impact of disability of a family member on the rest
of the family in the Eastern region of Nepal2011 Nandlal Banstola
3
Leprosy related disability and the association with
secondary mental health problems in the Eastern
region of Nepal
2011 Dr. K. P. Dhakal
4Further validation & reliability testing of the participation
scale2010 Nandlal Banstola
5 Rapid disability appraisal (disability survey) in Morang 2009 Nandlal Banstola
6 Quality of life of people with seeing related disabilities 2008
7 Quality of life of persons with dishabilles due to leprosy 2008
8 COMLEP 2006/2007
9 Accessibility of physiotherapy for leprosy patients 2006
10Community health education followed by impact
evaluation (KAP survey)2005
11 Quality of leprosy services from clients’ perspective
15 January to
06 February,
2004
12Feasibility study for implementation of M. leprae lateral
flow test2004/2005
13Effectiveness of prednisolone treatment of leprae
reactions and neuritis (retrospective study)2001
14 Impact of NLEC in public awareness about leprosy 1999

Pg 18 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 18 AAnnuall Report
5. Financial analysis
The following diagram shows some financial status of NLR support in Eastern Nepal;
Figure shows that out of total planned budget 89% has been allocated to leprosy control program
including rehabilitation where as 11% was allocated to rehabilitation pilot projects (general rehabilitation).
Out of total allocated budget 94% expenditure made on leprosy, 96% for rehabilitation where as total
expenditure of 2012 is 94% of total allocated budget.
Figure shows that out of total budget allocated 12% was admin budget & 88% was program budget
(this program & project budget has been defined on NLR RBM system). 88% expenditure is made out of
allocated program budget and 94% expenditure is made out of total allocated admin budget. According

Pg 19Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 19Annual RReportt
to NLR RBM system overall budget is divided into program & project budget differentiating CRO and field
projects. So that admin budget here includes cost for admin staff, house rent and other managerial costs.
Figure above shows the GON & NGO wise expenditure of program budget supported by NLR.
Expenditure made by NGOs seems quite higher because of CBR budget including piloting districts that
goes through NGO partners. GON and especially health program has recently started some initiations on
incorporating CBR but still lacking adequate structures.

Pg 20 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 20 AAnnuall Report
Figure shows the higher percentage of expenditure in Morang and Kailali because of rehabilitation
pilot project support for general as well as leprosy related disabilities. This pilot project is being phased
out by mid July 2013.
Figure shows higher percentage of expenditure made by NFDN in EDR as it includes other member
organizations at different districts. Expenditure made by NLR is still 16% in EDR & 81% in FWDR this is
because of hospital cost of regional leprosy referral clinic in Biratnagar & Dhangadhi. These clinics are
planned to handing over to Zonal hospitals existing in the regions within this project period. The process
has already been started but it still takes few more years.

Pg 21Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 21Annual RReportt
6. Some initiatives for local funding
NLR in Nepal, started to look for program funds out of its own. During the year 2012, we tried to
explore for available resources. Some examples of initiatives which we started:
1. This year, like last year also, we were able to include our agenda Plan Nepal’s annual PoA and
implemented together. eg training of teachers for inclusive education etc in ELCP area.
2. Now the government program has started to spend on patients’ travel cost for referrals, some
protective devices etc which previously we used to pay.
3. In Far West region, we were able to raise small fund from local business community for distribution
of tricycles to 12 needy persons with disabilities including persons affected by leprosy.
4. Discussion with local KOICA office is going on to work in partnership in five VDCs of Kailali
5. Dialogue with a local airline company is also continuing for their support in our work
6. NLR Nepal together with HQ prepared and submitted a number of funding proposals to different
donors but not yet succeeded eg: Post code lottery, Sight Savers and Firah.
7. We are still planning to write one or two proposals this year.

Pg 22 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 22 AAnnuall Report
7. Conclusion and recommendations
NLR is providing financial & technical support on two projects; leprosy control & rehabilitation of
persons with disabilities (PWD) in Eastern and Far western regions of Nepal. For rehabilitation, special
piloting is being done in Morang and Kailali districts. Budget for the disease control goes through GON
Redbook where as rehabilitation support goes through the NGO partners as mentioned in NLR project
agreement with the government. Programs as well as financial expenditure achievements of past fiscal
year are quite encouraging to meet the indicators as mentioned in NLR planning through LFA for this
project period 2011 – 2015. Besides this following are the major recommendations made to make this
project period grand success;
• • GON need to initiate taking over the ownership of regional level leprosy referral clinic by KZH &
SZH that is located within its premises
• NFDN and its network organizations should play the major role to enhance better coordination &
cooperation with related government line agencies and ministries
• Disability is developmental issue, it is social problem rather than the individual one and hence GON
agencies need to consider this as a high priority concern & plan accordingly
• Lot of progresses has been made on mainstreaming of leprosy related disabilities to general disabilities.
PWDL are getting absolute opportunities to entertain entitled GON provisions & facilities but still they
are passive receiver rather than the active community contributors. NFDN and others still need to
pay high priority for the capacity building & empowerment of PWDL ensuring their leading or decision
making roles.
• More activities are still needed to change the charity mind set of related stakeholders on both disease
control & disability management issues
• Strong monitoring mechanisms at national & sub national level needed to be established for the
proper implementation of already existing policies & strategies such as MDG, UNCRPD, CRS etc

Pg 23Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 23Annual RReportt

Pg 24 Annual Report
A REPORT CONTRIBUTING TO THE BETTER UNDERSTANDING OF NLR SUPPORTED PROGRAM ACTIVITIES IN NEPAL YEAR 2012
Pg 24 AAnnuall Report