Embed Size (px)
Citation preview

Annandale Public Schools
October 1, 2018 PEIP Health Insurance Plan Proposal
August 9, 2018
Mark Beltz (651) 480-1501

~RCE TR~ININGJ MONTHlY PREMIUM
DISTRICT MONTHlY PREMIUM
ANNANDALE HEALTH INSURANCE 2018-19
® MONTHlY PREMIUM
DISTRICT MONTHLY PREMIUM
(j)

Section Ill - PEIP Rates for Annandale Public Schools
This proposal includes rates for:
Health Coverage-
Dental Coverage-
Life Coverage-
PEIP's Advantage Plans
Delta Dental Preventive and Comprehensive Plan
Basic Life/AD&D, plus optional Supplemental Life and Dependent Life through Minnesota Life
Effective Date of Coverage:
¥-* Renewal/ Anniversary Date:
Number of Covered Individuals in Your Group:
15 months
Qn'uary1,~
160
,.A- Participation in PEIP will be for a two year term, with an annual rate renewal.
Premium Rating- Initial rates are based on the groups demographic and claims experience provided to the underwriters. Rates are effective October 1, 2018, and guaranteed for 15 months with the renewal on January 1, 2020. At renewal on 1/1/2020, renewal rates will be based on the group's premium tier and total claims of the PEIP pool; not based on the individual group's claims. Each group will remain in their rate tier with renewal rates guaranteed for 12 months at a time.
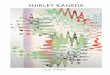
A historical illustration of the success of the PEIP pool renewals is shown below.
7/16/2018
History of PEIP Pool Renewals
July Group Average January Group Average
July, 2010 = +8.0%
July, 2011 =- 6.6%
July, 2012 =- 3.3% January, 2013 = +5.0%
July, 2013 = +6.0% January, 2014 = + .5%
July, 2014 = +1.9%
July, 2015 = +2.0%
July, 2016 = +5.9%
July, 2017 = +1.3% July, 2018 = +3.9%
January, 2015 = +2.4%
January, 2016 = +5.5%
January, 2017 = +3.5% January, 2018 = + .3%
Combined Pool Average = 2.4% *History includes all ACA taxes
P EIP pool average pool increase is
2.4% over the last 15 renewals.
Page 9

~ Step by Step Instructions for Enrollment in the Public Employees Insurance Program Advantage Plan
.. 13l,~\ <-.7·. ~\ '\
M=ta Employees Insumnce Program
To help explain your options in the Public Employees Insurance Program, we have created the following guide.
'-P<> Step 1- Choose Your Plan Level ~
The Public Employees Insurance Program Advantage Plan has cost sharing features that will help you and your employer to better control health care costs while maintaining flexibility in access to doctors and clinics. The Public Employees Insurance Program offers three Plan choices:
(!;J • Advantage (High) a I II I I ) • HSA (Low)
Choose the Benefit Level that best fits your needs. The premium and cost sharing will vary based on the Benefit Level you choose. You may change your Benefit level each year during your group's annual open enrollment.
'-P<> Step 2- Choose Your Health Plan/Network ~
The Public Employees Insurance Program offers three different Health Plans/Networks to choose from:
@ •IL , 2l _ • • Blue Cross Blue Shield
. Choose the network carrier that best fits your needs. Your network selection will not affect the cost of the plan; nor will it affect the premium rate. The benefits are similar under each network (HP includes a benefit for treatment of infertility). You may change your Health Plan/Network level each year during your group's annual renewal.
I @
'-P<> Step 3- Choose Your Primary Care Clinic ~
Primary Care Clinics have been placed into one of four cost levels, depending on the care system in which the provider participates and that care system's total cost/quality of delivering health care. The amount of cost sharing that is paid for health care services varies depending upon the cost level of the Health Plan and Network that you choose.
~ • Select a primary care clinic (PCC) for each family member
Each family member must select a primary care clinic (PCC). Family members may choose different PCCs- even in a different cost level, but all family members must enroll with the same Plan level and Network choice. Your enrollment form should include the primary care clinic# associated with your network carrier.
-1111 primary care clinics are broken into four tier levels that determine the benefits received by that family member. A
s~ of participa~i~g cli~i~s is available online t? he.lp y?u make your primary care clinic sel~c~ion. This_list includes your pnmary care chntc's chntc number that you w1ll need m order to enroll. You can change: chmcs by calling the phone number on your ID card (changes are effective on the 1st day of the following mOnth)'.;(:: .
Most medical care is coordinated through a Primary Care Clinic (PCC) and yo1:1 will gener:ally need a referral to see a specialist (referrals to a specialist's office will be covered at the same cost level as yourBCC). You may self-refer to certain specialists including OBGYN, chiropractors, and mental health/chemica1 dependency practitioners, providing the practitioner is part of the carrier's self-referral network. No referrals needed'for:·ur.gent care and emergencies. ~ . . A statewide primary care clinic listing and health plan documents, including the-Summaryls-eneflt Comparisons (SBC's) for all plan levels, are available online at www.innovomn.com/plan~information.htrmi'' · . .-/·: >:• '>.
IMPORTANT! Once enrolled, you will receive TWO ID cards. One card will be sentfro.m your health plan (HP, BCBS, POne) which is to be used for medical services. The second card from CVS is to be used .for all pharmacy charges. If you have questions please call us at 952.746.3101 or 800.829.5601 or email us [email protected],
8/17

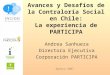
€)i 'd;;;;;;: iie~i~/,;i:;,OiiJ)C;;,;~~ihi~ 2iii8~ioi 9B:n~fits Schedule -Benefit Provision
...__..... Cost Level1- You Pay Cost Level2- You Pay Cost Levell- You Pay Cost Level4- You Pay
A. Preventive Care Services
tfsA- p l~V\ ® • Routine medical exams, cancer screening • Child health preventive services, routine • immunizations Nothing Nothing Nothing Nothing • Prenatal and postnatal care and exams • Adult immunizations • Routine eye and hearing exams B. Annual First Dollar Deductible $1,500 v $2,000
""" $3,000 $4,000
Combined Medical/Pharmacy (single coverage)
Combined Medical/Pharmacy (family coverage) $2,600 per family member $3,200 per family member $4,800 per family member $6,400 per family member $3,000 perfamily $4,000 perfamily j $6,000 per family $8,000 per family
C. Office visits for Illness/Injury, for Outpatient ~ _./ Physical, Occupational or Speech Therapy, and Urgent Care
$40 capay per visit $50 capay per visit $1 00 capay per visit $120 capay per visit • Outpatient visits in a physician's office • Chiropractic services annual deductible applies annual deductible applies annual deductible applies annual deductible applies • Outpatient mental health and chemical
dependency • Urgent Care clinic visits (in or out of network) D. In-Network Convenience Clinics and online $0copay $0 capay $0 capay $0 capay
care annual deductible applies annual deductible applies annual deductible applies annual deductible applies E. Emergency Care (in or out of network) $150 capay $150 capay $150 capay 50% coinsurance • Emergency care received in a hospital annual deductible applies annual deductible applies annual deductible applies annual deductible applies
emergency room F .Inpatient Hospital Co pay $400 capay $650 capay $1 ,500 co pay 50% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies G. Outpatient Surgery Copay $250 capay $400 capay $800 capay 50% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies H. Hospice and Skilled Nursing Facility Nothing after Nothing after Nothing after Nothing after
annual deductible annual deductible annual deductible annual deductible
I. Prosthetics and Durable Medical Equipment 20% coinsurance 25% coinsurance 30% coinsurance 50% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies J. Lab (including allergy shots), Pathology,
and X-ray (not included as part of preventive 20% coinsurance 25% coinsurance 30% coinsurance 50% coinsurance care and not subject to office visit or facility annual deductible applies annual deductible applies annual deductible applies annual deductible applies copayments)
K. MRI/CT Scans 20% coinsurance 25% coinsurance 30% coinsurance 50% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies L. Other expenses not covered in A- K
above, including but not limited to: • Ambulance • Home Health Care • Outpatient Hospital Services (non-surgical) 20% coinsurance 25% coinsurance 30% coinsurance 50% coinsurance
• Radiation/chemotherapy annual deductible applies annual deductible applies annual deductible applies annual deductible applies • Dialysis • Day treatment for mental health and
chemical dependency • Other diagnostic or treatment related
outpatient services M. Prescription Drugs $25 tier one $25 tier one $25 tier one $25 tier one
30-day supply of Tier 1, Tier 2, or Tier 3 $40 tier two $40 tier two $40 tier two $40 tier two prescription drugs, including insulin; or a $65 tier three $65 tier three $65 tier three $65 tier three 3-cycle supply of oral contraceptives. annual deductible applies :1 annual deductible applies annual deductible applies annual deductible applies
N. Plan Maximum Out-of-Pocket Expense•• $3,000 /$3,000~ $4,000 $5,000
(including prescription drugs) Single Coverage
Family Coverage $5,000 per family member $5,000 per family member J $6,850 per family member $6,850 per family member .. $6,000 per family $6,000 per family _..; $8,000 per family $10,000 per family "' ~ -· ---- -- ··----"- -- -"- L.---~"-'- --- -·· --- ----- - "- -- -- _.. __ ---~ _z .. ,__ -•- 1- -- -~- ~- ~'- - ·- L:. ·_:t. ·- --··- ...1 - ...1---~1..-..1 !- ---.<!---,.. -·-...1 ,- -1--.. -

(0) Minnesota Public Employees Insurance Program (PEIP) t-r~® ·---. -------n- ---------- ----- ---n-- -.------ -~-~ ---- ----- --~ ~----------
Benefit Provision Cost Level1 - You Pay Cost Level2- You Pay Cost Levell- You Pay Cost Level4- You Pay
A. Preventive Care Services • Routine medical exams, cancer screening • Child health preventive services, routine
immunizations Nothing Nothing Nothing Nothing • Prenatal and postnatal care and exams • Adult immunizations • Routine eye and hearing exams ~ B. Annual First Dollar Deductible
$150/300 ( $250/say $550/1,100 $1,250/2,500 (single/family)
C. Office visits for Illness/Injury, for Outpatient '--""" Physical, Occupational or Speech Therapy, and Urgent Care
$25 capay per visit $30 capay per visit $60 capay per visit $80 capay per visit • Outpatient visits in a physician's office • Chiropractic services annual deductible applies annual deductible applies annual deductible applies annual deductible applies • Outpatient mental health and chemical
dependency • Urgent Care clinic visits (in or out of network) D. In-network Convenience Clinics and online
$0 capay $0 capay $0 capay $0 capay care
E. Emergency Care (in or out of network) $100 capay $100 capay $100 capay 25% coinsurance • Emergency care received in a hospital
annual deductible applies annual deductible applies annual deductible applies annual deductible applies emergency room F.lnpatient Hospital Copay $100 capay $200 capay $500 capay 25% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies G. Outpatient Surgery Copay $60 capay $120 capay $250 capay 25% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies H. Hospice and Skilled Nursing Facility Nothing Nothing Nothing Nothing I. Prosthetics and Durable Medical
20% coinsurance 20% coinsurance 20% coinsurance 25% coinsurance
Equipment annual deductible applies J. Lab (including allergy shots), Pathology,
and X-ray (not included as part of preventive 5% coinsurance 5% coinsurance 20% coinsurance 25% coinsurance care and not subject to office visit or facility annual deductible applies annual deductible applies annual deductible applies annual deductible applies copayments)
K. MRIICT Scans 5% coinsurance 10% coinsurance 20% coinsurance 25% coinsurance annual deductible applies annual deductible applies annual deductible applies annual deductible applies
L. Other expenses not covered in A- K above, including but not limited to:
• Ambulance • Home Health Care • Outpatient Hospital Services (non-surgical) 5% coinsurance 5% coinsurance 20% coinsurance 25% coinsurance
• Radiation/chemotherapy annual deductible applies annual deductible applies annual deductible applies annual deductible applies • Dialysis
• Day treatment for mental health and chemical dependency
• Other diagnostic or treatment related outpatient services
M. Prescription Drugs $14 tier one 11"'""'~ Ill. Lft. $14 tier one $14 tier one
30-day supply of Tier 1, Tier 2, or Tier 3 prescription drugs, including insulin, or a
$25 tier two $25 tier two -4' $25 tier two $25 tier two .I $50tierthree l)l• ..,,
3-cycle supply of oral contraceptives $50 tier three $50 tier three $50 tier three
N. Plan Maximum Out-of-Pocket Expense for
"'~800/1,600 Prescription Drugs (excludes PKU, Infertility, $80011,600 $800/1,600 $800/1,600 growth hormones) (single/family)
0. Plan Maximum Out-of-Pocket Expense $1,200/2,400 r~ _0,1,200/2,400 $1,600/3,200 $2,600/5,200
(excluding prescription drugs) (single/family) -·--- -· ----
Emergency care or urgent care at a hospital emergency room or urgent care center out of the plan's service area or out of network is covered as described in sections C and E above.
This chart applies only to in-network coverage. Point of Service coverage is available only for members whose permanent residence is outside the State of Minnesota and outside the service areas of the health plans participating in Advantage. This category includes employees temporarily residing outside Minnesota on temporary assignment or paid leave flncluding sabbatical/eaves] and college students. It is a/so available to all dependent children and spouses permanently residing outside the service area. T11ese members pay a $350 single or $700 family deductible (separate and distinct from the deductibles listed in section B above) and 30% coinsurance to the out-of-pocket maximums described in section 0 above. Members pay the drug copayment described at section M above to the out-of-pocket maximum described at section N.
A standard set of benefits is offered in all PEIP Advantage Plans. There are still some differences from plan to plan in the way that benefits, including the transplant benefits, are administered, in the referral and diagnosis coding patterns of primary care clinics, and in the definition of Allowed Amount.
l'EIP.Idnmtuge 2
i I

®
-
(
>r
Minnesota Public Employees Insurance Program (PEIP Advantage Health Plan 2017-2018 Benefits Schedule
o~~+ .D·. ~· .. 1 6) fVe~~~ L SSJ~) btf co;;
- ~--
- ·' - - - - -- --- J
2017 ·2018 Benefit Provision Advantage High Advantage Value Advantage HSA
A. Preventive Care Services • Routine medical exams, cancer screening • Child health preventive services, routine 30% coinsurance 30% coinsurance 30% coinsurance
immunizations annual deductible applies annual deductible applies annual deductible applies
• Prenatal and postnatal care and exams • Adult immunizations • Routine eye and hearing exams
B. Annual First Dollar Deductible $3501$700 $3501$700 $1,5001$3.000
(single/family) C. Office visits for Illness/Injury, for Outpatient Physical,
Occupational or Speech Therapy, and Urgent Care within the service area 30% coinsurance 30% coinsurance 30% coinsurance
• Outpatient visits in a physician's office annual deductible applies annual deductible applies annual deductible applies
• Chiropractic services (except urgent care which is paid (except urgent care which is
• Outpatient mental health and chemical dependency at in-network levels) paid at in-network levels
• Urgent Care clinic visits (in or out of network) D. Convenience Clinics 30% coinsurance 30% coinsurance 30% coinsurance
annual deductible applies annual deductible applies annual deductible applies E. Emergency Care (in or out of network) Covered at in-network levels Covered at in-network levels Covered at in-network levels • Emergency care received in a hospital emergency room F.lnpatient Hospital Capay 30% coinsurance 30"/o coinsurance 30% coinsurance
I annual deductible applies annual deductible applies annual deductible applies
G. Outpatient Surgery Capay 30% coinsurance 30% coinsurance 30% coinsurance annual deductible applies annual deductible applies annual deductible applies
H. Hospice and Skilled Nursing Facility 30% coinsurance 30% coinsurance 30% coinsurance annual deductible applies annual deductible applies annual deductible applies
I. Prosthetics and Durable Medical Equipment 30% coinsurance 30% coinsurance 30% coinsurance
annual deductible applies annual deductible applies annual deductible applies
J. Lab (including allergy shots), Pathology, and X-ray (not 30% coinsurance 30% coinsurance 30% coinsurance
included as part of preventive care and not subject to office annual deductible applies annual deductible applies annual deductible applies
visit or facility copayments) K. MRI/CT Scans 30% coinsurance 30% coinsurance 30% coinsurance
annual deductible applies annual deductible applies annual deductible applies L. Other expenses not covered in A- K above, including but
not limited to: • Ambulance • Home Health Care
30% coinsurance 30% coinsurance 30% coinsurance • Outpatient Hospital Services (non-surgical) • Radiation/chemotherapy annual deductible applies annual deductible applies annual deductible applies • Dialysis • Day treatment for mental health and chemical
dependency • Other diaQnostic or treatment related outpatient services
M. Prescription Drugs $14 tier one $20 tier one
$25 tier one 30-day supply of Tier 1, Tier 2, or Tier 3
$25 tier two $40 tier two $40 tier two
prescription drugs, including insulin; or a $50 tier three $65 tier three
$65 tier three 3-cycle supply of oral contraceptives. Annual deductible applies
N. Plan Maximum Out-of-Pocket Expense for Prescription Drugs (excludes PKU, Infertility, $8001$1,600 $1,0001$2,000 n!a growth hormones) (single/family)
0. Plan Maximum Out-of-Pocket Expense $3,000 single (costlevel1, 2) (excluding prescription drugs) (single/family)
$1,2001$2,400 (cost /eve/1, 2) $2,2001$4,400 (cost level1, 2) $4,000 single (cost level3) $5,000 single (cost level4)
$1,6001$3,200 (cost /eve13) $3,2001$6,400 (cost level3) $6,000 family* (cost level1,2)
$2,6001$5,200 (cost level4) $4,2001$8,400 (cost level4) $8,000 family* (cost level3)
$10,000 family* (costlevel4)
·e

1"\ ,. -
10
-se~~cY tsx cr:tr J, I IPrimaryCare
County I City ST Clinic Number
BG Steams Alba~y MN 10022195
·ac Wright Albertville. MN IB061248
BC Wright Annandale MN IA262190
I'BC Sherburne Becker MN IC412206
BC Steams E!e!grade MN IC412B93
BC Sherburne Big Lake MN. IC412683
BC Steams Bropten MN IG072742
.QC. Wright BUffa.Jo MN. IA262155
I
Primary Care Clinic NumberEff311/18 !Clinic
oo33St476 I CerltraCare Cli~ic • Aibariy
oo321t034 I . . Stellis Health • Albertville-St. Michael
003208466 Ail ina Health Annandale Clinic
003217448 CentraCare Clinic • Becker
003204254 CentraCare Health Paynesville • Belgrade Clinic
003214310 CentraCare Clinic • Big Lake.
003216733 Bf!)Oten Medical Center.
003209592 Allina.H~Jith IMfalo COnic .
Address
320 Third Ave.
11091 Jason Ave: NE
440Eim St. E.
12800 Rolling Ridge Rd.
505 Nelson Ave.
16830 1981h AveNW
111 PleasantAve. N.
303 Calli~ St.
BC · 003542985 Allina.Healtll Clinic; Buffalo,crossroads 755. Crossi'O!IC[s Campus Drive
ec Wright Buffal9. IMN IB061248 003211034 Stellis ~alth • Buffalo Clinic 1700 Hwy. 25 N.
~c earver Chanhassen IMN IA262239 003196963 .. Al.!ina Health Charlhasstm .Clinic 7770 Dell Road, #1 tO
~1~C ~Ca~er •. .• !Chanhassen · IMN jp181366 003200844 Parj( N~llet Clinic. Ch.anh~en 300 Lake Drive East
BC· Carver Chanh~eit I MN IR352542 003208662 Ri~geview Ch~n~assen Clinic 7907 Powers Blvd.
8(; Caiver C::has~~ !M~ IA262489 00321Q387 Allin~ Healt!t Chaska Clinic 111 Hundertmark Road, #220
BC Caiver Chaska IMN IL051392 003209895 Lakt~viJw Clinic· ~haska 1'\0105PiorieerTrait Sie 100
BC Carver Chaska. IMN IR352542 003208662 Ridgeview Chi!Ska. "Ciin,ic 1 11 Hundertma.rk Road, 115N
BC Carver Chaska IMN IS731078 003200424 South Lake Pedi~r.ic;s • Chaska HtHundertmarkRd., #210
BC Carver Chaska IMN IV071086 003200963 Valley Family Pr'a&ttc• 822 Yellow.Brick Rd
BC Carver Chaska IMN IW242009 003200853. Wayzata Children's Clinic • Chaska 11 t Hundertmark Rd., #420
BC Wright Clearwater IMN IC412843 003642456 Clearwater Medical Clinic 615 Nelson Dr.
BC Wright Cokato IMN IA262147 003195248 Allina Health Cokato Clinic 110 Olsen Blvd.
e .. o.,. ~-~ e:!! ;t.·~ II C.. UJ!. ~a:
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
PCC
f1CC
PCC
PO
PCC
PO
PCC
PCC
Care System
CEN
WRS
ALL
CEN
PAY
CEN
ICM
ALL
ALL
WRS
ALL
PKN
IM'I
AL,L
LAK
IMT
PED
IMT
PED
STC
ALL
Finai2J;1}, Costle;~ denotes clinic moved to 2 for
2017 Cost Ieveii access)
~"'ifC4 '"
3 3
2
3
2*
3
2
2
2
2
2
3
2
2
3
2
3
2
2
2
1
2
3
3
3
2
2
2
1
2
1
2
2
2
2
2
2
2
2
2
December 4'2017

{'1" ' i!f Fin~ ca
u., ~.g Cost Level (* lh;; denotes clinic ·c ·-
Primary Care Primary Care Clinic 9.-l Care moved to 2 for ID County City ST Clinic Number Number Eff 3/1/18 Clinic Address
U II System 2017 Cost level access) ~It
BC Stearns Cold Spring MN C412693 003204257 CentraCare Health Paynesville • Cold Spring Clinic 308 5th Ave. S., #100 PCC PAY 2* 3
BC Steams ColdSpring MN C412845 003638585 Cold Spring Medical Clinic 402 N. Red River Ave., #2 PCC STC 2 2
BC Steams Cold Spring MN N042574 003200086 Wenner, Christopher J. MD, PA 218 Main Street PCC ICM 2 3
.BC Steams Collegeville MN C412847 003643510 CentraCare Quick Care 2850 Abbey Plaza, #109 PCC CEN 3 3
BC Wright Delano MN R352542 003208662 Ridgeview Delano Clinic 916 St. Peter Ave. PCC IMT 3 2
BC Wright Delano MN W242009 003200853 Wayzata Children's Clinic • Delano 916 St. Peter Ave., #120 PD CHI 2 2 ~
BC Sherburne Elk River MN A262271 003196091 Allina Health Elk River Clinic 14181 Business Center Dr. NW PCC ALL 2 2
BC Sherburne Elk River MN F262627 003198715 Fairview Clinics • Elk River 290 Main St. N.W., #100 PCC FAI 2 3
BC Sherburne Elk River MN N322309 003217675 North Memorial Health Clinic • Elk River 800 Freeport Avenue NW, #100 PCC NOR 2 2
BC Howard Lake 2 I Wright MN R352542 003208662 Ridgeview Howard Lake Clinic 900 6th St. #G PCC IMT 3 I
I
BC Steams Melrose MN C412553 003208713 CentraCare Clinic • Melrose 525 W. Main St. PCC CEN 3 3
BC Wright Monticello MN C412675 003209184 CentraCare Health • Monticello Medical Group 1107 Hart Blvd. PCC CEN 3 3
BC Wright Monticello MN B061248 003211034 Stellis Health • Monticello Clinic 1001 Hart Blvd., #100 PCC WRS 1 1
.Norwood BC Carver Young America MN L051392 003209895 Lakeview Clinic West· Norwood 406 Faxon Road PCC LAK 2 2
BC Steams Paynesville MN C412693 003204253 CentraCare Health Paynesville • Paynesville Clinic 200W.1st. St. PCC PAY 2* 3 I
BC Stearns Richmond MN C412693 003204255 CentraCare Health Paynesville • Richmond Clinic 130 First St. NE PCC PAY 2* 3 .
BC Stearns Sartell MN N042623 003216221 Sartell Pediatrics 111 Second St. South PD PED 2 2
BC Stearns Sartell MN W232322 003204919 Williams lntegracare Clinic 100 South 2nd St. PCC ICM 2 3 •
BC Stearns SaukCentre MN C412673 003206481 CentraCare Health System· Sauk Centre Clinic 425 Elm St. North PCC CEN 2* 3
BC Stearns St,·Cioud MN C412206 003217448 CentraCare Clinic • Health Plaza Family Medicine 1900 CentraCare Circle PCC CEN 3 3 CentraCare Clinic • Health Plaza Obstetrics &
BC Stearns St. Cloud MN C412042 003209689 Women's Health 1900 CentraCare Circle, #2300 PCC CEN 3 3 -- --
December 4 2017· ·

r~~ !' ~~n~ ~~ i:!':s Cost Level (*
~ -~ denotes clinic Primary Care Primary Care Clinic II :f Care moved to 2 for
ID County City ST Clinic Number Number Eff 3/1/18 Clinic Address u8 System 2017 Cost level acce11s) ~a..
BC Steams St. Cloud MN C412800 003365662 CentraCare Clinic • Midtown 3333 West Division Street, #218 PCC CEN 3 3
BC Steams St. Cloud MN C412206 003217449 CentraCare Clinic ·Northway Family Medicine 1555 Northway Drive, #100 PCC CEN 3 3
BC Steams St. Cloud MN C411808 003211800 CentraCare Clinic • River Campus 1200 Sixth Ave. North PCC CEN 3 3
BC Stearns St. Cloud MN M301956 003207233 CentraCare Family Health Center 1555 Northway Drive PCC CEN 3 3
BC Steams St. Cloud MN C412846 003638673 St. Cloud Medical Group • Northwest 251 County Road 120 PCC STC 2 2
BC Steams St. Cloud MN C412844 003642549 St. Cloud Medical Group • South 1301 • 33rd St. South PCC STC 2 2
BC Steams St. Joseph MN C412206 003217446 CentraCare Clinic • St. Joseph Clinic 1360 Elm St. East PCC CEN 3 3 !
i
BC Wright St. Michael MN A262451 003213244 Allina Health St. Michael Clinic 4300 Edgewood Dr. NE PCC ALL 2 2 I
BC Calver Waconia MN L051392 003209895 Lakeview Clinic ·Waconia 424 State Hwy. 5 W. PCC LAK 2 2
BC Calver Watertown MN C462270 003219353 Catalyst Medical Clinic ·Watertown 204 Lewis Ave. S., #201 PCC IMT 3 2
BC Carver Watertown MN L051392 003209895 Lakeview Clinic ·Watertown 309 Jefferson Ave SW PCC LAK 2 2
BC Sherburne Zimmerman MN F262625 003198716 FaiiView Clinics • Zimmennan 25945 GateWay Dr. PCC FAJ I 2 3
December 4 2017

\ @)·· ....... ...._ ....._ PUBLIC EMPLOYEES INSURANCE PROGRAM (PEIP)
ADVANTAGE HEALTH PLAN
@
2018 Questions & Answers .
(lnformatlonAiso AvailableOnlin·e@ www.innovornn~c6m).
Ql.· What i~ ~he Advantage ttealth. Plan and how does it w~rk?. · ..
Al. The State ofMim1esota implemented Advantage·in 2002to address'rapidly rising health care costs and to' mait1tain access to as manyh'E~alth Care prb\liders fotstate employees as . possible. The PEIP Advantage Plan was first offered in 2007 to all public employers. PEIP has had great success with the Advantage program. Over the last S~VE!n years,'PEIP's average pool increase has been approximately 2.3%.
Under AdvantC,tge, primary care clinicsyster:ns ~vailableto ernployees,-are .placed in costlevels according to their actual, risk-adjusted costs of delivering care and to meet geographic access needs. Employees and their family members are free to 'selectproviders oft heir choke 'tn' their area, and to change their select ibn during the year withit1 the s~mehealth carrier. The amount employees and family members payout.;.of-pocket for copays, deauctibles, and coinsurance varies according to the cost level of the provider used. The lower the cost level of the provider, the lower the out-of-pocket costs for Advantage members~
This award winning plan design and structure gives members flexibility and choice whiletaking advantage of best practices in provider competition and rnanagjngthe cost of care;
Q2. Why are there four Advantage provider cost levels?
A2. Advantage places health care providers in cost levels based on their actuaJ.costs of delivering care and to meet·geographic accessneedsi The purpose ohh-e costlevel~ is tO help inform employees and their families of differences in the cost of healthcaredelivery;'and to · create incentives for providers to control costs. The premium for each plan level does not change but employees pay differeht' levels Of co pays, deductibh~s/an'd coinstira·nce depending on the cost level of the provider they use. , ·· ' ·
>·(
Cqst l~vel four .reflects t .. he f~<:t that .a number pf.clin~cs.ystems,havecrnuch higher:.costs than . . .
others. Without <:ost le~el fo!Jr1 it likely .wo1..1ld nqt~be pos.sjb.l'e t();COt}tinl(e. offe~ing the highest cost providers to employees. Cost level four preserves the availability of these highest cost prQviders: Ern plqyees are free to choose any cqst levet provide(~ in dud ing thpse in cost level four. There is. no difference in mo.nthly premium, but. employees wiH.contin!Je to pay less outof-pocket in deductibles, co payments, etc. when using a provider with a lower cost level, and more when choosing a higher cost level provider.

@ Q3. How are the cost levels of the clinics determined?
A3. The cost levels of the clinics are determined based on an analysis of their actual costs of delivering care and to meet geographic access needs. In the analysis, the results are "risk adjusted/' which means that differences in patient populations have been taken into account to help ensure that providers do not appear to be more expensive simply because they are caring for patients who are more ill than others.
The very lowest cost clinics were put into level one. The next lowest group of clinics is in level two, and the highest cost clinics are in levels three and four. In order to provide access statewide to a level two option for all employees, some higher cost clinics or clinic groups were moved to level two, identified by * in the clinic directory. Also, a few differences exist in the cost level placement of individual clinics, depending on their health carrier affiliation(s) or as a result of some administrative limitations among the health carriers. Finally, some clinic groups have negotiated lower reimbursements in exchange for being offered at a lower cost level.
It is important for you check the most current clinic listing to verify your clinic's cost level during the open enrollment.
Q4. How often will the cost level of the clinics change? Can they change mid-year?
A4. The cost levels of clinic groups will be re-evaluated once per year. The cost level of a clinic could only increase to a higher level mid-year if the clinic changes its care system affiliation. If this were to occur, members of the clinic would be notified.
QS. How do I find out what cost level my clinic is in?
AS. You can view the 2018 state~wide clinic listings at www.innovomn.com/plan information.html.
QG. What is a "first dollar deductible"?
AG. A form of employee cost sharing called a "first dollar deductible" is a set amount that is paid annually before the plan benefits take effect. Once the deductible is paid, it is not charged again during that calendar year.
The deductible applies to all services except preventive care and prescription drugs (for Advantage and Value plan options. For the HSA, the deductible applies to all services except preventive care.) It is called a 11first dollar deductible" because the deductible must be paid first before the plan benefits take effect. If employees do not receive health care services during the calendar year, or if they receive only preventive services, they pay no deductible.
The purpose of the deductible is to help keep monthly premiums more affordable and to create greater awareness of the costs of health care services. This is a typical feature in many health plans. ©

~ @
Q7. What is the copay in the Advantage Plan?
A7. A co-payment (copay) is a flat dollar amount that is charged every time certain services are provided. Under Advantage, the amount of the copay varies, depending on the I( cost level" of the primary care clinic that the employee or their family members are enrolled in- generally, the higher the cost level of the primary care clinic, the higher the copay. Under Advantage, co pays are charged for the following types of services:
• Office visits • Emergency room visits • Inpatient admissions • Outpatient surgery • Prescription drugs
QB. What is coinsurance? What coinsurance will I have to pay with the Advantage Plan?
AB. Coinsurance is a percentage of the eligible cost that is charged for certain services after the annual deductible is paid. As with the copays and deductibles described above, the amount of coinsurance varies with the cost level of the primary care clinic. Coinsurance is in effect most often with cost level 4 providers.
Q9. Are there caps on the cost-sharing (copays, deductibles, and coinsurance) that I have to pay? What are the caps?
A9. There are caps known as the I( out-of-pocket maximums." There are two separate caps, one for prescription drugs, and one for all other services. The HSA compatible version of Advantage has a single combined out-of-pocket maximum. Once the out-of-pocket maximum is reached for the year, the employee pays no more cost sharing.
QlO. Are there any other costs with Advantage? What is not covered?
AlO. Advantage generally does not pay for I( non-network" services unless they are considered urgent or emergency care services. The "network" refers to the health care providers available to the employee through their primary care clinic and health carrier, including any referrals that are provided by the primary care clinic. Advantage pays Urgent care, and emergency costs as if you were treated through your network provider.

Qll. What are the rules for choosing a health carrier and primary care clinic under Advantage?
All. The following requirements apply:
• All members of a family must select the same health Network.
• Family members may choose different primary care clinics in different cost levels.
@
• Employees and dependents can change clinics two times per year if they are also changing cost levels. To make a clinic change, employees call the carrier directly.
• Employees and dependents can change clinics every month if they are not changing cost levels, subject to the health carrier's rules. To make a clinic change, employees call the carrier directly.
• Employees are encouraged to choose a clinic in the area in which they live or work so that they can access care easily.
Q12. If the premium is the same for each health carrier, and my clinic is available in more than one network, how should I choose a health carrier?
A12. Employees have a number of factors to consider when deciding on a health carrier. All dependents must be enrolled with the employee's health carrier; so employees will need to determine which carrier offers the primary care clinic of his/her dependents' choices.
Other factors to consider include the cost level and referral patterns of health carriers and particular specialist networks such as OB/GYNs, chiropractors, mental health providers, substance abuse professionals and routine vision services.
Q13. How do I see specialists under Advantage? What cost level will I receive?
A13. All care is coordinated through your primary care clinic (PCC). Generally, you will need a referral from your primary care clinic in order to see a specialist. Once referred, specialist services are covered at the same level as your primary care. For some specialty care, such as OB/GVN, chiropractic, routine vision, substance abuse and mental health, you may self refer, providing the practitioner is within the self referral network of the carrier you choose. See the Q and A's below for more information.
@)

~ ®
Q14. How do I see an OB/GVN?
A14. If you enroll in Blue Cross Blue Shield, you have access to all the OB/GYNs listed With the Blue Cross network of OB/GYNs.
If you enroll in Health Partners (HP) or PreferredOne (Pl), you will need to take some additional steps to confirm whether you can go to a specific OB/GYN without a referral. You can do this by going to the HP or Pl websites and using the provider search tool or by calling the carriers' customer service unit. The benefits received at the OB/GYN will be at the cost level of the primary care clinic (PCC) you select.
QlS. How can I see a chiropractor and mental health providers?
AlS. You may self-refer to certain chiropractors and mental health providers. Access tothese providers depends on the carrier and the primary care clinic chosen. If you enroll in Blue Cross Blue Shield, you can self refer to any chiropractor or mental health provider listed in the Blue Cross network. If you enroll in Health Partners, you can self-refer to anychiropractor or mental health provider listed in the Health Partners network. If you enroll in Preferred One (Pl), you will need to take some additional steps to confirm whether you can go to a specific chiropractor or mental health provider without a referral. You generally must use a provider that is associated with your primary care clinic. You can find providers by going to the Pl website and using the provider search tool or by calling the carrier's customer service unit. The benefits received at the chiropractic or mental health clinics will be at the cost level of the primary care clinic (PCC) you select.
QlG. Can I change health carriers at any time?
AlG. No. Employees can only change health carriers at openenrollmentor ifthey move out of the service area of their health carrier. You can change clinics during the year by callingthe number on your ID card. The clinic change will be effective on the first of the next month.
Q17. What out-of-network benefits are available to people who live out of state and out of the service area of the health carriers?
A17. Employees and their dependentswho live outside the State and the Advantage Service Area (includes early retirees, employees on sabbatical, college students): These individuals are eligible for the Point-of-Service (POS) benefit. There is a separate deductible and coinsurance amounts with this coverage. Individuals using POS benefits are not required to choose an out of area provider, but may receive discounted services by utilizing their health carrier's national preferred provider organization (PPO).

@ Q18. What benefits do students who live in state and within the service area of the health
carriers receive?
A18. If the eligible student is to receive services, the employee will need to choose a health carrier that offers primary care clinics for both the employee's and the student's locations. Employees and dependents can choose their own clinics- they do not need to choose the same clinic or clinics within the same cost level. Students who are eligible dependents living in the state and within the service area of the health carrier will receive the benefits at the cost level of the clinic they have enrolled in.
Q19. Where do employees get a detailed description of their coverage?
A19. The Summary of Benefits will be available to every employee as they enroll in the plan. Plan Documents are also available on the PEIP website at www.innovomn.com/plan information.html.
Q20. Is there a mail order program for prescriptions?
A20. Yes. You can receive up to a 90-day supply of certain maintenance medications through mail-order pharmacies. For mail order, you pay two co pays for a 90-day supply of these drugs; the plan pays 100% of the balance. The plan is administered by Navitus.
Q21. I went to my doctor for a yearly routine examination. I have had some concerns with a health condition that I have. I talked to my doctor about these and he ordered some additional tests. I was charged a copay for the visit. Is this correct?
A21. Yes. The routine preventive portion of the examination is covered at 100% without a copay. However, additional tests that are related to your health condition are not .considered preventive care, and the copay will apply.
Q22. I have diabetes so I need to see my doctor for care related to my condition four times per year. Willi have to pay the copay for these visits?
A22. Yes. Preventive care is generally one routine physical examination per year. Check-ups relating to an illness or injury are not considered preventive, and the copay will apply.
~

C8 @
Q23. Does Advantage offer a Health Club Benefit? What is the benefit?
A23. Yes. The PEIP Fitness Discount Program is provided through your network selection for medical coverage. All three carriers participate in the program. The Benefit: Work out at least 12 times per month and receive $20/month reimbursement towards your health club dues. Up to two members per household can participate in the program (with family medical coverage)must be 18 years old or older.
Q24. What are online clinics and how do they work?
A24. PEIP Advantage includes services from two online clinics. Members can use either online clinic service- no matter what carrier network you choose.
www.Virtuwell.com
www.OnlineCareAnywhereMN.com
Online clinics allow members to consult with a doctor or certified nurse practitioner online 24 hours a day, seven days a week. These health care professionals can make a diagnosis, create a personalized treatment plan or send a prescription, if needed, for over 50 routine conditions such as colds, flu, allergies, ear/eye/sinus infections, skin conditions, lice, etc.
It's easy, confidential and cost effective for the member.
Q25. What are convenience clinics and how do I find them?
A25. Convenience clinics provide walk-in services in a retail setting. Locations vary based on the carrier network you choose and the area in which you live. Not all areas of the state have convenience clinics. If available, convenience clinics provide routine services for minor ailments, similar to urgent care centers, but at a lower capay or out of pocket expense.
Below are examples. Members can contact their carrier for more convenience clinic information.
Note: All HSA-compatible plan copays are after the deductible has been met.
Please Note: These questions and answers are informational only. The Summary of Benefits includes more detailed information. The actual amount of payment for any claim will be determined by the health carrier based on the information submitted by the provider of services.