Embed Size (px)
DESCRIPTION
SPONDYLITIS
Citation preview

Traie
*U
C
I
I
o
AMm
2
Ankylosing Spondylitis: A ContemporaryPerspective on Diagnosis and Treatment
Mark Mansour,* Gurtej S. Cheema,† Stanley M. Naguwa,‡
Adam Greenspan,§ Andrea T. Borchers,� Carl L. Keen,¶ andM. Eric Gershwin#
Objectives: In recent years, great progress has been made in the development of diagnostic tools,therapeutic approaches, and validated outcome measures in the understanding of the pathogenesisof ankylosing spondylitis (AS). The purpose of this review was to summarize these developments.Methods: We performed a PubMed search for the period 1978 to 2005, using the keyword,“ankylosing spondylitis,” resulting in a total of 4878 publications, including 778 reviews. Articleswere then selected based on their discussion of recent diagnostic tools and new treatment ap-proaches in the pathogenesis of AS, leading to a final total of 104 articles.Results: In recent years, there have been 2 major developments in the management of AS that makeearlier diagnosis possible and offer the hope of alleviating pain and preventing structural changesthat result in loss of function. These developments include the use of magnetic resonance imagingto visualize the inflammatory changes in the sacroiliac joint and the axial spine, and the demon-stration that tumor necrosis factor blocking agents are highly efficacious in reducing spinal inflam-mation and possibly in slowing radiographic progression.Conclusions: There have been major advances in both the diagnostic tools and the therapeuticregimens available for patients with AS.© 2007 Elsevier Inc. All rights reserved. Semin Arthritis Rheum 36:210-223Keywords: seronegative spondyloarthritis, computed tomography, TNF blocking agents, sacroiliitis,HLA B27
pIaaEplUdciydoet
M
Wl
he prototypic seronegative spondyloarthropathy(SpA) is ankylosing spondylitis (AS); other formsinclude reactive arthritis (Reiter syndrome), pso-
iatic arthritis, enteropathic arthritis, and undifferenti-ted SpA. AS is a chronic inflammatory rheumatic diseasenvolving primarily the sacroiliac joint and the axial skel-ton, but also peripheral joints and entheses. It can be
Postdoctoral Fellow, Division of Rheumatology, Allergy, and Clinical Immunology,niversity of California, Davis, CA.†Assistant Clinical Professor of Medicine, Division of Rheumatology, Allergy, and
linical Immunology, University of California, Davis, CA.‡Clinical Professor of Medicine, Division of Rheumatology, Allergy, and Clinical
mmunology, University of California, Davis, CA.§Professor of Radiology, University of California, Davis, CA.�Visiting Postdoctoral Fellow, Division of Rheumatology, Allergy, and Clinical
mmunology, University of California, Davis, CA.¶Professor and Chair, Department of Nutrition, University of California, Davis, CA.#Professor and Chief, Division of Rheumatology, Allergy, and Clinical Immunol-
gy, University of California, Davis, CA.Address reprint requests to: M. Eric Gershwin, MD, Division of Rheumatology,
llergy, and Clinical Immunology, University of California at Davis School of
sedicine, 451 E. Health Sciences Drive, Suite 6510, Davis, CA 95616. E-mail:[email protected]
10 0049-0172/07/$-see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.semarthrit.2006.08.003
resent as primary AS or can be secondary to other SpAs.f patients present with AS before the age of 16 years, theyre classified as having juvenile AS or enthesitis-relatedrthritis, a subtype of juvenile idiopathic arthritis (1).ven though the prevalence of axial SpA is �5% amongatients with chronic back pain (2), it is frequently over-
ooked as a possible diagnosis especially in young patients.ntil recently, even if AS was considered a possibility, aecade or more frequently passed before the diagnosisould be considered definite. Furthermore, disease-mod-fying treatments were essentially unavailable. In recentears, great progress has been made in the development ofiagnostic tools, therapeutic approaches, and validatedutcome measures in the understanding of the pathogen-sis of AS. The purpose of this review was to summarizehese developments.
ETHODS
e performed a PubMed search using the terms “anky-osing spondylitis” in the period of 1978 to 2005, re-
tricted to the English language. This yielded a total of
4acpatAtvt
R
E
Hegttelb(asp
P
G
Ao
tgibStaBirtts
PM
TeTwao(tBfe
BvusHirpboismov(sn
Asmmfgte
M. Mansour et al. 211
878 publications, including 778 reviews. From this list,nd based on the abstract, a total of 427 articles werehosen that appear to highlight recent progress in theathogenesis of AS as well as in the use of diagnostic toolsnd therapeutic approaches. In addition, we also reviewedhe data in these 104 articles regarding the associations ofS with epidemiology and genetics. The clinical charac-
eristics of patients as well as diagnostic technological ad-ances were also compiled. Our final emphasis was on thereatment of AS.
ESULTS
pidemiology
istorically, AS was thought to be a disease that almostxclusively affected young men. More recent studies sug-est a male-to-female ratio of about 2 or 3 to 1, althoughhere can be considerable geographical and ethnic varia-ion. Disease onset generally occurs in late adolescence orarly adulthood, most frequently in the third decade ofife. For white populations, prevalence estimates rangeetween �0.1 and 1.4% (3-6). Human leukocyte antigenHLA)-B27 is strongly linked to disease susceptibility,nd there is a close correlation between the frequency ofeveral subtypes of this allele in a population and therevalence of AS.
athogenesis
enetics
positive family history of AS can be found in 15 to 20%
Abbreviations
AS ankylosing spondylitisASAS assessment in ASBASDAI Bath AS Disease Activity IndexBASFI Bath AS Functional Index�2m �2-microglobulinCD cluster of differentiationCT computed tomographyDISH diffuse idiopathic skeletal hyperostosisDMARD disease-modifying antirheumatic drugER endoplasmic reticulumESR erythrocyte sedimentation rateEULAR European League Against RheumatismFDA Food and Drug AdministrationHLA human leukocyte antigenIFN interferonIL interleukinMHC major histocompatibility complexMRI magnetic resonance imagingNSAIDs nonsteroidal antiinflammatory drugsRA rheumatoid arthritisRCT randomized controlled trialSpA spondyloarthropathySSZ sulfasalazineTNF tumor necrosis factor
f cases (7). Monozygotic twins have a concordance for b
he disease of 63 to 75% compared with 12.5% in dizy-otic twins (8). This suggests a major genetic componentn the pathogenesis of the disease. A strong associationetween HLA-B27 and susceptibility to AS and otherpAs has been recognized for decades and is illustrated byhe fact that �90% of AS patients of European ancestryre HLA-B27-positive, and concordance rates in HLA-27-positive dizygotic twins are significantly higher than
n dizygotic twins overall (27% versus 12.5%) (8). A keyole for HLA-B27 is further suggested by the fact that ratsransgenic for HLA-27 develop a progressive inflamma-ory arthritis whose clinical and histological features re-emble those of the inflammatory SpAs (9).
athogenic Immunologicechanisms of HLA-B27
here are at least 25 alleles or subtypes of HLA-B27 thatncode 23 different products: HLA-B*2701 to 2723.hese alleles are thought to have evolved from the mostidespread subtype, B*2705 (10), which is clearly associ-
ted with AS risk, as demonstrated by its presence in 90%f B-27-positive patients of northern European extraction11). Other common subtypes that confer susceptibilityo AS and other SpAs are B*2701, B*2702, B*2704,*2705, and B*2707. In contrast, B*2706 and B*2709,
ound in Southeast Asia and Sardinia, respectively, do notxhibit disease associations (10).
Several mechanisms for the pathogenic role of HLA-27 in AS and other SpAs have been proposed and in-olve its classical function as a restriction element, molec-lar mimicry, a role of HLA-B27 as an autoantigen, andome unique features in the intracellular processing of theLA-B27 heavy chains giving rise to their homodimer-
zation. It has been hypothesized that the pathogeneticole of HLA-B27 involves the presentation of a uniqueeptide of microbial or self-origin. In particular, it haseen postulated that microbial infections can lead to lossf self-tolerance when antibodies or T-cells elicited by thenfectious agents cross-react with a host protein because ithares extensive sequence homology with the microbialolecule. In support of such molecular mimicry, homol-
gy has been demonstrated between various bacterial oriral peptides and peptides derived from human proteins12-14). In addition, certain self-peptides not only shareequence homology with bacterial antigens, but are alsoatural ligands of HLA-B27 (12,15).The differential association of HLA-B27 alleles with
S suggests that disease-associated and nonassociatedubtypes differ in their peptide repertoire and/or theode of peptide presentation. Indeed, even though theajor disease-associated and nonassociated subtypes dif-
er by only a single residue within the peptide-bindingroove, their peptide and cytotoxic T-lymphocyte reper-oires do not completely overlap (14,15). In addition,ven when AS-associated and nonassociated subtypes
ind the same peptide, the mode of presentation can dif-
fmstmpbsr(prthtfa
(CCpadothaTbai
cmcfatfsmatwfAtdhItafchh
MtHo
bsbHtsfbcb
tapptdilbdoboiD((n1ct
vpmaasornrmcmutt
p
212 Ankylosing spondylitis
er dramatically. For example, striking differences in theode of peptide presentation were demonstrated for the
elf-peptide pVIPR from vasoactive intestinal peptideype 1 receptor and the viral peptide pLMP2 from latentembrane protein 2 of Epstein–Barr virus (16,17). Im-
ortantly, these peptides share 6 of 9 amino acid residues,ut exhibit extensive structural similarity only when pre-ented by B*2705, indicating that molecular mimicry isestricted to the disease-associated allele at least in this case16). Similarly, it was recently shown that another self-eptide with homology with enterobacterial antigens wasecognized by HLA-B27-restricted cluster of differentia-ion (CD)8 T-cells from AS patients, but not by those ofealthy controls (15). In contrast, other HLA-B27:pep-ide complexes are structurally, thermodynamically, andunctionally equivalent and are, therefore, unlikely to playrole in the pathogenesis of AS (18).Of note, although major histocompatibility complex
MHC) class I generally is a restriction element forD8� T-cells, the existence of MHC class I restrictedD4 T-cells has been demonstrated. It was recently re-orted that AS patients possessed CD4� T-cells that re-cted with HLA-B27 if it was expressed in cell lines withefective antigen-processing pathways (19). Several linesf evidence suggested that altered forms of B27, ratherhan the usual heterotrimeric complex consisting of aeavy chain associated with �2-microglobulin (�2m) andpeptide, were recognized by these CD4 T-lymphocytes.hese findings may be of pathogenetic relevance if micro-ial infections are capable of altering antigen processing,s has been shown for some viruses, or of otherwise induc-ng the expression of altered forms of B27.
HLA-B27 heavy chains have some highly unusualharacteristics in terms of their folding and complex for-ation with �2m in the endoplasmic reticulum (ER), the
ellular compartment in which proteins that are destinedor the cell surface or the extracellular space are processednd, in some cases, assembled into larger complexes. Dueo their unique B-pocket in the peptide-binding groove,olding of HLA-B27 heavy chains was found to be muchlower than folding of other HLA alleles, resulting in theirisfolding and degradation even in cells with an intact
ntigen-processing pathway (20). It has been suggestedhat the degradation pathway could become over-helmed and that the resulting accumulation of mis-
olded protein in the ER could trigger a stress response.lthough this would lead to activation of the transcrip-
ion factor NF-�B and, consequently, stimulate the pro-uction of proinflammatory cytokines, it remains unclearow this would contribute to the pathogenesis of AS.mpaired folding of HLA-B27 heavy chains also results inhe formation of 2 types of homodimers, 1 of which is notssociated with �2m, but can be detected on the cell sur-ace of HLA-B27-transfected T2 cells and appears to beapable of peptide binding (21,22). It is thought that theomodimerization would require unwinding of the �1
elix, which might then resemble the �-chain helix of an vHC class II molecule. This provides a possible explana-ion for the findings discussed above, suggesting thatLA-B27-reactive CD4� T-cells from AS patients rec-
gnized homodimeric B27 (19).There is increasing evidence that HLA-B27 itself could
e a source of antigenic peptides. Several such peptideshare sequence homology with bacterial antigens and toe natural ligands of HLA-B27 (12,15) and also ofLA-A2, which was able to cross-present these peptides
o CD4� T-cells (23). Based on molecular modelingtudies, it has even been proposed that �2m-free, peptide-ree heavy chains of HLA-B27 can undergo rotation of theackbone in such a way that residues 169 to 181 (whichorrespond to a known B27 ligand) can occupy its owninding groove (24).While B-27 has been shown to be unequivocally linked
o AS and other inflammatory SpAs, AS can occur in thebsence of HLA-B27. Only about 10% of HLA-B27-ositive subjects (who constitute �8% of the generalopulation) develop the disease (25), and even identicalwins who are HLA-B27-positive can be discordant forisease incidence as well as severity (8,26). This clearly
ndicates that HLA-B27 is neither sufficient nor abso-utely necessary for the occurrence of AS. Instead, it isecoming increasingly evident that AS is a polygeneticisease, in which HLA-B27 accounts for a minority of theverall genetic susceptibility to AS (25). Other genes haveeen implicated in either increasing disease susceptibilityr modifying the clinical expression of AS. Candidatesnclude other MHC genes such as HLA-B60, HLA-
RB1, and HLA-DR8, and tumor necrosis factorTNF), as well as non-MHC genes such as interleukinIL)-10, IL-1 receptor (IL-1R), and CYP2D6. In ge-ome-wide searches, chromosomes 1p, 2q, 6p, 9q, 10q,6q, and 19q have been linked to increased genetic sus-eptibility (25). To date, however, none of these associa-ions have been consistently seen in different populations.
Although the genetic component of AS is strong, de-elopment of AS obviously depends on a complex inter-lay of genetic and environmental factors. The involve-ent of bacterial infections in the pathogenesis of reactive
rthritis is well documented, and a variety of infectiousgents, including Shigella, Yersinia, and particularly Kleb-iella, have been implicated as triggering agents or sourcesf cross-reactive peptides in AS. However, a pathogenicole for microbial infections in the pathogenesis of AS hasot been shown conclusively. In contrast, it was recentlyeported that the magnitude of cellular and humoral im-une responses to Klebsiella pneumoniae, Yersinia entero-
olitica, Chlamydia trachomatis, and Salmonella typhi-urium did not differ significantly between AS patients,naffected family members, and unrelated healthy con-rols (27). This argues against a central role for these ar-hritogenic organisms in the pathogenesis of AS.
Subclinical ileal inflammation is seen in over 50% ofatients with SpA, including those with AS and, con-
ersely, almost 40% of patients with inflammatory bowel
dsBrflt
vscfcatatwpSct
lmadtccitnmvbtcpaeant
CTrappTmdspm
itttpmT
plIWchdltTcnjTwpa
C
Isppestgflflpimrbrmws
moi(b5ch
M. Mansour et al. 213
isease exhibit articular manifestations similar to thoseeen in SpA (13,28). In addition, rats transgenic for HLA-27 do not develop arthritis if raised in germ-free envi-
onments, but do so on reintroduction of commensalora. Although this suggests that gut bacteria could act asriggering agents in AS, their role remains speculative.
Enthesitis is a typical feature of AS and typically in-olves the fibrocartilaginous rather than the fibrous enthe-es (29). It also affects structures that are not classicallyonsidered entheses but share many of their structural andunctional characteristics as well as the presence of fibro-artilage (29). In addition, they are all exposed to largemounts of shear stress and microtrauma. This has led tohe hypothesis that the immune response in AS is targetedgainst fibrocartilage-rich entheses and enthesis-like struc-ures, and that mechanical stresses, possibly in conjunctionith bacteria or their products, trigger inflammatory andathological changes in genetically susceptible subjects (29).ince entheseal fibrocartilage is avascular, such pathologicalhanges would be necessary to expose fibrocartilaginous an-igens to circulating lymphocytes.
Like cartilage, fibrocartilage in entheses and enthesis-ike structures contains the proteoglycan aggrecan. Im-
unization of mice with this protein or its hyaluroniccid binding G1 globular domain induces spondylitis andiscitis (30). It was recently shown that 62% of AS pa-ients possessed circulating CD4� T-cells that specifi-ally recognized the G1 domain of aggrecan, and the per-entage was even higher when synovial T-cells werenvestigated (31). Aggrecan is also present within the in-ervertebral disc; the anterior uveal tract exhibits immu-oreactivity with antibodies to aggrecan, and smoothuscle cells in arterial tissue produce the proteoglycan
ersican, which also contains a globular G1 domain thatinds to hyaluronic acid (30). Thus, the tissue distribu-ion of the G1 domain of aggrecan and related proteogly-ans seems to provide an explanation for the tissue tro-ism of AS manifestations, ie, the fact that suchpparently diverse tissues as the axial skeleton, heart, andyes are affected. This explanation does not contradict thebove hypothesis involving shear stress in fibrocartilagi-ous structures since these are features of all the tissueshat express aggrecan or versican (29).
The finding that HLA-B27 can interact with bothD8� and CD4� T-cells raises the possibility that both-cell subsets are involved in the pathogenesis of AS. The
esults of the few available immunohistological studies onffected tissues in AS patients suggest that CD8� T-cellsredominate in the cellular infiltrate of entheses (32) andossibly also of synovial membranes (33), whereas CD4-cells are the major cell type in sacroiliac biopsy speci-ens (34). Oligoclonal expansion of CD8� T-cells, in-
icative of antigen-specific stimulation of this T-cell sub-et, was found to be much more extensive in HLA-B27-ositive AS patients compared with their healthy
onozygotic twins and unrelated healthy HLA-B27-pos- vtive subjects (35). It could not be established whetherhese expanded T-cells were HLA-B27 restricted. Impor-antly, however, oligoclonal expansion was also seen inhe CD4� T-cell subset of AS patients, but was com-letely absent in unaffected twins. In addition, animalodels of SpAs suggest a more important role for CD4�-cells in disease pathogenesis.As in almost any autoimmune disease, data on cytokine
rofiles in AS patients are rather conflicting (36). Highevels of circulating IL-6 and normal concentrations ofL-1� have been detected in several groups of AS patients.
hile some investigators reported increased serum con-entrations of TNF-� in AS patients compared withealthy controls, others were unable to detect significantifferences. Data on serum IL-10 and interferon (IFN)-�
evels are contradictory. Somewhat more consistently, in-racellular production of Th1 cytokines (IFN-�, IL-2,NF-�) was decreased in peripheral and gut mucosal T-
ells of AS patients compared with healthy controls. Ofote, in computer tomography (CT)-guided sacroiliac
oint biopsy samples from 5 AS patients, high levels ofNF-� mRNA were detected in the infiltrates (34). Asill be discussed further below, a role for TNF-� in theathogenesis of AS is clearly indicated by the efficacy ofnti-TNF agents in the treatment of this disease.
linical Features
nflammatory low back pain is the most typical presentingymptom of AS (37). Symptoms may be mild initially, andatients have difficulty pinpointing the exact date when theirain started. In fact, up to 10% of subjects with radiographicvidence of AS may be unaware of their disease becauseymptoms are either absent or very mild (38). The presenta-ion of back pain is not an uncommon occurrence in theeneral population, making it important to differentiate in-ammatory from noninflammatory causes of back pain. In-ammatory back pain is characterized by stiffness andain that is worse in the morning or after long periods ofnactivity and is improved with exercise. Patients com-
only complain of difficulty sleeping or pain that is notelieved with rest or lying down (39). In addition to lum-osacral pain, patients often report pain in the glutealegion, which most likely represents sacroiliac involve-ent. Sacroiliitis may cause piriformis muscle spasm,hich results in compression of the sciatic nerve and sub-
equent radiation of pain to the lower extremities (40).AS is not limited to the lumbar-sacral spine. Approxi-ately 70% of patients complain of neck pain. In a study
f 571 AS patients, radiographic evidence of cervical spinenvolvement was seen in more than half of the patients41). The risk of cervical spine involvement was found toe a function of disease duration, with 20% affected afteryears and 70% affected after 20 years. It was also asso-
iated with severity of hip and lumbar involvement and aistory of iritis, but not with age of onset or gender. Cer-
ical spine disease usually presents as neck pain and stiff-
naacp
sdutcalv((ePiqoctdatst(lp
(mll(tirdiooowtauMjcwtit
et
E
NaAdlltassipiao
pdchbbcstftdo
bldhomcsd
conriItfiltt
214 Ankylosing spondylitis
ess; however, torticollis has been reported. Cervical fix-tion in mild flexion causes the head to protrude forwardnd makes it difficult for patients to look straight ahead. Aompensatory flexion of the knees results in the classicosture of the patient with advanced AS.Peripheral arthritis can be the earliest symptom in a
ubstantial portion (�20%) of AS patients (37,42) andevelops at some point during the course of the disease inp to 60% of patients (6,42), although it becomes persis-ent in only about half of those affected; the pattern isommonly asymmetrical and mono- or oligoarticular. Inddition to hips and shoulders, the large joints of theower limbs are most frequently affected, although in-olvement of elbow, wrist, and hand is not uncommon37,42,43). Radiographs or magnetic resonance imagingMRI) of the affected joints show joint space narrowing,rosions with new bone formation, and synovitis (44-46).eripheral articular joint involvement is associated with
ncreased disease activity (43,47) and deterioration inuality of life (43). An association with worse functionalutcome has also been reported (43,48), but this is not aonsistent finding (47,49). A recent study in Korean pa-ients even suggests that patients with peripheral jointisease have less severe spinal disease than those withoutppendicular involvement (42). Bony ankylosis and os-eoarthritis can result in severe limitation of motion andubstantial to complete loss of function particularly inhe hip (50), but also in the knee and shoulder joints51). Approximately 8 to 15% of AS patients withong-term follow-up have to undergo total joint arthro-lasty (48,49).Enthesitis is a hallmark of AS and may involve synovial
including hip and shoulder) or cartilaginous joints, syndes-oses, and extra-articular entheses. Entheses of the lower
imbs are affected more frequently than those of the upperimbs and the most common site of enthesitis is the heel37,52). Heel enthesitis is thought to involve inflamma-ion at the site of attachment of the plantar fascia, result-ng in erosions of the calcaneus, followed by a periostealeaction with formation of bone spurs. The Achilles ten-on insertion is another common site that can become
nflamed resulting in heel pain. Note, however, that somether enthesopathies may be underdiagnosed. The resultsf a recent MRI study in AS patients suggest that synovitisf the knee and possibly of other peripheral joints is al-ays accompanied by enthesitis, although clinically de-
ectable in only a minority of cases (53). It had beenssumed that the shoulder pain of AS patients was attrib-table to synovitis, bursitis, or structural damage. A recentRI study, however, found synovitis of the glenohumeral
oint in only 12% of AS patients compared with 3% ofontrols (46). However, erosions of the greater tuberosityere seen in 65% of AS shoulders and only 14% of con-
rol shoulders. Importantly, these were the same patientsn whom clinical evaluation indicated the presence of ro-
ator cuff tendonitis. Together, these findings suggest that wnthesitis is the primary lesion in AS, underlying many ofhe skeletal manifestations of the disease.
xtra-Articular Manifestations
onspecific signs and symptoms such as fever, fatigue,nd weight loss can arise at any time during the course ofS. Extra-articular manifestations, such as uveitis and car-iovascular, pulmonary, and lung disease, can be the ear-
iest manifestations of disease, but most often occur atater stages. Acute anterior uveitis (iritis) is an inflamma-ion of the anterior portion of the eye leading to scarringnd blurring of vision if not treated appropriately. It iseen in up to 40% of patients with AS (48,49,54) and isignificantly more common in HLA-B27-positive thann HLA-B27-negative patients (54). Patients typicallyresent with ocular pain, redness, and photophobia. Uve-tis can be the first indication of AS and other HLA-B27-ssociated diseases in a substantial portion (almost 20%)f patients (55).
Cardiovascular disease can be seen in 10 to 40% ofatients with AS, and its incidence rises with increasingisease duration (56). Cardiovascular complications in-lude aortitis and aortic insufficiency, which can result ineart failure and death. In addition, conduction distur-ances including audiovisual block and bundle branchlock, as well as myocardial involvement resulting inompromise of left ventricular function, have been de-cribed in AS patients. While no specific recommenda-ions exist regarding the use of echocardiography to screenor cardiac disease in these patients, a significant propor-ion of patients with AS will have echocardiographic evi-ence of aortic root involvement before the clinical onsetf aortic regurgitation.
Pulmonary involvement in AS patients is related tooth mechanical and fibrotic changes. Decreased total
ung capacity is thought to be secondary to kyphosis andecreased chest expansion. In 17 AS patients, 11 of whomad had AS for �10 years, high-resolution chest CT dem-nstrated airway disease in 14 (82%), interstitial abnor-alities in 11 (65%), and emphysema in 6 (35%). These
hanges were not evident on plain radiographs (57). Veryimilar findings were reported in a study of patients whoseisease duration was �10 years (58).Renal manifestations are relatively rare in AS, but in-
lude such severe conditions as secondary renal amyloid-sis, IgA nephropathy, mesangioproliferative glomerulo-ephritis, and membranous nephropathy. Secondaryenal amyloidosis (62%) is the most common renal man-festation (59) and occurs in 1 to 2% of AS patients (48).gA nephropathy constitutes �30% of renal manifesta-ions in AS. Elevated serum IgA levels are a commonnding and may be attributable to impaired IgA catabo-
ism, as suggested by the observation that expression ofhe Fc� receptor (CD89) on blood monocytes and neu-rophils was significantly lower in AS patients compared
ith controls (60).
D
Tidatimcmcdittpct
imAsptvvpa
r“iclcp“a
o
stMtCcttr(vpit
Fvlyaj
M. Mansour et al. 215
iagnosis
he diagnosis of AS is based on clinical features and phys-cal examination findings as well as radiologic evidence ofisease. The modified New York diagnostic criteria are inlmost universal use (Table 1) (61). For the assessment ofhe clinical diagnostic criteria, the modified Schober tests used to measure anterior spinal flexion, and lateral spine
otion is assessed using lateral bending of the lumbosa-ral spine with the occiput to the wall. Chest expansion iseasured at the 4th intercostal space. Palpation or per-
ussion of the sacroiliac joints may elicit pain, but thisoes not reliably indicate the presence of sacroiliitis. Plac-
ng stress on the sacroiliac joints with the Flexion, Abduc-ion, and External Rotation maneuver and the Gaenslenest can illustrate sacroiliac joint dysfunction and may alsoroduce pain. Examination and review of the eyes and theardiovascular and pulmonary systems may uncover ex-ra-articular disease.
The use of radiographs in the assessment of sacroiliitiss instrumental in the diagnosis of AS. Sacroiliitis is the
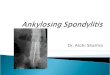
ost frequent and earliest radiographic manifestation ofS (62) (Fig. 1). Radiographic grading of sacroiliitis con-
ists of 5 grades, ranging from 0 � normal to IV � com-lete ankylosis (Table 2). Due to oblique orientation ofhe normal sacroiliac joints, the entire joint may not beisible on standard anteroposterior radiographs of the pel-is. An oblique angled or Ferguson view overcomes thisroblem (62) but there is no evidence that this approach isctually superior to the standard one (63).
Osteitis and subsequent erosions of the anterior supe-ior and inferior surfaces cause the classic finding ofsquaring” of the vertebral bodies (64) (Fig. 2). Measur-ng the vertebral concavity is helpful in monitoring theourse of the illness over time. Ossification of the spinaligaments that bridge the intervertebral discs results in theharacteristic bony protuberances called “syndesmo-hytes,” giving in advanced disease the appearance of abamboo spine” (Fig. 3). Hip joints are also frequentlyffected (Fig. 4).
Interpretation of sacroiliac radiographs is difficult andpen to interpretational variation, especially in the early
Table 1 Modified New York Criteria (61)
1. Radiological criterionBilateral sacroiliitis grade �II or unilateral sacroiliitisgrade III to IV
2. Clinical criteria(a) Low back pain and stiffness of at least 3 months
duration improved by exercise and not relievedby rest
(b) Limitation of motion of the lumbar spine in boththe sagittal and the frontal planes
(c) Limitation of chest expansion relative to valuesnormal for age and sex
Definite AS is diagnosed if the radiological criterion plus 2 of the
a3 clinical criteria are present.
tages of disease (62). In direct comparisons with conven-ional radiography, newer techniques such as CT and
RI demonstrate considerably higher sensitivity in iden-ifying sacroiliitis in the early stages of AS (65,66) (Fig. 5).T appears to be superior to MRI for the visualization of
hronic changes (63). On the other hand, MRI is the onlyechnique that can image acute and chronic lesions simul-aneously (63) and it seems to perform better than CT inevealing early cartilage changes and bone marrow edema66). A further advantage of MRI is that it does not in-olve radiation exposure. In addition, recent MRI studiesrovide evidence that the most frequent and severe lesionsn AS patients affect the thoracic spine (67). Large parts ofhe thoracic and lumbar spine cannot be adequately visu-
igure 1 Sacroiliitis. (A) Conventional radiograph of the pel-is of a 32-year-old man with stage II/III ankylosing spondy-itis shows bilateral sacroiliitis. (B) In another patient, a 50-ear-old man with advanced disease, both sacroiliac jointsre fused. Inflammatory arthritis affects also the right hipoint (arrow).
lized radiographically. Therefore, the ability to image

tt
dtai(teppseRrmdpdta
mhtTeh
Amrtaaspceuctalrt
t(rmafptchavelbdciat
Flta
216 Ankylosing spondylitis
his spinal region constitutes another important advan-age of MRI.
MRI of peripheral joints may also help in the earlyiagnosis of SA. It was recently reported that intense en-heseal bone marrow edema particularly in the acromiont the deltoid origin was a highly specific finding, presentn 41% of AS shoulders and none of the control shoulders46). When MRI was used in SpA and rheumatoid arthri-is (RA) patients with recent onset knee effusion, peri-ntheseal edema was detected in the knees of all 10 SpAatients and entheseal bone marrow edema in 6 of 10 SAatients, but in none of the RA patients (53). The lattertudy also reported the co-occurrence of synovitis andnthesitis in all AS patients, compared with none of theA patients. The specificity for AS of both the co-occur-
ence of synovitis and enthesitis and the presence of bonearrow edema in affected joints could have important
iagnostic implications in patients presenting only witheripheral arthritis. In addition to its role in the earlyiagnosis of AS, MRI is rapidly developing into a valuableool for the assessment of changes in spinal inflammationnd acute and chronic lesions due to treatment (68-70).
Nonetheless, conventional radiography remains theethod of choice for making the diagnosis of AS since the
igh cost and limited availability of MRI and CT restrictheir use in the routine evaluation of the sacroiliac joints.hese tests should be reserved for patients with normal or
quivocal radiographs for whom clinical suspicion of AS isigh.There are no laboratory findings that are diagnostic of
S. As in most disease states involving systemic inflam-ation, acute phase reactants (erythrocyte sedimentation
ate [ESR] and C-reactive protein) may be elevated, butheir concentrations show little correlation with diseasectivity. Rheumatoid factor and antinuclear antibodiesre absent. Alkaline phosphatase levels may be elevated inevere disease. Serum IgA levels are raised in many ASatients. Traditionally, testing for HLA-B27 has been dis-ouraged since it is not diagnostic of the disease. How-ver, the high prevalence of this antigen in AS makes these of HLA-B27 useful as an adjunct in diagnosis, espe-ially in cases where the physician has a strong suspicionhat AS is present (71). In ethnic groups such as Africannd Japanese patients where the presence of HLA-B27 isow, the positive-predictive value of a positive HLA-B27esult in conjunction with inflammatory back pain is ex-
Table 2 Radiographic Grading of Sacroiliitis (61)
Grade Appraisal
0 Normal—normal width, sharp joint marginsI SuspiciousII Sclerosis, some erosionsIII Severe erosions, pseudodilatation of the
joint space, partial ankylosisIV Complete ankylosis
remely high (71). m
It is not uncommon that 8 or more years pass betweenhe first symptoms of AS and its definitive diagnosis48,54). This is partly due to the fact that unequivocaladiographic evidence of sacroiliitis, as required by theodified New York criteria, often can be seen only years
fter the first symptoms of disease. Another contributingactor is the low awareness of the disease among generalractitioners. Since delay in diagnosis entails a delay ofreatment and truly disease-modifying therapies have be-ome available, early diagnosis is of utmost importance. Itas been proposed that an early diagnosis of axial SpA (ASnd undifferentiated SpA with predominant axial in-olvement) can be made with a high degree of confidenceven in patients who lack radiographic evidence of sacroi-iitis (2). In such cases, the diagnosis is based on a proba-ility of axial SpA of �90%, with this probability beingerived from the presence of inflammatory back pain inombination with at least 2 or 3 clinical, laboratory, ormaging features that are highly characteristic of SpA. Ex-mples of such features are a positive family history, en-hesitis, anterior uveitis, good response to nonsteroidal
igure 2 Early vertebral changes. Lateral radiograph of theumbar spine in a 28-year-old man shows squaring ofhe vertebral bodies secondary to small osseous erosionst the corners (so-called “shiny corners”). Note the syndes-
ophyte formation at the anterior L4 to 5 disk space (arrow).
M. Mansour et al. 217
Figure 3 Advanced vertebral changes.(A) Lateral radiograph of the cervicalspine in a 50-year-old man showsanterior syndesmophytes bridgingthe vertebral bodies, and posteriorfusion of the apophyseal joints. (B)Conventional tomography of thethoracic spine shows syndesmo-phytes to better advantage, produc-ing a “bamboo-spine” appearance.Note preservation of the interverte-bral disks. (C) Anteroposterior and(D) lateral radiographs of the lumbo-sacral spine show similar changes asin the cervical and thoracic seg-ments. Note complete fusion of thesacroiliac joints.

aBmtreccA
D
TpMsd
Nanfai((dehoI
T
Tmtrsapncprctd(hoaps
Fy
F3
218 Ankylosing spondylitis
ntiinflammatory drugs (NSAIDs), positivity for HLA-27 (in patients of European descent), and MRI abnor-alities. It will be of great interest to determine whether
his approach proves useful in clinical settings. A recenteview of the literature suggests that the combined pres-nce of inflammatory back pain and HLA-B27 positivityonstituted the best measures to help primary care physi-ians in deciding to refer patients to a rheumatologist forS (72).
ifferential Diagnosis
he differential diagnosis of lower back pain in youngatients includes mechanical and nonmechanical causes.echanical causes comprise sprains and strains, compres-
ion or traumatic fracture, spondylosis, and alignmentisorders (kyphosis, scoliosis, and spondylolisthesis).
igure 4 Complete ankylosis of the right hip joint in a 48-ear-old man with ankylosing spondylitis.
igure 5 Axial CT section shows bilateral sacroiliitis in a
A4-year-old man.onmechanical causes include the other SpAs, RA, osteo-rthritis of the spine, herniated disc, infection, and malig-ancy. Lower back pain can also be due to referred painrom pelvic, renal, or gastrointestinal disease, and aorticneurysm. When sacroiliitis can be confirmed throughmaging, the differential diagnosis becomes limitedTable 3). Diffuse idiopathic skeletal hyperostosisDISH) or Forestier disease may mimic AS in that syn-esmophytes and enthesopathy are present in both dis-ases. However, DISH usually presents later in life andas larger and horizontally rather than vertically orientedsteophytes, and there is no evidence of sacroiliitis (62).n addition, DISH is not associated with HLA-B27 (73).
reatment
he goals of therapy are divided into the 4 followingajor categories: (1) patient education in the natural his-
ory of the disease, treatment options, and the patient’sole in disease modifying behavior; (2) relief of pain andtiffness; (3) maintenance of spinal and overall mobilitynd prevention of disability through physical therapy andharmacological disease modifying agents; and (4) recog-ition and management of articular and extra-articularomplications. In some patients, physicotherapeutic andharmacologic approaches may be insufficient for painelief and maintenance of mobility. In such cases, surgicalorrection of spinal deformity and total joint arthroplas-ies for hip, knee, or shoulder abnormalities may provideurable pain relief and some functional improvement74). The International Assessment in AS (ASAS) groupas established a group of core domains for the assessmentf disease and response to treatment (75). These domainsre functional assessment, pain, stiffness, spinal mobility,atient’s global assessment, peripheral joints and enthe-es, acute phase reactants, fatigue, and radiographs. The
Table 3 Causes of Sacroiliitis (104)
SpondyloarthropathiesASReiter syndromePsoriatic arthritisSAPHO (synovitis acne pustolosis hyperostosis
osteitis) syndromeIntestinal bypass arthritis
InfectiousPyogenic infectionsTuberculosisBrucellosisWhipple disease
OthersHyperparathyroidismParaplegiaSarcoidosisUlcerative colitisCrohn’s disease
SAS20 has been validated for the assessment of short-

t2vpii�1f
ad(mnaeptbe
AghciosdsNsdtcts
dnas
orscp
ddhtpi
cAlaahidwa1rieawarc5ssAo(wttgyo3aHwr
susap(Ti
trhgi(arf
M. Mansour et al. 219
erm improvement and is defined as an improvement of0% or a positive change of at least 10 units on a 100-mmisual analog scale in at least 3 of the 4 ASAS domains,atient’s global assessment, spinal pain, function accord-ng to the Bath AS Functional Index (BASFI), and morn-ng stiffness. The remaining domain must not worsen by
20% or show a negative change of at least 10 units on a00-mm scale (76). The BASFI is a validated instrumentor the assessment of physical function (77).
The ASAS group together with the European Leaguegainst Rheumatism (EULAR) recently developed evi-ence-based recommendations for the management of AS78). These recommendations emphasize that the optimalanagement of AS patients “requires a combination of
onpharmacological and pharmacological treatments”nd stress the importance of patient education, regularxercise and/or physical therapy, and possibly social sup-ort groups. Home exercise programs, supervised groupherapy, and spa-exercise therapy have all been shown toe effective in improving function based on the BASFI,ven if the evidence is of moderate quality only (79).
First-line therapy to control pain and inflammation inS consists of NSAIDs. In patients with increased risk ofastrointestinal problems, selective cyclooxygenase-2 in-ibitors (coxibs) should be considered. Of note, in a re-ent 2-year randomized controlled trial (RCT) compar-ng continuous and on-demand treatment with celecoxibr another NSAID in 215 symptomatic AS patients, atrategy of continuous use resulted in a reduction of ra-iographic progression without increasing toxicity sub-tantially (80). Importantly, this is the first time thatSAIDs have been reported to slow radiographic progres-
ion. The most common side effects were hypertension,yspepsia, and abdominal pain. With growing evidencehat coxib and possibly even noncoxib NSAIDs are asso-iated with significant cardiovascular toxicity, both gas-rointestinal risk and cardiovascular risk need to be con-idered in choosing an NSAID.
Intra- or peri-articular corticosteroid injections are in-icated for relieving the pain of sacroiliitis (74). There areo clinical studies on their efficacy in peripheral arthritisnd enthesitis. There is no evidence supporting the use ofystemic corticosteroids.
Recurrences of uveitis are common during the coursef AS. Treatment usually begins with topical corticoste-oids; periocular corticosteroid injections are necessary inome patients, and resistant cases may require systemicorticosteroids. Sulfasalazine (SSZ) may be of benefit inreventing recurrences of uveitis (81).Despite their success in treating other inflammatory
iseases such as RA, disease-modifying antirheumaticrugs (DMARDs), including methotrexate and SSZ,ave not shown efficacy in treating the axial manifesta-ions of AS. However, SSZ may be beneficial in treatingeripheral joint disease in reducing ESR and easing morn-
ng stiffness. fAs mentioned previously, TNF-� is a proinflammatoryytokine found at elevated concentrations in the serum ofS patients (36) and whose mRNA is detectable in high
evels in sacroiliac biopsy samples (34). Currently avail-ble anti-TNF therapies include infliximab, etanercept,nd adalimimab, of which only infliximab and etanerceptave undergone RCTs. Results are available from 4 RCTs
n AS patients treated with subcutaneous etanercept at aose of 25 mg twice a week (82-85) and from 2 RCTsith infliximab given intravenously at a dose of 5 mg/kg
t 0, 2, and 6 weeks in 1 case (86) and at 0, 2, 6, 12, and8 weeks in the other (87). The response to both agents isapid, with improvement seen as early as 2 weeks afternitiation of therapy. Overall, the response rate according toither an ASAS20 response or a 50% disease repression asssessed via the Bath AS Disease Activity Index (BASDAI)as around 60% in the etanercept trials and between 51
nd 53% in the infliximab trials compared with responseates between 9 and 28% in the placebo groups. A majorlinical response to TNF-� inhibitors, as defined by a0% improvement in the BASDAI, was associated withhorter disease duration, younger age, and lower BASFIcores (88). Lower BASFI scores also predicted a betterSAS20 response in another analysis, as did higher levelsf C-reactive protein and a greater degree of back pain89). Since these findings come from groups of patientsith high disease activity at the beginning of anti-TNF
reatment, it remains to be established whether these fac-ors can also predict treatment response in AS patients ineneral. The clinical response is maintained for at least 2ears in the case of etanercept (90) and 3 years in the casef infliximab (68,91). Of note, discontinuation even afteryears of continuous treatment leads to relapse in virtu-
lly all patients (mean time to relapse 17.5 weeks) (92).owever, resumption of infliximab or etanercept therapyas safe and resulted in achievement of the same clinical
esponse as seen before cessation of treatment (92,93).Both etanercept and infliximab caused regression of
pinal inflammation, and this effect was not lost afterp to 2 years of treatment (68-70,94). Progression oftructural damage was not prevented by treatment withnti-TNF agents, but appeared to have been slowed, inatients with definite radiographic changes at baseline69,70). Furthermore, treatment of AS patients withNF-� inhibitors is associated with a significant decrease
n the number of anterior uveitis flares (95).Etanercept and infliximab have been approved for the
reatment of AS by the FDA and also in Europe, andecommendations regarding the use of these TNF-� in-ibitors in the treatment of AS have been set by the ASASroup (96). These recommendations include the follow-ng: (1) initiation only after a definitive diagnosis of ASusing modified New York criteria); (2) active disease fort least 4 weeks based on clinical symptoms, acute phaseeactants, and imaging; (3) refractory disease defined byailure of at least 2 NSAIDs during a 3-month period,
ailure of at least 1 intra-articular steroid injections, if
aiuafs
taMoem
ocwaitflCiv
D
AiiA1wsmaostBgssalihwpsoifm(vA
nicf
R
220 Ankylosing spondylitis
ppropriate, and failure of SSZ in patients with predom-nately peripheral arthritis; and (4) application of thesual precautions and contraindications for biologic ther-py (96). We would like to emphasize that, unlike in RA,ailure of 1 or more DMARDs is not a requirement in ASince DMARDs are not effective in treating axial disease.
While TNF-� inhibitors have shown great promise,heir expense and their potential toxicities, including re-ctivation of tuberculosis (which makes screening forycobacterium tuberculosis a standard prerequisite) and
verwhelming infection, have tempered optimism. How-ver, when carefully monitored and used in patients thateet certain criteria, their benefit is indisputable.When medical therapy fails, surgical intervention is an
ption for some patients. Hip replacement is the mostommon surgery and may be the only option in patientsith fixed flexion deformities of the hip to relieve pain
nd increase mobility. Surgical treatment of the spine isndicated in cases of severe instability, pain, vertebral frac-ure, and for those patients with such a degree of spinalexion that their range of vision is extremely limited.auda equina syndrome resulting from spinal instability
s a surgical emergency that requires rapid surgical inter-ention.
ISCUSSION
s discussed above, the treatment of AS has dramaticallymproved. In addition, the diagnostic tools as well as med-cal therapy have changed dramatically in the past decade.
prospective study of 150 war veterans with AS, begun in947, indicated that the prognosis for AS patients overallas good, with only 10 to 20% of patients becoming
ignificantly disabled (97). Most patients were able toaintain full-time employment with adequate treatment
nd lifestyle modifications. Few other data are availablen the outcome and prognosis in AS, and older studiesuffer from the lack of validated outcome measures. Suchools are now available, including the BASDAI (98), theASFI (77), and several instruments for assessing radio-raphic damage (99,100). Recent findings on patientseen in tertiary referral centers and, hence, from the moreevere end of the disease spectrum, suggest that diseasectivity remains relatively constant for extended fol-ow-up periods, whereas functional impairment steadilyncreases (49). There appears to be general agreement thatip involvement is an important prognostic factor fororse functional and radiographic outcomes, while otherredictors such as peripheral joint involvement, early re-triction of spinal mobility, male gender, younger age atnset, elevated ESR, and iritis have been less consistentlydentified (49,101,102). Unfortunately, AS patients stillace a significantly increased risk of mortality, most com-only due to cardiovascular and cerebrovascular disease
103). Finally, we note that the issue of premature cardio-ascular disease in inflammatory arthritis is not unique to
S and reflects an important issue that rheumatologistseed to emphasize in the management of their patients. Its also an important clinical problem that will continue tohallenge physicians as well as being a critical area foruture research.
EFERENCES
1. Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Gold-enberg J, et al. International League of Associations for Rheuma-tology classification of juvenile idiopathic arthritis: second revi-sion, Edmonton, 2001. J Rheumatol 2004;31:390-2.
2. Rudwaleit M, van der Heijde D, Khan MA, Braun J, Sieper J.How to diagnose axial spondyloarthritis early. Ann Rheum Dis2004;63:535-43.
3. Sieper J, Braun J, Rudwaleit M, Boonen A, Zink A. Ankylosingspondylitis: an overview. Ann Rheum Dis 2002;61(Suppl 3):iii8-18.
4. Braun J, Bollow M, Remlinger G, Eggens U, Rudwaleit M,Distler A, et al. Prevalence of spondylarthropathies in HLA-B27positive and negative blood donors. Arthritis Rheum 1998;41:58-67.
5. Saraux A, Guillemin F, Guggenbuhl P, Roux CH, Fardellone P,Le Bihan E, et al. Prevalence of spondyloarthropathies in France:2001. Ann Rheum Dis 2005;64:1431-5.
6. Trontzas P, Andrianakos A, Miyakis S, Pantelidou K, VafiadouE, Garantziotou V, et al. Seronegative spondyloarthropathies inGreece: a population-based study of prevalence, clinical pattern,and management. The ESORDIG study. Clin Rheumatol 2005;24:583-9.
7. Hochberg MC, Bias WB, Arnett FC Jr. Family studies in HLA-B27 associated arthritis. Medicine (Baltimore) 1978;57:463-75.
8. Brown MA, Kennedy LG, MacGregor AJ, Darke C, Duncan E,Shatford JL, et al. Susceptibility to ankylosing spondylitis intwins: the role of genes, HLA, and the environment. ArthritisRheum 1997;40:1823-8.
9. Hammer RE, Maika SD, Richardson JA, Tang JP, Taurog JD.Spontaneous inflammatory disease in transgenic rats expressingHLA-B27 and human beta 2m: an animal model of HLA-B27-associated human disorders. Cell 1990;63:1099-112.
10. Ball EJ, Khan MA. HLA-B27 polymorphism. Joint Bone Spine2001;68:378-82.
11. Khan MA. A worldwide overview: the epidemiology of HLA-B27 spondylarthritides. In: Calin A, Taurog JD, eds. Spondylar-thritides. Oxford, Oxford University Press, 1998;17-27.
12. Ramos M, Alvarez I, Sesma L, Logean A, Rognan D, Lopez deCastro JA. Molecular mimicry of an HLA-B27-derived ligand ofarthritis-linked subtypes with chlamydial proteins. J Biol Chem2002;277:37573-81.
13. Reveille JD, Arnett FC. Spondyloarthritis: update on pathogen-esis and management. Am J Med 2005;118:592-603.
14. Fiorillo MT, Maragno M, Butler R, Dupuis ML, Sorrentino R.CD8� T-cell autoreactivity to an HLA-B27-restricted self-epitope correlates with ankylosing spondylitis. J Clin Invest2000;106:47-53.
15. Frauendorf E, von Goessel H, May E, Märker-Hermann E.HLA-B27-restricted T cells from patients with ankylosing spon-dylitis recognize peptides from B*2705 that are similar to bacte-ria-derived peptides. Clin Exp Immunol 2003;134:351-9.
16. Fiorillo MT, Rückert C, Hülsmeyer M, Sorrentino R, SaengerW, Ziegler A, et al. Allele-dependent similarity between viral andself-peptide presentation by HLA-B27 subtypes. J Biol Chem2005;280:2962-71.
17. Hülsmeyer M, Fiorillo MT, Bettosini F, Sorrentino R, SaengerW, Ziegler A, et al. Dual, HLA-B27 subtype-dependent confor-mation of a self-peptide. J Exp Med 2004;199:271-81.
18. Hülsmeyer M, Welfle K, Pöhlmann T, Misselwitz R, Alexiev U,
Welfle H, et al. Thermodynamic and structural equivalence of
M. Mansour et al. 221
two HLA-B27 subtypes complexed with a self-peptide. J MolBiol 2005;346:1367-79.
19. Boyle LH, Goodall JC, Opat SS, Gaston JS. The recognition ofHLA-B27 by human CD4� T lymphocytes. J Immunol 2001;167:2619-24.
20. Mear JP, Schreiber KL, Münz C, Zhu X, Stevanovic S, Ram-mensee HG, et al. Misfolding of HLA-B27 as a result of its Bpocket suggests a novel mechanism for its role in susceptibility tospondyloarthropathies. J Immunol 1999;163:6665-70.
21. Dangoria NS, DeLay ML, Kingsbury DJ, Mear JP, Uchanska-Ziegler B, Ziegler A, et al. HLA-B27 misfolding is associatedwith aberrant intermolecular disulfide bond formation (dimer-ization) in the endoplasmic reticulum. J Biol Chem 2002;277:23459-68.
22. Allen RL, O’Callaghan CA, McMichael AJ, Bowness P. Cuttingedge: HLA-B27 can form a novel beta 2-microglobulin-freeheavy chain homodimer structure. J Immunol 1999;162:5045-8.
23. Boyle LH, Goodall JC, Gaston JS. Major histocompatibilitycomplex class I-restricted alloreactive CD4� T cells. Immunol-ogy 2004;112:54-63.
24. Luthra-Guptasarma M, Singh B. HLA-B27 lacking associated�2-microglobulin rearranges to auto-display or cross-display res-idues 169-181: a novel molecular mechanism for spondyloar-thropathies. FEBS Lett 2004;575:1-8.
25. Reveille JD, Ball EJ, Khan MA. HLA-B27 and genetic predis-posing factors in spondyloarthropathies. Curr Opin Rheumatol2001;13:265-72.
26. Brophy S, Hickey S, Menon A, Taylor G, Bradbury L, Ham-ersma J, et al. Concordance of disease severity among familymembers with ankylosing spondylitis? J Rheumatol 2004;31:1775-8.
27. Stone MA, Payne U, Schentag C, Rahman P, Pacheco-Tena C,Inman RD. Comparative immune responses to candidate arthri-togenic bacteria do not confirm a dominant role for Klebsiellapneumonia in the pathogenesis of familial ankylosing spondyli-tis. Rheumatology (Oxford) 2004;43:148-55.
28. Kim TH, Uhm WS, Inman RD. Pathogenesis of ankylosingspondylitis and reactive arthritis. Curr Opin Rheumatol 2005;17:400-5.
29. Benjamin M, McGonagle D. The anatomical basis for diseaselocalisation in seronegative spondyloarthropathy at entheses andrelated sites. J Anat 2001;199:503-26.
30. Poole AR. The histopathology of ankylosing spondylitis: arethere unifying hypotheses? Am J Med Sci 1998;316:228-33.
31. Zou J, Zhang Y, Thiel A, Rudwaleit M, Shi SL, Radbruch A, et al.Predominant cellular immune response to the cartilage autoanti-genic G1 aggrecan in ankylosing spondylitis and rheumatoid arthri-tis. Rheumatology (Oxford) 2003;42:846-55.
32. Laloux L, Voisin MC, Allain J, Martin N, Kerboull L, ChevalierX, et al. Immunohistological study of entheses in spondyloar-thropathies: comparison in rheumatoid arthritis and osteoarthri-tis. Ann Rheum Dis 2001;60:316-21.
33. Baeten D, Demetter P, Cuvelier C, Van Den Bosch F, KruithofE, Van Damme N, et al. Comparative study of the synovialhistology in rheumatoid arthritis, spondyloarthropathy, and os-teoarthritis: influence of disease duration and activity. AnnRheum Dis 2000;59:945-53.
34. Braun J, Bollow M, Neure L, Seipelt E, Seyrekbasan F, HerbstH, et al. Use of immunohistologic and in situ hybridizationtechniques in the examination of sacroiliac joint biopsy speci-mens from patients with ankylosing spondylitis. ArthritisRheum 1995;38:499-505.
35. Duchmann R, Lambert C, May E, Höhler T, Märker-Hermann E.CD4� and CD8� clonal T cell expansions indicate a role of anti-gens in ankylosing spondylitis; a study in HLA-B27� monozygotic
twins. Clin Exp Immunol 2001;123:315-22.36. Keller C, Webb A, Davis J. Cytokines in the seronegative spon-dyloarthropathies and their modification by TNF blockade: abrief report and literature review. Ann Rheum Dis 2003;62:1128-32.
37. Sampaio-Barros PD, Bertolo MB, Kraemer MH, Neto JF, Sa-mara AM. Primary ankylosing spondylitis: patterns of disease ina Brazilian population of 147 patients. J Rheumatol 2001;28:560-5.
38. Mader R. Atypical clinical presentation of ankylosing spondyli-tis. Semin Arthritis Rheum 1999;29:191-6.
39. van der Linden S, van der Heijde D. Ankylosing spondylitis.Clinical features. Rheum Dis Clin North Am 1998;24:663-76,vii.
40. Rodrigue T, Hardy RW. Diagnosis and treatment of piriformissyndrome. Neurosurg Clin N Am 2001;12:311-9.
41. Maghraoui AE, Bensabbah R, Bahiri R, Bezza A, Guedira N,Hajjaj-Hassouni N. Cervical spine involvement in ankylosingspondylitis. Clin Rheumatol 2003;22:94-8.
42. Baek HJ, Shin KC, Lee YJ, Kang SW, Lee EB, Yoo CD, et al.Clinical features of adult-onset ankylosing spondylitis in Koreanpatients: patients with peripheral joint disease (PJD) have lesssevere spinal disease course than those without PJD. Rheuma-tology (Oxford) 2004;43:1526-31.
43. Bostan EE, Borman P, Bodur H, Barca N. Functional disabilityand quality of life in patients with ankylosing spondylitis. Rheu-matol Int 2003;23:121-6.
44. Mundinger A, Ioannidou M, Meske S, Dinkel E, Beck A, Sig-mund G. MRI of knee arthritis in rheumatoid arthritis and spon-dylarthropathies. Rheumatol Int 1991;11:183-6.
45. Vinje O, Dale K, Moller P. Radiographic evaluation of patientswith Bechterew’s syndrome (ankylosing spondylitis). Findingsin peripheral joints, tendon insertions and the pubic symphysisand relations to non-radiographic findings. Scand J Rheumatol1985;14:279-88.
46. Lambert RG, Dhillon SS, Jhangri GS, Sacks J, Sacks H, WongB, et al. High prevalence of symptomatic enthesopathy of theshoulder in ankylosing spondylitis: deltoid origin involvementconstitutes a hallmark of disease. Arthritis Rheum 2004;51:681-90.
47. Heuft-Dorenbosch L, van Tubergen A, Spoorenberg A, Land-ewe R, Dougados M, Mielants H, et al. The influence of periph-eral arthritis on disease activity in ankylosing spondylitis patientsas measured with the Bath Ankylosing Spondylitis Disease Ac-tivity Index. Arthritis Rheum 2004;51:154-9.
48. Gran JT, Skomsvoll JF. The outcome of ankylosing spondylitis:a study of 100 patients. Br J Rheumatol 1997;36:766-71.
49. Robertson LP, Davis MJ. A longitudinal study of disease activityand functional status in a hospital cohort of patients with anky-losing spondylitis. Rheumatology (Oxford) 2004;43:1565-8.
50. Joshi AB, Markovic L, Hardinge K, Murphy JC. Total hip ar-throplasty in ankylosing spondylitis: an analysis of 181 hips.J Arthroplasty 2002;17:427-33.
51. Parvizi J, Duffy GP, Trousdale RT. Total knee arthroplasty inpatients with ankylosing spondylitis. J Bone Joint Surg Am2001;83A:1312-6.
52. Olivieri I, Barozzi L, Padula A. Enthesiopathy: clinical manifes-tations, imaging and treatment. Baillieres Clin Rheumatol 1998;12:665-81.
53. McGonagle D, Gibbon W, O’Connor P, Green M, Pease C,Emery P. Characteristic magnetic resonance imaging enthesealchanges of knee synovitis in spondylarthropathy. ArthritisRheum 1998;41:694-700.
54. Feldtkeller E, Khan MA, van der Heijde D, van der Linden S,Braun J. Age at disease onset and diagnosis delay in HLA-B27negative vs. positive patients with ankylosing spondylitis. Rheu-matol Int 2003;23:61-6.
55. Monnet D, Breban M, Hudry C, Dougados M, Brezin AP.
Ophthalmic findings and frequency of extraocular manifesta-
222 Ankylosing spondylitis
tions in patients with HLA-B27 uveitis: a study of 175 cases.Ophthalmology 2004;111:802-9.
56. Sukenik S, Pras A, Buskila D, Katz A, Snir Y, Horowitz J. Car-diovascular manifestations of ankylosing spondylitis. Clin Rheu-matol 1987;6:588-92.
57. Souza AS Jr, Muller NL, Marchiori E, Soares-Souza LV, deSouza Rocha M. Pulmonary abnormalities in ankylosing spon-dylitis: inspiratory and expiratory high-resolution CT findings in17 patients. J Thorac Imaging 2004;19:259-63.
58. Kiris A, Ozgocmen S, Kocakoc E, Ardicoglu O, Ogur E. Lungfindings on high resolution CT in early ankylosing spondylitis.Eur J Radiol 2003;47:71-6.
59. Strobel ES, Fritschka E. Renal diseases in ankylosing spondylitis:review of the literature illustrated by case reports. Clin Rheuma-tol 1998;17:524-30.
60. Montenegro V, Chiamolera M, Launay P, Goncalves CR, Mon-teiro RC. Impaired expression of IgA Fc receptors (CD89) byblood phagocytic cells in ankylosing spondylitis. J Rheumatol2000;27:411-7.
61. van der Linden S, Valkenburg HA, Cats A. Evaluation of diag-nostic criteria for ankylosing spondylitis. A proposal for modifi-cation of the New York criteria. Arthritis Rheum 1984;27:361-8.
62. Resnick D, Niwayama G. Ankylosing spondylitis. In: ResnickD, ed. Diagnosis of Bone and Joint Disorders. Philadelphia, WBSaunders, 1981;1040-102.
63. Braun J, van der Heijde D. Imaging and scoring in ankylosingspondylitis. Best Pract Res Clin Rheumatol 2002;16:573-604.
64. Aufdermaur M. Pathogenesis of square bodies in ankylosingspondylitis. Ann Rheum Dis 1989;48:628-31.
65. Geijer M, Sihlbom H, Gothlin JH, Nordborg E. The role of CTin the diagnosis of sacro-iliitis. Acta Radiol 1998;39:265-8.
66. Yu W, Feng F, Dion E, Yang H, Jiang M, Genant HK. Com-parison of radiography, computed tomography and magneticresonance imaging in the detection of sacroiliitis accompanyingankylosing spondylitis. Skeletal Radiol 1998;27:311-20.
67. Baraliakos X, Landewe R, Hermann KG, Listing J, Golder W,Brandt J, et al. Inflammation in ankylosing spondylitis: a system-atic description of the extent and frequency of acute spinalchanges using magnetic resonance imaging. Ann Rheum Dis2005;64:730-4.
68. Sieper J, Baraliakos X, Listing J, Brandt J, Haibel H, Rudwaleit M,et al. Persistent reduction of spinal inflammation as assessed bymagnetic resonance imaging in patients with ankylosing spondylitisafter 2 yrs of treatment with the anti-tumour necrosis factor agentinfliximab. Rheumatology (Oxford) 2005;44:1525-30.
69. Baraliakos X, Davis J, Tsuji W, Braun J. Magnetic resonanceimaging examinations of the spine in patients with ankylosingspondylitis before and after therapy with the tumor necrosisfactor � receptor fusion protein etanercept. Arthritis Rheum2005;52:1216-23.
70. Baraliakos X, Listing J, Rudwaleit M, Brandt J, Sieper J, Braun J.Radiographic progression in patients with ankylosing spondylitisafter 2 years of treatment with the tumour necrosis factor alphaantibody infliximab. Ann Rheum Dis 2005;64:1462-6.
71. Khan MA, Khan MK. Diagnostic value of HLA-B27 testingankylosing spondylitis and Reiter’s syndrome. Ann Intern Med1982;96:70-6.
72. Sieper J, Rudwaleit M. Early referral recommendations forankylosing spondylitis (including pre-radiographic and ra-diographic forms) in primary care. Ann Rheum Dis 2005;64:659-63.
73. Yagan R, Khan MA. Confusion of roentgenographic differentialdiagnosis between ankylosing hyperostosis (Forestier’s disease)and ankylosing spondylitis. Clin Rheumatol 1983;2:285-92.
74. Braun J, Baraliakos X, Godolias G, Bohm H. Therapy of anky-losing spondylitis—a review. Part I: Conventional medical treat-
ment and surgical therapy. Scand J Rheumatol 2005;34:97-108.75. van der Heijde D, Calin A, Dougados M, Khan MA, van derLinden S, Bellamy N. Selection of instruments in the core set forDC-ART, SMARD, physical therapy, and clinical record keep-ing in ankylosing spondylitis. Progress report of the ASAS Work-ing Group Assessments in Ankylosing Spondylitis. J Rheumatol1999;26:951-4.
76. Anderson JJ, Baron G, van der Heijde D, Felson DT, DougadosM. Ankylosing Spondylitis Assessment Group preliminary defi-nition of short-term improvement in ankylosing spondylitis. Ar-thritis Rheum 2001;44:1876-86.
77. Calin A, Garrett S, Whitelock H, Kennedy LG, O’Hea J, Mal-lorie P, et al. A new approach to defining functional ability inankylosing spondylitis: the development of the Bath AnkylosingSpondylitis Functional Index. J Rheumatol 1994;21:2281-5.
78. Zochling J, van der Heijde D, Burgos-Vargas R, Collantes E,Davis JC Jr, Dijkmans B, et al. ASAS/EULAR recommendationsfor the management of ankylosing spondylitis. Ann Rheum Dis2005;65:442-52.
79. Dagfinrud H, Kvien TK, Hagen KB. The Cochrane review ofphysiotherapy interventions for ankylosing spondylitis. J Rheu-matol 2005;32:1899-906.
80. Wanders A, Heijde D, Landewe R, Behier JM, Calin A, OlivieriI, et al. Nonsteroidal antiinflammatory drugs reduce radio-graphic progression in patients with ankylosing spondylitis: arandomized clinical trial. Arthritis Rheum 2005;52:1756-65.
81. Benitez-Del-Castillo JM, Garcia-Sanchez J, Iradier T, BanaresA. Sulfasalazine in the prevention of anterior uveitis associatedwith ankylosing spondylitis. Eye 2000;14(Pt. 3A):340-3.
82. Gorman JD, Sack KE, Davis JC Jr. Treatment of ankylosingspondylitis by inhibition of tumor necrosis factor alpha. N EnglJ Med 2002;346:1349-56.
83. Davis JC Jr, Van Der Heijde D, Braun J, Dougados M, Cush J,Clegg DO, et al. Recombinant human tumor necrosis factorreceptor (etanercept) for treating ankylosing spondylitis: a ran-domized, controlled trial. Arthritis Rheum 2003;48:3230-6.
84. Calin A, Dijkmans BA, Emery P, Hakala M, Kalden J, Leirisalo-Repo M, et al. Outcomes of a multicentre randomised clinicaltrial of etanercept to treat ankylosing spondylitis. Ann RheumDis 2004;63:1594-600.
85. Brandt J, Khariouzov A, Listing J, Haibel H, Sörensen H,Grassnickel L, et al. Six-month results of a double-blind, place-bo-controlled trial of etanercept treatment in patients with activeankylosing spondylitis. Arthritis Rheum 2003;48:1667-75.
86. Braun J, Brandt J, Listing J, Zink A, Alten R, Golder W, et al.Treatment of active ankylosing spondylitis with infliximab: arandomised controlled multicentre trial. Lancet 2002;359:1187-93.
87. van der Heijde D, Dijkmans B, Geusens P, Sieper J,DeWoody K, Williamson P, et al. Efficacy and safety of in-fliximab in patients with ankylosing spondylitis: results of arandomized, placebo-controlled trial (ASSERT). ArthritisRheum 2005;52:582-91.
88. Rudwaleit M, Listing J, Brandt J, Braun J, Sieper J. Prediction ofa major clinical response (BASDAI 50) to tumour necrosis factoralpha blockers in ankylosing spondylitis. Ann Rheum Dis 2004;63:665-70.
89. Davis JC Jr, Van der Heijde DM, Dougados M, Braun J, CushJJ, Clegg DO, et al. Baseline factors that influence ASAS 20response in patients with ankylosing spondylitis treated withetanercept. J Rheumatol 2005;32:1751-4.
90. Davis JC, van der Heijde DM, Braun J, Dougados M, Cush J,Clegg D, et al. Sustained durability and tolerability of etanerceptin ankylosing spondylitis for 96 weeks. Ann Rheum Dis 2005;64:1557-62.
91. Braun J, Baraliakos X, Brandt J, Listing J, Zink A, Alten R, et al.Persistent clinical response to the anti-TNF-� antibody inflix-imab in patients with ankylosing spondylitis over 3 years. Rheu-
matology (Oxford) 2005;44:670-6.
1
1
1
1
1
M. Mansour et al. 223
92. Baraliakos X, Listing J, Brandt J, Rudwaleit M, Sieper J, Braun J.Clinical response to discontinuation of anti-TNF therapy in pa-tients with ankylosing spondylitis after 3 years of continuoustreatment with infliximab. Arthritis Res Ther 2005;7:R439-44.
93. Brandt J, Listing J, Haibel H, Sorensen H, Schwebig A, Rudwa-leit M, et al. Long-term efficacy and safety of etanercept afterreadministration in patients with active ankylosing spondylitis.Rheumatology (Oxford) 2005;44:342-8.
94. Braun J, Baraliakos X, Golder W, Brandt J, Rudwaleit M, List-ing J, et al. Magnetic resonance imaging examinations of thespine in patients with ankylosing spondylitis, before and aftersuccessful therapy with infliximab: evaluation of a new scoringsystem. Arthritis Rheum 2003;48:1126-36.
95. Braun J, Baraliakos X, Listing J, Sieper J. Decreased incidence ofanterior uveitis in patients with ankylosing spondylitis treatedwith the anti-tumor necrosis factor agents infliximab and etan-ercept. Arthritis Rheum 2005;52:2447-51.
96. Braun J, Davis J, Dougados M, Sieper J, van der Linden S, vander Heijde D. First update of the International ASAS ConsensusStatement for the use of anti-TNF agents in patients with anky-losing spondylitis. Ann Rheum Dis 2005;65:316-20.
97. Carette S, Graham D, Little H, Rubenstein J, Rosen P. Thenatural disease course of ankylosing spondylitis. Arthritis Rheum
1983;26:186-90.98. Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P,Calin A. A new approach to defining disease status in ankylosingspondylitis: the Bath Ankylosing Spondylitis Disease ActivityIndex. J Rheumatol 1994;21:2286-91.
99. Creemers MC, Franssen MJ, van’t Hof MA, Gribnau FW, vande Putte LB, van Riel PL. Assessment of outcome in ankylosingspondylitis: an extended radiographic scoring system. AnnRheum Dis 2005;64:127-9.
00. MacKay K, Mack C, Brophy S, Calin A. The Bath AnkylosingSpondylitis Radiology Index (BASRI): a new, validated approach todisease assessment. Arthritis Rheum 1998;41:2263-70.
01. Doran MF, Brophy S, MacKay K, Taylor G, Calin A. Predictorsof longterm outcome in ankylosing spondylitis. J Rheumatol2003;30:316-20.
02. Braun J, Pincus T. Mortality, course of disease and prognosis ofpatients with ankylosing spondylitis. Clin Exp Rheumatol 2002;20:S16-22.
03. Peters MJ, van der Horst-Bruinsma IE, Dijkmans BA, Nurmo-hamed MT. Cardiovascular risk profile of patients with spondy-larthropathies, particularly ankylosing spondylitis and psoriaticarthritis. Semin Arthritis Rheum 2004;34:585-92.
04. Arnett FC Jr. Ankylosing spondylitis. In: Koopman WJ, ed.Arthritis and Allied Conditions: A Textbook of Rheumatology.14th ed. Philadelphia, Lippincott, Williams, and Wilkins, 2001;
1311-23.










![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://img.pdfslide.us/doc/110x75/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)