Embed Size (px)
Citation preview







The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S1
Supplement
Key Words: ANISA, neonatal, infection, outpatient, etiology
(Pediatr Infect Dis J 2016;35:S1–S2)
Although mortality in children younger than 5 years decreased globally by 39% from 9.9 million in 2000 to 5.9 million in
2015,1 mortality in neonates fell only 32% from 4 million to 2.7 million during the same period of time. As a result, the propor-tion of neonatal deaths in children younger than 5 years increased from 38% to 45%,2 and this has led to an heightened focus on reducing neonatal mortality. Most neonatal deaths continue to be because of 3 major causes: preterm birth, intrapartum com-plications (birth asphyxia) and neonatal sepsis/meningitis/pneu-monia that are also known as possible severe bacterial infections (pSBIs).1 A recent systematic review estimated that the incidence of neonatal infection globally in 2012 was between 5.5 and 8.3 million and the average case fatality rate was 9.8%.3 Interven-tions, such as simplified antibiotic regimens for outpatient-based treatment of neonatal pSBI where timely hospitalization is not feasible,4,5 have the potential to reduce global mortality from pSBI, but there is ever increasing concern about the emergence of antimicrobial resistance in the community and health facili-ties where women are being encouraged to deliver their babies. A recent systematic review and meta-analysis found that resist-ance rates to penicillin and gentamicin versus third-generation cephalosporins were 43% and 44%, respectively,6 meaning that first-line antibiotic regimens for hospitalized neonates (ampicil-lin/penicillin and gentamicin) and simplified regimens for neo-nates (amoxicillin and gentamicin) are potentially already com-promised globally although neonates with pSBI still responded clinically to penicillin/amoxicillin-based and gentamicin-based regimens in outpatients.4,5,7 The majority of the studies contrib-uting to the systematic review/meta-analysis included children taken to hospitals, rather than children with pSBI/neonatal sepsis in the community who may not be taken to hospitals with micro-biologic laboratories.
The diagnosis of neonatal sepsis/pSBI is challenging even in well-equipped tertiary care facilities in resource-rich settings.8,9 In settings where there is limited or no access to microbiologic,
hematologic and biochemical laboratory diagnostic tools, the World Health Organization’s (WHO) Integrated Management of Childhood Illness algorithm is used to make a clinical diagnosis pSBI, which encompasses neonatal sepsis/meningitis/pneumonia.10 However, the symptoms are nonspecific and can vary by language, cultural perspectives and the educational level of those provid-ing information. The algorithm, initially developed after the first WHO Young Infants Study in the 1990s, found 14 clinical signs and symptoms that had a reasonable sensitivity to predict isola-tion of bacteria in blood or cerebrospinal fluid, or culture-positive severe bacterial disease.11 These signs and symptoms were simpli-fied to the presence of any 1 of 7 clinical signs, and symptoms that predicted severe illness (based on an expert pediatrician’s assess-ment) in the second WHO Young Infants Clinical Signs Study.10 However, the signs and symptoms of Young Infants Clinical Signs Study were not evaluated against blood or cerebrospinal fluid cul-ture results, so the diagnosis likely includes respiratory distress associated with preterm birth, birth asphyxia and viral respiratory infections. Based on available data, it is still recommended that neonates with these signs and symptoms be referred to a hospital and treated for pSBI.
So it is clear that diagnosis of pSBI/neonatal sepsis is difficult, and studies based in hospitals may not capture the range of pathogens that cause pSBI/neonatal sepsis in the community. Given the new threats of antimicrobial resistance in the neonates who do present to referral facilities, the Aetiology of Neonatal Infections in South Asia study (ANISA) was initiated in 2010. The study was conceptualized by Child Health Research Foundation and Bill & Melinda Gates Foundation recognizing the urgent need to understand the organ-isms causing neonatal sepsis mortality and to determine appropriate interventions needed to reduce the burden of pSBI/neonatal sepsis. To manage this large initiative, ANISA project leadership at Child Health Research Foundation established a collaborative partnership of multiple organizations including the Centers for Disease Control and Prevention, United States, the WHO, Switzerland, International Centre for Diarrhoeal Disease Research, Bangladesh, University of Toronto, Canada, Oxford University, United Kingdom, and Johns Hopkins University, United States. The project coordination team worked together with the local institutions in Bangladesh, India and Pakistan to establish 5 study sites in South Asia.
In this supplement, the bold and innovative methods to study the etiology of community-based neonatal sepsis are described. ANISA’s strengths include (1) being a community-based study with a centralized data management system supported by Short Message Service for important study-related communi-cations, (2) use of innovative and novel diagnostics, (3) standard-ized approaches to diagnosis of pSBI/neonatal sepsis, training and laboratory-based methods at all sites, (4) monitoring by WHO and Centers for Disease Control and Prevention experts as well as external and internal quality control procedures, state-of-the-art monitoring and quality control through data-based systems and also physical visits by study personnel and external monitors to all sites following standardized check lists and (5) and most importantly use of labeling and tracking systems for processing of samples. Another unique feature of ANISA was the selection of controls using automated Short Message Service to address
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-00S1DOI: 10.1097/INF.0000000000001097
Population-based Novel Molecular Diagnostics to Move the Neonatal Sepsis Agenda Forward
Patricia L. Hibberd, MD, PhD,* and Shamim A. Qazi, MBBS, MSc, MD†
Accepted for publication January 10, 2016. From the *Division of Global Health, Department of Pediatrics, Massachusetts
General Hospital, Boston, Massachusetts; and †Department of Maternal, Newborn, Child and Adolescent Health World Health Organization, Geneva, Switzerland.
The ANISA study is funded by the Bill & Melinda Gates Foundation (grant no. OPPGH5307). The authors have no conflicts of interest to disclose.
Address for correspondence: Patricia L. Hibberd, MD, PhD, Division of Global Health, Department of Pediatrics, Massachusetts General Hospital, 125 Nashua Street Suite 8420, Boston, MA 02114. E-mail: [email protected].

Hibberd and Qazi The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S2 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
the interpretation of novel diagnostics—what would be found in neonates with real infections and what would be found in healthy neonates who did not have any illness. Finally, the ANISA team obtained complete clinical details of the neonates diagnosed with pSBI, their clinical course and outcomes so that it was possible to correlate clinical outcomes with the novel diagnostics and use a rigorous approach to ascertain whether isolated organisms were real pathogens or contaminants.
ANISA focused on South Asia where there is a highest burden of pSBI/neonatal sepsis, but did not have any African site where the burden is also very high. The ANISA sites had low rates of HIV-infected and exposed infants. There is an urgent need for a parallel study in sub-Saharan Africa that leverages the results of ANISA. It is time for the cousin of ANISA–ANISSA (Aetiology of Neonatal Infections in Sub Saharan Africa) with addition of some new innovative approaches to make a difference in neona-tal mortality globally. ANISA and ANISSA have to tell us about antimicrobial resistance patterns to pathogens causing neonatal infections as neonates globally just cannot be left behind.
REFERENCES 1. WHO. Global Health Observatory. Available at: http://www.who.int/gho/
child_health/mortality/causes/en/. Accessed March 15, 2016.
2. Oza S, Lawn JE, Hogan DR, et al. Neonatal cause-of-death estimates for the early and late neonatal periods for 194 countries: 2000-2013. Bull World Health Organ. 2015;93:19–28.
3. Seale AC, Blencowe H, Manu AA, et al; pSBI Investigator Group. Estimates of possible severe bacterial infection in neonates in sub-Saharan Africa,
south Asia, and Latin America for 2012: a systematic review and meta-analysis. Lancet Infect Dis. 2014;14:731–741.
4. Baqui AH, Saha SK, Ahmed AS, et al; Projahnmo Study Group in Bangladesh. Safety and efficacy of alternative antibiotic regimens compared with 7 day injectable procaine benzylpenicillin and gentamicin for outpa-tient treatment of neonates and young infants with clinical signs of severe infection when referral is not possible: a randomised, open-label, equiva-lence trial. Lancet Glob Health. 2015;3:e279–e287.
5. African Neonatal Sepsis Trial (AFRINEST) Group, Tshefu A, Lokangaka A, Ngaima S, et al. Simplified antibiotic regimens compared with inject-able procaine benzylpenicillin plus gentamicin for treatment of neonates and young infants with clinical signs of possible serious bacterial infection when referral is not possible: a randomised, open-label, equivalence trial. Lancet. 2015;385:1767–1776.
6. Downie L, Armiento R, Subhi R, et al. Community-acquired neonatal and infant sepsis in developing countries: efficacy of WHO’s currently recom-mended antibiotics—systematic review and meta-analysis. Arch Dis Child. 2013;98:146–154.
7. Esamai F, Tshefu AK, Ayede AI, et al. Ongoing trials of simplified antibiotic regimens for the treatment of serious infections in young infants in South Asia and sub-Saharan Africa: implications for policy. Pediatr Infect Dis J. 2013;32(suppl 1):S46–S49.
8. Machado JR, Soave DF, da Silva MV, et al. Neonatal sepsis and inflamma-tory mediators. Mediators Inflamm. 2014;2014:269681.
9. Stoll BJ, Bhan MK. New research on community management of severe neo-natal infections: an overview. Pediatr Infect Dis J. 2013;32(suppl 1):S1–S2.
10. Young Infants Clinical Signs Study Group. Clinical signs that predict severe illness in children under age 2 months: a multicentre study. Lancet. 2008;371:135–142.
11. Weber MW, Carlin JB, Gatchalian S, et al; WHO Young Infants Study Group. Predictors of neonatal sepsis in developing countries. Pediatr Infect Dis J. 2003;22:711–717.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S3
Supplement
Each year an estimated 6.9 million neonates require treatment for possible serious bacterial infection (PSBI) in South Asia
and Sub Saharan Africa.1 PSBI leads to more than 600,000 deaths2 the majority of which do not receive appropriate antibiotic treat-ment. There is an additional burden of long-term disability mostly unmeasured.3 Neonatal infections are the second leading infectious cause of death in children under 5 years old (second to pneumonia), with more annual child deaths than HIV and malaria combined.2
The global burden of neonatal infection can be reduced by prevention strategies and increased coverage of timely and appro-priate therapy for newborns with PSBI. Targeted research is needed to address a pipeline from upstream discovery science research to delivery/implementation research on how best to provide known interventions for all in need (Table 1). Research to open the black box of etiology is crucial throughout this process but must be tied to enhanced implementation. Contextual and environmental changes in the places where births occur, evolution of organisms, notably with resistance and host factors will affect strategies to maximize programmatic impact at scale. As more births occur in hospitals, a crucial priority is to improve quality and measurement of facility-based care at birth and care of sick newborns.3 When hospital refer-ral is not possible, treatment with simplified antibiotic regimens initiated at primary clinics is now incorporated into WHO guide-lines,6,7 and scale-up is underway.
Rapid results are possible as learning from implementation research is fed into programs. Upstream research including mater-nal immunization and novel drugs or drug delivery techniques has potential for impact in the medium to long term. Both research advances and programmatic scale up require knowledge of the changing pattern of cause of death, through improved descriptive epidemiology and etiological data to guide the research and action on neonatal infections (Table 1). Almost all studies on the etiology of neonatal infections are from high-income countries, focus on a
single organism (eg, Group B Streptococcus8) and are not popula-tion based, with the majority of published neonatal infection studies to date focused on neonatal intensive care units.9,10
Therefore, the Aetiology of Neonatal Infections in South Asia (ANISA) study is a major accomplishment. The largest ever population-based cohort of ~68,000 newborns, the study includes both sick infants with PSBI and healthy controls. Using a common protocol, the 5 study sites developed strategies for early identifica-tion of births and newborn evaluation within 24 hours, standard-ized techniques for sample collection and processing (cultures and molecular array testing), and systems for data collection and bio-banking of samples.11 The combination of diverse populations and techniques should improve our understanding of etiology beyond a linear single-sample, single-organism model through a richer data-set with relevant contextual and environmental information.
The accompanying article in this supplement describe the approach and methods applied to this enormous logistical under-taking, led by Professor Samir Saha,11 to conduct a study across 3 countries (Bangladesh, India and Pakistan) with over 1000 labo-ratory, clinical, surveillance and data management staff. Inher-ent challenges in such large-scale, multisite etiologic studies are addressed, notably:
1. Capture of cases through population-based surveillance: To fully capture both numerator and denominator is challenging in any age group, but more so at the time of birth since most deaths occur in the first few hours around labor and birth. Hence com-munity-based pregnancy surveillance is required. Yet, achieving contact with the family so soon after birth is not simple, and even in facility settings there is often misclassification between stillbirth and neonatal deaths. In addition, clinical case defi-nition of PSBI is highly sensitive but not specific and may be mixed with preterm birth complications or neonatal encepha-lopathy following peripartum hypoxia. The ANISA sites had to develop and implement a widespread system of identification of pregnancy and outcomes, collection and processing of biologi-cal samples, with many logistical challenges and lessons learned of what worked and which challenges remain.
2. Comparability of laboratory investigations: Quality control and assurance measures, and use and appropriate interpretation of molecular diagnostics to detect pathogens (including viruses) had to be followed. The multiple options that exist and the analy-sis of platform choice are described in this series.
While some questions may be answered by ANISA, the study will also highlight remaining knowledge gaps. No similar study has been conducted in Africa and most global health practitioners recognize that rates of infection and pathogens seen in Africa are likely different from Asian countries, and the difference may be of programmatic relevance. Infectious etiologies of stillbirths are also not addressed by ANISA and existing information remains patchy.12 Moving forward, better understanding of maternal infectious
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-00S3DOI: 10.1097/INF.0000000000001098
Opening the Black Box for Etiology of Neonatal Infections in High Burden Settings
The Contribution of ANISA
Joy E. Lawn, MBBS, FRCPCH, MPH, PhD,*† Janna Patterson, MD, MPH,‡ Mariam Claeson, MD, MPH,‡ Adejumoke Idowu Ayede, MBBS, MSc, FMCPaed, FRCPE,§ and Barbara Stoll, MD¶
Accepted for publication January 10, 2016. From the *Maternal, Adolescent, Reproductive Health (MARCH) Centre,
London School of Hygiene & Tropical Medicine, London, United King-dom; †Saving Newborn Lives, Save the Children, Washington D.C.; ‡Bill & Melinda Gates Foundation, Seattle, Washington; §Department of Paedi-atrics, College of Medicine, University of Ibadan and University College Hospital, Ibadan, Nigeria; and ¶McGovern Medical School, Houston, Texas.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OppGH5307) of which J.P. and M.C. are employees. The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Joy E. Lawn, MBBS, FRCPCH, MPH, PhD, Mater-nal, Adolescent, Reproductive Health (MARCH) Centre, London School of Hygiene & Tropical Medicine, London, United Kingdom. E-mail: [email protected].

Lawn et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S4 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
etiologies, as well as the interplay between infection and death of preterm or small-for-gestational age newborns will be critical to improving our ability to prevent and treat newborn infections.
While research gaps remain large, the investment in neo-natal infection research remains small. Neonatal infectious dis-eases account for an estimated 3% of disability-adjusted life-years. A recent analysis of public and philanthropic infectious disease research awards to UK institutions (1997–2013), assessed the “investment per DALY observed.” Yet neonatal infections received the lowest investment of all infections, £0.01 per DALY.13 By con-trast, HIV and malaria had investments of £0.46 and £0.34 per DALY and some neglected tropical diseases have strikingly high investments—for example, African trypanosomiasis received £9.06 per DALY.13 Increased investment in implementation science to reduce the burden of neonatal infection and infection-related death would likely have a considerable return on investment.
In conclusion, ANISA has been a monumental undertaking. The challenge now is to take what is learned from ANISA to reduce the burden of neonatal infection and infection-related neonatal deaths to investigate, innovate and implement where three-quarters of neonatal infectious deaths occur, in South Asia and sub Saharan Africa. We note great potential in the Child Health and Mortality Prevention Surveillance Network (CHAMPS) which includes sur-veillance of newborn etiology, with sites in these 2 subcontinents applying ANISA-like principles with pregnancy surveillance and etiologic studies, plus the innovation of minimally invasive tissue sampling.14 To maximize the value of these and other investments, ANISA has highlighted how crucial it is to have common standards for early identification of cases, as well as common protocols for newborn evaluation, sample collection and processing and for data collection and reporting. This rigor enables results to be pooled,
and advances our understanding of pathogenesis distinct from colo-nization. Indeed, insights from ANISA have already contributed to an extension of the Reporting of Observational Studies in Epide-miology (STROBE) guidelines15 as specifically applied to neonatal infections and in Strengthening Publications Reporting Infections in Newborns Globally (SPRING). However, while unified report-ing standards and more studies are needed, the burden of neonatal infections and the linked stillbirths and maternal deaths will only be reduced if these data are used locally by public health leaders and program managers, integrated within local healthcare systems, and with full awareness of local culture and customs.
REFERENCES 1. Seale AC, Blencowe H, Manu AA, et al. Estimates of possible severe bac-
terial infection in neonates in sub-Saharan Africa, south Asia, and Latin America for 2012: a systematic review and meta-analysis. Lancet Infect Dis. 2014;14:731–41.
2. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet (London, England). 2015;385:430–440.
3. Moxon SG, Rees-Forman H, Kerber K J, et al. Count every newborn; a measurement improvement roadmap for coverage data. BMC Pregnancy Childbirth. 2015;15 (Suppl 2):S8.
4. Lawn JE, Rudan I, Rubens C. Four million newborn deaths: is the global research agenda evidence-based? Early Hum Dev. 2008;84:809–814.
5. Yoshida S, Rudan I, Lawn JE, et al. Newborn health research priorities beyond 2015. Lancet (London, England). 2014;384: e27–e29.
6. Tshefu A, Lokangaka A, Ngaima S, et al. Oral amoxicillin compared with inject-able procaine benzylpenicillin plus gentamicin for treatment of neonates and young infants with fast breathing when referral is not possible: a randomised, open-label, equivalence trial. Lancet (London, England). 2015;385: 1758–1766.
7. Zaidi AK, Baqui AH, Qazi SA, et al. Scientific rationale for study design of community-based simplified antibiotic therapy trials in newborns
TABLE 1. Research Pipeline of Description, Discovery, Development and Delivery, with a Focus on Reducing the Burden of Infections Around the Time of Birth
Description Discovery Development Delivery
Research aim Descriptive epidemiology and understanding determi-nants and etiology
Discovery of basic sci-ence mechanisms and causes of disease providing foundation for new interventions (eg, new drugs and vaccines)
Developing new or adapting existing interventions to reduce the cost, increase effect, improve deliver-ability
Delivering existing interven-tions in new ways or in new settings (ie, implementation research for scale up in health systems)
Typical timeline before impact is seen (investment level)
Variable (variable) 5 to 15 years (very high) 5 to 10 years (moderate)
2 to 5 years (low to moderate depending on trial size and rigor of evaluation)
Probability of major impact (risk of failure)
Variable, if epidemiology or etiology results lead to programmatic intervention (low)
Variable (high) Moderate (low) Very high if high impact intervention and currently low coverage of care (low and moderate)
Specific examples for infections affecting neonates, stillbirths and mothers
Multiple studies in facility and community settings, with comparable proce-dures and investigations allowing pooling of data
Diagnosis: Novel rapid diagnostics to increase targeting of treatment
Diagnosis: Refin-ing algorithms, adapting technol-ogy, eg, using pulse oximetry.
Prevention: Impact, cost and/or feasibility of preventive care in various contexts, eg, chlorhexidine cord cleansing in facility settings.
Cross-sectional population- based studies (like ANISA) or cohort studies to better delineate infectious expo-sures, and outcomes for neonate, stillbirth, mater-nal and preterm birth/term small for gestational age and define short- and long-term outcomes
Prevention and treat-ment innovations: For example maternal immunizations, or new antimicrobials, particu-larly an effective oral antibiotic for neonatal sepsis
Treatment options: Further simplifica-tions of antibiotics regimes
Treatment systems: Impact, cost and/or feasibility of various models to provide simplified antibiotic regimes in varying health system contexts.
Program monitoring data: Feasible systems to track coverage, compliance, safety, antibiotic resistance etc.
Sources of data: Lawn et al4 and Yoshida et al.5

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Etiology of Neonatal Infections
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S5
and young infants with clinically diagnosed severe infections or fast breathing in South Asia and sub-Saharan Africa. Pediatric Infect Dis J. 2013;32(Suppl 1): S7–S11.
8. Edmond KM, Kortsalioudaki C, Scott S, et al. Group B streptococcal dis-ease in infants aged younger than 3 months: systematic review and meta-analysis. Lancet (London, England). 2012; 379: 547–556.
9. Seale AC, Blencowe H, Zaidi A, et al. Neonatal severe bacterial infection impairment estimates in South Asia, sub-Saharan Africa, and Latin America for 2010. Pediatr Res. 2013;74(Suppl 1): 73–85.
10. Stoll BJ. The global impact of neonatal infection. Clin Perinatol. 1997;24:1–21.
11. Saha SK, Islam MS, Qureshi SM, et al. Laboratory methods for determin-ing etiology of neonatal infection at population-based sites in South Asia: the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S16–S22.
12. Lawn JE, Blencowe H, Waiswa P, et al; for the Lancet Ending Preventable Stillbirths Series study group and the Lancet Stillbirth Epidemiology inves-tigator group. Stillbirths: rates, risk factors, and acceleration towards 2030. Lancet. 2016;387:587–603.
13. Seale AC, Head MG, Fitchett EJA, et al. Neonatal infection: a major burden with minimal funding. Lancet Global Health. 2015;3:e669–e770.
14. Martinez MJ, Massora S, Mandomando I, et al. Infectious cause of death determination using minimally invasive autopsies in developing countries. Diagn Microbiol Infect Dis. 2016;84: 80–86.
15. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guide-lines for reporting observational studies. Int J Surg (London, England). 2014;12:1495–1499.

S6 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
Supplement
The global commitment to reduce child mortality was further augmented in 2000 with the declaration of the millennium
development goals (MDGs). Combined efforts by countries, United Nations organizations, donors, civil society, private sector organi-zations and child health researchers have led to remarkable suc-cess in reducing child mortality worldwide. The number of under-5 deaths has been reduced from 12.7 million in 1990 to 6.3 million in 2013, which translates to 17,000 fewer deaths per day in 2013 compared with 1990. The rate of reduction has accelerated over time: 4.0% per year between 2005 and 2013 compared with 1.2% between 1990 and 1995 (http://www.unicef.org/media/files/Lev-els_and_Trends_in_Child_Mortality_2014.pdf).
However, the story is not as gratifying when achievement is further categorized by region. This is specifically true for South Asia and sub-Saharan Africa. Most of the countries in these regions performed suboptimally, particularly in preventing neonatal deaths, leading to an increased share of under-5 deaths that occur in the newborn period. In South Asia, neonatal deaths accounted for 54% of all under-5 deaths in 2013, a 33% increase from 1990. These fig-ures demonstrate the failure of many countries to achieve MDG4, and challenge our efforts to adhere to global commitments. Saving neonatal lives is not an isolated challenge; it is deeply embedded in the overall reduction of child mortality, the achievement of Sustain-able Development Goal 3 (ensure healthy lives and promote well-being for all at all ages; https://sustainabledevelopment.un.org/topics) and making the “Every Woman Every Child” (http://www.everywomaneverychild.org/) initiative a reality.
In the past decade, there has been copious literature in this field, and we are now clearer about the root causes of most neonatal deaths than we were in 1990. Neonatal deaths are primarily due to prematurity, intrapartum complications, severe infections and con-genital anomalies.1 However, we have yet to delineate the distribu-tion of these specific causes of death, and this remains a roadblock before we can precisely select and prioritize appropriate intervention strategies. Among all the known causes of deaths, severe infections are probably the easiest targets. We have the capacity to prevent and treat them, based on our successes with vaccines (eg, maternal teta-nus toxoid immunization), clean delivery and postpartum newborn
care [eg, thermal care, breastfeeding support, emollient therapy,2 kangaroo mother care (http://www.healthynewbornnetwork.org/topic/kangaroo-mother-care-kmc)] and antibiotic trials.3 However, before treating infections, we need to identify the causative organ-isms (etiology) along with their antibiotic susceptibility pattern, at least in the population concerned if not case-by-case.
To date, the infection slice in the global neonatal mortality pie is based on the existing World Health Organization defini-tion of possible serious bacterial infection (pSBI), which has been adapted to capture cases at the community level. However, clini-cal signs of sepsis among newborns significantly overlap with the signs of other clinical syndromes (eg, asphyxia or prematu-rity). In 2012, an estimated 6.9 million neonates received treat-ment for pSBI worldwide.4 Almost all the treatment, specifically in developing countries, was empirical as there are few data on the etiology of neonatal infections and their antibiotic susceptibil-ity. Furthermore, most of the available South Asian data are from hospital-based studies, where a large proportion of the infections were hospital acquired. The only population-based study from this region was carried out in a small rural population in Bangla-desh.5 Our knowledge about etiology of neonatal infections is still vastly incomplete.
In recent years, there has been notable improvement in microbiology techniques. Blood culture systems have improved significantly with respect to reducing turn-around time for results, and supporting the growth of fastidious organisms in prestandard-ized media. Despite these refinements, blood culture-based etiol-ogy studies which utilize clinical judgment or the World Health Organization clinical algorithm for pSBI show that only 5%–10% of all cases of suspected serious infection are positive for any bacteria.6–10 This strikingly low rate of culture positivity questions the sensitivity of blood culture methods and draws the attention of researchers toward more investigative, modern molecular diag-nostic tools with higher sensitivity for etiology detection. How-ever, state-of-the-art molecular diagnostics are mainly available in well-resourced parts of the world, thus carrying little or no value for the settings where most children die. This situation leads to an information gap that hinders us from formulating definitive policies for treatment and/or prevention. We believe that we can break this barrier; in 2009 we decided to take these technologies where they are needed the most.
A large research initiative, Aetiology of Neonatal Infec-tion in South Asia (ANISA), funded by the Bill & Melinda Gates Foundation, was conceived in 2009 to address questions around infections among newborns and bridge the gap of modern diag-nostics. A multidisciplinary team, representing different organi-zations (Fig. 1), was formed to coordinate a major initiative con-sisting of 5 population-based sites in South Asia (Bangladesh, India and Pakistan). The study team designed a comprehensive plan to address anticipated challenges with surveillance in the field and assays in the laboratory. The ANISA coordination team invited experts from different disciplines and various parts of the world to form a Technical Advisory Group. Together, we designed our final plans and moved to the field and the laboratory bench, simultaneously.
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-00S6DOI: 10.1097/INF.0000000000001099
Aetiology of Neonatal Infection in South Asia (ANISA)
An Initiative to Identify Appropriate Program Priorities to Save Newborns
Samir K. Saha, PhD,* Shams El Arifeen, DrPH,† and Stephanie J. Schrag, DrPhil‡
Accepted for publication January 10, 2016. From the *Child Health Research Foundation, Department of Microbiology,
Dhaka Shishu Hospital, Dhaka, Bangladesh; †Centre for Child and Adoles-cent Health, International Centre for Diarrhoeal Disease Research, Bangla-desh, Dhaka, Bangladesh; and ‡Centers for Disease Control and Prevention, Atlanta, Georgia.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OppGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Samir K. Saha, PhD, Department of Microbiol-ogy, Dhaka Shishu (Children’s) Hospital, Sher-E-Bangla Nagar, Dhaka 1207, Bangladesh. E-mail: [email protected].
(Pediatr Infect Dis J 2016;35:S6–S8)

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Etiology of Neonatal Infections
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S7
In 2008, Baqui et al11,12 conclusively showed that 70% of neonatal deaths in a rural Indian community occurred within the first 7 days after birth. Taking this into consideration, ANISA started its surveillance activities by identifying all married women of reproductive age at each of the 5 sites to reach infants as soon as possible after birth. Visits were continued up to 59 days of life to identify cases of pSBI. The number of visits was carefully crafted to avoid an excessive number that might lead to a Hawthorne effect and influence natural disease progression and outcomes in the com-munity. The team collected multiple specimens from each infant considering the pathophysiology of neonatal sepsis and the pos-sible niche of the target pathogens during the disease process. The specimens were processed by culture (blood) and state-of-the-art molecular diagnostics (blood and respiratory specimens).
ANISA has thus bridged the gap between settings with high child mortality and availability of advanced diagnostics. In addi-tion to an automated blood culture system, the project extended the best available molecular platforms to rural and suburban settings in South Asia, where the rate of neonatal mortality is high. This auto-mated platform of singleplex polymerase chain reaction is capable of detecting a large number of diverse etiologies (bacteria and virus) and has minimal possibility of being affected by human error.13
In addition to placing advanced technologies at each site, innovation touched each and every segment of ANISA—starting from data form design to data management through control selec-tion, harmonization of study procedures across the sites, speci-men transportation and tracking, prevention of contamination, etc. This supplement contains the details of all methods applied for ANISA implementation and management. The success of ANISA is ensured through these novel approaches. We believe that these method papers and description of challenges at individual sites will be useful for future researchers working on etiology of infections in any age group and location.
With ambitious planning, management and implementa-tion, ANISA has collected comprehensive and high-quality data on etiology of newborn infections. These data from a large cohort of ~68 000 newborns will significantly improve our understanding of the causes and epidemiology of neonatal infections in South Asian infants. Data generated by ANISA, along with those from other contemporary antibiotic treatment trials, will have a signifi-cant impact on the rational use of antibiotics. Thus, the study will contribute to restricting the emergence of antimicrobial resistance, another public health priority of the World Health Organization and global leaders of multiple disciplines. Altogether, ANISA results will facilitate evidence-based programmatic decisions which will reduce deaths and improve the well-being of newborns and age groups beyond.
REFERENCES 1. Liu L, Oza S, Hogan D, et al. Global, regional, and national causes of child
mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385:430–440.
2. Darmstadt GL, Bhutta ZA, Cousens S, et al. Evidence-based, cost-effective interventions: how many newborn babies can we save? Lancet. 2005;365:977–988.
3. Baqui AH, Saha SK, Ahmed AS, et al. Safety and efficacy of alternative antibiotic regimens compared with 7 day injectable procaine benzylpeni-cillin and gentamicin for outpatient treatment of neonates and young infants with clinical signs of severe infection when referral is not pos-sible: a randomised, open-label, equivalence trial. Lancet Glob Health. 2015;3:e279–287.
4. Seale AC, Blencowe H, Manu AA, et al. Estimates of possible severe bac-terial infection in neonates in sub-Saharan Africa, south Asia, and Latin America for 2012: a systematic review and meta-analysis. Lancet Infect Dis. 2014;14:731–741.
5. Darmstadt GL, Saha SK, Choi Y, et al. Population-based incidence and etiol-ogy of community-acquired neonatal bacteremia in Mirzapur, Bangladesh: an observational study. J Infect Dis. 2009;200:906–915.
FIGURE 1. ANISA collaboration and partnership.

Saha et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S8 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
6. The WHO Young Infants Study Group. Bacterial etiology of serious infec-tions in young infants in developing countries: results of a multicenter study. Pediatr Infect Dis J. 1999;18(10 Suppl):S17–S22.
7. Hamer DH, Darmstadt GL, Carlin JB, et al. Etiology of bacteremia in young infants in six countries. Pediatr Infect Dis J. 2015;34:e1–8.
8. Farzin A, Saha SK, Baqui AH, et al. Population-based incidence and eti-ology of community-acquired neonatal viral infections in Bangladesh: a community-based and hospital-based surveillance study. Pediatr Infect Dis J. 2015;34:706–711.
9. Blackburn RM, Muller-Pebody B, Planche T, et al. Neonatal sepsis–many blood samples, few positive cultures: implications for improving anti-biotic prescribing. Arch Dis Child Fetal Neonatal Ed. 2012;97:F487–F488.
10. Fjalstad JW, Stensvold HJ, Bergseng H, et al. Early-onset sepsis and anti-biotic exposure in term infants: a nationwide population-based study in Norway. Pediatr Infect Dis J. 2016;35:1–6.
11. Baqui AH, Darmstadt GL, Williams EK, et al. Rates, timing and causes of neonatal deaths in rural India: implications for neonatal health programmes. Bull World Health Organ. 2006;84:706–713.
12. Baqui AH, El-Arifeen S, Darmstadt GL, et al. Effect of community-based newborn-care intervention package implemented through two service-deliv-ery strategies in Sylhet district, Bangladesh: a cluster-randomised controlled trial. Lancet. 2008;371:1936–1944.
13. Diaz MH, Waller JL, Napoliello RA, et al. Optimization of multiple patho-gen detection using the TaqMan array card: application for a population-based study of neonatal infection. PLoS One. 2013;8:e66183.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S9
Supplement
Background: Insufficient knowledge of the etiology and risk factors for community-acquired neonatal infection in low-income countries is a bar-rier to designing appropriate intervention strategies for these settings to reduce the burden and treatment of young infant infection. To address these gaps, we are conducting the Aetiology of Neonatal Infection in South Asia (ANISA) study among young infants in Bangladesh, India and Pakistan. The objectives of ANISA are to establish a comprehensive surveillance system for registering newborns in study catchment areas and collecting data on bacterial and viral etiology and associated risk factors for infections among young infants aged 0–59 days.Methods: We are conducting active surveillance in 1 peri-urban and 4 rural communities. During 2 years of surveillance, we expect to enroll an esti-mated 66,000 newborns within 7 days of their birth and to follow-up them until 59 days of age. Community health workers visit each young infant in the study area 3 times in the first week of life and once a week thereafter. During these visits, community health workers assess the newborns using a clinical algorithm and refer young infants with signs of suspected infection to health care facilities where study physicians reassess them and provide care if needed. On physician confirmation of suspected infection, blood and respiratory specimens are collected and tested to identify the etiologic agent.
Conclusions: ANISA is one of the largest initiatives ever undertaken to understand the etiology of young infant infection in low-income countries. The data generated from this surveillance will help guide evidence-based decision making to improve health care in similar settings.
Key Words: community-acquired, neonatal, infection, etiology, surveillance, ANISA
(Pediatr Infect Dis J 2016;35:S9–S15)
Neonatal deaths account for almost 44% of global under-5 child deaths.1 Three South Asian countries (Bangladesh, India
and Pakistan) account for more than one third of all global neo-natal deaths, the majority of which occur at home.2–6 The World Health Organization (WHO) estimates that 26% of these deaths are because of infection.7 Neonatal mortality rates differ across set-tings and are higher where the neonatal infection rate is very high.3,8 Inherent difficulties in collecting and processing specimens from young infants are one of the main barriers to understanding the etiology of infections in neonates in low-income countries. Current evidence on neonatal infection etiology is based on the predomi-nantly hospital-based studies that identified bacterial pathogens by blood culture from only 5%–10% of neonates with suspected seri-ous infection.9–12 Limited knowledge in this area is a major impedi-ment to designing effective programs for successful prevention and management of neonatal infections.13 We are conducting the Aetiology of Neonatal Infection in South Asia (ANISA) study at 5 population-based sites in Bangladesh, India and Pakistan to pro-vide information on incidence, etiology and risk factors for com-munity-acquired neonatal infections. This study also enrolls young infants aged 28–59 days as they have a high risk of infection.14–16 We instituted pregnancy and birth surveillance to capture births in the catchment areas and record young infant infections. This article describes various aspects of the pregnancy and infection surveil-lance activities carried out at ANISA study sites.
PROJECT GOAL AND OBJECTIVESThe goal of the ANISA study is to provide data to design
appropriate treatment regimens and strategies for reducing serious bacterial and viral infections in young infants. The study has 4 pri-mary objectives: (1) to establish community-based surveillance to identify cases of possible serious bacterial infection among infants aged 0–59 days and collect specimens for etiologic evaluation; (2) to determine community-acquired etiology-specific incidence of bacterial and viral infections among infants by using standard and molecular diagnostic tools; (3) to identify the risk factors for
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-00S9DOI: 10.1097/INF.0000000000001100
Infection Surveillance Protocol for a Multicountry Population-based Study in South Asia to Determine the Incidence, Etiology and Risk Factors for Infections Among
Young Infants of 0 to 59 Days OldMohammad Shahidul Islam, MSc,* Abdullah H. Baqui, DrPh,† Anita K. Zaidi, SM,‡ Zulfiqar A. Bhutta, PhD,‡
Pinaki Panigrahi, PhD,§ Anuradha Bose, MD,¶ Sajid B. Soofi, FCPS,‡ Abdul Momin Kazi, MPH,‡ Dipak K. Mitra, PhD,† Rita Isaac, MD,¶ Pritish Nanda, MPH,║ Nicholas E. Connor, MSc,** Daniel E. Roth, PhD,††
Shamim A. Qazi, PhD,‡‡ Shams El Arifeen, DrPh,** and Samir K. Saha, PhD,* for the ANISA Methods Group
Accepted for publication January 10, 2016.From the *Department of Microbiology, Child Health Research Foundation,
Dhaka, Bangladesh; †Department of International Health, Johns Hopkins University, Baltimore, Maryland; ‡Department of Pediatrics and Child Health, The Aga Khan University, Karachi, Pakistan; §Department of Epidemiology and Pediatrics, University of Nebraska Medical Center, Omaha, Nebraska; ¶Department of Community Health, Christian Medical College, Vellore, India; ║Asian Institute of Public Health, Bhubaneswar, Odisha, India; **Centre for Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh; ††Department of Paediatrics, Hospital for Sick Children, Ontario, Canada; and ‡‡Department of Child and Adolescent Health and Development, World Health Organization, Geneva, Switzerland.
S.K.S., S.E.A., S.A.Q., A.H.B., A.K.Z., Z.A.B. and D.E.R. were involved in study design. M.S.I., N.E.C. and S.B.S. were involved in protocol develop-ment. A. M.K., D.K.M. and P.N. were involved in protocol implementation. A.H.B., P.P., A.B., A.K.Z. and Z.A.B. are the co-investigators of the project. S.K.S., S.E.A., A.H.B. and M.S.I. drafted the manuscript. All authors have reviewed and edited subsequent drafts.
The ANISA study is funded by the Bill & Melinda Gates Foundation (grant no. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Mohammad Shahidul Islam, MSc, Child Health Research Foundation, ANISA Project, Department of Microbiology, Dhaka Shishu (Children’s) Hospital, Sher-e-Bangla Nagar, Dhaka 1207, Bangla-desh. E-mail: [email protected].

Islam et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S10 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
community-acquired serious bacterial and viral infections in young infants and (4) to identify clinical features predictive of invasive viral and bacterial infections among ill-appearing young infants in the community.
STUDY DURATION AND TIMELINEWe intend to collect data in a similar manner at all study
sites to minimize reporting bias and allow pooled analysis. This requires developing the protocol and standard operating proce-dures, designing data collection forms, recruiting and training staff and arranging study logistics in a standardized manner, as well as harmonizing the processes across the field sites, study hospitals and site laboratories. Each site has gone through a pilot phase to adapt the protocol to its particular setting. The duration of this phase for individual sites varied based on the achievement of benchmark targets set at the beginning of the project.17 Once a site achieved these targets, it started enrolling study participants in the main study. At least 2 years of surveil-lance time has been scheduled for each site. We believe that this duration will permit us to understand the impact of sea-sonal variation on the types of pathogens isolated from enrolled cases. As different study sites have ended their pilot phases at different times, the start date of the main study varies by site. Start and end dates of surveillance activities at ANISA study sites are listed in Table 1.
ANISA STUDY SITESCollecting specimens from neonates at the community
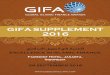
level is difficult in South Asia because caregivers are not able to bring their newborns to health care facilities given a variety of sociocultural barriers.18 We selected 5 sites where the investiga-tors had good records of working in the communities and had a thorough understanding of the local cultures in the expectation that these existing relationships would encourage caregivers to overcome barriers and bring their newborns to health care facili-ties for assessment, care and specimen collection. Among the sites, 4 are rural communities and 1 is peri-urban (Fig. 1). All the study sites have recently completed a population census, which provides baseline data on neonatal mortality rates. The sites also possess adequate laboratory facilities for performing microbio-logical and molecular analysis of clinical specimens. The notable features and expected number of clinical specimens to be col-lected at each site are listed in Table 2.
COMMUNITY-BASED ACTIVE SURVEILLANCE FOR INFECTION IN NEWBORNS
Community-based active surveillance for infection cases includes (1) registering married women of reproductive age (MWRA) in the target communities; (2) identifying pregnan-cies; (3) identifying live births as soon as possible after delivery; (4) identifying suspected infections among young infants in the community; (5) referring cases of suspected infection to study hospitals and (6) enrolling healthy controls. A group of project staff performs each activity. The key components of ANISA sur-veillance and laboratory activities are depicted in Table 3. To harmonize the study protocol across sites and train project staff in a similar manner, a 2-stage training program was conducted. In the first stage, experts from WHO trained supervisory staff from the sites and provided them with training guides, videos and booklets. These trained personnel then trained community health workers (CHWs) from their respective sites for 15–21 days, with the length depending on the experience of the CHWs, local pro-cedures and capacity.19,20
TABLE 1. Site-specific Enrollment Period of Each Study Site (Infants Born Within These Dates)
Country SiteEnrollment Start Date
Enrollment End Date
Bangladesh Sylhet November 1, 2011 December 31, 2013India Vellore September 1, 2013 February 28, 2015
Odisha September 1, 2013 February 28, 2015Pakistan Karachi January 1, 2012 December 31, 2013
Matiari March 1, 2012 December 31, 2013
FIGURE 1. Geographic location of 5 ANISA study sites.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Infection Surveillance
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S11
REGISTERING MARRIED WOMEN AND PREGNANCY SURVEILLANCE
The study area of each site is subdivided into clusters and blocks. One CHW is responsible for conducting surveillance in a particular area (1–3 blocks). A CHW makes bimonthly household visits to identify and register MWRA (13–49 years) in her area for the study. Unmarried women are excluded, as the possibility of finding a premarital pregnancy is remote given the cultural settings of the study sites. During MWRA surveillance, CHWs maintain individual planners for making household visits in each block and visit every house at least once every 2 months. During the visits, CHWs ask MWRAs for the date of their last menstrual period. An MWRA is considered to be pregnant if 2 months have passed since her last menstrual period.21,22 Pregnant women who provide verbal consent for themselves and their newborns for participation in the study are registered and tracked until their deliveries take place. Figure 2 shows the pregnancy and birth surveillance scheme of the ANISA study.
FOLLOW-UP OF PREGNANT WOMENOnce a CHW identifies a pregnancy, she places the preg-
nant woman on a roster and schedules 2 visits to that household
during the pregnancy. The first visit is immediately after preg-nancy identification, during which the CHW counsels the preg-nant woman about the importance of seeking routine antenatal care from a trained health worker. The CHW also collects demo-graphic, educational and previous pregnancy-related information about the woman and her family members to determine the risk factors for young infant infections. The CHW conducts the sec-ond antenatal visit in the 29th week of pregnancy, during which she provides information to the pregnant woman and her family members related to the health care of mothers and neonates. These visits help a CHW build rapport with families, which in turn helps early notification of births to the CHW and referral compliance if she suspects infection in a young infant under observation. The CHW provides her mobile phone number to family members so that they can inform her about the delivery. Study site personnel reimburse mobile phone call costs to the family to encourage early birth notification. The CHW also phones the family every other day starting in the 37th week of pregnancy to inquire whether the mother has delivered.
ANISA sites hire CHWs locally, so that they are familiar with traditional and other skilled birth attendants in the surveillance area and maintain contact with them to increase the likelihood of early birth notification.
TABLE 2. General Characteristics of ANISA Study Sites*
Category Sylhet, Bangladesh Karachi, Pakistan Matiari, Pakistan Odisha, India Vellore, India
Community setting Rural Peri-urban Rural Rural RuralSite principal investigator Abdullah H. Baqui Anita K. Zaidi Zulfiqar A. Bhutta Pinaki Panigrahi Anuradha BosePopulation 340,000 270,000 400,000 360,000 250,000Yearly birth cohort 10,000 8000 7500 4500 4000Expected number of neonatal infections
per year (10% of all neonates)1000 800 750 450 400
Expected number of blood and respiratory specimens (80%) per year
800 640 600 360 320
*Source: Demographic and health surveillance data from sites.
TABLE 3. Key Components of ANISA Surveillance and Laboratory Activities
Activities Objective By Whom Where How
MWRA registration Identifying and enrolling pregnant women, building rapport with community
CHWs Community level Visiting each household once every 2 mo
Pregnant women enrollment
Enhancing rapport with pregnant mothers and their family members, timely birth notification
CHWs Community level Recording LMP of all regis-tered women and following up until delivery
Birth notification Reaching babies as soon as birth takes place
Family members, CHWs, TBAs
Community level Scheduled visits, phone call, personal contact
Newborn assessment Identifying cases with pSBI CHW At neonate’s residence Using WHO-Young infant- IMCI guideline
Referral to health facilities Case management and specimens collection
CHW At neonate’s residence CHW accompanied neonates to health facility
Application of standard case definition for “suspected infection”
Identification of newborns with pSBI and their enrollment into ANISA
Study physician Health care facility Standardized physician assessment
Obtain consent for specimen collection
Human subjects protection- ensure agreement to speci-men collection is informed and voluntary
Study physician Study site health care facility
Using IRB stamped form
Specimen collection Following standard operating procedures
Phlebotomist/nurse/study physician
Study site health care facility/hospital/at neonate’s residence (only in Matiari)
Following good clinical practice
IMCI indicates Integrated Management of Childhood Illness; IRB, institutional review board; LMP, last menstrual period; pSBI, possible serious bacterial infection; TBA, tradi-tional birth attendant.

Islam et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S12 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
NEWBORN REGISTRATION IN THE STUDYThe ANISA study tries to identify and register each new-
born in the study area as soon as possible after birth to capture early neonatal infection cases. However, a CHW can register a newborn in the study up to 7 days after birth. At the time of reg-istration, the CHW administers 2 separate sets of questionnaires for recording the newborn’s health status and delivery history to capture the most likely risk factors for neonatal infection. We have described the detailed questionnaires elsewhere in this sup-plement. A CHW also makes a visit plan to keep the newborn under continuous follow-up until the age of 59 days.
IDENTIFYING SUSPECTED INFECTION CASESANISA is using CHWs to identify suspected infection
cases because previous studies have shown that trained CHWs can effectively identify suspected neonatal sepsis cases among young infants in a community setting using Integrated Man-agement of Childhood Illness guidelines.8,23,24 We designed the pregnancy and suspected infection surveillance to minimize the impact of a CHW’s visit on the natural burden of infection and yet capture all the suspected infection cases. CHWs visit each newborn on days 0, 2, 6, 13, 20, 27, 34, 41, 48 and 59. During these visits, they assess the newborns based on the clinical vari-ables listed in Table 4.
SUSPECTED INFECTION CASE REFERRALIf a CHW finds any of the signs from Table 4 in a newborn
during follow-up visits, she refers the newborn to a study-desig-nated health care facility. Whenever necessary, a CHW accompa-nies the mother and newborn to the facility. The CHW visits that household again the next day to reinforce referral if the family
members have not complied. In the health care facility, a study physician reexamines the newborn to confirm the presence of any sign of infection. In Matiari, Pakistan, there is no study-desig-nated health care facility for ANISA, so study physicians work
FIGURE 2. ANISA pregnancy and birth surveillance system. ANC indicates antenatal care; LMP, last menstrual period; pSBI, possible serious bacterial infection.
TABLE 4. Clinical Signs Assessed by CHWs During Young Infant Follow-up Visits
Severe chest in-drawingRespiratory rateConvulsionsAbnormal axillary temperature (<35.5°C or ≥38.0°C)Poor feedingLevel of consciousness and movement of the babySkin pustulesJaundiceUmbilicus red or discharging pusOther signs of infection
TABLE 5. ANISA Case Enrollment Criteria
Eligibility criteria History of not feeding well, confirmed by feeding assessment Fast breathing (respiratory rate ≥60/min on repeat count) Severe chest in-drawing Axillary temperature ≥38.0°C (≥100.4°F) or <35.5°C (<95.9°F) Movement only when stimulated or no movement at all. History of or observed convulsionExclusion criteria Infant hospitalized for 1 or more nights in the preceding 7 days
(except for postnatal hospital stays of facility-born neonates) Infant previously enrolled in the ANISA study with an episode
of suspected serious infection in the preceding 7 days

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Infection Surveillance
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S13
with CHWs as mobile teams and reassess newborns with sign(s) of suspected infection.
CASE ENROLLMENTA young infant is deemed eligible for enrollment as a case
of suspected infection if a study physician identifies any 1 of the 7 signs listed in Table 5 and none of the exclusion criteria (Table 5) are met. The exclusion criteria are intended to ensure
that the case is not nosocomial in nature and that each reported episode is an isolated event.25 The study team requests the fam-ily’s consent for blood and nasopharyngeal-oropharyngeal swab specimen collection from the enrolled newborn. The team also aims to collect cerebrospinal fluid in suspected cases of meningi-tis (patients with history of irritability, convulsions, high-pitched cry and full, bulging anterior fontanelle) if the family provides written consent.26 A flow diagram of the newborn registration,
FIGURE 3. Neonatal infection surveillance and case enrollment system conducted by CHWs and study physicians. CSF indicates cerebrospinal fluid; EDD, expected date of delivery; LMP, last menstrual period; NP-OP, nasopharyngeal-oropharyngeal; PCR, polymerase china reaction; pSBI, possible serious bacterial infection.

Islam et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S14 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
follow-up visits, case enrollments and specimen collections are shown in Figure 3.
PASSIVE SURVEILLANCE FOR INFECTION CASESAs CHWs visit the young infants on a fixed schedule, there
is a possibility of missing some infection cases between visits. To capture those cases, CHWs teach household members how to identify signs of infection in a young infant (Table 4) and requests family members to take the infant to a study-designated health care facility if they observe any of these signs. In the study-des-ignated hospitals, a study physician and other study staff assess a self-referred newborn for signs of infection and enroll the infant in ANISA if he/she meets the enrollment criteria (Table 5).
SAFETY CONSIDERATIONSMothers and other family members are encouraged to hos-
pitalize their ill-appearing newborns so that a study physician can confirm any of the 7 clinical signs of suspected infection. The hos-pital manages the admitted young infants according to the hospital policy. If caregivers refuse to hospitalize their sick young infants, study physicians provide standard outpatient care for the illness. A combination of penicillin and aminoglycoside (penicillin/ampi-cillin and gentamicin) is typically used to treat suspected infec-tion.2,27–31 For meningitis, a third-generation cephalosporin (cef-triaxone/cefotaxime) is used with or without an aminoglycoside. The results of blood and cerebrospinal fluid cultures are provided to treating physicians.
VERBAL AUTOPSYSupervisory staff members conduct a complete verbal
autopsy for each young infant who dies within the follow-up period (0–59 days),32–37 using validated WHO Verbal Autopsy Forms.37 Two physicians then independently review the completed forms. If the physicians do not concur, a third physician reviews the informa-tion and makes a conclusion on the cause of death.
ETHICAL CONSIDERATIONSConsent is requested from parents or caregivers at 2 points.
Informed verbal consent is taken at the time of registering a preg-nant woman in the study. Informed written consent is requested at the time of collecting specimens from a sick young infant with suspected infection. We obtained ethical clearance for the study from the ethical review committees or internal review boards of all the organizations involved in this study, and they have reviewed and approved the study protocol and consent and data collection forms. These organizations include the Bangladesh Institute of Child Health, WHO, Johns Hopkins Bloomberg School of Public Health, Aga Khan University, International Centre for Diarrhoeal Disease Research, Bangladesh, Christian Medical College and the Asian Institute of Public Health.
SUMMARYThe ANISA infection surveillance protocol is designed to
capture the population-based incidence, etiology and risk factors for community-acquired neonatal infections in South Asia. We expect that through this study we will able to report the etiology of young infant infections in South Asia to guide the future treat-ment policy for this group and help to develop strategies to reduce the burden of young infant infections across the world. We believe that the methodology described in this article will also be useful to design future population-based studies in resource-poor areas.
ACKNOWLEDGMENTSThe authors thank the experts who provided their valuable
thoughts in designing this protocol, the families who participated in this study and the project staff who are contributed their time, experience and hard work to make the study successful.
ANISA Methods Group: A. S. M. Nawshad Uddin Ahmed, FCPS, Belal Hossian, MSc, Maksuda Islam, BA, Tanvir Hossain, MSc, Qazi Sadeq-ur Rahman, MSc, Maureen Helen Diaz, PhD, Jonas Winchell, PhD, Nong Shang, PhD, Derrick Crook, MRCP, Vishawjeet Kumar, MPH, Aarti Kumar, MS, Stephen P. Luby, MD, Luke Mullany, PhD, Mathuram Santosham, MD, Yoonjoung Choi, PhD, Shahida M Qureshi, MSc, Imran Ahmed, MSc, Sheraz Ahmed, MBBS, Arif Mahmud, MBBS, Nazma Begum, MA, and Stephanie J. Schrag, DPhil.
REFERENCES 1. Darmstadt GL, Marchant T, Claeson M, et al. A strategy for reducing maternal and
newborn deaths by 2015 and beyond. BMC Pregnancy Childbirth. 2013;13:216.
2. Osrin D, Vergnano S, Costello A. Serious bacterial infections in newborn infants in developing countries. Curr Opin Infect Dis. 2004;17:217–224.
3. Lawn JE, Cousens S, Zupan J; Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: when? Where? Why? Lancet. 2005;365:891–900.
4. Baqui AH, Darmstadt GL, Williams EK, et al. Rates, timing and causes of neonatal deaths in rural India: implications for neonatal health programmes. Bull World Health Organ. 2006;84:706–713.
5. Baqui AH, El-Arifeen S, Darmstadt GL, et al; Projahnmo Study Group. Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: a clus-ter-randomised controlled trial. Lancet. 2008;371:1936–1944.
6. Ahmad OB, Lopez AD, Inoue M. The decline in child mortality: a reap-praisal. Bull World Health Organ. 2000;78:1175–1191.
7. World Health Organization. World Health Report 2005: Make Every Mother and Child Count. Geneva: World Health Organization; 2005.
8. Baqui AH, Arifeen SE, Williams EK, et al. Effectiveness of home-based management of newborn infections by community health workers in rural Bangladesh. Pediatr Infect Dis J. 2009;28:304–310.
9. Darmstadt GL, Zaidi AK, Stoll BJ. Neonatal infections: a global perspective. In: Remington JOK, Wilson CB, Nizet V, et al, eds. Infectious Diseases of the Fetus and Newborn Infant. 7th ed. Philadelphia, PA: Saunder/Elsevier; 2011:24–51.
10. Zaidi AK, Huskins WC, Thaver D, et al. Hospital-acquired neonatal infec-tions in developing countries. Lancet. 2005;365:1175–1188.
11. Zaidi AK, Thaver D, Ali SA, et al. Pathogens associated with sepsis in newborns and young infants in developing countries. Pediatr Infect Dis J. 2009;28(1 suppl):S10–S18.
12. Newton O, English M. Young infant sepsis: aetiology, antibiotic susceptibil-ity and clinical signs. Trans R Soc Trop Med Hyg. 2007;101:959–966.
13. Berkley JA, Maitland K, Mwangi I, et al. Use of clinical syndromes to tar-get antibiotic prescribing in seriously ill children in malaria endemic area: observational study. BMJ. 2005;330:995.
14. Byington CL, Enriquez FR, Hoff C, et al. Serious bacterial infections in febrile infants 1 to 90 days old with and without viral infections. Pediatrics. 2004;113:1662–1666.
15. Krief WI, Levine DA, Platt SL, et al; Multicenter RSV-SBI Study Group of the Pediatric Emergency Medicine Collaborative Research Committee of the American Academy of Pediatrics. Influenza virus infection and the risk of seri-ous bacterial infections in young febrile infants. Pediatrics. 2009;124:30–39.
16. Biondi E, Evans R, Mischler M, et al. Epidemiology of bacteremia in febrile infants in the United States. Pediatrics. 2013;132:990–996.
17. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35 (Suppl 1):S39–S44.
18. Syed U, Khadka N, Khan A, et al. Care-seeking practices in South Asia: using formative research to design program interventions to save newborn lives. J Perinatol. 2008;28 (suppl 2):S9–S13.
19. Bryce J, Boschi-Pinto C, Shibuya K, et al; WHO Child Health Epidemiology Reference Group. WHO estimates of the causes of death in children. Lancet. 2005;365:1147–1152.
20. World Health Organization, UNICEF. Handbook—Integrated Management of Childhood Illness (IMCI). Geneva: WHO; 2005.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Infection Surveillance
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S15
21. Darmstadt GL, Saha SK, Choi Y, et al; Bangladesh Projahnmo-2 (Mirzapur) Study Group. Population-based incidence and etiology of community-acquired neonatal bacteremia in Mirzapur, Bangladesh: an observational study. J Infect Dis. 2009;200:906–915.
22. Rosenberg RE, Ahmed AS, Ahmed S, et al. Determining gestational age in a low-resource setting: validity of last menstrual period. J Health Popul Nutr. 2009;27:332–338.
23. Baqui AH, Arifeen SE, Rosen HE, et al; Projahnmo Study Group. Community-based validation of assessment of newborn illnesses by trained community health workers in Sylhet district of Bangladesh. Trop Med Int Health. 2009;14:1448–1456.
24. Baqui AH, Ahmed S, El Arifeen S, et al; Projahnmo 1 Study Group. Effect of timing of first postnatal care home visit on neonatal mortality in Bangladesh: a observational cohort study. BMJ. 2009;339:b2826.
25. Darmstadt GL, Saha SK, Ahmed AS, et al. Effect of topical treatment with skin barrier-enhancing emollients on nosocomial infections in preterm infants in Bangladesh: a randomised controlled trial. Lancet. 2005;365:1039–1045.
26. Curtis S, Stobart K, Vandermeer B, et al. Clinical features suggestive of meningitis in children: a systematic review of prospective data. Pediatrics. 2010;126:952–960.
27. Laving AM, Musoke RN, Wasunna AO, et al. Neonatal bacterial menin-gitis at the newborn unit of Kenyatta National Hospital. East Afr Med J. 2003;80:456–462.
28. Bacterial etiology of serious infections in young infants in developing coun-tries: results of a multicenter study. The WHO Young Infants Study Group. Pediatr Infect Dis J. 1999;18:S17–S22.
29. Darmstadt GL, Hossain MM, Jana AK, et al. Determination of extended-interval gentamicin dosing for neonatal patients in developing countries. Pediatr Infect Dis J. 2007;26:501–507.
30. Bang AT, Bang RA, Baitule SB, et al. Effect of home-based neonatal care and management of sepsis on neonatal mortality: field trial in rural India. Lancet. 1999;354:1955–1961.
31. Fortney JA, Susanti I, Gadalla S, et al. Reproductive mortality in two devel-oping countries. Am J Public Health. 1986;76:134–138.
32. Garenne M, Fontaine O. Assessing probable causes of death using a stand-ardized questionnaire: a study in rural Senegal. Bull World Health Organ. 2006;84:248–253.
33. Gray RH, Smith G, Barss P. The Use of Verbal Autopsy to Determine Selected Causes of Death in Children. Baltimore, MD: The Johns Hopkins University School of Hygiene and Public Health; 1990.
34. Bang AT, Bang RA. Diagnosis of causes of childhood deaths in developing countries by verbal autopsy: suggested criteria. The SEARCH Team. Bull World Health Organ. 1992;70:499–507.
35. Ross DA. Monitoring Cause-specific Infant and Child Mortality Rates in Areas Where Death Certification Systems Are Weak. Geneva: World Health Organization; 1992.
36. Snow B, Marsh K. How useful are verbal autopsies to estimate childhood causes of death? Health Policy Plan. 1992;7:22–29.
37. Anker M, Black RE, Coldham C, et al. A Standard Verbal Autopsy Method for Investigating Causes of Death in Infants and Young Children. Geneva: World Health Organization; 1999.

S16 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
Supplement
Background: The Aetiology of Neonatal Infection in South Asia (ANISA) study aims to determine the etiology of neonatal infections in 5 population-based sites in Bangladesh, India and Pakistan.Methods: The main laboratory challenges in ANISA were selection and consistent implementation of laboratory methods at participating sites with varied infrastructure. The other specific challenges included (1) specimen collection and transport to designated study laboratories and timely processing in rural settings; (2) minimal or nonexistent lab-oratory facilities at the field sites; (3) obtaining sufficient volumes of blood from enrolled infants aged 0–59 days and (4) caregivers’ concerns about collection of clinical specimens from young infants. An additional challenge was selecting an appropriate molecular platform from multiple available options, all with limited field validation, for use in determining infection in young infants.Conclusions: This article describes how the challenges of specimen col-lection, transport and processing and implementation of laboratory meth-ods have been addressed in the ANISA study. It also describes the meas-ures taken to improve detection of microorganisms causing young infant infections by enhancing the sensitivity of existing laboratory methods for pathogen detection.
Key Words: ANISA, etiology, neonatal, sepsis, blood culture, molecular diagnostics
(Pediatr Infect Dis J 2016;35:S16–S22)
Although one third of global neonatal deaths occur in Bang-ladesh, India and Pakistan,1 little is known about the etiol-
ogy of community-acquired neonatal infections in South Asia. Most previous studies in this region have focused on hospitalized
patients and thus included nosocomial infections. The limited available data on community-acquired infections are mainly from outpatient-based clinical studies with limited etiologic charac-terization.2,3 Finally, the few available population-based studies reporting etiology of neonatal infections have relied solely on bacterial culture for diagnostic evaluation despite significant advances in laboratory diagnostics.4,5
Data on etiology of community-acquired neonatal sepsis in South Asia are scarce,5 which is not surprising considering the numerous challenges in performing an etiology study with new-borns in this region. Specific challenges may hinder the investiga-tion of neonatal infections, including (1) lack of laboratory infra-structure and modern diagnostics; (2) reaching infants at home where most births take place; (3) collection of blood from newborns and (4) timely and temperature-controlled specimen transport from remote settings. The Aetiology of Neonatal Infection in South Asia (ANISA) project is a comprehensive population-based study to better understand the etiologies of infection in young infants up to 2 months of age at 5 sites in Bangladesh, India and Pakistan. The approaches and solutions to overcome specific challenges identified in the ANISA study can be extrapolated to other large-scale studies of newborns in similar communities.
In this article, we describe the laboratory methods of ANISA, including the rationale for molecular platform selection and the associated challenges of implementing this testing in dif-ficult field settings. We also discuss measures taken to improve the detection of a wide range of bacteria and viruses through molecular testing of blood and respiratory specimens along with the comple-mentary traditional culture methods employed.
SPECIMENS FOR DETECTING ETIOLOGY OF NEONATAL INFECTIONS
The ANISA study aims to collect blood and nasopharyn-geal-oropharyngeal (NP-OP) swab specimens from all young infants (0–59 days of age) with possible serious bacterial infec-tion (pSBI) in the surveillance area, defined as physician con-firmation of any one of the clinical signs outlined by the World Health Organization.6 Cerebrospinal fluid (CSF) is collected from pSBI cases with clinical signs of meningitis.7 Both blood and CSF specimens are tested by bacterial culture and molecular assays, whereas NP-OP specimens are tested by molecular methods only. To understand the significance of detected viruses and bacteria in specimens from pSBI cases, we also enrolled and collected NP-OP and blood specimens from a subset of age- and seasonal-ity-matched healthy controls for molecular testing.8
SPECIMEN COLLECTIONBlood and CSF specimens are collected by applying standard
clinical procedures.9 In addition, ANISA uses a stringent protocol
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S16DOI: 10.1097/INF.0000000000001101
Laboratory Methods for Determining Etiology of Neonatal Infection at Population-based Sites in South Asia
The ANISA Study
Samir K. Saha, PhD,* Mohammad Shahidul Islam, MSc,* Shahida M. Qureshi, MSc,† Belal Hossain, MSc,* Maksuda Islam, BA,* Anita K. Zaidi, SM,† Joyanta K. Modak, MSc,* Hasan M. Al-Emran, MSc,*
Maureen H. Diaz, PhD,‡ Lesley McGee, PhD,‡ and Jonas M. Winchell, PhD,‡ for the ANISA Methods Group
Accepted for publication January 10, 2016. From the *Child Health Research Foundation, Dhaka, Bangladesh; †The Aga
Khan University, Karachi, Pakistan; and ‡Respiratory Disease Branch, Centers for Disease Control and Prevention, Atlanta, Georgia.
S.K.S. and A.K.Z. were primarily responsible for the study design. S.K.S., J.M.W., M.H.D., M.S.I. and L.M. designed and developed the TAC panels. B.H., M.I., S.M.Q., J.K.M., M.H.A., M.D. and L.M. participated in different aspects of formative research and implementation of the protocol. S.K.S. drafted the manuscript. All authors reviewed and edited subsequent drafts.
The ANISA study is funded by the Bill & Melinda Gates Foundation (grant no. OPPGH5307). The authors have no conflicts of interest to disclose.
Address for correspondence: Samir K. Saha, PhD, Department of Microbiol-ogy, Dhaka Shishu (Children’s) Hospital, Sher-E-Bangla Nagar, Dhaka 1207, Bangladesh. E-mail: [email protected].

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Etiology Detection Methodologies
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S17
to reduce the rate of contamination during specimen collection. Adequate volume of blood is an important requirement for success-ful blood culture, as inadequate volume frequently leads to false-negative results.10 In addition to blood culture, ANISA also aims to collect blood specimens for molecular assays and biobanking, for future testing with new diagnostics. Considering these needs and emphasizing blood culture as the gold standard for detection of infection etiology, ANISA developed a priority algorithm for the allocation of blood for culture, molecular tests and biobanking to ensure that culture bottles are inoculated with the maximum avail-able blood volumes (Table 1). Volume is tracked at each step: the amount of blood drawn is recorded by a phlebotomist; the quantity inoculated in the culture bottle is measured by weighing the prein-oculated and postinoculated bottle; and the amount placed in the ethylenediaminetetraacetic acid tube for molecular tests and biore-pository are recorded by laboratory personnel.
The primary aim of ANISA is to identify predominant etio-logical agents causing infection in newborns. Therefore, in addition to blood, we collect respiratory swabs, including both NP and OP swabs, taking into account that some microorganisms are selec-tively predominant in 1 of the 2 niches.11 We use flocked swabs (Copan Diagnostics, Brescia, Italy), which consist of thousands of short, perpendicular, polyamide bristles for collecting NP-OP specimens.12 This swab can hold a large volume of specimen and spontaneously elutes the whole specimen into liquid medium within a few seconds.13 After collection, both the NP and OP swabs are placed together in the same vial containing universal transport medium (Copan Diagnostics).
SEQUENCE OF SPECIMEN COLLECTIONSpecimens are collected primarily at community-level clinics.
In these settings, caregivers may be apprehensive about the procedures for clinical specimens, and the risk of blood culture contamination remains high. Venous blood is collected before NP-OP swabs to avoid agitating the baby to obtain an optimal volume of blood and limiting the possibility of contamination. CSF specimens are collected only from hospitalized newborns with clinical signs of meningitis.
STORAGE AND TRANSPORTATION OF SPECIMENS FROM FIELD TO LABORATORY
Specimen transportation modalities are customized accord-ing to the location and transportation facilities available at the specific sites. None of the community-based rural and peri-urban ANISA sites has a comprehensive specimen processing facility in the area of case enrollment. Therefore, sites transport the specimens to the local ANISA site laboratories for processing and testing. Blood culture bottles inoculated at collection sites are transported at ambient temperature and ethylenediaminetetraacetic acid blood and NP-OP specimens at 4°C. For remote sites (Sylhet, Bangla-desh, and Matiari, Pakistan), specimens are aliquoted and stored
(−20°C) at ANISA field laboratories and transported weekly in liquid nitrogen to other laboratories with molecular testing capac-ity. For quality control, the temperature of specimens is monitored by placing a thermometer inside the transport containers, and the temperature is recorded in a log book at the times of dispatch and receipt at the laboratory (Fig. 1).
DIAGNOSTIC TESTS FOR DETECTION OF PATHOGENS
Although blood culture remains the primary means to deter-mine sepsis etiology, this important diagnostic approach can only support the isolation of certain bacterial species. However, infections may also be caused by viruses and other atypical bacteria that are not able to be recovered using traditional blood culture methods. In addition, sensitivity of blood culture can be compromised because of previous antibiotic therapy, suboptimal blood volume, contamination and/or low levels of bacteremia. To obtain a comprehensive assess-ment of potential pathogens, we perform real-time polymerase chain reaction (PCR) tests on NP-OP and whole blood specimens for the detection of specific bacteria, viruses and other atypical organisms that may cause infection in newborns in this setting.
BLOOD CULTURE SYSTEMAutomated blood culture techniques have improved signifi-
cantly in recent years to support the growth of fastidious organisms.14 Furthermore, automated blood culture systems reduce workload by limiting subculture; the machine provides a signal for expected growth-positive bottles. Therefore, we use an automated blood cul-ture system and specific bottles for pediatric patients (BACTEC, Bec-ton, Dickinson and Company, Franklin Lakes, NJ or BacT/Alert®3D, Biomerieux, Marcy l'Etoile, France) at all field laboratories.
We also monitor and record the time to positivity (TTP) and delayed vial entry (DVE) and consider these parameters when interpreting blood culture results. To minimize deviation at the sites, ANISA provided a study-specific protocol for standardization and interpretation of blood culture methods across all sites.
TTPThe automated blood culture machine sounds an alarm
(beeps) when microbial growth is detected in a blood culture bottle. For beep-positive bottles, the BACTEC system records TTP based on the time the bottle is placed into the instrument to the time of the alarm. This can be used as a proxy for quantitative culture as the value of TTP is inversely proportional to the magnitude of bactere-mia, depending on the type of organism.15 During the interim analy-sis and at the end of the study, duration of TTP along with other parameters will be used in classifying the isolates as true pathogens or contaminants.16
DVEAs per manufacturer’s recommendations, blood culture bot-
tles should be loaded into the BACTEC machine immediately after inoculation. However, real-time loading of bottles is not feasible at most ANISA sites because of the distance between the place of specimen collection and the field laboratories. Studies have shown that DVE up to 12 hours at room temperature has no significant impact on results.17 Considering the possible diversity of patho-gens in newborns and environmental temperatures at ANISA sites, we carried out a formative study to mimic the field situation of Sylhet, Bangladesh, where the possibility of DVE is the highest. Blood culture bottles inoculated with 5–10 cfu/mL of Klebsiella pneumoniae or Streptococcus pneumoniae were held at tempera-tures of 20 and 37°C for 6 and 10 hours, before placing them in
TABLE 1. Distribution Priorities of Blood for Downstream Processing in the ANISA Study
Blood Volume Obtained (mL)
Distribution of Blood After Collection (mL)
In BACTEC Bottle In EDTA Tube
0.5–1.0 Full volume Nil>1.0–2 0.5–1.5 0.5*>2 >1.0 1.0†
*Molecular testing only.†Molecular testing and biorepository.EDTA indicates ethylenediaminetetraacetic acid.

Saha et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S18 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
the BACTEC machine. Experiments were conducted in duplicate, and average TTP was recorded. Every inoculated bottle resulted in a beep. However, TTP was considerably shorter for specimens with a DVE of 10 hours at 37°C, specifically for K. pneumoniae. On the basis of literature review, manufacturer’s instructions and our formative research findings, we conservatively decided to transport the bottles at room temperature, record the time of blood collec-tion and of loading into the BACTEC machine and subculture the aspirates from blood culture bottles before loading into the BAC-TEC machine if the delay between collection and loading was more than 8 hours. The subculture step is expected to facilitate earlier isolation of bacteria in bacteremic cases because the organism is expected to multiply significantly during the delay. It should also avoid false beep negativity caused by significant bacterial growth in the bottle before loading it into the machine.
ADDITIONAL EFFORTS TO IMPROVE DETECTION OF BACTERIAL PATHOGENS
Immunochromatographic TestIn an automated blood culture system, it is not uncommon
to have a machine-positive case (beep positive) without any growth on subculture (beep positive but culture negative [BPCN]). This can be because of erratic functioning of the machine leading to false alarms, or autolysis of bacteria because of delay in subcultur-ing, especially true for S. pneumoniae after its exponential growth phase.18 Because pneumococcus is commonly detected in South Asia in the 0- to 59-day age group,19 and BPCN cases occur more
commonly with pneumococcus, we included the pneumococcal BinaxNOW® (Portland, ME) test for all ANISA BPCN specimens to capture cases that are missed by blood culture.
Culturing Contaminated Specimens on Selective Media
Extensive measures were taken to minimize potential con-tamination of blood cultures; a maximum of 10% of specimens was selected as the tolerable limit of contamination based on the stand-ard practice guidelines and practical considerations of field labora-tory settings. Contamination may preclude the detection of slow-growing true pathogens such as S. pneumoniae and Haemophilus influenzae, which are intrinsically resistant to aminoglycoside and bacitracin, respectively.20,21 We performed culture of all contami-nated blood cultures on sheep blood agar with gentamicin and choc-olate agar with bacitracin to unmask these pathogens by inhibiting other potentially faster growing contaminating organisms.21
Molecular TestsBecause blood culture has limited sensitivity, we additionally
employ molecular diagnostics to potentially improve detection of spe-cific bacterial and viral etiologies within whole blood. Multipatho-gen molecular testing is also applied to NP-OP specimens. Although newer molecular methods may improve detection of microorganisms, none of these has proven to be more sensitive than blood culture, particularly in detecting pathogens from neonatal blood specimens.22 However, these methods can use “add-on” tests to increase the overall probability of detecting etiology within blood and NP-OP specimens.
FIGURE 1. ANISA specimen flowchart.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Etiology Detection Methodologies
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S19
Selection of Molecular PlatformAn appropriate molecular method is important for simul-
taneous detection of diverse bacteria and viruses (including both RNA and DNA viruses) in multiple specimen types (respiratory and blood) to determine the etiology of pSBI cases. Based on recommendations from the Pneumonia Etiology Research for Child Health study team,23 the following platforms were com-pared for suitability in the context of ANISA: (1) MassTag PCR, (2) Taqman Array Card (TAC) and (3) Fast-track Diagnostics respiratory pathogen panel (Fast-track Diagnostics, Malta). These methods and platforms were compared based on the performance characteristics (sensitivity/specificity), flexibility in customization for detection of selected pathogens, required specimen volume, user friendliness for laboratories with limited molecular testing experience, risk of contamination and war-ranty coverage or availability of technical support from manu-facturer (Table 2).
We selected the TAC platform (Life Technologies, Foster City, CA) for ANISA.25 This method has the following criteria:
A. Customized design including multiple parallel singleplex real-time reverse transcriptase PCR assays
1. Allows testing for select bacteria and viruses predicted to cause infection in newborns rather than a generic panel of potential pathogenic microorganisms.
2. No loss of sensitivity as often seen during multiplexing.
B. Minimum specimen volume (50 μL) required for simultaneous testing selected target pathogens on a single card (22 pathogens).
C. Simple assay setup, including minimal reagent preparation, minimizing the possibility of error during specimen processing.
D. Closed system with limited possibility of cross-contamination.
In addition, we use separate cards for blood (and CSF) and NP-OP specimens to detect more diverse etiological agents in the same patient (Fig. 2A and B).
Extraction of Total Nucleic AcidOptimal extraction of total nucleic acid from blood is chal-
lenging as it contains substances that may interfere with nucleic acid extraction or inhibit downstream applications such as PCR. The ANISA laboratory team developed a protocol to improve nucleic acid extraction performance, including implementation of a prelysis treatment step and use of an automated extraction platform (MagNA Pure Compact, Roche Applied Science, Indianapolis, IN) as previously described.25
Selection of Target PathogensBetween specific TACs for testing NP-OP and blood speci-
mens, each patient is tested for 28 etiological agents, including 15 bacteria and 13 viruses. NP-OP and blood specimens are tested for 22 and 12 organisms, respectively (Fig. 2A and B). However, the list of definite, probable and potential pathogens for newborn sepsis is more extensive. To generate the most appropriate and comprehensive custom panel of agents for testing respiratory and blood specimens from newborns in South Asia, we performed a literature review to pre-pare a broad list of the most common pathogens identified in neonatal blood and respiratory (NP-OP) specimens. This list of pathogens was refined by applying the Delphi method. Briefly, a list of potential path-ogens for blood and respiratory specimens was shared with 9 external experts to rank the pathogens in hierarchical tiers based on their per-ceived potential for causing infection in young infants in South Asia. The final list of pathogens for blood and NP-OP cards was selected by the ANISA coordination team and technical advisory group (TAG) members. Additional changes were made to the custom TAC designs, including an increased number of assay replicates on the ANISA TAC for blood specimens (Fig. 2B) and removal of some assays, based on the findings of testing during the study pilot phase (Fig. 2A and B).
Testing of Specimens from Healthy Control Infants
Detection of certain bacteria and respiratory viruses, particularly in NP-OP specimens, does not alone establish an
TABLE 2. Comparison of Select Contemporary Multipathogen Molecular Detection Platforms With Regards to Suitability for the ANISA Study
Method Advantages Limitations
MASS Tag Multiplex PCR platformRobust in detecting 30 different etiologies simultaneouslySensitivity is comparable with real-time PCR.24
Establishment of multiplex is complex because these may vary from singleplex optimization.
Multiplexing for new etiologies would be challenging.Optimization remains in the hand of manufacturer.Requires constant supply of nitrogen gas.Needs uninterrupted power supply.
Fast Track Pre-optimized real-time multiplex PCRTest panels are with prespecified set of disease syndrome
specific pathogens (eg, respiratory, gastrointestinal).The kits are available in different pack sizesFlexibility of using different real-time PCR platforms.The system has internal controls to ensure the test validity.Equipment and kits are appropriate for laboratories with
limited resources.
Maximum 4 target pathogens per multiplex assay.Establishment of multiplex is complex as it may vary from
singleplex optimization parameters.Multiplexing for new etiologies would be challenging and
may not be successful.Whole testing procedure is time consuming.The system is open, thus has a risk of contamination when
working in resource-poor setting.Taqman Array
CardSingleplex real-time PCR The method is expensive compared with Fast Track.Requires small volume of specimens It needs specific platform to run the cards.The platform uses a specialized card for simultaneous detec-
tion of 21 bacterial and/or viral targetsThe process needs special equipment which includes centri-
fuge machine, sealer.Closed cards with 384 wells with lyophilized primers and
probes optimized for specific targetsEach well takes 1.0 μL of specimen. So, the sensitivity may
be less than the singleplex real-time PCR.All targets are in duplicate, which can be increased further to
increase the sensitivity, if neededThe testing cards has built-in positive and negative controlsThe turnaround time is only 3 h for testing 6 specimens for
22 different targets

Saha et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S20 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
FIGURE 2. (A) Layout of ANISA TAC for testing blood specimens. (B) Layout of ANISA TAC for testing respiratory specimens (NP-OP). CMV indicates cytomegalovirus; HMPV, human metapneumovirus; RNP3, ribonuclease P3; IPC, internal positive control; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; RSV, respiratory syncytial virus.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Etiology Detection Methodologies
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S21
organism as the cause of a pSBI episode. Some viruses and bacteria may be present as natural colonizers of the respiratory tract. Past studies with respiratory specimens have shown that the prevalence of such organisms can vary across populations and age groups and by season.26 For blood specimens, there is biologic plausibility that molecular tests with higher sensitiv-ity and ability to detect the genome of nonviable organisms may also result in the detection of potential infection-causing organisms’ genome in the blood of clinically healthy young infants.
LABORATORY DATA SYSTEMThe quality of ANISA data, which will ensure correct
study conclusions, largely depends on consistent high-quality laboratory performance in multiple field sites in 3 different countries. Identification of inconsistent practices or unexpected laboratory results is a challenge for any large study. The task becomes particularly difficult if the final result has only been noted on a hard copy laboratory book and tests cannot be repeated (Davidson H. Hamer, personal communication, 2009). ANISA data capture forms (DCFs) were created to document the rel-evant details of every specimen processing step, such as prelysis and nucleic acid extraction specimens and physical, biochemical and serological characterization of blood culture isolates. DCFs are tailored to capture details of specimens identified as con-taminated to learn about the contamination and ensure that the recovered organism(s) is properly classified. These DCFs can replace traditional laboratory notebooks; opportunities for tran-scription errors are limited by built-in checks in the data entry system.27 All laboratory data on DCFs are entered into ANISA databases at the respective sites in real time by the laboratory personnel performing the tests. The data are transferred weekly to the central data server for all sites in Dhaka, Bangladesh, and monitoring reports are generated routinely. These features are intended to minimize the frequency of error during data entry and transfer and to decrease the probability of data loss. Routine monitoring of laboratory data by the ANISA coordination team ensures prompt identification and resolution of errors in speci-men collection, transport and testing activities.28
CONCLUSIONThe ANISA study coordination team is supported by an
experienced multidisciplinary TAG that includes clinicians, epidemiologists and laboratory experts in both molecular and microbiologic methods related to bacteria and viruses. The coor-dination team and TAG utilized a literature review, knowledge of the local demography of participating sites and personal under-standing of site-specific needs to design the study procedures described here and throughout this supplement. When necessary and possible, laboratory decisions were also informed by forma-tive research, focused experiments and testing of pilot speci-mens. The approaches described were developed to address spe-cific challenges faced in ANISA but may be applicable to future population-based etiology studies in resource-limited settings. Laboratory results generated during ANISA will provide addi-tional validation data to support the use of selected methods at the field settings of future studies.
ACKNOWLEDGMENTSThe authors thank their colleagues at the US Centers for
Disease Control and Prevention for their technical assistance in development and implementation of the molecular test systems for ANISA. They also acknowledge the input of experts from around the
world for helping them choose the etiological agents to be included in the molecular test platforms.
REFERENCES 1. UNICEF, World Health Organization, The World Bank, et al. Levels & Trends in
Child Mortality Report 2011. New York: United Nations Children’s Fund; 2012.
2. Arifeen SE, Mullany LC, Shah R, et al. The effect of cord cleansing with chlorhexidine on neonatal mortality in rural Bangladesh: a community-based, cluster-randomised trial. Lancet. 2012;379:1022–1028.
3. Baqui AH, Saha SK, Ahmed AS, et al. Safety and efficacy of simplified antibiotic regimens for outpatient treatment of serious infection in neo-nates and young infants 0-59 days of age in Bangladesh: design of a rand-omized controlled trial. Pediatr Infect Dis J. 2013;32(suppl 1):S12–S18.
4. Zaidi AK, Huskins WC, Thaver D, et al. Hospital-acquired neonatal infec-tions in developing countries. Lancet. 2005;365:1175–1188.
5. Zaidi AK, Thaver D, Ali SA, et al. Pathogens associated with sepsis in newborns and young infants in developing countries. Pediatr Infect Dis J. 2009;28(1 suppl):S10–S18.
6. Gove S. Integrated management of childhood illness by outpatient health workers: technical basis and overview. The WHO Working Group on Guidelines for Integrated Management of the Sick Child. Bull World Health Organ. 1997;75(suppl 1):7–24.
7. Curtis S, Stobart K, Vandermeer B, et al. Clinical features suggestive of meningitis in children: a systematic review of prospective data. Pediatrics. 2010;126:952–960.
8. Islam MS, Rahman QS, Hossain T, et al. Using text messages for critical real-time data capture in the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S35–S38.
9. Jurado R, Walker HK. Cerebrospinal fluid. In: Walker HK, Hall WD, Hurst JW, eds. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990.
10. Connell TG, Rele M, Cowley D, et al. How reliable is a negative blood cul-ture result? Volume of blood submitted for culture in routine practice in a children’s hospital. Pediatrics. 2007;119:891–896.
11. Kim C, Ahmed JA, Eidex RB, et al. Comparison of nasopharyngeal and oro-pharyngeal swabs for the diagnosis of eight respiratory viruses by real-time reverse transcription-PCR assays. PLoS One. 2011;6:e21610.
12. Esposito S, Molteni CG, Daleno C, et al. Comparison of nasopharyngeal nylon flocked swabs with universal transport medium and rayon-bud swabs with a sponge reservoir of viral transport medium in the diagnosis of paedi-atric influenza. J Med Microbiol. 2010;59(pt 1):96–99.
13. Jones G, Matthews R, Cunningham R, et al. Comparison of automated process-ing of flocked swabs with manual processing of fiber swabs for detection of nasal carriage of Staphylococcus aureus. J Clin Microbiol. 2011;49:2717–2718.
14. Murray PR, Masur H. Current approaches to the diagnosis of bacterial and fungal bloodstream infections in the intensive care unit. Crit Care Med. 2012;40:3277–3282.
15. Hossain B, Weber MW, Hamer DH, et al. Classification of blood culture iso-lates into contaminants and pathogens on the basis of clinical and laboratory data. Pediatr Infect Dis J. 2016;35(suppl 1):S52–S54.
16. Peralta G, Rodríguez-Lera MJ, Garrido JC, et al. Time to positivity in blood cultures of adults with Streptococcus pneumoniae bacteremia. BMC Infect Dis. 2006;6:79.
17. Sautter RL, Bills AR, Lang DL, et al. Effects of delayed-entry condi-tions on the recovery and detection of microorganisms from BacT/ALERT and BACTEC blood culture bottles. J Clin Microbiol. 2006;44:1245–1249.
18. Vasallo FJ, López-Miragaya I, Rodríguez A, et al. Apparently false-positive blood cultures due to autolyzed Streptococcus pneumoniae. Clin Microbiol Infect. 2000;6:688–689.
19. Darmstadt GL, Saha SK, Choi Y, et al; Bangladesh Projahnmo-2 (Mirzapur) Study Group. Population-based incidence and etiology of community-acquired neonatal bacteremia in Mirzapur, Bangladesh: an observational study. J Infect Dis. 2009;200:906–915.
20. Crawford JJ, Barden L, Kirkman JB Jr. Selective culture medium to survey the incidence of Haemophilus species. Appl Microbiol. 1969;18:646–649.
21. Saha S, Darmstadt G, Naheed A, et al. Improving the sensitivity of blood culture for Streptococcus pneumoniae. J Trop Pediatr. 2011;57:192–196.
22. Huttunen R, Syrjänen J, Vuento R, et al. Current concepts in the diagnosis of blood stream infections. Are novel molecular methods useful in clinical practice? Int J Infect Dis. 2013;17:e934–e938.

Saha et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S22 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
23. Murdoch DR, O’Brien KL, Driscoll AJ, et al; Pneumonia Methods Working Group; PERCH Core Team. Laboratory methods for determining pneumonia etiology in children. Clin Infect Dis. 2012;54(suppl 2):S146–S152.
24. Briese T, Palacios G, Kokoris M, et al. Diagnostic system for rapid and sensi-tive differential detection of pathogens. Emerg Infect Dis. 2005;11:310–313.
25. Diaz MH, Waller JL, Napoliello RA, et al. Optimization of multiple patho-gen detection using the TaqMan Array Card: application for a population-based study of neonatal infection. PLoS One. 2013;8:e66183.
26. Bizzarro MJ, Raskind C, Baltimore RS, et al. Seventy-five years of neonatal sepsis at Yale: 1928-2003. Pediatrics. 2005;116:595–602.
27. Rahman QS, Islam MS, Hossain B, et al. Centralized data management in a multicountry, multisite population-based study. Pediatr Infect Dis J. 2016;35(Suppl 1):S23–S28.
28. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35(Suppl 1):S39–S44.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S23
Supplement
Background: A centralized data management system was developed for data collection and processing for the Aetiology of Neonatal Infection in South Asia (ANISA) study. ANISA is a longitudinal cohort study involving neo-natal infection surveillance and etiology detection in multiple sites in South Asia. The primary goal of designing such a system was to collect and store data from different sites in a standardized way to pool the data for analysis.Methods: We designed the data management system centrally and imple-mented it to enable data entry at individual sites. This system uses vali-dation rules and audit that reduce errors. The study sites employ a dual data entry method to minimize keystroke errors. They upload collected data weekly to a central server via internet to create a pooled central database. Any inconsistent data identified in the central database are flagged and cor-rected after discussion with the relevant site. The ANISA Data Coordination Centre in Dhaka provides technical support for operations, maintenance and updating the data management system centrally. Password-protected login identifications and audit trails are maintained for the management system to ensure the integrity and safety of stored data.Conclusion: Centralized management of the ANISA database helps to use common data capture forms (DCFs), adapted to site-specific contextual requirements. DCFs and data entry interfaces allow on-site data entry. This reduces the workload as DCFs do not need to be shipped to a single location for entry. It also improves data quality as all collected data from ANISA goes through the same quality check and cleaning process.
Key Words: data management, population-based, young infants, multi-center, ANISA
(Pediatr Infect Dis J 2016;35:S23–S28)
Collection, management and transmission of reliable and scien-tifically sound data are critical to the success of any research
study. A centralized data management system can improve the data quality and performance of multicenter studies.1–3 Aetiology of Neonatal Infection in South Asia (ANISA) is a longitudinal cohort study being carried out in 5 population-based sites in Bangladesh, India and Pakistan. We developed and implemented a manage-ment system centrally for capture, entry, storage and distribution of the ANISA data. In this study, approximately 300,000 married women of reproductive age (15–49 years) are under surveillance across the 5 study sites for a 2-year period. We expect to register 66,000 live births in this population and follow them up to the age of 59 days. The data system is designed to collect, store and trans-mit information related to sociodemographics, pregnancy, antena-tal and essential newborn care for the enrolled pregnant women and their newborns; and home-based follow-up information for the young infants. The young infant follow-up includes clinical assess-ment for possible serious bacterial infections by community health workers (CHWs) and care-seeking history, physician assessments for possible serious bacterial infections and the laboratory testing of clinical specimens. This article describes the design and devel-opment of the ANISA data management system as implemented across the participating entities.
ANISA DATA MANAGEMENT SYSTEM DESIGN REQUIREMENTS
The ANISA Data Coordination Centre (DCC) ensures that all data for ANISA are recorded, processed, securely stored and transmitted using standardized methods at every stage. It helps coordinate and monitor data management activities, and provides support to the study sites when necessary. In consultation with the ANISA Study Coordination Team, the DCC established require-ments and principles for the ANISA data management system (Table 1).
ANISA DATA MANAGEMENT SYSTEMANISA requires data collection from communities, hospi-
tals and laboratories. This situation makes the management of data very complex, as each set requires proper linkage at individual level. It also necessitates having appropriate data security and audit systems in place.4 Therefore, DCC has not only designed and devel-oped a system to meet these needs but also works closely with the site data teams to ensure that the system functions optimally at all locations. The design and development process of the ANISA data management system involves 5 key activities:
Data Capture FormsData capture forms (DCFs) were designed in a manner
that allows efficient collection and processing of data at all study sites.4 The ANISA Study Coordination Team and DCC have been responsible for developing the study procedures and DCFs. Follow-ing the research protocol, we initially mapped out procedures for
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S23DOI: 10.1097/INF.0000000000001102
Centralized Data Management in a Multicountry, Multisite Population-based Study
Qazi Sadeq-ur Rahman, MSc,* Mohammad Shahidul Islam, MSc,† Belal Hossain, MSc,† Tanvir Hossain, MSc,* Nicholas E. Connor, MSc,* Md. Jahiduj Jaman, MA,* Md. Mahmudur Rahman, MSc,† A. S. M. Nawshad Uddin Ahmed, FCPS,† Imran Ahmed, MA,§ Murtaza Ali, MBBS,§
Syed Mamun Ibne Moin, BSc,‡ Luke Mullany, PhD,‡ Samir K. Saha, PhD,† and Shams El Arifeen, DrPH,* for the ANISA Methods Group
Accepted for publication January 10, 2016. From the *Centre for Child and Adolescent Health, International Centre for
Diarrhoeal Disease Research, Bangladesh, Dhaka, Bangladesh; †Child Health Research Foundation, Dhaka, Bangladesh; ‡International Center for Maternal and Newborn Health, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; §Aga Khan University, Karachi, Pakistan; and ¶Cen-ters for Disease Control and Prevention, Atlanta, Georgia.
The members of the ANISA Methods Group are listed in the Acknowledgments. The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No.
OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Shams El Arifeen, DrPH, Director, Centre for Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Bangladesh, Mohakhali, Dhaka 1212, Bangladesh. E-mail: [email protected].

Rahman et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S24 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
enrollment and follow-up of pregnant women and newborns. A lit-erature review was conducted to determine maternal and neonatal risk factors that could be measured practically in the context of all ANISA study sites. The Coordination team reviewed the latest avail-able Demographic and Health Survey instruments from Bangladesh, India and Pakistan to ensure that similar socio-demographic varia-bles were measured in a comparable way using tried and tested ques-tions.5–7 The drafts of DCFs were shared with the sites for review and testing at field level. Each site data team re-examined the forms, tested them in the field and shared their feedback. The number of feedback reports we received on each version of the DCFs is shown in Figure 1. Once the generic DCFs were finalized, site-specific DCFs were developed. These site-specific forms differ from each other only in the mother and newborn identification sections and site-specific responses to some of the questions, for example, caste, types of facilities and providers. DCFs were translated into local languages by the site teams. DCC checked the translations of the forms independently to ensure that the intended meanings of ques-tions and responses were preserved in these translations. Detailed instruction manuals for each form were also provided to the sites. A summary of the ANISA DCFs is given in Table 2.
Assigning Identification Numbers to Study Participants
We follow a unique numbering system to identify the study participants (both the pregnant women and their newborns) and respective clinical specimens.8 A woman receives a unique 7-digit identification number (ID) for each pregnancy registered. The first digit of an ID refers to the study site where the pregnancy is reg-istered with the last digit always zero (0), while the 5 digits in-between are study participant identifiers that are generated sequen-tially by the data server of respective sites. Each live birth receives a 7-digit ID. The first 6 digits are the same as for the correspond-ing mother, while the seventh digit refers to the child’s serial birth outcome from the same pregnancy (1 for first birth, 2 for second birth, etc.). The list of pregnancy IDs is generated by the ANISA data management software at each site, and CHWs allocate those to study participants. Each CHW can only use the IDs from her own list.
Data Management ApplicationThe ANISA data management application was designed and
developed using Microsoft SQL Server 2008 R2 for data storage, Dot net (.Net) with Code Behind C Sharp (C#) and Visual Basic 6.0 for interfaces and Crystal Report 8.0 for reporting.9,10 Some site-specific modifications have been made for capturing site-spe-cific information (eg, the local identification part). Every site uses this application for entry and storage of its own data. The 5 pri-mary components of the ANISA data management application are detailed in the following sections.
User InterfacesThe primary graphical user interface for data entry is tradi-
tional keyboard input. The graphical user interface is designed for data entry to match the DCFs with an emphasis on ease and speed. Simultaneous data entry is possible through multiple client com-puters connected to a local server. Validation rules are set to prevent inconsistency and other errors during data entry. These validation rules include logical checks, range checks, uniqueness check of IDs and skipping rules for avoiding entry of undesired information. The data entry system has 2 parts linked by the study ID, the field data entry system and the laboratory data entry system. The interface for laboratory data entry also includes a bar-code reader for logging specimen repository and entry of specimen testing results. This interface also has the facility of importing molecular test results from the molecular Taqman array machine (Life Technologies, Fos-ter City, CA). Additional user interfaces include report generation, ID creation, data editing and text message processing systems.
DatabasesA relational management system is used for the databases,
and all data tables are linked through primary and foreign keys. The primary key of a relational table uniquely identifies each record in the table. The foreign key in a relational table identifies the primary key of another table. The foreign keys are used to uniquely identify the relationship between 2 tables. The detailed architecture of the database system is shown in Figure 2.
Data Storage and Uploading SystemEach study site maintains its ANISA database in a local
server and extracts its own data for error checking, reporting and study monitoring. Sites upload their data weekly to the central server located at the Child Health Research Foundation, Dhaka, Bangladesh. ANISA uses ADO.NET’s SqlBulk Copy program for quick uploading of the data via the internet. If data upload to the central server is not successful or is not carried out as scheduled, an automatic notification email is sent to the responsible persons at the site and the DCC.
Specimen Tracking and Biorepository SystemBoth the newborn and the specimen IDs are recorded in
the specimens collection form and physician assessment form so that both IDs can be linked in the databases. A virtual specimen
TABLE 1. Principles and Requirements for ANISA Data Management
• Exactly the same paper DCFs should be used for primary data collection in all sites, with a few site-specific adaptations• The data management application should not require advanced hardware and software, and should thus be compatible with existing data infra-
structure at each study site• A user-friendly interface will be developed for all data entry and access• The entry of population surveillance, clinical and laboratory data will be linked, including specimen tracking• An audit trail for tracking any change in data already entered will be maintained• Stored data may be extracted in a format suitable for statistical analyses• Data will be stored securely and backed up at regular intervals
0
100
200
300
400
Num
ber
of F
eedb
ack
FIGURE 1. Number of feedback reports received on each version of ANISA DCFs.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Data Management
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S25
biorepository is created in every site database, mirroring the actual location of a specimen in the freezer. The specimen tracking and biorepository system is described in detail elsewhere in this sup-plement.8
Text Message SystemANISA uses mobile phone-based text messages as an eas-
ily accessible method of information input and output for the data management application. This permits entering some critical data in the site databases in real time. The use of text messaging in ANISA is described separately in this supplement.11
Application TestingDuring the development of the ANISA data management
application, software testing personnel were assigned to work with the programmers. After development of the data entry interface for each DCF, that interface was tested with different ranges/values to check whether the application could flag inconsistent data, follow skip rules and capture the values within ranges. The beta version of the data management application was also tested by 3 of the site teams with real study data.
Quality ControlThe ANISA DCC aims to ensure generation of high quality
and reliable data from all sites through the following set of activi-ties, processes and procedures.
Training on the ANISA Data Management SystemBefore the pilot phase of the project, we conducted a 3-day
workshop on the ANISA data management system. The lead of the data team and a data supervisor from each site attended the work-shop, where the following issues were covered:
• Use of the instruction manual for the ANISA data management system and code book of the data files;
• Configuring the MS SQL server and restoring the ANISA data management system in the site servers;
• Installation and use of ANISA data management application;• Guidelines for data entry and comparing the first and second
entry of data;• Guidelines for data editing, cleaning and uploading;• Configuring the database server to run the text message software.
TABLE 2. Key Information Recorded in Different DCFs Used in ANISA
Information Collected
Field-based DCFs Laboratory-based DCFs
For
m 1
: Pre
gnan
t W
oman
Reg
istr
atio
n
For
m 2
: Pre
gnan
cy O
utc
ome
Reg
istr
atio
n
For
m 3
: New
born
Reg
istr
atio
n
For
m 4
a: N
ewbo
rn F
ollo
w-u
p, 0
–6 D
ays
For
m 4
b: N
ewbo
rn F
ollo
w-u
p, 8
–59
Day
s
For
m 5
: Un
sch
edu
led
CH
W V
isit
s
For
m 5
A: F
ollo
w-u
p of
Cu
ltu
re-p
osit
ive
Cas
es
For
m 6
: Ph
ysic
ian
’s A
sses
smen
t
For
m 8
: Hos
pita
l Dis
char
ge
For
m 7
a: B
lood
Col
lect
ion
For
m 7
b: R
espi
rato
ry S
peci
men
Col
lect
ion
For
m 7
c: C
SF
Spe
cim
en C
olle
ctio
n
For
m 9
a: B
lood
Lab
orat
ory
Boo
k
For
m 9
b:C
SF
Lab
orat
ory
Boo
k
For
m 1
0: V
erba
l Au
tops
y
Current and previous pregnancy history √Maternal nutritional status √ √Demographic information √Socioeconomic status √Antenatal care √Smoking and tobacco use √ √ √Complications and care seeking during pregnancy and delivery √ √Labor and delivery outcome √ √Respiratory illness of mother/family in 7 days before delivery √Newborn registration and control selection √Newborn care and practice √ √Feeding practice √ √Illness, care-seeking and treatment history of newborn √ √ √ √ √Illness history in subsequent 6 days after specimen collection √History of illness between visits √ √Treatment received for illness √ √ √ √ √Clinical assessment √ √ √ √CHW’s visit outcome √ √ √ √ √ √ √Immunization history √Case enrollment √Case management and medication √ √Specimen collection √ √ √Blood specimen quality and transportation √ √Blood culture results √CSF culture results √Specimen preservation √ √Cause of death √

Rahman et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S26 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
Data CleaningEach site uses its own monitoring procedure to check data
consistency and validity. Field supervisors review each DCF filled out by a CHW before entry into the system. A clinical supervisor checks each DCF filled out by the study physicians. In addition, using STATA 12.0 the DCC has developed a program to identify inconsistent values within and between tables and variables. This program generates a list of study IDs with inconsistent entries, which is shared with the sites for corrective action.
Double Data EntryKeystroke errors during data entry are common and can
affect quality. The ANISA data management software allows study sites to enter the same data twice. ANISA’s built-in comparison pro-gram checks the entries in both sets of data and identifies the differ-ence between the 2 entries. Data supervisors at the study sites check the mismatches and correct the values after reviewing the DCFs. A web page (http://chu.icddrb.org/anisa) that automatically displays site-specific data entry progress has been designed to monitor data entry at each site.
Data Security and Audit TrailThe data at site servers are secured by user-specific pass-
words that require separate permissions for data entry and editing. An audit trail system was added to the data management applica-tion for keeping track of every update made in the databases after data entry and identifying the persons who made the changes with time and date.
Data BackupEach site is responsible for making a backup of their site-
specific databases at periodic intervals. At the Coordination Centre, we create a backup of the entire database on an optical disc once a month and store it in a location separate from that of the server. In addition, we maintain a backup copy of the entire database on a different server in a different physical location.
CHALLENGES AND KEY LESSONSAll the ANISA study sites have experience in data collection
with printed DCFs. A key challenge in using paper-based DCFs is that any change to a form creates difficulties in data capture, entry and analysis. Although the site teams evaluated the DCFs dur-ing their creation and the piloting of the study, the DCC still make changes to the DCFs as necessary. These changes are reflected simultaneously in the DCFs across all sites. The data management application is updated accordingly to facilitate smooth data entry with the modified DCFs. We tried to create a data entry interface that allows speedy data entry and minimizes backlog. Most of the DCF data is entered into the database within 1 month of collection (Fig. 3), which helps to monitor study progress in real time. We are using MS SQL Server for data storage that allows convenient export of the data to other formats (eg, MS Excel, STATA, SAS, etc.) for analysis.
Programmers from the DCC resolve issues with the data management software as they arise. They also use TeamViewer soft-ware to access the site servers remotely for troubleshooting. The
Laboratory-based data entry• Specimen collection• Lab book
CHW
Send text message for• Pregnancy registration• Birth registration• pSBI case referral by CHW• Healthy control enrollment • pSBI case enrollment
Generate StudyID
Reply text message to • CHW for control selection• Physician for referral of pSBI cases• Supervisor about selection of control
Internet
Internet
http://chu.icddrb.org/anisa
End user
1
Data collection
Submit data forms
Field-based data entry• Pregnancy and birth registration• Demographic and maternal
information • Newborn care, child assessment and
treatment
Site database server• AnisaMain (field data)• AnisaLab (laboratory data)
ANISA Coordination Center(pooled database)
Data upload
Data storage
Data store
Data backup• External hard disk• Compact disk• Cloud
CHW or Physician
2
3
4
5
6
7
8
9
FIGURE 2. ANISA data flow and text messaging architecture.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Data Management
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S27
combination of the high volume of transmitted data and fluctuating internet connectivity has always caused problems during uploading of data to the central database. We have separated the data uploading system from the audit table for making data upload events smooth. A snapshot of the successful data upload status in the central server
at 2 stages of the study is shown in Figure 4A, B. Data cleaning has been a continuous challenge throughout the project as missing values and data entry errors are almost unavoidable in an extensive data-base. The DCC regularly meets with site data teams either physically or online (Webex and Skype) to review the progress of data entry and cleaning. These meetings help to overcome any data entry backlog and correct data entry problems including missing values and incon-sistencies. Some key messages learned during the use of our data system at field level are listed in Table 3.
SUMMARYAlthough the design and implementation of the ANISA data
management application across multiple sites was challenging, cen-tralized management of the system has resulted in smooth handling of study data. It has also facilitated sharing of the workload by ena-bling sites to enter data locally and allowing the DCC to focus on identifying specific data inconsistencies and clarifying ambiguities. Site teams are also not required to develop their individual data cap-ture and management software and are thus relieved from trouble-shooting the system. Data entry at all study sites is thus expedited;
FIGURE 4. A) Data upload status of at the beginning of the project (March–April 2012) showing the gaps of unsuccessful uploads in the central data server at the initial stage of ANISA.B) Data upload status in the middle of the project (June–July 2013) showing high rates of successful data upload in the central data server.
0
20
40
60
80
100
Perc
ent o
f fo
rms
ente
red
FIGURE 3. ANISA DCFs entered into the database within 2 months of information collection.

Rahman et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S28 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
ANISA has a minimal data entry backlog at any given point in time and is producing a harmonized dataset from all sites with very lim-ited data entry errors. This gives us confidence in the quality and validity of the ANISA data and of the resulting study outcomes.
ACKNOWLEDGMENTSWe acknowledge the contribution of Mr. Abu Mohammad
Saleheen from the International Centre for Diarrhoeal Disease Research, Bangladesh in developing the ANISA software. We are indebted to CSL Software Resources Ltd. for helping us in design-ing the text messages component of the ANISA data management software. We thank the site teams for their valuable feedback on this application to make it functional.
The ANISA Methods Group: Aarti Kumar: Community Empowerment Lab, Lucknow, India; Abdul Momin Kazi: The Aga Khan University, Karachi, Pakistan; Abdullah H. Baqui: Johns Hopkins Bloomberg School of Public Health, Johns Hopkins Uni-versity, Baltimore, Maryland; Anita K. Zaidi: The Aga Khan Uni-versity, Karachi, Pakistan; Anuradha Bose: Christian Medical Col-lege, Vellore, India; Arif Billah: Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; Daniel E. Roth: Department of Paediatrics, Hospital for Sick Chil-dren and University of Toronto, Canada; Derrick Crook: John Radcliffe Hospital, University of Oxford, Oxford, United King-dom; Hamidul Haque: Child Health Research Foundation, Dhaka, Bangladesh; Jonas M. Winchell: Centers for Disease Control and Prevention, Atlanta, Georgia; Maksuda Islam: Child Health Research Foundation, Dhaka, Bangladesh; Mathuram Santosham: Johns Hopkins Bloomberg School of Public Health, Johns Hopkins
University, Baltimore, Maryland; Maureen H. Diaz: Centers for Disease Control and Prevention, Atlanta, Georgia; Nazma Begum: Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; Nong Shang: Centers for Dis-ease Control and Prevention, Atlanta, Georgia; Pinaki Panigrahi: University of Nebraska Medical Center, Omaha, Nebraska; Sajid B. Soofi: The Aga Khan University, Karachi, Pakistan; Shahida M. Qureshi: The Aga Khan University, Karachi, Pakistan; Shamim A. Qazi: Department of Maternal, Newborn, Child and Adolescent Health, World Health Organization, Geneva, Switzerland; Sheraz Ahmed: The Aga Khan University, Karachi, Pakistan; Stephen P. Luby: Stanford Woods Institute for the Environment, Stanford University, Stanford, California; Vishwajeet Kumar: Community Empowerment Lab, Lucknow, India; Yoonjoung Choi: Centers for Disease Control and Prevention, Atlanta, Georgia; Zulfiqar A. Bhutta: The Aga Khan University, Karachi, Pakistan; and Steph-anie J. Schrag, Dphil: Centers for Disease Control and Prevention, Atlanta, Georgia.
REFERENCES 1. Onyango AW, Pinol AJ, de Onis M. Managing data for a multicountry lon-
gitudinal study: experience from the WHO Multicentre Growth Reference Study. Food Nutr Bull. 2004;25(1 Suppl):S46–S52.
2. Biswas K, Carty C, Horney R, et al. Data management and other logistical challenges for the GEMS: the data coordinating center perspective. Clin Infect Dis. 2012;55(Suppl 4):S254–S261.
3. Krishnankutty B, Bellary S, Kumar NB, et al. Data management in clinical research: an overview. Indian J Pharmacol. 2012;44:168–172.
4. Prokscha S. Practical Guide to Clinical Data Management. 3rd ed. Boca Raton, FL: CRC Press; 2012.
5. National Institute of Population Studies (Pakistan). Pakistan Demographic and Health Survey 2006–2007. Calverton, MD: Macro International, Inc.; 2007.
6. International Institute for Population Sciences (India). India Demographic and Health Survey 2005–2006. Calverton, MD: Macro International, Inc.;2007.
7. USAID, NIPORT. Bangladesh Demography and Health Survey 2007. Calverton, MD: Macro International Inc.; 2007.
8. Connor NE, Hossain T, Rahman QS, et al. Development and implementa-tion of the ANISA labeling and tracking system for biological specimens. Pediatr Infect Dis J. 2016;35 (Suppl 1):S29–S34.
9. Carter J. Database Design and Programming with Access, SQL, Visual Basic, and ASP. New York, NY: McGraw-Hill; 2002.
10. Peck G. Crystal Reports 2008: The Complete Reference. New York, NY: McGraw-Hill; 2008.
11. Islam MS, Rahman QS, Hossain T, et al. Using text messages for critical real-time data capture in the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S35–S38.
TABLE 3. Key Messages on Data Management System Development
• Detailed planning and adequate time and effort to design and prepare, based on good understanding of site contexts and care-ful anticipation of challenges, is critical
• Being careful in choices (software, tools and procedures) is important, but so is having the flexibility to change as needed
• Piloting is essential and should be done in the study area where the DCFs are being used and by the people who are going to use the system
• Close monitoring and data checking from the very beginning and having continuous and close interactions with site data teams are critical for ensuring good quality data
• Entering data in real time is very important as this permits the correction of missing or inconsistent information

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S29
Supplement
Background: The Aetiology of Neonatal Infection in South Asia study is a major effort to determine the causes of community-acquired neonatal infec-tions. It involves collecting epidemiological, clinical and laboratory data in 5 sites in 3 countries. The field and laboratory research operations are stream-lined to maintain integrity and validity while operating in complex and vari-able environments. We developed a customized system for implementation of labeling and tracking biological specimen in both rural and urban community settings and integrated into all study laboratories. This report outlines the development and implementation of this harmonized system. Design: The system links and tracks specimens with study participants and results generated from laboratory tests. Each biological specimen and its aliquots are tracked through key steps of the protocol, from collection and transport through molecular testing and long-term storage.Conclusion: The labeling and tracking system allows for standardization and monitoring of laboratory processes and improves the accuracy of Aeti-ology of Neonatal Infection in South Asia data. Community-based scien-tific projects could greatly benefit by adopting this, or a similar, system for specimen tracking and data linkage.
Key Words: specimen tracking, barcode, preanalytical error, ANISA, biorepository
(Pediatr Infect Dis J 2016;35:S29–S34)
Preanalytical errors are those occurring at any point before a specimen is analyzed—during collection, labeling, transporta-
tion to a laboratory, processing of specimens within a laboratory and/or when placing specimens into storage.1 Mishandling and mislabeling errors during sample collection and subsequent patient misidentification can lead to specimen loss, misdiagnosis and, in some instances, serious adverse events such as blood product mis-matching or administration of inappropriate medical treatment.2,3 Mislabeling or mishandling of specimens in an etiology study such as Aetiology of Neonatal Infection in South Asia (ANISA) could very likely result in errors in pathogen-specific incidence, risk fac-tor analysis, treatment success and other analyses and could impact
the validity of the conclusions drawn. Preanalytical error rates vary greatly across countries and facilities, owing mainly to dif-ferent available resources, standards and oversight of procedures.2,4 They account for the majority of errors in the modern laboratory, whereas analytical laboratory errors have seen a 10-fold decrease over the past 5 decades through introduction of higher standardiza-tion, technology and automation. During this time, the proportion of preanalytical errors has grown from 70% to 93% of all diag-nostic errors.5–9 The threat these errors pose to scientific validity underscores the need for significant efforts to keep preanalytical errors to a minimum.
Barcode-based labeling systems have been used to improve accuracy in a variety of tasks and ensure staff follow processes.10 The development and introduction of barcode systems designed to work alongside a specific work flow have been shown to dramati-cally reduce laboratory specimen misidentifications while simul-taneously increasing protocol adherence and diagnostic efficiency in both hospital-based laboratory settings11 and community-based research in developing countries.12
The ANISA study is taking place at community-level sites in Bangladesh, India and Pakistan. The field teams collect data and biological specimens from both community-acquired cases of pos-sible serious bacterial infection and healthy controls in a variety of urban and rural settings in these countries. We assumed that the risk of preanalytical errors would be potentially high in the ANISA study because each site had different clinical and field set-tings, health practitioners and pre-existing laboratory procedures, whereby specimens would be transported to various laboratories both inside and outside the respective countries. The validity of the ANISA study findings depends on accurately detecting pathogens present in biological specimens and reliably linking these labora-tory results to the correct study participant data. Thus, we devel-oped a centrally designed barcode-based specimen labeling and tracking system and complementary customized software to iden-tify and track specimens and store data in a central database. This article describes the design and implementation of that system.
DESIGNThe key elements of the barcoded labeling system were
designed by the project coordination team located in Dhaka, Bang-ladesh. Careful customization was needed to match the project field and laboratory protocols for streamlining, integration and adoption of the new system by project staff. Furthermore, this system had to be designed to operate as a fully integrated part of the larger cus-tom-designed ANISA data management system, which was devised and supported by the ANISA Data Coordination Center.13
ANISA site teams capture data on community-acquired neonatal infection cases and healthy controls from 0 to 59 days of life, using an active and passive surveillance system, and speci-mens are drawn upon physician diagnosis without delay.14 Speci-men collection takes place at various locations ranging from for-mal hospital settings to rural community health clinics to mobile teams in households. Therefore, the specimen labeling and tracking
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S29DOI: 10.1097/INF.0000000000001103
Development and Implementation of the ANISA Labeling and Tracking System for Biological Specimens
Nicholas E. Connor, MSc,* Tanvir Hossain, MSc,* Qazi Sadeq-ur Rahman, MSc,* Mohammad Shahidul Islam, MSc,† Maksuda Islam, BA,† Belal Hossain, MSc,† Lesley McGee, PhD,‡ Maureen Helen Diaz, PhD,‡
Stephanie J. Schrag, DPhil,‡ Shams El Arifeen, DrPH,* and Samir K. Saha, PhD,† for the ANISA Methods Group
Accepted for publication January 10, 2016.From the *Centre for Child and Adolescent Health, International Centre for
Diarrhoeal Disease Research, Dhaka, Bangladesh; †Child Health Research Foundation, Dhaka, Bangladesh; and ‡Respiratory Diseases Branch, Divi-sion of Bacterial Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OppGH5307). The authors have no other funding or conflicts of inter-est to disclose.
Address for correspondence: Nicholas E. Connor, MSc, Child Health Research Foundation, 10-Ga, Road 2, Shyamoli, Dhaka 1207, Bangladesh. E-mail: [email protected].

Connor et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S30 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
procedures have to be versatile and straight forward enough to be used in a variety of field conditions.
The study physician and a trained phlebotomist are respon-sible for collection of a maximum of 3 specimen types upon diag-nosis: (i) blood; (ii) pooled nasopharyngeal and oropharyngeal (NP-OP) swabs and (iii) cerebrospinal fluid (CSF). Collection of all 3 specimen types does not always occur and is not always per-formed at the same time, in the same place or in some cases by the same practitioner. CSF samples are collected rarely, only in cases where young infants are hospitalized for suspected menin-gitis. Each of these biological specimens can be collected in up to 4 separate receptacles, requiring different processing, storage and specific shipment temperatures during transport to the laboratory. Different specimens from a single young infant follow a variety of processing paths (Fig. 1). Follow-up specimens are requested if the blood specimen yields bacteria upon culture and the child’s condi-tion has not improved or has deteriorated after 72 hours.
Once specimens are received at the laboratory, each recepta-cle is directed to different diagnostic testing pathways and the sam-ple separated accordingly into multiple aliquots. Thus, each par-ticular specimen type, episode and individual receptacle requires an identifier unique to that specific event, specimen and receptacle, and all specimens have to be reliably and inextricably linked to the individual from whom they are drawn.
Taking these conditions into account, the tracking system was designed to be reliable and accurate while following the path of each specimen and aliquot through collection, transfer to alternate receptacles during each laboratory processing step and during ship-ment between laboratories and to a biorepository. The system was intended to be as simple as possible for the end user to increase effi-ciency and accuracy and be easily adopted by partner laboratories.
System DevelopmentThe initial step in design of the labeling system was con-
sultation with the staff at the central laboratory in Dhaka. The staff determined the required areas in the protocol where labels would be useful and agreed upon a list of features that would be helpful to incorporate into the specimen tracking system. First, the labeling system had to be easily understandable, accurate and include an open field for writing additional information, such as study iden-tification number (ID), date and bacterial isolate description. Sec-ond, the labels would ideally include a color-coded band to identify specimen source type throughout the processing chain for easy
visual identification by phlebotomists, porters and laboratory tech-nicians (red for blood, green for NP-OP and gray for CSF). Labels had to be easily readable for staff and compatible with locally avail-able generic barcode scanners. The label dimensions had to fit the smallest specimen collection vessels, vials and sample tubes used in the laboratory. Labels had to be durable and easy to use and affix onto containers and laboratory paperwork. All materials used in the labels also had to be highly resistant to both the tropical heat and the extreme cold of liquid nitrogen (as high as 40°C and as low as −190°C), including the ink and adhesives, which had to remain unaffected by moisture and frost from conventional and ultra-low freezers. The system also needed to include extra labels in case midstream modification of the laboratory protocol was required. Finally, the system would preferably be low cost.
Various iterations of the specimen labeling and tracking sys-tem were reviewed and modified to ensure that laboratory staff were comfortable with plans for daily use of the end product and felt a degree of ownership in the design. During successive consultations with staff and project data programmers, a detailed standard operat-ing procedure and explanatory animated PowerPoint presentation was produced and refined to clarify both the laboratory protocol for using the labeling system and the integrated data entry steps. Feedback was obtained in the early stages to ensure smooth inte-gration of the specimen labeling and tracking system into ANISA laboratory procedures.
Label Creation and TestingWe contracted Symbology Inc. (Maple Grove, MN; www.
symbology.com) for label production and guidance in selecting appropriate materials and in other aspects of printing custom labels and barcodes. The organization provided a written guarantee that each label sheet would have a unique specimen ID with no duplica-tions. To ensure that labels would stand up to study requirements, samples were sent to the central laboratory at Dhaka and tested by simulating field and laboratory conditions. The printed barcodes were tested using locally purchased scanners in the central labora-tory before the finalization of the label orders.
All specimen labels came in sets, which were preprinted on rolls of bleached glassine backing containing 100 specimen collec-tion sets per roll, with perforations between each sheet. Each sheet contained 12 individual labels made of white polypropylene backed with an emulsion acrylic adhesive. Labels had a temperature toler-ance range of −196°C to 90°C and identical dimensions (25.4 mm
FIGURE 1. Example of specimen pathways for 1 young infant in the ANISA study. *Not taken in healthy controls. †EDTA label, anticoagulant blood sample container. ‡UTM, universal transport medium. TAC indicates TaqMan array card; TNA, total nucleic acid.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Specimen Tracking in ANISA
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S31
× 25.0 mm). Every label sheet (Fig. 2) included a header portion for writing the study ID once the sheet was assigned to a child’s specimen collection and for stapling the label set onto the specimen collection form.
Production ConsiderationsBased on extensive consultation with both laboratory and
Symbology staff, the label design was finalized, and a single custom aluminum die cast was developed to cut out the team’s specimen label sheets. The same die cast was used for each of the 3 specimen types with customized label suffix patterns for the blood, NP-OP and CSF specimens. Label rolls of 100 were printed in separate specimen-specific batches to aid in inventory control at the sites. The custom die cast had a considerable upfront cost (~US$1000), but once the die was finalized the label spools could be produced at high speed and with guaranteed accuracy to any number, reduc-ing the cost of a single label sheet to under US$0.40. Site print ranges were ordered, programmed, printed, boxed and shipped to each study site directly (Fig. 2).
Defining Label RangesAll labels required for a complete battery of tests had a
predefined specimen ID taken from the range assigned for each site. Selected ranges allow for each label set and individual label throughout the project to have a unique barcode ID. Each bar-coded label contains encoded information identifying the speci-men type, study site and specimen number (Table 1). For example, B10001-B19999 is the specimen ID range available for blood (B) samples from site 1 (Sylhet). Furthermore, each label in a set also had a label-specific suffix from 1 to 4 characters in length. These suffixes corresponded to the specific use for the particular label of that particular specimen type (Fig. 2). The suffixes were as simple as possible; for example, each label set has one label with the suffix “FORM,” indicating that it is to be used for the specimen collection form. Similarly, the “EDTA” label is always affixed to the EDTA
blood collection tube. This simple strategy clarifies for laboratory staff which label is to be used for each process for that particular specimen. Each label’s contents were both encoded into the bar-code, as well as printed on the label in 7 pt Arial font. This compo-sition ensured that every specimen, obtained anywhere in the study, had a unique specimen number and suffix to indicate the specific processing step (Table 2).
In practice, study staff can simply take a sheet of specimen labels from a color-coded roll and staple it onto the correct speci-men collection form. Specimen IDs are independently assigned so that they are neither linked to a particular ANISA child nor to any other specimens beforehand. In short, the critical linkage in the ANISA database between a child’s different specimen types is only created in the data set using the ANISA study ID upon arrival at the laboratory.
Specimen Collection and Labeling ProcessStandard specimen collection procedures were established,
and performance results were centrally monitored to ensure qual-ity and consistency.15 Project staff used collection forms stapled together with the barcode label sheets during specimen collection. The label set is first affixed to the appropriate collection form, and the young infant’s ANISA ID is written on the top portion of the specimen form and label sheet. Then the FORM barcode label is placed into the designated space on the collection form so that the specimen barcode ID and the ANISA study ID are on both docu-ments, ensuring rematching in case of detachment. Each recep-tacle is then labeled before the specimen collection attempt. The specimens are then drawn following standard procedures. Evidence shows that checklists improve both adherence to protocol and qual-ity control in other critical medical and nonmedical areas.16 There-fore, the NP-OP swabbing and phlebotomy are performed using centrally developed ANISA guidelines, which include the labeling step to standardize procedures and limit contamination before spec-imen arrival at site laboratories.17
FIGURE 2. ANISA specimen label set design elements.

Connor et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S32 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
Specimen TransportationAll labeled specimens and paired forms are transported
together promptly to the designated laboratories. The inoculated blood culture bottles and CSF specimens are kept at room tem-perature (between 20°C and 37°C), avoiding extremes, whereas the NP-OP swabs and EDTA blood tubes are kept between 4°C and 8°C during transport. In cases where immediate transport is not available, the specimens are placed in temporary incubators or refrigerators, as appropriate, until transport can be arranged. Transfer of specimens between laboratories is recorded using the ANISA specimen collection form, which records relevant information regarding collection and transport conditions.
Specimen ReceiptUpon arrival at the laboratory, the specimen collection FORM
barcode is scanned into the computer system to record specimen
receipt. The system, customized for this purpose and linked to the ANISA database, recognizes the barcode label that contains the spec-imen type, and the appropriate data entry screen for that specimen type is prompted automatically. To record and detect problems dur-ing specimen transportation, the receiving microbiologist then enters data directly into the computer from the collection form, including the arrival temperature, sample volume and sample container integ-rity. An automated time stamp of specimen arrival at the laboratory is also recorded and compared with the specimen collection time so that transport time can be calculated. The specimen ID is then paired with the ANISA ID. This first pairing event links the ANISA study participant with each of their specimens. This linkage is used in all subsequent tracking and analysis steps. Cross-confirmation using 2 or more linked numbers has been shown to substantially reduce critical errors in matching patients before blood transfusions.18 The ANISA ID is later reconfirmed with the specimen ID recorded on the
TABLE 1. Specimen Label Contents, Ranges and Specified Uses
Color Prefix Site No. Specimen No. Suffix Use of Label
B 1–6 0001-9999 -FORM Specimen collection Form 7AB 1–6 0001-9999 -BCTC Bactec bottleB 1–6 0001-9999 -EDTA EDTA tubeB 1–6 0001-9999 -BOOK Blood specimen lab bookB 1–6 0001-9999 -MLEC Molecular aliquot—record volumeB 1–6 0001-9999 -BANK Blood sample for biorepositoryB 1–6 0001-9999 -TNA Eluted TNA from MagNA PureB 1–6 0001-9999 -XFRM for TNA extraction log formB 1–6 0001-9999 -TLDA TAC processing sheetB 1–6 0001-9999 -1 Extra–Strain isolates, etc.B 1–6 0001-9999 -2 Extra–Strain isolates, etc.B 1–6 0001-9999 -3 Extra–Bactec broth from culture negativesR 1–6 0001-9999 -FORM Label specimen collection Form 7BR 1–6 0001-9999 -SWAB Label Copan UTM tubeR 1–6 0001-9999 -MLEC Label molecular aliquotR 1–6 0001-9999 -BANK Label NP-OP sample for biorepositoryR 1–6 0001-9999 -TNA Label Eluted TNA from MagNA PureR 1–6 0001-9999 -XFRM Label for TNA extraction log formR 1–6 0001-9999 -TLDA Label TAC processing sheetR 1–6 0001-9999 -1 Extra NP-OP labelR 1–6 0001-9999 -2 Extra NP-OP labelR 1–6 0001-9999 -3 Extra NP-OP labelR 1–6 0001-9999 -4 Extra NP-OP labelR 1–6 0001-9999 -5 Extra NP-OP labelC 1–6 0001-9999 -FORM Label specimen collection Form 7CC 1–6 0001-9999 -TUBE Label CSF collection tubeC 1–6 0001-9999 -BOOK Label CSF specimen lab bookC 1–6 0001-9999 -MLEC Label molecular aliquotC 1–6 0001-9999 -BANK Label blood sample for biorepositoryC 1–6 0001-9999 -TNA Label Eluted TNA from MagNA PureC 1–6 0001-9999 -XFRM Label for TNA extraction log formC 1–6 0001-9999 -TLDA Label TAC processing sheetC 1–6 0001-9999 -1 Extra CSF label—strain isolates, etc.C 1–6 0001-9999 -2 Extra CSF label—strain isolates, etc.C 1–6 0001-9999 -3 Extra CSF label—strain isolates, etc.C 1–6 0001-9999 -4 Extra CSF label—strain isolates, etc.
TABLE 2. Specimen Label Range Definitions
Numbering Range ANISA Site Print Run Blood Print Run Respiratory Print Run CSF
10001–19999 Sylhet Site 10001–12001 10001–12001 10001–1020130001–39999 Matiari Site 30001–32001 30001–32001 30001–3020140001–49999 Karachi Site 40001–42001 40001–42001 40001–4020150000–59999 Vellore Site 50001–51500 50001–51500 50001–5010060000–69999 Odisha Site 60001–61500 60001–61500 60001–60100

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Specimen Tracking in ANISA
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S33
physician assessment form to further ensure accuracy. Synchroniza-tion of the ANISA study ID with the specimen ID in the ANISA data management system is required for results of laboratory tests to then be matched with all of the information previously collected on the demographic, risk factors and medical history of the mother-child pair. Once all laboratory tests are completed, laboratory data are rou-tinely uploaded to the ANISA central database.13
Laboratory TrackingOnce specimens are successfully received and entered, the
specimen tracking system is able to follow them through each step of the laboratory protocol, including the processing of each speci-men, its location, volume, distribution into multiple aliquots and so on. Finally, the system links each of the subsequent results of con-ventional and molecular diagnostic methods. The use of barcode labels in the laboratory is made easier by the presence of barcode scanners connected directly to the molecular machinery, including the MagNA Pure Compact System (Roche Diagnostics, Indianapo-lis, IN) and the ViiA 7 Real-Time PCR System (Thermo Fisher Scientific Inc., Waltham, MA). Barcode scanners are used along with customized tracking forms and facilitate accurate recording of ANISA laboratory activities, including documentation of any deviation from the standard operating procedure. Together these systems ensure that preanalytical errors are minimized, that ANI-SA’s molecular steps are performed within the parameters of the protocol and that all results are reliably linked to the full results of the TaqMan array card (Thermo Fisher Scientific Inc.) runs in the ANISA central database.
BiorepositoryThe location of all of the stored specimens is recorded for all
sites in the custom-built ANISA data system and in the integrated biorepository software system, which relies on the barcode labels to store the various specimen aliquots. The system retains informa-tion on the count, volume, freeze-thaw events and exact locations and ages of all stored specimens across all ANISA site laboratories. This system is also color-matched with the barcode labels to ensure
simplicity and error reduction during long-term storage in the −80°C freezers (Fig. 3). Full tracking records of specimen processing and any anomalies at various steps are recorded and will be available to inform the final interpretation of the end results of the project.
DISCUSSIONThe custom ANISA specimen labeling and tracking system
along with the ANISA data capture system ensures harmonized multinational specimen collection, testing and archiving for bio-logical specimens. This system streamlines work processes in the laboratories and reduces complexity and time for laboratory staff, minimizing opportunities for preanalytical errors, and thus directly protecting valuable specimens and data.
The inherent time lag between physical collection and entry of data forms from the field creates a gap as young infants become ill very early in life; specimen receipt is often the first time that the data system captures the existence/birth of a sick (or control) neonate via the collection of specimens. This computerized system provides reliable real-time information on the project’s performance and important input for the data-based monitoring activities,19 allowing the coordination team to quickly and accurately track study progress and performance in the laboratories and clinics.
By including rigid rules for input of laboratory data into the data capture system relying heavily on the barcode labels, the system reinforces logical sequences of processing steps to be followed by staff, improving protocol adherence and maintaining a linear specimen pro-cessing protocol via integrated real-time computer entry by staff.
The extent of automation within the laboratory, especially in the molecular methodology, which employs a highly auto-mated total nucleic acid extraction platform and TaqMan array card processes, is facilitated by the barcode-based specimen labe-ling system. Integration into these automated procedures reduces or prevents preanalytical labeling errors, which can waste time, considerable resources and even misattribute specimen findings. Because specimen labels are matched with ANISA IDs and the history of the ANISA child, the results of the molecular tests are
FIGURE 3. Biorepository software screenshot.

Connor et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S34 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
directly synchronized with each ANISA child’s and mother’s data, avoiding human transcription errors.
In summary, the system standardizes laboratory protocols, assists in project monitoring and safeguards specimens and data against human errors, greatly limiting the chances for preanalytical errors, improving consistency and protecting the validity of study findings.
Potential ImprovementsIn the future, full digitization of forms in the field by using
personal digital assistants and direct electronic entry may mean that barcode-labeled specimens have even greater potential to reliably link community-based research with laboratory-based investigations. The use of machine-readable specimen labels can and should be expanded to field management and can systematically protect high-value speci-mens from human error and loss. Local production of resilient labels and guaranteed label printing runs would further cut the costs of implementing this type of system. Traditional 2-dimensional barcodes may also be improved with more advanced compound barcodes and even more versatile Radio Frequency Identification (known as RFID) labeling in the near future as prices are reduced.20 Regardless of the underlying technology, centralized design efforts must incorporate input from the staff who will be using the labeling system to improve adoption, understanding and confidence in these types of systems.
ACKNOWLEDGMENTSThe authors gratefully acknowledge the technical assistance
and team work of Mr. Mahmudur Rahman, Ms. Mahfuza Marzan, Mr. Iftekhar Rafiquillah and Mr. Md. Hasanuzzaman. They also acknowledge our numerous other talented and supportive col-leagues at the Child Health Research Foundation, the icddr,b and the Centers for Disease Control and Prevention, Atlanta.
REFERENCES 1. Plebani M. Quality indicators to detect pre-analytical errors in laboratory
testing. Clin Biochem Rev. 2012;33:85–88.
2. Murphy MF, Kay JD. Patient identification: problems and potential solu-tions. Vox Sang. 2004;87(suppl 2):197–202.
3. Lippi G, Blanckaert N, Bonini P, et al. Causes, consequences, detection, and prevention of identification errors in laboratory diagnostics. Clin Chem Lab Med. 2009;47:143–153.
4. Dzik WH, Murphy MF, Andreu G, et al.; Biomedical Excellence for Safer Transfusion (BEST) Working Party of the International Society for Blood
Transfusion. An international study of the performance of sample collection from patients. Vox Sang. 2003;85:40–47.
5. Lippi G, Becan-McBride K, Behúlová D, et al. Preanalytical quality improvement: in quality we trust. Clin Chem Lab Med. 2013;51:229–241.
6. Plebani M. Exploring the iceberg of errors in laboratory medicine. Clin Chim Acta. 2009;404:16–23.
7. Lippi G, Guidi GC, Mattiuzzi C, et al. Preanalytical variability: the dark side of the moon in laboratory testing. Clin Chem Lab Med. 2006;44:358–365.
8. Lippi G, Chance JJ, Church S, et al. Preanalytical quality improvement: from dream to reality. Clin Chem Lab Med. 2011;49:1113–1126.
9. Plebani M. The detection and prevention of errors in laboratory medicine. Ann Clin Biochem. 2010;47(pt 2):101–110.
10. Murphy MF, Kay JD. Barcode identification for transfusion safety. Curr Opin Hematol. 2004;11:334–338.
11. Zarbo RJ, Tuthill JM, D’Angelo R, et al. The Henry Ford Production System: reduction of surgical pathology in-process misidentification defects by bar code-specified work process standardization. Am J Clin Pathol. 2009;131:468–477.
12. Avilés W, Ortega O, Kuan G, et al. Quantitative assessment of the benefits of specific information technologies applied to clinical studies in developing countries. Am J Trop Med Hyg. 2008;78:311–315.
13. Rahman QS, Islam MS, Hossain B, et al. Centralized data management in a multicountry, multisite population-based study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S23–S28.
14. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
15. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35 (Suppl 1):S39–S44.
16. Ely JW, Graber ML, Croskerry P. Checklists to reduce diagnostic errors. Acad Med. 2011;86:307–313.
17. Hossain B, Weber MW, Hamer DH, et al. Classification of blood culture iso-lates into contaminants and pathogens on the basis of clinical and laboratory data. Pediatr Infect Dis J. 2016;35 (Suppl 1):S52–S54.
18. Askeland RW, McGrane S, Levitt JS, et al. Improving transfusion safety: implementation of a comprehensive computerized bar code-based tracking system for detecting and preventing errors. Transfusion. 2008;48:1308–1317.
19. Connor NE, Manary MJ, Maleta K. Monitoring the adequacy of catch-up growth among moderately malnourished children receiving home-based therapy using mid-upper arm circumference in southern Malawi. Matern Child Health J. 2011;15:980–984.
20. Shim H, Uh Y, Lee SH, et al. A new specimen management system using RFID technology. J Med Syst. 2011;35:1403–1412.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S35
Supplement
Background: The Aetiology of Neonatal Infection in South Asia (ANISA) study takes advantage of text messaging technology to record information required for randomizing the study population into a control subcohort. The text message system is also used for monitoring various study activities.Methods: When a child-health worker registers a newborn in the study, she sends a text message to a database server containing the study identification number and newborn’s age at the time of registration. For each possible seri-ous bacterial infection case, a study physician also sends a text message to the same server with the age of the young infant at the time of illness assess-ment. Using this information, a computer-based algorithm randomizes the newborn into a control subcohort. Text messages are also sent to alert the study physicians and study supervisors of a possible serious bacterial infec-tion case being referred to health-care facilities. Phlebotomists working at remote specimen collection sites send text messages to the site laboratory personnel before sending the specimens through porters.Discussion: Real-time data entry and monitoring are challenging for any population-based study conducted in remote areas. Our text messaging sys-tem provides an opportunity to overcome this barrier where availability of data entry facilities is limited.
Key Words: text message, healthy control, ANISA, seasonality, age-matched
(Pediatr Infect Dis J 2016;35:S35–S38)
The Aetiology of Neonatal Infection in South Asia (ANISA) study collects blood and nasopharyngeal–oropharyngeal (NP–
OP) swab specimens from young infants with community-acquired possible serious bacterial infection (pSBI). These young infants are identified through active surveillance by community-health work-ers (CHWs) and through referral to physicians at 5 study sites in Bangladesh, India and Pakistan. The ANISA study team has devel-oped procedures for evaluating the strength of the epidemiological association between pathogen presence in the clinical specimens
obtained from ill-appearing young infants and the risk of their ill-ness in that community. A critical challenge is the expectation that many of the same pathogens found in sick young infants may also be detected in specimens from healthy ones although possibly at a lower rate.1 Many of the target viruses and bacteria are also part of the normal flora in the naso-oropharynx of this age group.2–5 Hence, in this study, we collect blood and NP–OP swab specimens from a control subcohort of enrolled healthy young infants. For selecting this subcohort, we use mobile phone text message (often referred to as “SMS”) technology. Although this system was ini-tially introduced in ANISA for selecting and enrolling the control subcohort, we have extended its use to real-time critical data cap-ture. In this article, we describe our experience with using text messages in ANISA.
ANISA STUDY METHODSA CHW visits every household in her study area once
every 2 months to identify and register pregnant women. She fol-lows every newborn on days 0, 2, 6, 13, 20, 27, 34, 42, 48 and 59 after birth, making a total of 10 postnatal home visits. If a CHW determines any young infant to be sick based on predefined clinical criteria, she refers the child to a specific facility for reassessment by a study physician. If the physician confirms the young infant (either referred by a CHW or self-referred) as a case of pSBI, blood and NP–OP specimens are collected after written consent from the newborn’s legal guardian. The detailed methodology of the preg-nancy and newborn surveillance activities for this study has been described elsewhere in this supplement.6
CONTROL SELECTION CRITERIAIn ANISA, control specimens are collected matching
3 features of the cases. First, we considered that ANISA field sites are geographically distinct and present different pathogen sets. Thus, each study field site was considered its own stratum, and we planned to collect equal numbers of controls from each study site. Young infant infection and mortality data from South Asia, as well as historical data from industrialized countries, show a dispropor-tionately high incidence of early-onset versus late-onset sepsis.7,8 In addition, many pathogens, particularly viral respiratory pathogens, have a distinct seasonality.9 Because of this association between age and infection, we collect control specimens matching the dis-tribution of young infants’ ages when they become sick. Finally, for seasonal matching of cases, in each calendar month a certain number of enrolled newborns are selected for the control subco-hort; this number is proportionate to the total number of live births in that month.
Operational Challenges With Control SelectionBy design, all ANISA study data are collected using paper-
based forms, which results in a significant lag between actual data collection and entry into the database. During study design, we were particularly concerned that newborns registered at age 0 or 2 days should have a specific probability of being selected as
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S35DOI: 10.1097/INF.0000000000001104
Using Text Messages for Critical Real-time Data Capture in the ANISA Study
Mohammad Shahidul Islam, MSc,* Qazi Sadeq-ur Rahman, MSc,† Tanvir Hossain, MSc,† Nicholas E. Connor, MSc,† Belal Hossain, MSc,* Md. Mahmudur Rahman, MSc,* Ranjan Neogi, MCom,‡
Samir K. Saha, PhD,* and Shams El Arifeen, DrPH†
Accepted for publication January 10, 2016. From the *Department of Microbiology, Child Health Research Foundation,
Dhaka, Bangladesh; †Centre for Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh; and ‡CSL Software Resources Ltd., Dhaka, Bangladesh.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Shams El Arifeen, DrPH, Centre for Child and Adolescent Health, icddr,b, Mohakhali, Dhaka-1212, Bangladesh. E-mail: [email protected].
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s website (www.pidj.com).

Islam et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S36 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
healthy controls at that age. This probability is conditional to the age distribution of pSBI cases and seasonal distribution of births. It would be difficult to carry this out without selection bias, given the delay in entering data from paper-based forms. Therefore, we opted for the mobile phone text message as a technological solu-tion. This choice was driven by the simplicity of the technology, expected skills of the CHWs, and widespread availability and use of mobile phones in the targeted communities. The communities in the study sites have very few areas with no mobile phone coverage. An additional advantage of using text messages is that the technol-ogy works exactly the same way in all 5 ANISA study sites in 3 different countries and is compatible with all mobile phones.
CRITICAL STEPS FOR EFFECTIVE USE OF TEXT MESSAGES
Selecting healthy controls using text messages involves 3 steps: sending a text message for registration of a newborn in the database, running an algorithm based on selected data and generating a feedback text message to the CHW with the control selection status of the newborn (control or not control). The procedure is described in Figure 1. For these 3 steps to work and all data to link correctly at the time the newborn registration text message is sent, the database must receive the pregnancy registration information before sending the newborn registration text message. This is a challenge for ANISA because there is a delay in entry of the paper-based data capture forms
(DCFs). Therefore, a CHW must also send a text message when enrolling a pregnant woman. This text message registers the preg-nancy in the database in real time and creates a record that is linked to the newborn registration ID. If any newborn registration ID does not correlate with the corresponding pregnancy ID, the server does not accept the newborn ID, and the data are not processed. The sec-ond step involves the need to frequency match the age of the controls for providing specimens for the age distribution of pSBI cases with successful collection of blood and/or NP–OP specimens. We use the age distribution of pSBI cases as of the week before (to account for seasonality) the newborn is enrolled. Thus, upon enrollment and suc-cessful collection of specimens from a pSBI case, the study physician also sends a text message to the database server including the age of the young infant at the time of assessment. The control selection process is also self-adjustable with actual healthy control enrollment rates, particularly when there are shortfalls from the previous month.
Sending Text Messages to the Data ServerTo address the 3 required steps mentioned earlier, a CHW
sends a text message to a site-specific phone number at the time of registration of a pregnant woman or a newborn in the ANISA study. These messages include the mother’s ID and the newborn’s age. The study physician also sends a text message with the age of the newborn to the same phone number when he/she is success-fully enrolled as a pSBI case or as a healthy control. Table 1 shows the different text message formats used in this system. A General
FIGURE 1. Architecture of text message system and control selection process in ANISA.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Real-time Data Capture
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S37
Packet Radio Service (known as GPRS) modem is used for text message transmission and data transfer to the site’s server.
RANDOMIZATION OF NEWBORNSUsing an algorithm developed by the ANISA Data Coordina-
tion Center, a site’s server randomizes each newborn at the time of registration into one of 2 subcohorts10: the control subcohort where the selected newborn will be asked to provide a NP–OP specimen or the noncontrol subcohort where the selected newborn will not need to provide clinical specimens unless he/she becomes sick. If a newborn is selected into the control subcohort, the algorithm deter-mines at which age the newborn is required to provide specimens. This age will always coincide with the CHW home visits scheduled for that newborn. Once the randomization and date assignment pro-cess are complete, the server generates a return text message to inform the CHW to which subcohort that particular newborn will belong; and if selected for the control subcohort, at what age the selected newborn should provide specimens.
Principles of the Algorithm Used for Randomization
We decided to collect 400 control specimens (NP–OP) from each site. We estimated that the total number of registered newborns over a period of 2 years in each of the 5 study sites would range between 6000 and 20000. Therefore, between 2% and 7% of the reg-istered newborns would need to provide specimens as healthy con-trols (referred to as the site-specific base probability). This probabil-ity is first equally divided (by 10) across all 10 visit ages. The (visit) age-specific base probability is adjusted every week according to the age distribution of enrolled cases up to the previous week. Because the actual ages of case enrollment differ from the visit ages, we cre-ated non-overlapping time frames around each scheduled visit age with no gaps between consecutive time frames. At this point in the process, the algorithm ensures that controls and cases are frequency-matched by age and season. The sum of all adjusted visit age-specific base probability adds up exactly to the overall base probability for the site (between 4% and 7%). This probability is adjusted based on the failure rate in the control specimen collection and any shortfall in actual cumulative enrollment up to the preceding week. A final adjustment (+3% additional selection) is made to allow for the con-trols that are eventually excluded by becoming ill within 7 days of control specimen collection. The number of births in most South Asian populations shows strong seasonality, usually peaking in late autumn and early winter. To adjust site-specific base selection prob-ability for each week, we used historical records of seasonal varia-tion in the number of births from each site to estimate the number of births expected and controls to be selected in each calendar week.
Step-by-step details of the algorithm are presented in Sup-plemental Digital Content 1, http://links.lww.com/INF/C405.
PROBLEMS AND SOLUTIONSWe identified several problems with using text messages
in ANISA surveillance. The number of selected controls and their
proportionality to the age distribution of cases may be jeopardized if study physicians fail to send text messages consistently. As indi-cated earlier, this input is 1 of the 2 critical steps for the control selection process. In addition, the parents of a significant propor-tion of selected young infants refuse to provide control specimens on the particular day for which they are selected by the system. The actual rate of refusal in enrolling controls (75%), is consider-ably higher than the assumption (30%) when designing the study. We increased the base control selection probability in 2 stages to account for the control enrollment failure. Another issue is that the data server calculates the age of an enrolled newborn when it receives a text message from a CHW. If there is a problem with phone network connectivity, the CHW will not receive any reply text message. To address this issue, we created an option in the ANISA data entry system to allow direct manual input of text mes-sages by data management staff after CHWs provide the relevant information over the phone.
EXTENDED USE OF TEXT MESSAGESThe 3 steps of the control selection process prompt several
additional uses of text messages, especially in real-time monitoring of critical study performance indicators. The real-time data generated by the text messages enable study coordinators and supervisors to keep track of pregnancies and newborns being registered and cases and controls being enrolled in the study. The data are disaggregated by a supervisor and the CHW, enabling identification of staff in need of additional support, monitoring and training. The data from text messages help monitor the data entry lag and locate missing forms. Initially, the average delay in entry of the newborn registration DCFs was over 60 days, which has decreased to fewer than 40 days with continuous monitoring through the text message data uploaded to the server (Fig. 2). Figure 3 shows the numbers of pregnancies recorded in the database from text messages and paper-based DCFs at 4 different time points. This chart is characterized by dips in
TABLE 1. Text Message Formats for Updating the Database on ANISA Surveillance Activities
Type of Text Message Text Message Formats Sender
Pregnancy registration P Middle five digit of Study ID CHWNewborn registration C Middle five digit of Study ID # Child serial # Child Age CHWSuspected PSBI case referral by CHW R Middle five digit of Study ID # Child serial CHWHealthy control enrollment (with specimen) H Middle five digit of Study ID # Child serial # Child Age PhysicianPSBI case enrollment (with specimen) S Middle five digit of Study ID # Child serial # Child Age Physician
FIGURE 2. Monthly mean time lag between registration of birth with text messages and data entry from paper-based DCFs, March 2012–November 2013.

Islam et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S38 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
the 2 or 3 months before each peak. Also, in the first month (June 2012), the low pregnancy registration rate indicates that the study site data teams were still learning to manage the processing of the paper-based DCFs. The text message system helps in reducing the workload of project staff, as study physicians receive alert messages before referral, so that they do not have to be available on-site around the clock. This is particularly helpful during holidays. Similarly, text messages alert the laboratory staff about the arrival of specimens. As ANISA study sites include remote areas and specimens are collected around the clock, laboratory staff need to be informed in advance about incoming specimens and tentative times of arrival so that they can prepare for specimen processing. Finally, using the text message data, study supervisors can track young infants who do not comply with referral and arrange follow-up visits.
SUMMARYUse of text messages for health purposes has mostly occurred
in developed countries while the experience from low-income coun-tries remains mostly anecdotal although some recent studies have used text message systems to collect data from communities. In ANISA, we are using a text message system in a large cohort for
real-time data entry and monitoring study progress in resource-poor settings. The methodology described in this paper allows us to rand-omize the newborns enrolled in the study based on age and seasonal distribution of cases. In addition, this system is very useful in off-site study supervision and monitoring. We believe that extended use of this mobile phone technology in community-based public health research can improve study performance and data quality.
ACKNOWLEDGMENTSThe authors gratefully acknowledge the financial support of
the Bill & Melinda Gates Foundation as well as the technical assis-tance of our colleagues at the Child Health Research Foundation, Dhaka, the International Centre for Diarrhoeal Disease Research, Bangladesh and the Centers for Disease Control and Prevention.
REFERENCES 1. Jansen RR, Wieringa J, Koekkoek SM, et al. Frequent detection of respira-
tory viruses without symptoms: toward defining clinically relevant cutoff values. J Clin Microbiol. 2011;49:2631–2636.
2. Bosch AA, Biesbroek G, Trzcinski K, et al. Viral and bacterial interactions in the upper respiratory tract. PLoS Pathog. 2013;9:e1003057.
3. Mathisen M, Strand TA, Valentiner-Branth P, et al. Respiratory viruses in nepalese children with and without pneumonia: a case-control study. Pediatr Infect Dis J. 2010;29:731–735.
4. Bogaert D, van Belkum A, Sluijter M, et al. Colonisation by Streptococcus pneumoniae and Staphylococcus aureus in healthy children. Lancet. 2004;363:1871–1872.
5. Robinson J. Colonization and infection of the respiratory tract: What do we know? Paediatr Child Health. 2004;9:21–24.
6. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
7. Stoll BJ, Hansen NI, Sánchez PJ, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011;127:817–826.
8. Bizzarro MJ, Raskind C, Baltimore RS, et al. Seventy-five years of neonatal sepsis at Yale: 1928-2003. Pediatrics. 2005;116:595–602.
9. Gardinassi LG, Marques Simas PV, Salomão JB, et al. Seasonality of viral respiratory infections in southeast of Brazil: the influence of temperature and air humidity. Braz J Microbiol. 2012;43:98–108.
10. Rahman QS, Islam MS, Hossain B, et al. Centralized data management in a multicountry, multisite population-based study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S23–S28.
FIGURE 3. Number of pregnancies recorded in the database from text messages and from paper-based form entry, May 2012 –December 2013 (Bangladesh and Pakistan sites).

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S39
Supplement
Background: The Aetiology of Neonatal Infection in South Asia (ANISA) study maintains operations in Bangladesh, India and Pakistan. We developed and deployed a multilayered monitoring system to measure performance indicators of field sites and laboratory operations. This system allows for real-time provision of feedback to study site teams and project stakeholders. The goal of this monitoring and evaluation system is to promote optimal per-formance and consistency in protocol application at all sites over the course of the study, thereby safeguarding the validity of project findings. This article describes each of the interdependent monitoring layers that were conceptual-ized, developed and employed by the ANISA coordination team.Methods: Layers of monitoring include site-level, central and database-related activities along with periodic site visitation. We provide a number of real-world examples of how feedback from the ANISA monitoring system directly informs a number of crucial decisions and course corrections dur-ing the project.Conclusion: The ANISA monitoring system represents a transparent, understandable and practical resource for development of project monitor-ing systems in complex multisite health research projects.
Key Words: monitoring and evaluation, multi-site, ANISA, neonatal, surveillance, project design
(Pediatr Infect Dis J 2016;35:S39–S44)
The Aetiology of Neonatal Infection in South Asia (ANISA) study is designed to collect high quality demographic, epi-
demiological, clinical and microbiological data to describe the
risk factors and etiology of young infant infections in South Asian communities. This project captures infection cases in the community from the first day of life up to 2 months of age (0–59 days) in a mix of periurban and rural settings.1 The project team is composed of local field and laboratory staff at study sites in Bangladesh, India and Pakistan led by pediatric and global health experts, whereas overall activities are coordinated by the Child Health Research Foundation (CHRF), located in Dhaka, Bangladesh. The monitoring activities operate under the close oversight and guid-ance of the project principal investigator (PI) and the project coordi-nation team, which includes personnel from the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), the World Health Organization and the U.S. Centers for Disease Control and Prevention (CDC). An external Technical Advisory Group provides advice to the PI and coordination team. The study’s findings will be used to inform meaningful strategies to improve child survival.2
ANISA’s combination of intensive pregnancy and neona-tal infection surveillance, referral, clinical assessment, specimen collection from both cases and controls and diagnostic laboratory activities is complicated.3 Furthermore, the project is conducted under different conditions and preexisting management structures at each site. Managing this complexity and achieving project goals necessitates harmonization of key project activities by using a com-prehensive monitoring and evaluation system.
STUDY OPERATIONSThe ANISA study is located at 5 sites: Karachi and Matiari
in Pakistan; Odisha and Vellore in India and Sylhet in Bangladesh. In total, the study employs nearly 400 community health workers (CHWs), myriad laboratory staff, clinicians, nurses, phlebotomists, researchers, adjunct staff and site managers. Community-based possible serious bacterial infection (pSBI) surveillance takes place at sites that have a total population of over 2 million and repre-sent a broad cross-section of the South Asian population.3 CHWs and clinicians fill out a set of data collection forms for each study participant. A centrally designed specimen labeling and tracking system records details of specimens drawn from cases and healthy controls, from collection to diagnostic testing.4 Standardized labo-ratory forms are also used to record each logical step of the diag-nostic procedures performed on each specimen type.
A standard data capture system was developed to record data collection forms from the field, as well as from the laboratory data collection forms, which are all uploaded weekly to the central study database in Dhaka. The ANISA data system also includes a customized text message system that operates in real time to select healthy controls in the field.5
The strength of the ANISA study rests on the expertise of its partner sites that were chosen based on their experience in con-ducting population-based maternal and child health studies in their
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S39DOI: 10.1097/INF.0000000000001105
Methods Employed in Monitoring and Evaluating Field and Laboratory Systems in the ANISA Study
Ensuring Quality
Nicholas E. Connor, MSc,* Mohammad Shahidul Islam, MSc,† Melissa L. Arvay, MPH,‡ Abdullah H. Baqui, DrPH,§ Anita K. Zaidi, SM,¶ Sajid B. Soofi, FCPS,¶ Pinaki Panigrahi, PhD,║
Anuradha Bose, MD,** Maksuda Islam, BA,† Shams El Arifeen, DrPH,* Samir K. Saha, PhD,† and Shamim A. Qazi, PhD,†† for the ANISA Methods Group
Accepted for publication January 10, 2016. From the *Centre for Child and Adolescent Health, International Centre for Diar-
rhoeal Disease Research, Dhaka, Bangladesh; †Child Health Research Founda-tion, Dhaka, Bangladesh; ‡Centers for Disease Control and Prevention, Atlanta, Georgia; §Department of International Health, International Center for Maternal and Newborn Health, Johns Hopkins Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; ¶The Aga Khan University, Karachi, Pakistan; ║Center for Global Health and Development, College of Public Health, University of Nebraska Medical Center, Omaha, Nebraska; **Christian Medi-cal College, Vellore, India; and ††Department of Maternal, Newborn, Child and Adolescent Health, World Health Organization, Geneva, Switzerland.
The members of the ANISA Methods Group are listed in the Acknowledgments. The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No.
OppGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Nicholas E. Connor, MSc, Child Health Research Foundation, 10-Ga, Road-2, Shyamoli, Dhaka-1207, Bangladesh. E-mail: [email protected].

Connor et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S40 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
communities.2,3,6–13 Although the coordination team in Dhaka has to ensure that the protocol is properly implemented, the team relies on the experience and innovation of the site teams to apply the pro-tocol and fulfill study objectives while taking local conditions into account. Thus, the monitoring and evaluation system needs to be vigilant enough to provide useful feedback to sites while taking their different contexts into account.
DESIGN OF THE MONITORING STRUCTUREThe ANISA project employs a 4-level monitoring struc-
ture, which can be conceptualized as a pyramid, with the base sup-porting and informing the subsequent higher layers. Internal qual-ity assurance/quality control (QA/QC) activities are conducted on a weekly basis by site personnel. These activities underpin the figures in the monthly reports that are returned to the coordina-tion team. An additional layer of monitoring through a series of queries to the database is repeated on a bimonthly basis to moni-tor adherence to protocols. Lastly, periodic site visits ensure that the aforementioned monitoring activities are working properly (Fig. 1). This system provides a common platform for collection of monitoring information and informs questions and feedback between the Coordination Center in Dhaka, its affiliates (icddr,b and CDC) and the field and laboratory teams (Fig. 2). This feed-back allows for detailed, confident reporting of study progress to the coordination center via web conferences, and from Dhaka to other study stakeholders.
Level 1: Internal Routine Site QA/QC ChecksThe base of the monitoring pyramid relies on direct site-
level QA/QC of all field and laboratory activities. Although man-agement structures vary by site, the basic field hierarchy involves site managers overseeing field supervisors, who then oversee the CHW supervisors, who in turn oversee the CHWs.
Among CHWs, supervision and auditing with feedback are effective in achieving and maintaining high-quality performance, and having several parallel support and monitoring techniques improves and maintains performance levels.14 Therefore, ANISA project sites employ various mutually supportive methods to ensure optimal continued performance of CHWs. These methods include routine data collection form rechecking and random observations of visits by supervisors, who subsequently provide feedback or re-training to CHWs to improve and maintain performance. CHW home visits are observed by supervisors, who also conduct random independent visits at a subset of households to re-check the CHW’s assessment accuracy and data collection form entry. The coordina-tion team provides guidelines, including minimum frequencies of random and systematic checks, although sites are free to increase their oversight in this regard (Table 1). Additionally, refresher train-ing is provided via both regular and targeted retraining to maintain quality of young infant assessment and record-keeping skills over time. Common inconsistencies found in the on-site data centers are relayed to field management, so that they can identify the source of these errors and correct problems in filling out the data collection forms. Together, these internal site QA/QC techniques allow for rapid detection and correction of issues and serve to safeguard the quality of study data.
All sites face different contextual challenges, including dif-ferent levels of in-migration and out-migration, internal movement of pregnant women, traffic conditions, weather, law-and-order situ-ations as well as unique geographical features. Study staff address these challenges by employing locally appropriate strategies. Strong internal site QA, setting realistic site-specific targets for activities and ongoing community engagement create a system of accountability and project ownership at the site level, forming the strong base of the monitoring and evaluation pyramid.
Level 2: Performance Monitoring via Monthly Field and Laboratory Report Forms
The primary goal of the study is the collection and analy-sis of a representative sample of quality biological specimens from both sick young infants showing signs of pSBI and healthy control infants, in the first 59 days of life in community settings. Achiev-ing this goal involves coordination of research activities in the field and laboratories via continuous monitoring of a number of perfor-mance indicators. These indicators are connected through a chain of dependent activities at each site, starting from recruitment of participants and scheduled visitation, toward the successful collec-tion and processing of specimens. Each stage of the workflow may potentially act as a bottleneck and limit the overall field success and thus the representativeness of the study, threatening the valid-ity of findings. The coordination team monitors activities using quantitative report forms submitted by the sites on a monthly basis. These forms contain 64 numerical elements of the field (40) and laboratory (24) components with specific significance to project performance (Table 2). Laboratory forms capture key numbers, samples tested, bacterial isolates from blood culture and molecular test results.
FIGURE 1. ANISA monitoring pyramid.
FIGURE 2. Monitoring and feedback structure and stakeholders.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Ensuring Quality
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S41
Monthly report evaluation is performed across all sites using simple, transparent formulae allowing for the pooling and cross-comparison of overall project performance data. When evaluating these forms, readily interpretable estimates are used to show per-formance, initiate dialogue, and encourage site teams to continue real progress or undertake appropriate corrective actions where indicated. The economy of elements in field and laboratory activi-ties and straightforward evaluation and feedback are preferable in our multisite study to more complex calculations, which could lead to disagreements about the calculations, rather than a discussion of underlying performance.
The monthly monitoring reports are collected from all sites within 10 days of the end of the preceding month. The figures from these reports are recorded in Microsoft Excel, which is used to pro-duce routine performance charts each month. This method provides a comparison of the same metrics against both the study targets and performance of the site in previous months. Charts and figures are reviewed and shared; monthly declines in performance of over 10% in any of the critical areas or other interesting trends are routinely discussed with each respective site during conference calls.
Level 3: Database-based MonitoringAll completed field data collection forms and laboratory
results are uploaded to a central database and are available for anal-ysis by the coordination team to support monitoring and evaluation activities. Querying incoming data allows for more in-depth moni-toring of field, clinical and laboratory performance than is possible via the monthly reports. The database query also helps determine if
a site’s data upload quantity and quality are being maintained and are consistent with expectations.
Database frequency tables of entered forms are routinely cross-compared with the expected number of forms collected and studied alongside the monthly reports. This cross-comparison is key to evaluating a site’s data entry performance and to avoid any large form entry backlog.
The quality of the incoming data is scrutinized using (i) the proportion of data collection forms that undergo the required double entry and (ii) automated internal consistency and logical checking algorithms. Feedback tables are regularly shared with data personnel and site teams to ensure early resolu-tion of problems. We utilize historical data on field activities, detected clinical signs and real-time data found in the text mes-sage system, which synchronizes with the data server daily to detect births, case diagnoses and control enrollment. Together these data sets are scrutinized, and feedback is provided to sites. With the help of the site teams, appropriate inquiries and solutions are devised by cross-comparing monthly monitoring forms, the database and the text message data. Table 3 illustrates how we used the database to identify and solve problems related to healthy control selection.
Project laboratory data are entered into the site database directly by the laboratory staff. These data are securely trans-mitted to the coordination center and subsequently to CDC for in-depth analysis, evaluation, detailed feedback and suggestions for resolution of problems found in processing and analysis of specimens. The project database allows the coordination team
TABLE 1. Minimum Internal Monitoring Guidelines
Monitoring Method and Responsible Person(s) Minimum Random Check Guidelines for Monitored Field Activities
CHW Home Visits Sick Infant Assessment
Supervisor-observed CHW visits 5% 5%Independent Supervisor visits (without the CHW) 1.5% 5%Random checks by field supervisor Monthly MonthlyData-driven checks by field supervisor As indicated by supervisor As indicated by supervisorTreatment outcome follow-up by field supervisor N/A Monthly
TABLE 2. Elements of the Monthly Reporting Forms
Monitoring Metric Study Element Use for Feedback
Population under surveillance MWRAs under surveillance Active site MWRA catchment figure, implementationStudy Population New pregnancies identified Fertility trend
Live births identified Denominator for enrollmentEnrollments (total) from 0 to 6 d Proportion of enrollments over live births identifiedEnrollment failure Common reasons for failure to enroll, proportion of failuresEnrollment ending/withdrawal Participants who are no longer in the study: lost to follow-up, deaths
and normal study completionTiming of first assessment Under 6, 12 and 24 hr Charting performance of site teams in reaching infants early in life,
when sepsis onset is most commonReferral success CHW referrals CHW referral frequency
Referral compliance Number of participants compliedAssessment and treatment Physician confirmation Number of physician-confirmed cases from both CHWs and
self-referralsTreatment Ethics complianceHospitalizations Hospitalization provided
Consent to specimen collection Cases and controls Cases with physician-confirmed pSBI (or controls) who give consent for specimen collection, acceptability of sampling
Count of specimens collected from cases and controls
Blood Sampling successNasopharyngeal–oropharyngeal swab Sampling successCerebrospinal fluid Sampling successCollected from infants who later died Indicator of how well site is capturing the most hard-to-reach cases
MWRA indicates married women of reproductive age (13–49 years).

Connor et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S42 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
to confirm and detail issues detected by the monthly monitoring reports, streamline data capture, ensure data quality and inform CDC of all relevant laboratory details for evaluation and feed-back.
Level 4: Site VisitsAlthough local, monthly and data monitoring and evaluation
activities provide the coordination team with copious monitoring
data, there is no alternative for meeting with and observing project personnel in action. Thus, periodic visits are made to the study sites by internal and external monitors to observe implementation of the protocol, the daily activities of staff operating in the community, health care facilities, data centers and study laboratories. Internal monitors are selected from the ANISA coordination team and pro-ject administrators, whereas external monitors are subject matter experts from the World Health Organization, the Hospital for Sick Children in Toronto, CDC and other affiliated organizations with expertise in critical appraisal of similar projects in complex field and laboratory environments.
These visits are informed by monthly database monitor-ing activities and provide further information on site functionality, workflow, staff skills and other practical issues.
The monitors write comprehensive visit reports, which are reviewed and shared with the coordination team and the site leaders for discussion and prompt resolution of detected issues. External monitors also provide expert advice and ideas that are beneficial to project implementation at the site. A standard list of project ele-ments is checked during these visits (Table 4), including logistical aspects. Site visits are scheduled once or twice a year and are indis-pensable for detecting and resolving issues.
Both internal and external monitors are briefed in detail before these visits and provided with site-specific recommenda-tions generated by previous visits and current database and monthly monitoring reports. Site visits present a unique opportunity to build rapport, provide feedback to sites and solve in person any pending
TABLE 3. Text Message Frequency Correction
The coordination team found that there had been a low number of healthy control enrollments after evaluating monthly reporting forms, suggesting that the control algorithm was not selecting enough controls. If the algorithm did not work as planned it would be detrimental to the overall project design. Thankfully, all data related to the text message-mediated control selection algorithm were available in the central database. The monthly reports were cross-checked with data on text messaging to determine why the selection of the controls was not working as planned. It was quickly determined that the algorithm program was in fact working properly; however, the number of sick cases was underreported because of lagging physician text messages. Upon discussion with the site and presentation of this information, the site teams reinforced the importance of the text message system in the overall study design. The selection of controls recovered up to the desired level over the subsequent months.
TABLE 4. Routine Elements for the Study Protocol Adherence Review for Site Visits
Element Aspect to Review
Study documentation Updated protocols and amendments availableStudy manual availableStandard operating procedures available to staffConsent forms up to dateIRB approval letters in placeDocuments stored properly in designated cabinets with adequate space
Study progress Expected no. of enrollments versus actual enrollmentsReferral rates and referral compliance ratesPhysician assessment and pSBI confirmation rates
Screening of participants Observation of CHW screenings—proficiency, manner and expertiseObservation of physician screenings—proficiency, manner and expertiseChecking of register and assessment documentation—completeness, systemMaintenance of follow-up visit calendar—check in detailFrequency of data collection form submission, backlog
Culture laboratory Transportation and receipt of blood specimens from fieldProcess in laboratory for tracking of specimens (barcode scanning)Processes followed in using automated blood culture machinesUse of ANISA laboratory books in culture of blood and cerebrospinal fluid
processing, and characterization of isolatesMolecular laboratory Timing and processes for aliquoting of molecular specimens
Molecular processing—storage, extraction and testing of molecular speci-mens, interpretation and QA/QC
Procedures to prepare specimens for biorepositoryData management Data entry facilities, staffing
Number of forms due, completed, enteredRegular transmission of data to the central database; expected/actual and
backlog from both field and laboratory dataStorage sites for hard data and soft dataFrequency of backup (date of last backup)Completeness and internal checking systems (10–20% data collection forms)
Communications Frequency of communications with the coordination teamFrequency of communications with site PIDates of last communications with coordination team
Funds utilization Expected expenditure/actual expenditure*Inventory control and procurement
Serious adverse events Check of all serious adverse events and systems to report them
*Request site leaders to justify any variance over 10%.IRB indicates institutional review board.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Ensuring Quality
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S43
issues flagged by other monitoring activities. Feedback from these visits and recommendations for improvement of protocol applica-tion are shared with the sites and stakeholders, so appropriate reme-dial actions can be agreed together with the site leaders.
APPLICATION AND UTILITY OF THE MONITORING STRUCTURE—THE ANISA EXPERIENCE
Pilot StudyThe pilot phase of the study was implemented at each
ANISA site. All study physicians, support and laboratory staff and data entry personnel used this time period to become famil-iar with the protocol and to gain proficiency working together in implementing it, identifying issues, and providing feedback to the coordination team. Critically, the monitoring system was in place, and monitoring data were collected from the beginning of the pilot phase. The pilot phase also allowed for refinement and improvement of the elements within the monitoring tools and analysis techniques used.
The pilot phase involved monitoring key performance ele-ments such as the timing of the first assessment of the newborn after delivery, the proportion of successful referrals, levels of consent to specimen collection, timing of specimens reaching the laboratory and blood contamination rates. For the sites in Bangladesh and Paki-stan, basic thresholds were agreed upon by the respective site PIs and the coordination team to indicate whether the site was operating satisfactorily (Table 5). Based on evaluation of this site performance data, the site leaders and the coordination team agreed upon the end date of the pilot phase and commencement of the main study at that site in a retrospective manner (see Fig. 3 for more details)
For the sites in Bangladesh and Pakistan, the earliest sites to commence, the pilot phase was retroactively defined (as explained above), but the Indian sites undertook a predefined pilot period of 1 month as they started much later and had the benefit of joining the study after extensive streamlining of procedures. Conduct-ing a pilot phase at an ANISA site until the desired performance levels were reached and maintaining that performance afterwards required commitment of the site leaders and regular feedback from the coordination team and stakeholders.
SUMMARY AND CONCLUSIONTogether, ANISA’s 4 overlapping monitoring layers and
straightforward evaluation and communications allow the study investigators to detect issues and track numerous developments in the field, clinical and laboratory components of the project to make informed decisions.
A comprehensive system of harmonized site monitoring ele-ments increases the odds that each site will adhere strictly to all ele-ments in the study protocol evenly. It allows for both the coordination
team and the donor to be confident in the site investigators’ under-standing and control of issues within the bounds of the study. The ability to examine the key activities across project sites in a simple, inclusive and transparent way also allows for a shift from an imple-mentation focus to a management focus. Finally, it enables a shift to a results-based monitoring focus once the sites are functioning satis-factorily, and the project is on a path towards fulfilling its objectives.
Continuous monitoring of project activities leads to the adoption of various new strategies, staffing and oversight which strengthen both the active and passive surveillance structures at study sites. These strategies have already improved coverage and maximized engagement of sites with their at-risk communities.
A blood contamination workshop in February 2012 (Fig. 4) was the direct result of regular monitoring of contamination rates at the study sites from the pilot phase. If the results of laboratory investigations had not been monitored and scrutinized so regularly and closely, it would not have been possible to justify devising new strategies and developing more intensive guidelines for limit-ing contamination of neonatal blood specimens; it certainly would not have allowed these measures to be implemented mid-stream to improve study outcomes.
TABLE 5. Minimum Graduation Criteria from Pilot Phase
Element Minimum Threshold for Graduation
First assessment ≥50% of neonates reached and assessed within 24 hr of birthWorkers in field ≥80% of CHWs trained and operating in communityQA/QC ≥5% of home visits rechecked by supervisorsReferral from field ≥80% of referred children assessed by physicianSpecimen collection ≥80% of consenting casesBlood volume ≥80% of blood specimens contain ≥1 mL of bloodSpecimens At minimum, specimens preserved for later analysisBlood culture Done successfully and results used properlyData system Data entry functional, regular uploads to central serverHealthy controls Text message-mediated healthy control selection system in
place and functioning
FIGURE 3. Minimum graduation criteria in ANISA.
The project leaders expected that a fully functional study should assess more than 50% of
community-born neonates within 24 hours of birth, so this timing was monitored. It was
also incorporated into the pilot phase graduation criteria as the minimum acceptable
performance for the study sites. Sites were then encouraged to continue to improve towards
the desired levels each month. Other graduation criteria (Table 2) were also monitored and
charted in a similar way for discussion and decision-making by the coordination team, and
pooled charts were shared with the donor and other stakeholders to determine graduation
points. An example of project performance reaching children in the first day of life and pilot
graduation can be found below.
0
25
50
75
100
Tim
ing
of f
irst
vis
it (%
of
tota
l enr
ollm
ent)
Pilot phase
< 6 hours of birth
< 12 hours of birth
< 24 hours of birth
Pilot phase

Connor et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S44 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
In conclusion, the straightforward monitoring structure of ANISA is indispensable to identifying, sharing and resolving underlying issues with the help of partners and continues to facili-tate the success of the project and safeguarding of the validity of the study findings.
ACKNOWLEDGMENTSThe authors gratefully acknowledge the technical assistance
of Mr. Mahmudur Rahman and Ms. Mahfuza Marzan, as well as our numerous talented and supportive colleagues at CHRF, icddr,b and CDC.
The ANISA Methods Group: A. S. M. Nawshad Uddin Ahmed and Belal Hossain (Child Health Research Foundation, Dhaka, Bangladesh); Qazi Sadeq-ur Rahman and Tanvir Hos-sain (Centre for Child and Adolescent Health, International Cen-trefor Diarrhoeal Disease Research, Dhaka, Bangladesh); Jonas M.Winchell, Maureen H. Diaz, Nong Shang, Yoonjoung Choi, and Stephanie J. Schrag, DPhil (Centers for Disease Control and Pre-vention, Atlanta, GA); Aarti Kumar and Vishwajeet Kumar (Com-munity Empowerment Lab, Lucknow, India); Arif Billah, LukeMul-lany, Mathuram Santosham and Nazma Begum (Johns Hopkins
Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD); Daniel E. Roth (Department of Paediatrics, Hos-pital for Sick Children and University of Toronto, Canada); Der-rick Crook (John Radcliffe Hospital, University of Oxford, Oxford, United Kingdom); Stephen P. Luby (Stanford Woods Institute for the Environment, Stanford University, Stanford, CA) and Abdul Momin Kazi, Imran Ahmed, Shahida M. Qureshi,Sheraz Ahmed and Zulfiqar A. Bhutta (The Aga Khan University, Karachi, Pakistan).
REFERENCES 1. Waters D, Jawad I, Ahmad A, et al. Aetiology of community-acquired
neonatal sepsis in low and middle income countries. J Glob Health. 2011;1:154–170.
2. Saha SK, Arifeen SE, Schrag SJ. Aetiology of Neonatal Infection in South Asia (ANISA): an initiative to identify appropriate program priorities to save newborns. Pediatr Infect Dis J. 2016;35 (Suppl 1):S6–S8.
3. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
4. Connor NE, Hossain T, Rahman QS, et al. Development and implementa-tion of the ANISA labeling and tracking system for biological specimens. Pediatr Infect Dis J. 2016;35 (Suppl 1):S29–S34.
5. Rahman QS, Islam MS, Hossain B, et al. Centralized data management in a multicountry, multisite population-based study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S23–S28.
6. Zaidi AK, Tikmani SS, Sultana S, et al. Simplified antibiotic regimens for the management of clinically diagnosed severe infections in newborns and young infants in first-level facilities in Karachi, Pakistan: study design for an outpatient randomized controlled equivalence trial. Pediatr Infect Dis J. 2013;32 (Suppl 1):S19–S25.
7. Bhutta ZA, Memon ZA, Soofi S, et al. Implementing community-based perinatal care: results from a pilot study in rural Pakistan. Bull World Health Organ. 2008;86:452–459.
8. Bhutta ZA, Soofi S, Cousens S, et al. Improvement of perinatal and new-born care in rural Pakistan through community-based strategies: a cluster-randomised effectiveness trial. Lancet. 2011;377:403–412.
9. Baqui AH, El-Arifeen S, Darmstadt GL, et al; Projahnmo Study Group. Effect of community-based newborn-care intervention pack-age implemented through two service-delivery strategies in Sylhet district, Bangladesh: a cluster-randomised controlled trial. Lancet. 2008;371:1936–1944.
10. Arifeen SE, Mullany LC, Shah R, et al. The effect of cord cleansing with chlorhexidine on neonatal mortality in rural Bangladesh: a community-based, cluster-randomised trial. Lancet. 2012;379:1022–1028.
11. Singh JC, Kekre NS. CMC Vellore—in the service of our nation for more than a century. Indian J Surg. 2009;71:284–287.
12. John SM, Thomas RJ, Kaki S, et al. Establishment of the MAL-ED birth cohort study site in Vellore, Southern India. Clin Infect Dis. 2014;59 (Suppl 4):S295–S299.
13. Chandel DS, Johnson JA, Chaudhry R, et al. Extended-spectrum beta-lacta-mase-producing Gram-negative bacteria causing neonatal sepsis in India in rural and urban settings. J Med Microbiol. 2011;60(Pt 4):500–507.
14. Rowe AK, de Savigny D, Lanata CF, et al. How can we achieve and main-tain high-quality performance of health workers in low-resource settings? Lancet. 2005;366:1026–1035.
FIGURE 4. Controlling blood culture contamination.
In August 2012, routine monitoring of laboratory data found that the level of blood culture
contamination was high at the project sites. Subsequently, a workshop with senior scientists
was convened to devise preventive measures to minimize blood contamination and define
blood culture contamination in neonates. The coordination team agreed that all sites should
have less than 5% blood specimen contamination, and contamination should always be below a
maximum of 10% for all blood cultures. The team also agreed that a standardized procedure
should be followed at all specimen collection sites for each blood draw. There was a focus on
allowing sufficient time for each of the steps, ensuring oversight of each draw, as well as use of a
phlebotomy checklist. This oversight resulted in contamination levels remaining well below the
target for the rest of the project period.
0
5
10
15
20
25
Con
tam
inat
ion
rate
(%
of
tota
l no.
of
bloo
d cu
lture
)
Pilot phase
Maximum acceptable rate of contamination (10%)
Contamination Rate Threshold Target
Pilot phase

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S45
Supplement
Background: Interpretation of blood culture isolates is challenging due to a lack of standard methodologies for identifying contaminants. This problem becomes more complex when the specimens are from sick young infants, as a wide range of bacteria can cause illness among this group.Methods: We used 43 key words to find articles published between 1970 and 2011 on blood culture isolates and possible contaminants in the PubMed database. Experts were also consulted to obtain other relevant articles. Selec-tion of articles followed systematic methods considering opinions from more than 1 reviewer.Results: After reviewing the titles of 3869 articles extracted from the data-base, we found 307 relevant to our objective. Based on the abstracts, 42 articles were selected for the literature review. In addition, we included 7 more articles based on cross-references and expert advice. The most common methods for differentiating blood culture isolates were multiple blood cultures from the same subject, antibiograms and molecular testing. Streptococcus pneumoniae, Hemophilus influenzae, Neisseria meningitidis and group A and B streptococ-cus were always considered as pathogens, whereas Bacillus sp., Diphtheroids, Propionibacterium and Micrococcus were commonly regarded as contami-nants. Coagulase-negative staphylococci were the most frequent isolates and usually reported as contaminants unless the patient had a specific condition, such as long-term hospitalization or use of invasive devices (catheters).Conclusions: Inaccurate interpretation of blood culture may falsely guide treatment and also has long-term policy implications. The combination of clinical and microbiological knowledge, patient’s clinical history and labo-ratory findings are essential for appropriate interpretation of blood culture.
Key Words: neonatal, infection, blood culture, contamination, review, ANISA
(Pediatr Infect Dis J 2016;35:S45–S51)
The Aetiology of Neonatal Infection in South Asia (ANISA) study is one of the largest initiatives for obtaining data on the
etiology of community-acquired neonatal infections in the region.1 A wide range of bacteria can cause bloodstream infection in young infants, but many of these organisms are also part of normal skin flora.2 Contamination of blood culture during specimen collection and processing is common and accounts for up to half of all positive blood culture results.3 This situation can lead to incorrect treatment and has policy implications for designing appropriate strategies for the prevention and management of young infant infections.4,5 Con-sidering this, ANISA has undertaken an elaborate initiative to pre-vent contamination during blood collection. Despite these efforts, bacterial contamination in blood culture may still occur. With this situation in mind, we conducted a review of relevant literature to understand different approaches to differentiating true bacterial pathogens from contaminants in blood culture. In this article, we narrate the summary of that review.
METHODSBased on the preliminary observations of 3 peer-reviewed
articles,5–7 we selected 43 key words to be used independently or in combinations to carry out the search process. We looked for articles that had both the phrases “blood culture” and “contami-nation” either in the title or in the abstract or that contained the phrase blood culture and any of the key words in the title (Table 1). We limited our search to the National Institutes of Health PubMed database and articles published between 1970 and 2011. Screening of articles for final use was done in 3 steps. First, each selected title was reviewed by 2 individuals, and all articles deemed irrel-evant by them were excluded from subsequent screening. A third reviewer made a final decision where the first 2 reviewers disa-greed. Second, each abstract was reviewed by 2 individuals. We discarded case reports and articles that did not use blood culture for etiology detection. After these 2 steps, 3 individuals carried out a full review of the selected articles and rated each one from A to C based on its relevance. Articles were selected for analysis if at least 2 reviewers scored an article as “A.” In addition to this screening,
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S45DOI: 10.1097/INF.0000000000001106
Understanding Bacterial Isolates in Blood Culture and Approaches Used to Define Bacteria as Contaminants
A Literature Review
Belal Hossain, MSc,* Mohammad Shahidul Islam, MSc,* Atiqur Rahman, MSc,* Mahfuza Marzan, MSc,* Iftekhar Rafiqullah, MSc,* Nicholas E. Connor, MSc,† Mohammad Hasanuzzaman, MSc,* Maksuda Islam, BA,*
Davidson H. Hamer, MD,‡ Patricia L. Hibberd, MD, PhD,§ and Samir K. Saha, PhD*
Accepted for publication January 10, 2016.From the *Child Health Research Foundation, Dhaka, Bangladesh; †Centre for
Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh; ‡Department of Global Health and Center for Global Health and Development, Boston University School of Public Health, Boston, Massachusetts; and §Division of Global Health, Massachusetts General Hospital, Boston, Massachusetts.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Belal Hossain, MSc, Child Health Research Founda-tion, Department of Microbiology, Dhaka Shishu (Children) Hospital, Sher-e-Bangla Nagar, Dhaka 1207, Bangladesh. E-mail: [email protected].
TABLE 1. Article Search Strategies in PubMed
Search Strategy I: Blood Culture + Contamination [Title] OR Blood Culture + Contamination [Abstract]
Search Strategy II: Blood Culture [Title] + Any of the Keywords [Title]
Selected Key Words: Analysis, Aerococcus, Bacillus, Candida, Child, Clinical, Coagu-
lase-negative Staphylococc, Community-acquired, Comparison, Contaminant, Control, Corynebacterium, Cross, Diagnosis, Ente-rococc, Enterobacteriaceae, Enterobacter, False Positive, False Negative, Gram-positive, Gram-negative, Guideline, Interpreta-tion, Infant, Klebsiella, Laboratory, Microbiology, Micrococcus, Neonate, Newborn, Pathogen, Pediatric, Propionibacterium, Pseudomonas, Review, Staphylococc, Serratia, Shigella, Significant, Study, True Negative, True Positive, Yeast.

Hossain et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S46 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
we included some articles from cross-references and others sug-gested by experts in neonatology.
Search OutcomesThrough the search strategies, we extracted 3869 articles and
checked the titles for their relevance to our objectives. Of these arti-cles, 307 were marked for the next step, review of the abstracts. After reviewing the abstract, 168 articles went through a full-text screening. From this screening, 42 articles were selected for a full-text review of blood culture outcome interpretations and their relevance to infec-tion.8–49 In addition, we included 2 relevant articles from cross-refer-ences50,51 and 5 articles based on expert advice,52–56 which were not captured in our search methodologies (Fig. 1). The selected articles were from various parts of the world: Africa (n = 4), Asia (n = 8), Australia (n = 1), Europe (n = 11), North America (n = 21) and South America (n = 1). One article reported bacterial etiology from multi-center studies in Asia and Africa, and 3 were review articles. Of these articles, 5.5% (n = 3) were published in the 1980s, 21.8% (n = 12) in the 1990s, 54.5% (n = 30) from 2000 to 2010 and 16.4% (n = 9) in 2011. Twenty-three articles contained information about strategies to define blood culture isolates and 4 contained information about strate-gies or methods to reduce blood culture contamination; 13 articles were etiological studies, 3 were reviews and 6 were on other related topics. A brief summary of the primary features of the selected arti-cles is shown in Table 2.
Identity of Blood Culture IsolatesResearch confirmed that both Gram-positive and Gram-neg-
ative bacteria cause bloodstream infections. Gram-negative bacteria predominated during the neonatal period, whereas Gram-positive bacteria were more common in older patients.56 Hemophilus influen-zae, Streptococcus pneumoniae, Neisseria meningitidis and group A and B streptococcus were reported as potential causes of bloodstream infection in children; these organisms were described as a true cause in all the studies reviewed.8,10,11,46,52,55,56 Bacillus sp., Diphtheroids, Propionibacterium and Micrococcus were common contaminants in
blood culture.9,16,18,41,44,50,55 Coagulase-negative Staphylococci (CoNS) were the most frequent isolates.30,51 These bacteria are commonly found in skin flora,2 and 85% of the time they occur during blood col-lection.3 Therefore, many studies considered these as contaminants, and they were labeled as pathogens only under certain conditions, such as when a patient used invasive devices (catheters)20,22,26,31,34,47 or stayed in an intensive care unit for a long time.14,15,17,32,43 Other common bloodstream pathogens were Staphylococcus aureus, Salmonella sp., Pseudomonas aeruginosa, Klebsiella pneumoniae, Escherichia coli, Acinetobacter sp., Enterobacter sp., Proteus sp. and Candida sp.8,10–12,52,55,56 S. aureus, K. pneumoniae and E. coli are sometimes found in skin flora2 and thus may often appear in the cul-ture as a contaminant. Hence, these pathogens need special review when they are found in blood cultures.
Strategies for Interpreting Blood Culture IsolatesResearchers linked multiple clinical and microbiological
parameters to define blood culture isolates where the isolates were not obvious blood-borne pathogens. The parameters, as described in detail below, include (i) type of bacteria; (ii) antibiogram of the isolate; (iii) antibiotic therapy response of the patient; (iv) time-to-positivity (TTP) of the blood culture and (v) isolation of the same bacterium from a second blood culture done at the same time or on follow-up.5
Type of BacteriaIn all clinical research, identity of a bacterium was a major
criterion to consider it as a true pathogen.5 Bacteria such as S. pneu-moniae, H. influenzae and N. meningitidis were always considered as pathogens regardless of the patient’s clinical condition.5,8,10–12,52,55,56 Many researchers considered CoNS, Bacillus sp., Diphtheroids, Propionibacterium and Micrococcus as contaminants.55 E. coli and other potential bacteria were reviewed case-by-case to determine their association with illness.
Antibiogram of the IsolateIn many studies, drug susceptibility patterns were correlated
with treatment outcomes to decide whether to label isolated bacte-ria as pathogens. An isolate was considered as a pathogen when the patient showed clinical improvement in response to treatment and the isolated organism was susceptible to the drug used for treatment, or the patient showed no clinical improvement and the isolated organ-ism was resistant to the treatment drug. An isolate was considered as a contaminant if the patient did not respond to an antibiotic to which the respective isolate was susceptible or responded to an antibiotic to which the isolate was not susceptible.5,31,32,39,50
Time-to-positivityTTP is measured based on the time the blood culture bottle
remains in the incubator and is inversely proportional to the magnitude of bacteria in the blood. Infected blood has a higher inoculum com-pared with contaminated blood and should have a shorter incubation time to yield growth.5 Thus, any blood culture that yields growth within a short duration has a higher probability of being a true pathogen.34
Multiple Blood Culture Vials or Repeat Blood CulturesBlood culture in duplicate was ideal to exclude contamina-
tion, that is, to confirm the isolate as a true pathogen. In many stud-ies, multiple blood cultures (more than 2 within a 12-hour period) were performed, and if more than 1 culture was positive for the same bacterium, then the isolate was considered as a true pathogen.5,29,30,32
Genotyping and Plasmid ProfilesThe genetic fingerprints of isolated bacteria from the
same patient are good tools for differentiating contaminants from
FIGURE 1. Flow diagram of article selection following literature search in PubMed (7 articles included that did not meet the search criteria).

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Blood Culture Contamination
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S47
TABLE 2. Key Features of Articles Reviewed
AuthorStudy Location
and YearStudy Setting (Age Group) Comments
AfricaAdhikari et al8 South Africa, 1988–1991 IPD (0–59 days) Bacterial meningitis cases were defined by positive blood culture or
positive bacterial antigen test. The isolated bacteria were group B Streptococcus, K. pneumoniae, E. coli, S. pneumoniae, P. aerugi-nosa, Salmonella sp., Proteus mirabilis, Enterobacter cloacae and Acinetobacter anitratus. CoNS were not reported as pathogens.
Berkley et al9 Kenya,1998–2002 IPD S. pneumoniae, H. influenzae and E. coli were reported as most common blood-borne pathogens in children. CoNS, Bacillus and Micrococcus were the most common blood culture isolates, but none of them were reported as pathogens.
Kohli-Kochhar et al10
Kenya, 2000–2009 IPD (0–59 days) The most common pathogens were S. pneumoniae, Yeast ( Candida), Acinetobacter sp., Aeromonas sp., S. pneumoniae, group B Strep-tococcus, Streptococcus sp., E. cloacae and Klebsiella sp. CoNS were the predominant isolates but not reported as pathogens as the authors were not certain whether these organisms were true pathogens.
Sigaúque et al11 Mozambique, 2001–2006 Community (<15 years) CoNS, Corynebacterium sp., Bacillus and Viridans streptococcus were considered as contaminants in community-acquired sepsis cases. S. pneumoniae, group A and B streptococcus, K. pneumoniae, E. coli, P. aeruginosa, Salmonella sp., N. meningitidis, H. influenzae, as well as other bacteria were considered pathogens.
Arifeen et al52 Bangladesh, 2004–2007 Community Reported E. coli, S. aureus, Streptococcus sp., Salmonella typhi, H. influenzae, S. pneumoniae as pathogens in community-acquired sepsis cases. CoNS were not reported as pathogens.
Ashkenazi- Hoffnung et al12
Israel, 2003–2007 Hospitals (all ages) Reported seasonal pattern of Bacillus sp. detection rate in blood culture.
Huang et al13 Taiwan, 1998–2001 IPD (0–59 months) CoNS were defined as pathogens if same strains of CoNS isolated in sequential blood cultures were positive and correlated with clinical signs.
Huang et al14 Taiwan, 1999–2000 NICU CoNS isolated from cultures of paired blood specimens obtained simultaneously from different peripheral sites from infants usually represent true infection.
Kim et al50 Republic of Korea, 2009 IPD (all age groups) Three infectious disease specialists independently classified each isolate from single positive blood cultures into different groups: likely contaminant, possible contaminant or true pathogen based on antibiogram. CoNS and Bacillus were the most frequent likely contaminants.
Matrai-Kovalskis et al15
Israel, 1990–1996 NICU Reviewed policy of using vancomycin in infants with CoNS-positive blood cultures in NICU. Use of vancomycin was associated with low morbidity and mortality.
Quiambao et al16 Philippines, 1994–2000 Community based (0–59 days)
Reported Gram-negative nonfermenting bacteria as doubtful pathogen causing sepsis in a population without severe immu-nosuppression or in-dwelling foreign bodies and were considered contaminants. CoNS, Diptheroids, Bacillus sp. and Micrococci were also considered as contaminants.
Bradford et al17 Australia, 1998–2002 NICU Used genetic markers to differentiate clinically relevant and con-taminating CoNS isolates in blood culture collected from very low birth weight infants in NICU. Genetic markers were not effective in differentiating pathogens from contaminants.
Arnason et al18 Iceland, 1994–2005 Community and hospital (0–18 years)
Blood and cerebrospinal fluid isolates were classified as contaminant, probable contaminant, probable infection or definite infection based on microbiological criteria. Three bacteria (Bacillus sp., Micrococcus sp. and Propionibacterium) were classified as definite contaminants, 14 types of bacteria including CoNS as probable contaminants, 6 types as probable pathogens and 28 types as pathogens. After reviewing the case reports of each isolate, 38 (n = 465) were reported as probable or definite pathogens.
Burnie et al19 United Kingdom, 1993–1994
Community and hospital (all ages)
Analyzed 115 CoNS isolates, which caused bacteremia among prema-ture neonates and adults experiencing leukemia. Similar types of bacteria from hospital staff working in the relevant units during that time were also isolated.
Guerti et al20 Belgium, 2001 IPD (0–59 days) Correlated TTP of blood culture with type of isolates. Sepsis episode was defined where a definite pathogen was isolated or a possible pathogen was isolated in presence of a central vascular catheter or from 2 blood samples taken from 2 different puncture sites. Median TTPs were significantly shorter in episodes of proven sepsis compared with nonproven sepsis.
Klingenberg et al21 Norway, 1989–2000 IPD (0–59 days) CoNS isolates were analyzed based on CDC guidelines and correlated with C-reactive protein (>10 mg/L) and TPP of blood cultures (within 2 days of blood culture) to understand clinical relevance. Based on these criteria, 85 isolates from 81 patients were considered as invasive and 95 isolates from 77 patients were considered as contaminants.
(Continued)

Hossain et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S48 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
Koksal et al22 Turkey, 1999–2006 IPD (all ages) Reported drug resistance patterns of CoNS isolates. CoNS were consid-ered as pathogens if more than one blood culture was positive and correlated with clinical signs and treatment outcome and fulfilled CDC definitions for nosocomial infection. Two hundred cases of CoNS were considered as bloodstream infections. All of these cases had either vascular catheterizations or had burn and immune deficiency.
Krause et al23 Austria, — 19–89 years Single blood culture was not considered as pathogen. PFGE and molecular typing were used to differentiate CoNS isolates if multi-ple blood cultures from same patient were positive; 1% of healthy controls yielded CoNS isolates with similar PFGE patterns and similar types of bacteria were also isolated from skin of subjects.
Leyssene et al24 France, 2007–2008 IPD (not mentioned) Blood culture isolates were classified as pathogens or contaminants based on clinical signs, cytology (white blood cell count) and number of positive bottles per set (out of 6 bottles). A U-shaped relationship with number of positive bottles per set of blood culture was found. Common contaminants such as Corynebacterium and Micrococcus sp. grew in a maximum of 3 of 6 bottles, whereas pathogens such as E.coli and S. aureus grew more frequently in 6 of 6 bottles.
Mulder and Degener25
Netherlands, 1990–1992 IPD (not mentioned) Slime production capacity of CoNS was compared with differentiate pathogenic strains from contaminants. CoNS strains (51.8%) that were considered as clinically relevant based on other algorithms had more slime producing ability than contaminating CoNS strains.
Schuetz et al26 Switzerland, 2005 IPD (>18 years) Used PCT concentration along with clinical and microbiological features to differentiate CoNS isolates. A positive correlation between CoNS infection and PCT was reported. Of 40 cases, only 7 were reported as CoNS-related infection; all of these had vascular catheters at the time of blood collection.
Senger et al27 Turkey, 2003–2004 IPD (not mentioned) CoNS from single blood culture were not considered as true patho-gens. Cases where more than one blood culture was positive were further analyzed based on PFGE pattern. Only 50% of paired samples of 38 patients yielded similar CoNS strains, and those cases were classified as true CoNS infections.
Viagappan and Kelsey28
United Kingdom, 1994 Community and hospi-tal (all ages)
Clinical condition was used to define CoNS isolates. Based on this cri-terion, 88% of isolated CoNS were reported as contaminants (n = 28/32).
Al Wohoush et al29 USA, 2006–2008 IPD Nosocomial infection by CoNS was identified based on CDC criteria of more than 2 positive blood cultures within 48 hours, clinical signs of infection and type of species isolated in each episode. Authors found combination of methods more useful than using only one to differentiate contaminating CoNS.
Beekmann et al30 USA, 1999–2000 IPD (all age groups) CoNS were defined as pathogens when 2 blood cultures were positive within 5 days or 1 blood culture was positive with clinical evidence of sepsis. Of 405 isolates, only 89 were considered as pathogens with the remaining 316 considered as contaminants.
Benjamin et al31 USA, 2004–2007 IPD (0–120 days) Invasive candidiasis in low birth weight infants was determined through a prospective observational study that reported 137 cases. Broad-spectrum antibiotics and central catheters were 2 major risk factors.
Calnen et al32 USA, 1980–1981 IPD (NICU) (0–28 days) CoNS cases were grouped in 3 categories: 20% of the cases were con-sidered as true bacteremia as 2 or more blood cultures were posi-tive for CoNS with identical antibiotic susceptibility patterns; 57% of CoNS isolates were considered as probable contaminants as only 1 of the 2 blood cultures was positive for CoNS; 23% of the CoNS were considered as indeterminant as only 1 culture was done.
Chandran and Rennie33
Canada, 1999 IPD and OPD (all age groups)
Authors suggested that an antibiotic susceptibility test is not required for all CoNS isolates, as most are contaminants.
Haimi-Cohen et al34
USA, 1998–2001 IPD and OPD (children >2 weeks of age)
Demonstrated TTP values as an indicator to differentiate infec-tion and contamination for CoNS growth. TTPs were consider-ably shorter in true bacteremia cases (median TTP 11.4 hours) compared with contaminant cases from healthy infants (median TTP 19 hours) or contaminant cases from sick infants (median TTP 24 hours). A TTP of ≤15 hours had a positive predictive value of 84% for diagnosis of infection. A TTP of ≥22 hours had a positive predictive value of 87% for diagnosis of contaminants.
Herwaldt et al35 USA, 1986–1989 IPD (all age groups) Determined positive predictive value of isolated blood cultures based on specific bloodstream infection definition. Of the 227 CoNS isolates, 60 were considered pathogens.
Kim et al36 USA, 1996–1997 IPD (all age groups) CoNS were defined as pathogens based on CDC surveillance defini-tion of primary bloodstream infection and ≥2 blood culture isolates of CoNS. Of 171 CoNS isolates, only 17 were considered pathogens, while others were considered contaminants.
TABLE 2. (Continued)
AuthorStudy Location
and YearStudy Setting (Age Group) Comments
(Continued)

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Blood Culture Contamination
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S49
Kirchhoff and Sheagren37
USA, 1978–1980 IPD (all age groups) Number of blood cultures and clinical criteria were used to define CoNS as pathogens; 85% of all CoNS isolates were found to be contaminants.
Kassis et al38 USA, 2005–2008 University of Texas, M.D. Anderson Cancer Center
Authors suggested that CoNS isolates with TTP of <16 hours reflect high-grade bacteremia with CFU of >100 per mL and required an active therapeutic approach. TTP of >20 hours indicated possible contamination with a CFU of <10 per mL, and active therapy was required.
Khatib et al39 USA, 1993 IPD (all age groups) Strain relatedness among CoNS found in 24 of 47 episodes of bactere-mia by plasmid typing, determination of species and antibiotyping.
Nataro et al40 USA, 1989–1991 IPD (0–6 months) CoNS were defined as pathogens if identical isolates grew in multiple blood cultures. Among 59 episodes, 25 were considered pathogens and 34 contaminants.
Segal and Chamberlain41
USA, 1994–1996 — 209 cultures were reviewed; 85 were contaminants, 123 were patho-gens. CoNS, Micrococcus sp., α-hemolytic Streptococcus, nonhemo-lytic Streptococcus and diphtheroids were listed as contaminants.
Seybold et al42 USA, 2001 IPD (all age groups) PFGE typing was used to differentiate genetically unrelated and distinct CoNS from 2 blood cultures from each patient. Of 38 pairs of stains, 15 pairs were found genetically distinct from each other.
Sidebottom et al43 USA, 1970–1984 IPD (neonates) CoNS were detected as principal pathogens of nosocomial infection in NICU, with overall incidence of 4.4/100 admissions.
Souvenir et al44 USA, 1995 IPD (>18 years) CoNS were categorized as contaminants or pathogens based on predetermined clinical criteria (prolonged temperature, hypoten-sion, disseminated intravascular coagulation) and risk factors. Of 81 CoNS isolates, 20 were considered pathogens, 10 indeterminant, 59 contaminants. Coryneforms (n = 58), Bacillus sp. (n = 52), and viridans group Streptococci (n = 52) were considered as probable contaminants.
Stoll et al53 USA, 1991–1993 and 1998–2000
IPD (≤72 hours) Compared early onset of neonatal sepsis pathogens in low birth weight babies from 2 different times.
Stoll et al54 USA, 2006–2009 IPD (≤72 hours) Prospective surveillance for early-onset sepsis reported group B Streptococcus, E. coli, viridans Streptococcus, S. aureus and some other bacteria as pathogens (N = 370).
Struthers et al45 Canada, 1999–2000 IPD (0–28 days) Patients with positive CoNS cultures from 2 different body sites were considered. Discordant results from cultures from 2 sites were regarded as contamination. Using a single culture alone would have resulted in a 31% increase in number of infants with CoNS infection.
Weston et al46 USA, 2005–2008 Population based (0–72 hours)
Reported bacterial etiology of early onset of sepsis. The most frequently isolated pathogens were group B Streptococcus, E. coli, viridans Streptococcus, S. aureus, H. influenzae (N = 739).
Zaidi et al47 USA, 1994–1995 — PFGE was used to characterize CoNS isolated from sequential blood cultures from neonates and children. Authors concluded that even repeated cultures of CoNS may represent contamination if blood was drawn through a cardiovascular catheter or a second sample was obtained >1 day after administration of antibiotics.
García et al48 Chile, 2000–2001 IPD CoNS were categorized as contaminants or pathogens based on clini-cal and laboratory criteria such as TTP, colony morphology, species determination, biotype, antibiotic sensitivity result, PFGE pattern and adherence capacity. In 20 patients where only 1 blood culture was positive, 18 were considered contaminants and only 1 was considered a true pathogen.
WHO Young Infants Study55
Multicenter study, 4 countries
Population based (0–90 days)
Bacteria in definite pathogen group (eg, S. pneumoniae, H. influenzae, group A and B Streptococcus, Salmonella sp.) were considered as pathogens if any blood cultures were positive. Bacteria in probable group (eg, K. pneumoniae, S. aureus, Enterobacter faecalis group D) were considered as pathogens if both (1 if only 1 sample collected) bottles were positive within 48 hours of inoculation. Isolates that did not fulfill these criteria, or CoNS, Micrococcus sp. and Bacillus sp., were regarded as contaminants.
Peltola49 Sub-Saharan Africa, 1958–1997
Review Reviewed meningitidis etiology and found that H. influenzae, S. pneu-moniae and N. meningitidis are the leading causes of meningitis in sub-Saharan Africa.
Thylefors et al51 — Review Analyzed CoNS isolates reported in different articles and reported CoNS as most frequent contaminants of positive blood cultures (58.5–83%). Isolation rate of CoNS has been increasing over years.
Zaidi et al56 — Review Reported etiology of neonatal sepsis in developing countries. Limited information was available on etiology of serious bacterial infec-tions in community settings. Hospital-based studies suggested that wide range of bacteria (Gram positive and Gram negative) cause neonatal sepsis. This review did not report CoNS as pathogens.
CDC indicates Centers for Disease Control and Prevention; CFU, colony-forming units; IPD, in-patient department; NICU, neonatal intensive care unit; OPD, outpatient depart-ment; PCT, serum procalcitonin; PFGE, pulsed-field gel electrophoresis; TTP, time-to-positivity.
TABLE 2. (Continued)
AuthorStudy Location
and YearStudy Setting (Age Group) Comments

Hossain et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S50 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
opportunistic pathogens. In some studies, the plasmid or DNA pro-files of 2 strains isolated from the same patient were compared, and if they matched, then they were considered as true pathogens.17,23,27,48 These molecular techniques were mainly used to differentiate con-taminant CoNS from pathogenic ones.
DISCUSSIONBlood culture contamination is a long-standing challenge in
clinical microbiology as normal skin flora also consists of potential pathogens. The aim of this literature review was to extract existing infor-mation on defining blood culture isolates. The findings of this review assisted the ANISA study team and an external expert panel to develop a guideline for properly interpreting blood culture outcomes. This land-scape analysis shows that a wide range of bacteria can cause infection in humans, especially at an early age. Some bacteria were universally con-sidered either as pathogens or as contaminants, whereas some needed to be reviewed case-by-case. The process for assigning causality is never straightforward in an etiology study, and it requires integration of clini-cal knowledge, practical experience and expert opinion.
This review has some potential limitations. The literature search was designed to capture articles reporting blood culture contamination, so it could have missed studies that reported blood culture isolates but did not discuss contamination. In addition, our search was limited to PubMed and articles published in English. Therefore, we may have not seen useful articles published in other languages. We tried to compensate for such limitations by the inclu-sion of relevant cross-references and articles suggested by experts.
CONCLUSIONThe current review provides an insight into our existing
knowledge about classifying blood culture isolates as true pathogens or contaminants based on an integrated algorithm and case-specific clinical and microbiological information. ANISA aims to use these findings to prevent the misclassification of blood culture results at 2 stages: (i) reduction of contamination by employing preventive strategies and (ii) teasing out contaminants from the isolates.
REFERENCES 1. Saha SK, Arifeen SE, Schrag SJ. Aetiology of Neonatal Infection in South
Asia (ANISA): an initiative to identify appropriate program priorities to save newborns. Pediatr Infect Dis J. 2016;35 (Suppl 1):S6–S8.
2. Mullany LC, Saha SK, Shah R, et al. Impact of 4.0% chlorhexidine cord cleansing on the bacteriologic profile of the newborn umbilical stump in rural Sylhet District, Bangladesh: a community-based, cluster-randomized trial. Pediatr Infect Dis J. 2012;31:444–450.
3. Weinstein MP, Towns ML, Quartey SM, et al. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evalu-ation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997;24:584–602.
4. Alahmadi YM, Aldeyab MA, McElnay JC, et al. Clinical and economic impact of contaminated blood cultures within the hospital setting. J Hosp Infect. 2011;77:233–236.
5. Hall KK, Lyman JA. Updated review of blood culture contamination. Clin Microbiol Rev. 2006;19:788–802.
6. Bryan CS. Clinical implications of positive blood cultures. Clin Microbiol Rev. 1989;2:329–353.
7. Weinstein MP. Current blood culture methods and systems: clini-cal concepts, technology, and interpretation of results. Clin Infect Dis. 1996;23:40–46.
8. Adhikari M, Coovadia YM, Singh D. A 4-year study of neonatal meningitis: clinical and microbiological findings. J Trop Pediatr. 1995;41:81–85.
9. Berkley JA, Lowe BS, Mwangi I, et al. Bacteremia among children admitted to a rural hospital in Kenya. N Engl J Med. 2005;352:39–47.
10. Kohli-Kochhar R, Omuse G, Revathi G. A ten-year review of neonatal bloodstream infections in a tertiary private hospital in Kenya. J Infect Dev Ctries. 2011;5:799–803.
11. Sigaúque B, Roca A, Mandomando I, et al. Community-acquired bactere-mia among children admitted to a rural hospital in Mozambique. Pediatr Infect Dis J. 2009;28:108–113.
12. Ashkenazi-Hoffnung L, Kaufman Z, Bromberg M, et al. Seasonality of Bacillus species isolated from blood cultures and its potential implications. Am J Infect Control. 2009;37:495–499.
13. Huang SY, Tang RB, Chen SJ, et al. Coagulase-negative staphylococcal bac-teremia in critically ill children: risk factors and antimicrobial susceptibility. J Microbiol Immunol Infect. 2003;36:51–55.
14. Huang YC, Wang YH, Su LH, et al. Determining the significance of coagu-lase-negative staphylococci identified in cultures of paired blood specimens from neonates by species identification and strain clonality. Infect Control Hosp Epidemiol. 2006;27:70–73.
15. Matrai-Kovalskis Y, Greenberg D, Shinwell ES, et al. Positive blood cultures for coagulase-negative staphylococci in neonates: does highly selective van-comycin usage affect outcome? Infection. 1998;26:85–92.
16. Quiambao BP, Simoes EA, Ladesma EA, et al. Serious community-acquired neonatal infections in rural Southeast Asia (Bohol Island, Philippines). J Perinatol. 2007;27:112–119.
17. Bradford R, Abdul Manan R, Daley AJ, et al. Coagulase-negative staphy-lococci in very-low-birth-weight infants: inability of genetic markers to distinguish invasive strains from blood culture contaminants. Eur J Clin Microbiol Infect Dis. 2006;25:283–290.
18. Arnason S, Thors VS, Gudnason T, et al. [Bacteraemia in children in Iceland 1994-2005]. Laeknabladid. 2008;94:523–529.
19. Burnie JP, Naderi-Nasab M, Loudon KW, et al. An epidemiological study of blood culture isolates of coagulase-negative staphylococci demonstrating hospital-acquired infection. J Clin Microbiol. 1997;35:1746–1750.
20. Guerti K, Devos H, Ieven MM, et al. Time to positivity of neonatal blood cultures: fast and furious? J Med Microbiol. 2011;60(pt 4):446–453.
21. Klingenberg C, Sundsfjord A, Rønnestad A, et al. Phenotypic and geno-typic aminoglycoside resistance in blood culture isolates of coagulase-neg-ative staphylococci from a single neonatal intensive care unit, 1989-2000. J Antimicrob Chemother. 2004;54:889–896.
22. Koksal F, Yasar H, Samasti M. Antibiotic resistance patterns of coagulase-negative staphylococcus strains isolated from blood cultures of septicemic patients in Turkey. Microbiol Res. 2009;164:404–410.
23. Krause R, Haberl R, Wölfler A, et al. Molecular typing of coagulase-negative staphylococcal blood and skin culture isolates to differentiate between bacteremia and contamination. Eur J Clin Microbiol Infect Dis. 2003;22:760–763.
24. Leyssene D, Gardes S, Vilquin P, et al. Species-driven interpretation guide-lines in case of a single-sampling strategy for blood culture. Eur J Clin Microbiol Infect Dis. 2011;30:1537–1541.
25. Mulder JG, Degener JE. Slime-producing properties of coagulase-neg-ative staphylococci isolated from blood cultures. Clin Microbiol Infect. 1998;4:689–694.
26. Schuetz P, Mueller B, Trampuz A. Serum procalcitonin for discrimination of blood contamination from bloodstream infection due to coagulase-negative staphylococci. Infection. 2007;35:352–355.
27. Senger SS, Saccozza ME, Yuce A. Compatibility of pulsed-field gel electro-phoresis findings and clinical criteria commonly used to distinguish between true coagulase-negative staphylococcal bacteremia and contamination. Infect Control Hosp Epidemiol. 2007;28:992–996.
28. Viagappan M, Kelsey MC. The origin of coagulase-negative staphylococci isolated from blood cultures. J Hosp Infect. 1995;30:217–223.
29. Al Wohoush I, Rivera J, Cairo J, et al. Comparing clinical and microbio-logical methods for the diagnosis of true bacteraemia among patients with multiple blood cultures positive for coagulase-negative staphylococci. Clin Microbiol Infect. 2011;17:569–571.
30. Beekmann SE, Diekema DJ, Doern GV. Determining the clinical signifi-cance of coagulase-negative staphylococci isolated from blood cultures. Infect Control Hosp Epidemiol. 2005;26:559–566.
31. Benjamin DK Jr., Stoll BJ, Gantz MG, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Neonatal candidiasis: epidemiology, risk factors, and clinical judgment. Pediatrics. 2010;126:e865–e873.
32. Calnen G, Campognone P, Peter G. Coagulase-negative staphylococcal bac-teremia in newborns. Clin Pediatr (Phila). 1984;23:542–544.
33. Chandran AU, Rennie R. Routine antimicrobial susceptibility testing of coagulase-negative staphylococci isolated from blood cultures: is it neces-sary? Clin Microbiol Infect. 2005;11:1037–1040.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Blood Culture Contamination
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S51
34. Haimi-Cohen Y, Shafinoori S, Tucci V, et al. Use of incubation time to detec-tion in BACTEC 9240 to distinguish coagulase-negative staphylococcal contamination from infection in pediatric blood cultures. Pediatr Infect Dis J. 2003;22:968–974.
35. Herwaldt LA, Geiss M, Kao C, et al. The positive predictive value of isolat-ing coagulase-negative staphylococci from blood cultures. Clin Infect Dis. 1996;22:14–20.
36. Kim SD, McDonald LC, Jarvis WR, et al. Determining the significance of coagulase-negative staphylococci isolated from blood cultures at a commu-nity hospital: a role for species and strain identification. Infect Control Hosp Epidemiol. 2000;21:213–217.
37. Kirchhoff LV, Sheagren JN. Epidemiology and clinical significance of blood cultures positive for coagulase-negative staphylococcus. Infect Control. 1985;6:479–486.
38. Kassis C, Rangaraj G, Jiang Y, et al. Differentiating culture samples repre-senting coagulase-negative staphylococcal bacteremia from those represent-ing contamination by use of time-to-positivity and quantitative blood culture methods. J Clin Microbiol. 2009;47:3255–3260.
39. Khatib R, Riederer KM, Clark JA, et al. Coagulase-negative staphylococci in multiple blood cultures: strain relatedness and determinants of same-strain bacteremia. J Clin Microbiol. 1995;33:816–820.
40. Nataro JP, Corcoran L, Zirin S, et al. Prospective analysis of coagulase-neg-ative staphylococcal infection in hospitalized infants. J Pediatr. 1994;125(5 pt 1):798–804.
41. Segal GS, Chamberlain JM. Resource utilization and contaminated blood cultures in children at risk for occult bacteremia. Arch Pediatr Adolesc Med. 2000;154:469–473.
42. Seybold U, Reichardt C, Halvosa JS, et al. Clonal diversity in episodes with multiple coagulase-negative Staphylococcus bloodstream isolates suggest-ing frequent contamination. Infection. 2009;37:256–260.
43. Sidebottom DG, Freeman J, Platt R, et al. Fifteen-year experience with bloodstream isolates of coagulase-negative staphylococci in neonatal inten-sive care. J Clin Microbiol. 1988;26:713–718.
44. Souvenir D, Anderson DE Jr., Palpant S, et al. Blood cultures positive for coagulase-negative staphylococci: antisepsis, pseudobacteremia, and ther-apy of patients. J Clin Microbiol. 1998;36:1923–1926.
45. Struthers S, Underhill H, Albersheim S, et al. A comparison of two versus one blood culture in the diagnosis and treatment of coagulase-negative staphylococ-cus in the neonatal intensive care unit. J Perinatol. 2002;22:547–549.
46. Weston EJ, Pondo T, Lewis MM, et al. The burden of invasive early-onset neonatal sepsis in the United States, 2005-2008. Pediatr Infect Dis J. 2011;30:937–941.
47. Zaidi AK, Harrell LJ, Rost JR, et al. Assessment of similarity among coag-ulase-negative staphylococci from sequential blood cultures of neonates and children by pulsed-field gel electrophoresis. J Infect Dis. 1996;174:1010–1014.
48. García P, Benítez R, Lam M, et al. Coagulase-negative staphylococci: clini-cal, microbiological and molecular features to predict true bacteraemia. J Med Microbiol. 2004;53(pt 1):67–72.
49. Peltola H. Burden of meningitis and other severe bacterial infections of chil-dren in Africa: implications for prevention. Clin Infect Dis. 2001;32:64–75.
50. Kim NH, Kim M, Lee S, et al. Effect of routine sterile gloving on contami-nation rates in blood culture: a cluster randomized trial. Ann Intern Med. 2011;154:145–151.
51. Thylefors JD, Harbarth S, Pittet D. Increasing bacteremia due to coagulase-negative staphylococci: fiction or reality? Infect Control Hosp Epidemiol. 1998;19:581–589.
52. Arifeen SE, Saha SK, Rahman S, et al. Invasive pneumococcal disease among children in rural Bangladesh: results from a population-based sur-veillance. Clin Infect Dis. 2009;48(suppl 2):S103–S113.
53. Stoll BJ, Hansen N, Fanaroff AA, et al. Changes in pathogens causing early-onset sepsis in very-low-birth-weight infants. N Engl J Med. 2002;347:240–247.
54. Stoll BJ, Hansen NI, Sánchez PJ, et al.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011;127:817–826.
55. The WHO Young Infants Study Group. Bacterial etiology of serious infec-tions in young infants in developing countries: results of a multicenter study. Pediatr Infect Dis J. 1999;18(suppl 10):S17–S22.
56. Zaidi AK, Thaver D, Ali SA, et al. Pathogens associated with sepsis in newborns and young infants in developing countries. Pediatr Infect Dis J. 2009;28(1 suppl):S10–S18.

S52 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
Supplement
Abstract: The multisite community-based study, Aetiology of Neonatal Infection in South Asia (ANISA), uses blood culture as the gold standard for identifying the etiology of neonatal infection. Considering the impor-tance of this age-old diagnostic tool and the risk of contamination, ANISA has employed rigorous measures to prevent contamination at all stages of blood collection, processing and culture. Because contamination may still occur, an independent expert group evaluates the routinely collected clini-cal and laboratory data to determine whether a blood culture isolate is a contaminant or a true pathogen. This article describes the methodology used by ANISA to determine whether a blood culture isolate is likely to be a true pathogen or a contaminant in neonatal sepsis.
Key Words: neonate, infection, blood culture, contamination, ANISA
(Pediatr Infect Dis J 2016;35:S52–S54)
Even with substantial improvements in global child health, about 6.5 million children younger than 5 years died in 2013. Two
thirds (2.8 million) of these deaths occurred in the neonatal period (<28 days of age); 51% (1.4 million) of neonatal deaths are pre-sumed to be because of infections.1,2 However, most estimates of infection-related deaths contain limited direct evidence on infec-tions and their etiology.
As the most recent studies on etiology of neonatal sepsis are from a small population in Bangladesh, the results are not sufficient to inform targeted etiology-specific interventions to reduce deaths from neonatal infection.3,4 To fill this gap, we are conducting the Aetiology of Neonatal Infection in South Asia (ANISA) study in 5 population-based sites in Bangladesh, India and Pakistan. In this
study, we collect blood and nasopharyngeal-oropharyngeal swabs from newborns aged 0–59 days who show 1 or more signs of possi-ble serious bacterial infection.5 We test these specimens using both conventional and molecular methods to detect bacterial and viral pathogens.
Among the diagnostic methods for detecting bacterial etiology of neonatal infection, blood culture is still consid-ered the gold standard. In recent years, blood culture methods have improved with the availability of enriched media that have passed quality control measures, with the ability to support the growth of fastidious organisms and neutralize the action of anti-biotics present in the specimens. However, all these advances may be jeopardized because of contamination of blood cul-ture leading to false-positive results. The main source of this contamination is skin flora, which often become the source of contamination in blood culture bottles during phlebotomy and specimen processing.6
Skin flora-mediated contamination is a major risk for the ANISA study because the skin surface of a South Asian baby is colonized with a high density of bacteria. Furthermore, these colonizing organisms are diverse, and many are known for being common etiologies of neonatal sepsis.7,8 Considering the afore-mentioned challenges, ANISA has taken stringent antisepsis measures and introduced monitoring schemes to avoid contamina-tion during phlebotomy. However, despite all efforts, completely eliminating the access of skin flora and/or environmental bacteria into blood specimens during phlebotomy and inoculation of blood culture bottles is not possible. Contamination can also occur at the laboratory, while processing the specimens and culture plates. Taking these issues into account, the ANISA team designed labo-ratory data capture forms for detailed recording of all laboratory activities. These sources of information facilitate the evaluation of blood culture isolates and thus assist in classifying them as true pathogens, by teasing out contaminants based on the demographic, clinical and microbiologic data.
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S52DOI: 10.1097/INF.0000000000001107
Classification of Blood Culture Isolates Into Contaminants and Pathogens on the Basis of Clinical and Laboratory Data
Belal Hossain, MSc,* Martin W. Weber, PhD,† Davidson H. Hamer, MD,‡ Patricia L. Hibberd, MD, PhD,§ A. S. M. Nawshad Uddin Ahmed, FCPS,* Mahfuza Marzan, MSc,* Maksuda Islam, BA,* Nicholas E. Connor,
MSc,¶ Mohammad Shahidul Islam, MSc,* Anita K. Zaidi, SM,║ Abdullah H. Baqui, DrPH,** Zulfiqar A. Bhutta, PhD,║ Shahida M. Qureshi, MSc,║ Iftekhar Rafiqullah, MSc,* Lesley McGee, PhD,†† and Samir K. Saha, PhD*
Accepted for publication January 10, 2016. From the *Child Health Research Foundation, Dhaka, Bangladesh; †Child and
Adolescent Health Department, World Health Organization, Geneva, Swit-zerland; ‡Department of Global Health and Center for Global Health and Development, Boston University School of Public Health, Boston, Massa-chusetts; §Division of Global Health, Massachusetts General Hospital, Bos-ton, Massachusetts; ¶Centre for Child and Adolescent Health, International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh; ║Department of Paediatrics and Child Health, The Aga Khan University, Karachi, Pakistan; **Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland; and ††Streptococcus Laboratory, Cen-ters for Disease Control and Prevention, Atlanta, Georgia.
The ANISA study is funded by the Bill & Melinda Gates Foundation (grant no. OPPGH5307). The authors have no conflicts of interest to disclose.
Address for correspondence: Davidson H. Hamer, MD, Center for Global Health and Development, Crosstown 3rd Floor, 801 Massachusetts Avenue, Boston, MA 02118. E-mail: [email protected].
TABLE 1. Classification of Bacterial Isolates Based on ANISA Blood Culture Literature Review9
Definite pathogen: Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis, Escherichia coli, Klebsiella pneumoniae, Enterococcus spp., Enterobacter spp., Pseudomonas aeruginosa, Acinetobacter spp., Aeromonas spp., Serratia marcescens, Neisseria spp., Listeria monocytogenes, Group A streptococcus, Group B strep-tococcus, Group D streptococcus, Salmonella spp., Proteus mirabilis, Citrobacter spp., Flavobacterium meningosepticum
Probable pathogen: Staphylococcus aureus, Streptococcus virid-ians, Leuconostoc spp., Morganella morganii, Nocardia spp., Moraxella spp., Corynebacterium jeikeium, Shigella spp., Campylobacter jejuni, Candida spp.
Definite contaminant: Coagulase-negative Staphylococcus spp., Bacillus spp., Micrococcus spp., Corynebacterium spp., Propionibacterium spp., Diphtheroids

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Blood Culture Interpretation
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S53
In this article, we describe the stepwise plan of the ANISA study for dealing with blood culture isolates and for determining their clinical significance for the respective infants.
DEFINING BLOOD CULTURE ISOLATES AS PATHOGENS AND CONTAMINANTS
The ANISA study group convened a workshop on Feb-ruary 13–14, 2012, in Atlanta to plan the best way to perform valid blood cultures, ranging from phlebotomy to identification of potential pathogens. The workshop participants reached a consen-sus to designate isolates as (1) contaminants, (2) true pathogens or (3) probable pathogens. This classification was informed by an extensive literature review and experts’ analyses of neonatal infection etiology. Among these 3 groups, the contaminants and the true pathogens (Table 1) were classified using a predeter-mined approach based on the literature review9 and the opinions of the Technical Advisory Group members. The participants also decided that microbiologic characteristics of the common con-taminants would be recorded in a standardized laboratory book and entered into a database for future review.
PROBABLE PATHOGENSThis group of isolates is a challenge for the ANISA study
for 3 reasons:
1. Most of the probable pathogens are omnipresent in the South Asian environment.
2. They frequently colonize the skin of newborns.6
3. Colonizing organisms may also be causative agents of bloodstream infection in newborns.
The ANISA study introduced different tools for collection of additional data (Table 2) to enrich microbiologic and clinical information and facilitate the classification of probable pathogens as true pathogens or contaminants.
GROWTH OF MULTIPLE ORGANISMSIn the ANISA protocol, growth of multiple organisms in
blood culture is considered as a strong sign of contamination. This classification was made based on the study design that involves identifying infants with possible serious bacterial infection by active surveillance in the community and referring the cases to a study physician at the primary stage of disease. Infants having underlying diseases, congenital anomalies, a compromised immune system or recent hospitalization (to eliminate potential nosocomial acquisition) are excluded.
All cases of multiple isolates are thoroughly analyzed and decisions on their classification are made as per the protocol:
1. Mixed growth with all contaminating organisms are dis-carded as contaminants.
2. Any nonskin colonizing pathogen (eg, Streptococcus pneumoniae, Haemophilus influenzae) among mixed growths is considered as a true pathogen.;
3. Skin colonizing true pathogens (Klebsiella pneumoniae, Escherichia coli, etc) and any mixture of probable patho-gens are placed for expert review, as we do for pure iso-lates of probable pathogens (see above).
As mentioned in the ANISA microbiology methods article,10 specimens with multiple pathogens are also cultured on selective media (gentamicin blood agar for S. pneumoniae and bacitracin chocolate agar for H. influenzae) to determine whether the fastidious slow-growing true pathogens are masked by the fast-growing ones.
EXPERT REVIEWSOn the basis of information mentioned in Table 2, a 4-member
expert team (consisting of 2 infectious disease specialists, a pediatri-cian and a microbiologist) reviews all cases of probable and definite pathogens and mixed growths from blood culture. The team’s decisions are finalized by consensus. In case of disagreement or insufficient data to reach a conclusion, the expert team requests additional information from the database and the site teams on the respective cases and then reevaluates them. This stepwise review by the experts is based on the multiple criteria including (1) clinical condition of the particular infant at the time of enrollment; (2) identification of the pathogen and its role in causing sepsis; (3) antibiogram with minimal inhibitory concentra-tion level or zone diameter; (4) antibiotic(s) given and their relation-ship to the susceptibility pattern; (5) clinical condition of the baby in the days after enrollment as a case and (6) finally, in case of treatment failure, the result of the second blood culture.
CONCLUSIONThe comprehensive evaluation of blood culture isolates will
facilitate the identification of true cases of bloodstream infection. This process should generate high-quality data on blood culture-based etiology of neonatal infections and contribute to the analysis of disease burden data on neonatal sepsis and mortality in South Asia.
REFERENCES 1. Baqui AH, El-Arifeen S, Darmstadt GL, et al; Projahnmo Study Group.
Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: a clus-ter-randomised controlled trial. Lancet. 2008;371:1936–1944.
TABLE 2. Information Used to Classify Probable Pathogens in the ANISA Study
Data Used for Analysis Comments
Time to positivity (time of inoculation to beep positivity) Data available from BACTEC machine (Becton, Dickinson and Company, Franklin Lakes, NJ). In case of true positives, magnitude remains high leading to low time to positivity
Clinical data collected as part of active surveillance Available from ANISA routine follow-up in longitudinal cohortExtra visit to household for infants with beep-positive blood
cultures for clinical assessment and obtaining history of treatment of infant
These data help to assess patient’s response to treatment
Antibiogram of the isolate (true and probable pathogens) Antibiotic susceptibility pattern helps correlate treatment with clinical success/failure
Clinical response on follow-up As aboveSecond blood culture if there is no response to treatment and
change of antibiotic warrantedThis step helps to identify persistence of organism in cases of
treatment failure

Hossain et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S54 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
2. Baqui AH, Darmstadt GL, Williams EK, et al. Rates, timing and causes of neonatal deaths in rural India: implications for neonatal health programmes. Bull World Health Organ. 2006;84:706–713.
3. Farzin A, Saha SK, Baqui AH, et al; Bangladesh Projahnmo-2 (Mirzapur) Study Group. Population-based incidence and etiology of community-acquired neonatal viral infections in Bangladesh: a community-based and hospital-based surveillance study. Pediatr Infect Dis J. 2015;34:706–711.
4. Darmstadt GL, Saha SK, Choi Y, et al; Bangladesh Projahnmo-2 (Mirzapur) Study Group. Population-based incidence and etiology of community-acquired neonatal bacteremia in Mirzapur, Bangladesh: an observational study. J Infect Dis. 2009;200:906–915.
5. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
6. Hall KK, Lyman JA. Updated review of blood culture contamination. Clin Microbiol Rev. 2006;19:788–802.
7. Mullany LC, Saha SK, Shah R, et al. Impact of 4.0% chlorhexidine cord cleansing on the bacteriologic profile of the newborn umbilical stump in rural Sylhet District, Bangladesh: a community-based, cluster-randomized trial. Pediatr Infect Dis J. 2012;31:444–450.
8. Choi Y, Saha SK, Ahmed AS, et al. Routine skin cultures in predicting sepsis pathogens among hospitalized preterm neonates in Bangladesh. Neonatology. 2008;94:123–131.
9. Hossain B, Islam MS, Rahman A, et al. Understanding bacterial isolates in blood culture and approaches used to define bacteria as contaminants: a literature review. Pediatr Infect Dis J. 2016;35 (Suppl 1):S45–S51.
10. Saha SK, Islam MS, Qureshi SM, et al. Laboratory methods for determin-ing etiology of neonatal infection at population-based sites in South Asia: the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S16–S22.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S55
Supplement
Background: Despite the high rate of deaths in young infants (0-59 days) attrib-utable to infections in resource-poor countries, data on bacterial and viral eti-ologies of community-acquired infections in this age group are limited. These data are needed to develop appropriate preventive strategies and suitable anti-biotic treatment regimens for reducing the number of young infant deaths from infections. The Aetiology of Neonatal Infection in South Asia (ANISA) study is designed to generate these critical data and is being implemented in Bangladesh, India and Pakistan. The Sylhet site in Bangladesh was selected because neonatal mortality is high in this country and particularly in Sylhet District. In this article, we describe the contextual challenges in implementing the ANISA study in Syl-het, as well as the strategies developed by our team to address these challenges.Contextual Challenges: The major challenge in implementing the ANISA pro-tocol in Sylhet is conducting the first postnatal visit within 24 hours of birth. This problem stems from several social, cultural and geographical characteris-tics of the study population and its demographic profile. In this area, most births take place at home, referral compliance for newborn illness to health facilities is low and the blood culture contamination rate is high. Community mobilization, cellphone-based birth notification by families, delivery of quality services at study hospitals and referral support to families in need were some of the strate-gies adopted by the Sylhet site team for overcoming these challenges during study implementation. Quality control in specimen collection, transportation and processing also plays a role in ensuring satisfactory performance.Conclusion: Our research team, with support from the ANISA coordina-tion center, has successfully addressed these challenges and is implement-ing the study protocol while maintaining the high quality benchmark set by the coordination center.
Key Words: Sylhet, neonatal, pSBI, referral compliance, ANISA, commu-nity based
(Pediatr Infect Dis J 2016;35:S55–S59)
Data on etiologies and risk factors for community-acquired newborn infections are limited from developing countries
where the burden of neonatal deaths is high and up to half of these
deaths are attributable to infections.1–8 The Aetiology of Neonatal Infection in South Asia (ANISA) study, being conducted in Bang-ladesh, India and Pakistan, is designed to generate these critical data. The study objectives are to generate population-based data on bacterial and viral etiologies, risk factors and antibiotic resist-ance patterns of community-acquired infections in young infants less than 2 months old.
Bangladesh is one of the 10 countries of the world with the highest rates of neonatal mortality.9 The ANISA study is being conducted in Sylhet, Bangladesh, by the Project for Advancing Health of Newborns and Mothers (Projahnmo) study group, a research partnership of the Johns Hopkins University, Child Health Research Foundation, the International Centre for Diarrhoeal Dis-ease Research and Shimantik (a Bangladeshi nongovernmental organization). Since 2001, Projahnmo has conducted 2 large clus-ter-randomized controlled trials10,11 and a dozen formative research and observational studies in the Sylhet site. Bimonthly community surveillance for identifying and recording pregnancies, births, neo-natal morbidity and mortality is well established in the study areas. However, the site had not conducted an etiology study on this scale.
The ANISA study design and methodologies are described in separate articles in this supplement.12–14 Since the inception of ANISA in Sylhet, trained Community Health Workers (CHWs) fol-low all married women of reproductive age in a defined geographi-cal area for identification of pregnancies and births. CHWs visit all newborns 10 times in the first 59 days of life (3 times in the first week and once a week for the subsequent 7 weeks). At every visit, CHWs assess newborns for signs of possible serious bacterial infection (pSBI) and refer ill-appearing newborns to a designated health care facility where they are evaluated by trained physicians and treated as per World Health Organization Integrated Manage-ment of Childhood Illness guidelines. Blood and nasopharyngeal-oropharyngeal (NP-OP) swabs are collected from physician-con-firmed cases. Samples are also collected from randomly selected healthy young infants who are stratified by age and seasonality.15 These specimens are transported to the site laboratory in Sylhet and tested for viral and bacterial pathogens using conventional and molecular techniques. A text message-based system is used to record pregnancies, births, referral of sick young infants, enroll-ment of physician-confirmed pSBI cases and selection of healthy controls.15 In this article, we describe the contextual challenges encountered in implementing the ANISA study in the Sylhet site and the remedial measures the study team has undertaken to over-come these challenges.
STUDY SITE AND ITS DEMOGRAPHIC CHARACTERISTICS
The Sylhet site is located in the northeast of the country, 270 km from the capital city of Dhaka (Fig. 1). The ANISA study is conducted in 14 of the 18 unions (lowest administrative unit with average population of 25,000) of 2 subdistricts (Zakiganj and Kan-aighat) with a total area of 670 km2, a population of ~400,000 and
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S55DOI: 10.1097/INF.0000000000001108
Implementation of the ANISA Protocol in Sylhet, Bangladesh
Challenges and Solutions
Dipak K. Mitra, PhD, MPH, MBBS,* Arif Mahmud, MIH,* Nazma Begum, MA,* Iftekhar Rafiqullah, MSc,† Arunangshu Roy, MBBS,* Syed Mamun Ibne Moin, BSc,* Maksuda Islam, BA,† Md Abdul Quaiyum, MBBS,‡
Jannatul Ferdous, MPH,‡ Jennifer A. Applegate, MSPH,* Samir K. Saha, PhD,† and Abdullah H. Baqui, DrPH*
Accepted for publication January 10, 2016. From the *Johns Hopkins Bloomberg School of Public Health, Johns Hopkins
University, Baltimore, Maryland; †Child Health Research Foundation, Dhaka, Bangladesh; and ‡Centre for Reproductive Health, International Centre for Diarrhoeal Disease Research, Bangladesh, Dhaka, Bangladesh.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Dipak Kumar Mitra, PhD, MPH, MBBS, Depart-ment of International Health, International Center for Maternal and New-born Health, Bloomberg School of Public Health, Johns Hopkins University, 615 N. Wolfe Street, Baltimore, MD 21205. E-mail: [email protected].

Mitra et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S56 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
an estimated annual birth cohort of 9000. The remaining 4 unions were excluded because they were involved in an earlier randomized trial with interventions to reduce newborn infections. The study area represents a typical rural community in Bangladesh with the majority of the population employed in agriculture. The area was previously mapped and enumerated, and all households were sur-veyed for sociodemographic information. Geographic information system data were collected from the area, including coordinates of households, health workers’ residences and available health ser-vices in the vicinity.
Sylhet District has the poorest health indicators in Bangla-desh.16 Selected health and family planning indicators of the study population are shown in Table 1.
The pilot phase was initiated in one third of the Sylhet site on June 20, 2011. The entire area was brought under full study cov-erage by the end of August 2011. The site’s performance was evalu-ated by the ANISA Technical Advisory Group against benchmark indicators (Table 2), and the site was incorporated into the main study in November 2011.
Project staffs are grouped into 4 teams: (1) field surveil-lance; (2) study hospital; (3) laboratory and 4) data management. Most of the field personnel were recruited from the pool of expe-rienced staff working in previous studies. The field surveillance
team is responsible for identification of pregnancies, births and cases of pSBI in the community. Female CHWs are the frontline staff for surveillance activities, each working in an area of ~3000 population. In most instances, a CHW has at least a 10th grade education and is a resident of her surveillance area. The hospital team consists of research assistants, phlebotomists, study physi-cians and porters. Research assistants help the team in overall study activities, while phlebotomists collect clinical specimens from young infants. Study physicians screen referred newborns for signs of pSBI, and the porters pick up and transport specimens to the site laboratory in Sylhet for processing, testing, storage and shipping to the reference laboratory in Dhaka. The data manage-ment team is responsible for data entry and cleaning, and regular upload of data to the central server located at the ANISA Data Coordination Center in Dhaka.
The ANISA Study Coordination team organized a 6-day master training in Dhaka for physicians and senior project staff from all sites. This training included field procedures, pSBI assessment of newborns and laboratory activities for site personnel. Standard-ized training materials include field manuals, laboratory operating procedures and data capture forms. The Sylhet team developed a site-specific training plan for staff in light of these materials. Study documents for field workers include the pregnant women register and CHW monthly planner. All tools have been translated into Bangla, the local language. pSBI assessment training for CHWs and field supervisors was organized in the pediatric and obstetric wards of Sylhet M.A.G. Osmani Medical College Hospital with sick and healthy newborns for training and standardizing the work of all field workers. Six-monthly refresher training is conducted for all field staff, and on-the-job training is imparted regularly to CHWs by supervisory staff.
ETHICS CLEARANCEThe study protocol was reviewed and approved by the Ethi-
cal Review Committee of the International Centre for Diarrhoeal Disease Research and the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health.
FIGURE 1. ANISA study site in Sylhet, Bangladesh.
TABLE 1. Selected Health and Family Planning Indicators in Bangladesh and Sylhet District of Bangladesh, 200716
Indicator BangladeshSylhet District
Neonatal mortality rate/1000 live births 32 45Infant mortality rate/1000 live births 43 59<5 mortality rate/1000 live births 53 71Contraceptive use rate (%) 61.2 44.8Total fertility rate 2.3 3.1Crude birth rate/1000 population 18.5 21.3Facility delivery rate 15% 8.6%

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Sylhet, Bangladesh
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S57
CHALLENGES IN ADOPTION OF THE ANISA PROTOCOL AND REMEDIAL ACTIONS
Field ActivitiesEarly First Postnatal Home Visit by CHW
Achieving 80% of first postnatal visits within 12 hours of birth, including 50% of visits within 6 hours, presents a great chal-lenge to the team, even though 87% of first visits were conducted within 24 hours of birth in the Projahnmo study.17 The majority (80%) of births take place at home, and CHWs need to be notified as soon as possible after a birth has taken place so that they can plan and conduct a visit. Moreover, half the births take place at night, and it is difficult for the female CHWs in these rural communities to visit the newborns then due to limited availability of transport. We deployed a system to receive notifications as soon as possible via a mobile phone call to CHWs by family members (82% own a mobile phone) and trained birth attendants in that area. We also set up a 24-hour call center to facilitate real-time planning for early postnatal visits by CHWs based on birth notifications. We compen-sate CHWs for additional work hours and cover their transportation costs for working outside stipulated office hours to make an early postnatal visit (Table 3).
We conduct extensive community mobilization and family counseling activities highlighting the importance of the ANISA study, particularly for ensuring the security of CHWs while
working during the early morning or late afternoon. These efforts have improved the proportion of birth notifications within 1 hour of delivery from less than 50% in the pilot phase to nearly 80% in the main study (study monitoring data). Almost 90% of neonates born in the surveillance area are successfully registered by CHWs within 7 days of birth. The proportion of newborns visited within 6, 12 and 24 hours after delivery has remained consistently high throughout the study period (Fig. 2). However, despite this high rate of early first postnatal visits, 43% (363/849) of neonatal deaths occur before the CHWs can reach newborns.
Referral Compliance of Sick Newborns to Designated Study Hospitals
Achieving high referral compliance for sick newborns to study hospitals is critical but has been a great challenge. Through dialogue with community leaders and stakeholders, we identified barriers to referral compliance, and designed and implemented various strategies to improve them.
Shortage of physicians and interrupted supply of drugs are 2 important shortcomings of the public sector health system in Bangladesh.18–20 Most of the families in the study area seek health care from private health care providers. To address this issue, we recruited full-time physicians at the government-run subdistrict hospitals and provide required medications at no cost to patients. Inability to pay transportation costs and unavailability of a family member to accompany the mother of a sick newborn to the hospital are 2 additional barriers to referral compliance. In response, we reimburse transportation costs to poor families from project funds. Upon a mother’s request, a CHW accompanies her and her sick newborn to a designated study hospital. Referral compliance has continued to improve with these efforts (Fig. 3).
Specimen Collection from Young InfantsCollection of blood and NP-OP specimens from young
infants, particularly from healthy controls, has been a major chal-lenge. Obtaining specimens for microbiologic diagnosis of pSBI is not a routine practice at subdistrict hospitals. We identify key com-munity stakeholders, including local government representatives, schoolteachers and community leaders and hold regular meetings with them. Speaking in the local language and manner, we discuss the study’s purposes and its direct benefits to sick newborns as well as its long-term societal benefits. Our field monitoring data show
TABLE 2. Etiology of Neonatal Infection in South Asia Technical Advisory Group Process Targets
Indicator Achievable Target
Pregnancy identification against estimated number of pregnancies 95%Enrollment of live-born infants born to registered pregnant women 90%First postnatal visits within 6 hours of delivery 50%Blood specimen collection from all physician-confirmed infection cases 80%NP-OP specimen collection from all physician-confirmed infection cases 90%Blood specimen collection from healthy control infants 50%NP-OP specimen collection from healthy control infants 95%
TABLE 3. Compensation Protocol for Additional Work by CHWs
Time Birth Information Received Time of First Postnatal Visit Additional Cost
Between 6:00 am and 9:00 am Immediately after information YesBetween 9:00 am and 4:00 pm Immediately after information NoBetween 4:00 pm and 6:00 pm Immediately after information YesBetween 6:00 pm and 6:00 am As early as possible after 6:00 am No
*Source: ANISA data from database
40
60
80
100
Firs
t pos
tnat
al v
isit
timin
g (%
)
Within 6 hours
Within 12 hours
Within 24 hours
FIGURE 2. Timing of first postnatal visit by CHWs, November 2011–November 2013.

Mitra et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S58 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
rates of blood and NP-OP specimen collection from physician-con-firmed pSBI cases to be 80% and 88%, respectively.
Laboratory ActivitiesTransportation of Specimens from Study Hospitals
The average travel time between hospitals and the laboratory is 4 hours using public transport, making transportation of speci-mens to the site laboratory within 6 to 8 hours of collection (the time after which the probability of false negative results increases) challenging. We recruited additional porters and established hourly shipment from the hospitals so that specimens reach the laboratory within 6 hours of collection. Using this strategy, we can transport 85% of specimens within the required time. Specimens collected in late afternoon or at night are kept at the hospitals in incubators and are shipped the next morning. Blood culture bottles received at the site laboratory after 8 hours of inoculation are treated as delayed vial entry and are processed using improved laboratory techniques designed for this study.13
Contamination of Blood CultureDuring the initial months of the study, we experienced a high
contamination rate in blood cultures. Our team carried out several measures to contain the contamination rate at the acceptable level (<10%) set by the Technical Advisory Group. We deployed a team of 2 phlebotomists instead of one to assist each other in ensuring proper aseptic procedures. Supervision and monitoring of phle-botomists are enhanced by using a checklist and video recording of blood collection procedures. The study team holds weekly meet-ings to review findings of the checklists and videos. This strategy has been extremely helpful in identifying errors and undertaking
subsequent remedial actions. Several measures have helped to bring down the contamination rate from 25% in the pilot phase to less than 10% and maintain it throughout the main study (Fig. 4): introduction of a separate specimen collection area with restricted entry; blood collection tables with easily cleanable surfaces; dis-posable sterile sheets for every young infant; regular cleaning of window screens and weekly fumigation of the rooms.
Data Management ActivitiesWe faced several issues with data management at the begin-
ning of the study. One major challenge was the training of CHWs on correctly sending text messages to the central server located in Dhaka, as the CHWs use mobile phones that differ in system configuration and network carrier. To overcome this issue, we pro-vided one particular model of cell phone with a single carrier to all CHWs.
SUMMARY AND CONCLUSIONSANISA is a large etiology study that should generate inval-
uable data for future decision-making in improving young infant health in low-resource settings. The major objective of ANISA is to capture all episodes of infection in young infants (0–59 days) including early onset ones. This study should detect vertical trans-mission of infections, such as group B streptoccocus, in this pop-ulation. We detect viral etiologies using sophisticated molecular techniques that will add useful data to the evidence base of neona-tal infections. Blood and NP-OP specimens from healthy controls for molecular testing should help in interpreting the findings from pSBI cases.
Even in an established research site such as Sylhet, imple-mentation of the ANISA protocol has not been easy. However, the Sylhet site team, with support from the ANISA Study Coordination Team, has successfully overcome most of the challenges in imple-mentation. Lessons learned in this setting are expected to be of value to researchers in designing and implementing similar studies in resource-poor settings.
ACKNOWLEDGMENTSThe authors thank the members of the Projahnmo study team
and colleagues at the Bangladesh Ministry of Health and Family Welfare for their valuable help and advice. The authors also thank the individuals in Sylhet District who gave their time generously, including the community of the research site who are participating in this study.
REFERENCES 1. Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? where?
why? Lancet. 2005;365:891–900.
2. Stoll BJ. The global impact of neonatal infection. Clin Perinatol. 1997;24:1–21.
3. Bahl R, Martines J, Ali N, et al. Research priorities to reduce global mortality from newborn infections by 2015. Pediatr Infect Dis J. 2009;28:S43–S48.
4. Baqui AH, Darmstadt GL, Williams EK, et al. Rates, timing and causes of neonatal deaths in rural India: implications for neonatal health programmes. Bull World Health Organ. 2006;84:706–713.
5. Newton O, English M. Young infant sepsis: aetiology, antibiotic susceptibil-ity and clinical signs. Trans R Soc Trop Med Hyg. 2007;101:959–966.
6. Darmstadt GL, Batra M, Zaidi AK. Oral antibiotics in the management of serious neonatal bacterial infections in developing country communities. Pediatr Infect Dis J. 2009;28(1 Suppl):S31–S36.
7. Ganatra HA, Zaidi AK. Neonatal infections in the developing world. Semin Perinatol. 2010;34:416–425.
8. Ganatra HA, Stoll BJ, Zaidi AK. International perspective on early-onset neonatal sepsis. Clin Perinatol. 2010;37:501–523.
*Source: ANISA data from database
40
60
80
100
Ref
erra
l com
plia
nce
(%)
0-6 Days 7-59 Days
FIGURE 3. Referral compliance of sick young infants, November 2011–January 2014.
*Source: Laboratory monitoring data
0
10
20
30
40
50
Con
tam
inat
ion
(%)
FIGURE 4. Blood culture contamination rate, July 2011–November 2013.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Sylhet, Bangladesh
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S59
9. Lawn JE, Kerber K, Enweronu-Laryea C, et al. 3.6 million neona-tal deaths–what is progressing and what is not? Semin Perinatol. 2010;34:371–386.
10. Baqui AH, El-Arifeen S, Darmstadt GL, et al. Effect of community-based newborn-care intervention package implemented through two service-deliv-ery strategies in Sylhet district, Bangladesh: a cluster-randomised controlled trial. Lancet. 2008;371:1936–1944.
11. Arifeen SE, Mullany LC, Shah R, et al. The effect of cord cleansing with chlorhexidine on neonatal mortality in rural Bangladesh: a community-based, cluster-randomised trial. Lancet. 2012;379:1022–1028.
12. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
13. Saha SK, Islam MS, Qureshi SM, et al. Laboratory methods for determining etiology of neonatal infection at population-based sites in South Asia: the ANISA study. Pediatr Infect Dis J. 2016;35 (suppl 1):S16–S22.
14. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35 (Suppl 1):S39–S44.
15. Islam MS, Rahman QS, Hossain T, et al. Using text messages for critical real-time data capture in the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S35–S38.
16. Bangladesh Demographic and Health Survey. Bangladesh Demographic and Health Survey 2007. Dhaka, Bangladesh and Calverton, Maryland, USA: National Institute of Population Research and Training, Mitra and Associates, and Macro International; 2009.
17. Shah R, Munos MK, Winch PJ, et al. Community-based health workers achieve high coverage in neonatal intervention trials: a case study from Sylhet, Bangladesh. J Health Popul Nutr. 2010;28:610–618.
18. Mendoza Aldana J, Piechulek H, et al. Client satisfaction and qual-ity of health care in rural Bangladesh. Bull World Health Organ. 2001;79:512–517.
19. Roy SR, Ahmed MS. Perception of indoor patients on the services of some Thana Health Complexes. Bangladesh Med Res Counc Bull. 1995;21:46–49.
20. Chowdhury S, Hossain SA, Halim A. Assessment of quality of care in maternal and newborn health services available in public health care facilities in Bangladesh. Bangladesh Med Res Counc Bull. 2009;35:53–56.

S60 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
Supplement
Background: Aetiology of Neonatal Infection in South Asia (ANISA) is a multicenter study in Bangladesh, India and Pakistan exploring the inci-dence and etiology of neonatal infections. A periurban site in Karachi was selected for its representativeness of the general population in neonatal health indicators. An established demographic surveillance system and other infrastructure needed for conducting the study already existed at this site. ANISA presents a unique challenge because of the need to capture every birth outcome in the community within a few hours of delivery to reliably estimate the incidence and etiology of early-onset sepsis in a setting where home births and deaths are common.Contextual Challenges: Major challenges at the Karachi site are related to early birth reporting and newborn assessment for births outside the catch-ment areas, parental refusal to participate, diverse ethnicity of the popu-lation, collection of biological specimens from healthy controls, political instability and crime, power outages and blood culture contamination. Some of the remedial actions taken include prolonging working hours; developing counseling skills of field workers; hiring staff with different linguistic abili-ties from within the study community; liaising with health facilities, key community informants, Lady Health Workers and traditional birth attend-ants; hiring community mobilizers; enhancing community sensitization; developing contingency plans for field work interruptions and procuring backup generators. The specimen contamination rate has decreased through training, supervision and video monitoring of blood collection procedures with individualized counseling of phlebotomists.Conclusion: ANISA offers lessons for successful implementation of com-plex study protocols in areas of high child mortality and challenging social environments.
Key Words: Karachi, challenges, surveillance, ANISA, etiology, possible serious bacterial infection
(Pediatr Infect Dis J 2016;35:S60–S64)
Aetiology of Neonatal Infection in South Asia (ANISA) is a multicenter study in Bangladesh, India and Pakistan. Its pri-
mary objective is to determine the population-based incidence, etiological agents and antibiotic resistance profiles of community-
acquired infections in the first 59 days of life and to determine the risk factors for these infections.
The study site in Karachi is representative of communities in Pakistan where the incidence of neonatal infection is high. This site was selected for ANISA because it had already conducted exten-sive community-based surveillance for identification and follow-up of pregnancies, births and suspected infection cases among new-borns.1 Biological specimens from suspected infection cases were being collected before the start of ANISA.
The detailed methods of ANISA study components have been described elsewhere.2–4 This article aims to highlight the con-textual challenges faced during implementation of the ANISA pro-tocol in the Karachi, Pakistan, site and the remedial actions taken to overcome them. A workflow diagram of key ANISA activities at the Karachi site is detailed in Figure 1.
STUDY SITE AND POPULATIONThe study areas in Karachi consist of 4 periurban low-income
settlements in coastal Karachi [Rehri Goth, Ibrahim Hyderi, Ali Akbar Shah Goth and Bhains (Cattle) Colony] and an urban local-ity (Bilal Colony) covering a total area of 19.8 km2 (Fig. 2). Resi-dents in the coastal areas make their living mainly by fishing, rais-ing dairy cattle and running small retail businesses. Bilal Colony is an urban squatter settlement located in an industrial area where the leather industry is the dominant business.1 The majority of the population resides in small, 1- or 2-room houses made of bricks or bamboo. Where the municipal water supply network is not accessi-ble, residents collect water from community tanks or from vendors.
The Department of Pediatrics and Child Health at Aga Khan University (AKU) conducted a baseline census in the study area in 2010. During that year, the population was 274,000; 25% were women of reproductive age (13–49 years), and 12% were children aged less than 5 years. The gross fertility rate was 131/1000 women of reproductive age, the under-5 mortality rate was 68.8 per 1000 live births and the neonatal mortality rate was 42.7 per 1000 live births. The annual birth cohort is around 8000, and 10.7% of new-borns experience systemic infection within 28 days of birth.
The Karachi site provides an ideal setting for the ANISA study. The Department of Pediatrics and Child Health at AKU has been conducting household surveillance in the study areas for several years, and quarterly pregnancy and newborn surveillance have been in place since 2003. Pregnant women are followed up until delivery, and newborns are followed up until 59 days of age. Trained community health workers (CHWs) assess newborns for signs of possible serious bacterial infection (pSBI) and refer them to 1 of the 5 primary health centers (PHCs) for treatment and/or referral to a hospital. These PHCs are run by AKU and staffed by physicians and paramedics trained in Integrated Management of Childhood Illness.5 This area served as the only community-based site for the Young Infants Clinical Signs Study II, which ended in 2005.6 In 2013, the site completed the multicenter Simplified Anti-biotic Therapy Trial, which evaluated regimens for the management
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S60DOI: 10.1097/INF.0000000000001109
Implementation of the ANISA Study in Karachi, Pakistan
Challenges and Solutions
Yasir Shafiq, MSc, Muhammad Imran Nisar, MSc, Abdul Momin Kazi, MPH, Murtaza Ali, BS, Saima Jamal, MA, Muhammad Ilyas, MSc, Fyezah Jehan, MSc, Shazia Sultana, MSc, Shahida M. Qureshi, MSc,
Aneeta Hotwani, MSc, and Anita K. Zaidi, SM
Accepted for publication January 10, 2016.From The Aga Khan University, Karachi, Pakistan.The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant
No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Muhammad Imran Nisar, MSc, Department of Pediatrics and Child Health, The Aga Khan University, Karachi, Pakistan. E-mail: [email protected].

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Karachi, Pakistan
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S61
ANIS
A L
ab O
pera
tions
AN
ISA
Fie
ld O
pera
tions
AN
ISA
Dat
a M
anag
emen
t
Mai
n La
b Fi
eld
Team
C
ompo
nent
A
NIS
A P
roce
dure
Fi
eld
Mai
n D
ata
Man
agem
ent U
nit
Det
aile
d lo
ggin
g
100%
QC
Sin
gle
& d
oubl
e da
ta e
ntry
Spe
cim
en p
roce
ssin
g
Res
ult g
ener
atio
n
QA
/QC
of t
he s
peci
men
te
sted
Fina
l dat
a st
orag
e &
bio
ba
nkin
g
Pla
ce in
C
olem
an (2
-8o C
)w
ith ic
e pa
ck;
trans
port
with
in 2
hr
s. to
IDR
L;
keep
in
refri
gera
tor a
t fie
ld s
ite la
b un
til
trans
porte
d to
ID
RL
Bot
h th
roat
and
na
sal f
lock
ed
swab
s co
llect
ed
and
plac
ed in
V
iral T
rans
port
Med
ium
(VTM
)
Mar
ried
wom
en
surv
eilla
nce
team
s
Pre
gnan
t wom
en
follo
w u
p te
ams
Birt
h C
aptu
ring
team
s
New
born
follo
w
up te
ams
3 m
onth
ly m
arrie
d w
omen
sur
veill
ance
Pre
gnan
t wom
en
iden
tific
atio
n &
re
gist
ratio
n
Per
iodi
c pr
egna
nt
wom
en fo
llow
-up
Pre
gnan
cy o
utco
me
&
birth
ass
essm
ent
2 6
1320
2734
4148
59P
ost n
atal
follo
w-u
pvi
sit d
ays
Birt
h re
gist
ratio
n - S
MS
sys
tem
Sel
ecte
d as
he
alth
y co
ntro
l
Ref
erra
l
Ass
essm
ent b
y ph
ysic
ian
Hea
lthy
baby
Con
sent
& e
nrol
led
for s
peci
men
s
Ste
p 9-
Con
sent
&
enro
lled
for
spec
imen
s
Elig
ible
as
susp
ecte
d se
psis
cas
e
Sen
d ba
ck H
ome
Ste
p 1-
Con
sent
&
case
rep
ort F
orm
1
Preg
nanc
y &
de
mog
raph
ic
info
rmat
ion
Ste
p 2
- Ant
enat
alco
unse
ling
pack
age
Ste
p 3
– C
ase
repo
rt fo
rm 2
& 3
Birt
h in
form
atio
n &
se
psis
scr
eeni
ng
Ste
p 5
– C
ase
repo
rt fo
rm 4
a (v
isit
2,6)
& 4
b (v
isit
13-
59)
Ste
p 6
– S
uspe
cted
se
psis
infe
ctio
n
Ste
p 7
– R
efer
ral t
o he
alth
faci
lity
Ste
p 8
– C
ase
repo
rt fo
rm 6
Elig
ibili
ty c
riter
ia
asse
ssed
by
phys
icia
n
Not
elig
ible
as
susp
ecte
d se
psis
ca
se
Stud
y ID
al
lotm
ent
100%
QC
of
case
rep
ort
form
s
Log
of
case
re
port
for
m
Prim
ary
stor
age
of c
ase
repo
rt
form
s
Ent
ry o
f key
id
entif
ier f
or
follo
w-u
p
sche
dulin
g
Det
aile
d lo
ggin
g
100%
QC
& p
ost
codi
ng
Sing
le &
dou
ble
data
en
try
Dua
l err
or d
iscr
epan
cy
clea
ning
CR
F m
ergi
ng to
cre
ate
fina
l cas
e fi
le
Inco
nsis
tent
& lo
gica
l da
ta c
lean
ing
Fina
l dat
a st
orag
e
ED
TA T
ube
(1.0
ml)
for b
oth
heal
thy
cont
rol &
se
psis
cas
e
Bac
tec
bottl
e (2
.0
ml)
for s
epsi
s ca
se o
nly
Pla
ce b
ottle
in
Col
eman
with
out
ice
pack
s (2
5-28
o C);
tran
spor
t w
ithin
2 h
rs. t
o ID
RL
for
pr
oces
sing
Cas
e re
port
form
7b
-Blo
od
spec
imen
s
Cas
e re
port
form
7a
-Nas
al &
Ora
l sp
ecim
ens
FIG
UR
E 1.
Workfl
ow diagram
of k
ey ANISA activities at Ka
rach
i site
, Pakistan. EDTA
indicates ethy
lene
diam
inetetraacetic acid; Q
A, q
uality assuranc
e; Q
C, q
uality
control.

Shafiq et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S62 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
of clinically diagnosed severe infections in newborns and young infants in first-level facilities.1
ANISA was launched at the Karachi site in August 2011. Several performance indicators were used to evaluate the site’s sta-tus to qualify for moving from the pilot phase to the main study. Implementation of all key field and laboratory activities was peri-odically monitored during the pilot phase. The Karachi site joined the main study on January 1, 2012, upon satisfactory performance in these key activities.4
Standardized training material was provided by the ANISA Coordination Team for harmonization of project objectives across all study sites. Training materials, manuals and data collection forms were translated to Urdu, the most commonly spoken language in the area. A site-specific training plan for each group of project staff was devised and implemented by the site principal investigator. Refresher training was held every 6 months in groups of 25 participants, con-ducted by senior research staff. The needs-based training sessions were held for both individuals and groups based on monthly per-formance and monitoring reports. The study physicians were trained according to the World Health Organization Integrated Management of Childhood Illness protocols, and periodic refresher courses were held every 6 months. All newly hired staff were trained on the basic package during their first week of employment and accompanied a senior team member for at least 1 month in the field after that.
ETHICS CLEARANCEThe project protocol, consent forms and data collection
forms were approved by the Ethical Review Committee at AKU. Six monthly progress reports are submitted to the Committee.
CHALLENGES IN IMPLEMENTING THE ANISA PROTOCOL AND REMEDIAL ACTIONS
Field ActivitiesEarly Newborn Registration and Assessment
Registration and assessment of newborns within 24 hours of birth for signs of pSBI is difficult in a periurban setting. Around 30% of the mothers in the study area deliver at any 1 of the more than 100 facilities spread across the city of Karachi. Therefore, we needed to maintain a list of health care facilities, both within and outside the surveillance area, where around 60% of the facility deliveries take place. We obtained approval from these facilities for study staff to independently assess newborns there. Through these arrangements, we have been able to register and assess nearly 30% of the ANISA infants born in facilities outside the surveillance area.
To encourage early birth notification, staff regularly coun-sel families about the importance of the study and the benefits
of a comprehensive newborn assessment by a well-trained CHW. These measures have contributed to the reporting of 30% of births by the families themselves. We also enlist the help of key inform-ants working in the locality, including government-employed Lady Health Workers and independent traditional birth attendants, to assist in timely notification of births. Around 8%–10% of births are reported by these key informants.
Selected senior CHWs residing in the community are paid overtime to make home visits when families notify them of births that have taken place outside regular CHW working hours.
Parental Refusal for Newborn AssessmentAround 10% of families refuse assessment of their new-
borns in the early days after birth for sociocultural reasons. These families are approached by senior project staff who assure them that the assessment will not harm the newborn and can in fact ben-efit the infant by identifying underlying health problems. The social mobilizers are able to convince nearly 50% of the families who initially refused to consent to the newborn assessment.
Diverse Ethnic DistributionThe diverse sociodemographic and ethnic distribution of the
Karachi site can sometimes create obstacles to efficient data collec-tion. A wide array of languages is spoken, and CHWs do not always speak the same language as the household residents. To remedy this problem, almost all the health workers are hired and trained from within blocks of homogenous ethnic distribution. In instances where study participants do not speak the same language as data collectors, help is sought from a translator in the same or a neigh-boring household.
Collection of Biological Specimens From Healthy Controls
Parents of healthy newborns selected as controls are often reluctant to provide blood and nasopharyngeal and oropharyngeal specimens, especially on the first day of life. Community mobiliz-ers were hired and received a 1-week training course to sensitize the community and counsel parents about the importance of the study in the local, regional and global context. This strategy reduced the refusal rate for the first day of life from 70% to around 57% and has helped in enrolling the required number of controls for the case-control component of the study.
Political Instability and CrimeThe study sites are at times affected by strikes, protests and
shutdowns, which result in suspension of routine field activities. A contingency plan is in place to prioritize early newborn registra-tion and assessments. Specific CHWs residing in affected areas are
FIGURE 2. ANISA study sites in Karachi, Pakistan, August 2011 to December 2013.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Karachi, Pakistan
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S63
assigned to register and assess newborns, taking their own safety into account. Activities in 1 of the 5 study sites, Bilal Colony, were completely suspended after October 2013 because of the deteriorat-ing safety situation, including the kidnapping of one of the study physicians who was later rescued alive.
Power OutagesPower outages are frequent in the city of Karachi and affect
the field site PHCs, which serve as the site offices for the study staff and house the site laboratories. Backup generators are in place at the PHCs to ensure an uninterrupted power supply and smooth operations.
Laboratory ActivitiesKarachi site’s facilities consist of 5 field laboratories for
specimen collection and a central Infectious Disease Research Laboratory (IDRL) at AKU, located an hour’s drive from the field laboratories. All specimens are collected at these field sites, and a designated person has been hired to make 2 round trips per day to collect specimens from the laboratories and bring them to the IDRL where further processing is carried out (Fig. 3).
Blood culture contamination was initially the biggest laboratory-related challenge at the Karachi site, and the site has
instituted several measures to address this. A laboratory coordina-tor was hired to visit all field sites to ensure proper blood draw-ing by the phlebotomists. Every specimen is collected under the direct supervision of a study physician who fills out a checklist, and every blood draw is video recorded after obtaining consent of the family. The videos and checklists are used to perform causal analysis if contamination occurs. Antiseptic chlorhexidine spray and sterile gloves are also used to enhance asepsis during speci-men collection. Fly-proof nylon netting is placed on all open win-dows at PHCs. Turnover of trained phlebotomists is managed by monthly refresher training using pictorial and video training tools to demonstrate aseptic blood collection techniques. These reme-dial actions have successfully brought down the contamination rate from as high as 22% in the first 6 months of the study to less than 3% (Fig. 4).
In the molecular section of the laboratory, one of the machines, a TaqMan Array Card platform (Life Technologies, Fos-ter City, CA), for processing the blood and nasopharyngeal and oropharyngeal specimens malfunctioned, creating a large backlog of specimens to be tested. A replacement TaQMan Low Density Arrays machine was provided by the ANISA Coordination Team and has helped to reduce the backlog.
FIGURE 3. Specimen collection and transportation flow at Karachi, Pakistan, site.

Shafiq et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S64 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
Data ManagementData management is a challenge because of the large num-
ber of cases and data collection forms. To handle around 30,000 cases with an estimated data collection form volume of 212,600, storage was organized on multiple levels with forms sorted accord-ing to study identification number. We used a system of logging and rigorous checking at every step of data entry and storage.
For data management software, e-mail communications with details and screen shots of problems were used to resolve database management issues. The ANISA Data Coordination Center staff used TeamViewer (TeamViewer GmbH, Göppingen, Germany) software for remote administration of site computers, for addressing data range checks and for other bug fixing related to the database.
In some of our surveillance areas, mobile phone networks are occasionally blocked by the government for national security reasons, which impedes the text message-based system of control selection. A person at the site’s data management unit regularly checks the ANISA main system’s text message module for controls selected in areas with no mobile phone coverage and notifies the field supervisor immediately to arrange the assignment of a CHW for that newborn’s registration as a control.
SUMMARY AND CONCLUSIONANISA presents a unique challenge and also an opportu-
nity to the study team in Karachi. Challenges range from field site activities such as collection, transport and analysis of specimens to management of large amounts of data. Issues in these domains have been tackled successfully by the Karachi site team led by the site’s principal investigator, reaffirming that large and complex studies in the regions with the highest disease burden can be carried out by local teams in a highly efficient manner.
However, a few challenges could not be overcome. The most important was registering and assessing the newborns who died in the first few hours after birth. As most of these deaths took place at home, CHWs could not reach the house before death and no interventions could be made. In addition, no cerebrospinal fluid specimens have been collected from the young infants identified with pSBI, as this type of specimen collection is not possible in the
primary care settings where cases are enrolled. Finally, although we were able to bring down the refusal rate for control enrollment, the families of more than half of the controls selected on the first day still refuse to participate.
We believe that ANISA’s results will inform local clinicians, public health professionals and policy makers about the burden and causes of serious illness in the first 59 days of life. Moreover, ANISA will open doors for more research studies to be carried out by local teams in the field of child health.
ACKNOWLEDGMENTSThe authors are indebted to all the study participants and
their parents. They also thank all the study physicians, field and data management staff who are working relentlessly to make this a successful project, and the study coordination team at the Child Health Research Foundation, Dhaka, for their support. They are grateful to Dr. Shamim A. Qazi, Dr. Salim Saddruddin and Dr. Daniel E. Roth for their invaluable suggestions during moni-toring visits.
REFERENCES 1. Zaidi AK, Tikmani SS, Sultana S, et al. Simplified antibiotic regimens for
the management of clinically diagnosed severe infections in newborns and young infants in first-level facilities in Karachi, Pakistan: study design for an outpatient randomized controlled equivalence trial. Pediatr Infect Dis J. 2013;32(suppl 1):S19–S25.
2. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
3. Rahman QS, Islam MS, Hossain B, et al. Centralized data management in a multicountry, multisite population-based study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S23–S28.
4. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35 (suppl 1):S39–S44.
5. World Health Organization, UNICEF. Integrated Management of Childhood Illness (IMCI) Chart Booklet. Geneva, Switzerland: World Health Organization; 2008.
6. The Young Infants Clinical Signs Study Group. Clinical signs that predict severe illness in children under age 2 months: a multicentre study. Lancet. 2008;371:135.
Jan-
12
Apr-1
2
Jul-1
2
Oct-12
Jan-
13
Apr-1
3
Jul-1
3FIGURE 4. Blood contamination rate at Karachi, Pakistan site, January 2012 to August 2013.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 www.pidj.com | S65
Supplement
Background: The Aetiology of Neonatal Infection in South Asia (ANISA) study is a population-based study with sites in Bangladesh, India and Pakistan. It aims to determine community-acquired incidence, etiology and associated risk factors for neonatal infections. Matiari, a rural site in Pakistan, was chosen for the study due to its high neonatal mortality rate and the presence of an estab-lished pregnancy and birth surveillance system. This article summarizes various challenges, remedial measures taken and lessons learned during the implementa-tion of the ANISA study protocol in the unique rural setting of Matiari where the majority of births take place at home and accessibility to health care is limited. Challenges: Achieving and maintaining project targets of early registration of birth and collection of biological specimens in households have been chal-lenging in Matiari. Capturing births of study subjects that occur outside the catchment areas and those taking place during public holidays and acquiring parental consent for specimen collection from healthy controls require exten-sive community mobilization. Contamination and power outages that affect the laboratory equipment are 2 of the major logistic challenges faced. We keep track of pregnancy outcomes through mobile phones and reimburse the costs for birth notifications to the caller. We created separate dedicated mobile teams that visit newborns outside the catchment area and carry out possible serious bacterial infection assessments. We also formed mobile teams for specimen collection from residences of newborns as there is no facility for specimen collection at this site. Our study personnel work on holidays and weekends to improve the study’s performance. We nurture strong community liaison by employing staff from within the community. We train the study physicians on communication and counseling skills required for overcoming refusal for referral and specimen collection. The contamination rate is controlled by repeated training and supervision and extensive monitoring of phlebotomy activities. The majority of phlebotomy procedures are recorded on video in the field to provide feedback to phlebotomists for improving their performance. Conclusion: The contextual challenges faced in field implementation of the ANISA protocol in the rural setting of Matiari are unique. These challenges are being successfully addressed through hard work, strict monitoring and improvisation. This experience can be used for improving study perfor-mance in similar settings elsewhere.
Key Words: Matiari, neonatal, surveillance, possible serious bacterial infection, etiology, sepsis, ANISA
(Pediatr Infect Dis J 2016;35:S65–S69)
The Aetiology of Neonatal Infection in South Asia (ANISA) uses standard and molecular diagnostic tests for detecting the eti-
ology of community-acquired infections. ANISA staff also collect pre- and postpregnancy information for identifying associated risk factors for possible serious bacterial infection (pSBI) in neonates. These data are collected alongside bimonthly pregnancy surveil-lance, birth surveillance and surveillance of newborns for pSBI. Young infants are followed up to 59 days of age. Blood and naso-pharyngeal-oropharyngeal (NP-OP) swabs are collected from phy-sician-confirmed pSBI cases. Detailed study activities have been described elsewhere in this supplement.1–4 Matiari, Pakistan, was chosen as a study site for ANISA due to its high neonatal mortal-ity rate and the presence of an established community surveillance system.5–8
STUDY SITE AND POPULATIONANISA is conducted in 10 union councils (UCs) in Mat-
iari District, located 185 km north of Karachi (Fig. 1). The study area covers a catchment population of 350,000 with approxi-mately 55,000 married women of reproductive age (MWRA), aged 13–49 years and an annual birth cohort of 8500. One field office is located in Matiari city and another in Hala city, 35 km from Matiari. The site data management unit and site laboratory are located in Matiari city.
Matiari is mainly a rural area, and the primary economic activity of its inhabitants is agriculture. The existing health care infrastructure includes primary, secondary and tertiary care facili-ties.The Matiari study site has 3 rural health centers, 6 basic health units, 1 dispensary and around 220 lady health workers (LHWs). The rural health centers are the primary and secondary care facili-ties, whereas Taluka headquarters and district headquarters are the referral/tertiary care hospitals. LHWs are community-based females employed by Pakistan’s Ministry of Health who deliver maternal and child health services at the household level. LHWs also serve as a link between communities and tertiary level health facilities.
ANISA pilot activities in Matiari were initiated in July 2011 and the site became incorporated into the main study in March 2012 after fulfilling set criteria.4 These criteria included employ-ment and activation of a minimum of 80% of community health workers (CHWs) and their supervisors, active bimonthly MWRA surveillance in place with 5% of CHW visits observed by a supervi-sor, 80% of CHW referrals validated by study physicians, success-ful clinical specimen collection from more than 80% of physician-confirmed pSBI cases and blood collection volume of >1 mL in 80% of phlebotomies conducted.
Staff recruitment started in May 2011. The study team includes 60 CHWs, 18 team leaders, 8 study physicians, 8 phle-botomists and 2 field supervisors. The study area originally was composed of 8 UCs; 2 more UCs were added at the time of gradua-tion. With the expansion of the study area, an additional 60 CHWs, 2 physicians and 2 phlebotomists were recruited in July 2012. Each team is led by a research associate with either a master’s degree or a
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S65DOI: 10.1097/INF.0000000000001110
Challenges in Implementation of the ANISA Protocol at the Matiari Site, Pakistan
Sheraz Ahmed, MSPH,* Shabina Ariff, FCPS,* Sajid Bashir Soofi, FCPS,* Amjad Hussain, MA,* Aneeta Hotwani, MSc,* Muhammad Yaqoob, MSc,* Shahida M. Qureshi, MSc,* Imran Ahmed, MSc,*
Mohammad Shahidul Islam, MSc,† Samir K. Saha, PhD,† and Zulfiqar A. Bhutta, PhD*
Accepted for publication January 10, 2016.From *The Aga Khan University, Karachi, Pakistan; and †Child Health Research
Foundation, Dhaka, Bangladesh.This publication was supported by a subagreement from the Child Health
Research Foundation with funds provided from the Bill & Melinda Gates Foundation (Grant No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Sajid Bashir Soofi, FCPS, Department of Paedi-atrics and Child Health, The Aga Khan University, Stadium Road, Karachi 74800, Pakistan. E-mail: [email protected].

Ahmed et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S66 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
minimum of 14 years of education and with experience of working in the community. The team leader is responsible for supervision of surveillance activities and counseling of caregivers who refuse to provide clinical specimens from selected young infants.
The CHWs have a minimum of 12 years of education, are residents of the study area and are fluent in Sindhi, the local lan-guage. They are responsible for registration of pregnant women and follow-up until birth, 10 subsequent postnatal visits to registered newborns, newborn screening for pSBI and referral of cases to study physicians. The study physicians are registered practition-ers with at least 1 year of clinical experience. They are responsible for confirmation of clinical signs of pSBI, enrollment of cases and collection of clinical specimens from confirmed pSBI cases. Our phlebotomists are proficient in drawing blood from young infants in hospital settings and have been successfully collecting blood in the field. The 2 field supervisors are responsible for ensuring data quality and supervision of overall surveillance activities. The pro-ject workflow at Matari site is detailed in Figure 2.
The ANISA study coordination team trained 2 master train-ers for CHWs and 2 for study physicians from each ANISA site. These master trainers trained the CHWs and team leaders of the Matiari site through a 12-day workshop. The training focused on communication skills, antenatal and newborn care, identifying signs of pSBI in young infants, clinical assessment of newborns and
understanding the data capture forms. The World Health Organi-zation’s Integrated Management of Childhood Illness curriculum,9 role-plays and video aids were used for explaining different study activities to the CHWs. Refresher training is conducted every 2 months to reinforce proper and timely text message notification of newborn registration and control enrollment. A senior anthropolo-gist from The Aga Khan University (AKU), Pakistan, conducted a 1-day training course for study physicians on communication and counseling in the consent process. We also conducted a 3-day train-ing course for the physicians on study protocol and surveillance activities, and they received quarterly refresher training from AKU faculty. The phlebotomists are trained on collection and storage of blood and NP-OP specimens every 2 months.
ETHICS CLEARANCEEthical approval was obtained from World Health Organiza-
tion, and site-specific approval has been obtained from the AKU Ethical Review Committee in 2011 and in subsequent years.
CHALLENGES IN THE IMPLEMENTATION OF THE ANISA PROTOCOL AND REMEDIAL ACTIONS
Field ActivitiesLow Rate of Newborn Registration Within 24 hours of Birth
During the pilot phase, the rate of newborn registration within 24 hours of birth was low (17%) in Matiari. To facilitate early identification of pregnancy outcomes, ANISA’s Technical Advisory Group revised the target to at least 80% newborn regis-tration within 24 hours of birth.
In response, the Matiari site team made adjustments to its field teams and reallocated 32 CHWs along with 8 vehicles to birth registration activities. Additional staff were hired after the approval of a supplementary budget. These adjustments made additional human resources available for birth registration. To further improve the early birth registration rate, MWRA surveillance teams also provide information on pregnancy outcomes (Fig. 3).
At the Matiari site, about 65% of births take place at health care facilities, and approximately one third of these facilities are situated outside the study area. About 30%–40% of pregnant women in the study area travel to these facilities for delivery and
FIGURE 1. Geographical location of the rural study site Matiari, Pakistan.
PRIN
CIP
AL
IN
VE
STIG
AT
OR
Co-investigators
Study coordinator
Married women surveillance 10 teams in 10 UCs
4 data collectors and one team
leader
Young infant surveillance 30 teams in 10 UCs 4 CHWs and one
team leader
PSBI enrollment 10 teams in 10 UCs Study physician and phlebotomist
Verbal autopsy 2 teams for Halaand Matiari
2 research assistants and 2 male facilitators
Monitoring teams 8 monitors 4 female and 4 male monitors
Mobile birth registration team
2 teams for Halaand Matiari
One CHW and one team leader
Data manager Data management unit supervisor Data coordinator Data entry
operators
Research laboratory manager Field lab in-charge Lab technicians
and assistants2 lab technicians
2 lab assistantsFIGURE 2. Project workflow diagram at the Matiari site.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Matiari, Pakistan
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S67
newborn care. It is not feasible for the birth registration teams to visit newborns both within and outside the study area. To overcome this problem, 2 mobile birth registration teams were formed and tasked with registering births that took place at health facilities outside the study area. Simultaneously, staff at the facilities were requested to notify the project office of every live birth as soon as possible through mobile phones.
Liaison between study staff and families of pregnant women, LHWs and traditional birth attendants (TBAs) is well established, and 2 staff members are stationed at the study office to receive their birth notification calls. In addition, LHWs, TBAs and the families of pregnant women receive prepaid phone cards worth 100 Pakistani Rupees (~US$ 1.00) for every birth notification. In areas where LHWs or TBAs are not available, residents of the vil-lages with access to mobile phones are requested to notify study
staff of births, and the cost of calling is reimbursed. The prepaid phone card is also used by parents to inform the study staff of any illness among enrolled young infants. Office staff, in turn, relay information to the mobile surveillance team to organize a home visit. Study staff also make calls to pregnant women and inquire about pregnancy outcomes. Of 13,753 calls received so far, 71% were made by parents, 11% by TBAs and 8% by LHWs. Improving early birth registration has a positive impact on early enrollment of pSBI cases and facilitates tracking of the incidence of illness among young infants. We also have instituted mandatory documen-tation of reasons for failure (approximately 25%–30%) to register newborns within 24 hours of birth, which has led to accountability and improved performance of study teams (Fig. 4A).
One challenge that remains is the limited working hours for field staff, from 9:00 am to 5:00 pm. Field travel after sunset is not advisable because of security concerns. Cultural barriers in rural areas, such as unwillingness to remain outdoors after sunset, also serve as major obstacles in extending working hours. Therefore, teams are unable to capture infants born after working hours until the next morning.
About 12%–14% of births can be missed due to holidays. To overcome this problem, 8 birth registration teams work on holi-days, resulting in a 10% increase in birth registration. The Matiari site team has managed to register 62% of births within 24 hours (Fig. 4B) against the targeted 80%.
Blood and NP-OP Specimen Collection From Enrolled pSBI Cases
CHWs screen the young infants on each of the 10 follow-up visits for signs of pSBI.1 If a CHW detects any one of the signs, she refers the infant to study physicians. The study physician validates the identified case and refers the infant to the nearest health care facility for treatment as soon as possible. In cases where the fam-ily is unable to reach the health facility due to lack of transport, the study team assists. Before referral to a health care facility, a study physician collects respiratory specimens and a phlebotomist collects blood from the young infant. One of the difficulties faced in collection of specimens is refusal to provide consent. In these cases, the study physicians visit the families for counseling to over-come refusal. Despite the challenges, of 1857 enrolled pSBI cases, blood specimens have been collected for 1499 (81%) and NP-OP specimens for 1604 (86%).
Second Blood Culture CollectionTo interpret blood culture outcomes, we collect a second
blood specimen from enrolled pSBI cases whose condition does not improve or deteriorates by the time their blood culture bottles
Pregnant women follow ups in last
trimester and around EDD by
CHWs
Pregnancy outcome tracking
system
Liaison with TBAs / LHWs /key informants
in study area
Bi-monthly HH surveillance through
data collectors Information from hospital-based
informants
Families encouraged to contact through mobile phone for birth notification within 24 hours
FIGURE 3. Pregnancy outcome tracking system at the Matiari site. EDD indicates expected date of delivery; HH, household.
0
200
400
600
800
1000
1200
Num
ber
of L
ive
Bir
ths
(n)
Total live births 0-6 days births < 6 hours< 12 hours < 24 hours
0
20
40
60
80
100
Ear
ly b
irth
reg
istr
atio
n ra
te (
%)
0-6 days births
< 6 hours
< 12 hours
< 24 hours
FIGURE 4. A, Timing of live birth registrations in pilot and main study phases, August 2011 to December 2013. B, Timing of live birth registrations in pilot and main study phases as a percentage of all birth registrations, August 2011 to October 2013.

Ahmed et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S68 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
indicate bacterial growth. In these cases, CHWs make additional household visits to reassess the young infants. Upon confirma-tion by the CHW and study physician, the phlebotomists collect a second blood specimen. In cases where blood has been drawn recently and the newborn is still unwell, significant time and effort are required to counsel caregivers regarding the need for a second blood specimen.
Healthy Control Specimen CollectionTo understand the normal flora of young infants, potential
healthy controls are selected using the ANISA database software.3 A newborn can be selected as a healthy control on any of the 10 postnatal follow-up visits. On the day of healthy control selec-tion, if the selected newborn does not manifest any sign or symptom of pSBI, blood and respiratory specimens are collected. Obtaining caregiver consent for collection of specimens from healthy young infants, especially on day 0, is problematic. To overcome this chal-lenge, CHWs initiate counseling and sensitizing of caregivers from the day of newborn registration, followed by study physician coun-seling. Because of this approach and liaison with the community, only 11% of the 800 potential healthy controls have refused to pro-vide specimens (Fig. 5).
Blood Culture Collection TechniqueThe Matiari site does not have a fixed specimen collec-
tion point where procedures can be performed under optimal aseptic conditions. Collection of blood and NP-OP specimens in a home setting makes it challenging to achieve the project’s target of a contamination rate of less than 5%. This rate was 8% in the pilot phase, and several interventions were introduced to reduce it. Clean plastic sheets are placed under an infant during collection. Hand sanitizers are provided to study physicians and phlebotomists because water for hand washing is not available at most households. Phlebotomists also wear disposable gloves dur-ing specimen collection. Because of the dusty environment, all laboratory consumables are kept in resealable plastic bags. The skin of a newborn is thoroughly cleaned with antiseptic swabs before blood collection. We initially used povidone-iodine and later replaced it with 4% chlorhexidine spray to ease cleansing of the puncture site. Cleaning of the puncture site with alcohol followed by 4% chlorhexidine spray and again with alcohol is enforced if a vein is palpated again. A checklist for blood collec-tion technique is available for the study physicians to ensure the completeness of all steps performed by the phlebotomists. After the implementation of abovementioned measures, the contamina-tion rate decreased to 4% (Fig. 6).
Interruptions in Electricity Supply of Field LaboratoryEnsuring uninterrupted power supply to the BACTEC
(Becton Dickinson Diagnostic Instrument Systems, Sparks, MD), blood culture machine is challenging in Matiari as this area suffers from frequent power outages. Interruptions in power supply may result in beep-positive culture-negative (BPCN) blood specimens. BPCN is a false alarm for the possible pres-ence of organisms in the blood culture bottle. A heavy-duty diesel generator and voltage stabilizers have been installed at the site laboratory to maintain an uninterrupted power supply to the BACTEC machine. Despite these efforts, the BPCN rate has remained at 4%.
Laboratory ActivitiesPathogen Isolation
During the initial period of the study, pathogen isolation from blood culture was lower than the expected 5%. Insufficient blood volume and prior antibiotic administration in 25% of cases are considered possible reasons for this low yield of pathogens. Therefore, phlebotomists are encouraged to collect the maximum recommended volume of blood (3 mL). Separate mobile medical teams are tasked with collecting blood from pSBI cases on public holidays. However, the pathogen isolation rate remains low at 2%, although it has improved from 1% in the initial 8 months of the study period.
Specimen and Reagent TransportBlood culture bottles, NP-OP specimens and blood in eth-
ylenediaminetetraacetic acid (EDTA) tubes must be transported from the field site to the field laboratory within 2 hours of collec-tion. There is a dedicated vehicle for this purpose. Average speci-men transportation time from collection site to laboratory is 1 hour and 48 minutes. Blood culture bottles are transported at 25–28°C and NP-OP and EDTA tubes at 2–8°C in coolers. A thermometer is placed in the cooler, and phlebotomists monitor the temperature during transportation. If the temperature rises above the specified levels, phlebotomists add more ice packs to bring it down. The temperature inside the cooler is also recorded by personnel at the time of arrival at the field laboratory. Blood culture bottles are put inside the BACTEC machine, whereas EDTA and NP-OP speci-mens are transported daily to the Infectious Diseases Research Laboratory at AKU in Karachi.
40
60
80
100
Cco
ntro
l spe
cim
en c
olle
ctio
n ra
te (
%)
Blood specimen NP-OP specimen
FIGURE 5. Blood and NP-OP specimen collection rate from selected healthy controls, February 2012 to December 2013.
0
5
10
15
20
25
Con
tam
inat
ion
Rat
e (%
of
tota
l blo
od c
ultu
re)
P
C V
CL
PP
P= Phlebotomists training CL= Procedure observation checklist C= introduction of chlorhexidine spray in replacement of pyodine V= video recording of procedure with feedback during training.
FIGURE 6. The impact of interventions in the rate of blood culture contamination in Matiari, Pakistan (August 2011 to December 2013).

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Matiari, Pakistan
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S69
SUMMARY AND CONCLUSIONANISA protocol implementation in a large cohort under
surveillance in a rural setting with specimen collection and new-born assessment occurring at household level has offered a novel experience to the Matiari site team.
The success of the ANISA protocol implementation has been largely due to cohesive team work and able leadership. Some of the strategies implemented include creation and sustenance of community liaison, comprehensive training, focused tasks for each field staff member, extensive supervision and monitoring of field activities. The interventions adopted to reduce blood culture con-tamination in the community offer opportunities for replication in settings where the contamination rate is high.
One of the challenges that we have not been able to over-come entirely is the late registration of newborns, predominantly due to accessibility and time. More young infants could be saved if we adopted the model of village-based female volunteers who can reach newborns soon after birth and promptly treat or refer them in case of illness.
ACKNOWLEDGMENTSThis study would not be a success without the commitment
and dedication of the field and laboratory staff and the sustained cooperation of the study community. The authors thank the ANISA study coordination team at the Child Health Research Founda-tion, Dhaka, for their support, especially Mr. Nicholas Connor. They are also indebted to Dr. Shamim Qazi and Dr. Salim Sad-druddin for their invaluable suggestions given during monitoring
visits. Special thanks go to the administrative support and data management staff from AKU.
REFERENCES 1. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a
multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
2. Saha SK, Islam MS, Qureshi SM, et al. Laboratory methods for determining etiology of neonatal infection at population-based sites in South Asia: the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S16–S22.
3. Islam MS, Rahman QS, Hossain T, et al. Using text messages for critical real-time data capture in the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S35–S38.
4. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35 (Suppl 1):S39–S44.
5. Bhutta ZA, Memon ZA, Soofi S, et al. Implementing community-based perinatal care: results from a pilot study in rural Pakistan. Bull World Health Organ. 2008;86:452–459.
6. Bhutta ZA, Soofi S, Cousens S, et al. Improvement of perinatal and new-born care in rural Pakistan through community-based strategies: a cluster-randomised effectiveness trial. Lancet. 2011;377:403–412.
7. Soofi S, Ahmed S, Fox MP, et al. Effectiveness of community case man-agement of severe pneumonia with oral amoxicillin in children aged 2-59 months in Matiari district, rural Pakistan: a cluster-randomised controlled trial. Lancet. 2012;379:729–737.
8. Soofi S, Cousens S, Iqbal SP, et al. Effect of provision of daily zinc and iron with several micronutrients on growth and morbidity among young children in Pakistan: a cluster-randomised trial. Lancet. 2013;382:29–40.
9. World Health Organization, UNICEF. Integrated Management of Childhood Illness (IMCI) Chart Booklet. Geneva: World Health Organization; 2008.

S70 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
Supplement
Background: The Aetiology of Neonatal Infection in South Asia (ANISA) study aims to determine the population-based incidence, etiology, risk fac-tors and antibiotic resistance profiles of community-acquired young infant infections in Bangladesh, India and Pakistan using community-based sur-veillance and standard newer diagnostic tests. The data generated will help plan preventive and treatment strategies to reduce neonatal and infant mor-tality in this region. The aim of this article is to describe the site-specific characteristics, challenges and solutions in implementing the ANISA proto-col at the Vellore site, India.Challenges: Vellore joined the ANISA study 2 years after the sites in Bang-ladesh and Pakistan, and some challenges relate to the need for rapid imple-mentation. The Vellore site differs primarily in the high rate of institutional deliveries, actively promoted by the Government of India’s conditional cash transfer program. The Vellore site hospitals are regular care providers for the study population, which leads to very high rates of consent for enroll-ment and collection of samples. Keeping blood culture contamination rates low was a challenge the site team overcame by adhering strictly to the pro-tocol. Issues related to incorporation of a large study into a busy clinical services laboratory were overcome by meticulously setting up algorithms related to receipt, processing and storage of samples.Conclusion: ANISA is a complex study, but the challenges in implementa-tion have been largely resolved and documented.
Key Words: Vellore, neonatal, infections, ANISA, pSBI, surveillance
(Pediatr Infect Dis J 2016;35:S70–S73)
Neonatal infections, including sepsis, pneumonia and men-ingitis (hereafter referred to as “infections”) account for an
estimated 700,000 neonatal deaths worldwide every year.1,2 About 60% of these deaths occur in the first week of life,3 leaving a narrow window of opportunity to intervene. The risk of death in the second month of life is also high, and a vast majority of these deaths occur in low-resource settings in Asia and Africa.4 Three South Asian countries—Bangladesh, India and Pakistan—account for more than one third of all global neonatal deaths. The majority of births and deaths in these countries occur at home.5
The etiology of more than 90% of suspected young infant (0–59 days) infections remains unknown. A substantial proportion
may be due to bacteria or viruses that are currently unrecognized as causes. Despite the large burden of neonatal deaths in the commu-nity attributable to infections, almost no data exist on the etiology of community-acquired infant infections6,7 or on geographic varia-tions in etiology.5,8 Substantial gaps in knowledge remain about risk factors associated with community-acquired infections in young infants in resource-poor settings.
The Aetiology of Neonatal Infection in South Asia (ANISA) study aims to determine the population-based inci-dence, etiology, risk factors and antibiotic resistance profiles of community-acquired young infant infections in Bangladesh, India and Pakistan using community-based surveillance and standard and new diagnostic tests. An improved understanding of risk fac-tors in the ANISA surveillance sites will highlight potential routes for primary prevention of serious infections, as well as enable the development of interventions targeting identifiable subgroups of infants at the highest risk of disease. The ANISA study’s meth-ods for surveillance, enrollment of newborns and sample collec-tion are detailed elsewhere.9,10 The main aims of this article are to describe challenges to implementing the ANISA protocol in the Vellore, India, site and the solutions the site team developed to overcome them.
Study Site and PopulationVellore District is located in Tamil Nadu, an Indian state
with a highly functional health care delivery system where more than 90% of deliveries occur in a health facility (Table 1). The Vel-lore site differs from other ANISA sites primarily in this high rate of facility births, largely due to mothers benefiting from the Gov-ernment of India’s conditional cash transfer program.
The infant mortality rate in the state is 24 per 1000 live births,11 and the neonatal mortality rate is 16 per 1000 live births.12 In Kaniyambadi block, the study area, the population falls mostly in the middle-income group (47%), with 27% and 26% belonging to low- and high-income groups, respectively. About 45% of the population is engaged in agriculture.
The 2 subsites in Vellore are based at the Community Heath and Development (CHAD) hospital and the Rural Unit for Health and Social Affairs (RUHSA; Fig. 1). Both hospitals are units of the Chris-tian Medical College (CMC), Vellore. CHAD hospital is a secondary level facility with 140 beds, situated at the edge of Vellore town; the rural block under surveillance, Kaniyambadi, abuts it. This hospital also serves Vellore town urban slums, and thus this subsite includes a popu-lation from both periurban and urban areas. About 3000 births occur annually in this hospital, which has a pediatric ward and 16 second-ary care neonatal beds. RUHSA hospital is located 25 km from Vellore town. Around 1200 deliveries occur per year at RUHSA hospital, which features a dedicated ward for pediatric patients.
The ANISA surveillance population in Vellore consists of all married women of reproductive age (13–49) and all live-born infants delivered in the Kaniyambadi block (population 111 676) and the K.V. Kuppam block (population 137 000). Both subsites have a defined area with a complete census of the study population and some form of ongoing maternal and young infant surveillance.
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S70DOI: 10.1097/INF.0000000000001111
Challenges in Implementation of ANISA Protocol at the Vellore Site, India
Anuradha Bose, MD, Rita Isaac, MD, Veeraraghavan Balaji, MD, Winsley Rose, MD, Venkataraghava Mohan, MD, Shalini Anandan, MD, Jasmin Helan Prasad, MD, Asha Abraham, MD, Manjunath Krishna,
and Kumaran Viswanathan, MD
Accepted for publication January 10, 2016. From the Christian Medical College, Vellore, India.The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant
No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Anuradha Bose, MD, Professor of Paediatrics, Christian Medical College, Bagayam, Vellore 632002, India. E-mail: [email protected].

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Vellore, India
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S71
The CHAD area is mapped by a geographic information system, which may be useful when looking at mortality data.
CHAD and RUHSA hospitals are the regular health care pro-viders for this population. Around 99% of the parents approached agreed to participate in the study, including permitting samples to be taken and treatment to be administered. Infants are observed and examined daily while in hospital, by the clinical team and by the ANISA study physician.
Unlike the ANISA sites in Bangladesh and Pakistan, the Tamil Nadu Government provides a direct cash transfer of 12,000 Indian Rupees (INR) (~US$200) to mothers to encourage delivery in a hospital. Thus in Vellore, most newborns enrolled in ANISA are born in hospitals. Since the Vellore site hospitals are regular care providers for the study population, rates for enrollment, refer-ral, treatment and specimen collection are high.
The senior investigators at the Vellore site have experience relevant to a study as large and complex as ANISA. They have been principal investigators of similar large projects, where 3000–5000 newborns have been enrolled and followed up for 2 years. The investigators are affiliated with the Department of Commu-nity Health at CMC Vellore. The Department played a significant role in the recent introduction of the Hemophilus influenza type
B and rotavirus vaccines into the Indian national immunization schedule.13 The Department of Microbiology at CMC Vellore is a regional World Health Organization (WHO) reference laboratory for pneumococcus.
The Vellore site initially joined ANISA in March 2013 and was integrated into the main study after a 1-month pilot phase. Specimen collection and transfer to the laboratories had not been piloted because of time constraints, and this subsequently was the source of some difficulties. The first enrollment was on July 10, 2013. Enrollment continued until December 31, 2014 and follow-up was completed by February 28, 2015.
The field team was comprised of 36 community health workers (CHWs) and 5 supervisors. Each CHW covers a popula-tion of roughly 8000, and each supervisor is directly responsible for 7 or 8 CHWs. The team has a prepaid Closed User Group mobile communication system and members can phone each other at no charge at any time, facilitating smooth functioning of the system and pre-empting the challenge of poor communication.
Centralized training for the investigators was conducted in Dhaka in April 2013. Following recruitment, CHWs and supervi-sors from both Vellore subsites were trained together locally. The 15-day training was conducted by the principal investigator, the physicians and the study coordinator. The challenge of teaching workers with a high school education and helping them understand the significance of the data that would be collected was overcome with the help of a centralized training manual provided by the ANISA coordination team in Dhaka. Sessions were taught with the help of role-plays, videos and tests. CHWs and supervisors were shown how to estimate the date of delivery for pregnancies and to identify possible serious bacterial infection (pSBI) using the WHO Integrated Management of Childhood Illness guidelines. The importance of effective and appropriate communication was stressed and taught using audiovisual aids and role-plays. Training in the use of text messages was also conducted.
TABLE 1. Health Indicators for India and Tamil Nadu State11
Indicator India Tamil Nadu
Neonatal mortality rate/1000 live births (2010) 33 16Infant mortality rate (2009) 49 24<5 mortality rate/1000 live births 52 30Contraceptive use rate (%) (2006) 56 61Total fertility rate (2006) 1.7 1.8Facility delivery rate (%) 38 78
FIGURE 1. Map of India highlighting Tamil Nadu State and Vellore district.

Bose et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S72 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
As communication with mothers was anticipated to be a challenge, each pregnant woman is given INR100 (~US$1.50) per month for the last 2 months of her pregnancy to recharge her mobile phone to be able to call the local CHW when she goes into labor or has any health emergency. The communication between the CHW and the pregnant woman is strengthened by scheduled phone calls made by the CHWs. These calls occur approximately once per month in the early stages of pregnancy and increase to once per week from the 36th week of gestation and to once per day in the week before the expected date of delivery.
Newborns are screened while in hospital and again at home based on the standard ANISA protocol. CHWs identify young infants up to 59 days old with pSBI using the young infant WHO Integrated Management of Childhood Illness criteria.
Ethics ClearanceThe Institutional Review Board for Research and Ethics of
CMC Vellore approved the ANISA study protocol. All enrolled pregnant women provide consent for their participation and that of their newborn. A detailed process is undertaken to ensure that par-ticipating women understand the nature of the home-based infant surveillance that will begin shortly after newborn delivery. Written informed consent follows in all cases, as well as further consent from the parents of young infants who are enrolled either as cases or controls.
CHALLENGES IN THE ADOPTION OF THE ANISA PROTOCOL AND REMEDIAL ACTIONS
Field ActivitiesEnrolling Pregnant Women and Newborns
The team faced several challenges in the enrollment of pregnant women. The families were not always cooperative and appeared to resent the time required to complete forms and receive repeated visits to establish rapport. Around 25% of young mothers in the study area move to their parents’ homes for delivery, mean-ing that CHWs have to identify 2 addresses for surveillance. To overcome this challenge, supervisors hold weekly meetings and encourage the CHWs to pursue enrollment. On account of intense heat during the summer, working hours are set as 6:00 to 10:00 AM and 3:00 to 6:00 PM.
As in all ANISA sites, the Vellore site aims to enroll at least 50% of newborns within 6 hours of birth. Although the site reg-isters 60% of births within this time, families often forget to call CHWs to inform them of births. The team, therefore, worked out a schedule for CHWs to call mothers to enquire about the status of their pregnancies. Too many phone calls could annoy the family, so finding the right balance in the timing and frequency of calls is critical. There were weekly calls after enrollment of the pregnant woman, and daily calls in the last week of the pregnancy, if it pro-ceeded to term. Births in the study hospital were identified by a daily review of newborns by the study nurses.
Despite providing financial assistance to recharge mobile phones in the last 2 months of the pregnancy, the CHWs are not always informed immediately of births. Early birth notification continues to be a challenge, especially in the event of premature delivery.
Births also take place on holidays and weekends, which means that CHWs have no protected days off, an ongoing chal-lenge. Since fixed days off could lead to missed enrollments, we provided the equivalent of 30 days’ additional wages annually, equal to one day off per week, for the CHWs and supervisors. This was done at the end of 1 year and pro rata for the remaining 6 months of enrollment.
Referral Compliance and Specimen CollectionIf a young infant is not doing well, some persuasion may
be required to ensure successful hospital referral for assessment and specimen collection. In the event of an adverse outcome of an illness, the family may blame the CHW. As the state government’s permission is required for collection of clinical specimens from neonates born in a government-run health center, these centers cannot collect clinical specimens for ANISA.
Laboratory ActivitiesThe microbiology laboratory at CMC Vellore is large in
terms of size and patient load, which makes strict adherence to the study protocol difficult. We established a separate protected area in the laboratory for ANISA activities. The team faced challenges related to incorporation of a large study into a busy clinical ser-vices laboratory, due mostly to logistics and different versions of computer software. We overcame these challenges by meticulously setting up algorithms related to receipt, processing and storage of samples.
Contamination of Blood CulturesBlood culture contamination was an issue at the outset.
Collecting blood from young infants while maintaining an aseptic environment requires great skill. Improvement was observed after retraining the nurses, ensuring that only 2 or 3 designated staff members performed all the specimen collection (Fig. 2). Special and dedicated blood culture sets are prepared for every specimen collection procedure, consisting of sterile containers, drapes and instruments. The contamination rate decreased to less than 5%, down from 10%.
Data ManagementThe Vellore site systematized the data entry process to
minimize lag time between data collection and data entry. CHWs submit checked and corrected data collection forms to their super-visors every day. The corrected forms are submitted weekly, result-ing in a 1- to 2-week lag in data entry. Three operators carry out entry (including different operators entering data a second time) and data checks. On average, 100 forms are entered every day. The specimens are scanned using a barcode scanner, and the forms are entered twice in the laboratory.14
Errors in Data Collection Forms or Data EntryIn case of any data entry error or inconsistency, mismatch
or missing data, the forms are checked by the data manager in the presence of the supervisor and CHW and corrections made. Every
0
5
10
15
20
25
Blo
od c
ultu
re c
onta
min
atio
n ra
te (
%)
Intervention activitiesP- Phlebotomist training W- Handwashing training
P
P
P W
P
FIGURE 2. Rate of blood specimen contamination at the Vellore site.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Vellore, India
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S73
week before data are uploaded to the central database (in Dhaka), entry errors are checked by comparing the 2 sets of data entered by different operators.
Some items on the data collection form cannot be entered into the database as there was no provision to account for the slight differences in the forms at the Vellore site. The resolution of these differences helped overcome a delay in entering the forms, as all items need to be completed on the form before the system permits data entry to proceed.
Text Messaging and Selection of ControlsThe text messaging and synchronization programs are
installed in the same system at CHAD, which runs 24 hours a day. A mobile subscriber information module and a general packet radio service modem are used. On average, 25–30 text messages are received and sent per day.
Data Upload, Security and BackupProtecting data is a priority. Every Thursday, the data man-
ager uploads field and laboratory data to the central server in Dhaka. A screenshot of the upload status is saved for the site’s reference. The data entry system and the database are password-protected. A daily backup of the database is maintained. Data are also backed up weekly in a Dropbox folder (Dropbox Inc., San Francisco, CA), which is shared with the principal investigator, coprincipal investi-gators and data manager. A backup of monthly data is copied onto compact disks/DVDs and kept in a separate place for data security.
SUMMARY AND CONCLUSIONAbout 3900 newborns have been identified and enrolled at
the Vellore site. Sixty percent of all live-born infants in the catch-ment population received a first postnatal visit within 6 hours of birth and 80% within 24 hours of birth. Nine percent of young infants have been enrolled as pSBI cases during their first 59 days of life, and laboratory tests have been conducted for about 99% of them. Blood cultures were performed before the start of antibiotics. The average hospital stay is 24 hours after a vaginal delivery and 5 days after a caesarean section.
The process of identifying and overcoming challenges has been useful, as documented in this article. The ANISA study addresses an important issue, and a successful outcome will likely benefit large numbers of young infants in the country.
ACKNOWLEDGMENTSWe gratefully acknowledge the study participants and their
parents. We thank the study and data coordinators, Ms. Ranjitha,
Ms. Shanthala and Ms. Hannah, who had an excellent relationship with the team and kept morale high. We thank also the other staff at the study sites, including the doctors, nurses and support staff. We appreciate the support provided by the Head of the Department of Community Health, and the support of the medical practitioners in the area for their referrals. We acknowledge the contribution of Ms. Meghan Scott in the editing of the article.
REFERENCES 1. Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? where?
why? Lancet. 2005;365:891–900.
2. Baqui AH, Arifeen SE, Darmstadt GL, et al. Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: a cluster-randomized con-trolled trial. Lancet. 2008;371:1936–1944.
3. Baqui AH, Darmstadt GL, Williams EK, et al. Rates, timing and causes of neonatal deaths in rural India: implications for neonatal health programmes. Bull World Health Organ. 2006;84:706–713.
4. Qazi SA, Stoll BJ. Neonatal sepsis: a major global public health challenge. Pediatr Infect Dis J. 2009;28(1 Suppl):S1–S2.
5. Zaidi AK, Thaver D, Ali SA, et al. Pathogens associated with sepsis in newborns and young infants in developing countries. Pediatr Infect Dis J. 2009;28(1 Suppl):S10–S18.
6. Newton O, English M. Young infant sepsis: aetiology, antibiotic suscepti-bility and clinical signs. Trans R Soc Trop Med Hyg. 2007;101:959–966.
7. Darmstadt GL, Batra M, Zaidi AK. Oral antibiotics in the management of serious neonatal bacterial infections in developing country communities. Pediatr Infect Dis J. 2009;28(1 Suppl):S31–S36.
8. Vergnano S, Sharland M, Kazembe P, et al. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2005;90:F220–F224.
9. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
10. Saha SK, Islam MS, Qureshi SM, et al. Laboratory methods for determining etiology of neonatal infection at population-based sites in South Asia: the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S16–S22.
11. Ministry of Health and Family Welfare, Government of India. State Wise Information, Tamilnadu [National Health Mission web site]. Available at: http://nrhm.gov.in/nrhm-in-state/state-wise-information/tamil-nadu.html. Accessed July 14, 2014.
12. Ministry of Health and Family Welfare, Government of India. Approval of State Programme Implementation Plan 2012–13: Tamilnadu. [National Rural Health Mission website]. May, 2012. Available at: http://www.nrhmtn.gov.in/ropPDF/NPCC-12-13.pdf. Accessed July 4, 2014.
13. Gupta M, Kumar R, Deb AK, et al. Multi-center surveillance for pneumonia & meningitis among children (<2 yr.) for Hib vaccine probe trial preparation in India. Indian J Med Res. 2010;131:649–658.
14. Rahman QS, Islam MS, Hossain B, et al. Centralized data management in a multicountry, multisite population-based study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S23–S28.

S74 | www.pidj.com The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
Supplement
Background: The Aetiology of Neonatal Infection in South Asia (ANISA) study is being carried out at 5 sites across Bangladesh, India and Pakistan, generating in-depth information on etiologic agents in the community setting. Pregnancies are identified, births are registered and young infants are followed up to 59 days old with regular assessments for possible serious bacterial infec-tion following a generic protocol. Specimens are collected from suspected cases. This article describes the challenges in implementing the generic ANISA protocol and modifications made to accommodate the Odisha site, India.Challenges: Primary challenges in implementing the protocol are the large geographic area, with a population of over 350,000, to be covered; assessing young infants at home and arranging timely transport of sick young infants to study hospitals for physician confirmation of illness; and specimen col-lection and treatment. A large workforce is deployed in a 3-tier system in the field, while clinical, microbiology, laboratory and data management teams collaborate dynamically. Mobile phones with text message capability, inte-gration with the Odisha State government’s health system, involvement of local communities and strict monitoring at different levels have been critical in addressing these challenges.Conclusion: This article describes the challenges and modalities adopted to collect complex and accurate data on etiology, timing of disease and associated factors for community-acquired neonatal infections. Attention to local culture and customs, training and employing community level workers and supervisors, involving existing government machinery, using technol-ogy (cell phones), and uninterrupted systematic monitoring are critical for implementing such complex protocols that aim to collect population-based data to drive policy.
Key Words: neonatal, surveillance, pSBI, etiology, ANISA, Odisha, Rour-kela, Bhubaneswar
(Pediatr Infect Dis J 2016;35:S74–S78)
The Aetiology of Neonatal Infection in South Asia (ANISA) study aims to identify the incidence, timing, etiologic agents,
antibiotic resistance and risk factors for neonatal infections. The first phase of the study involves establishment of community-based pregnancy, birth and neonatal surveillance for identifying cases of possible serious bacterial infection (pSBI) in the 0–59 day age group and collecting specimens for etiologic evaluation using blood culture and state-of-the-art molecular techniques. Crucially, controls are also enrolled to identify natural colonizers that do not produce disease.1,2
The Odisha state site research hubs are located in Rourkela and Bhubaneswar in eastern India, areas that continue to record very high infant and neonatal mortality.3 The 2 sites were chosen to participate in ANISA because of their diversity, including coastal, rural, tribal, mining and periurban areas, as well as neonatal disease prevalence. The site investigators have previous experience con-ducting large-scale community and hospital-based surveillance and intervention studies among neonates.4–8 Established rapport with the state government health systems and availability of a trained workforce in the community, along with facilities for data manage-ment, microbiological analyses and long-term storage of biological specimens, were considered major strengths of the site. This article outlines the diverse nature of the communities and the associated operational, socio-cultural and scientific challenges faced while implementing the ANISA protocol at Rourkela and Bhubaneswar in Odisha.
STUDY SITES AND POPULATIONThe state of Odisha, home to 3.4% of India’s population,
records the second-highest infant mortality rate (62/1000 live births) among the 29 states and 11 union territories in the country.3 Odisha is divided into 30 districts and each district is divided into blocks, with a population of approximately 100,000 in each block. Odisha’s population density is 265/km2, and its birth rate is 20/1000 popula-tion.9 The 2 study hubs are located in the major cities of Rourkela, in Sundargarh District, and Bhubaneswar, in Khordha District, where the neonatal mortality rates are 39 and 46/1000 live births, respec-tively (Fig. 1 and Table 1).9 These 2 areas are about 500 km apart, and their inhabitants are diverse in ethnic, socio-cultural, envi-ronmental, occupational and economic characteristics. The study area in Rourkela covers about 480 km2 and in Bhubaneswar 161 km2. The 105 study units in the Rourkela site have a total popu-lation of 204,000, and the 75 study units at the Bhubaneswar site have a population of 156,000. These units comprise 3 to 7 villages with populations of 600–1200 each. At the time of study initiation, there were 36,718 and 25,677 married women of reproductive age (13–49 years) in Rourkela and Bhubaneswar, respectively, for a total of 62,395 women eligible for enrollment in ANISA.
Villages around the Rourkela site are spread over hilly and mining areas of Lathikata and Kuarmunda Blocks, with indige-nous tribes predominating in the population. Many small villages are dispersed in the study area, with the population living a tra-ditional lifestyle with minimal outside interaction. The villagers earn their livelihood from forestry, rearing animals and raising
Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution-Non Commercial License 4.0 (CCBY-NC), where it is permis-sible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially.
ISSN: 0891-3668/16/3505-0S74DOI: 10.1097/INF.0000000000001112
Challenges in Implementation of the ANISA Protocol at the Odisha Site in India
Radhanath Satpathy, MD,* Pritish Nanda, MPH,* Nimai C. Nanda, MD,† Himadri B. Bal, PhD,* Ranjita Mohanty, BDS,* Archana Mishra, MSc,* Tapoja Swain, MSc,* Keshab C. Pradhan, MBA,*
Kalpana Panigrahi, PhD,‡ Ambarish Dutta, PhD,* Pravas R. Misra, MVSc,* Sailajanandan Parida, MD,§ and Pinaki Panigrahi, MD‡
Accepted for publication January 10, 2016. From the *Asian Institute of Public Health, Bhubaneswar, Odisha, India; †Ispat
General Hospital, Rourkela, Odisha, India; ‡Center for Global Health and Development, College of Public Health, University of Nebraska Medical Center, Omaha, Nebraska; and §Sri Ramachandra Bhanj Medical College, Cuttack, Odisha, India.
The ANISA study is funded by the Bill & Melinda Gates Foundation (Grant No. OPPGH5307). The authors have no other funding or conflicts of interest to disclose.
Address for correspondence: Pinaki Panigrahi, MD, PhD, Center for Global Health and Development, College of Public Health, University of Nebraska Medical Center, Omaha, Nebraska 68198. E-mail: [email protected].

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Odisha Site, India
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S75
arid crops. Some of those who live close to townships work for daily wages, and others have salaried employment in local coal and iron mines. In contrast, inhabitants of Balianata and Balipatana Blocks in Khordha District in the Bhubaneswar site depend on irrigated agriculture and work in government offices and small industries. They are relatively more affluent and live in densely populated villages that are close to each other. Apart from primary and community health centers, each site has one tertiary care municipal hospital that provides most health care for
free. Capital Hospital, a large multispecialty government facil-ity in the city of Bhubaneswar, and Ispat General Hospital, an Indian government undertaking with the steel industry in Rour-kela, serve as the research hubs for ANISA.
TRAINING AND RECRUITMENT OF PERSONNELAnganwadi (meaning “courtyard shelter”) Centers have
been functional for more than 4 decades in our study areas, pro-viding preschool mid-day meals, assessing nutritional status of children, and acting as a common place for health education, immunization, minor health check-ups and referral services. Female, high-school (or higher) educated Anganwadi workers are from the same or nearby villages and have been critical partners in the implementation of ANISA in Odisha, particularly in building rapport with families and birth registration. A new cadre of vil-lage-level workers, Accredited Social Health Activists (ASHAs), has been introduced in the area and they are also part of the exist-ing community health structure. The ASHAs and the Anganwadi workers were incorporated into the ANISA project design to help maintain regular surveillance and facilitate bringing pregnant women to facilities for delivery. Both the Anganwadi workers and ASHAs work in concert with our dedicated community health volunteers (CHVs).
FIGURE 1. Population-based study areas in the districts of Sundargarh and Khorda in Odisha state.
TABLE 1. Neonatal Health Indicators in India and in Odisha State
Indicator India Odisha
Neonatal mortality rate/1000 live births* 33 39Infant mortality rate/1000 live births* 47 59<5 mortality rate/1000 live births* 59 79Crude birth rate/1000 population* 21.6 19.8Current use of contraception (%)† 64.0 59.4Facility delivery rate (%)‡ 72.9 75.5
*Census of India, 2013.†National Fertility Health Survey 3 (2005–2006).‡Coverage Evaluation Survey 2009, UNICEF.

Satpathy et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S76 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
We follow a 3-tier reporting and monitoring system that we designed and have been using for the past 12 years. Considering the significant distance between the study units, an extra tier of block coordinators is utilized in Rourkela. Otherwise, each study site has 1 CHV, a woman from the same village. About 10 CHVs are super-vised by 1 area coordinator, who reports either through block coor-dinators (in Rourkela only) or directly to program managers. A sen-ior program officer is in charge of overall field operations (Fig. 2)
After receiving centralized training at the Child Health Research Foundation (CHRF) in Dhaka, senior clinicians, microbi-ologists and senior program officers trained 185 CHVs, 25 area coor-dinators, 6 block coordinators and 2 program managers on site. The training lasted 6 or 7 days and included common protocols, use of the ANISA text messaging system, and a 1-day clinical observation (newborn assessment, identification of pSBI cases admitted to hospi-tal and other neonatal ailments). Three months after study initiation, we conducted a retraining at the district-level ANISA field offices. Pre- and post-training tests were conducted using pretested questions, and all personnel showed proficiency by the end of the pilot phase.
During January and May, 2013, additional rooms were made available by study hospital authorities for clinical and data manage-ment activities. The microbiology operations required many major changes, including controlled airflow in culture areas. Experts from CHRF and the US Centers for Disease Control and Prevention (CDC), Atlanta, as well as University of Nebraska-based investiga-tors, provided hands-on training through troubleshooting and estab-lishing different steps of specimen collection, analyses, storage and shipment. Information technology (IT) staff from CHRF helped the local IT manager in Bhubaneswar to install software remotely and conducted a site visit to provide further training and troubleshoot-ing in various procedures for logging and tracking the text message report generation and other ancillary IT-related activities.
The Odisha field sites started piloting in June 2012 and graduated to the main study activities in August 2013 based upon satisfactory fulfillment of performance indicators.10 Healthy con-trol selection also began at that time.
ETHICAL CLEARANCE AND OTHER APPROVALSThe study protocol was approved by the Ethical Review
Committee of the Asian Institute of Public Health which is respon-sible for the overall implementation of the study protocol at Odisha. Approval was also obtained from the Ispat General Hospital Ethical Review Committee. Since government health systems were utilized, we obtained additional approval from the Department of Health and Family Welfare of the Government of Odisha. The protocol was then reviewed (including an external peer review) by the Foreign Projects Department of the Indian Council of Medical Research. Final clearance from the Health Ministry Screening Committee of the Government of India was received along with approval from the Department of Home Affairs.
CHALLENGES IN THE ADOPTION OF THE ANISA PROTOCOL AND REMEDIAL ACTIONS
Field ActivitiesReaching Newborns Within 24 Hours of Birth
Although 88%–94% of all births in the Odisha site now take place in hospitals, we faced the initial challenge of capturing these births early. A majority (55%–62%) of mothers live far from hospi-tals, so it was difficult for CHVs and supervisors to reach the hospi-tals in time to collect initial information to enroll newborns within 24 hours. During the first 3 months of the study, we captured only about half of all births within this time frame (Fig. 3). Although this rate improved to some extent after retraining, it was inconsistent and dropped during the cold season (December). We then employed nurses to cover both day and night shifts at the hospitals where most deliveries took place. January and February, 2014, showed an increase in reporting in the first 6 hours after birth. A second round of refresher training was conducted in April 2014, and helped to maintain this high level in the first 6 hours of life, with most other births recorded within the first 24 hours (Fig. 3).
Ensuring Accurate Newborn Assessments and Referral of pSBI Cases to Study Hospitals from Villages
Our second biggest challenge was identification of pSBI cases by CHVs at the community level and timely referral to study hospitals. Initially the identification rate was very low (2%–4%). A field office for each site was opened in the community for rigorous reinforcement of the protocol and training every fortnight. Utiliza-tion of our 3-tiered monitoring system using the mother-baby card (described below) along with routine use of mobile phones to call supervisory staff increased the rate to a steady 20% of all births
FIGURE 2. ANISA management structure at Odisha site, India. PI, principal investigator.
0
20
40
60
80
100
Firs
t pos
tnat
al v
isit
timin
g (%
)
0-6 hrs
6-12 hrs
12-24 hrs
FIGURE 3. Time of first assessment of newborns at Odisha site, July 2013–June 2014.

The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016 Challenges in Odisha Site, India
© 2016 Wolters Kluwer Health, Inc. All rights reserved. www.pidj.com | S77
(Fig. 4). During this transition and improvement, we worked hard to prevent unnecessary referral. The regular presence of study phy-sicians in the field for confirmation or rejection of a diagnosis of pSBI made by the CHVs and comonitoring by area coordinators and program managers provided an additional level of confidence to the field workers to discern milder ailments while not missing any pSBI cases. We are now able to maintain specificity without losing sensitivity; about half of the referred cases are admitted after evaluation by a study physician (Fig. 5).
Large Study Area, Difficult Terrain, Delay in Case Identi-fication and Transport
The distance to be covered by CHVs and area coordina-tors in a 480 km2 area with forest and hills was a challenge in Rourkela. The recruitment of 15 additional CHVs permitted strict home monitoring. While each CHV sometimes visited only 3 or 4 homes (compared with more than 15 by others) because of the terrain, the time involved was necessary and the only way to conduct true population-based surveillance in areas where many deaths occur due to lack of communication and timely transport of sick young infants to hospitals. Even in coastal areas, the time taken for transportation of sick young infants and their parents was a challenge. Instead of utilizing one study vehicle in each area, we introduced a system where local owners of 3-wheeled auto-rickshaws provided transport upon receiving a phone call and received immediate payment at the study hospital according to set rates.
Enrolling Healthy ControlsThe enrollment of healthy controls was considered to be of
paramount importance in the study to rule out normal colonizers that do not cause disease. The local institutional review board wanted study participants to perceive specific benefits apart from rigorous
health monitoring in the most critical period of infancy. Since meta-bolic screens were still not part of routine care, we offered free thy-roid screening to rule out congenital hypothyroidism that can cause serious morbidity. The offer of this screening, along with counseling by field personnel and study physicians, allowed our site to recruit the required number of controls for this study.
Hospital and Laboratory ActivitiesQA/QC of Blood Culture
There were initial problems with contamination of blood cultures which needed to be addressed (Fig. 6). Allocation of a dedicated clean room for blood draws as well as training of nurses and completion of a physician-observed checklist helped maintain a contamination level below 5%. However, to achieve this level required constant vigilance. We found that even a small decrease in monitoring by laboratory staff resulted in increased contamina-tion at both locations. We continue to have problems of contamina-tion in cases where the young infant requires immediate oxygen and other life support in the crowded pediatric ward and cannot be brought to the research sampling room.
Uninterrupted Power Supply and Maintenance of Major Equipment
We installed generators for freezers and automated blood culture machines, and uninterruptible power sources for all data management equipment. Although there are maintenance con-tracts at each site, we have faced time lags for factory-approved technicians to repair equipment. Our proactive measure was to provide a second −80°C freezer at each site which prevented thaw-ing of valuable specimens when one of the freezers was out of order for nearly a week.
International Shipment of SpecimensWhile there are multiple air couriers, it was difficult to find
ones that allowed dry ice shipments and assured refilling during transit. In fact, our first shipment arrived at CDC when Atlanta was experiencing an unusual ice storm, resulting in flight cancellations and road traffic problems. However, due to the availability of stor-age facilities and the ability of the courier to refill the shipment with dry ice, all specimens were maintained at the required tem-perature until delivery.
Unique Activities at the Odisha SiteMother-baby Card and Manual of Newborn Care
A mother-baby card written in the local language, Odia, is given to the mother in the last trimester of pregnancy for follow-up. This card is kept with the mother throughout the study period. It bears a serial number (for internal tracking by field staff) and the
0
5
10
15
20
25
CH
W r
efer
rals
for
PSB
I (%
of
birt
hs)
FIGURE 4. Rate of CHV referral for pSBI compared with number of births, July 2013–May 2014.
0
25
50
75
Phys
icia
n-co
nfir
med
pSB
I (%
of
CH
V R
efer
rals
)
FIGURE 5. Physician-confirmed pSBI rates among CHV-referred young infants, July 2013–June 2014.
0
10
20
30
40
50
Con
tam
inat
ion
rate
(%
)
FIGURE 6. Rate of contamination at RKL-BBS site (July 2013–June 2014).

Satpathy et al The Pediatric Infectious Disease Journal • Volume 35, Number 5, Supplement 1, May 2016
S78 | www.pidj.com © 2016 Wolters Kluwer Health, Inc. All rights reserved.
ANISA study identification number. There are spaces for record-ing health status and the signatures of the CHV, area coordinator and a third-level supervisor/study physician. These signatures, with dates and times, in conjunction with scheduled and surprise visits by supervisors, provide a strict monitoring system for field workers. This card also serves as identification for the mother and infant when they come to the study hospital for treatment.
SUMMARY AND CONCLUSIONImplementing ANISA in a population of over 350,000
spread across a large area with diverse geographic, socio-cultural and economic backgrounds was a formidable task. Involvement and assistance from state health department personnel, hiring local full-time study staff, enhancing individual family contacts, moti-vating marginal and minority communities and providing direct support to needy cases at health service points played important roles in attaining the necessary quality for our site to graduate from piloting to the main study phase in a relatively short time period. Implementation was a team effort with field staff, clinicians, micro-biologists and data management staff working together on a regular basis. The ability of all our field staff to use mobile phones and text messaging was invaluable. The assistance provided by skilled domain experts at CHRF and CDC at every step was instrumental in addressing deficiencies in a timely fashion. Although the site is halfway into the main study, reaching sick young infants and trans-porting them to our study hospitals (and not to other private care providers or village doctors) will continue to be a challenge as we attempt to track and collect biological specimens from every young infant with pSBI for bacterial and viral analyses.
ACKNOWLEDGMENTSThe authors thank the officials at the Indian Council of
Medical Research for reviewing this protocol. This study could not have been implemented without the ownership and keen interest of the Cabinet Minister and Principal Secretary, Department of Health and Family Welfare, Government of Odisha. We are grate-ful to Mahendra Pradhan, Ranjan K. Raul, Basil Kullu, Karuna-kar Panda, Sunita Patel, Sabita Behera, Janaki Shaw and Jyoti R. Mohanty for their support in the data center, field and hospital.
Our thanks are also due to over 250 field staff, including the CHVs and supervisory staff, and all the Anganwadi workers and ASHAs in the districts of Rourkela and Bhubaneswar for their sincere dis-charge of the duties assigned to them, as well as to the parents of the infants enrolled in this important study for their cooperation. We are grateful to Meghan Scott for her assistance in developing the manuscript.
REFERENCES 1. Islam MS, Baqui AH, Zaidi AK, et al. Infection surveillance protocol for a
multicountry population-based study in South Asia to determine the inci-dence, etiology, and risk factors for infections among young infants 0 to 59 days old. Pediatr Infect Dis J. 2016;35 (Suppl 1):S9–S15.
2. Islam MS, Rahman QS, Hossain T, et al. Using text messages for critical real-time data capture in the ANISA study. Pediatr Infect Dis J. 2016;35 (Suppl 1):S35–S38.
3. Directorate of Census Operations, Orissa. Provisional Population Totals – Orissa - Data Sheet: 2011. New Delhi, India: Office of the Registrar General and Census Commissioner; 2011. Available at: http://censusin-dia.gov.in/2011-prov-results/data_files/orissa/Data%20Sheet-%20Orissa-Provisional.pdf. Accessed September 19, 2014.
4. Panigrahi P. Effectiveness of a Lactobacillus plantarum synbiotic against late onset sepsis in neonates [Abstract 3618.2]. In: 24th Annual Meeting of Pediatric Academic Societies, Washington, DC; May 4–7,2013. The Woodlands, TX: Pediatric Academic Societies; 2013.
5. Carlo M, Gouder S, Jehan I, et al. High mortality rates for very low birth weight infants in developing countries despite training. Pediatrics. 2010;126:e1072–1080.
6. Carlo WA, Goudar SS, Jehan I, et al. Newborn-care training and perinatal mortality in developing countries. N Engl J Med. 2010;362:614–623.
7. Panigrahi P, Parida S, Pradhan L, et al. Long-term colonization of a Lactobacillus plantarum synbiotic preparation in the neonatal gut. J Pediatr Gastroenterol Nutr. 2008;47:45–53.
8. McClure EM, Wright LL, Goldenberg RL et al. The global network: a pro-spective study of stillbirths in developing countries. Am J Obstet Gynecol. 2007;197:247.e1–e5.
9. Registrar General & Census Commissioner, India. Annual Health Survey Bulletin 2011–12, Odisha. New Delhi, India: Office of the Registrar General and Census Commissioner; 2012. Available at: http://censusindia.gov.in/vital_statistics/AHSBulletins/files2012/Odisha_Bulletin%202011–12.pdf. Accessed September 19, 2014.
10. Connor NE, Islam MS, Arvay ML, et al. Methods employed in monitoring and evaluating field and laboratory systems in the ANISA study: ensuring quality. Pediatr Infect Dis J. 2016;35 (Suppl 1):S39–S44.