-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
1/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
www.medscape.com
Abstract and Introduction
Abstract
A variety of head and neck vascular emergencies, such as
nosebleeds or neoplastic hemorrhages, can occur spontaneously o
result from blunt or penetrating trauma. As most traumatic
venous bleeding can be resolved with direct pressure, the main
focus is on arterial injury. The role of catheter angiography in
the acute trauma setting has shifted over the past 15 years,
with
the concomitant advances in computed tomography (CT) angiography
for diagnosis, and development of microcatheters and
embolic agents for therapy.
Introduction
A variety of head and neck vascular emergencies, such as
nosebleeds or neoplastic hemorrhages, can occur spontaneously o
result from blunt or penetrating trauma. As most traumatic
venous bleeding can be resolved with direct pressure, the main
focus is on arterial injury. The role of catheter angiography in
the acute trauma setting has shifted over the past 15 years,
with
the concomitant advances in computed tomography (CT) angiography
for diagnosis, and development of microcatheters andembolic agents
for therapy.
Regional trauma associations have proposed algorithms for which
patients should be evaluated by CT angiography and/or
catheter angiography for traumatic head and neck vascular
injuries.[13] These include high-risk mechanisms such as: high-
energy collisions, neck hyperextension injury, intra-oral
trauma, and near-hanging with anoxic brain injury. Additionally, CT
or
catheter angiography should be considered in patients with
LeFort/midface fractures, cervical spine or basilar skull
fractures,
diffuse axonal injury with Glasgow Coma Scale (GCS) < 6, a
new focal neurological deficit, neurological examination
incongruous with head CT findings, or imaging evidence of a new
cerebral infarct in the setting of trauma.
Clinically occult head and neck vascular injury is rare;
however, aggressive CT screening in asymptomatic patients has
become
commonplace given the potentially devastating sequelae of a
missed diagnosis,[46] combined with ease of access to CT
angiography. Ongoing discussion in the trauma community
continues regarding patient selection criteria, given the concerns
of
cost effectiveness of broad screening in asymptomatic patients
as well as minimizing unnecessary radiation exposure.
There remain cases in which conventional angiogram remains the
'gold standard.' These include CT angiograms limited by
artifact from dental implants/amalgam, from metal or shrapnel,
situations where appropriate bolus timing cannot be achieved,
and hemodynamically unstable patients with a high probability of
requiring endovascular intervention. Diagnostic catheter
angiogram should always be considered in a patient with high
suspicion for cervical vascular injury in the setting of a normal
CT
angiogram, as this is a dynamic disease process and contrast
opacification of a vessel on cross-sectional imaging may not
fully reflect flow dynamics and collateral pathways.
Large Arterial Lacerations, Pseudoaneurysms, and Arteriovenous
Fistulae
Damage to the arterial wall can result in life-threatening
hemorrhage, and patients with large arterial lacerations due to
penetrating trauma have significant mortality before reaching
hospital care. Alternatively, hemorrhage may be contained by
development of a pseudoaneurysm or diverted through a traumatic
arterial-venous fistula. In dealing with a patient with a
potential arterial laceration, it is crucial to maintain
hemodynamic and ventilatory support throughout the search for
and
treatment of the active bleeding site.
Exploration of anterior neck wounds is usually done surgically,
given adequate exposure and direct visualization of the carotid
arteries.[7] In patients with active hemorrhage from a carotid
or vertebral laceration, there is a high risk of stroke or even
death
despite aggressive treatment, including surgical ligation or
endovascular embolization of the vessel. Given the difficult
surgical
approach to the carotid artery at the skull base and the
vertebral arteries, [8,9] the interventional neuroradiologist can
provide
great support to the trauma team with an endovascular approach
to treatment at these sites. [10,11,12] Additionally, in
patients
Angiographic Evaluation and Treatment for Head and Neck Vascular
InjuryJulie Bykowski, MD; Wade Wong, DO, FACR, FAOCR
Posted: 04/26/2012; Appl Radio l. 2012;41(3):10-16. 2012
Anderson Publishing, Ltd.
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
2/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
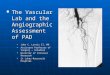
with extensive facial fractures or penetrating injuries, an
endovascular approach to control bleeding is preferred (Figure
1).
Figure 1. (A) CT scan of a 22-year-old man with massive facial
hemorrhage following a gunshot wound. (B) Early arterial
phase of left external carotid arteriogram shows active contrast
extravasation (arrowhead). (C) Left external carotidarteriogram
after embolization with gel foam slurry confirms cessation of
extravasation.
Pseudoaneurysms result from arterial bleeding into the wall of
an injured vessel. This can manifest as a focally expanded
dissection with containment by the adventitia, or containment of
leakage outside of the vessel wall by a layer of clot. While
some extremity pseudoaneurysms have been reported to resolve
spontaneously, [13] asymptomatic pseudoaneurysms of the
carotid arteries are generally treated to preclude
thromboembolic stroke and reduce the risk of re-bleeding.
Endovascular
embolization with coils or balloon occlusion is often favored
over direct surgical exploration; [14,15] however, it should be
done
with care as re-bleeding is common given the fragility of
structures containing the site of injury (Figure 2). In some
situations, a
stent may be sufficient to divert flow, allowing the
pseudoaneurysm to thrombose without coil deployment.[1618] Some
controversy persists regarding the risks and benefits of stent
placement, with long-term stent occlusion rates reported in up
to
45% of patients in early series.[19] Discussion continues about
the ideal timing of treatment, perceived benefits of different
sten
features, and optimal concomitant antiplatelet therapy in these
patients.[20]
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
3/12
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
4/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
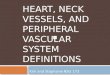
Figure 3. (A) 38-year-old woman complained of "swooshing" sound
after whiplash injury. Right external carotid
arteriogram confirms arteriovenous fistula, supplied by small
branches of the right occipital artery. (B) A microcatheter was
advanced into the right occipital artery and successful
embolization of feeder branches was performed with 200-micron
polyvinyl alcohol (PVA) particles.
Figure 4. (A) CT scan in 18-year-old-man with facial trauma
revealed an enlarged left superior ophthalmic vein. (B) Left
internal carotid arteriogram confirmed the presence of a carotid
cavernous fistula. (C) Arteriogram repeated after
detachable balloon placement in the single hole shunt of the
fistula shows occlusion of the fistula.
In situations where vessel sacrifice is considered, occlusion by
balloons or coils should only be done after a thorough test
balloon occlusion to ensure there will not be undesired,
irreversible neurological sequelae. Unilateral vertebral artery
occlusion
is considered more forgiving as long as the contralateral,
uninjured vertebral artery has adequate caliber and the
embolization
material can be deployed proximal to the posterior inferior
cerebellar artery (PICA), preserving collateral supply on the side
of
injury.[24,25] A typical balloon test occlusion is performed by
anticoagulating the patient with heparin and then advancing an
occlusive balloon across or distal to the site of injury, to
cause cessation of blood flow. Neurological testing for the
carotid
artery would include evaluation of pronator drift, motor,
sensory, and memory function. Vertebral artery neurological
testing
during balloon occlusion is less reliable, however, and emphasis
should be placed on coordination, motor, and sensory
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
5/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
function. The balloon test occlusion is typically maintained for
30 minutes or until the patient fails the procedure.
Extracranial Arterial Dissections and Occlusions
Arterial dissections in the head and neck usually are associated
with deceleration and shear injuries. These include injuries to
the proximal cervical vertebral artery, and the distal internal
carotid and vertebral arteries below the skull base. Vertebral
artery
dissections can also occur at the sites of transverse foramen
fractures, and these areas should be carefully evaluated in the
setting of cervical spine trauma.[26] Occlusions can result from
sluggish flow in the dissected vessel, compounded by
underlying atherosclerotic disease.
In the acute setting, CT angiography is commonly used to
evaluate for vessel irregularity and filling defects. MR
imaging,
particularly T1 fat-saturated sequences, is sensitive for the
detection of methemoglobin in a false lumen of a dissection
[27]
(Figure 5). However, within the first 3 days after the traumatic
event, the blood products often have only intermediate signal
changes. Diagnostic catheter angiography may be needed in
patients with artifact from bullet fragments or dental amalgam
or
difficult evaluation at the skull base.
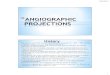
Figure 5. (A) MR imaging reveals T1-hyperintense methemoglobin
(black arrowhead) surrounding a narrowed left internal
carotid artery, confirming dissection. (B) Corresponding
angiogram confirms focal vessel narrowing at the point of
dissection (lower arrowhead). Thrombus is also noted distally
within the left internal carotid artery (upper arrowhead), as
an intraluminal filling defect.
Treatment of carotid and vertebral arterial dissections remains
somewhat controversial. [2] The most conservative approach
includes medical management, with ongoing debate as to whether
anticoagulation with heparin and/or antiplatelet therapy is
more effective.[19,26,28,30] There remains concern about the use
of these agents in the setting of acute multitrauma,[30]
althoug
successful treatment with antiplatelet agents has also been
described in the setting of pre-existing intracranial hemorrhage.
[31]
Medical management has resulted in 50% to 70% successful
arterial recanalization rates. [32,33] However, these patients
remain at risk for thromboembolic events in the days to weeks
following the traumatic event [34] or delayed formation of
dissecting aneurysms. Much of the healing of dissections occurs
36 months after the inciting event.[35,36]
Stents have been used to treat patients who have
contraindications to anticoagulation or antiplatelet therapy, [37]
although
adjunctive antiplatelet therapy is often used to ensure
long-term stent patency.[20] Endovascular treatment with stents has
also
been described in patients who fail medical management either
with ongoing or new neurological symptoms, or enlargement of
a dissecting aneurysm on follow-up evaluation. [38]
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
6/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
If an ischemic stroke has occurred, coordination with the stroke
neurology team is essential. Brain imaging, including
diffusion-
and perfusion-weighted imaging, should be a consideration,
understanding that there may be time constraints if
revascularization is indicated. If imaging suggests an embolic
mechanism for the stroke, techniques similar to stroke
thrombolysis or thromboembolectomy may be used. If a large
vessel occlusion is present, angioplasty or stenting may not be
wise as this may cause a reperfusion hemorrhage in the
brain.
Branch Vessel Arterial Lacerations
Trauma to the face, neck, and scalp can result in damage to
branches of the external carotid arteries that cannot be
controlled
by direct pressure alone. Understanding the trauma mechanism and
having cross-sectional imaging of the head and neck arehelpful in
the acute setting to tailor the angiogram most expeditiously to
areas of interest. One should always consider the rich
collateral supply to the face and neck, and the thyrocervical
trunk, vertebral artery, and internal carotid artery branches
should
also be scrutinized (Figure 6).
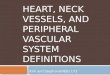
Figure 6. (A) Right common carotid arteriogram in patient with
hematochezia reveals active extravasation from a branch
of right superior thyroid artery (arrowhead). (B) Selective
arteriogram after embolization with 200-micron PVA particles
confirms cessation of flow distal to the micrcatheter and
absence of further extravastion from the right superior thyroid
artery.
The goal is to decrease the pressure head within the injured
vessel with resulting cessation of bleeding. Generally, it is
important to place the tip of the catheter as close to the
bleeding site as practical to avoid occlusion of normal
branches.
Additionally, prior to any particle embolization, one should be
well aware of potential dangerous anastamotic collaterals.[39]
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
7/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
These include: distal external carotid artery ethmoidal
perforators to the ophthalmic artery, superficial temporal artery
to the
middle cerebral artery, middle meningeal artery to the
ophthalmic artery, and occipital artery to the vertebral artery
(Figure 7).
Additional embolization hazards, such as scalp necrosis, should
be kept in mind when targeting sites in the superficial
temporal and occipital arteries.
Figure 7. (A) Retrograde flow can be seen from the external
carotid into the distal internal carotid via ethmoidal
perforators and the ophthalmic arteries (arrowhead). (B)
Collateral flow is identified from the occipital artery branch of
the
external carotid artery, to the vertebral artery (arrowheads).
This can present hazards during embolization.
In areas where potential neurological deficit or collateral flow
would be detrimental, provocative testing with 2 ml 1%
lidocaine
(20 mg) with concomitant neurological testing can be helpful.
For example, provocative testing can reveal neurological deficits
o
cranial nerves V, VII, and X associated with the ascending
pharyngeal artery before embolization, allowing for appropriate
change in the therapy plan.
Temporary occlusive agents, such as gel foam and particles, are
the preferred embolization material in most situations, as
coils, glue, and balloons may preclude access in the setting of
re-bleeding. Gel foam can be made into a slurry with contrast,
allowing safe, targeted delivery through a 3 or 4 French
catheter. Particles, such as 200700 micron polyvinyl alcohol,
are
usually mixed with Iohexol 240 contrast to create an evenly
distributed isobaric solution. Polyvinyl alcohol particles are
injected
via a microcatheter fast enough to be visualized but not so fast
as to create reflux into normal vessels. As the embolization
progresses, the injection rate typically slows until stagnation
and flow are angiographically evident. The use of smaller
particles
increases the risk of nontarget embolization by particle
migration via small collateral vessels.
Epistaxis
Nosebleeds are common and can be spontaneous, traumatic, or
secondary to underlying telangiectasia, arteriovenousmalformations
or neoplasms, such as juvenile nasal angiofibromas. The first step
is to identify the site of bleeding.
Most commonly, the bleeding site is anterior, supplied from
Kiesselbach plexus (sphenopalatine, descending palatine,
superior
labial branches from ECA and anterior and posterior ethmoidal
arteries from the ophthalmic artery). [40,41] Anterior nasal
bleeding can often be stopped with direct pressure, packing, or
cautery, given the ease of access. If the bleeding site is
posteriorly located, endovascular embolization is preferred over
arterial ligation, as it allows repeated access in the event of
re-
bleeding via collateral branches.[42, 43] This is usually best
accomplished via the internal maxillary arteries (Figure 8),
with
microcatheter placement distal to the origins of the middle
meningeal and accessory meningeal arteries.
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
8/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
Figure 8. (A) 62-year-old woman presented with nasal congestion.
Coronal CT scan reveals a right nasal cavity mass.
Extensive uncontrolled hemorrhage occurred after biopsy. (B)
Right external carotid arteriogram reveals active contrast
pooling after the arterial stage, indicating active bleeding.
This was successfully treated with microcatheter selection of
the
distal internal maxillary artery (arrowhead) and embolization
with 300-micron PVA particles.
In all cases of nasal and facial embolization, it is essential
to evaluate collateral supply via the ophthalmic and facial
arteries to
avoid undesirable non-target embolization.[44] Collateral supply
can occur via the artery of the foramen rotundum, the vidian
andascending pharyngeal arteries, as well as communications between
the facial, sphenopalatine and ophthalmic arteries.
Preferred treatment is with temporary occlusive agents, such as
200500 micron polyvinyl alcohol particles. It is important to
closely monitor the injection rate, to avoid reflux into other
branch vessels. If subselective arterial positioning cannot be
achieved or the vascular anatomy is altered by prior surgical
intervention, gelfoam injection into the larger, feeding artery
may
sufficiently diminish the pressure and stop the bleeding. We
typically avoid using coils to treat epistaxis, as these
permanent
devices preclude future access, if re-bleeding occurs. Having to
access the bleed via collateral sources such as the ophthalmic
artery makes the embolization procedure much more hazardous.
Neoplastic Bleeds
Vascular head and neck neoplasms, such as thyroid cancer and
paraganglioma, may bleed spontaneously and be difficult to
control externally. Often, the only finding is hypervascular
oozing. In such cases, partial embolization of the tumor may
sufficiently shut down the vascular bed.
More commonly, head and neck cancers can erode into a blood
vessel wall and cause spontaneous hemorrhage. The search
for neoplastic bleeding source can be challenging (Figure 9),
and surgical exploration can be difficult in patients with prior
neck
dissection or radiation therapy. In the setting of neoplastic
bleeding, one may see hypervascular tumor blush or there may be
actual active extravasation.[45] In some cases, such as carotid
blow-out, bleeding can be profuse and life-threatening. In this
setting, emergent endovascular therapy with stents, balloon
occlusion and liquid glue have been reported, [46,47,48] with
the
understanding that these are often palliative measures.
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
9/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
10/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
Figure 9. (A) 81-year-old with metastatic thyroid cancer eroding
into the right mainstem bronchus, with intermittent
hematochezia. In this case, left subclavian angiography
demonstrated that the expected thyrocervical artery (white
arrowhead) was not the actual source. (B) Vascular contribution
to the tumor mass originated from the right superior
thyroid artery, demonstrated on subselective catheterization.
(C) After treatment with 200-micron PVA particles, right
superior thyroid arteriogram shows successful embolization.
Conclusion
Catheter angiography continues to serve a role in the diagnosis
of head and neck vascular trauma, particularly in cases with
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
11/12
9/12 Angiographic Evaluation for Head and Neck Vascular Injury
(printer-friendly)
ww.medscape.com/viewarticle/761133_print
high suspicion for vascular injury or where CT angiography is
limited due to artifact from dental amalgam or gunshot debris.
The
neurointerventionalist continues to play an increasing role in
the acute setting to identify and stop bleeding, with an
increasing
number of temporary and permanent agents within their
armamentarium. Before embolization, it is crucial to assess
collateral
vascular supply, both to avoid nontarget embolization and
undesired permanent sequelae when vessel sacrifice is required.
Endovascular procedures can also be a useful adjunct in patients
who have failed conservative management. The population of
head and neck vascular trauma and bleeding is heterogeneous and
techniques continue to advance to serve these unique
cases.
References
1. Biffl WL, Cothren CC, Moore EE, et al. Western Trauma
Association critical decisions in trauma: screening for and
treatment of blunt cerebrovascular injuries. JTrauma.
2009;67:11501153.
2. Miller PR, Fabian TC, Croce MA, et al. Prospective screening
for blunt cerebrovascular injuries: Analysis of diagnostic
modalities and outcomes.Ann Surg. 2002;236:386393.
3. Bromberg WJ, Collier BC, Diebel LN, et al. Blunt
cerebrovascular injury practice management guidelines: The
Eastern
Association for the Surgery of Trauma. J Trauma.
2010;68:471477.
4. Cogbill TH, Moore EE, Meissner M, et al. The spectrum of
blunt injury to the carotid artery: A mult icenter perspective.
J
Trauma. 1994;37: 473479.
5. Biffl WL, Moore EE, Ryu RK, et al. The unrecognized epidemic
of blunt carotid arterial injuries: Early diagnosis improves
neurologic outcome.Ann Surg. 1998;228:462470.
6. Berne JD, Norwood SH, McAuley CE, et al. The high morbidity
of blunt cerebrovascular injury in an unscreened
population: More evidence of the need for mandatory screening
protocols. J Am Coll Surg. 2001;192:314321.
7. Feliciano DV. Management of penetrating injuries to the
carotid artery. World J. Surg. 2001; 25:10281035.
8. Sclafani SJ, Panetta T, Goldstein AS, et al. The management
of arterial injuries caused by penetration of Zone III of the
neck. J Trauma. 1985;25:871881.
9. Sclafani AP, Sclafani SJ. Angiography and transcatheter
arterial embolization of vascular injuries of the face and
neck.
Laryngoscope. 1996;106:168173.
10. Reuben BC, Whitten MG, Sarfati M, Kraiss LW. Increasing use
of endovascular therapy in acute arterial injuries:
Analysis of the National Trauma Data Bank. J Vasc Surg.
2007;46:12221226.
11. Rao PM, Ivatury RR, Sharma P, et al. Cervical vascular
injuries: A trauma center experience. Surgery. 1993;114:527
531.
12. Herrera DA, Vargas SA, Dublin AB. Endovascular treatment of
penetrating traumatic injuries of the extracranial carotid
artery. J Vasc Interv Radiol. 2011;22:2833.13. Toursarkissian B,
Allen BT, Petrinec D, et al. Spontaneous closure of selected
iatrogenic pseudoaneurysms and
arteriovenous fistulae. J Vasc Surg. 1997;25:803809.
14. Cox MW, Whittaker DR, Martinez C, et al. Traumatic
pseudoaneurysms of the head and neck: Early endovascular
intervention. J Vasc Surg. 2007;46:12271233.
15. Herrera DA, Vargas SA, Dublin AB. Endovascular treatment of
traumatic injuries of the vertebral artery.AJNR Am J
Neuroradiol. 2008;29:15851589.
16. Berne JD, Reuland KR, Villarreal DH, et al. Internal carotid
artery stenting for blunt carotid artery injuries with an
associated pseudoaneurysm. J Trauma. 2008;64:398405.
17. Yi AC, Palmer E, Luh GY, et al. Endovascular treatment of
carotid and vertebral pseudoaneurysms with covered stents.
AJNR Am J Neuroradiol. 2008;29:983987.
18. Coldwell DM, Novak Z, Ryu RK, et al. Treatment of
posttraumatic internal carotid arterial pseudoaneurysms with
endovascular stents. J Trauma. 2000;48:470472.
19. Cothren CC, Moore EE, Biffl WL, et al. Anticoagulation is
the gold standard therapy for blunt carotid injuries to reduce
stroke rate.Arch Surg. 2004;139:540545.
20. DuBose J, Recinos G, Teixeira PG, et al. Endovascular
stenting for the treatment of traumatic internal carotid
injuries:
Expanding experience. J Trauma. 2008;65:15611566.
21. Gemmete JJ, Ansari SA, Gandhi DM. Endovascular techniques
for treatment of carotid-cavernous fistula. J Neuro-
Ophthalmol. 2009;29:6271.
22. Higashida RT, Halbach VV, Tsai FY, et al. Interventional
neurovascular treatment of traumatic carotid and vertebral
arter
lesions: Results in 234 cases.AJR Am J Roentgenol.
1989;153:577582.
23. Kirsch M, Henkes H, Liebig T, et al. Endovascular management
of dural carotid-cavernous sinus fistulas in 141 patients
Neuroradiology. 2006;48:486490.
-
7/28/2019 Angiographic Evaluation for Head and Neck Vascular
Injury (Printer-friendly)
12/12