Embed Size (px)
Citation preview

Angela Karnes
RD, CNSC, LDN

To identify in the adult inpatient population:
What is malnutrition?
Why should we care?
How do we diagnose malnutrition?
What can be done?

An inadequate intake of protein and/or energy over prolonged periods of time resulting in the loss of fat stores and/or
muscle stores. (1)

Characterized by:
Presence and degree of inflammation
No inflammation
Mild – moderate inflammation
Severe inflammation
The severity of malnutrition, based on observation of specific clinical characteristics can be:
Moderate
Severe

Starvation related • Chronic starvation without inflammation
• I.e. anorexia nervosa, chronic food insecurity
Chronic disease-related • Inflammation is present, chronic, and of mild to moderate degree
• I.e. organ failure, cancer, sarcopenic obesity
Acute disease- or injury related • Inflammation is present, acute, and of severe degree
• I.e. major infection, trauma, burns, closed head injury
(1)
Patient must have at least 2 of 6 characteristics to meet definition of malnutrition
Insufficient food intake compared with estimated nutrition requirements
Weight loss over time Loss of muscle mass Loss of fat mass Fluid accumulation Measurably diminished grip strength
Once at least 2 characteristics are identified, malnutrition is categorized as either MODERATE or SEVERE, depending on the severity of the above characteristics
(1)

One could say:
Criteria is met for:
Moderate malnutrition in the context of chronic illness
Severe malnutrition in the context of social or environmental circumstances
Severe malnutrition in the context of acute illness or injury


Pop Quiz
A. Impaired immunity
B. Increased risk of infection
C. Increased frequency of hospital admissions
D. Delayed recovery from illness
E. All of the above
(3)

Malnourished patients:
Have 3 times the risk for surgical site infection (4)
Are twice as likely to develop pressure ulcers (5)
Are at increased risk for falls
45% of patients who fall are malnourished (6)
Those with recent, unintentional weight loss are at increased risk for hospital readmission (7)

Hospitalized patients in medical and surgical
intensive care units experience increased morbidity and mortality related to poor
nutrition status prior to and/or during hospitalization (8)

Negative energy balance during the first 14 days in the ICU is an independent factor of ICU mortality in those needing prolonged mechanical ventilation. (9)
Underfeeding in the ICU has been associated with: Increased rate of infection
Poor wound healing
Reduced respiratory muscle mass
Delayed weaning from mechanical ventilation
Increased ICU LOS
Increased health care costs (10)

Protein-energy deficit occurs in 43 – 88% of critically ill patients (11, 12)
At least 1/3 of patients are malnourished upon hospital admission (11, 13, 14)
Without treatment ~ 2/3 of these will experience further nutritional decline during their hospital stay (15)
An estimated 38% of patients admitted well nourished will experience a nutritional decline during their hospital stay (15)
Both those who are malnourished upon admission and those who
become malnourished during their hospital stay will have increased
healthcare costs.
(15, 16, 17)

Malnourished patients spent an average of 12.6 days in the hospital compared to 4.4 days for well-nourished patients
Resulting in hospital costs almost 3 times higher for malnourished patients
$26,944 versus $9,485
(18)

Hospital infections
Cost ~$33 billion per year (19)
30 day readmissions
Cost ~$26 billion per year (20)
Treatment of hospital malnutrition has been shown to reduced incidence of both

Payment to hospitals can now be withheld for certain preventable conditions including:
Surgical site infections (5)
Pressure ulcers (4)
Falls (6)

All less likely when a patient is adequately nourished
Surgical Infections
Falls
Pressure Ulcers

Hospitals can be penalized for high rates of readmission for:
Heart attack
Heart failure
Pneumonia
In 2013, 2,225 hospitals were penalized $280 million related to excessive readmissions
(21)

Treating hospital malnutrition
Estimated 28% decrease in avoidable
readmissions
BIG SAVINGS
(22)

25% decrease in incidence of
pressure ulcers (23)
14% fewer overall
complications (24)
Average reduced LOS of ~2 days
(25, 26)
Decreased mortality
(27 – 32)
Improved quality of life
(33)


Identify at risk patients

Is Inflammation Present?

Albumin/Prealbumin Patients with low albumin or
prealbumin may or may not be malnourished. Both may be reduced by the systemic response to injury, disease, or inflammation.
White Blood Cell: nonspecific indicators that may
suggest inflammatory response
C-reactive protein: positive acute phase reactant may be measured to help clarify
whether active inflammation is present
These are NOT RELIABLE MARKERS of NUTRITION
They are indicative of the presence of inflammation,
disease severity, morbidity and mortality risk.
In order to diagnose malnutrition – additional
evidence is warranted.
(34 – 35)
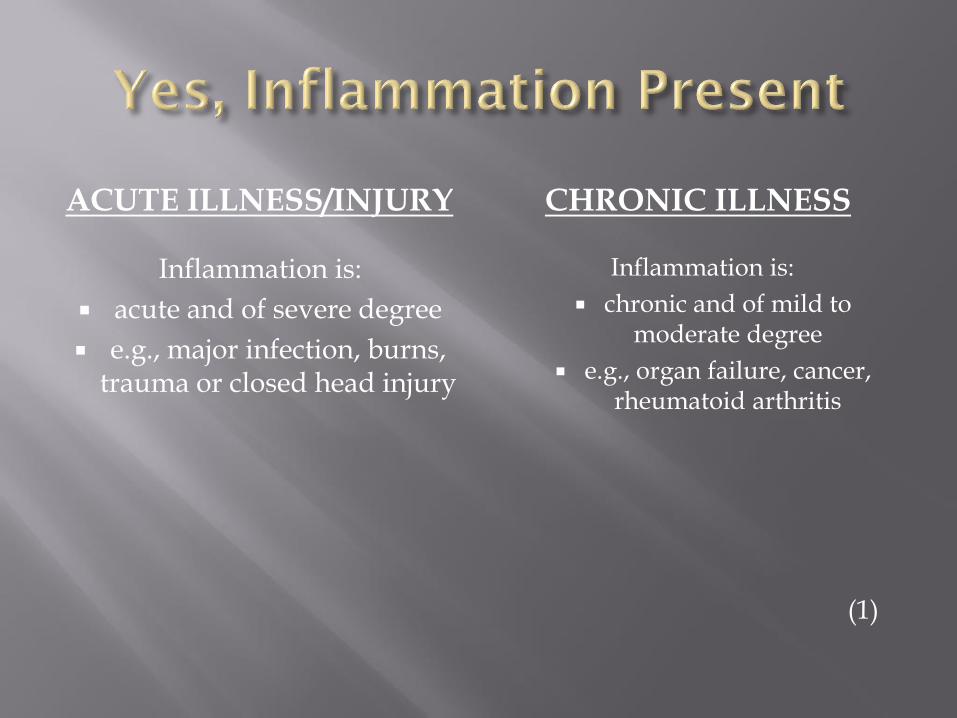
ACUTE ILLNESS/INJURY CHRONIC ILLNESS
Inflammation is:
acute and of severe degree
e.g., major infection, burns, trauma or closed head injury
Inflammation is:
chronic and of mild to moderate degree
e.g., organ failure, cancer, rheumatoid arthritis
(1)

Social/Environmental Circumstances (Pure Starvation)
*Chronic starvation without inflammation
* I.e. anorexia nervosa, longstanding food insecurity
(1)

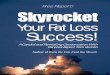
Nutrition Focused Physical Exam

Exam Areas Tips Severe Malnutrition Mild-Moderate
Malnutrition Well Nourished
Subcutaneous Fat Loss
Orbital region—
surrounding the eye
View patient when
standing directly in front
of them, touch above
cheekbone.
Hollow look, depressions,
dark circles, loose skin
Slightly dark circles,
somewhat hollow look
Slightly bulged fat pads,
fluid retention may mask
loss
Upper arm region—
triceps/biceps
Arm bent, roll skin
between fingers; do not
include muscle in pinch.
Very little space between
folds, fingers touch
Some depth pinch, but not
ample
Ample fat tissue obvious
between folds of skin
Thoracic and lumbar
region—ribs, lower back,
midaxillary line
Have patient press hands
hard against a solid object.
Depression between the
ribs very apparent; iliac
crest very prominent
Ribs apparent,
depressions between them
less pronounced; iliac crest
somewhat prominent
Chest is full, ribs do not
show; slight to no
protrusion of the iliac crest

Exam Areas Tips Severe Malnutrition Mild-Moderate
Malnutrition Well Nourished
Muscle Loss
Temple region—
temporalis muscle
View patient when
standing directly in front
of them, ask patient to
turn head side to side.
Hollowing, scooping,
depression Slight depression
Can see/feel well-defined
muscle
Clavicle bone region—
pectoralis major, deltoid,
trapezius muscles
Look for prominent bone.
Make sure patient is not
hunched forward.
Protruding, prominent
bone
Visible in male, some
protrusion in female
Not visible in male, visible
but not prominent in
female
Clavicle and acromion
bone region—deltoid
muscle
Patient arms at side,
observe shape.
Shoulder to arm joint
looks square, bones
prominent, acromion
protrution very prominent
Acromion process may
slightly protrude
Rounded, curves at
arm/shoulder/neck
Scapular bone region—
trapezius, supraspinus,
infraspinus muscles
Ask patient to extend
hands straight out, push
against solid object.
Prominent, visible bones,
depressions between
ribs/scapula or
shoulder/spine
Mild depression or bone
may show slightly
Bones not prominent, no
significant depressions
Dorsal hand—
interosseous muscle
Look at thumb side of
hand; look at pads of
thumb when tip of
forefinger touching tip of
thumb.
Depressed area between
thumb-forefinger Slightly depressed
Muscle bulges, could be
flat in some well-
nourished people

Lower Body Less Sensitive to Change – Muscle Loss
Patellar region—
quadricep muscle
Ask patient to sit with leg
propped up, bent at knee.
Bones prominent, little
sign of muscle around
knee
Knee cap less prominent,
more rounded
Muscles protrude, bones
not prominent
Anterior thigh region—
quadriceps muscles
Ask patient to sit, prop leg
up on low furniture.
Grasp quads to
differentiate amount of
muscle tissue from fat
tissue.
Depression/line on thigh,
obviously thin
Mild depression on inner
thigh
Well rounded, well
developed
Posterior calf region—
gastrocnemius muscle
Grasp the calf muscle to
determine amount of
tissue.
Thin, minimal to no
muscle definition Not well developed
Well-developed bulb of
muscle
Edema
Rule out other causes of
edema, patient at dry
weight
View scrotum/vulva in
activity-restricted patient;
ankles in mobile patient.
Deep to very deep pitting,
depression lasts a short to
moderate time (31-60 s),
extremity looks swollen
(3-4+)
Mild to moderate pitting,
slight swelling of the
extremity, indentation
subsides quickly (0-30 s)
No sign of fluid
accumulation
Exam Areas Tips Severe Malnutrition Mild-Moderate
Malnutrition Well Nourished
(36)

Result of:
Aging (Sarcopenia)
Acute or chronic inflammatory condition
Neurologic impairment
Pure starvation
Lack of physical activity
(34)

Associated with frailty, mortality, and worse surgical and nonsurgical outcomes
Significantly more expensive to care for
For Patients undergoing major general or vascular surgery, decreasing lean core muscle size is associated with increasing cost. Mean Payer Cost:
Sarcopenia : $34,796
Nonsarcopenia: $21,380
(35)

Muscle Loss Depressed area between thumb and forefinger


Severe Muscle Loss = Obvious
depression / line on thigh; thin
Severe Muscle Loss = Thin, minimal to no muscle
definition and firmness
Little sign of muscle around
the patella


Temple Region Severe Muscle Loss = Hollowing, scooping
depression
Severe Fat Loss = Hollow look,
depressions, dark circles, loose skin


Severe Muscle Loss Protruding/Prominent
clavicle bone
Severe Muscle Loss Scapular bone/upper
back Prominent bones with
definitive angles. Depressions easily seen.
Severe muscle loss Shoulder appears square with sharp
angle
Severe fat loss = very little
space between folds, fingers
touch
Severe fat loss =
Ribs very apparent. iliac crest
very prominen
t

Presence of 2 or More Characteristics?

Weight Loss Amount Time Frame
Nutritional Intake <50% <75% Time Frame
Functional Status Muscle Wasting
Mild, Moderate, or Severe
Fat Loss Mild, Moderate, or Severe
Edema Mild, Moderate, or Severe
(1)

Malnourished??
Yes or No?
Moderate or Severe?


Weight loss: 1-2% -- 1 week 5% -- 1 month 7.5% -- 3 months
Energy intake: <75% for >7 days
Body fat: Mild depletion
Muscle mass: Mild depletion
Fluid accumulation: Mild

Weight loss: 5% -- 1 month 7.5% -- 3 months 10% -- 6 months 20% -- 1 year
Energy intake:
<75% for >1 month
Body fat: Mild depletion Muscle mass: Mild depletion Fluid accumulation: Mild

Weight loss 5% -- 1 month 7.5% -- 3 months 10% -- 6 months 20% -- 1 year
Energy intake - <75% for >3 months
Body fat - Mild depletion Muscle mass - Mild depletion Fluid accumulation – Mild


Weight loss >2% -- 1 week >5% -- 1 month >7.5% -- 3 months
Energy intake - <50% for >5 days
Body fat - Moderate depletion Muscle mass - Moderate depletion Fluid accumulation – Moderate to severe

Weight loss >5% -- 1 month >7.5% -- 3 months >10% -- 6 months >20% -- 1 year
Energy intake - <75% for >1 month
Body fat - Severe depletion
Muscle mass - Severe depletion
Fluid accumulation – Severe

Weight loss >5% -- 1 month >7.5% -- 3 months >10% -- 6 months >20% -- 1 year
Energy intake - <50% for >1 month
Body fat - Severe depletion Muscle mass - Severe depletion Fluid accumulation – Severe
(37)
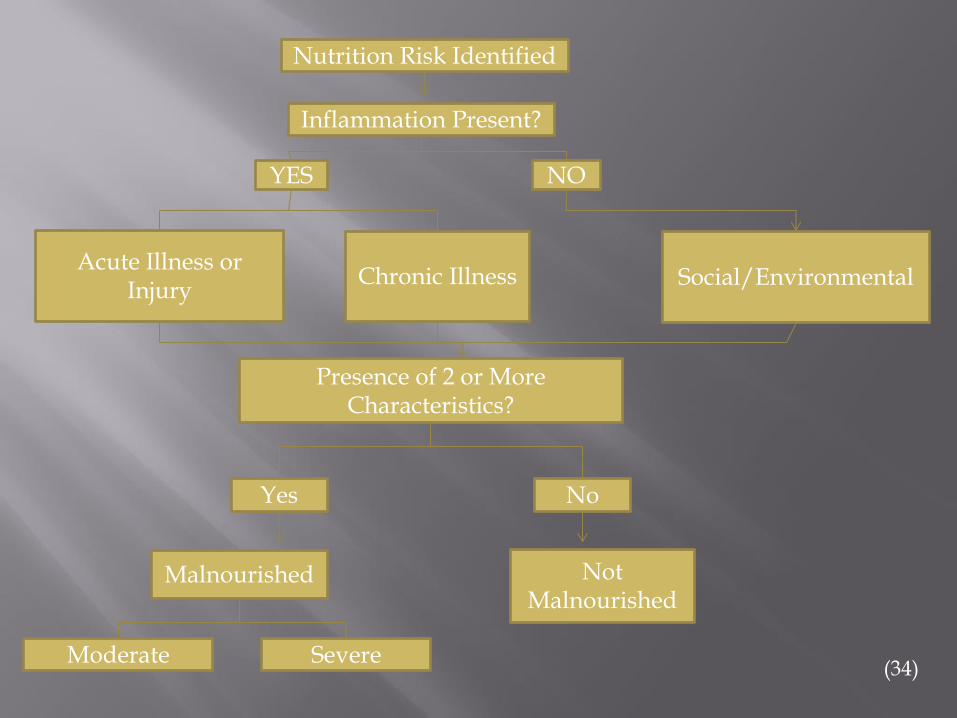
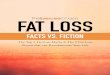
YES NO
Acute Illness or Injury
Chronic Illness Social/Environmental
Presence of 2 or More Characteristics?
Yes No
Not Malnourished
Malnourished
Moderate Severe
Nutrition Risk Identified
Inflammation Present?
(34)
Pop Quiz

Mr P is a 51 year old male admitted to the CVICU for heart failure exacerbation . Found to have a stage 3 pressure ulcer to his left heel – present on admission. PMH: ESRD on HD, HTN, DM type 2 Height: 183cm / 72in Admit Weight: 123kg Dry Weight (per patient report): 117kg BMI: 34.9 – class 1 obesity (based on dry weight) Weight History: Pt reports significant weight loss a few months back during a hospitalization at an OSH. 01/12/16 123.5kg 09/08/15 149.19kg Oral Intake History: Pt reports good appetite / intake currently Labs: BUN: 46 Creat: 7.37 GFR: 8 K+: 5.9 Nutrition Focused Physical Exam Moderate to Severe Temporal Wasting and depletion of orbital fat pads. Clavicle is quite prominent. Unable to visualize other muscle wasting secondary to body habitus/edema. Skin Breakdown: Stage 3 Pressure Ulcer - left heel

A. Severe malnutrition in the context of chronic illness
B. Moderate malnutrition in the context of chronic illness
C. Moderate malnutrition in the context of social/environmental situation
D. Does not meet criteria for malnutrition

Four Part Action Plan

Improve recognition of at risk patients Malnutrition is:
under-recognized
under-treated (33)
Screen, assess, and diagnose patients at malnutrition risk Difficulty chewing/swallowing
Age > 70 years
History of decreased appetite
History of unintentional weight loss
Regular use of oral nutrition supplements
Dependence on enteral/parenteral nutrition support
History of gastric bypass

Implement interventions without delay
For example: Early initiation of enteral nutrition support
Minimizing cessation of enteral nutrition/NPO status
Liberalization of diet order to encourage p.o. intake
Addition of snacks
Assistance with meal set up and feeding
Educating patients on the importance of eating enough
Addition of oral nutrition supplement

ONS are consistently shown to have beneficial clinical effects with economic implications (38)
Significant increase in total protein/energy intake with little suppression of normal food intake (38)
Use of high protein ONS is associated with improved functional outcomes (handgrip strength), decrease LOS, reduction in hospital readmission rates (39)
Readmission reductions
26 - 29% readmission rate with ONS vs 40- 48% without ONS (40, 41)
19% reduction in complications – including infection rates, healing of surgical wounds, pressure ulcers (42)

Empower all clinicians to address patients’ nutritional needs
Educate all clinicians on the recognition and diagnosing of malnutrition
Engage nurses in understanding malnutrition risk factors and create policies that allow nurses to help provide nutrition care
Initiate a nutrition care plan within 48 hours of admission for patients with or at risk of malnutrition
Integrate the dietitian into the interdisciplinary ICU team
Consult the dietitian immediately if malnutrition is suspected
Consider allowing registered dietitians to have ordering privileges for diet orders, oral nutrition supplements, and vitamins/minerals
(33)

Create culture where nutrition is seen as a priority for improving: Care Quality Cost
Create an open dialogue on potential institutional changes For example:
Easier availability of snacks/supplements Designated and protected meal times Improved quality of hospital food Enhanced menu selection Use of standardized written instructions for nutrition care at
home post-discharge and/or prior to admission for elective procedures (33)

Case Study

Mr K is a 70yo Male admitted to the Neuro ICU for rule out CVA. PMH: CAD, HTN, HLD, Chronic Alcoholism, and previous strokes. Height: 68in Current Weight: 80.8kg BMI: 26.99 (adequate for age) Weight History: 87.9kg 08/04/16 – 1 month ago 102kg 01/03/16 -7 months ago Oral Intake: Pt’s wife reports that he has been in and out of the hospital 6 times over the past 8 months. Pt dislikes hospital food. His oral intake is fair at home (eating ~50% of his meals) but very poor during his admissions. This has resulted in weight loss. Labs: WBC 11.8 Physical Exam: No pressure ulcers indicated Mild Muscle Wasting at temporal and clavicle regions

Does Mr. K. meet criteria for malnutrition??

A. Moderate malnutrition in the context of chronic disease
B. Moderate malnutrition in the context of social/environmental situation
C. Severe malnutrition in the context of chronic disease
C. Severe malnutrition in the context of acute illness/injury

- Liberalization of diet order to regular diet
- Addition of oral nutrition supplement
- Assistance with tray set up/feeding
- Addition of daily MVI, thiamine, folic acid
(given history of ETOH)
Malnutrition is under-recognized and often untreated although it is associated with increased:
Complication rates
Length of stay
Readmission rates
Mortality
Diagnosis and treatment of malnutrition has been consistently shown to improve patient outcomes (33)

We need to look at changing the attitude about the importance of hospital nutrition in both patients and providers (43)
Consider nutritional status an essential part of the patient’s condition
Make nutrition interventions a core component of medical therapy (33)
Better nourished patients translate to:
Improved care
Improved quality of life
Decreased costs (33)

We Can’t Afford Not To


1. Jensen et al. Adult starvation and disease-related malnutrition: A proposal for etiology-based diagnosis in the clinical practice setting from the International Consensus Guideline Committee. JPEN . 2010;34:156-159.
2. White JV, et al. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the indentification and documentation of adult malnutrition. JPEN J Parenter Enteral Nutr. 2012; 36: 275 – 283.
3. Elia M. Nutrition and health economics. Nutrition. 2006; 22: 576-578.
4. Fry DE, et al. Patient characteristics and the occurrence of never events. Arch Surg. 2010; 145:148 – 151.
5. Banks M, et al. Malnutrition and pressure ulcer risks in adults in Australian health care facilities. Nutrition. 2010; 26: 896-901.
6. Bauer JD, et al. Nutritional status of patients who have fallen in an acute care setting. J. Hum Nutr Diet. 2007; 20:558-564.
7. Coats KG, et al. Hospital-associated malnutrition: a re-evaluation 12 years later. J Am Diet Assoc. 1993; 93:27-33.
8. Esper DH, et al. Utilization of nutrition-focused physical assessment in identifying micronutrient deficiencies. Nutr Clin Pract. 2015; 30 (2): 194-202.
9. Zilberberg MD, et al. Prolonged acute mechanical ventilation, hospital resource utilization, and mortality in the United States. Crit Care Med. 2008; 36: 724-730.

10. Faisy C, et al. Impact of energy deficit calculated by a predictive method on outcome in medical patients requiring prolonged acute mechanical ventilation. Brit J Nutr. 2009; 101: 1079 – 1087 11. Giner M, et al. In 1995 a correlation between malnutrition and poor outcome in critically ill patients still exists. Nutrition. 12; 23 – 29 .
12. Barr J, et al. Outcomes in critically ill patients before and after the implementation of an evidence-based nutritional management protocol. Chest. 125; 1446 – 1457. 13. Coats KG, et al. Hospital associated malnutrition: a reevaluation. J Am Diet Assoc. 1992; 93: 27 – 33.
14. Thomas DR, et al. Malnutrition in subacute care. Am J Clin Nutr. 2002; 75: 308 - 313. 15. Braunschweig C, et al. Impact of declines in nutritional status on outcomes in adult patients hospitalized for more than 7 days. J Am Diet Assoc. 2000; 100: 1316 – 1322. 16. Chima CS, et al. Relationship of nutritional status to length of stay, hospital costs, and discharge status of patients hospitalized in the medicine service. J Am Diet Assoc. 1997; 97: 975 – 978
17. Correia MI, et al. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr. 2003; 22: 235 – 239.
18. Corkins MR, et al. Malnutrition diagnoses in hospitalized patients: United States, 2010. JPEN. 2014; 38: 186 – 195. 19. Centers for Disease Control and Prevention and the Association of State and Territorial Health Official. Eliminating Health-Care Associated Infections: State Policy Options. March 2011.

20. The Revolving Door. A Report on Hospital Readmission. Robert Wood Johnson Foundation. February 2013.
21. Rau J. “Armed with Bigger Fines, Medicare to Punish 2,225 Hospitals for Excess Readmissions”. Kaiser Health News, August 2, 2013.
22. Gariballa S, et al. A randomized, double-blind, palcebo-controlled trial of nutritional supplementation during acute illness. Am J Med. 2006; 119: 693 – 699.
23. Stratton RJ, et al. Enteral nutritional support in prevention and treatment of pressure ulcers: a systematic review and metaanalysis. Ageing Res Rev. 2005; 4: 422-450
24. Milne AC, et al. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Datatbase Syst Rev. 2009: CD003288.
25. Brugler L, et al. The five year evolution of a malnutrition treatment program in a community hospital. J Qual Improv. 1999; 25: 191 – 206
26. Smith PE, et al. High-quality nutritional interventions reduce costs. Healthc Financ Manage. 1997; 51: 66 – 69.

27. Potter J, et al. Routine protein energy supplementation in adults: Systematic review. Br Med J. 1998; 317: 495 – 501.
28. Potter JM, et al. Protein energy supplements in unwell elderly patients? A randomized controlled trial. JPEN. 2001; 25: 323- 329.
29. Delmi M, et al. Dietary supplementation in elderly patients with fractured neck of the femur. Lancet. 1990; 335: 1013 – 1016.
30. Lacson E Jr, et al. Outcomes associated with intradialytic oral nutritional supplements in patients undergoing maintenance hemodialysis. Am J Kidney Dis. 2012; 60: 591 – 600.
31. Stratton RJ, et al. Are oral nutritional supplements of benefit to patients in the community? Findings from a systematic review. Curr Opin Clin Nutr Metab Care. 2000; 3: 311 – 315.
32. Davidson W, et al. Weight stabilisation in associated with improved survival duration and quality of life in unresectable pancreatic cancer. Clin Nutr 2004; 23: 239 – 247.
33. Alliance to Advance Patient Nutrition. Alleviating Hospital-based Malnutrition : A Baseline Progress Report. July 2014.

34. Fischer M, et al. Evaluation of muscle and fat loss as diagnostic criteria for malnutrition. Nutr Clin Pract. 2015; 30 (2): 241.
35. Jensen G, et al. Nutrition Screening and Assessment. ASPEN Nutrition Support Core Curriculum, 2nd ed. 155 – 167.
36. Secker DJ, et al. How to perform subjective global nutritional assessment. J Acad Nutr Diet. 2012; 112:424-431.
37. Skipper A, et al. Academy of Nutrition and Dietetics (Academy)/American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) clinical characteristics that the clinician can obtain and document to support a diagnosis of malnutrition. J Acad Nutr Diet. 2012; 112 (5): 734 -735
38. Stratton RJ, et at. A review of reviews: a new look at the evidence for oral nutritional supplements in clinical practice. Clin Nutr Suppl. 2, 5 -23.
39. Curtis, L. 2010. Unit Cost of Health and Social Care. Personal Social Services Research Unit. University of Kent, Canterbury.
40. Gariballa S, et al. A randomized, double-blind, placebo-controlled trial of nutritional supplementation during
acute illness. Am J Med. 2006; 119: 693 – 699.

41. Norman K, et al. Three month intervention with protein and energy rich supplements improve muscle function and quality of life in malnourished patients with non-neoplastic GI disease – a randomized controlled trial. Clin Nutr. 2008; 27: 48 – 56.
42. Li P, et al. Amino acids and immune function. Br J Nutr. 2007; 98: 237 – 252.
43. Hiesmayr M, et al. Decreased food intake is a risk factor for mortality in hopitalised patients: The NutritionDay survey 2006. Clin Nutr. 2009; 28: 484 – 491.