Embed Size (px)
Citation preview

Anesthetic Potency and Cardiopulmonary Effects of Sevofluranein Goats: Comparison with Isoflurane and Halothane
Yoshiaki Hikasa, Kaihei Okuyama, Tomoko Kakuta, Katsuaki Takase, and Shigeo Ogasawara
ABSTRACT
The anesthetic potency and car-diopulmonary effects of sevofluranewere compared with those of isoflu-rane and halothane in goats. The(mean ± SD) minimal alveolar con-centration (MAC) was 0.96 ± 0.12%for halothane, 1.29 ± 0.11% forisoflurane, and 2.33 + 0.15% forsevoflurane. Cardiopulmonaryeffects of sevoflurane, halothaneand isoflurane were examined atend-tidal concentrations equivalentto 1, 1.5 and 2 MAC during eitherspontaneous or controlled ventila-tion (SV or CV). During SV, therewere no significant differences inrespiration rate, tidal volume andminute ventilation between anes-thetics. Dose-dependent decreasesin both tidal volume and minuteventilation induced by halothanewere greater than those by eithersevoflurane or isoflurane. Hyper-capnia and acidosis induced bysevoflurane were not significantlydifferent from those by eitherisoflurane or halothane at 1 and1.5 MAC, but were less than thoseby halothane at 2 MAC. There wasno significant difference in heartrate between anesthetics during SVand CV. During SV, all anestheticsinduced dose-dependent decreasesin arterial pressure, rate pressureproduct, systemic vascular resis-tance, left ventricular minute workindex and left ventricular strokework index. Systemic vascularresistance with isoflurane at 2 MACwas lower than that with sevoflu-rane. During CV, sevofluraneinduced dose-dependent circulatorydepression (decreases in arterial
pressure, cardiac index, rate pres-sure product, systemic vascularresistance, left ventricular minutework index and right ventricularminute work index), similar toisoflurane. Halothane did not sig-nificantly alter systemic vascularresistance from 1 to 2 MAC.
RESUME
L'efficacite anesthesiante et leseffets cardiorespiratoires du sevo-flurane ont ete compares a ceux del'isoflurane et de l'halotane chezdes chevres. La concentration alveo-laire minimale (CAM) (moyenne ±ET) etait de 0,96 ± 0,12 % pourl'halotane, 1,29 ± 0,11 % pourl'isoflurane et de 2,33 ± 0,15 %pour le sevoflurane. Les effetscardiorespiratoire du sevoflurane,de l'halotane et de l'isoflurane a desconcentrations en fin d'expirationequivalentes a 1, 1,5 et 2 fois laCAM ont ete examines lors de venti-lation spontanee ou controlee (VSou VC). Aucune difference signi-ficative ne fut observee entre lesagents anesthesiants durant la VSquant au rythme respiratoire,au volume courant et a la ventila-tion minute. La diminution dose-dependante du volume courant etde la ventilation minute induite parl'halotane etait plus important quecelles induites par le sevoflurane oul'isoflurane. L'hypercapnie et l'aci-dose induites par le sevoflurane n'-taient pas significativement dif-ferentes de celles induites parl'isoflurane ou l'halotane a desvaleurs de 1 et 1,5 fois la CAM,mais etaient plus petites que celles
de l'halotane 'a 2 fois la CAM.Aucune difference significative durythme cardiaque ne fut noteedurant la VS et la VC entre lesagents anesthesiants. Au cours de laVS, tous les agents anesthesiantsont induit une diminution dose-dependante de la pression arterielle,du produit frequence-pression, dela resistance vasculaire systemique,de l'index du travail ventriculairegauche par minute et de l'index dutravail d'ejection du ventriculegauche. La resistance vasculairesystemique avec l'isoflurane a 2 foisla CAM etait plus basse que celleavec le sevoflurane. Au cours dela VC, le sevoflurane a induitune depression circulatoire dose-dependente (diminution de la pres-sion arterielle, de l'index cardiaque,du produit frequence-pression, dela resistance vasculaire systemique,de l'index du travail ventriculairegauche par minute, et de l'index dutravail ventriculaire droit parminute) semblable a celle produitepar l'isoflurane. Des concentrationd'halotane de 1 a 2 fois la CAMn'ont pas modifiees significati-vement la resistance vasculairesystemique.
(Traduitpar docteur Serge Messier)
INTRODUCTION
A non-flammable, halogenatedinhalant, sevoflurane, has a lowblood/gas partition coefficient similarto nitrous oxide (1), and producesrapid induction of and recovery fromanesthesia and rapid alteration ofanesthetic depth (2-7). The arrhyth-mogenic dose of adrenaline for
Department of Veterinary Medicine, Faculty of Agriculture, Tottori University, Koyama-Minami, Tottori-shi, Tottori 680, Japan (Hikasa); Departmentof Veterinary Surgery, School of Veterinary Medicine and Animal Sciences, Kitasato University, Towada-shi, Aomori 034, Japan (Okuyama, Kakuta,Takase, Ogasawara).Correspondence to: Yoshiaki Hikasa, DVM, PhD, Department of Veterinary Medicine, Faculty of Agriculture, Tottori University, Koyama, Tottori-shi,Tottori 680, Japan. Phone: +81 857 31 5432, Fax: +81 857 31 5432. e-mail: [email protected] December 24, 1997.
Can J Vet Res 1998; 62: 299-306 299

sevoflurane is higher than that forhalothane and enflurane, and similarto that for isoflurane in dogs (8-10)and cats (11). Sevoflurane appears tobe a new anesthetic showing promise.The anesthetic potency and car-
diopulmonary effects of halothaneand isoflurane have been welldescribed in goats (12) and otherruminants (13-17). Sevoflurane hasbeen used as an effective anestheticproducing a rapid recovery in adultcattle (18) and horses (19). However,there is no information available onthe cardiopulmonary effects ofsevoflurane anesthesia in small rumi-nants. In this study, we compared theanesthetic potencies and cardiopul-monary effects of sevoflurane, isoflu-rane, and halothane anesthesia underspontaneous or controlled ventilationin goats.
MATERIALS AND METHODS
ANIMALS
Eighteen healthy Shiba goats(Capra hircus) of either sex, 1.5 to7 y of age, weighing from 18 to 39 kgbody weight (mean 24.6 ± 7.9 kg),were used in this investigation. Healthstatus was evaluated on the base ofhistory, physical examinations, com-plete blood counts, serum biochemi-cal profiles, and electrocardiogramsusing standard methods. They weregiven a commercial ruminant concen-trate, hay and water ad libitum. Allgoats were fasted for 12 h and werenot medicated before anesthesia.Anesthesia was carried out in a roomcontrolled at 21 to 24°C.ANESTHETIC PROCEDURES
In the experiment for determinationof the minimal alveolar concentration(MAC), 6 male goats were anes-thetized repeatedly at 2-week inter-vals with sevoflurane, isoflurane orhalothane in randomized order as fol-lows: 2 goats were anesthetized withsevoflurane, isoflurane and halothane,in that order. Another 2 goats wereanesthetized with isoflurane, halo-thane and sevoflurane, in that order.The remaining goats were anes-thetized with halothane, sevofluraneand isoflurane, in that order. Eachanesthetic was vaporised in an out-of-circuit vaporiser. Agent-specific pre-cision vaporisers were used for
halothane (Honey Matic M-3, KimuraMed., Tokyo) and sevoflurane(Mark II, Acoma Med., Tokyo), andisoflurane was vaporised from anotherhalothane vaporiser substituted forisoflurane. Gas samples were drawnfrom the breathing circuit through atube attached to an adapter positionedbetween the Y-piece connection andthe oral end of the endotracheal tube.The end-tidal anesthetic concentra-tions were measured continuouslyusing infrared gas analysers (halo-thane: RI-507M, Riken Keiki FineInstrument Co., Tokyo, Japan; isoflu-rane and sevoflurane: Capnomac,Datex, Helsinki, Finland). Airway gaswas continuously sampled at the rateof 200 mL/min and the gas was notreturned to the circuit. Anesthesia wasinduced with 4% halothane (HoechstJapan, Tokyo), 4% isoflurane (Forane,Dinabott, Osaka), or 5% sevoflurane(Sevofrane, Maruishi PharmaceuticalCo., Osaka) in oxygen, at a total gasflow rate of 1.5 L/min using a facemask attached to a circle anestheticsystem (Beaver 20, Kimura Med.,Tokyo). After induction of anesthesia,a cuffed endotracheal tube wasinserted and the cuff was inflated. Thegoats were placed in right lateralrecumbency and ventilated mechani-cally to maintain at an arterial carbondioxide pressure level of 35 ±5 mmHg. Blood samples for gas anal-ysis were collected from a polyethy-lene 22-gauge catheter inserted intothe auricular artery. After an end-tidalanesthetic concentration of approxi-mately 1 MAC, based on dogs asavailable reference (3), was adminis-tered for 15 min, the tail was clampedwith a Kocher's forcep for 45 s. Theinitial values were for 0.9% for halo-thane, 1.3% for isoflurane, and 2.3%for sevoflurane. A positive responseto this painful stimulus was defined asgross purposeful muscular movementof the head or extremities. If the ani-mal showed a positive response to thestimulus, the end-tidal concentrationwas increased by 10%; if the animaldid not show a positive response, theconcentration was decreased by 10%.The painful stimulus was repeated at15-minute intervals until at least twocross-over pairs of positive/negativeresponses were obtained. The MACwas defined as the average of the end-tidal anesthetic concentrations of thepositive/negative responses.
In the spontaneous ventilation (SV)experiment, 6 goats (5 males, 1female) were an anesthetized repeatedlyat 2-week intervals with halothane,isoflurane or sevoflurane in random-ized order. In the controlled ventila-tion (CV) experiment, 6 male goatswere also anesthetized repeatedly at2-week intervals in randomized order.Pre-anesthetic values for heart rate(HR), respiration rate (RR) and arte-rial blood gases were obtained withthe goat resting in a room 15 to30 min before induction of anesthesia.In both experiments anesthesia wasinduced as described above. After acuffed endotracheal tube was inserted,goats were placed in right lateralrecumbency and maintained at a sur-gical plane of anesthesia while breath-ing spontaneously. For arterial pres-sure monitoring and blood gassampling, a polyethylene 20-gaugecatheter was inserted into the skinloop of left jugular artery preparedpreviously. Electrocardiogram (ECG)electrodes were placed at the Apex-Base. A Swan-Ganz catheter (7-French)was inserted through the jugular vein,passed into the right ventricle andadvanced into the pulmonary artery.These preparations for cardiopul-monary measurements were com-pleted 25-35 min after induction ofanesthesia. Subsequently, the goatswere kept at end-tidal concentrationsequivalent to 1 MAC of each anes-thetic as determined in the first phaseof this study. Cardiopulmonary vari-ables were recorded during either SVor CV after 15 min stabilization. Theend-tidal anesthetic concentration wasthen increased from 1 to 1.5 MAC,and from 1.5 to 2 MAC. After 15 minat each anesthetic level, cardiopul-monary variables were recorded. Dur-ing SV, each anesthesia was main-tained at oxygen flow rate of1.5 L/min using a circle anestheticsystem.
CARDIOPULMONARY MEASUREMENTS
At each anesthetic level, systolicand diastolic arterial blood pressures(SAP and DAP) were measuredthrough the arterial catheter. Themean arterial blood pressure (MAP)was calculated as DAP + 1/3 pulsepressure (SAP-DAP). Mean rightatrial pressure (MRAP), mean pul-monary arterial pressure (MPAP), andpulmonary capillary wedge pressure
300
(PCWP) were measured through theSwan-Gantz catheter. These pressureswere measured using pressure trans-ducers placed at the heart level and amulti-channel polygraph (RM-6100,Nihon Koden, Japan). A lead Apex-Base ECG was recorded to monitorheart rate and heart rhythm. Cardiacoutput (CO) was determined by thethermodilution technique with aninjection of 5% glucose solution(5 mL, 0°C) into the right atrium dur-ing the expiratory phase of ventila-tion. The cardiovascular variables cal-culated from above values were asfollows: cardiac index (CI) = CO/body weight (kg); stroke volumeindex (SVI) = CI X 1000/HR; sys-temic vascular resistance (SVR) =(MAP-MRAP)/CI; rate pressure prod-uct (RPP) = HR X SAP; pulmonaryvascular resistance (PVR) = (MPAP-PCWP)/CI; left ventricular minutework index (LVMWI) = CI X (MAP-PAWP) X 13.6; left ventricular strokework index (LVSWI) = SVI X (MAP-PAWP) X 0.0136; right ventricularminute work index (RVMWI) = CI X(MPAP-MRAP) X 13.6; and rightventricular stroke work index(RVSWI) = SVI X (MPAP-MRAP)x 0.0136.The RR was measured by counting
movements of the thorax or the re-breathing bag. Respiratory tidal vol-ume (TV) was measured using arespirometer (Ohmeda RM 121,Japan) placed between the breathinghose and the endotracheal tube andminute ventilation (MV) was calcu-lated. Arterial blood samples weretaken anaerobically into heparinizedsyringes. The volume of blood drawnfor each blood gas analysis was0.3 mL. Arterial oxygen and carbondioxide partial pressures (PaO2 andPaCO2, respectively) and arterial pH(pHa) were measured with a blood gasanalyser (Blood Gas System 278,Ciba Corning Diagnostic Corp.,Tokyo) at 37°C and corrected for eachgoat's rectal temperature. The arterialbicarbonate ([HCO3-]a) and baseexcess (BEa) were derived using stan-dard formulae (20). All measurementsand arterial blood sampling were per-formed at the end of the 15-minutemaintenance period at each anestheticlevel. The PaCO2 during CV wasmaintained between 30 and 40 mmHgby adjustment of respiratory fre-quency (10 to 15/min) at a constant
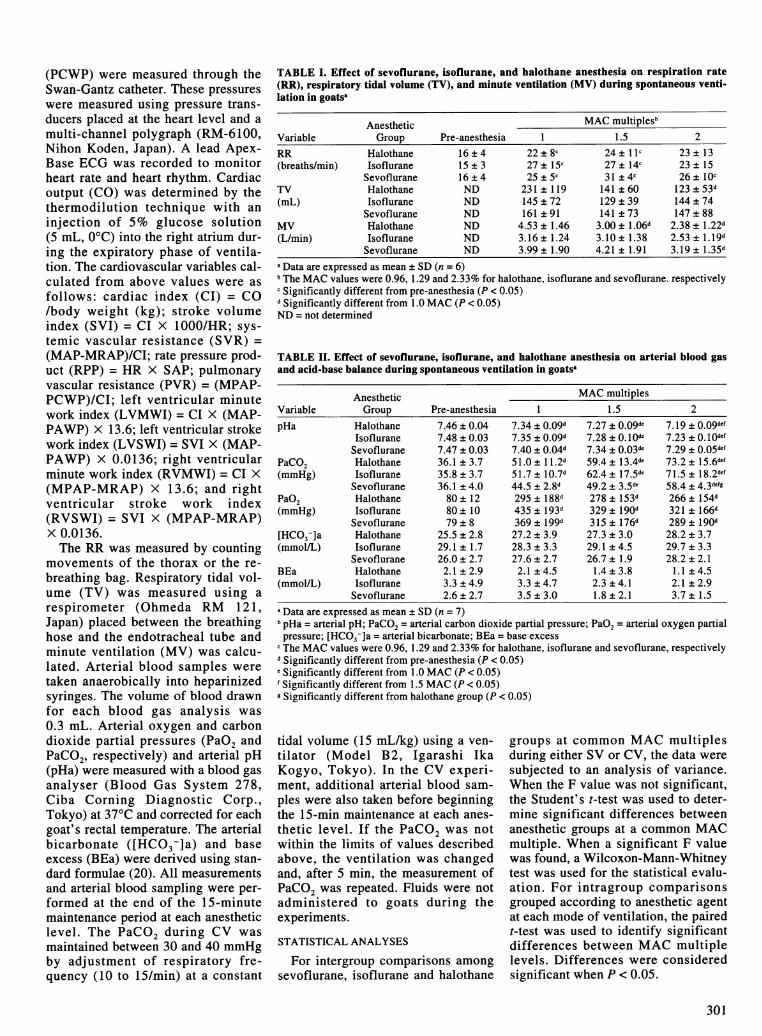
TABLE I. Effect of sevoflurane, isoflurane, and halothane anesthesia on respiration rate(RR), respiratory tidal volume (TV), and minute ventilation (MV) during spontaneous venti-lation in goatsa
Anesthetic MAC multiplesbVariable Group Pre-anesthesia 1 1.5 2
RR Halothane 16 + 4 22 ± 8c 24± llc 23 ± 13(breaths/min) Isoflurane 15 ± 3 27 ± 15c 27 ± 14c 23 ± 15
Sevoflurane 16 ± 4 25 ± 5c 31 ± 4c 26 ± 10cTV Halothane ND 231 ± 119 141 ± 60 123 ± 53d(mL) Isoflurane ND 145 ± 72 129 ± 39 144 ± 74
Sevoflurane ND 161 ± 91 141 ± 73 147 ± 88MV Halothane ND 4.53 ± 1.46 3.00 ± 1.06d 2.38 ± 1.22d(L/min) Isoflurane ND 3.16 ± 1.24 3.10 ± 1.38 2.53 ± J.19d
Sevoflurane ND 3.99 ± 1.90 4.21 ± 1.91 3.19 ± 1.35da Data are expressed as mean ± SD (n = 6)b The MAC values were 0.96, 1.29 and 2.33% for halothane, isoflurane and sevoflurane. respectivelyc Significantly different from pre-anesthesia (P < 0.05)d Significantly different from 1.0 MAC (P < 0.05)ND = not determined
TABLE II. Effect of sevoflurane, isoflurane, and halothane anesthesia on arterial blood gasand acid-base balance during spontaneous ventilation in goatsa
Anesthetic MAC multiplesVariable Group Pre-anesthesia 1 1.5 2
pHa Halothane 7.46 ± 0.04 7.34 ± 0.09d 7.27 ± O.09de 7.19 ± 0.09defIsoflurane 7.48 ± 0.03 7.35 ± 0.09d 7.28 ±0.IOde 7.23 ± 0.1OdefSevoflurane 7.47 ± 0.03 7.40 ± 0.04d 7.34 ± 0.03de 7.29 ± O.05def
PaCO2 Halothane 36.1 ±3.7 51.0±11.2d 59.4±13.4de 73.2 ±15.6def(mmHg) Isoflurane 35.8 ± 3.7 51.7 ± 10.7d 62.4 ± 17.5de 71.5 ± 18.2def
Sevoflurane 36.1 ± 4.0 44.5 ± 2.8d 49.2 ± 3.5de 58.4 ± 4.3defgPaO2 Halothane 80 ± 12 295 ± 188d 278 ± 153d 266 ± 154d(mmHg) Isoflurane 80 ± 10 435 ± 193d 329 ± 190d 321 ± 166d
Sevoflurane 79 ± 8 369 ± 199d 315 ± 176d 289 ± 190d[HCO3-]a Halothane 25.5 ± 2.8 27.2 ± 3.9 27.3 ± 3.0 28.2 ± 3.7(mmol/L) Isoflurane 29.1 ± 1.7 28.3 ± 3.3 29.1 ± 4.5 29.7 ± 3.3
Sevoflurane 26.0 ± 2.7 27.6 ± 2.7 26.7 ± 1.9 28.2 ± 2.1BEa Halothane 2.1 ± 2.9 2.1 ± 4.5 1.4 ± 3.8 1.1 ± 4.5(mmol/L) Isoflurane 3.3 ± 4.9 3.3 ± 4.7 2.3 ± 4.1 2.1 ± 2.9
Sevoflurane 2.6 ± 2.7 3.5 ± 3.0 1.8 ± 2.1 3.7 ± 1.5a Data are expressed as mean ± SD (n = 7)b pHa = arterial pH; PaCO2 = arterial carbon dioxide partial pressure; PaO2 = arterial oxygen partialpressure; [HCO3j]a = arterial bicarbonate; BEa = base excess
c The MAC values were 0.96, 1.29 and 2.33% for halothane, isoflurane and sevoflurane, respectivelyd Significantly different from pre-anesthesia (P < 0.05)e Significantly different from 1.0 MAC (P < 0.05)f Significantly different from 1.5 MAC (P < 0.05)g Significantly different from halothane group (P < 0.05)
tidal volume (15 mL/kg) using a ven-tilator (Model B2, Igarashi IkaKogyo, Tokyo). In the CV experi-ment, additional arterial blood sam-ples were also taken before beginningthe 15-min maintenance at each anes-thetic level. If the PaCO2 was notwithin the limits of values describedabove, the ventilation was changedand, after 5 min, the measurement ofPaCO2 was repeated. Fluids were notadministered to goats during theexperiments.
STATISTICAL ANALYSES
For intergroup comparisons amongsevoflurane, isoflurane and halothane
groups at common MAC multiplesduring either SV or CV, the data weresubjected to an analysis of variance.When the F value was not significant,the Student's t-test was used to deter-mine significant differences betweenanesthetic groups at a common MACmultiple. When a significant F valuewas found, a Wilcoxon-Mann-Whitneytest was used for the statistical evalu-ation. For intragroup comparisonsgrouped according to anesthetic agentat each mode of ventilation, the pairedt-test was used to identify significantdifferences between MAC multiplelevels. Differences were consideredsignificant when P < 0.05.
301

TABLE III. Cardiovascular effects of sevoflurane, isoflurane, and halothane anesthesia dur-ing spontaneous ventilation in goatsa
Anesthetic MAC multiplescVariableb Group Pre-anesthesia 1 1.5 2
HR Halothane 93 ±14 109 ± 8 118 ± 13 115 ± 12(beats/min) Isoflurane 95 ± 21 118 ± 9 116 ± 13 109 ± 13
Sevoflurane 86±9 113 ± lld 111 ± 17 104± 15MAP Halothane 101 ± 14 91 ± 15e 76 ± lOef(mmHg) Isoflurane 98 ± 17 79 ± 24e 65 ± 13e
Sevoflurane 104 ± 15 86 ± 16e 79 ± 17eCI Halothane 0.11 ± 0.03 0.12±0.03 0.11 ±0.03(L/min/kg) Isoflurane 0.15 ± 0.0 0.15 ± 0.04 0.13 ± 0.0
Sevoflurane 0.12 ± 0.03 0.11 ± 0.03 0.10 ± 0.03SVI Halothane 1.04 ± 0.25 1.01 ± 0.26 0.97 ± 0.30(mL/kg) Isoflurane 1.26 ± 0.33 1.26 ± 0.39 1.16 ± 0.32
Sevoflurane 1.07 ± 0.32 0.98 ± 0.33 0.95 ± 0.31RPP Halothane 13598 ± 2291 13987 ± 3822 12215 ± 31401(mmHg.beat/min) Isoflurane 14546 ± 3397 12678 ± 4273 9983 ± 2887ef
Sevoflurane 15046 ± 2972 12570 ± 3867e 11397 ± 3845eMPAP Halothane 14.4 ± 4.8 16.4 ± 2.7 15.4 ± 2.0(mmHg) Isoflurane 13.5 ± 3.6 13.8 ± 3.7 16.2 ± 6.0
Sevoflurane 16.1 ± 6.8 15.8 ± 6.9 16.0 ± 7.9SVR Halothane 959 ±384 824 ±359 721 ± 277e(mmHg.L/min/kg) Isoflurane 682 ± 228 564 ± 224e 523 ± 154e
Sevoflurane 902 ±265 852 ±331 820± 275ehPVR Halothane 89.7 ± 51.7 84.0 ± 31.7 80.7 ± 31.3(mmHg.L/min/kg) Isoflurane 58.3 ± 17.8 49.5 ± 17.O8 61.3 ± 24.9
Sevoflurane 72.8 ± 57.6 82.0 ± 70.9 83.7 ± 78.8LVMWI Halothane 146 ± 44 133 ± 31 103 ± 34ef(g-mnkg/min) Isoflurane 194 ± 76 147 ± 67e 104 ± 52e'
Sevoflurane 154 ±46 111 ± 45e 97 ± 39eLVSWI Halothane 1.36 ± 0.34 1.14 ± 0.26 0.91 ± 0.29e(g.m/kg) Isoflurane 1.62 ± 0.59 1.23 ± 0.49e 0.95 ± 0.45ef
Sevoflurane 1.37 ± 0.44 1.02 ± 0.41e 0.90 ± 0.31eRVMWI Halothane 17.0 ± 6.8 19.7 ± 4.9 18.0 ± 6.6(g.m/kg/min) Isoflurane 20.7 ± 7.8 19.2 ± 7.2 24.1 ± 18.8
Sevoflurane 20.5 ± 6.3 17.4 ± 9.0 16.6 ± 8.4RVSWI Halothane 0.16 ± 0.07 0.17 ± 0.05 0.16 ± 0.06(g.m/kg) Isoflurane 0.18 ± 0.06 0.16 ± 0.05 0.21 ± 0.16
Sevoflurane 0.18 ± 0.06 0.17 ± 0.10 0.16 ± 0.08a Data are expressed as mean ± SD (n = 6)b HR = heart rate; MAP = mean arterial blood pressure; CI = cardiac index; SVI = stroke volumeindex; RPP = rate pressure product; MPAP = mean pulmonary arterial pressure; SVR = systemicvascular resistance; PVR = pulmonary vascular resistance; LVMWI = left ventricular minutework index; LVSWI = left ventricular stroke work index; RVMWI = right ventricular minutework index; RVSWI = right ventricular stroke work index
c The MAC values were 0.96, 1.29 and 2.33% for halothane, isoflurane and sevoflurane, respectivelyd Significantly different from pre-anesthesia (P < 0.05)e Significantly different from 1.0 MAC (P < 0.05)f Significantly different from 1.5 MAC (P < 0.05)9 Significantly different from halothane group (P < 0.05)h Significantly different from isoflurane group (P < 0.05)
RESULTS
MAC OF SEVOFLURANE, ISOFLURANE,AND HALOTHANE
The MAC values (mean ± SD) were0.96 ± 0.12% for halothane, 1.29 +0.11% for isoflurane, and 2.33 +0.15% for sevoflurane. There weresignificant differences between thegroups in MAC values.
PULMONARY FINDINGS DURING SV
The RR, TV and MV values areshown in Table I. Sevoflurane,halothane and isoflurane at each MACmultiple caused a significant increased
in RR when compared with pre-anesthesia values. The TV in thehalothane group decreased signifi-cantly at 2 MAC multiple when com-pared with 1 MAC. The MV in halo-thane group decreased significantlywith the increase in the anestheticconcentration. The MV in sevofluraneand isoflurane groups decreased sig-nificantly at 2 MAC multiple whencompared with 1 MAC. However,there were no significant differencesin RR, TV and MV among any of thegroups at equipotent MAC multiples.Respiratory arrest did not occur in anygoat.
Blood gases and acid-base variablesare summarized in Table II. All anes-thetics induced significant increasesin PaCO2 and significant decreases inpHa with increasing inhalant concen-tration. Both PaCO2 and pHa levels inisoflurane group were very similar tothose in halothane group at equipotentMAC multiples. The PaCO2 at 2 MACin sevoflurane group was significantlylower than that in halothane group.The PaO2 in all groups increased
significantly at each MAC multiplewhen compared with pre-anesthesiavalues, but there was no significantdifference in PaO2 among any of thegroups at each MAC multiple. Both[HCO3-]a and BEa at each MAC mul-tiple in all groups did not significantlychange from pre-anesthesia values.There was no significant difference ineither [HCO3-]a or BEa among any ofthe groups at equipotent MAC multiples.
CARDIOVASCULAR FINDINGS DURING SV
The results are summarized inTable III. The HR in all groups tendedto be higher at each MAC multiplewhen compared to pre-anesthetic val-ues, but there was no significant dif-ference in HR among any of thegroups at equipotent MAC multiples.No arrhythmias were observed in anygroup.The MAP, RPP, SVR, LVMWI and
LVSWI in all groups decreased sig-nificantly with increasing anestheticconcentration. However, CI, SVI,PVR, MPAP, RVMWI and RVSWI inall groups did not significantly changewith increasing anesthetic concentra-tions from 1 to 2 MAC multiples. TheMAP, RPP, SVR, PVR, LVMWI andLVSWI at each MAC multiple ofsevoflurane were very similar to thoseof halothane. The MAP in isofluranegroup tended to be lower than that inother groups at 1.5 to 2 MAC multi-ples, but not significantly. The SVRin isoflurane group tended to be lowerthan that in other groups at each MACmultiple, and was significantly lowerthan that in sevoflurane group at2 MAC multiple. There were no sig-nificant differences in CI, SVI, RPP,MPAP, LVMWI, LVSWI, RVMWIand RVSWI among any of the groupsat equipotent MAC multiples.
CARDIOVASCULAR FINDINGS DURING CV
The results are summarized inTable IV. The HR in all groups was
302
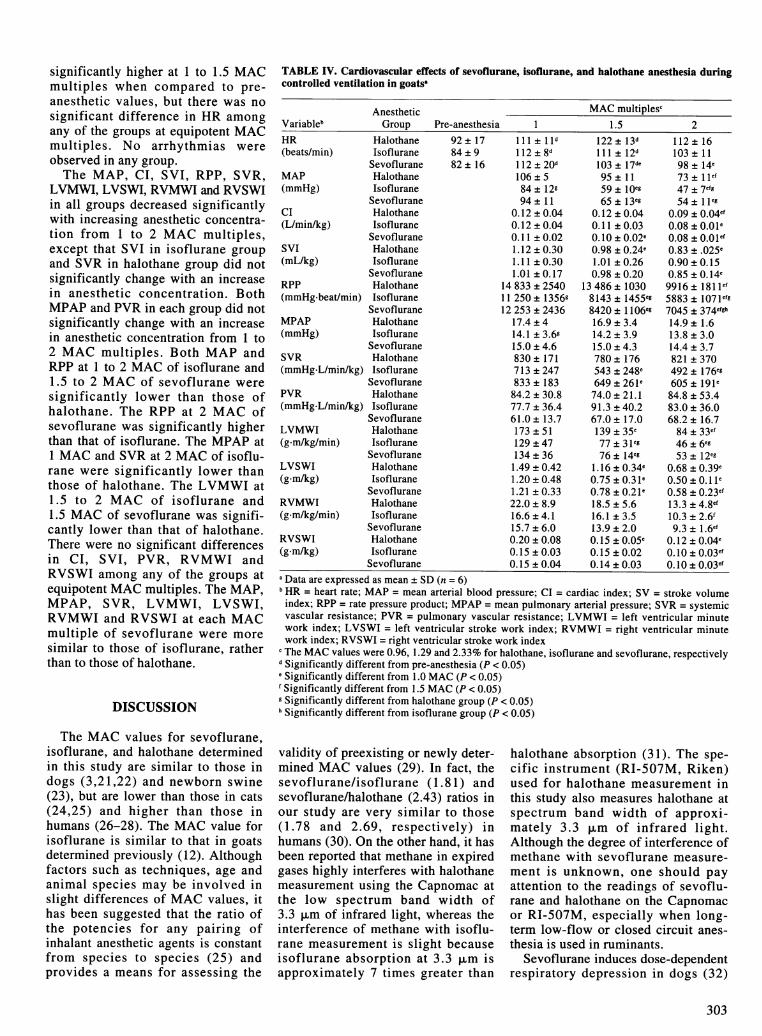
significantly higher at 1 to 1.5 MACmultiples when compared to pre-anesthetic values, but there was nosignificant difference in HR amongany of the groups at equipotent MACmultiples. No arrhythmias wereobserved in any group.The MAP, CI, SVI, RPP, SVR,
LVMWI, LVSWI, RVMWI and RVSWIin all groups decreased significantlywith increasing anesthetic concentra-tion from 1 to 2 MAC multiples,except that SVI in isoflurane groupand SVR in halothane group did notsignificantly change with an increasein anesthetic concentration. BothMPAP and PVR in each group did notsignificantly change with an increasein anesthetic concentration from 1 to2 MAC multiples. Both MAP andRPP at 1 to 2 MAC of isoflurane and1.5 to 2 MAC of sevoflurane weresignificantly lower than those ofhalothane. The RPP at 2 MAC ofsevoflurane was significantly higherthan that of isoflurane. The MPAP at1 MAC and SVR at 2 MAC of isoflu-rane were significantly lower thanthose of halothane. The LVMWI at1.5 to 2 MAC of isoflurane and1.5 MAC of sevoflurane was signifi-cantly lower than that of halothane.There were no significant differencesin CI, SVI, PVR, RVMWI andRVSWI among any of the groups atequipotent MAC multiples. The MAP,MPAP, SVR, LVMWI, LVSWI,RVMWI and RVSWI at each MACmultiple of sevoflurane were moresimilar to those of isoflurane, ratherthan to those of halothane.
DISCUSSION
TABLE IV. Cardiovascular effects of sevoflurane, isoflurane, and halothane anesthesia duringcontrolled ventilation in goatsa
AnestheticVariableb GroupHR Halothane(beats/min) Isoflurane
SevofluraneMAP Halothane(mmHg) Isoflurane
SevofluraneCI Halothane(L/min/kg) Isoflurane
SevofluraneSVI Halothane(mL/kg) Isoflurane
SevofluraneRPP Halothane(mmHg-beat/min) Isoflurane
SevofluraneMPAP Halothane(mmHg) Isoflurane
SevofluraneSVR Halothane(mmHg-L/min/kg) Isoflurane
SevofluranePVR Halothane(mmHg.L/min/kg) Isoflurane
SevofluraneLVMWI Halothane(gnm/kg/min) Isoflurane
SevofluraneLVSWI Halothane(g.m/kg) Isoflurane
SevofluraneRVMWI Halothane(g.m/kg/min) Isoflurane
SevofluraneRVSWI Halothane(g.m/kg) Isoflurane
Sevoflurane
Pre-anesthesia 192 ± 17 111±+1 ld84 ± 9 112 ± 8d82 ± 16 112 ± 20d
106 ± 584 ± 12g94± 11
0.12 ± 0.040.12 ± 0.040.11 ± 0.021.12 ± 0.301.11 ± 0.301.01 ±0.17
14 833 ± 254011 250 ± 1356g12 253 ± 2436
17.4 ± 414.1 ± 3.6g15.0 ± 4.6830 ± 171713 ± 247833 ± 18384.2 ± 30.877.7 ± 36.461.0 ± 13.7173 ± 51129 ± 47134 ± 361.49 ± 0.421.20 ± 0.481.21 ± 0.3322.0 ± 8.916.6 ± 4.115.7 ± 6.00.20 ± 0.080.15 ± 0.030.15 ± 0.04
MAC multiplesc1.5 2
122 ± 13d 112 ± 16111 ± 12d 103 ± 11103 ± 17de 98 ± 14e95 ± 11 73 ± l lef59± IOeg 47 ± 7efg65±13eg 54±18eg
0.12 ± 0.04 0.09 ± 0.04ef0.11 ± 0.03 0.08 ±0.Ole0.10 ± 0.02e 0.08 ± 0.OIef0.98 ± 0.24e 0.83 ± .025e1.01 ± 0.26 0.90±0.150.98 ± 0.20 0.85 ± 0.14e
13 486 ± 1030 9916 ± 1811"e8143 ± 1455eg 5883 ± 107 1efg8420 ± 1106eg 7045 ± 374efgh16.9 ± 3.4 14.9 ± 1.614.2±3.9 13.8±3.015.0±4.3 14.4±3.7780 ± 176 821 ± 370543 ± 248e 492 ± 176eg649 ± 261e 605 ± l91e74.0±21.1 84.8±53.491.3 ± 40.2 83.0 ± 36.067.0 ± 17.0 68.2 ± 16.7139±35e 84±33ef77 ± 31eg 46+ 6eg76 ± 14eg 53 + 12eg
1.16 ± 0.34e 0.68 ± 0.39e0.75 ± 0.31e 0.50 ± 0. l le0.78 ± 0.21e 0.58 ± 0.23ef18.5 ± 5.6 13.3 ± 4.8ef16.1 ± 3.5 10.3 ± 2.6113.9 ± 2.0 9.3 ± 1.6e'0.15 ± 0.05e 0.12 ± 0.04e0.15 ± 0.02 0.10 ± 0.03ef0.14 ± 0.03 0.10± 0.03ef
a Data are expressed as mean ± SD (n = 6)bHR = heart rate; MAP = mean arterial blood pressure; CI = cardiac index; SV = stroke volumeindex; RPP = rate pressure product; MPAP = mean pulmonary arterial pressure; SVR = systemicvascular resistance; PVR = pulmonary vascular resistance; LVMWI = left ventricular minutework index; LVSWI = left ventricular stroke work index; RVMWI = right ventricular minutework index; RVSWI = right ventricular stroke work index
c The MAC values were 0.96, 1.29 and 2.33% for halothane, isoflurane and sevoflurane, respectivelydSignificantly different from pre-anesthesia (P < 0.05)eSignificantly different from 1.0 MAC (P < 0.05)f Significantly different from 1.5 MAC (P < 0.05)9 Significantly different from halothane group (P < 0.05)Significantly different from isoflurane group (P < 0.05)
The MAC values for sevoflurane,isoflurane, and halothane determinedin this study are similar to those indogs (3,21,22) and newborn swine(23), but are lower than those in cats(24,25) and higher than those inhumans (26-28). The MAC value forisoflurane is similar to that in goatsdetermined previously (12). Althoughfactors such as techniques, age andanimal species may be involved inslight differences of MAC values, ithas been suggested that the ratio ofthe potencies for any pairing ofinhalant anesthetic agents is constantfrom species to species (25) andprovides a means for assessing the
validity of preexisting or newly deter-mined MAC values (29). In fact, thesevoflurane/isoflurane (1.81) andsevoflurane/halothane (2.43) ratios inour study are very similar to those(1.78 and 2.69, respectively) inhumans (30). On the other hand, it hasbeen reported that methane in expiredgases highly interferes with halothanemeasurement using the Capnomac atthe low spectrum band width of3.3 ,um of infrared light, whereas theinterference of methane with isoflu-rane measurement is slight becauseisoflurane absorption at 3.3 ,um isapproximately 7 times greater than
halothane absorption (31). The spe-cific instrument (RI-507M, Riken)used for halothane measurement inthis study also measures halothane atspectrum band width of approxi-mately 3.3 ,um of infrared light.Although the degree of interference ofmethane with sevoflurane measure-ment is unknown, one should payattention to the readings of sevoflu-rane and halothane on the Capnomacor RI-507M, especially when long-term low-flow or closed circuit anes-thesia is used in ruminants.
Sevoflurane induces dose-dependentrespiratory depression in dogs (32)
303

and humans (33). The RR in dogs at1.5 to 2 MAC multiples with sevoflu-rane is reportedly lower than that withhalothane (32). The present findingsin goats revealed that sevoflurane,isoflurane and halothane increasedRR at 1 to 2 MAC multiples whencompared with pre-anesthesia duringSV, but RR with sevoflurane does notdiffer from that with both halothaneand isoflurane. The TV and MV withsevoflurane did not significantly dif-fer from those with either halothaneor isoflurane at each MAC multiple;however, a dose-dependent decreasein both TV and MV from 1 to 2 MACmultiples with halothane tended to begreater than that with either sevoflu-rane or isoflurane. This study alsorevealed that the 3 anesthetics pro-duced a dose-dependent respiratoryacidosis (increase in PaCO2 anddecrease in pHa), and that the degreeof respiratory acidosis induced bysevoflurane did not differ from thatinduced by either isoflurane orhalothane at 1 to 1.5 MAC multiples,but was less than that induced byhalothane at 2 MAC multiples. There-fore, the present findings in goatsindicate that sevoflurane induces res-piratory depression which is less thanthat induced by halothane at higherconcentrations. In dogs, the degree ofhypercapnia induced by sevofluranedoes not differ from that induced byhalothane (32), whereas the hypercap-nia with isoflurane at 1.5 MAC multi-ple is greater than that with halothane(34). However, previous studies incats have shown that the degree ofhypercapnia and acidosis with halo-thane is greater than with isoflurane(21,35). These findings in dogs andcats somewhat differ from thoseobtained in goats. In the presentstudy, the PaCO2 during SV with allanesthetics is higher than thatreported previously in dogs (21,32),cats (35,36), and humans (33). Inruminants, distension of the rumendue to increasing ruminal gasesimpairs the ventilation (37), and posi-tioning in lateral recumbency is asso-ciated with respiratory depression(38). These factors may be involvedin profound hypercapnia during anes-thesia in this study. Furthermore, theincreased RR with all anesthetics inthis study might be in part due to pro-found hypercapnia, because centraland peripheral chemoreceptors respond-
ing to increases in PaCO2 can causean increase in RR.As we studied in an order of an
increasing MAC multiples, asopposed to randomizing the order, anorder effect on cardiopulmonary mea-surements might have occurred, espe-cially during SV. It was reported indogs that respiratory function was lit-tle changed for as long as 7 h of con-stant 1.2 MAC halothane anesthesia,but that a time-related progressiverise in PaCO2 occurred at constant1.7 MAC halothane anesthesia (39).The time-related increase in PaCO2was also reported to occur during 5 hof constant 1.2 MAC halothane orisoflurane anesthesia in laterallyrecumbent, spontaneously breathinghorses (40,41), although the PaCO2did not significantly change for aslong as 1 h of constant-dose anesthe-sia. In humans, it was reported thatrespiratory depression remainedunchanged for as long as 3 h of con-stant-depth halothane anesthesia andthereafter ventilation tended to beimproved (42). In our study, there-fore, the duration of anesthesia at 1.5to 2.0 MAC multiple of each anes-thetic might have somewhat influ-enced the rise in PaCO2. In addition,the maintenance and replacement flu-ids were not administered intra-venously during anesthesia in thisstudy. This might have also influ-enced the cardiopulmonary data ofthis study, particularly at a high MACmultiple.The HR is unchanged or decreased
slightly as sevoflurane concentrationincreased in dogs (4,43) and pigs (2),however, it is also reported toincrease in dogs (44,45). Isofluranehas been reported to induce a slightincrease HR in dogs (44-46).Halothane does not significantly alterHR at 1 to 2 MAC multiples in dogs(45). On the other hand, halothane,isoflurane and sevoflurane decreaseHR at 0.5 to 1.5 MAC multiples com-pared to the awake HR in newbornswine (23). The present findingsrevealed that the three anesthetics sig-nificantly increased or tended toincrease HR at 1 to 1.5 MAC multi-ples when compared to pre-anestheticvalues during both SV and CV, butthere was no significant difference inHR among the three anesthetics atequipotent MAC multiples. There-fore, the present findings indicate that
sevoflurane produces a stable HRsimilar to both isoflurane andhalothane in goats.
Sevoflurane produces a dose-dependent decrease in arterial bloodpressure (AP), cardiac output, leftventricular work and peripheral vas-cular resistance in dogs (4,43-45) andpigs (2). Halothane induces a dose-dependent decrease in AP and cardiacoutput, but has little effect on totalperipheral resistance in dogs (21) andcats (35,47,48). In contrast, isofluranecauses a greater fall in peripheral vas-cular resistance with a decrease in APand a smaller decrease in cardiac out-put in dogs and cats (21,22). In chron-ically instrumented dogs the haemo-dynamic properties of sevoflurane arealmost identical to those of isoflurane,and the vasodilatory action ofsevoflurane is more comparable tothat of isoflurane than halothane(44,45). The present findings in goatsrevealed that the three anestheticsinduced dose-dependent decreases inMAP, RPP, SVR, LVMWI andLVSWI during SV, and that these cir-culatory changes with sevofluranewere similar to those with halothanerather than isoflurane. The SVR athigher MAC multiples was lower inisoflurane than sevoflurane duringSV. On the other hand, the presentfindings revealed that the three anes-thetics induced dose-dependentdecreases in MAP, CI, SVI, RPP,SVR, LVMWI, LVSWI, RVMWI andRVSWI during CV, except that SVIof isoflurane and SVR of halothanedid not significantly change from 1 to2 MAC multiples. Our results furtherrevealed that circulatory depressionduring CV by sevoflurane was similarto those of isoflurane rather thanhalothane, and MAP and SVR athigher MAC multiples of eitherisoflurane or sevoflurane were signifi-cantly lower than those of halothaneduring CV. Therefore, during CV,hemodynamic properties of sevoflu-rane are almost identical to those ofisoflurane, and the vasodilatory actionof sevoflurane is more comparable tothat of isoflurane than halothane ingoats. Halothane induces circulatorydepression without a significant effecton total peripheral resistance duringCV in goats.Some of the cardiovascular depres-
sion such as MAP, CI and LVMWIwere greater under conditions of CV
304

than SV in this study. As artificialventilation with positive pressurereduces venous return to the heart byraising intrathoracic pressure, result-ing in decreases in mean arterial pres-sure and cardiac output (49,50), theseeffects may be involved in a great car-diovascular depression in the CV ofthis study. On the other hand, it maybe possible that the differencebetween CV and SV found in ourstudy is in part due to the effect ofhypercapnia, because carbon dioxideis a direct cardiac depressant andvasodilator, but it causes indirect car-diovascular stimulation via the sym-pathetic nervous system (51). How-ever, in this study, there was nosignificant difference in HR betweenSV and CV. The decrease in sympa-thetic activity such as depression ofganglionic transmission and centralsympathetic depression occurs duringhalothane anesthesia (52,53). There-fore, indirect cardiovascular stimula-tion via the sympathetic nervous sys-tem by hypercapnia may not beresponsible for the differences in car-diovascular responses between CVand SV in this study. Furthermore, inthis study, SVR with halothane anes-thesia did not significantly changefrom 1 to 2 MAC multiples duringCV, whereas it decreased signifi-cantly at 2 MAC multiple comparedto 1 MAC multiple during SV.Although the precise mechanism ofthis difference is unknown, combinedeffects of both the depression of sym-pathetic activity by halothane and theperipheral vasodilation by hypercap-nia may be involved in the decrease inSVR induced by halothane at 2 MACmultiple during SV in this study.
In conclusion, the present findingsindicate that respiratory depressioninduced by sevoflurane is less thanthat induced by halothane in goats.Furthermore, sevoflurane producesheart rate similar to both halothaneand isoflurane, and it causes circula-tory depression similar to isofluranerather than halothane during CV.
ACKNOWLEDGMENTS
The authors thank Maruishi Phar-maceutical Co., Ltd. for the gift of sevo-flurane, and Mr. Satoru Hokushin,Mr. Shigenori Satoh and Miss YukoSuzuyama for their technical assistance.
REFERENCES
1. STRUM DP, EGER El II. Partition coef-ficients for sevoflurane in human blood,saline, and olive oil. Anesth Analg 1987;66: 654-656.
2. MANOHAR M, PARKS CM. Porcinesystemic and regional organ blood flowduring 1.0 and 1.5 minimum alveolar con-centrations of sevoflurane anaesthesiawithout and with 50 per cent nitrous oxide.J Pharmacol Exp Ther 1984; 231:640-648.
3. KAZAMA T, IKEDA K. Comparison ofMAC and the rate of rise of alveolar con-
centration of sevoflurane with halothaneand isoflurane in the dog. Anesthesiology1988; 68:435-437.
4. KAZAMA T, IKEDA K. The comparativecardiovascular effects of sevoflurane withhalothane and isoflurane. J Anesth 1988;2: 63-68.
5. EGER EI II, JOHNSON BH. Rate ofawakening from anesthesia with I-653,halothane, isoflurane, and sevoflurane: atest of the effect of anesthetic concentra-tion and duration in rats. Anesth Analg1987; 66: 977-982.
6. HIKASA Y, KAWANABE H, TAKASEK, OGASAWARA S. Comparisons ofsevoflurane, isoflurane, and halothaneanesthesia in spontaneously breathing cats.Vet Surg 1996; 25: 234-243.
7. HIKASA Y, YOSHIKAI T, TAKASE K,OGASAWARA S. Comparison of pro-longed sevoflurane, isoflurane, andhalothane anaesthesia combined withnitrous oxide in spontaneously breathingcats. J Vet Med A 1997; 44: 427-442.
8. WALLIN RF, REGAN BM, NAPOLIMD, STERN IJ. Sevoflurane: a new
inhalational anesthetic agent. AnesthAnalg 1975; 54: 758-766.
9. IMAMURA S, IKEDA K. Comparison ofthe epinephrine-induced arrhythmogeniceffect of sevoflurane with isoflurane andhalothane. J Anesth 1987; 1: 62-68.
10. HAYASHI Y, SUMIKAWA K,TASHIRO C, YAMATODANI A,YOSHIYA I. Arrhythmogenic thresholdof epinephrine during sevoflurane, enflu-rane, and isoflurane anesthesia in dogs.Anesthesiology 1988; 69: 145-147.
11. HIKASA Y, OKABE C, TAKASE K,OGASAWARA S. Ventricular arrhythmo-genic dose of adrenaline during sevoflu-rane, isoflurane, and halothane anaesthesiaeither with or without ketamine andthiopentone in cats. Res Vet Sci 1996; 60:134-137.
12. ANTOGNINI JF, EISELE PH. Anes-thetic potency and cardiopulmonaryeffects of enflurane, halothane, and isoflu-rane in goats. Lab Anim Sci 1993; 43:607-610.
13. STEFFEY EP, HOWLAND D. Halothaneanesthesia in calves. Am J Vet Res 1979;40: 372-376.
14. MATTHEWS NS, GLEED RD, SHORTCE. Cardiopulmonary effects of generalanesthesia in adult cattle. Mod Vet Pract1986; 67: 618-620.
15. BRETT CM, TEITEL DF, HEYMANNMA, RUDOLPH AM. The cardiovascular
effects of isoflurane in lambs. Anesthesiol-ogy 1987; 67: 60-65.
16. GREENE SA, TYNER CL, MORRISDL, HARTSFIELD SM. Comparison ofcardiopulmonary effects of isoflurane andhalothane after atropine-guaifenesin-thiamylal anesthesia for rumenotomy insteers. Am J Vet Res 1988; 49: 1891-1893.
17. SOBTI VK, PRASAD B. Physiologicaleffects of halothane anaesthesia underspontaneous breathing in calves. Acta VetHung 1988; 36: 81-86.
18. HIKASA Y, TAKASE K, KONDOU K,OGASAWARA S. Sevoflurane anesthesiafollowing administration of atropine-guaifenesin-thiopental in spontaneousbreathing adult cattle. J Vet Med Sci 1994;56: 613-616.
19. HIKASA Y, TAKASE K, OGASAWARAS. Sevoflurane and oxygen anaesthesiafollowing administration of atropine-xylazine-guaifenesin-thiopental in sponta-neous breathing horses. J Vet Med A 1994;41: 700-708.
20. SIGGAARD-ANDERSEN 0. Titratableacid or base of body fluids. Annal NewYork Acad Sci 1966; 133: 41-58.
21. STEFFEY EP, HOWLAND D. Isofluranepotency in the dog and cat. Am J Vet Res1977; 38: 1833-1836.
22. STEFFEY EP, HOWLAND D. Potencyof enflurane in dogs: comparison withhalothane and isoflurane. Am J Vet Res1978; 39: 573-577.
23. LERMAN J, OYSTON J, GALLAGHERTM, MIYASAKA K, VOLGYESI GA,BURROWS FA. The minimum alveolarconcentration (MAC) and hemodynamiceffects of halothane, isoflurane, andsevoflurane in newborn swine. Anesthesi-ology 1990; 73: 717-721.
24. DRUMMOND JC, TODD MM, SHAR-PIRO HM. Minimal alveolar concentra-tion for halothane, enflurane, and isoflu-rane in the cat. J Am Vet Med Assoc 1983;182: 1099-1101.
25. DOI M, YUNOKI H, IKEDA K. Theminimum alveolar concentration ofsevoflurane in cats. J Anesth 1988; 2:113-1 14.
26. KATOH T, IKEDA K. The minimal alve-olar concentration of sevoflurane (MAC)in humans. Anesthesiology 1987; 66:301-303.
27. SAIDMAN LJ, EGER El II, MUNSONES, BABAD AA, MUALLEM M.Minimum alveolar concentrations ofmethoxyflurane, halothane, ether andcyclopropane in man: correlation with the-ories of anesthesia. Anesthesiology 1967;28: 994-1002.
28. STEVENS WD, DOLAN WM, GIB-BONS RT, WHITE A, EGER El, MILLERRD, DEJONG RH, ELASHOFF RM.Minimum alveolar concentrations (MAC)of isoflurane with and without nitrousoxide in patients of various ages. Anesthe-siology 1975; 42: 197-200.
29. DRUMMOND JC. MAC for halothane,enflurane, and isoflurane in the NewZealand white rabbit: and a test for thevalidity of MAC determinations. Anesthe-siology 1985; 62: 336-338.
30. SCHELLER MS, SAIDMAN LJ, PAR-TRIDGE BL. MAC of sevoflurane in
305

humans and the New Zealand white rabbit.Can J Anaesth 1988; 35: 153-156.
31. MOENS Y, GOOTJES P, LAGERWEIJE. The influence of methane on theinfrared measurement of halothane in thehorse. J Vet Anaesth 1991; 18: 4-7.
32. DOI M, KATOH T, TAKII T, YURA M,IKEDA K. The respiratory effects ofsevoflurane in dogs. Masui 1987; 36:1053-1057.
33. DOI M, IKEDA K. Respiratory effects ofsevoflurane. Anesth Analg 1987; 66:241-244.
34. HELLEBREKERS LJ. Comparison ofisoflurane and halothane as inhalationanesthetics in the dog. Vet Quart 1986; 8:183-188.
35. GRANDY JL, HODGSON DS, DUN-LOP CI, CURTIS CR, HEATH RB. Car-diopulmonary effects of halothane anes-thesia in cats. Am J Vet Res 1989; 50:1729-1732.
36. HIKASA Y, OHE N, TAKASE K, OGA-SAWARA S. Cardiopulmonary effects ofsevoflurane in cats: comparison withisoflurane, halothane, and enflurane. ResVet Sci 1997; 63: 205-210.
37. UNGERER T, ORR JA, BISGARD GE,WILL JA. Cardiopulmonary effects ofmechanical distension of the rumen innonanesthetized sheep. Am J Vet Res1976; 37: 807-810.
38. FUJIMOTO JL, LENEHAN TM. Theinfluence of body position on the bloodgas and acid-base status of halothane-anesthetized sheep. Vet Surg 1985; 14:169-172.
39. STEFFEY EP, FARVER TB, WOLINERMJ. Cardiopulmonary function during 7 h
of constant-dose halothane and methoxy-flurane. J Appl Physiol 1987; 63:1351-1359.
40. STEFFEY EP, HODGSON DS, DUN-LOP CI, MILLER MF, WOLINER MJ,HEATH RB, GRANDY J. Cardiopul-monary function during 5 hours of con-stant-dose isoflurane in laterally recum-bent, spontaneously breathing horses. JVet Pharmacol Ther 1987; 10: 290-297.
41. STEFFEY EP, KELLY AB, WOLINERMJ. Time-related responses of sponta-neously breathing, laterally recumbenthorses to prolonged anesthesia withhalothane. Am J Vet Res 1987; 48:952-957.
42. FOURCADE HE, LARSON CP JR,HICKEY RF, BAHLMAN SH, EGER EIII. Effects of time on ventilation duringhalothane and cyclopropane anesthesia.Anesthesiology 1972; 36: 83-88.
43. AKAZAWA S, SHIMIZU R, KASUDAH, NEMOTO K, YOSHIZAWA Y,INUE S. Effects of sevoflurane on cardio-vascular dynamics, coronary circulationand myocardial metabolism in dogs. JAnesth 1988; 2: 227-241.
44. BERNARD J-M, WOUTERS PF, DOUR-SOUT M-F, FLORENCE B, CHELLYJE, MERIN RG. Effects of sevofluraneand isoflurane on cardiac and coronarydynamics in chronically instrumenteddogs. Anesthesiology 1990; 72: 659-662.
45. FRINK EJ, MORGAN SE, COETZEEA, CONZEN PF, BROWN BR. Theeffects of sevoflurane, halothane, enflu-rane, and isoflurane on hepatic blood flowand oxygenation in chronically instru-
mented greyhound dogs. Anesthesiology1992; 76: 85-90.
46. KLIDE AM. Cardiopulmonary effects ofenflurane and isoflurane in dogs. Am J VetRes 1976; 37: 127-131.
47. HARTSFIELD SM, SAWYER DC. Car-diopulmonary effects of rebreathing andnonrebreathing systems during halothaneanesthesia in the cat. Am J Vet Res 1976;37: 1461-1466.
48. INGWERSEN W, ALLEN DG, DYSONDH, PASCOE PJ, O'GRANDY MR.Cardiopulmonary effects of a halothane/oxygen combination in healthy cats. Can JVet Res 1988; 52: 386-391.
49. PREWITT RM, WOOD LD. Effect ofpositive end-expiratory pressure on ven-tricular function in dogs. Am J Physiol1979; 236: H534-544.
50. PINSKY MR. The effects of mechanicalventilation on the cardiovascular system.Crit Care Clin 1990; 6: 663-678.
51. RICHARDSON DW, WASSERMAN AJ,PATTERSON JL. General and regionalcirculatory responses to change in bloodpH and carbon dioxide tension. J ClinInvest 1961; 40: 31-43.
52. RORIE DK, TYCE GM, MACKENZIERA. Evidence that halothane inhibits nor-epinephrine release from sympatheticnerve endings in dog saphenous vein bystimulation of presynaptic inhibitory mus-carinic receptors. Anesth Analg 1984; 63:1059-1064.
53. DEEGAN R, HE HB, KRIVORUK Y,WOOD AJ, WOOD M. Regulation ofnorepinephrine release by 32-adrenergicreceptors during halothane anesthesia.Anesthesiology 1995; 82: 1417-1425.
306





























