Embed Size (px)
Citation preview

Right ventricular failure
Anesthesia for the cardiac
compromised patient
Right ventricular failure
Steffen Rex
Dept. of Anesthesiology
University Hospital, RWTH Aachen
Germany
26th International Winter Symposium
Update in Cardiothoracic Anesthesia
January 7th - 8th, 2011
Leuven, Belgium

Right ventricular failure
Starr I, Jeffers WA, Meade RH
The absence of conspicuous increments of
venous pressure after severe damage to the right
ventricle of the dog, with a discussion of the relation
between clinical congestive failure and heart
disease.
Am Heart J 1943; 26:291–301
Significance of the right ventricle

Right ventricular failure
Fontan-SurgeryPaul Khairy, Nancy Poirier and Lise-Andrée Mercier
Univentricular Heart.
Circulation 2007;115;800-812
Significance of the right ventricle

Right ventricular failure
RV-function independent predictor of morbidity und mortalityin patients with:
COPD Burgess MI: Comparison of echocardiographic markers of right ventricular function in determining prognosis in chronic pulmonary disease. J Am
Soc. Echocardiogr 2002; 15: 633-9
PPH D'Alonzo GE: Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991; 115: 343-9
Left-sided valvular heart disease Nagel E: Importance of the right ventricle in valvular heart disease. Eur.Heart J 1996; 17: 829-36
Inferior myocardial infarction Mehta SR: Impact of right ventricular involvement on mortality and morbidity in patients with inferior
myocardial infarction. J Am Coll.Cardiol 2001; 37: 37-43
Chronic Heart Failure de Groote P: Right ventricular ejection fraction is an independent predictor of survival in patients
with moderate heart failure. J.Am.Coll.Cardiol 1998; 32: 948-54
Congenital Heart Disease Graham TP: Long-term outcome in congenitally corrected transposition of the great arteries: a multi-institutional study.
J Am Coll Cardiol 2000; 36: 255-61
Pulmonary Artery Embolism Ghaye B: Severe pulmonary embolism:pulmonary artery clot load scores and cardiovascular
parameters as predictors of mortality. Radiology 2006 Jun;239(3):884-91
ARDS Monchi M: Early predictive factors of survival in the acute respiratory distress syndrome. A multivariate analysis. Am J Respir.Crit Care Med 1998; 158: 1076-81
Cardiothoracic Surgery Reichert CL: Prognostic value of biventricular function in hypotensive patients after cardiac surgery as assessed by transesophageal
echocardiography. J Cardiothorac Vasc Anesth 1992; 6: 429-32
Liver Transplantation Le Pavec J: Portopulmonary Hypertension: Survival and Prognostic Factors . Am J Respir Crit Care Med 2008; 178: 637–643
Significance of the right ventricle

Right ventricular failure
Cardiac Surgery
Few prospective data
48% of LCOS, mortality 44% Davila-Roman, Ann Thor Surg 1995
Heart transplant: 50% of early complications; 42%
of perioperative mortality Haddad, CanJCardiol 2008
LVAD-implantation: 30-50%; mortality: 46% Matthews, JACC 2008
Epidemiology of RV failure
in the perioperative period
ARDS
Few prospective data
25-30% using modern ventilation strategies
(mortality: 30-40%) Vieillard-Baron, CCM 2001; Jardin, ICM 2007; Osman , ICM2009

Right ventricular failure
Passive ConduitActive part of circulatory
homeostasis
RV AfterloadLow Increased
Right ventricular paradoxon

Right ventricular failure
Anatomy of the right ventricle
The right ventricle is not just a small left ventricle!
Shape: triangular/crescent (LV: ellipsoid)
Thin-walled (2-5mm vs. LV: 7-11mm):
poor contractile reserves
LVRV
LV

Right ventricular failure
Increased susceptibility to
elevations of afterload
Pathophysiology of the right ventricle
Consequences of an increase in afterload
Haddad F et al.
The Right Ventricle in Cardiac Surgery, a Perioperative
Perspective: I. Anatomy, Physiology, and Assessment
Anesth Analg 2009;108:407–21
Specific anatomy
Poor contractile reserves
1) RV Output ↓

Right ventricular failure
Diastolic ventricular interaction:
Leftward septal shift LV preload ↓
Systolic ventricular interaction:
Leftward septal shift LV contractility ↓
Ventricular Interdependence
2) LV Output ↓
Pathophysiology of the right ventricle
Consequences of an increase in afterload

Right ventricular failure
Systolic ventricular interaction:
Leftward septal shift LV contractility ↓ RV output ↓
Ventricular Interdependence
Pathophysiology of the right ventricle
Consequences of an increase in afterload
3) Septal dysfunction RV Output ↓

Right ventricular failure
Pathophysiology of the right ventricle
Consequences of an increase in afterload
4) RV Coronary Perfusion ↓
Van Wolferen et al.
Right coronary artery flow impairment
in patients with pulmonary hypertension.
European Heart Journal (2008) 29, 120–127
Systole Diastole
Normal
Systole Diastole
PHT

Right ventricular failure
Pathophysiology of the right ventricle
Consequences of an increase in afterload
5) Activation of apoptotic pathways
• ↓ RV and septal expressions of Bcl-2 (antiapoptotic)
• No changes in expressions of Bax (proapoptotic)
↑ Bax/Bcl-2 ratio (proapoptotic)
• ↑ RV caspase-8, caspase-9 and caspase-3 (proapoptotic)
Dewachter C et al.
Activation of apoptotic pathways in experimental acute
afterload-induced right ventricular failure
Crit Care Med 2010; 38:1405–1413

Right ventricular failure
Pathophysiology of the right ventricle
The vicious cycle of RV failure
↓ RV Output
↓ Cardiac outputSystemic
hypotension
↓ RV O2Supply/Demand
↓ LV contractility
Acute RV Failureand Dilation
Leftward
septal shift
Right-Left-Shunting
↑ RV wall tension
↓ LV compliance
↓ LV preload
A. B.
↓ RV contractility
↑ RV Afterload↑ RV Preload
TricuspidRegurgitation
↓ RV coronaryperfusion

Right ventricular failure
Pathophysiology of the right ventricle
The vicious cycle of RV failure
↑ RV afterload
RV dilatation RV dysfunction
↑ RV wall tension
↓ RV contractility
RV ischemia
VenousCongestion
Gaynor et al.
Right Atrial and Ventricular Adaptation to Chronic Right Ventricular Pressure Overload.
Circulation. 2005;112[suppl I]:I-212–I-218
Tricuspid
Regurgitation
Liver Failure
Renal Failure
↑ RV diastolic dysfunction

Right ventricular failure
Etiology of RV failure
in the perioperative period
RV
Afterload
RV
PreloadTricuspid regurgitation
Pulmonary regurgitation
Ischemia
Postoperative contractile dysfunction
(Stunning, Air embolism)
PHT
CPB
Pulmonary Embolism
Mechanical Ventilation
ALI/ARDS
Pulmonary Valve Stenosis
Sepsis
Cardiac Surgery
„Adult congenital
heart disease“
Intracardiac shunt
RV Contractility

Right ventricular failure
• Air Embolism (RCA!)
• Suboptimal myocardial protection (Stunning)
• RV Ischaemia
• Protamine
• CPB-associated PHT
• Release of pulmonary vasoconstrictors
• Depression of pulmonary vasodilators
0
2
4
6
8
10
12
Baseline Pre-CPB Post-CPB 6h ICU 24h ICU
Art
eri
al E
nd
oth
elin
(fm
ol/m
L)
CPB
Off Pump
CPB and NO
CPB and Endothelin
Courtesy P. Wouters
Etiology of RV failure
Post-Cardiotomy

Right ventricular failure
CVP
PAP
RVP
Pulmonary Artery Catheter
Monitoring the right ventricle
in the perioperative period

Right ventricular failure
• RV Shape
• Relative Size
• IVS
• IAS
• RVSP
• RVEDA < 0.7 LVEDA
• RVFAC > 40%
Echocardiography
Monitoring the right ventricle
in the perioperative period

Right ventricular failure
Echocardiography: Longitudinal Function!
Monitoring the right ventricle
in the perioperative period
TAPSE =
Tricuspid Anular Plane Systolic
Excursion
Vogel et al.
Validation of Myocardial Acceleration During Isovolumic Contraction
as a Novel Noninvasive Index of Right Ventricular Contractility.
Circulation. 2002;105:1693-1699
Misannt, Rex et al.
Load-sensitivity of Regional Tissue Deformation in the Right Ventricle:
Isovolumic versus Ejection-phase Indices of Contractility.
Eur Heart J 2008
Tissue Doppler
Imaging
IVA

Right ventricular failure
Mw
(m
Wa
tt s
ml-1
)
0
1
2
3
4
5
Control
TEA
Mw
(m
Wa
tt s
ml-1
)
0
2
4
6
8
10
12
14
Control
TEA
Baseline Hypoxia Baseline
°
*
°°
*
Hypoxia
RV
Rex et al.
Thoracic epidural anesthesia impairs the hemodynamic response to acute pulmonary hypertension by deteriorating right ventricular–pulmonary arterial coupling.
Crit Care Med 2007; 35:222–229
Therapy/Prevention of RV failure
in the perioperative period
Maintain RV intrinsic protective mechanism:
Homeometric Autoregulation:
Adaptation of RV contractility to match an increase in afterload
Avoid/Stop Sympathicolysis

Right ventricular failure
Missant C., Rex S. et al.
Differential effects of lumbar and thoracic epidural anaesthesia on the haemodynamic response to acute right ventricular pressure overload.
British Journal of Anaesthesia 104 (2): 143–9 (2010)
Maintain Homeometric
Autoregulation:
Avoid/stop cardiac
sympathicolysis
Therapy/Prevention of RV failure
in the perioperative period

Right ventricular failure
Therapy/Prevention of RV failure
in the perioperative period
Hypoxic Pulmonary Vasoconstriction
Avoid Hypoxia
Hypoxia
β-NADH ↑
cADP-Ribose
SR
Ca++
KATP
Ca++-
Channel
Ca++
Contraction
Ca++
K+
(-)
(+)
Depolarization
0
10
20
30
40
50
60
50 60 70 80 90 100 110 120 130 140 150
RV
P (m
mH
g)
RVV (ml)
40%
21%
15%
FiO2

Right ventricular failure
Therapy/Prevention of RV failure
in the perioperative period
Extra-alveolar vessels
Avoid hypoxia
HPV
Alveolar vessels
Compression by overinflation
Avoid high airway pressures/
high tidal volumes
Total PVR
Pu
lmo
na
ryV
as
cu
lar
Re
sis
tan
ce
Lung Volume
FRC TLCRV
Adjust the ventilator
PEEP

Right ventricular failure
↑ RV Afterload
RV Dilatation RV Dysfunction
↓ RV Output Leftward septal
shift
↓ LV Preload
↓ CO Hypotension
↓ Coronary
perfusion
pressure
↓ RV DO2
↑ RV VO2
↑ RV wall tension
RV Ischemia
RV diastolic
dysfunction
Venous Congestion Shunt (R-L)
Vasodilation
Vasopressors
↓ RV
contractility
InotropyInodilators
Vasopressors
Optimization Preload
Pharmacological Therapy of RV failure
in the perioperative period

Right ventricular failure
Therapy of RV failure
in the perioperative period
No RCT‘s!
Therapeutic concepts derived from LV failure
Volume: Caution!• Tricuspid regurgitation
• Wall tension
Inotropy• Poor contractile reserves of RV
• Inodilator (levosimendan, milrinone) vs. Inopressor (epinephrine)
Vasoconstriction• Coronary artery perfusion pressure
• Optimization of ventricular interdependence
• Caution: PVR
Vasodilation• Caution: Systemic hypotension / oxygenation
• Selective pulmonary vasodilation (iNO, iloprost)

Right ventricular failure
Inhaled NO Problems:•Non-Responders
•Toxic metabolites (NO2-, NOx)
•Sophisticated monitoring (NO, NO2-)
•Met-Hemoglobinemia
•Inhibition of platelet-aggregation
•Rebound-effects (PHT, Hypoxia)
•Extremely short duration of action
•Not approved
•Costs
•No proven impact on outcome (ARDS)
Haddad E. et al.
Use of Inhaled Nitric Oxide Perioperatively and in Intensive Care Patients.
Anesthesiology 2000; 92(6): 1821-1825
Dosing:
•20 (bis zu 40) ppm, weaning!
Therapy of RV failure
Selective pulmonary vasodilation

Right ventricular failure
Therapy of RV failure
Selective pulmonary vasodilation
Clinical experience suggests that in … acute RV
dysfunction and elevated PVR, use of iNO may
result in haemodynamic improvement when used
during or after cardiac surgery
Prior to iNO administration RV function should
be optimised with conventional treatment

Right ventricular failure
Advantages
Stable carbacyclin derivative
of PGI2
Half-life: 6-9 mins
Duration of action: 20-60 mins
Intermittent nebulization
Solution stable at room
temperature
Solution stable at physiologic
pH
Light-stable
Disadvantages
Special nebulizer required
Ill-defined dose-response-
relationship
Non-responders
Costs
No impact on outcome
Dosing:
•20 (up to 40) µg, every 1-4-6 h
Therapy of RV failure
Selective pulmonary vasodilation: Iloprost

Right ventricular failure
T1 T2 T3 T4
PV
RI/S
VR
I
0.0
0.1
0.2
0.3
0.4 Iloprost
Control
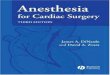
Rex et al.
Inhaled iloprost to control pulmonary artery hypertension in patients undergoing mitral valve surgery: a prospective, randomized-controlled trial.
Acta Anaesthesiol Scand 2008; 52: 65–72
T1 T2 T3 T4
SV
I (m
L/m
²)
0
10
20
30
40
Iloprost
Control
25µ
g ilo
pro
st
vs. 0
.5 µ
g/k
g/m
in N
TG
25µ
g ilo
pro
st
vs. 0
.5 µ
g/k
g/m
in N
TG
25µ
g ilo
pro
st
vs. 0
.5 µ
g/k
g/m
in N
TG
*#
Therapy of RV failure
Selective pulmonary vasodilation: Iloprost
25µ
g ilo
pro
st
vs. 0
.5 µ
g/k
g/m
in N
TG

Right ventricular failure
Sildenafil
Advantages:
•„selective“ inhibition of PDE-V cGMP
•Low costs
•Inotropic effects in RV hypertrophy
Disadvantages:
•Few experience
•Systemic vasodilation
Indications:
•Mitigation of rebound-PHT during weaning
from iNO
•Chronic therapy of PHT
•Combination therapy with inhaled iloprost
Dosing:
Start: 3x12.5mg p.o., then increase to up to
3x50mg, Caution: SVR!!!
Therapy of RV failure
Selective pulmonary vasodilation

Right ventricular failure
PA
-Ea
(m
mH
g.m
L-1
)
0.0
0.5
1.0
1.5
C
L
F : 2.751
P : 0.042
**
* *
**
†
AU
C E
a (
mm
Hg
.mL
-1.m
in)
-60
-40
-20
0
20
40
C
L
P : 0.009
Levosimendan
Mw
(m
Watt
.s.m
L-1
)
0
1
2
3
4
C
L†
*
* *
†
†
†
F : 3.344
P : 0.019
CA
UC
Mw
(m
Watt
.s.m
L-1
.min
)0
100
200
300
400
P : 0.021
L
Em
ax
/ E
a
0.0
0.5
1.0
1.5
2.0
2.5
C
L F : 4.016
P : 0.008
*
*
AU
C E
ma
x /
Ea
(m
in)
0
20
40
60
80
100
120
C L
P : 0.009
AU
C T
au
(m
in)
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
Ta
u (
Fra
ctio
n o
f R
R -
in
terv
al)
0.00
0.02
0.04
0.06
0.08
0.10
0.12
L
C
***
*F : NS
P : NS
P : NS
C L
Missant C, Rex S, Segers P, Wouters P
Levosimendan improves right ventriculovascular coupling in a porcine model of right ventricular dysfunction.
Crit Care Med 2007; 35:707–715
BL I/R T15 T60 T120 BL I/R T15 T60 T120
BL I/R T15 T60 T120 BL I/R T15 T60 T120
RV-Contractility
RV-Afterload
RV-Coupling
RV Diastolic Function
Therapy of RV failure
Inodilators

Right ventricular failure
RV failure
Summary
o Neglected problem in anaesthesia and intensive care
medicine
o Poor prognosis
o Unique (patho)physiological characteristics
o Necessitate tailored prophylaxis and therapy
o Therapy: Selective pulmonary vasodilation,
vasopressors, inodilators
o Need for RCT‘s

Right ventricular failureThank you very much for your attention