Embed Size (px)
Citation preview

Anesthesia for Supratentorial Anesthesia for Supratentorial TumorsTumors
Pekka O. Talke, MDPekka O. Talke, MD
Department of Anesthesia andDepartment of Anesthesia and
Neurosurgery, CottrellNeurosurgery, Cottrell
Chief of NeuroanesthesiaChief of Neuroanesthesia
University of California, San FranciscoUniversity of California, San Francisco
TitleTitle
• 35.000 brain tumors/yr35.000 brain tumors/yr
• 85% primary85% primary
• 60% primary and supratentorial60% primary and supratentorial
• 15% mets (1/6 of tumors)15% mets (1/6 of tumors)

General ConsiderationsGeneral Considerations
• Surgical exposure (retraction)Surgical exposure (retraction)
• Intracranial pressure (ICP)Intracranial pressure (ICP)
• Secondary insult to brainSecondary insult to brain
• Hemorrhage, seizures, air emboliHemorrhage, seizures, air emboli
• Rapid emergenceRapid emergence
• Stress responseStress response
ICPICP
• Tissue, blood, CSFTissue, blood, CSF
• Intracranial-Volume relationshipIntracranial-Volume relationship
• Effects of anesthetics on ICPEffects of anesthetics on ICP
• Tumor mass and edema (steroids)Tumor mass and edema (steroids)
AnestheticsAnesthetics
• Intravenous anesthetics (not ketamine) are Intravenous anesthetics (not ketamine) are cerebral vasoconstrictorscerebral vasoconstrictors
• Reduce CMRReduce CMR
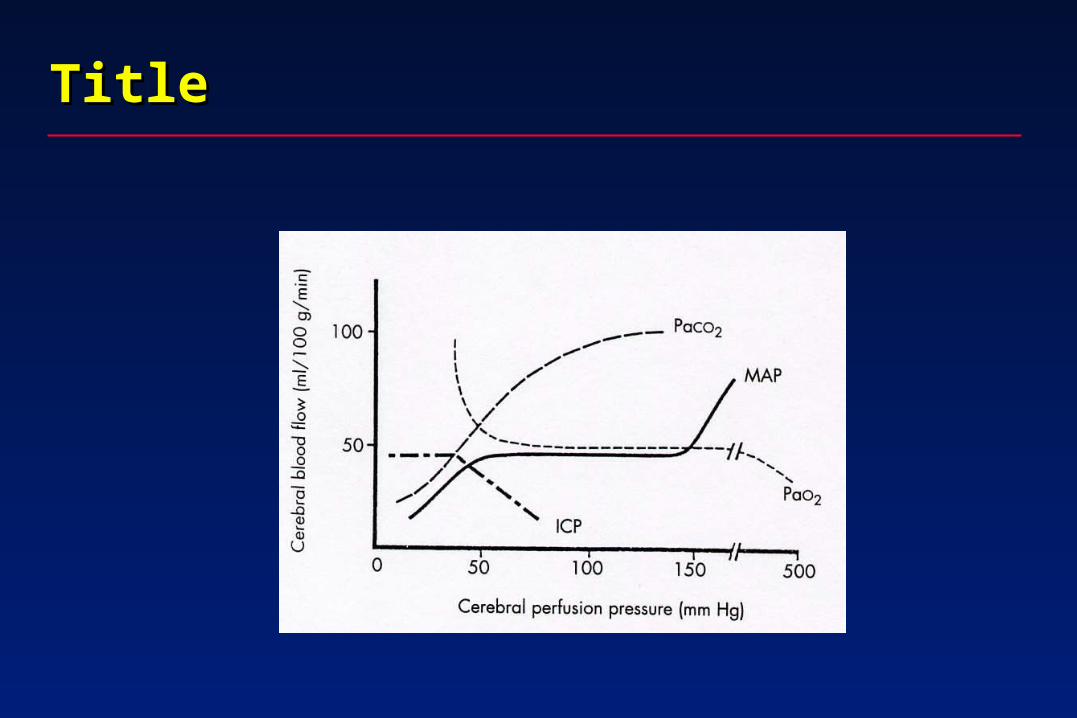
• CO2 reactivity intactCO2 reactivity intact
Anesthetics cont.Anesthetics cont.
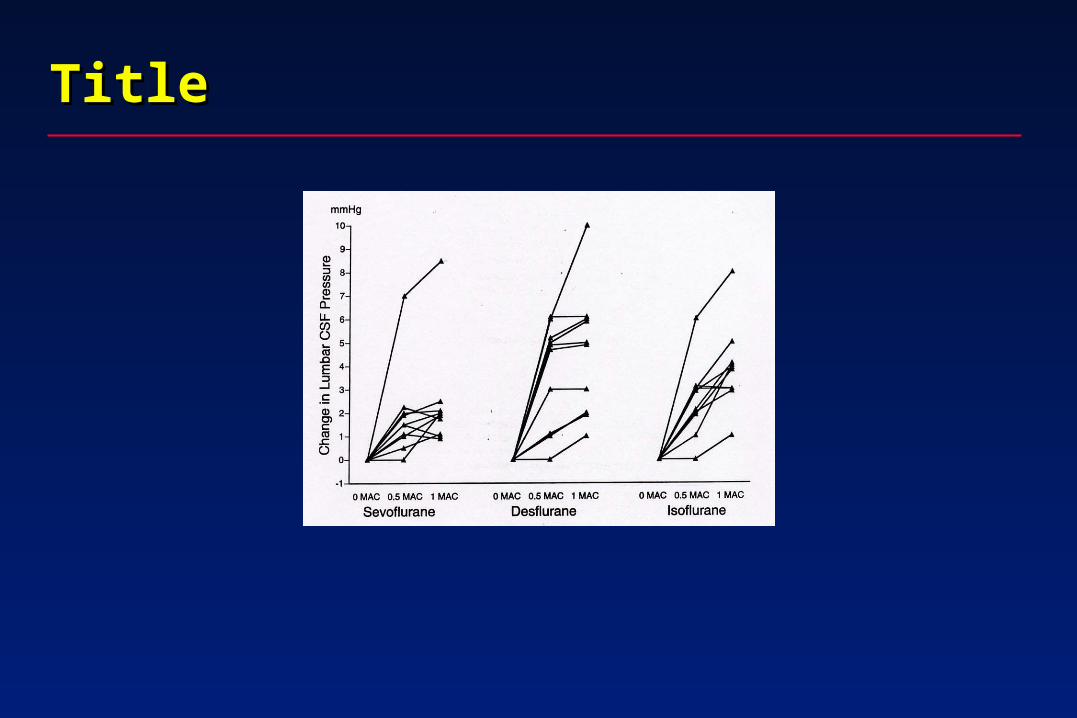
• Volatile anesthetics are cerebral Volatile anesthetics are cerebral vasodilatorsvasodilators
• Increase ICPIncrease ICP
• Reduce CMRReduce CMR
• CO2 reactivity intactCO2 reactivity intact
Anesthetics cont.Anesthetics cont.
• Nitrous oxide increases CMR and ICPNitrous oxide increases CMR and ICP
• Can be controlled by hypocapniaCan be controlled by hypocapnia
• Opioids reduce CMROpioids reduce CMR
• CO2 reactivity intactCO2 reactivity intact
• Nitroglycerine, nitroprusside, hydralazine Nitroglycerine, nitroprusside, hydralazine are cerebral vasodilatorsare cerebral vasodilators

Reduction of ICPReduction of ICP
• Intravenous anestheticsIntravenous anesthetics
• Hyperventilation (30-35 mmHg)Hyperventilation (30-35 mmHg)
• Mannitol (0.5-1.0 gm/kg, 320 mOsm/kg), Mannitol (0.5-1.0 gm/kg, 320 mOsm/kg), (hypernatremia, hypokalemia, hypovolemia) (hypernatremia, hypokalemia, hypovolemia) hypertonic salinehypertonic saline
• LasixLasix
• CSF drainageCSF drainage
• Hypoxia, hypovolemiaHypoxia, hypovolemia
• Head position (venous drainage)Head position (venous drainage)
• Increase MAPIncrease MAP
Preop PlanPreop Plan
• Vascular accessVascular access
• Fluid therapyFluid therapy
• AnestheticsAnesthetics
• VentilationVentilation
• MonitoringMonitoring
• NeuromonitoringNeuromonitoring
PreopPreop
• Sedation=hypercapnia, hypoxia, obstructionSedation=hypercapnia, hypoxia, obstruction
• Stress: increased CMR, CBFStress: increased CMR, CBF
• Analgesia/sedation midas 0.5.-2.0 Analgesia/sedation midas 0.5.-2.0 mg/fentanyl (25- 100 ug)mg/fentanyl (25- 100 ug)
• SteroidsSteroids
• Anticonvulsants (relaxants, loading SLOW)Anticonvulsants (relaxants, loading SLOW)

Preop cont.Preop cont.
• Two large IvsTwo large Ivs
• A-line (CPP, ABG, glucose, osm)A-line (CPP, ABG, glucose, osm)
• Asleep? To avoid stressAsleep? To avoid stress
MonitoringMonitoring
• BP, HR, CVP?BP, HR, CVP?
• Pulse oxPulse ox
• ERTCo2ERTCo2
• Temperature (hypothermia?)Temperature (hypothermia?)
• UrineUrine
• Relaxometry (hemiplegia, dilantin, tegretol)Relaxometry (hemiplegia, dilantin, tegretol)
• Glucose, Hg, HctGlucose, Hg, Hct

Monitoring cont.Monitoring cont.
• EEGEEG
• SSEPSSEP
• ICP?ICP?
• Motor mappingMotor mapping
InductionInduction
• Avoid hypoxia, hypercarbia, stress Avoid hypoxia, hypercarbia, stress responseresponse
• Propofol/pentothal/hyperventilatePropofol/pentothal/hyperventilate
• Opioids/relaxantsOpioids/relaxants
• Head position (venous obstruction)Head position (venous obstruction)
• More drugs for intubation/pinningMore drugs for intubation/pinning
MaintenanceMaintenance
• Control CMR, CBFControl CMR, CBF
• Good depth of anesthesiaGood depth of anesthesia
• Adequate CPPAdequate CPP
Maintenance cont.Maintenance cont.
• Volatile (<1 MAC)/intravenous Volatile (<1 MAC)/intravenous anesthetics/N2Oanesthetics/N2O
• Mild hyperventilationMild hyperventilation
• Aim for speedy emergence (CT scan)Aim for speedy emergence (CT scan)
Increased ICPIncreased ICP
• HyperventilateHyperventilate
• Venous drainageVenous drainage
• RelaxationRelaxation
• Change to IV anesthesiaChange to IV anesthesia
• Delete N2ODelete N2O
• DiureticsDiuretics
FluidsFluids
• Not hypoosmolarNot hypoosmolar
• Colloids (bleeding)Colloids (bleeding)
• Mannitol (320 mOsm/g)Mannitol (320 mOsm/g)
EmergenceEmergence
• Attenuate stress response (autoregulation Attenuate stress response (autoregulation impaired/labetalol)impaired/labetalol)
• Avoid hypercarbia, hypoxia (opioids)Avoid hypercarbia, hypoxia (opioids)
• Avoid coughingAvoid coughing
• Slow awakening (CT)Slow awakening (CT)
• Seizure, edema, hematoma, Seizure, edema, hematoma, pheumocephalus, vessel occlusion, pheumocephalus, vessel occlusion, ischemia, metabolicischemia, metabolic
TitleTitle
TitleTitle

TitleTitle
IntracranialIntracranial
• Increased intracranial pressureIncreased intracranial pressure
• Midline shift: tearing of the cerebral vesselsMidline shift: tearing of the cerebral vessels
• Herniation: falx, transtentorial, trans-Herniation: falx, transtentorial, trans-foramenforamen
• Magnum, transcraniotomyMagnum, transcraniotomy
• EpilepsyEpilepsy
• VasospasmVasospasm

SystemicSystemic
• HypercapniaHypercapnia
• HypoxemiaHypoxemia
• Hypotension or hypertensionHypotension or hypertension
• Hypoosmolality or hyperosmolalityHypoosmolality or hyperosmolality
• HypoglycemiaHypoglycemia
• HyperglycemiaHyperglycemia
• Shivering or pyrexiaShivering or pyrexia
• Low cardiac outputLow cardiac output
PreventionPrevention
• No overhydrationNo overhydration
• Sedation, analgesia, anxiolysisSedation, analgesia, anxiolysis
• No noxious stimulus applied without sedation and No noxious stimulus applied without sedation and Local AnesthesiaLocal Anesthesia
• Head-up position, no compression of the jugular Head-up position, no compression of the jugular veins, head straightveins, head straight
• Osmotic agents: mannitol, hypertonic salineOsmotic agents: mannitol, hypertonic saline
Prevention cont.Prevention cont.
• Beta-blockers or clonidine or lidocaineBeta-blockers or clonidine or lidocaine
• Steroids, if a tumor is presentSteroids, if a tumor is present
• Adequate hemodynamics: MAP, CVP, PCWP, HRAdequate hemodynamics: MAP, CVP, PCWP, HR
• Adequate ventilation: PacoAdequate ventilation: Paco22>100 mm Hg, Paco>100 mm Hg, Paco22 35 mm Hg 35 mm Hg
• Intrathoracic pressure as low as possibleIntrathoracic pressure as low as possible
• Hyperventilation on demand before inductionHyperventilation on demand before induction
• Use of intravenous anesthetic agents for induction and Use of intravenous anesthetic agents for induction and maintenance in case of tensed brainmaintenance in case of tensed brain

TreatmentTreatment
• CSF drainage if ventricular or lumbar catheter in situCSF drainage if ventricular or lumbar catheter in situ
• Osmotic agentsOsmotic agents
• HyperventilationHyperventilation
• Augmentation of anesthesia with intravenous anesthetic Augmentation of anesthesia with intravenous anesthetic agents: propofol, thiopentone, etomidateagents: propofol, thiopentone, etomidate
• Muscle relaxantMuscle relaxant
• Venous drainage: head up no PEEP, reduction of Venous drainage: head up no PEEP, reduction of inspiratory timeinspiratory time
• Mild controlled hypertension if autoregulation presentMild controlled hypertension if autoregulation present
HistoryHistory
• SeizureSeizure
• Increased intracranial pressure (ICP): headache, Increased intracranial pressure (ICP): headache, nausea, vomiting, blurred visionnausea, vomiting, blurred vision
• Decreased level of consciousness, somnolenceDecreased level of consciousness, somnolence
• Focal neurologic signs: hemiparesis, sensory Focal neurologic signs: hemiparesis, sensory deficits, cranial nerve deficits, and so ondeficits, cranial nerve deficits, and so on
• Paraneoplastic syndromes including presence of Paraneoplastic syndromes including presence of thrombosisthrombosis

Physical EvaluationPhysical Evaluation
• Mental statusMental status
• Papilledema (increased ICP) Papilledema (increased ICP)
• Signs of Cushing’s response: hypertensive Signs of Cushing’s response: hypertensive bradycardiabradycardia
• Pupil size, speech deficit, Glasgow coma score, Pupil size, speech deficit, Glasgow coma score, focal signsfocal signs
• MedicationMedication
• SteroidsSteroids
• Antiepileptic drugsAntiepileptic drugs
Technical Examination (CT or MRI Scan)Technical Examination (CT or MRI Scan)
• Size and location of the tumor: silent or eloquent Size and location of the tumor: silent or eloquent area, near a major vessel, and so onarea, near a major vessel, and so on
• Intracranial mass effect: midline shift, decreased Intracranial mass effect: midline shift, decreased size of the ventricles, temporal lobe hernia size of the ventricles, temporal lobe hernia
• Intracranial mass effect: hydrocephalus, Intracranial mass effect: hydrocephalus, cerebrospinal fluid space around brainstemcerebrospinal fluid space around brainstem
• Others: edema, brainstem involvement, Others: edema, brainstem involvement, pneumocephalus (recraniotomy)pneumocephalus (recraniotomy)
Evaluation of Hydration StatusEvaluation of Hydration Status
• Duration of bed restDuration of bed rest
• Fluid intakeFluid intake
• DiureticsDiuretics
• Inappropriate secretion of antidiuretic Inappropriate secretion of antidiuretic hormonehormone
InductionInduction
• Adequate anxiolysis in the anesthetic roomAdequate anxiolysis in the anesthetic room
• Adequate fluid loading (5 to 7 ml/kg of NaCl 0.9%)Adequate fluid loading (5 to 7 ml/kg of NaCl 0.9%)
• ECG leads in place; capnometer, pulse oximeter, ECG leads in place; capnometer, pulse oximeter, and noninvasive blood pressure monitorsand noninvasive blood pressure monitors
• Insertion of intravenous and arterial lines under Insertion of intravenous and arterial lines under local anesthesialocal anesthesia
• Fentanyl 1 to 2 Fentanyl 1 to 2 g/kg or alfentanil, sufentanil, or g/kg or alfentanil, sufentanil, or remifentanilremifentanil
Induction cont.Induction cont.
• Preoxygenation and voluntary hyperventilationPreoxygenation and voluntary hyperventilation
• Propofol 1.25 to 2.5 mg/kg or thiopentone 3 to 6 mg/kg Propofol 1.25 to 2.5 mg/kg or thiopentone 3 to 6 mg/kg for inductionfor induction
• Nondepolarizing muscle relaxant: vecuronium, Nondepolarizing muscle relaxant: vecuronium, rocuronium, or other controlled ventilation at Pacorocuronium, or other controlled ventilation at Paco22 of of
35 mm Hg35 mm Hg
• Propofol 50 to 150 Propofol 50 to 150 g /kg/min or isoflurance 0.5% to g /kg/min or isoflurance 0.5% to 1.5% (or sevoflurane of desflurane) for maintenance 1.5% (or sevoflurane of desflurane) for maintenance and fentanyl (or alfentanil, sufentanil, or remifentanil) 1 and fentanyl (or alfentanil, sufentanil, or remifentanil) 1 to 2 to 2 g/kg or alfentanil, sufentanil, or remifentanilg/kg or alfentanil, sufentanil, or remifentanil
Induction cont.Induction cont.
• Lignocaine 1.5 mg/kgLignocaine 1.5 mg/kg
• IntubationIntubation
• Local anesthesia and intravenous fentanyl 2 Local anesthesia and intravenous fentanyl 2 g/kg for g/kg for skull-pin head-holder placement and skin incision skull-pin head-holder placement and skin incision adequate head-up positioning; no compression of the adequate head-up positioning; no compression of the jugular veinsjugular veins
• Mannitol 0.5 to 0.75 g/kgMannitol 0.5 to 0.75 g/kg
• Insertion of a lumbar drainInsertion of a lumbar drain
• Possibly NPossibly N22O when the dura is open and brain is slackO when the dura is open and brain is slack
• Normovolemia with the use of NaCl 0.9% or starch 6%—Normovolemia with the use of NaCl 0.9% or starch 6%—nono Ringer’s lactateRinger’s lactate

ICP ControlICP Control
• Mild hyperosmolality (use NaCl 0.9% [304 Mild hyperosmolality (use NaCl 0.9% [304 mOsm/kg]mOsm/kg]
as baseline infusion; give mannitol [1319 as baseline infusion; give mannitol [1319 mOsm/kg]mOsm/kg]
0.5 to 0.75 g/kg or hypertonic saline [7.5% 2533 0.5 to 0.75 g/kg or hypertonic saline [7.5% 2533 mOsm/kg] 3 to 5 ml/kg before bone flap removal)mOsm/kg] 3 to 5 ml/kg before bone flap removal)
• Intravenous anesthetic agent (propofol), adequate Intravenous anesthetic agent (propofol), adequate depth of anesthesiadepth of anesthesia
• Mild hyperventilation, mild hyperoxygenationMild hyperventilation, mild hyperoxygenation
ICP Control cont.ICP Control cont.
• Mild controlled hypertension: MAP maintained around 100 Mild controlled hypertension: MAP maintained around 100 mm Hg in order to decrease CBV and ICPmm Hg in order to decrease CBV and ICP
• Normovolemia; no vasodilatorsNormovolemia; no vasodilators
• Mild hyperoxiaMild hyperoxia
• Together with:Together with:– Adequate head-up positioning– Free venous drainage; no compression of the jugular veins– No PEEP, no ventilator fight (myorelaxants)– Lumbar drainage– Avoidance of brain retractors
AwakeningAwakening
• Neurosurgical awakening should maintain:Neurosurgical awakening should maintain:–Stable arterial blood pressure and thus
cerebral blood flow and intracranial pressure–Stable oxygenation and carbon dioxide
tension–Stable CMRO2
–Normothermia

Awakening cont.Awakening cont.
• Neurosurgical awakening should avoid:Neurosurgical awakening should avoid:–Coughing–Tracheal suctioning–Airway overpressure during extubation
–Patient-ventilator dyssynchrony
Awakening cont.Awakening cont.
• Neurosurgical awakening should provide:Neurosurgical awakening should provide:–Optimal conditions for neurologic examination