Embed Size (px)
Citation preview

Anesthesia for cesarean section
Tom Archer, MD, MBA
UCSD Anesthesia

A unique psychosocial surgery

Outline
• C-section – a unique psychosocial surgery
• How the OB anesthetist should behave.
• Evolution of techniques
• Neuraxial block physiology and management
• GA physiology and management.
• Management of common problems

C-section – a unique psychosocial surgery
• Psychological / interpersonal aspects– Unique surgery, happy event gone awry.– Strike a balance between “happy event” and
“risky surgery”.– Most patients are awake– and want to be.– Team approach (patient, family, nursing, OB,
anesthesia)– Support person present in OR.– Family members in the labor room (face
them).– Discretion about medical info– JW, drug use,
previous abortions, etc.

Anticipate and be available
• Know every patient on the floor. Introduce yourself early.
• Be accessible to OBs and nurses.
• Get informed early about potential problems (airway, obesity, coagulopathy JW, congenital heart disease)
• Remember the basics (IV access, airway)

Anticipate and be available
• We need a certain knowledge of OB to know what is going to happen. Try to think one or two steps ahead.
– “Placenta isn’t out yet in room 7”– “The lady in 6 has a pretty bad tear.”– “Strip review in 3, please.”– “We can’t get an IV on the lady in 4.”– “Can you give us a whiff of anesthesia in 8? We don’t
need much.”

Evolution of technique
• Last 30 years: decreasing use of GA, now about 5% of cases. Was 20-30% in 70’s at UCSD.
• Epidural was “all the rage” in 70’s and 80’s.
• SAB (or epidural) are now preferred anesthetics.

Anesthesia for C/S—basic interventions
• Happy event (sort of)
• Gastric acid neutralization
• Left uterine displacement
• Fluid loading
• Supplemental oxygen
• Support person in room (regional only)

Anesthesia for C/S—Complications
• Sympathectomy / hypotension
• Nausea
• Bradycardia
• High spinal / respiratory paralysis
• Aspiration
• Difficult intubation
• Local anesthetic toxicity
• Failed regional anesthesia
• Persistent neurological deficit

C/S red flags
• “I don’t feel so good…I think I’m going to throw up…” (Hypotension until proven otherwise).
• “Doc, I feel like I’m not getting enough to breathe…”
• The “floppy arm sign.”
• The “shaking head sign.”

Spinal-- advantages
• Uniquely appropriate in C/S (happy event).
• Really amazing when you think about it.– Awake and smiling.– Arms and hands are normal. – Major surgery inside the abdomen.
• Quick, solid, simple, reliable, pretty safe.
• LA + narcotic gives great block.
• Can give long-acting analgesia (intrathecal MS)

Regional anesthesia for c/s in Turkey (SOAP outreach)

Spinal-- disadvantages
• Fixed duration (unless continuous spinal).
• Rapid onset of sympathectomy or high block.
• Small chance of PDPH.

SAB– absolute contraindications
• Patient refusal
• Uncorrected hypovolemia
• Clinical coagulopathy
• Infection at site of injection

SAB– obsolete contraindication
• Severe pre-eclampsia—
• Not associated with increased chance of severe hypotension with neuraxial block.
• Show me the literature if you disagree.

SAB– relative contraindications
• Spinal cord, LE nerve disease.
• Spinal deformity, instrumentation
• Back problems / fear of block
• Laboratory coagulopathy
• Bacteremia

SAB– relative contraindications
• Potential for hypovolemia
• Stenotic cardiac valve lesions (?)
• Pulmonary hypertension (?)

Basic C/S monitoring
• Talk with the patient!
• Does her face display anxiety?
• “Take a deep breath!”
• Have her squeeze your fingers
• What is her hand temperature?
• Are the hand veins dilated?
• “Do your hands feel normal or do they feel a little numb?”

SAB / epidural cause sympathectomy
• Dilation of capacitance vessels (70-80% of blood volume)– May cause drop in CO
• Dilation of resistance arterioles (0.1-0.4 mm diameter).– Drop in SVR

SAB / epidural cause sympathectomy
www.cvphysiology.com/Blood%20Pressure/BP019.htm

SAB / epidural cause sympathectomy
www.cvphysiology.com/Blood%20Pressure/BP019.htm

SAB / epidural cause sympathectomy
rfumsphysiology.pbwiki.com/Characteristics+of...

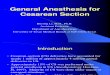
38 y.o. female, repeat c/s, 420 #, gestational hypertension, continuous spinal: fall in SVR, rise in CO with onset of block. Increased SVR with
phenylephrine.

When is sympathectomy(low SVR) bad?
• BP = CO x SVR
• Whenever you can’t increase CO!– Uncorrected hypovolemia– IVC compression– Stenotic valve lesions– Pulmonary hypertension

Tricuspid
Pulmonic
Pulmonary capillaries
Mitral
Aortic stenosis
Resistance arterioles
Aortic stenosis at rest
Cardiac output not sufficient to cause critically high LV intracavitary pressure / LV failure.
LV dilation / hypertrophy

Tricuspid
Pulmonic
Pulmonary capillaries (edema)
Mitral
Aortic
Stenosis
Resistance arterioles– decreased SVR
Aortic stenosis with SAB: increased cardiac output / arteriolar vasodilation:
Decreased SVR Fall in systemic BP and / or increase in LV intracavitary pressure ischemia or LV failure.
LV failure / ischemia

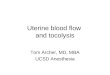
38 y.o. female, repeat c/s, 420#, continuous SAB. Delivery with increased CO at 17, oxytocin 3 U bolus at 18, phenylephrine at 19

When is sympathectomy(low SVR) bad?
• With bolus of other vasodilator (oxytocin)

Oxytocin 10 u bolus

Phenylephrine bolus for hypotension
Delivery of baby
Oxytocin 5U IV push
C/S under epidural in pt with previous peripartum cardiomyopathy (May 30, 2007)
Both delivery and oxytocin cause increase in cardiac output.

When is sympathectomy(low SVR) bad?
• When drop in SVR could exacerbate R > L shunt.– ASD– VSD– PDA

LA
RA
LV
RV
Decreased SVR desaturation
Increased pulmonary vascular resistance desaturation
Ao
PA
Decompensated patient with ASD, VSD or PDA-- Decreased SVR or increased pulmonary vascular resistance increased RL shunt and increased arterial desaturation.
Decompensated patient with REAL RL shunt.

38 y.o. female, repeat c/s, 420 #, gestational hypertension, continuous spinal: fall in SVR, rise in CO with onset of block. Increased SVR with
phenylephrine.

LA
RA
LV
RV
High SVR,
Minimal RL shunt
Ao
PALow pulmonary vascular resistance
Normal, compensated patient with ASD, VSD or PDA-- high SVR and low pulmonary vascular resistance minimal RL shunt.
Compensated patient with POTENTIAL RL shunt.

JW with previa / accreta for c-hyst. GA. Induction at 7, 8, intubation before 9, incision after 9. Note rise in SVR and fall in CO with GA.

How to prevent a sympathectomy from being a problem
• Keep the SVR up with a vasopressor like phenylephrine.

Preventing or treating hypotensionfrom sympathectomy: augment venous return (CO).
• Trendelenburg (empty capacitance vessels into central thoracic veins)
• LUD (get pressure off vena cava)
• Fluid loading (fill capacitance vessels)– Crystalloid– Hetastarch
• Arteriolar constrictors (inc SVR)– Ephedrine, phenylephrine
• Venous constrictors (inc venous return)– Ephedrine, phenylephrine

Hypotension with SAB or epidural
• Pre-load does not prevent reliably.
• 500 mL hetastarch better than 1500 mL crystalloid.
• First symptom is nausea or “I don’t feel so good.”

Hypotension
• Use phenylephrine (neosynephrine) if tachycardia.
• Use ephedrine if bradycardia.
• Use atropine if severe bradycardia.
• Glycopyrolate works slowly.

Sympathectomywww.sympathectomy.co.uk/ETS.php

Sympathectomy

Endoscopic transthoracic sympathectomy
Virtually all patients immediately develop warm, dry hands and leave the hospital the same day as surgery.
www.sd-neurosurgeon.com/.../hyperhidrosis.html

Hyperhydrosis Rx’d with T3 sympathectomy

Horner’s syndrome

Horner’s syndrome

Bradycardia
• With hypotension: High block of “cardioaccelerator fibers” (T1-T5).
• Also can be reflex bradycardia with hypertension from phenylephrine

Inc SVR and BP with bradycardia from neo 50 mcgm at 4. Brady occurs after SVR and BP changes.

Left Uterine Displacement(LUD)

Colman-Brochu S 2004

http://www.manbit.com/OA/f28-1.htm

Manbit imageshttp://www.manbit.com/OA/f28-1.htm

Chestnut chap. 2

www.siumed.edu/~dking2/erg/images/placenta.jpgfrom Google images

)
Umbilical artery (UA)Umbilical vein (UV)
Uterine arteriesUterine veinsMom
Fetus
Normal placental function: fetal and maternal circulations separated by thin membrane (syncytiotrophoblast).
“Lakes” of maternal blood
Archer TL 2006 unpublished
Fetal capillaries in chorionic villi
Precariously oxygenated environment

P1 = uterine artery pressure
P2 = uterine vein pressure
R = placental resistance (fixed in short term)
Ohm’s Law of the placenta: O2 delivery = Placental blood flow = (P1 – P2) / R
Aorto-caval compression decreases P1 (“aorto”) and increases P2 (“caval”)
Therefore, aorto-caval compression decreases O2 delivery to fetus.
Placenta blood flow (O2 delivery) =
(P1 – P2) / R
Archer TL 2006

General anesthesia-- advantages
• Fast
• Reliable (if you get the tube in).
• Doesn’t cause sympathectomy
• Duration is flexible
• Patient is not awake (to experience problems).
• Can be given despite coagulopathy

General anesthesia-- disadvantages
• Patient not awake for birth.
• Unprotected airway.
• Possible “can’t intubate, can’t ventilate” scenario.
• Nausea, post-op pain, sore throat.

Functional residual capacity (FRC) is our “air tank” for apnea.
www.picture-newsletter.com/scuba-diving/scuba... from Google images

Pregnant Mom has a smaller “air tank”.
Non-pregnant woman
www.pyramydair.com/blog/images/scuba-web.jpg

GA for C/S—
• Thorough pre-oxygenation• Cricoid pressure• Small tube (6.0-7.0)• RSI• 50% N2O until delivery + 0.5 MAC
volatile.• 60-70% N2O after delivery + midazolam +
narcotic.• Small dose non-depolarizing NMB, if
needed.

General anesthesia-- advantages
• SVR is maintained high (no need to increase CO)
– Hypovolemia– Stenotic cardiac valve lesion– Pulmonary hypertension– Potential R>L shunt

JW with previa / accreta for c-hyst. GA. Induction at 7, 8, intubation before 9, incision after 9. Note rise in SVR and fall in CO with GA.

Managing common problems

High block– patient can’t breathe
• Move to anesthesia mask and circle system early. Don’t fuss around “assessing” the patient!
• Reassure patient, tell them this happens, and tell them you will help them breathe.
• You usually don’t have to intubate.
• Sometimes patients will panic and shake head back and forth to get the mask off of their face.
• Assume accompanying hypotension. Give ephedrine or neo as you reach for the mask.

High block– patient can’t breathe
• If patient becomes unresponsive, you probably should intubate– BUT VENTILATE FIRST AND DON’T PANIC.
• Assistant can give cricoid pressure– but VENTILATE, above all!
• May not need relaxant to intubate.
• Respiratory paralysis usually does not last long (5-15 minutes).

Failed regional anesthesia
• Be honest with yourself– recognize failure.
• Move on to plan B.

Aspiration
• 16 y.o. WF, “Crystal”, +Hx substance abuse, C/S for failure to progress.
• Epidural, patchy block, supplemented with ketamine, fentanyl, diazepam.
• I was vigilant with breath sounds (precordial stethoscope era).
• Baby OK. Mother OK in PACU at 4PM.

Aspiration
• Called at home next AM: Pt SOB, transferred to ICU and intubated.
• I go to hospital, review nurses’ notes.
• Nauseated during the night, got MS several doses. Lying flat during the night.
• SOB at 4AM. Aspiration? When? My fault?
• Died 10 days later of progressive ARDS, hypoxia.

Aspiration
• Not only during GA!
• Use “triple Rx” freely (on everybody?)
• Beware with– High spinal– Heavy supplementation for bad block– “Never turn your back on a spinal.”

“STAT C/S”
• Often “a flail”.• “We’ve got to go. NOW!”• Egos and emotions run high.• Does the patient know what is happening?• Talk to patient. Informed consent.• Don’t endanger the mother to “save” the baby.• Know when and how to say “no” to the OB.• Stay calm.• Cover the basics (H&P, IV access, airway,
informed consent, patient asleep before incision.)

A stat C/S, once upon a time…
• Fetal decels• Rush to the OR• Anesthesiologist is sure he can get the tube in fast• He skips the pre-O2.• He can’t intubate or ventilate• Patient arrests.• Code blue called, staff intubates.• Post op seizures, hypoxic encepalopathy.• Patient recovers after several days.

Summary
• Regional anesthesia is elegant and uniquely suited to C-section.
• GA still has its place, and its dangers.
• Early warning, good communications and equanimity under pressure promote good outcomes.

The End






![Evidence-Based Obstetric Anesthesia: An Update on ...cdn.intechopen.com/pdfs/37215.pdf · Evidence-Based Obstetric Anesthesia: An Update on Anesthesia for Cesarean Delivery 71 [6]](https://img.pdfslide.us/doc/110x75/5d4f1fe388c993790d8baf75/evidence-based-obstetric-anesthesia-an-update-on-cdn-evidence-based-obstetric.jpg)