Embed Size (px)
Citation preview

“And bring a ton of quarters” [Cheney 2012]

Pure Mental harm and the GEPIC
Nick Ford BMed Sc Hons, BM BS, FRANZCP
Snr Clinical Lecturer Uni Adelaide
All case material used with patients permission.
Outline
The GEPIC
The report format
Sample Case
Maximal Medical Improvement
Truth, mistruth and the problems in establishing this
The GEPIC Pros and Cons.
Brain injury….

How things are

How things seem

Photos courtesy of Manuel Ubler
www.seifertuebler.com/welzow-tagebau

“Why is my light withdrawn?”
“Surely I am one before whom men spit?”
“My nights are filled with anguish until the dawn”
“And the pain that gnaws me takes no rest”
From the Book of Job, Holy Bible ~ 600 BC

What I think you see
Stigma of psychiatric illness with adverse treatment in most
jurisdictions and on occasion woolly, judgemental or inflated
opinions.
Role of personal responsibility vs a disease of the mind
Recommendations for treatment; that don’t happen
Access and willingness to access treatment
The iatrogenic effects of the claims process

Traffic accidents and the assessment of Psychiatric
impairment
The guide to the evaluation of Psych impairment [GEPIC]
A psychiatric diagnosis [DSMV] and maximal medical improvement
An Injury Severity Value {ISV}
“Pure Mental Harm” only.
Observation + Data
One examination only

The GEPIC& Psychiatric impairment I
Introduced in Victoria in 1997
Measures impairment not disability
[ accredited] observer rated measures; based on one session +
documentation/observation over time
Good inter rater correlations BUT problems of bias/rapport/
observational ability remain…calibration of the instrument.

The GEPIC& Psychiatric impairment II
Associations with prognosis in epidemiological studies remains unknown [ the same measures have been used for 50 + years in psych research] HDRS, MDRS, CAPS etc .
A psychiatric diagnosis must be made according to DSM 5
DSM V is widely disliked by psychiatrists; lack of prognostic and treatment relevance. [NIGH RDOC matrix]
Absence of online guides ;://aworkcovervictimsdiary.com/2014/03/are-you-missing-out-on-compensation-or-a-payout-from-workcover/

Factors assessed in the GEPIC
Intelligence
Thinking
Perception
Behaviour
Judgement
Mood
Each is linked to a number of “anchors” in the training manual;

E.g. Perception
Class
1 Minimal or no altering of sensorium
2 Heightening or dulling or perception to
semi dissociative flashbacks
3 Dissociative flashbacks in 1 or more
sensory domains. pseudo hallucinations
4 Hallucinations with varying digress of
preoccupation and insight

‘I feel dead people”
GEPIC Classes of psychiatric impairment I
1 MINIMAL
2 MILD
3 MODERATE
4 SEVERE
5 EXTREME

GEPIC Classes of psychiatric
impairment II intra class ranges
1 Minimal Low, Medium and High ranges
2 Mild Low, Medium and High ranges
3 Moderate Low, Medium and High ranges
4 Severe Low, Medium and High ranges
5 Extreme Low, Medium and High ranges

GEPIC Classes of psychiatric impairment II intra class ranges
THESE ARE NOT USED IN TRAFFIC
ACCIDENTS
1 Minimal Low, Medium and High ranges
2 Mild Low, Medium and High ranges
3 Moderate Low, Medium and High ranges
4 Severe Low, Medium and High ranges
5 Extreme Low, Medium and High ranges

GEPIC; Full version
The full version provides a percentage impairment, the MAIAS version does not permit this.
From this pre existing and consequential mental harm can be subtracted if appropriate [does not occur in the MAIAS}
The subtractions are inevitably informed guesses [but do not occur in the MAIAS]
Leading to a percentage of pure mental harm [does not occur in the MAIAS]

Injury Severity Values
A range
Pure mental harm ISV 10-13 [mild, moderate, severe and extreme]
Corresponding to GEPIC Levels 1 & 2, 3,4 and 5
a range for each ISV dependent upon severity within the GEPIC level
?Compensation…..at moderate impairment [ISV 7+, GEPIC level 3 i.e. 25% WPI]
Cannot be secondary to a physical injury; although a GEPIC report may elevate the range for the ISV

Pure and consequential mental harm
Consequential follows on from a physical injury
There may be a mixture of pure and consequential mental harm in the
same patient
Dominant injury [ is likely to be physical]
The psych report may lift the ISV value to the top of the range
Separation of pure vs consequential e.g. separating out fear./horror
from pain/loss of function can be described
Class Of
Impairment
Normal to
slight
Mild Moderate Moderately
Severe
Severe
Mental function 1 2 3 4 5

Class Of
Impairment
Normal to
slight
Mild Moderate Moderately
Severe
Severe
Mental function 1 2 3 4 5
Intelligence
Thinking
Perception
Judgment
Mood
Behaviour

Percent
Impairment
<5 10-20 25-50 55-70 >75
Class Of
Impairment
Normal to
slight
Mild Moderate Moderately
Severe
Severe
Mental function 1 2 3 4 5
Intelligence
Thinking
Perception
Judgment
Mood
Behaviour




Opinion Patient F.
1. Opinion; major depressive disorder, chronic. Chronic PTSD is subsumed by the
major depression but is present. Death of companion in bridge collapse and
inability to recover the body is noted..
2. Prognosis; Poor
3. Injury stability; MMI has been reached following comprehensive treatment, and the
passage of time.
4. The injury is consistent with the stated cause [see 5 below].
5. The effect of the accident on any pre existing injury. There is increased pain
perception of a pre existing shoulder wound which was previously quiescent
6. The effect of the accident on subsequent injury; there are no subsequent injuries.

7. The GEPIC rating with detailed reasoning; patient F
F has shown an impaired ability to forward plan business
eneavours and some decrease in memory; this is the upper end
of class 1. There is diminished speed of thought and speech,
with a pre occupation with themes of loss, ruminations of the
event which are difficult to suppress. He is in the upper end of
class 2. Perceptions are impaired with visual , auditory and
somatic flashbacks at least twice weekly . He is in the lower
range of class 3. Judgement is impaired with withdrawal,
requiring prompts for self care from his friend Sam &
alienation from some previous relationships.. He is in class 3,
mid range. Mood is pervasively low, with loss of weight,
despair, apathy low energy & anhedonia. He is in the mid
range of class 3. Behaviour shows fair function but markedly
diminished stress tolerance. He is in class 2 , high range.
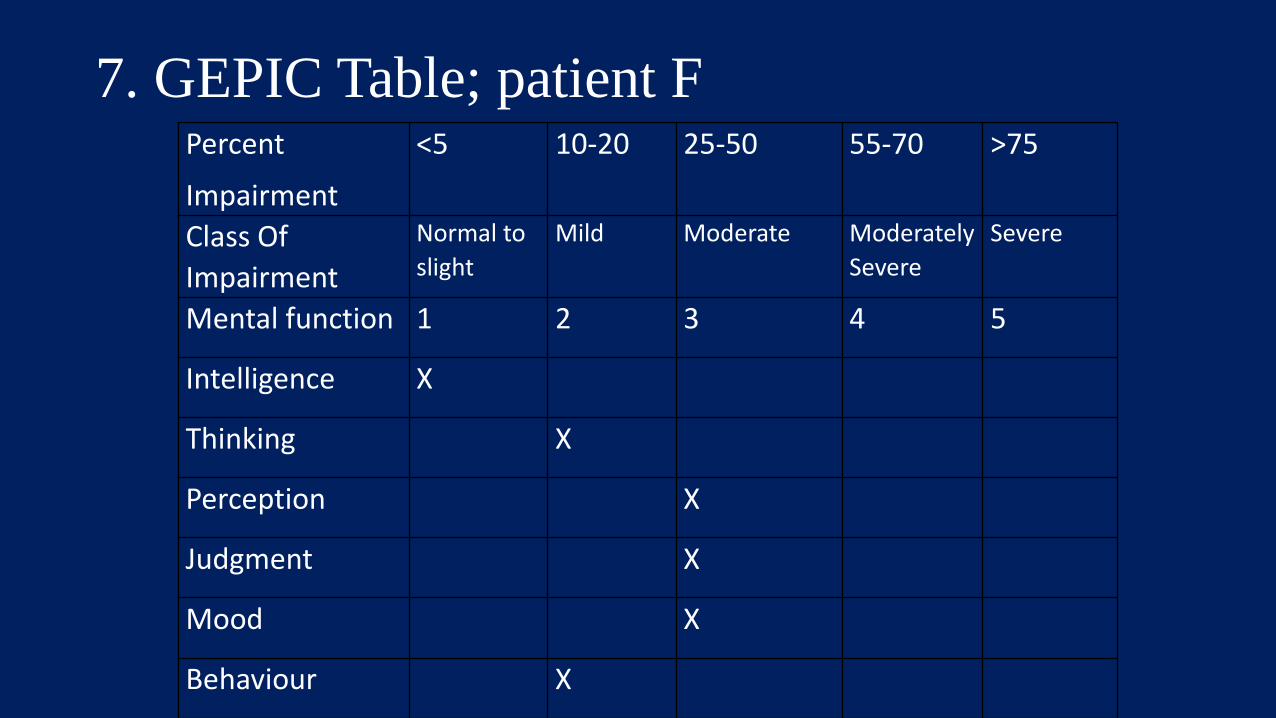
Percent
Impairment
<5 10-20 25-50 55-70 >75
Class Of
Impairment
Normal to
slight
Mild Moderate Moderately
Severe
Severe
Mental function 1 2 3 4 5
Intelligence X
Thinking X
Perception X
Judgment X
Mood X
Behaviour X
7. GEPIC Table; patient F

GEPIC Rating; Patient F.
The classes in order are:122333.
The median class is 2.5; which is rounded up to 3
according to the training manual.
8. The ISV is thus 12. This is in the lower range of the
ISV range.

Stability?
Unlikely to change substantially, with or without treatment in the
next year, or so.
Reasonable treatment?
Compliance, Access including geography
Many illnesses are prone to relapse
Vulnerable periods and unpredictable hazards

Maximal Medical Improvement
Case by case
2 or more antidepressants , at adequate dosage+ a psychotherapy [not
just chatting]
Time ill
Losses incurred [job, family etc]
TRD 2 + years
PTSD 2+ years
More legal than medical

Texas Medication Algorithm Project
Non Psychotic major depression]
1. Antidepressant [1a +/- augmentation]
2. Different class [2a+/- augmentation]
3. TCA [3a +/- augmentation]
4 Lithium augmentation
5. Combination antidepressants [mirtaz + SSRI/SNRI, Bupropion +
SSRI, TCA + SSRI]
6 ECT
7 Other [Lamotrigine, TCA + MAOI]

Results of Tertiary treatment of TRD [Fekadu et al 2012]
150 patients; 13 deceased [suicide/cardiovascular], 118 consent to
follow up.
60% sustained recovery [ > 6/12 remission] over 3 years [intent to
treat analysis]
Social support, severity of treatment resistance, MAOI’s, SNRI’s
[duloxetine]

Trauma
“Everyone has their
breaking point Willard,
you and I have, and he
has obviously become
insane”’
Herr, Apocalypse Now

PTSD Predictors of Poor outcome
Late +/- inadequate treatment
Deaths, burning and distortion of the human form
Entrapment
Lack of social support [including self induced]
Substance abuse and dependence
High conflict claims management
Past and family psych history
Prior resolved PTSD may “inoculate”

Relapse with incomplete recovery [Judd LL et al 1998]

Combined psychotherapy and
PharMAIASotherapy [Pampallano et al 2004]

Resilience and your genes; COMT alleles&vulnerability to PTSD; Rwanda

Sometimes it gets chronic

Chronicity & MMI
Adequate and thorough treatment failed
Access to adequate and thorough treatment
Motivation to engage
Pre; Prior unresolved trauma or Lack of prior trauma and an entitled privileged background
Intra ; loss of loved ones, disabling physical injuries, guilt
Post; losses, opiates for pain, poor claims management
Patients at >15- 20% WPI after adequate Rx are unlikely to recover and continue to be seen ass outpatients/inpatients

Credibility and both sides of the fence
New ice,
A coiled snake,
The sons of Kings,
And an insurance case
These are the things not to be trusted
Germanic 2-500 AD [with modifications]
Credibility I
False imputation and symptom exaggeration are not common [ 5-10%
of claims]
Time course of symptoms
Consistency of history and affect
Response to probe questions
Technical language
Unusual reactions to treatment interventions
Judgement and the gestalt [1+2 always equals 3]

Credibility II
Evasiveness , and responses to alternative information.
Unchanging dreams in PTSD
“ the good old days”, idealised prior function.
Prior history withheld [ illness, legal issues, and
compensation]…..some reports are less than complete
Resistance to active rather than passive treatments.
Wide scatter of impairment classes eg 111333

Credibility III Interviewing styles
Rapport is respect, interest and compassion
Rapport is not judgment, sympathy or humiliation
Reassure about how deep the interview might go; and then start
probing
Explain why a past history is important, but talk about privacy
Look for links and observe the emotional response

Issues in compensation matters
Focus on character weaknesses of the targeted individual
Spreading of false information
Encroachments on private property;
Surveillance open and covert
Intimidation
Harassment and threats
Delays in investigation

Zersetzen; Stasi, East Germany;
1978-1989 [http://zersetzen.wikispaces.com/, Appelbaum 2014 ]
Focus on character weaknesses of the targeted individual
Spreading of false information
Encroachments on private property;
Surveillance open and covert
Intimidation
Harassment and threats
Delays in investigation

Disability; High and low stress compensation claims at 6 years, low risk
grouping [Grant et al 2014]

Case Management Issues, decreasing order of
prediction of disability at 5 years. [Grant et al 2014]
1. Not understanding requirements and the system.
2. Duration of the process
3. Being listened to.
4. Number of medical appointments
5. Respect and dignity
6. Amount of compensation

The GEPIC Pros and Cons
One assessor only… Medical Panels a or the Hot Tub?
Observational..and quite hard to fake good or bad on
No longer term data in proper epidemiological studies
Where should the compensable point be?
Conversion disorder and tremors
Who should assess Brain Injury…and How?
Would a percentage impairment better guide the court, or would it
lead to more argument?

Questions?

KR beating.
#1; penetrating injury r eye,
traumatic avulsion left middle
finger, multiple scars.
#2; fracture/malunion L tibia
Flashbacks/nightmares, 4 hrs
sleep, active/altruistic ++
Brain Injury
ISV’s 5-9
Ranges 0- 100
Minor TBI vs Concussion?
Neuropsych impairment?....happens with psych injury too
Imaging? ….the better the image, the more you find
GCS…mostly but not always accurate [moderate complex TBI

Head injury; Initial Severity markers
Glasgow coma scale
Post traumatic and retrograde amnesia
CSF leak, Anosmia, racoon eyes, battle sign
focal neurological signs
Skull fracture
Multiple injury sites
Biomarkers ? S100b, GFAP
Nick Ford Bed Sc [Hons] FRANZCP 3/24/2017
54





























