Embed Size (px)
Citation preview
1
ANCA‐associated vasculitis in China
Renal Division, Peking University First Hospital,Beijing 100034, P. R. China
Min Chen
2
• General introduction of AAV in China– Disease spectrum and ANCA type
• Clinical and pathological study– Treatment and outcomes
• Pathogenic studies – Complement and neutrophils
3
• General introduction of AAV in China– Disease spectrum and ANCA type
• Clinical and pathological study– Treatment and outcomes
• Pathogenic studies – Complement and neutrophils
4
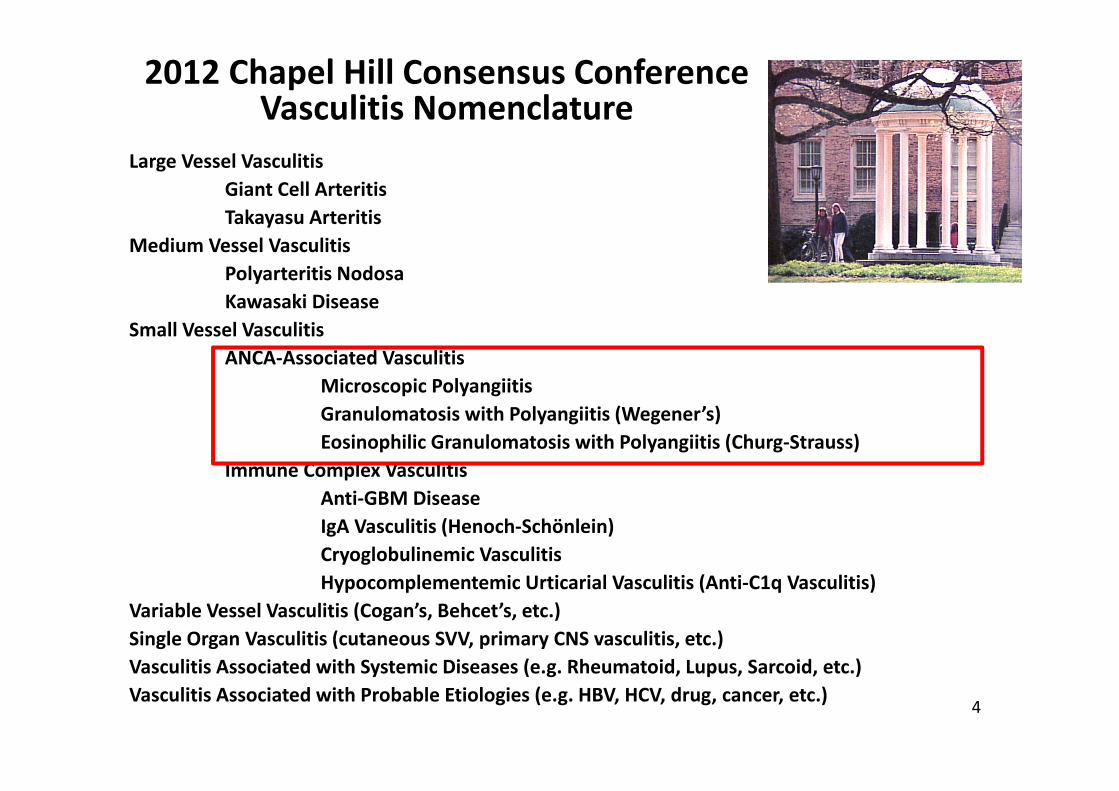
Large Vessel VasculitisGiant Cell ArteritisTakayasu Arteritis
Medium Vessel VasculitisPolyarteritis NodosaKawasaki Disease
Small Vessel VasculitisANCA‐Associated Vasculitis
Microscopic PolyangiitisGranulomatosis with Polyangiitis (Wegener’s)Eosinophilic Granulomatosis with Polyangiitis (Churg‐Strauss)
Immune Complex VasculitisAnti‐GBM DiseaseIgA Vasculitis (Henoch‐Schönlein)Cryoglobulinemic VasculitisHypocomplementemic Urticarial Vasculitis (Anti‐C1q Vasculitis)
Variable Vessel Vasculitis (Cogan’s, Behcet’s, etc.)Single Organ Vasculitis (cutaneous SVV, primary CNS vasculitis, etc.)Vasculitis Associated with Systemic Diseases (e.g. Rheumatoid, Lupus, Sarcoid, etc.)Vasculitis Associated with Probable Etiologies (e.g. HBV, HCV, drug, cancer, etc.)
2012 Chapel Hill Consensus Conference Vasculitis Nomenclature
5
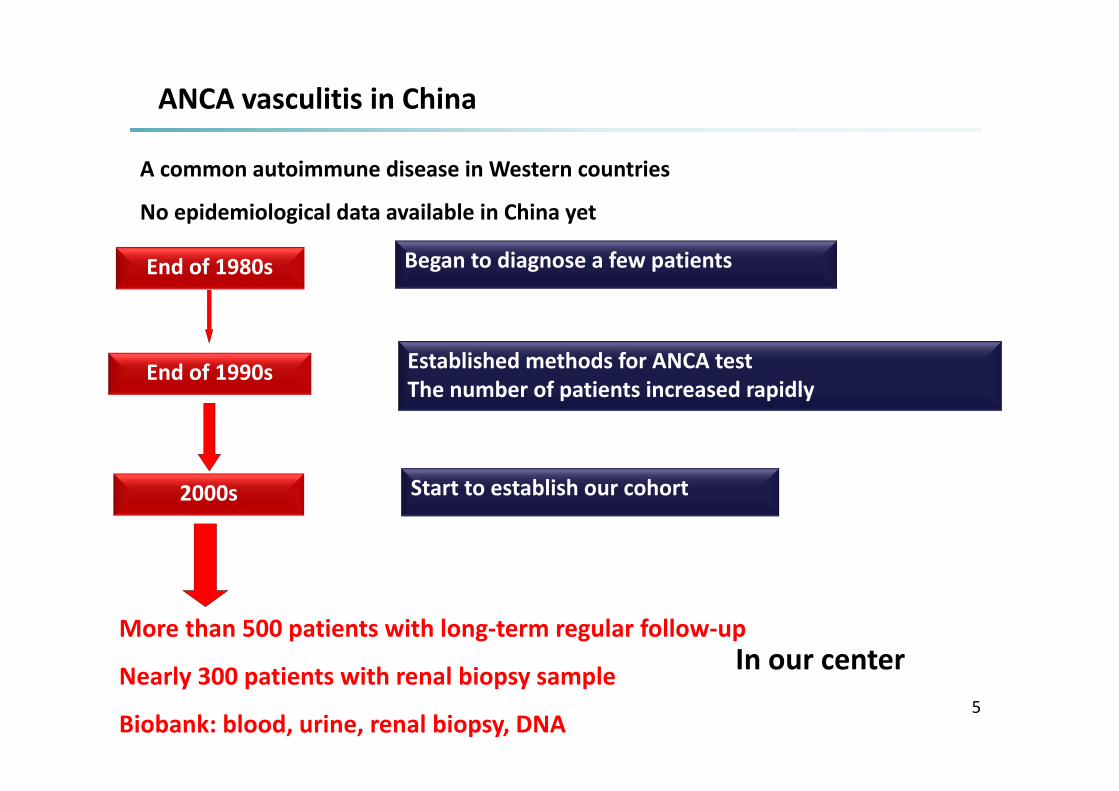
End of 1980s
End of 1990s
2000s
Began to diagnose a few patients
Established methods for ANCA testThe number of patients increased rapidly
Start to establish our cohort
More than 500 patients with long‐term regular follow‐up
Nearly 300 patients with renal biopsy sample
Biobank: blood, urine, renal biopsy, DNA
ANCA vasculitis in China
A common autoimmune disease in Western countries
No epidemiological data available in China yet
In our center
6
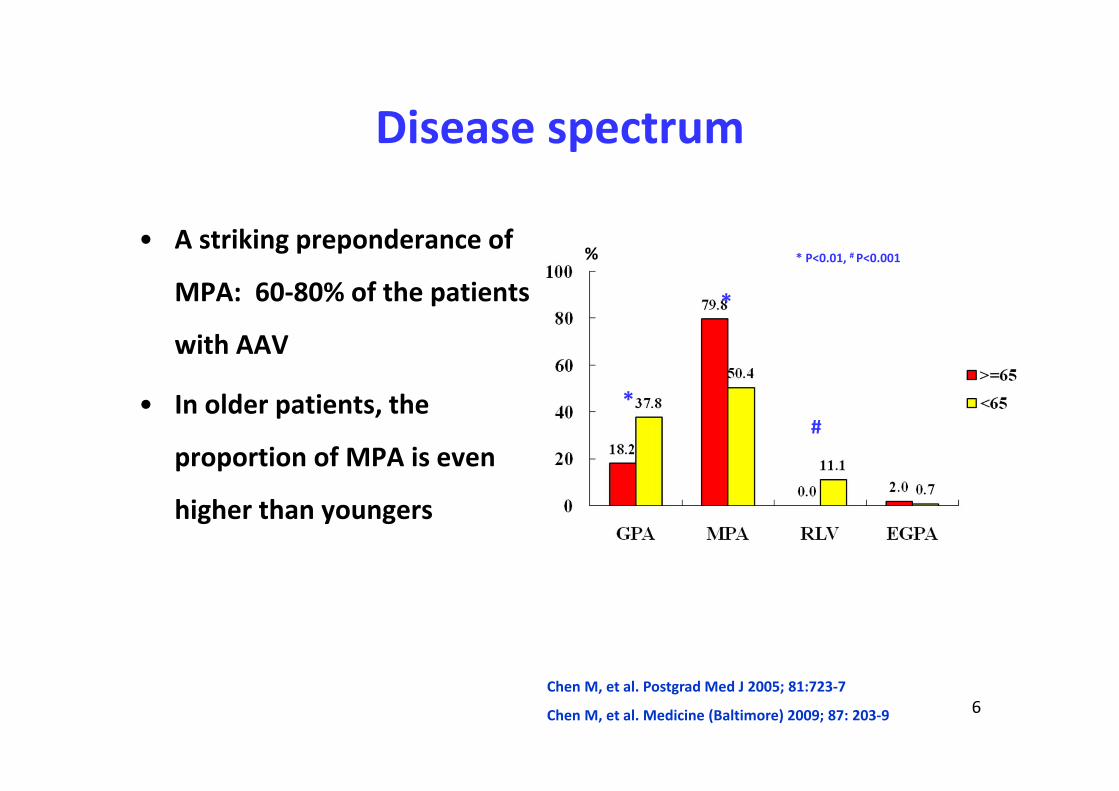
Disease spectrum
• A striking preponderance of
MPA: 60‐80% of the patients
with AAV
• In older patients, the
proportion of MPA is even
higher than youngers
%
*
*
#
* P<0.01, # P<0.001
Chen M, et al. Postgrad Med J 2005; 81:723‐7
Chen M, et al. Medicine (Baltimore) 2009; 87: 203‐9
7
61,8%81,5%
27,8%
55,8%
0%
25%
50%
75%
100%
eye ear
MPO -ANCA PR3-ANCA
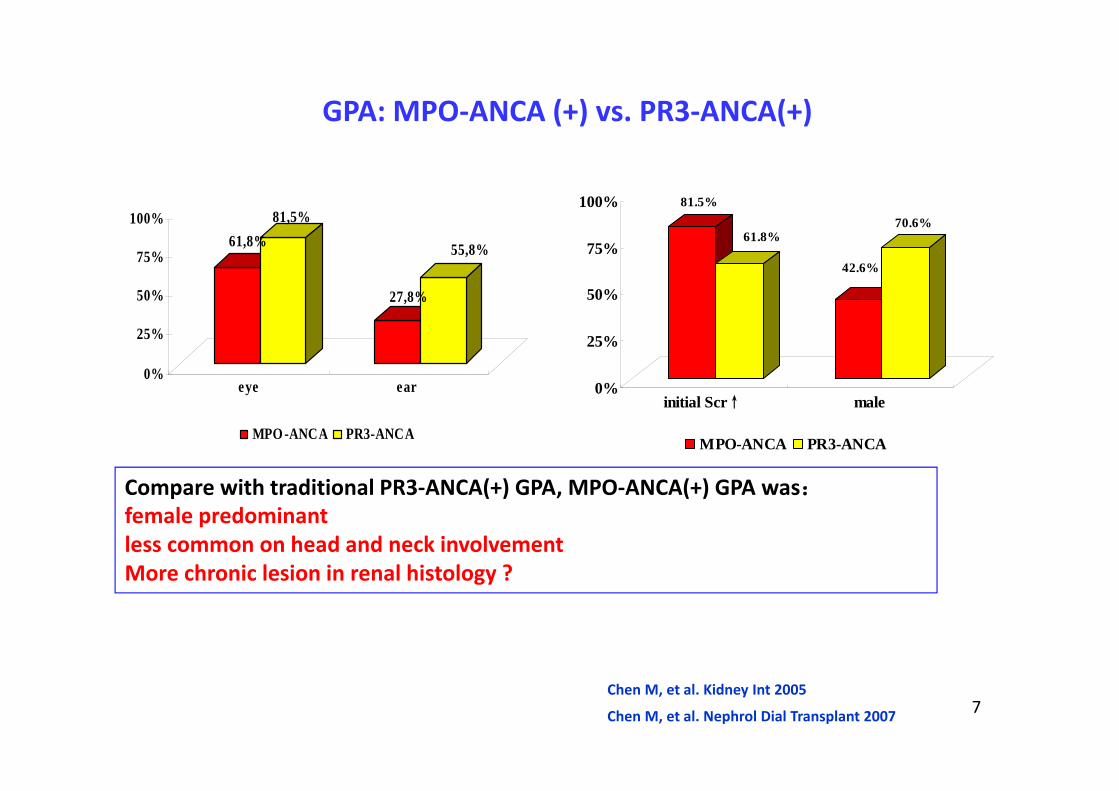
GPA: MPO‐ANCA (+) vs. PR3‐ANCA(+)
81.5%
61.8%
42.6%
70.6%
0%
25%
50%
75%
100%
initial Scr↑ male
MPO-ANCA PR3-ANCA
Chen M, et al. Kidney Int 2005
Chen M, et al. Nephrol Dial Transplant 2007
Compare with traditional PR3‐ANCA(+) GPA, MPO‐ANCA(+) GPA was:female predominantless common on head and neck involvementMore chronic lesion in renal histology ?
8
• General introduction of AAV in China– Disease spectrum and ANCA type
• Clinical and pathological study– Treatment and outcomes
• Pathogenic studies – Complement and neutrophils
Treatment• Induction therapy
– Corticosteroids plus CTX /Rituximab– Plasma exchange for severe ones
• Maintenance therapy– AZA– MMF– …
Dose of immunosuppressant is less than Caucasians
9
Outcomes
• Mortality• Relapse and treatment resistance• Renal outcomes
10
11
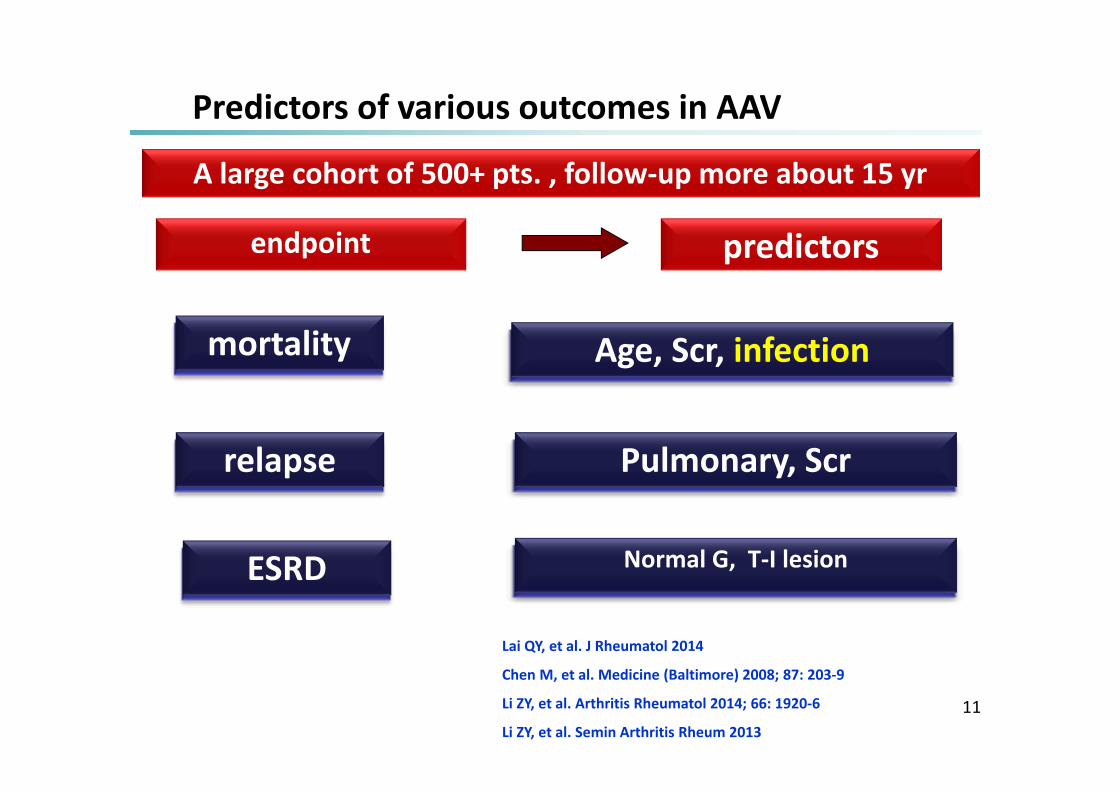
endpoint predictors
mortality
ESRD
relapse
Age, Scr, infection
Normal G, T‐I lesion
Pulmonary, Scr
Predictors of various outcomes in AAV
Lai QY, et al. J Rheumatol 2014
Chen M, et al. Medicine (Baltimore) 2008; 87: 203‐9
Li ZY, et al. Arthritis Rheumatol 2014; 66: 1920‐6
Li ZY, et al. Semin Arthritis Rheum 2013
A large cohort of 500+ pts. , follow‐up more about 15 yr
Mortality
• Study from EUVAS: early mortality is a crucial issue
– Active vasculitis per se
– Complication from heavy burden of immunosuppressive
therapy: esp. infection
Ann Rheum Dis 2009
13
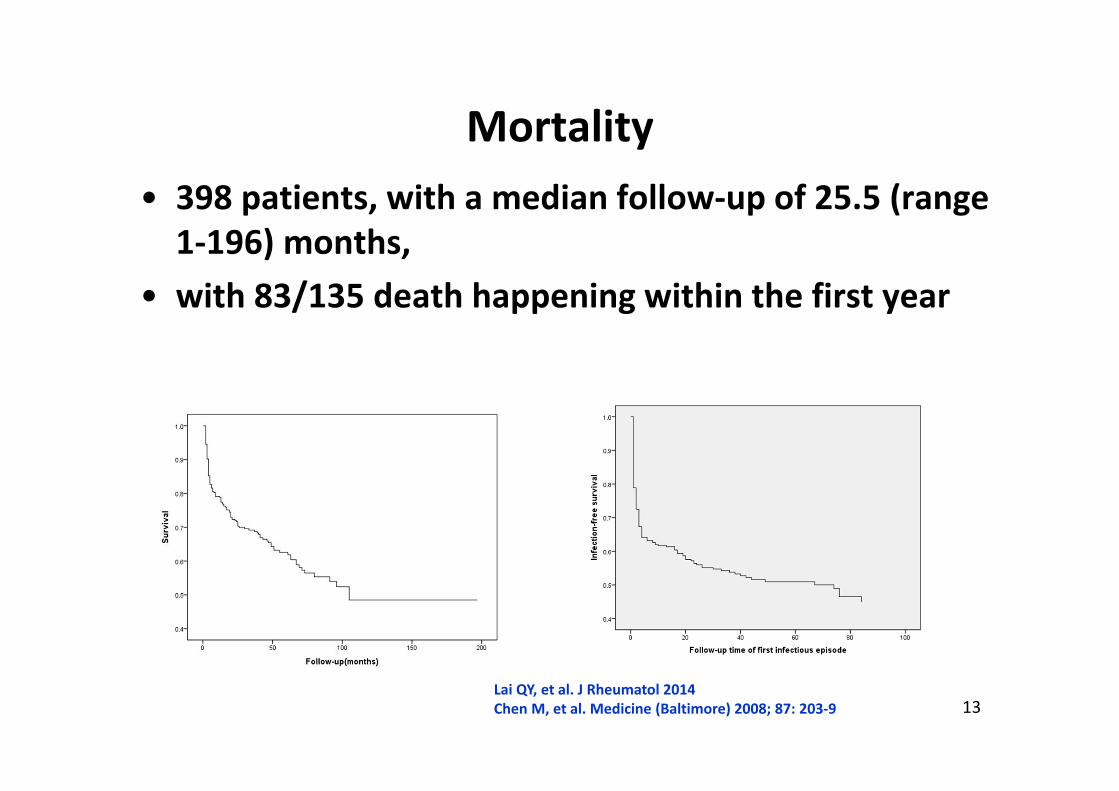
Mortality• 398 patients, with a median follow‐up of 25.5 (range 1‐196) months,
• with 83/135 death happening within the first year
Lai QY, et al. J Rheumatol 2014 Chen M, et al. Medicine (Baltimore) 2008; 87: 203‐9
14
• Predictors of all‐cause mortality:– older age (p<0.001),
– secondary infection (p<0.001)
– initial Scr (p<0.001)
• Leading cause of death– Within 1 year: secondary infection (53/153, 39.3%)
– After 1 year: cardiovascular events (15/53, 28.8%)
• Predictors of secondary infection– lymphocyte counts in the peripheral blood (p=0.004)
– basic pulmonary involvement of AAV (p<0.001)
– older age
Lai QY, et al. J Rheumatol 2014
Chen M, et al. Medicine (Baltimore) 2008; 87: 203‐9
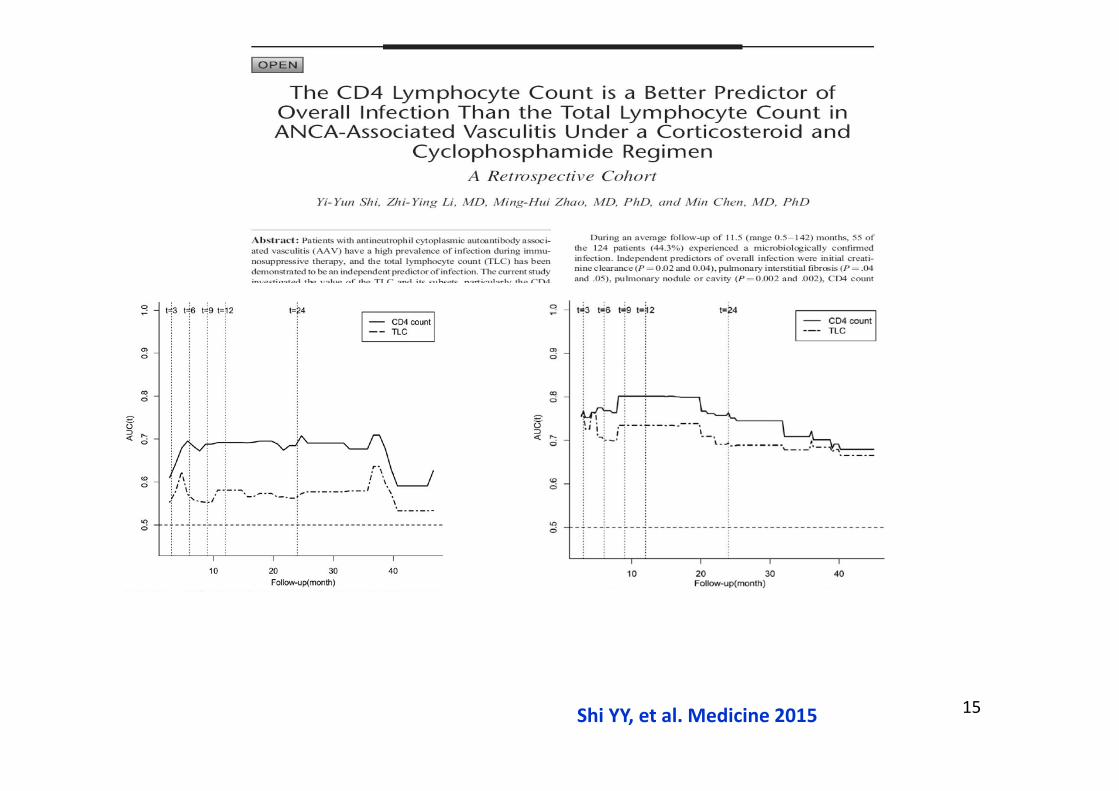
15Shi YY, et al. Medicine 2015
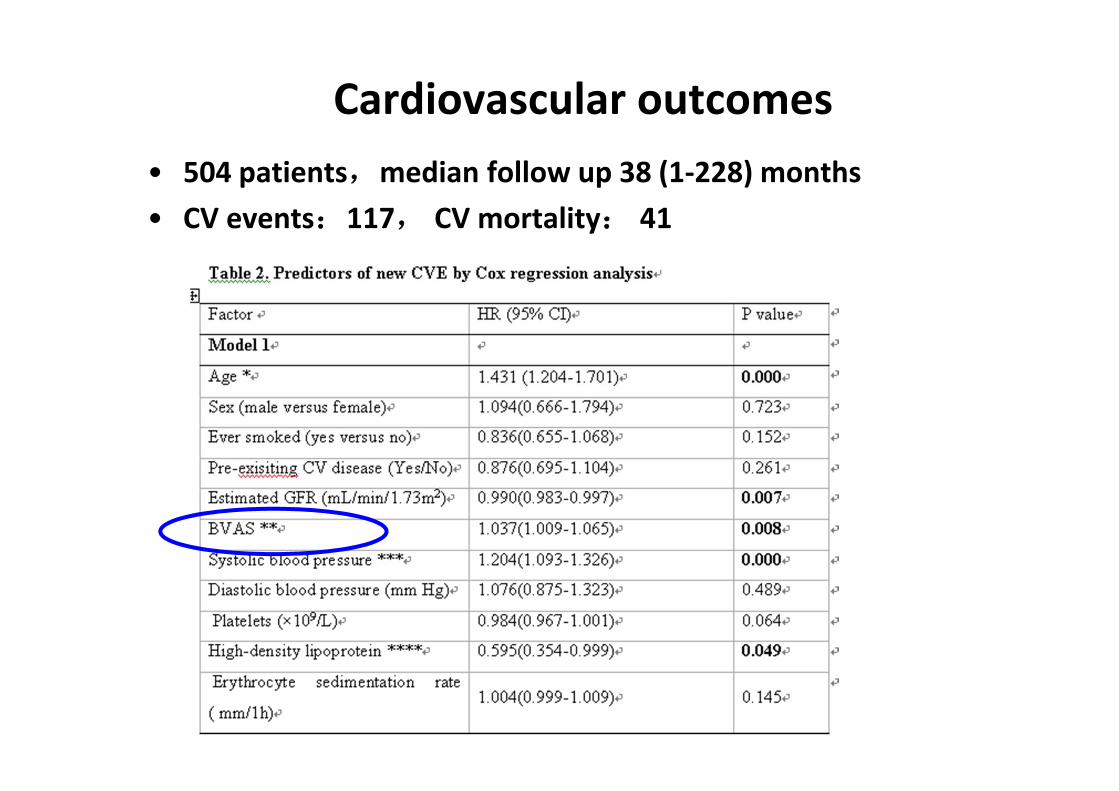
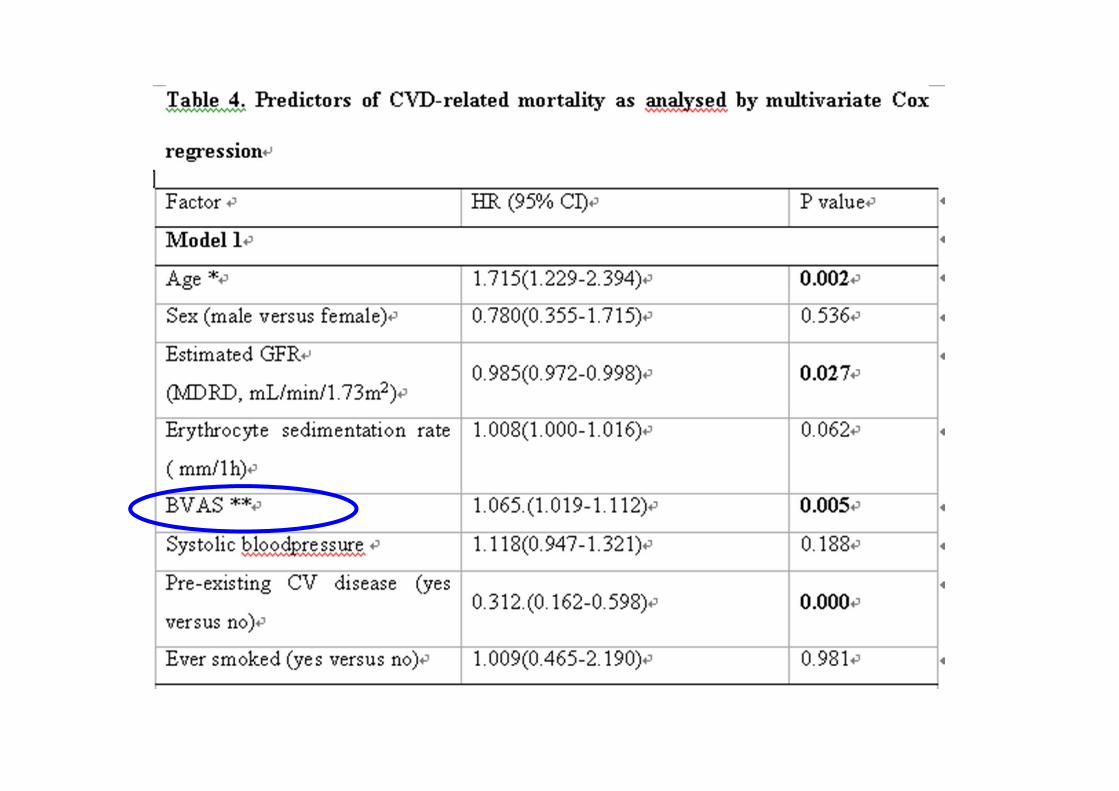
Cardiovascular outcomes• 504 patients,median follow up 38 (1‐228) months• CV events:117, CV mortality: 41
• Relapse is an independent predictor of ESRD
• Study from North Carolina and France– Predictors of relapse
• PR3-ANCA• Upper respiratory tract and lung involvement• Lung involvement
– Predictors of treatment resistance• Older age• Female• African American• MPO-ANCA• Poor renal function
Hogan SL, et al. Ann Intern Med. 2005;143:621-631.Pagnoux C, et al.. Arthritis Rheum. 2008;58:2908-2918.
Treatment resistance and relapse
19
• Our center: 439 AAV patients
• Treatment resistance: 47/439 (10.7%)– higher Scr (OR 1.087, 95%CI 1.001‐1.180, P=0.047)
– ESR level (OR 1.009, 95%CI 1.001‐1.018, P=0.025)
• Relapse: 128/392 in 48 (range 3‐171) months – lung involvement (HR 1.768, 95%CI 1.088‐2.872, P=0.021)
– lower Scr (HR 0.925, 95%CI 0.872‐0.981, P=0.009)
Treatment resistance and relapse
Li ZY, et al. Arthritis Rheumatol 2014; 66: 1920‐6
20
Predictors for renal restoration in severe ANCA‐GN
• 89 ANCA‐GN patients on dialysis at presentation• At the 6th month of treatment,
– 28.1% dialysis‐independent,– 50.6% ESRD,– 21.3% died, including 9/19 died from infection
• Predictor of renal restoration– Proportion of normal G – Extent of tubular atrophy and intersititial fibrosis
• Leading cause of death: infection
Li ZY, et al. Semin Arthritis Rheum 2013
21
Prospective
• How to control active AAV
• How to avoid infection
• Cardiovascular disease
• Malignancy
• Quality of life/mental health
• Biomarkers to predict disease severity/outcomes
22
• General introduction of AAV in China– Disease spectrum and ANCA type
• Clinical and pathological study– Treatment and outcomes
• Pathogenic studies – Complement activation
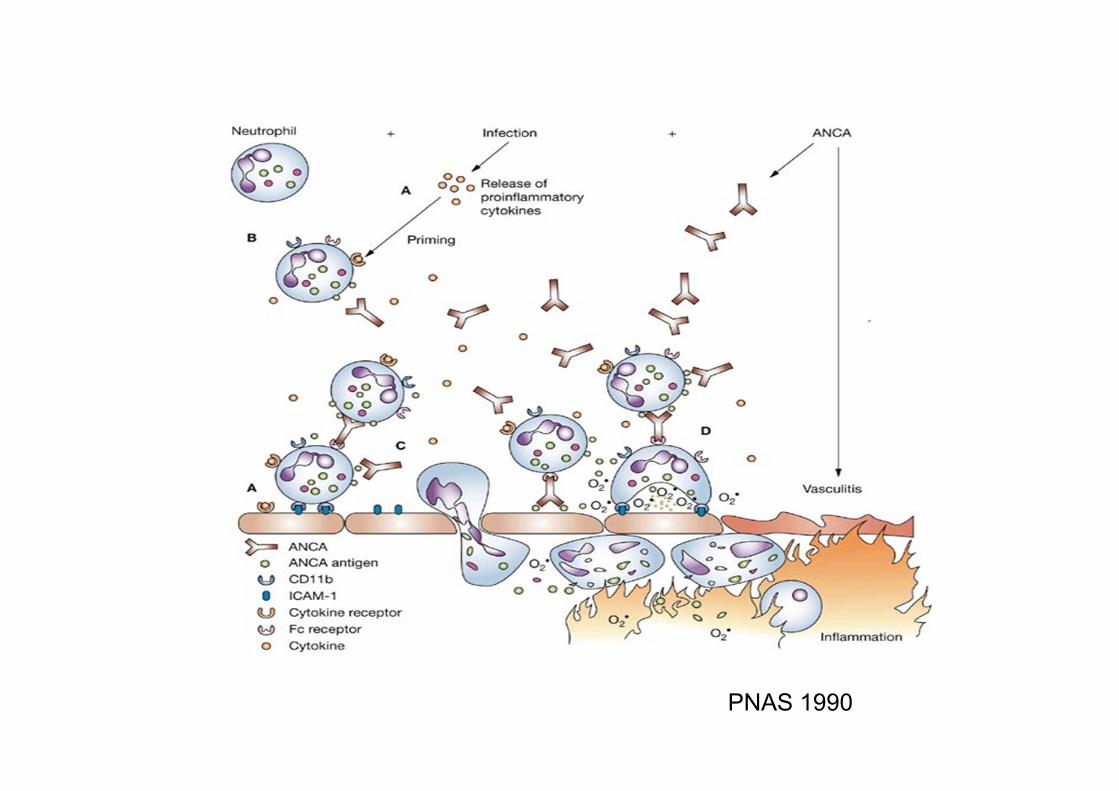
PNAS 1990
24
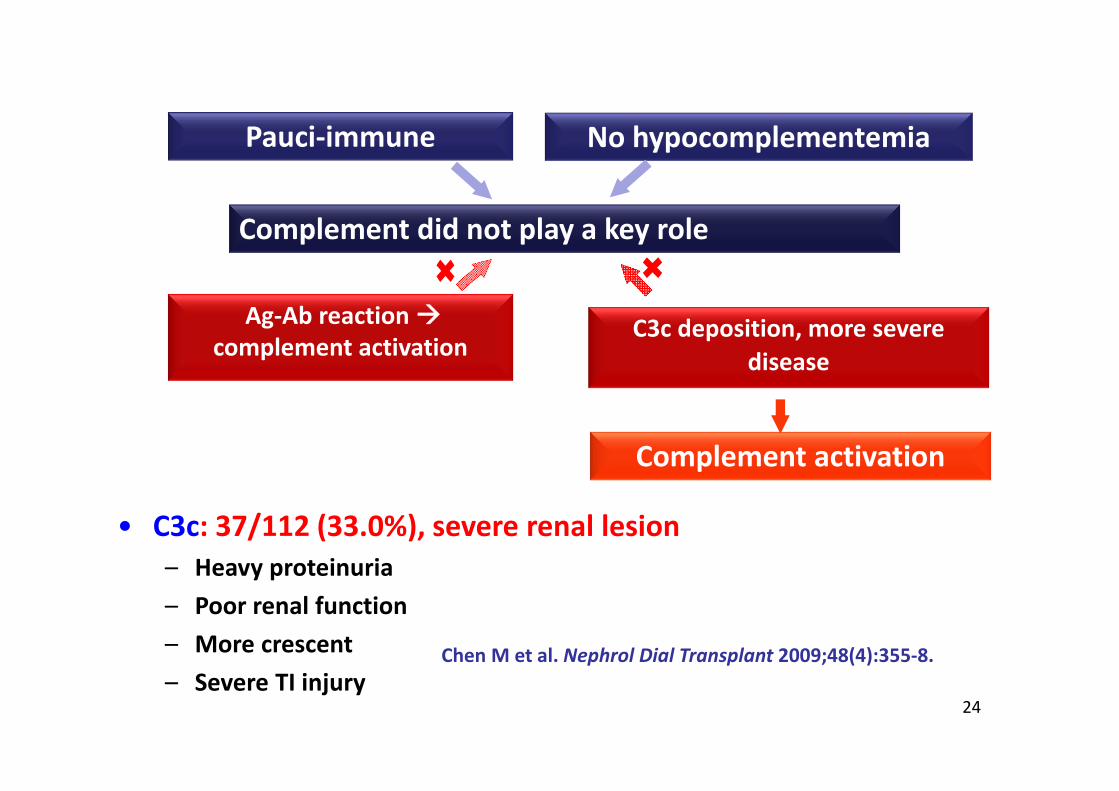
Complement did not play a key role
Ag‐Ab reaction complement activation
No hypocomplementemia Pauci‐immune
C3c deposition, more severe disease
Complement activation
• C3c: 37/112 (33.0%), severe renal lesion– Heavy proteinuria– Poor renal function– More crescent– Severe TI injury
Chen M et al. Nephrol Dial Transplant 2009;48(4):355‐8.
25
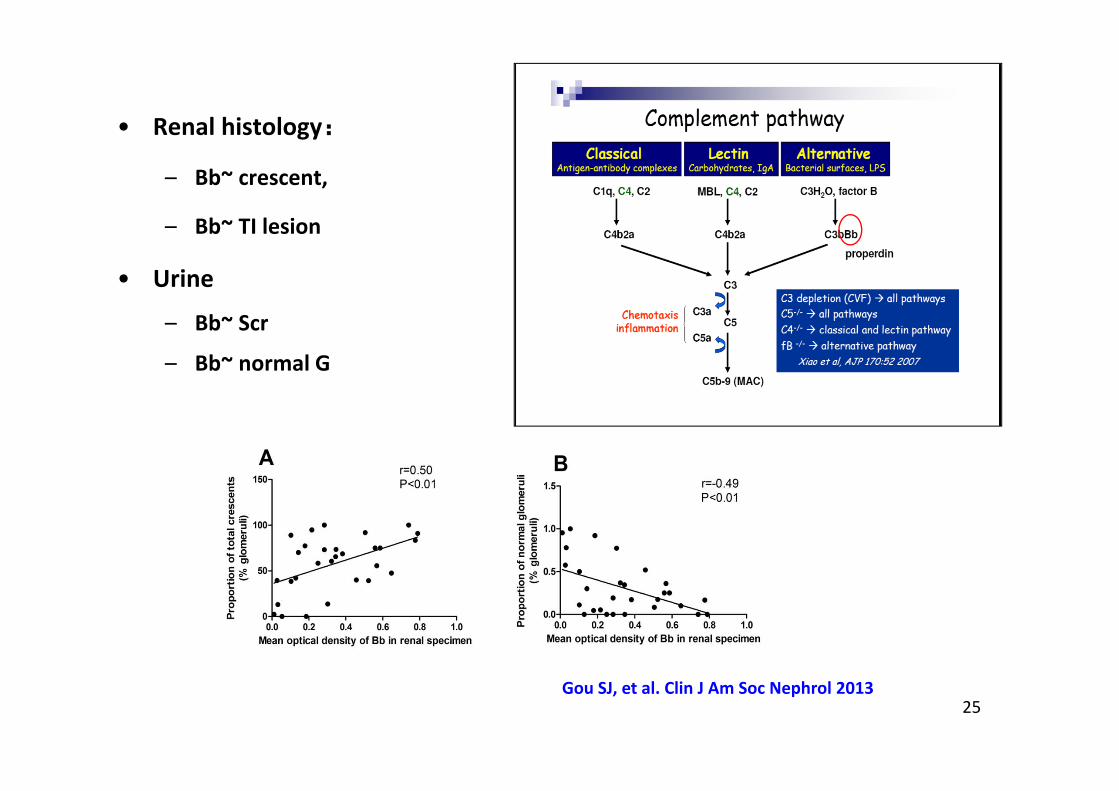
• Renal histology:
– Bb~ crescent,
– Bb~ TI lesion
• Urine
– Bb~ Scr
– Bb~ normal G
Gou SJ, et al. Clin J Am Soc Nephrol 2013
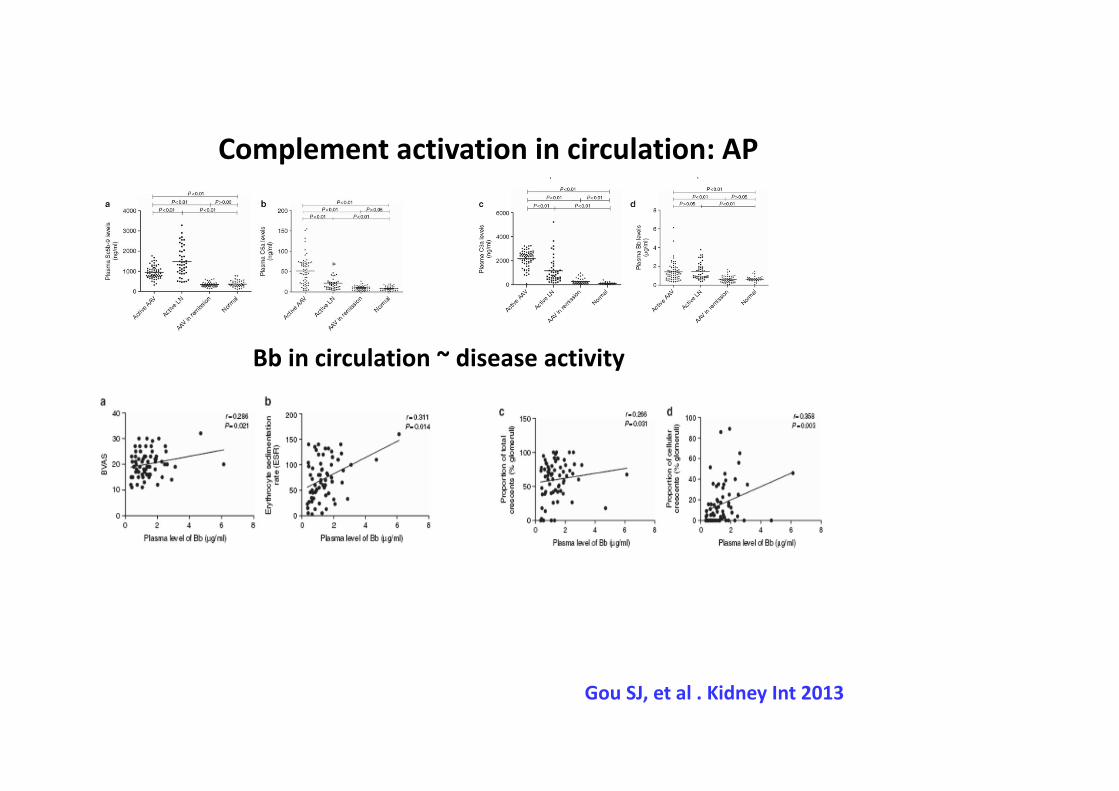
Bb in circulation ~ disease activity
Gou SJ, et al . Kidney Int 2013
Complement activation in circulation: AP
Chen SF, et al. Arthritis Res Ther 2015
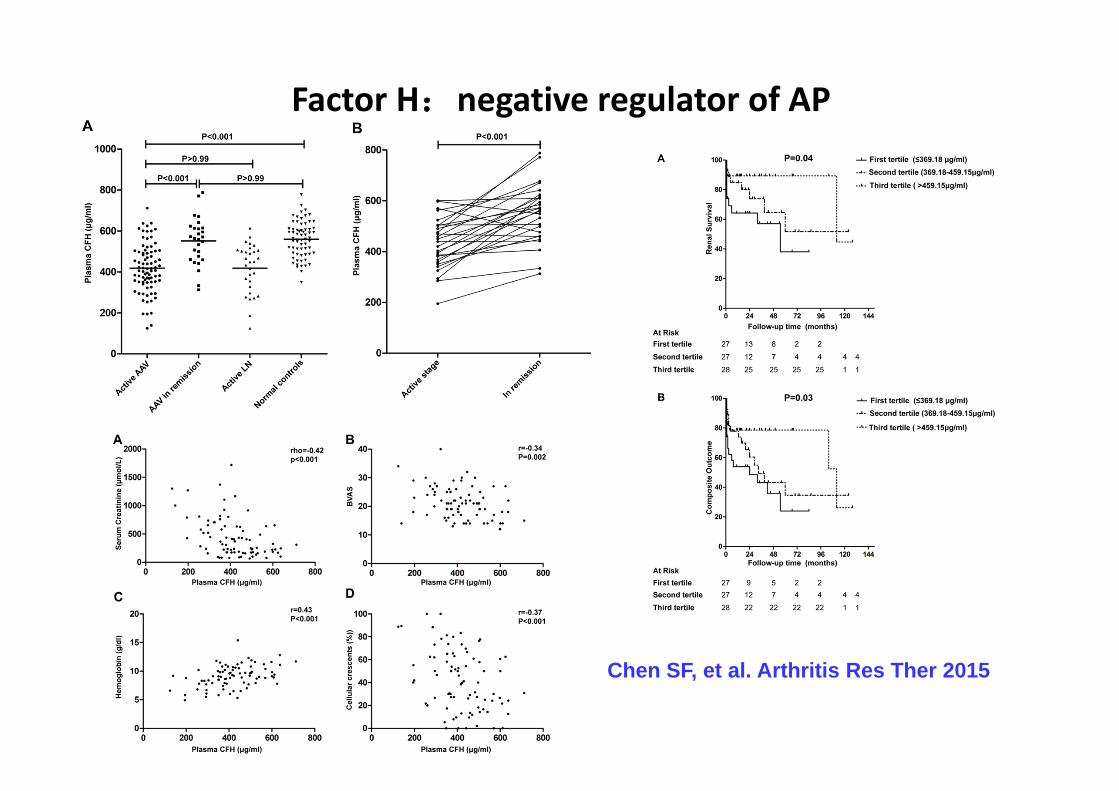
Factor H:negative regulator of AP
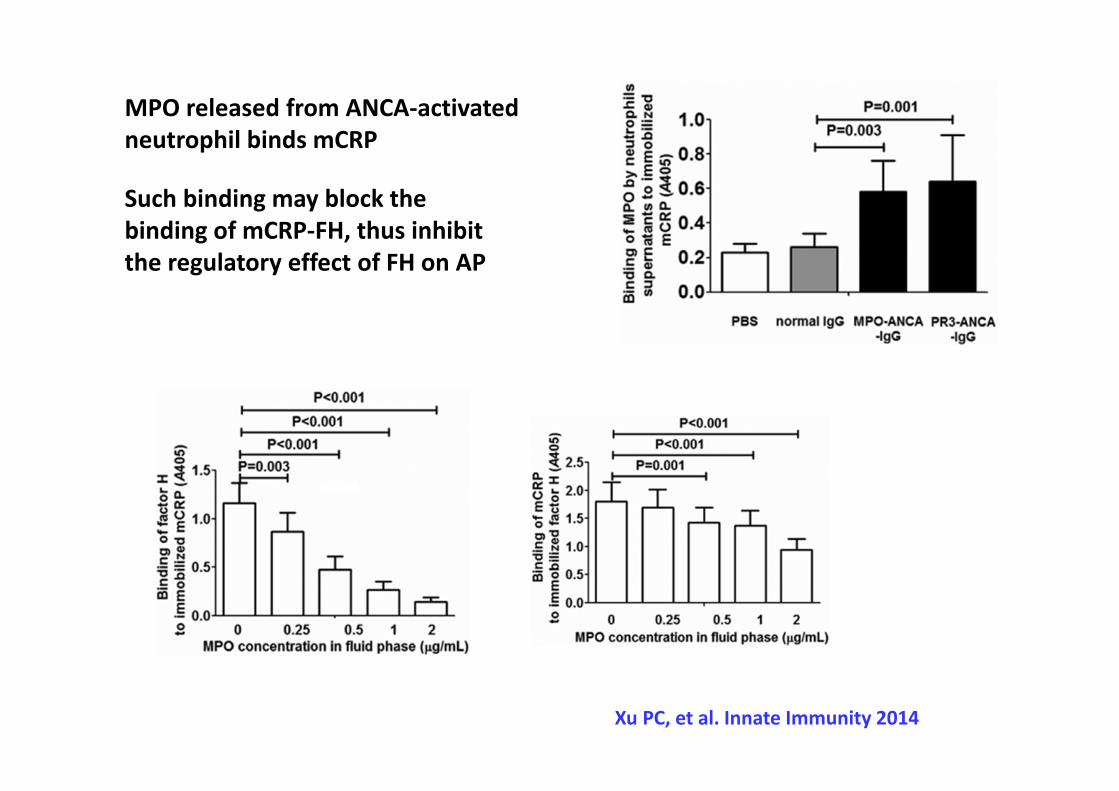
MPO released from ANCA‐activated neutrophil binds mCRP
Such binding may block the binding of mCRP‐FH, thus inhibit the regulatory effect of FH on AP
Xu PC, et al. Innate Immunity 2014
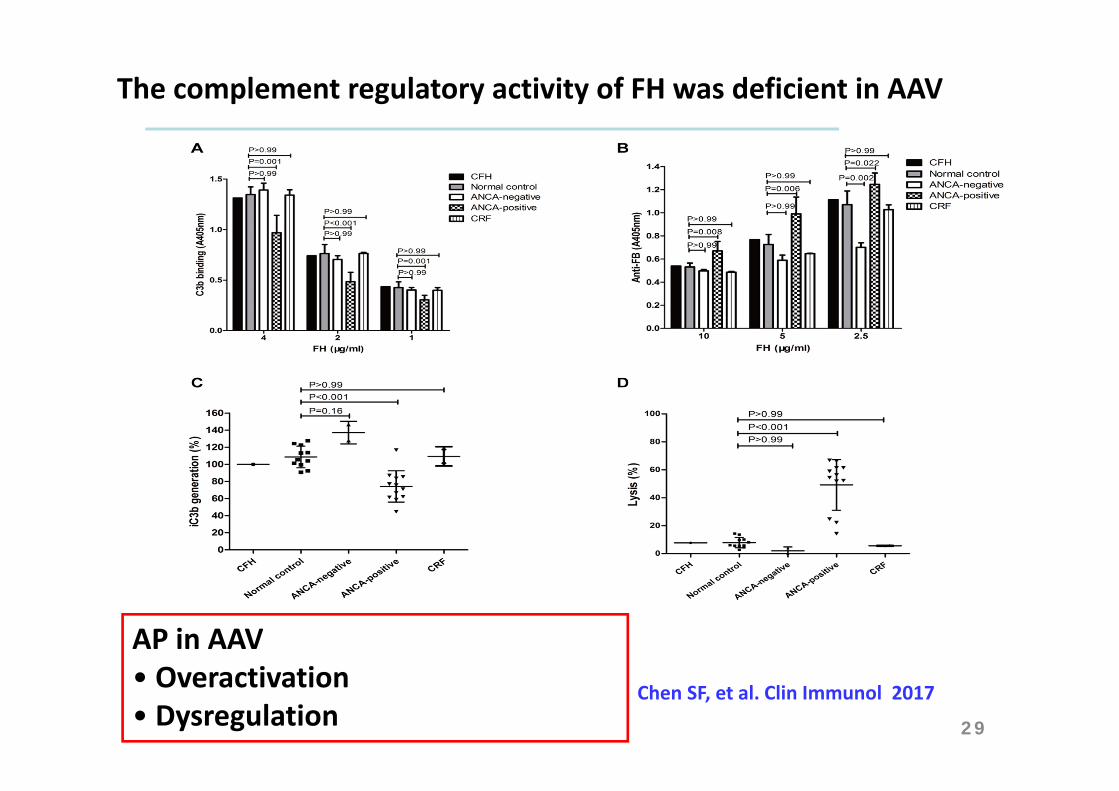
Chen SF, et al. Clin Immunol 2017
The complement regulatory activity of FH was deficient in AAV
29
AP in AAV• Overactivation• Dysregulation
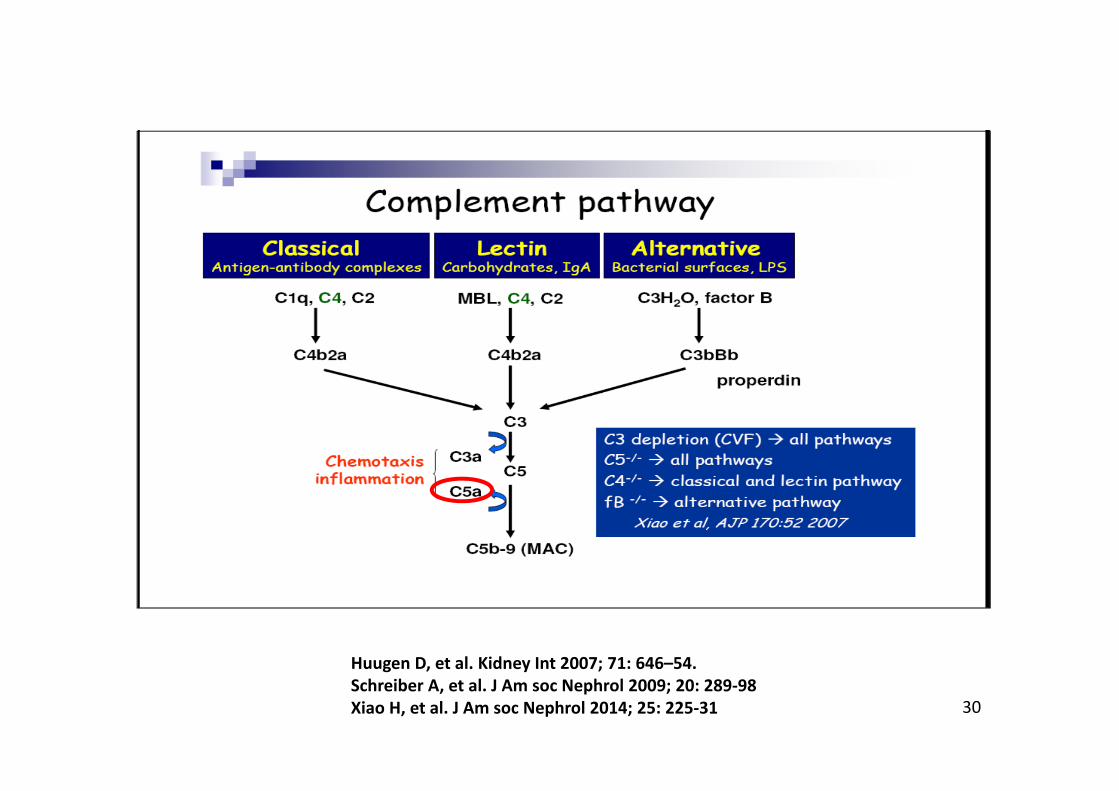
30
Huugen D, et al. Kidney Int 2007; 71: 646–54.Schreiber A, et al. J Am soc Nephrol 2009; 20: 289‐98Xiao H, et al. J Am soc Nephrol 2014; 25: 225‐31
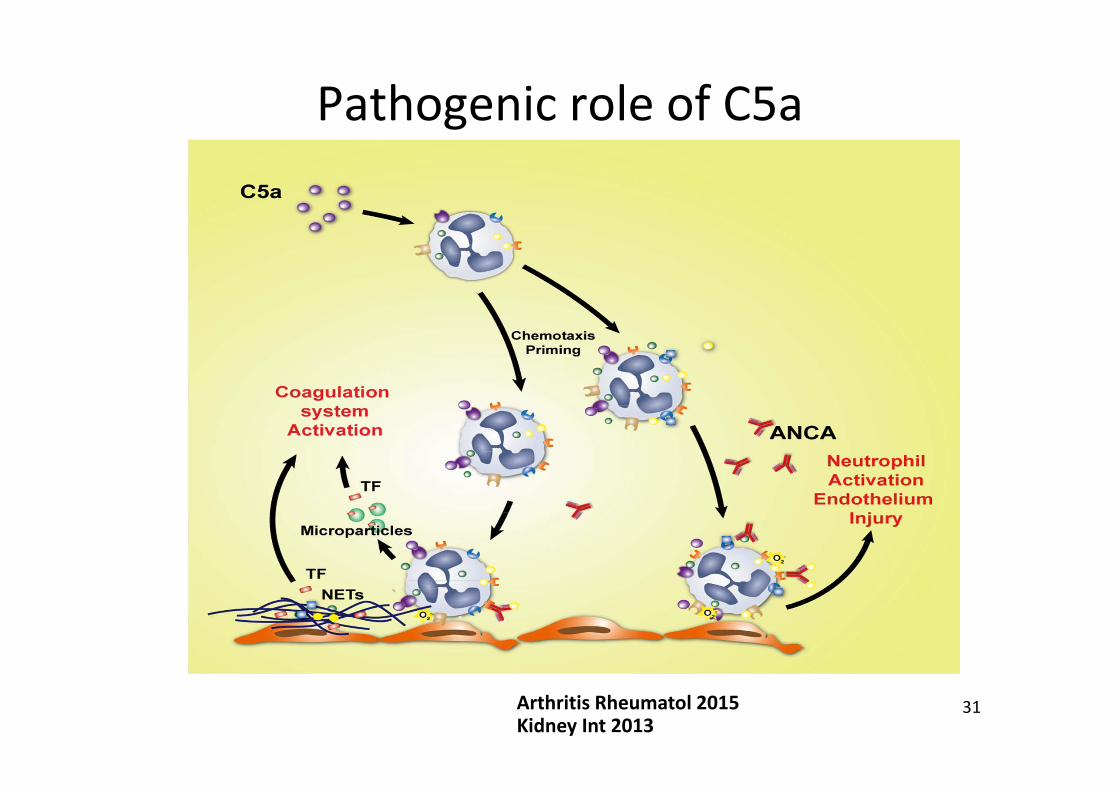
31
Pathogenic role of C5a
Kidney Int 2013Arthritis Rheumatol 2015
32
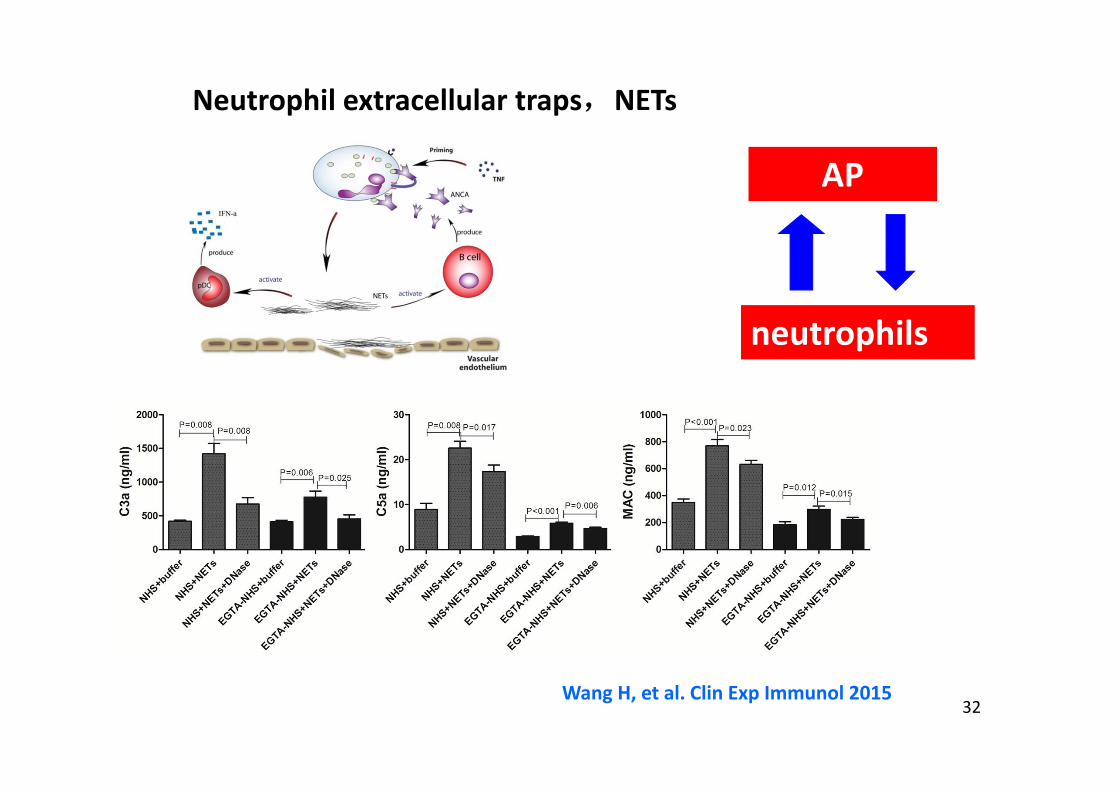
Neutrophil extracellular traps,NETs
AP
neutrophils
Wang H, et al. Clin Exp Immunol 2015
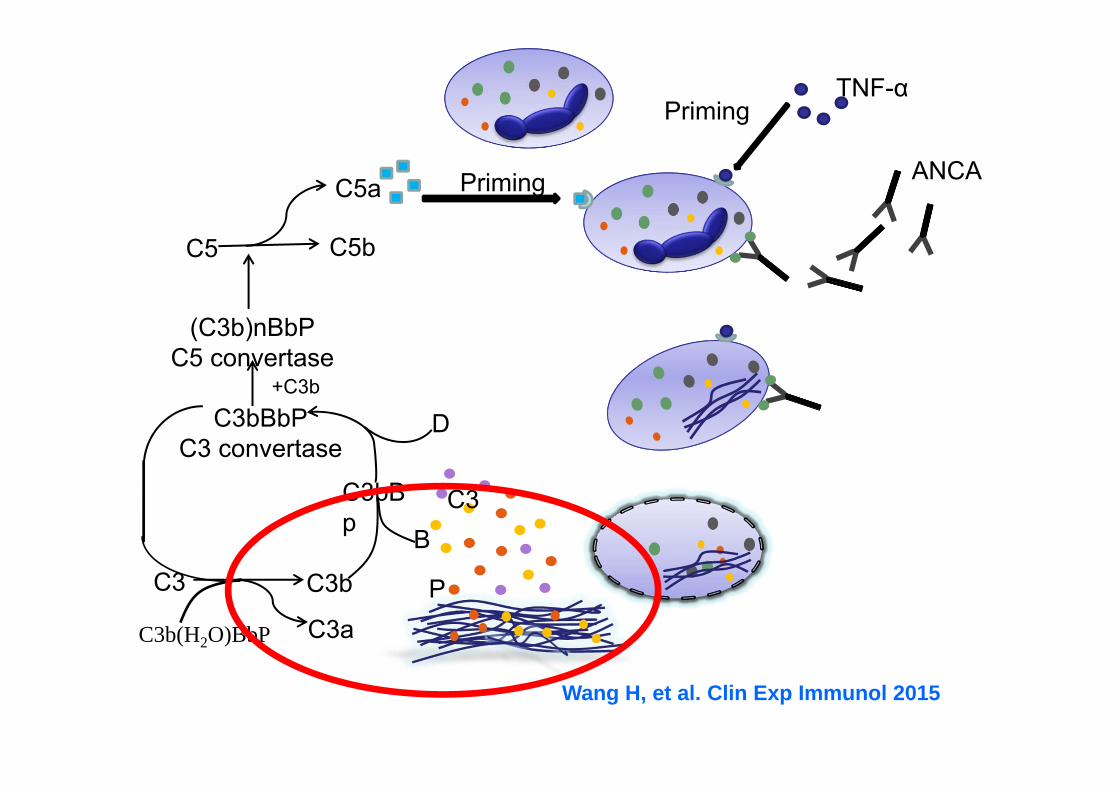
PrimingTNF-α
ANCAPrimingC5a
BC3
PC3bC3
C3b(H2O)BbP C3a
C3bBp
C3bBbPC3 convertase
D
C5bC5
+C3b
(C3b)nBbPC5 convertase
Wang H, et al. Clin Exp Immunol 2015
• CCX168 successfully replaced glucocorticoid treatment, with a more rapid onset of action based on
– BVAS, – UACR, – HRQOL,– a lower incidence of steroid-related adverse effects.
Jayne D et al. J Am Soc Nephrol 2017
(1) prednisone 60mg/day,
(2) CCX168 30 mg b.i.d.+ prednisone 20 mg
(3) CCX168 30 mg b.i.d.
+ CTX or RTX
C5aR/CD88 small molecule antagonist CCX168 in AAV: The CLEAR trial
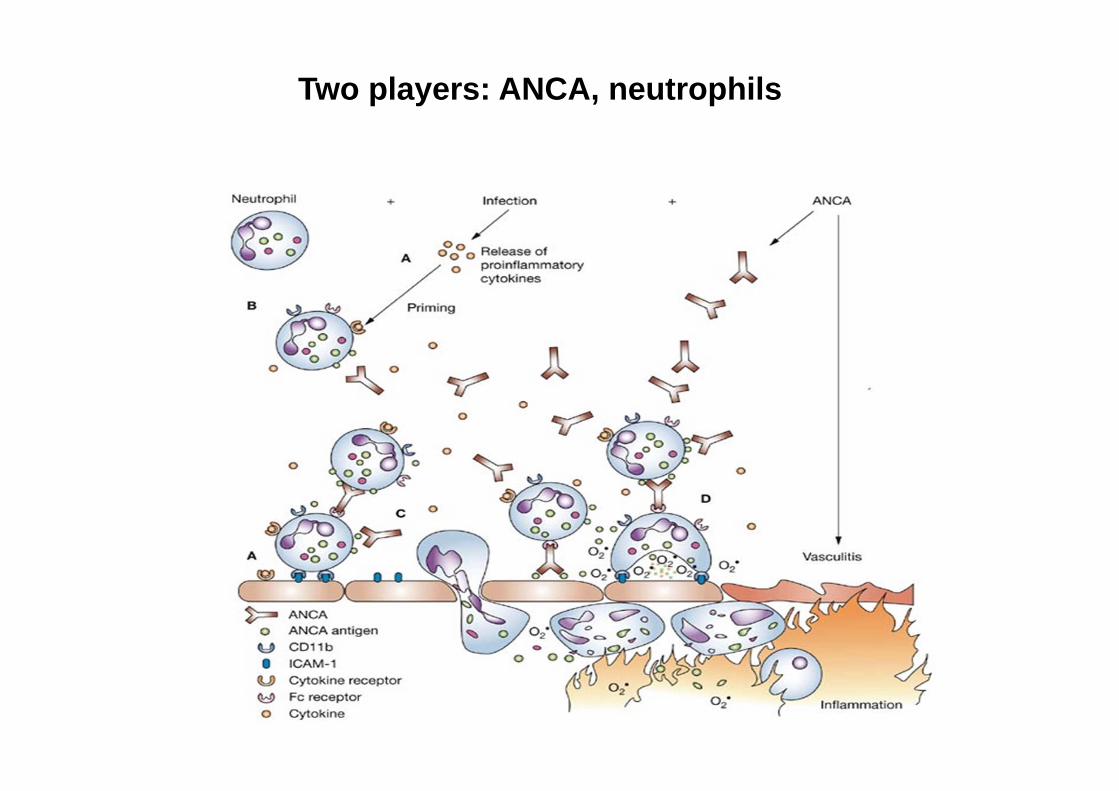
Two players: ANCA, neutrophils
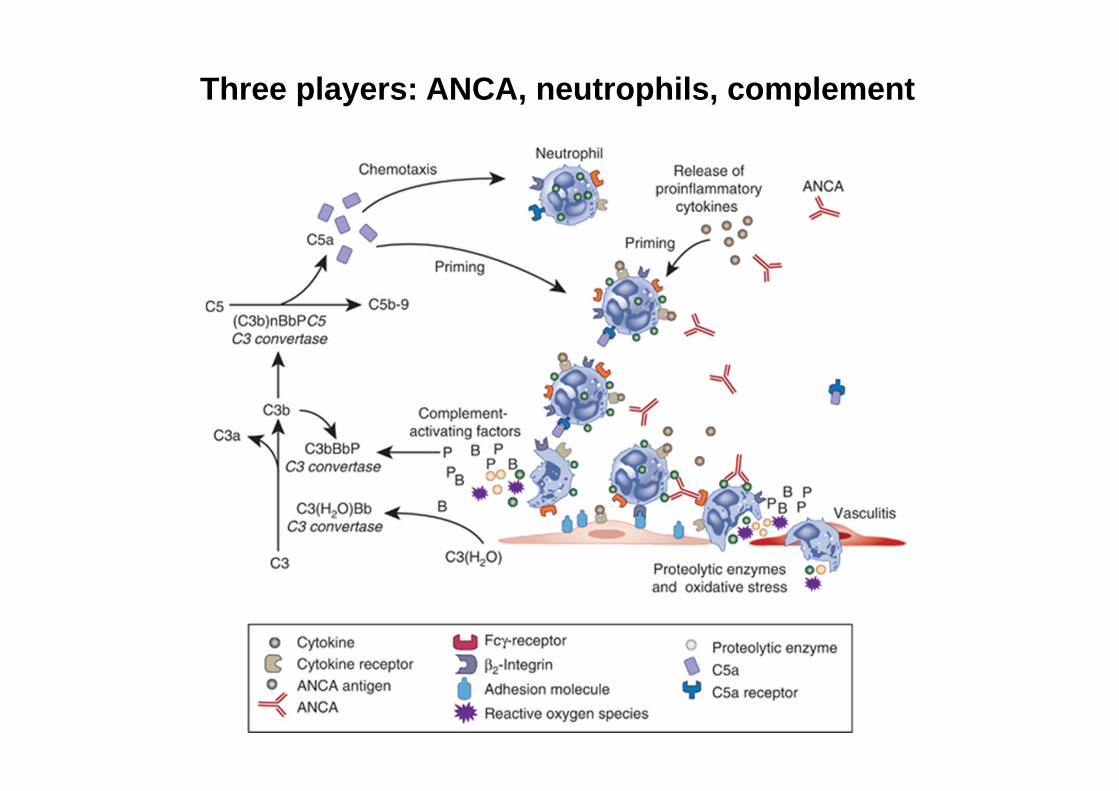
Three players: ANCA, neutrophils, complement
Take home message
• AAV is a group of common autoimmune disease in China, MPO‐AAV is the most common type
• Pred + CTX is the mainstay of treatment, secondary infection the main cause of death nowadays.
• Complement activation is a crucial aspect in the pathogenesis and treatment target

38