Embed Size (px)
Citation preview

Nicolas Kluger, MD PhDDermatology, Helsinki University Central [email protected]
16 March 2019 SNNDV
ANCA associated vasculitides&
Polyarteritis nodosa

2012 Revised Chapel Hill Consensus
Jennette JC, et al. Arthritis Rheum 1994; 37: 187-92Jennette JC, et al. Arthritis Rheum 2013;65:1-11.
CHCC is a nomenclature system
It is not a diagnostic or a classification system
All 3 major categories can affect any size artery

All intraparenchymal vessels (intraparenchymal arteries, arterioles, capillaries, venules and veins) are small vessels
Small biopsies usually contain only small vessels(even the ”largest” ones in the specimen)
In the skin, there are only small vessels !
Jennette JC, et al. Arthritis Rheum 2013;65:1-11.

• Skin-limited vasculitis• Skin-dominant vasculitis variants
Sunderkötter CH, et al. Arthritis Rheum 2018;70:171-184.
SPECIAL ARTICLE
Nomenclature of Cutaneous VasculitisDermatologic Addendum to the 2012 Revised International Chapel Hill
Consensus Conference Nomenclature of Vasculitides
Cord H. Sunderk€otter,1 Bernhard Zelger,2 Ko-Ron Chen,3 Luis Requena,4 Warren Piette,5
J. Andrew Carlson,6 Jan Dutz,7 Peter Lamprecht,8 Alfred Mahr ,9 Elisabeth Aberer,10
Victoria P. Werth,11 David A. Wetter,12 Seiji Kawana,13 Raashid Luqmani,14 Camille Frances,15
Joseph Jorizzo,16 J. Richard Watts,17 Dieter Metze,18 Marzia Caproni,19 Erkan Alpsoy,20
Jeffrey P. Callen,21 David Fiorentino,22 Peter A. Merkel,23 Ronald J. Falk,24 and J. Charles Jennette24
Objective. To prepare a dermatologic addendumto the 2012 revised International Chapel Hill ConsensusConference Nomenclature of Vasculitides (CHCC2012) toaddress vasculitides affecting the skin (D-CHCC). The goalwas to standardize the names and definitions for cutaneousvasculitis.
Methods. A nominal group technique with a facili-tator was used to reach consensus on the D-CHCC nomen-clature, using multiple face-to-face meetings, e-maildiscussions, and teleconferences.
Results. Standardized names, definitions, and de-scriptions were adopted for cutaneous components of sys-temic vasculitides (e.g., cutaneous IgA vasculitis as acomponent of systemic IgA vasculitis), skin-limited variantsof systemic vasculitides (e.g., skin-limited IgA vasculitis,
drug-induced skin-limited antineutrophil cytoplasmic anti-body–associated vasculitis), and cutaneous single-organ vas-culitides that have no systemic counterparts (e.g., nodularvasculitis). Cutaneous vasculitides that were not includedin the CHCC2012 nomenclature were introduced.
Conclusion. Standardized names and definitionsare a prerequisite for developing validated classificationand diagnostic criteria for cutaneous vasculitis. Accurateidentification of specifically defined variants of systemicand skin-limited vasculitides requires knowledgeableintegration of data from clinical, laboratory, and patho-logic studies. This proposed nomenclature of vas-culitides affecting the skin, the D-CHCC, provides astandard framework both for clinicians and forinvestigators.
Supported in part by the European Academy of Dermatologyand Venereology (grant 2014-028; Project on Nomenclature andDiagnostic Criteria of Cutaneous Vasculitis).
1Cord H. Sunderk€otter, MD: University Hospital of Halle,Halle (Saale), Germany, and University of M€unster, M€unster, Germany;2Bernhard Zelger, MD: Medical University Innsbruck, Innsbruck, Aus-tria; 3Ko-Ron Chen, MD, PhD: Meguro Chen Dermatology Clinic,Tokyo, Japan; 4Luis Requena, MD: Universidad Aut"onoma, Madrid,Spain; 5Warren Piette, MD: John H. Stroger Jr. Hospital of CookCounty and Rush University Medical Center, Chicago, Illinois;6J. Andrew Carlson, MD: Albany Medical College, Albany, New York;7Jan Dutz, MD, FRCPC: University of British Columbia, Vancouver,British Columbia, Canada; 8Peter Lamprecht, MD: University ofL€ubeck, L€ubeck, Germany; 9Alfred Mahr, MD, PhD: Hospital Saint-Louis, University Paris 7, Paris, France; 10Elisabeth Aberer, MD: Medi-cal University of Graz, Graz, Austria; 11Victoria P. Werth, MD: Univer-sity of Pennsylvania and Corporal Michael J. Crescenz Veterans AffairsMedical Center, Philadelphia, Pennsylvania; 12David A. Wetter, MD:Mayo Clinic, Rochester, Minnesota; 13Seiji Kawana, MD, PhD: Nip-pon Medical School, Tokyo, Japan; 14Raashid Luqmani, DM: Univer-sity of Oxford, Oxford, UK; 15Camille Frances, MD: University Paris 6,Hopital Tenon, Paris, France; 16Joseph Jorizzo, MD: Wake ForestSchool of Medicine, Winston Salem, North Carolina; 17J. Richard
Watts, MD: Ipswich Hospital NHS Trust, Ipswich, UK, and NorwichMedical School University of East Anglia, Norwich, UK; 18DieterMetze, MD: University of M€unster, M€unster, Germany; 19MarziaCaproni, MD: University of Florence, Florence, Italy; 20Erkan Alpsoy,MD: Akdeniz University School of Medicine, Antalya, Turkey; 21JeffreyP. Callen, MD: University of Louisville, Louisville, Kentucky; 22DavidFiorentino, MD, PhD: Stanford University School of Medicine, Stanford,California; 23Peter A. Merkel, MD, MPH: University of Pennsylvania,Philadelphia; 24Ronald J. Falk, MD, J. Charles Jennette, MD: Universityof North Carolina at Chapel Hill.
Dr. Sunderk€otter has received consulting fees and/or speak-ing fees from Pfizer, Actelion, Janssen, and Novartis (less than$10,000 each). Dr. Jorizzo has received consulting fees from Amgen(less than $10,000). Dr. Jennette has received consulting fees, speak-ing fees, and/or honoraria from Genentech (more than $10,000).
Address correspondence to Cord H. Sunderk€otter, MD,Department of Translational Dermatoinfectiology, University of Mün-ster and Department of Dermatology, University Hospital of Halle,Ernst-Grube-Strasse 40, 06120 Halle (Saale), Germany. E-mail:[email protected].
Submitted for publication June 24, 2017; accepted in revisedform November 8, 2017.
171
ARTHRITIS & RHEUMATOLOGYVol. 70, No. 2, February 2018, pp 171–184DOI 10.1002/art.40375© 2017, American College of Rheumatology
The cutaneous component of systemic vasculitides,as well as skin-limited variants of systemic vasculitides andSOVof the skin, are defined and described in Tables 2–5.To conclude that a patient fulfills the definition of skin-limited vasculitis or cutaneous SOV in a clinical setting,there must be no detectable involvement of another, non-cutaneous organ by vasculitis.
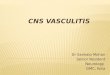
The CHCC work group’s definition of skin includesthe panniculus (subcutis) and mucosa, although mostvasculitides that are restricted to the skin do not affectthe mucosa. The skin has small arteries, arterioles, capillar-ies, venules, and small veins (Figure 1). CHCC2012 distin-guishes small vessels from medium vessels based onstructure and function, rather than diameter. Small vessels
are intraparenchymal arteries, arterioles, capillaries,venules, and veins, while medium vessels comprise mainvisceral arteries and veins and their initial branches. Thelargest arteries and veins in the septae of the panniculusare medium vessels. The histopathologic features of cuta-neous vasculitis are influenced by treatment and durationof time since onset. Demonstration of, e.g., leukocytoclasticimmune complex vasculitis (LCV) in a biopsy specimen isbest achieved by selecting a lesion that is between 24 and48 hours old. Immunofluorescence analysis for demonstra-tion of immunoreactants in dermal vessels ideally requiresbiopsy of an early or histamine-induced lesion, becauseimmunoglobulins may disappear over time (2,3).
Large vessel vasculitis
Large vessel vasculitis (LVV) affects large arteriesmore often than other vasculitides (Table 2). Large arter-ies are defined as the aorta and its major branches,although arteries of any size may be affected. There areno large arteries in the dermis or subcutaneous tissues;however, as illustrated in Figure 1, LVV can involve me-dium vessels, and even small vessels. The 2 major formsof LVVare Takayasu arteritis (TAK) and giant cell arteri-tis (GCA). No cutaneous vasculitis has been reported inTAK, although nonvasculitic dermatoses may occur.
In most cases of GCA, vessels of the skin are notaffected; however, occlusion of inflamed extracutaneousarteries that feed the skin or the mucosa results innecrosis of supplied tissue, e.g., tongue necrosis due toarteritis of the lingual artery (4). There are single casereports of GCA affecting small arteries in the panniculus (5).
Medium vessel vasculitisMedium vessel vasculitis (MVV) predominantly
affects medium arteries, although arteries of any size maybe affected (Table 3 and Figure 1). Since both some small
Table 2. Systemic and cutaneous variants of large vessel vasculitis*
CHCC2012vasculitis name
AbbreviatedCHCC2012 definition
Cutaneous component ofsystemic vasculitis
Skin-limited orskin-dominant variant
Takayasu arteritis Arteritis, often granulomatous,predominantly affecting the aorta and/orits major branches; onset at age <50 years
No definite vasculitic lesions in the skin None
Giant cell arteritis Arteritis, often granulomatous, usuallyaffecting the aorta and/or its majorbranches, with a predilection for thebranches of the carotid and vertebralarteries; onset at age >50 years
Occlusive vasculitis of extracutaneousarteries, possibly leading to cutaneousinfarction; very rare involvement of smallarteries in subcutis or submucosa
None
* Large vessel vasculitis affects large arteries more often than other vasculitides. Large arteries are the aorta and its major branches. Anysize artery may be affected. The 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides (CHCC2012)definitions are detailed in ref. 1.
Figure 1. Distribution of vessel involvement in large vessel vasculitis(LVV), medium vessel vasculitis (MVV), and small vessel vasculitis(SVV). The heights of the trapezoids indicate the predilections of thedifferent categories of vasculitis for different types of vessels. Thebrackets delineate the types of vessels in the dermis, subcutis, andadjacent tissues. Not shown is variable vessel vasculitis, which canaffect any type of vessel, from aorta to veins. Note that LVV, MVV,and SVV are not confined to large, medium, or small vessels. Vasculi-tis in the dermis is most likely to be SVV, and LVV and MVV aremore often seen in the subcutaneous tissue and adjacent soft tissuethan in the dermis.
NOMENCLATURE OF CUTANEOUS VASCULITIDES (D-CHCC) 173

• Retrospective review withcutaneous vasculitisconfirmed by biopsy (2000-2010)
• n=112– n=62 (55%) with an
underlying cause– ANCA-associated vasculitis
n=4 (6%) • 3 GPA, 1 cANCA
Bouiller et al. Medicine 2016

A definite diagnosis of vasculitis requires
Histology in almost all cases
Clinical history
Physical findingsLaboratoryfindings
+/- angiographicfeatures

ANTI-NEUTROPHILS CYTOPLASMIC ANTIBODIESANCA associated vasculitides and Polyarteritis Nodosa

Bossuyt X et al. Revised 2017 international consensus on testing of ANCAs in granulomatosis with polyangiitis and microscopic polyangiitis Nat. Rev. Rheumatol 2017
ANCAs are best demonstrated by using a combination of IIF and immunoassay (PR3-ANCA or MPO-ANCA) and that IIF must be performed on all serum samples of patients suspected of having AAV1. Serum samples containing ANCAs by IIF should then be tested for PR3-ANCAs and MPO-ANCAs1. The testing algorithm proposed by this consensus was validated in 2002 in a meta-analysis study, leading to the conclusion that com-bining results obtained by IIF and ELISA (combining either C-ANCA and PR3-ANCA or P-ANCA and MPO-ANCA findings) optimizes the diagnostic performance of ANCA testing for AAV26.
Incorporation of ANCA tests in clinical decisions. In the early 1990s, classification criteria and nomenclature for the small-vessel vasculitides were assigned by the American College of Rheumatology27,28 and the Chapel Hill Consensus Conference (CHCC), respectively29. These criteria were based on clinical manifestations and hallmark pathological features of tissue biopsy samples, but did not incorporate ANCA testing. Small-vessel vas-culitides were originally considered to be only ANCA-associated, but subsequent animal model studies showed that ANCAs also have pathogenic potential30,31, which was clearly demonstrated for MPO-ANCAs in 2002 (REF. 32), and later indirectly for PR3-ANCAs33. The fact that different approaches were needed to demonstrate the pathogenic potential of MPO-ANCAs and PR3-ANCAs in these studies increased the awareness that instead of distinguishing between patients with GPA, MPA and EGPA, differentiating between patients with MPO-ANCAs or PR3-ANCAs might be more clinically rel-evant34–37. This notion was underscored in 2012 by the finding that these autoantibodies can be used to differ-entiate between genetically distinct subsets of patients with AAV38. The combined potential pathogenic role of these auto antibodies32,33 and the good test performances of the ANCA-assays26, formed the basis for incorporating ANCAs into nomenclature criteria; in the 2012 CHCC update on the nomenclature of the vasculitides, AAV was included as a category of vasculitis39. Importantly, CHCC is a nomenclature system, not a classification system or a diagnostic system, and at present there are no vali-dated diagnostic criteria for AAV. ANCA detection was included as part of a consensus methodology developed in 2007 for the classification of AAV and polyarteritis nodosa in epidemiological studies40, and EULAR have pointed to considering ANCA in diagnostic and classification criteria for systemic vasculitis41.
Novel technical developments in ANCA detection. Since the description of the first commercial ANCA ELISA in 1990 (REF. 42), an increasing number of com-mercial ANCA assays have become available. ELISAs have evolved in the way in which antigens are cou-pled to the carrier: from direct antigen binding (first generation ELISA) to capture-based antigen binding (second generation ELISA) and anchor-based antigen binding (third generation ELISA)2,3,43–48. Similarly, IIF has also undergone technical innovations: neutrophil substrates have been combined with antigen-specific
Figure 1 | Historical landmarks of ANCA-testing in small vessel vasculitis. In the past 25 years, substantial progress has been made in the development of assays for detecting anti-neutrophil cytoplasmic antibodies (ANCAs). Achievements have been made in antigen characterization (indicated in green), in the standardization of ANCA assays (indicated in blue), in incorporation of ANCAs in nomenclature and classification proposals (indicated in pink) and in ANCA technology (indicated in grey). Consensus statements on ANCA testing are indicated in orange. In this timeline, the dates for the distinct assays formats concern the publications of commercially available immunoassays. CHCC, Chapel Hill Consensus Conference; C-ANCA, cytoplasmic ANCA staining pattern; ELISA, enzyme-linked immunosorbent assay; GPA, granulomatosis with polyangiitis; IIF, indirect immunofluorescence; MPO, myeloperoxidase; PR3, proteinase 3; P-ANCA, perinuclear ANCA staining pattern.
ANCA interpretation can be improved with test-result intervals
Nature Reviews | Rheumatology
Antigen characterizationANCA technologyIncorporation of ANCAs into criteriaANCA standardization
1982
1985
1988
1989
1990
1998
1999
2000
2002
2005
2007
2006
2009
2010
2012
2013
2014
2016
2017
C-ANCA observed in patients with GPA
P-ANCA observed in patients with GPA
identi edas autoantigen
Commercial capture ELISA
Dot and Line Immunoassay
Fluorescent-enzyme Immunoassay
Addressable Laser-Bead Immunoassay
BioChip IIFassay
PR3-ANCAsshown to bepotentiallypathogenic
Automatic ANCA pattern recognition
Chemiluminescentimmunoassays
Cytobead IIF assay
Revised consensus on ANCA-testing
s rst associated with glomerulonephritis
identi ed as autoantigen
Commercial ANCA ELISA
International consensus on ANCA-testing published
MPO-ANCAs shown to be pathogenic
EULAR consider ANCAs for inclusion in diagnostic criteria
IUIS-CDC ANCA referencepreparationsbecame available
Revised CHCC nomenclature includes ANCAs
erti ed material for MPO-ANCAs became available
AnchorELISA
Consensus statements on ANCA testing
C O N S E N S U S S TAT E M E N T
NATURE REVIEWS | RHEUMATOLOGY VOLUME 13 | NOVEMBER 2017 | 685
ǟɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ
Anticorps anticytoplasme des polynucléaires neutrophiles 597
Figure 2. Anticorps anticytoplasme des polynucléaires neu-trophiles (ANCA) de fluorescence cytoplasmique (c-ANCA) enimmunofluorescence indirecte.
Les c-ANCA correspondent à une fluorescence granulairediffuse restant cytoplasmique sur des PNN fixés au formolou au méthanol (Fig. 2). Cet aspect typique de c-ANCA estle plus souvent associé à la cible antigénique PR3.
Les p-ANCA donnent un marquage intense de la périphé-rie des lobes nucléaires avec un centre presque négatif,conférant une image de « chou-fleur » (Fig. 3). Sur les PNNfixés au formol, l’aspect est cytoplasmique identique à celleobservée pour les c-ANCA. Il n’y a pas de marquage pourles PNN fixés au méthanol. Les antigènes reconnus sontnotamment la protéine MPO ou des protéines cationiques.Distinguer un p-ANCA d’un Ac antinucléaire est la principaledifficulté de l’IFI sur PNN fixés à l’éthanol.
Un aspect atypique des ANCA (p-ANCA atypique) est par-fois observé. Il associe un marquage de pourtour des lobesnucléaires sur PNN fixés à l’éthanol et un absence de mar-quage sur les PNN fixés au formol.
Figure 3. Anticorps anticytoplasme des polynucléaires neu-trophiles (ANCA) de fluorescence périnucléaire (p-ANCA) enimmunofluorescence indirecte.
Les ANCA sont une famille d’auto-Ac dirigés contre descibles variées. La deuxième étape obligatoire est donc lacaractérisation de la cible reconnue par les ANCA par tech-nique Elisa, immunodot (membrane sur laquelle la protéinePR3 ou MPO est fixée) ou test fluorométrique (PR3 ou MPOfixée sur des billes fluorescentes). Ces trois techniques sontsemi-quantitatives, le résultat est exprimé en ratio établigrâce à un calibreur dépendant de la technique. Le résultatpeut être négatif (inférieur à 1) ou faiblement positif, posi-tif ou fortement positif. Compte tenu de l’absence d’étaloninternational, les résultats ne peuvent être comparés d’unlaboratoire à l’autre. L’identification des ANCA-MPO et desANCA-PR3 est primordiale pour le diagnostic. L’identificationdes autres cibles aidera le biologiste dans son interprétationet rassurera le clinicien quant à l’absence de spécificitésassociées aux vascularites nécrosantes.
Signification pathologique
Une positivité des ANCA en IFI doit obligatoirement êtreconfirmée par test Elisa. Leur signification pathologiquenécessite une bonne confrontation entre les résultatsimmunologiques, la clinique et les résultats histologiques(Fig. 1).
Les vascularites à ANCA (granulomatose de Wegener,polyangéite microscopique et syndrome de Churg et Strauss)correspondent à des auto-anticorps dirigés contre lesprotéines PR3 ou MPO. Ainsi, la sensibilité des c-ANCA anti-PR3 est de 90 % dans la maladie de Wegener, leur spécificitéest supérieure à 90 %. Leur titre est d’autant plus élevé quela maladie est en poussée clinique. Des p-ANCA anti-MPOsont trouvés dans 80 % des polyangéites microscopiques et30 % des syndromes de Churg et Strauss [3]. Les critères diag-nostiques et principales manifestations de ces trois maladiessont rappelés dans le Tableau 2.
La présence d’ANCA, en général de fluorescence péri-nucléaire atypique et de cible antigénique non-PR3 ou MPO(BPI, élastase, cathepsine G. . .), peut être trouvée dansde multiples circonstances : infections, maladies digestives,hémopathies ou cancers solides, lors de traitements par cer-tains médicaments ou de prise de cocaïne, connectivitesou maladies rhumatologiques inflammatoires, autres vas-cularites, sarcoïdose, dermatoses neutrophiliques, autresconnectivites : périartérite noueuse, lupus érythémateuxsystémique, la polyarthrite rhumatoïde (surtout s’il existeune vascularite associée) [11].
Au cours des colites inflammatoires, les p-ANCA aty-piques, de cible antigénique variée, en général non-MPO,sont positifs dans 60 % des rectocolites hémorragiquesversus 15 % des maladies de Crohn, alors que les Ac anti-Saccharomyces cerevisiae (ASCA) montrent des chiffres depositivité exactement inverses [12]. Ainsi, la recherched’ANCA, combinée à celle des ASCA, est utile pour le diag-nostic étiologique des colites difficiles à classer.
Les messages clés de l’article sont rappelés dans l’Annexe1.
Déclaration d’intérêtsLes auteurs déclarent ne pas avoir de conflits d’intérêts enrelation avec cet article.
Anticorps anticytoplasme des polynucléaires neutrophiles 597
Figure 2. Anticorps anticytoplasme des polynucléaires neu-trophiles (ANCA) de fluorescence cytoplasmique (c-ANCA) enimmunofluorescence indirecte.
Les c-ANCA correspondent à une fluorescence granulairediffuse restant cytoplasmique sur des PNN fixés au formolou au méthanol (Fig. 2). Cet aspect typique de c-ANCA estle plus souvent associé à la cible antigénique PR3.
Les p-ANCA donnent un marquage intense de la périphé-rie des lobes nucléaires avec un centre presque négatif,conférant une image de « chou-fleur » (Fig. 3). Sur les PNNfixés au formol, l’aspect est cytoplasmique identique à celleobservée pour les c-ANCA. Il n’y a pas de marquage pourles PNN fixés au méthanol. Les antigènes reconnus sontnotamment la protéine MPO ou des protéines cationiques.Distinguer un p-ANCA d’un Ac antinucléaire est la principaledifficulté de l’IFI sur PNN fixés à l’éthanol.
Un aspect atypique des ANCA (p-ANCA atypique) est par-fois observé. Il associe un marquage de pourtour des lobesnucléaires sur PNN fixés à l’éthanol et un absence de mar-quage sur les PNN fixés au formol.
Figure 3. Anticorps anticytoplasme des polynucléaires neu-trophiles (ANCA) de fluorescence périnucléaire (p-ANCA) enimmunofluorescence indirecte.
Les ANCA sont une famille d’auto-Ac dirigés contre descibles variées. La deuxième étape obligatoire est donc lacaractérisation de la cible reconnue par les ANCA par tech-nique Elisa, immunodot (membrane sur laquelle la protéinePR3 ou MPO est fixée) ou test fluorométrique (PR3 ou MPOfixée sur des billes fluorescentes). Ces trois techniques sontsemi-quantitatives, le résultat est exprimé en ratio établigrâce à un calibreur dépendant de la technique. Le résultatpeut être négatif (inférieur à 1) ou faiblement positif, posi-tif ou fortement positif. Compte tenu de l’absence d’étaloninternational, les résultats ne peuvent être comparés d’unlaboratoire à l’autre. L’identification des ANCA-MPO et desANCA-PR3 est primordiale pour le diagnostic. L’identificationdes autres cibles aidera le biologiste dans son interprétationet rassurera le clinicien quant à l’absence de spécificitésassociées aux vascularites nécrosantes.
Signification pathologique
Une positivité des ANCA en IFI doit obligatoirement êtreconfirmée par test Elisa. Leur signification pathologiquenécessite une bonne confrontation entre les résultatsimmunologiques, la clinique et les résultats histologiques(Fig. 1).
Les vascularites à ANCA (granulomatose de Wegener,polyangéite microscopique et syndrome de Churg et Strauss)correspondent à des auto-anticorps dirigés contre lesprotéines PR3 ou MPO. Ainsi, la sensibilité des c-ANCA anti-PR3 est de 90 % dans la maladie de Wegener, leur spécificitéest supérieure à 90 %. Leur titre est d’autant plus élevé quela maladie est en poussée clinique. Des p-ANCA anti-MPOsont trouvés dans 80 % des polyangéites microscopiques et30 % des syndromes de Churg et Strauss [3]. Les critères diag-nostiques et principales manifestations de ces trois maladiessont rappelés dans le Tableau 2.
La présence d’ANCA, en général de fluorescence péri-nucléaire atypique et de cible antigénique non-PR3 ou MPO(BPI, élastase, cathepsine G. . .), peut être trouvée dansde multiples circonstances : infections, maladies digestives,hémopathies ou cancers solides, lors de traitements par cer-tains médicaments ou de prise de cocaïne, connectivitesou maladies rhumatologiques inflammatoires, autres vas-cularites, sarcoïdose, dermatoses neutrophiliques, autresconnectivites : périartérite noueuse, lupus érythémateuxsystémique, la polyarthrite rhumatoïde (surtout s’il existeune vascularite associée) [11].
Au cours des colites inflammatoires, les p-ANCA aty-piques, de cible antigénique variée, en général non-MPO,sont positifs dans 60 % des rectocolites hémorragiquesversus 15 % des maladies de Crohn, alors que les Ac anti-Saccharomyces cerevisiae (ASCA) montrent des chiffres depositivité exactement inverses [12]. Ainsi, la recherched’ANCA, combinée à celle des ASCA, est utile pour le diag-nostic étiologique des colites difficiles à classer.
Les messages clés de l’article sont rappelés dans l’Annexe1.
Déclaration d’intérêtsLes auteurs déclarent ne pas avoir de conflits d’intérêts enrelation avec cet article.
C-ANCA (cytoplasmic) P-ANCA (perinuclear)
IIF
Antibodies against neutrophils and monocytes
ELISA
PR3 MPO MPO negPR3 neg ANCA vasculitis

Bosch X, et al. Lancet 2006Bossuyt X et al. Nat. Rev. Rheumatol 2017
Likelihood ratiosThe probability of a specific result occuring in a group of patients divided by the probability of the same result occuring in a group of controls.
Post-test probabilityProbability of an individual having a disease with prior knowledge of the results of
laboratory tests.
Single immunoassays never have a sensitivity and specificity of 100%. In patients where there is a high degree of clinical suspicion and negative ANCA test results, testing by another method can be useful to increase sensitivity (recommendation 3). False-positive results do occur with immunoassays, mainly in samples with a low degree of positivity78. Therefore, performing a second assay or IIF can marginally increase the spec-ificity in cases of low-positive test results10. When new assays are introduced (including assays not included in the EUVAS study6), the diagnostic performance of such assays should be checked based on samples from patients with GPA or MPA and relevant disease controls.
A diagnosis of AAV cannot be excluded for ANCA-negative patients (recommendation 4) and biopsies of the affected organs should be performed in seronegative patients6. Although ANCAs are helpful in the diagnosis of AAV, the diagnosis of AAV should be based on clinico-pathological features (recommendation 5).
Interpretation of test results can be improved by the application of appropriately designed reference ranges (and test result intervals) for antibody levels (rec-ommendation 6). The concept of test result interval- specific likelihood ratios is explained in the next section.
The specific role of IIF testing in ANCA testing algo-rithms should be determined individually by diagnostic laboratories on the basis of the specific clinical need and circumstances of the laboratory. If a laboratory prefers to use IIF as a screening assay in locally determined best-testing algorithms, then the laboratory needs to ensure that the IIF operates at a high level of sensitivity, as the performance of IIF varies greatly between laboratories.
Improving clinical interpretationsAs immunoassays are expected to be increasingly used to screen for AAV, retrieving the maximum amount of clin-ically useful information from PR3-ANCA and MPO-ANCA test results is important. Traditionally, a single cut-off value is employed to predict clinically- relevant reactivity. However, a lot of information is lost when only binary results (positive or negative) are considered, whereas the likelihood for AAV increases with increasing levels of PR3-ANCAs and MPO-ANCAs79.
The likelihood ratio helps to describe the clinical value of a test result. This ratio can be defined for differ-ent test result intervals of an assay and is independent of the disease prevalence and pre-test probability. A like-lihood ratio of 1 indicates no difference in pre-test to post-test probability, whereas likelihood ratios of >10 or <0.1 indicate large, often clinically important differences in pre-test to post-test probability79,80,81.
A detailed analysis of the large dataset from the multi-national EUVAS study6 exemplified and confirmed that the likelihood ratio for AAV increases with increasing levels of PR3-ANCAs and MPO-ANCAs for all immuno-assays included in the study78. For example, the likelihood ratio for AAV was calculated to be 0.1, 1.2, 10.2, 64.6, and ∞ for test result intervals of 0–12 CU, 12–24 CU, 24–78 CU, 78–1,050 CU, and 1,050–3,500 CU, respec-tively, when using the PR3-ANCA and MPO-ANCA QuantaFlash CLIA (Inova)78.
Knowledge of test result-specific likelihood ratios can help clinicians and laboratory professionals to bet-ter interpret results. Having the likelihood ratios enables the calculation of the post-test probability for a disease
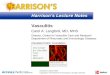
Figure 3 | Visual representation of the 1999 recommendations and revised 2017 recommendations. a| In the 1999 consensus document, the recommended approach for anti-neutrophil cytoplasmic antibody (ANCA) detection was to screen for ANCA by indirect immunofluorescence (IIF) and to test for proteinase 3 (PR3)-ANCAs and myeloperoxidase (MPO)-ANCAs in IIF-positive samples; the ideal approach was to perform IIF and immunoassay on all samples. b| In the 2017 consensus, the use of high-quality immunoassays is recommended as the preferred first screening method for ANCA detection in patients suspected of having the ANCA-associated vaculitides granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA). ANCA detection for non-ANCA-associated vasculitis conditions is not included in this consensus. *A second PR3-MPO-ANCA or IIF can be considered for negative results in patients with a high clinical suspicion (to increase sensitivity) or in case of low antibody levels (to increase specificity). Take antibody level into account.
a 1999 consensus
Ideal approach
b 2017 consensus
Nature Reviews | Rheumatology
IIF
IIF+
ANCA–IIF+
ANCA+
IIF
PR3-ANCA and MPO-ANCA Immunoassays
PR3-ANCA and MPO-ANCA Immunoassays
Not covered bythis consensus
ANCA– ANCA+
Secondassay*
Secondassay*
Gatingstrategy
SuspectedAAV
Non AAV
Recommended approach Recommended approach
IIF– IIF+
PR3-ANCA and MPO-ANCA Immunoassays
IIF–
ANCA–IIF–
ANCA+IIF+
ANCA–IIF+
ANCA+
C O N S E N S U S S TAT E M E N T
688 | NOVEMBER 2017 | VOLUME 13 www.nature.com/nrrheum
ǟɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ
ANCA PR3 + ANCA MPO +GPAGeneralized formLimited form
70-80%60%
10%
EGPA 30% 60%MPA 30% 60%
1999

Bossuyt X et al. Revised 2017 international consensus on testing of ANCAs in granulomatosis with polyangiitis and microscopic polyangiitis Nat. Rev. Rheumatol 2017
Likelihood ratiosThe probability of a specific result occuring in a group of patients divided by the probability of the same result occuring in a group of controls.
Post-test probabilityProbability of an individual having a disease with prior knowledge of the results of
laboratory tests.
Single immunoassays never have a sensitivity and specificity of 100%. In patients where there is a high degree of clinical suspicion and negative ANCA test results, testing by another method can be useful to increase sensitivity (recommendation 3). False-positive results do occur with immunoassays, mainly in samples with a low degree of positivity78. Therefore, performing a second assay or IIF can marginally increase the spec-ificity in cases of low-positive test results10. When new assays are introduced (including assays not included in the EUVAS study6), the diagnostic performance of such assays should be checked based on samples from patients with GPA or MPA and relevant disease controls.
A diagnosis of AAV cannot be excluded for ANCA-negative patients (recommendation 4) and biopsies of the affected organs should be performed in seronegative patients6. Although ANCAs are helpful in the diagnosis of AAV, the diagnosis of AAV should be based on clinico-pathological features (recommendation 5).
Interpretation of test results can be improved by the application of appropriately designed reference ranges (and test result intervals) for antibody levels (rec-ommendation 6). The concept of test result interval- specific likelihood ratios is explained in the next section.
The specific role of IIF testing in ANCA testing algo-rithms should be determined individually by diagnostic laboratories on the basis of the specific clinical need and circumstances of the laboratory. If a laboratory prefers to use IIF as a screening assay in locally determined best-testing algorithms, then the laboratory needs to ensure that the IIF operates at a high level of sensitivity, as the performance of IIF varies greatly between laboratories.
Improving clinical interpretationsAs immunoassays are expected to be increasingly used to screen for AAV, retrieving the maximum amount of clin-ically useful information from PR3-ANCA and MPO-ANCA test results is important. Traditionally, a single cut-off value is employed to predict clinically- relevant reactivity. However, a lot of information is lost when only binary results (positive or negative) are considered, whereas the likelihood for AAV increases with increasing levels of PR3-ANCAs and MPO-ANCAs79.
The likelihood ratio helps to describe the clinical value of a test result. This ratio can be defined for differ-ent test result intervals of an assay and is independent of the disease prevalence and pre-test probability. A like-lihood ratio of 1 indicates no difference in pre-test to post-test probability, whereas likelihood ratios of >10 or <0.1 indicate large, often clinically important differences in pre-test to post-test probability79,80,81.
A detailed analysis of the large dataset from the multi-national EUVAS study6 exemplified and confirmed that the likelihood ratio for AAV increases with increasing levels of PR3-ANCAs and MPO-ANCAs for all immuno-assays included in the study78. For example, the likelihood ratio for AAV was calculated to be 0.1, 1.2, 10.2, 64.6, and ∞ for test result intervals of 0–12 CU, 12–24 CU, 24–78 CU, 78–1,050 CU, and 1,050–3,500 CU, respec-tively, when using the PR3-ANCA and MPO-ANCA QuantaFlash CLIA (Inova)78.
Knowledge of test result-specific likelihood ratios can help clinicians and laboratory professionals to bet-ter interpret results. Having the likelihood ratios enables the calculation of the post-test probability for a disease
Figure 3 | Visual representation of the 1999 recommendations and revised 2017 recommendations. a| In the 1999 consensus document, the recommended approach for anti-neutrophil cytoplasmic antibody (ANCA) detection was to screen for ANCA by indirect immunofluorescence (IIF) and to test for proteinase 3 (PR3)-ANCAs and myeloperoxidase (MPO)-ANCAs in IIF-positive samples; the ideal approach was to perform IIF and immunoassay on all samples. b| In the 2017 consensus, the use of high-quality immunoassays is recommended as the preferred first screening method for ANCA detection in patients suspected of having the ANCA-associated vaculitides granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA). ANCA detection for non-ANCA-associated vasculitis conditions is not included in this consensus. *A second PR3-MPO-ANCA or IIF can be considered for negative results in patients with a high clinical suspicion (to increase sensitivity) or in case of low antibody levels (to increase specificity). Take antibody level into account.
a 1999 consensus
Ideal approach
b 2017 consensus
Nature Reviews | Rheumatology
IIF
IIF+
ANCA–IIF+
ANCA+
IIF
PR3-ANCA and MPO-ANCA Immunoassays
PR3-ANCA and MPO-ANCA Immunoassays
Not covered bythis consensus
ANCA– ANCA+
Secondassay*
Secondassay*
Gatingstrategy
SuspectedAAV
Non AAV
Recommended approach Recommended approach
IIF– IIF+
PR3-ANCA and MPO-ANCA Immunoassays
IIF–
ANCA–IIF–
ANCA+IIF+
ANCA–IIF+
ANCA+
C O N S E N S U S S TAT E M E N T
688 | NOVEMBER 2017 | VOLUME 13 www.nature.com/nrrheum
ǟɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ
OddsThe conversion of probability to odds is carried out using the equation odds = probability/(1−probability).
when the pre-test probability is known using the formula: post-test odds = pre-test odds × likelihood ratio78. FIGURE 4 illustrates the post-test probability for AAV as a function of the pre-test probability (using the formula mentioned above) for different test result intervals. Such graphical representation is a better way to help the interpretation of a test result than describing the sensitivity and spec-ificity of an assay82 and enables the post-test probability to be estimated from the assay test result without the need for a calculation. However, an estimate of the pre-test probability is first required; the pre-test probabilities for AAV associated with particular clinical presentations can be obtained from the literature26,83,84 and have been
previously summarized78. For instance, the pre-test prob-ability for AAV in adult patients presenting with hae-maturia, proteinuria and creatinine levels of 1.5–3 mg/dL is 7%84. If ANCA testing reveals a test result with a likelihood ratio of 60 (for example, a test result between 78–1,050 CU by QuantaFlash), then the post-test prob-ability for AAV will be 82%. By contrast, the post-test probability of a test result with a likelihood ratio of 10.2 or 0.1 will be, respectively, 47% and 0.7%. Such knowledge might add value to a specific test result and help in the clinical interpretation of the result.
Contraindications and considerationsThe consensus recommendations proposed in this manu-script are for detecting ANCAs in AAV, in particular GPA and MPA. However, ANCAs can also be found in several other conditions. In this section, we give an overview of these conditions to further help with clinical interpretation of ANCA test results.
ANCAs in other small-vessel vasculitides. ANCAs are also found in 30–38% of patients with EGPA85, a dis-ease characterized by asthma, eosinophilia and gran-ulomatous inflammation, and in 20–35% of patients with anti-glomerular basement membrane (anti-GBM) disease86. The majority of these ANCA-positive patients have MPO-ANCAs87. As the phenotypes of patients with EGPA are heterogeneous, EGPA was not included in this Consensus Statement.
ANCAs in gastrointestinal disorders. In addition to vas-culitis, ANCAs are found in patients with gastrointestinal disorders such as IBD88, primary sclerosing cholangitis89 and inflammatory liver diseases (such as autoimmune hepatitis, primary biliary cirrhosis and chronic viral hep-atitis)90. These diseases are associated with a slightly aber-rant P-ANCA pattern that is often referred to as atypical P-ANCA or X-ANCA88.
In gastrointestinal disorders, P-ANCA is mainly observed in patients with ulcerative colitis (50–67%), but is also seen in patients with Crohn’s disease (6–15%), and to a lesser extent in disease controls (<11%)88. Combining P-ANCA with anti-Saccharomyces cerevisiae antibody (ASCA) measurements might improve the clinical utility of this marker. ASCAs are found in 40–60% of patients with Crohn’s disease, 4–14% of patients with ulcerative colitis and <5% of controls88. The combination of an ASCA-positive and P-ANCA-negative test result is asso-ciated with Crohn’s disease, whereas the combination of an ASCA-negative and P-ANCA-positive test result is asso-ciated with ulcerative colitis. However, the clinical useful-ness of ANCAs in IBD has been questioned. Given the limited sensitivity of ANCA detection in ulcerative colitis, a European evidence-based consensus on the diagnosis and management of ulcerative colitis concluded that rou-tine use of ANCA detection for diagnosis and therapeutic decisions was not clinically justified91.
In the past few years, studies have also reported that sensitive immunoassays can detect PR3-ANCAs in patients with ulcerative colitis50,92,93 and primary sclerosing cholangitis94.
Box 1 | Recommendations for ANCA testing
The following new international recommendations should be considered for anti-neutrophil cytoplasmic antibody (ANCA) detection in the small-vessel vasculitides granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA):
Recommandation 1A gating policy for requesting an ANCA test is advisable and adherence to clinical guidelines for ANCA testing (BOX 2) is recommended.
Recommandation 2High-quality antigen-specific assays for proteinase 3 (PR3)-ANCAs and myeloperoxidase (MPO)-ANCAs should be used as the primary screening method for ANCA.
Recommandation 3If results for both PR3-ANCAs and MPO-ANCAs are negative, and there is still a strong suspicion of small-vessel vasculitis, then use of other immunoassays and/or indirect immunofluorescence (IIF), or referral to an experienced laboratory is recommended. Performing a second assay or IIF can also marginally increase the specificity in cases of low-positive test results.
Recommandation 4A diagnosis of ANCA-associated vasculitis (AAV) cannot be excluded on the basis of negative PR3-ANCA and MPO-ANCA results.
Recommandation 5A positive PR3-ANCA and/or MPO-ANCA result only contributes to the diagnostic work-up for AAV and is not diagnostic by itself.
Recommandation 6Taking into account antibody levels improves clinical interpretation.
Box 2 | Clinical indications for ANCA testing
In order to assure appropriate anti-neutrophil cytoplasmic antibody (ANCA)-test usage to support the diagnosis of ANCA-associated vasculitis (AAV), ANCA should be requested for patients with the following clinical indications.
• Glomerulonephritis, especially rapidly progressive glomerulonephritis
• Pulmonary haemorrhage, especially pulmonary renal syndrome
• Cutaneous vasculitis with systemic features
• Multiple lung nodules
• Chronic destructive disease of the upper airways
• Long-standing sinusitis or otitis
• Subglottic tracheal stenoses
• Mononeuritis multiplex or other peripheral neuropathy
• Retro-orbital mass
• Scleritis
Reproduced and adapted with permissions from Judy Savige, et al. International consensus statement on testing and reporting of antineutrophil cytoplasmic antibodies (ANCA) (1999) American Journal of Clinical Pathology 111 (4); 507–513 (1999). Published online at: https://academic.oup.com/ajcp/article/111/4/507/1758310
C O N S E N S U S S TAT E M E N T
NATURE REVIEWS | RHEUMATOLOGY VOLUME 13 | NOVEMBER 2017 | 689
ǟɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ
2017

OddsThe conversion of probability to odds is carried out using the equation odds = probability/(1−probability).
when the pre-test probability is known using the formula: post-test odds = pre-test odds × likelihood ratio78. FIGURE 4 illustrates the post-test probability for AAV as a function of the pre-test probability (using the formula mentioned above) for different test result intervals. Such graphical representation is a better way to help the interpretation of a test result than describing the sensitivity and spec-ificity of an assay82 and enables the post-test probability to be estimated from the assay test result without the need for a calculation. However, an estimate of the pre-test probability is first required; the pre-test probabilities for AAV associated with particular clinical presentations can be obtained from the literature26,83,84 and have been
previously summarized78. For instance, the pre-test prob-ability for AAV in adult patients presenting with hae-maturia, proteinuria and creatinine levels of 1.5–3 mg/dL is 7%84. If ANCA testing reveals a test result with a likelihood ratio of 60 (for example, a test result between 78–1,050 CU by QuantaFlash), then the post-test prob-ability for AAV will be 82%. By contrast, the post-test probability of a test result with a likelihood ratio of 10.2 or 0.1 will be, respectively, 47% and 0.7%. Such knowledge might add value to a specific test result and help in the clinical interpretation of the result.
Contraindications and considerationsThe consensus recommendations proposed in this manu-script are for detecting ANCAs in AAV, in particular GPA and MPA. However, ANCAs can also be found in several other conditions. In this section, we give an overview of these conditions to further help with clinical interpretation of ANCA test results.
ANCAs in other small-vessel vasculitides. ANCAs are also found in 30–38% of patients with EGPA85, a dis-ease characterized by asthma, eosinophilia and gran-ulomatous inflammation, and in 20–35% of patients with anti-glomerular basement membrane (anti-GBM) disease86. The majority of these ANCA-positive patients have MPO-ANCAs87. As the phenotypes of patients with EGPA are heterogeneous, EGPA was not included in this Consensus Statement.
ANCAs in gastrointestinal disorders. In addition to vas-culitis, ANCAs are found in patients with gastrointestinal disorders such as IBD88, primary sclerosing cholangitis89 and inflammatory liver diseases (such as autoimmune hepatitis, primary biliary cirrhosis and chronic viral hep-atitis)90. These diseases are associated with a slightly aber-rant P-ANCA pattern that is often referred to as atypical P-ANCA or X-ANCA88.
In gastrointestinal disorders, P-ANCA is mainly observed in patients with ulcerative colitis (50–67%), but is also seen in patients with Crohn’s disease (6–15%), and to a lesser extent in disease controls (<11%)88. Combining P-ANCA with anti-Saccharomyces cerevisiae antibody (ASCA) measurements might improve the clinical utility of this marker. ASCAs are found in 40–60% of patients with Crohn’s disease, 4–14% of patients with ulcerative colitis and <5% of controls88. The combination of an ASCA-positive and P-ANCA-negative test result is asso-ciated with Crohn’s disease, whereas the combination of an ASCA-negative and P-ANCA-positive test result is asso-ciated with ulcerative colitis. However, the clinical useful-ness of ANCAs in IBD has been questioned. Given the limited sensitivity of ANCA detection in ulcerative colitis, a European evidence-based consensus on the diagnosis and management of ulcerative colitis concluded that rou-tine use of ANCA detection for diagnosis and therapeutic decisions was not clinically justified91.
In the past few years, studies have also reported that sensitive immunoassays can detect PR3-ANCAs in patients with ulcerative colitis50,92,93 and primary sclerosing cholangitis94.
Box 1 | Recommendations for ANCA testing
The following new international recommendations should be considered for anti-neutrophil cytoplasmic antibody (ANCA) detection in the small-vessel vasculitides granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA):
Recommandation 1A gating policy for requesting an ANCA test is advisable and adherence to clinical guidelines for ANCA testing (BOX 2) is recommended.
Recommandation 2High-quality antigen-specific assays for proteinase 3 (PR3)-ANCAs and myeloperoxidase (MPO)-ANCAs should be used as the primary screening method for ANCA.
Recommandation 3If results for both PR3-ANCAs and MPO-ANCAs are negative, and there is still a strong suspicion of small-vessel vasculitis, then use of other immunoassays and/or indirect immunofluorescence (IIF), or referral to an experienced laboratory is recommended. Performing a second assay or IIF can also marginally increase the specificity in cases of low-positive test results.
Recommandation 4A diagnosis of ANCA-associated vasculitis (AAV) cannot be excluded on the basis of negative PR3-ANCA and MPO-ANCA results.
Recommandation 5A positive PR3-ANCA and/or MPO-ANCA result only contributes to the diagnostic work-up for AAV and is not diagnostic by itself.
Recommandation 6Taking into account antibody levels improves clinical interpretation.
Box 2 | Clinical indications for ANCA testing
In order to assure appropriate anti-neutrophil cytoplasmic antibody (ANCA)-test usage to support the diagnosis of ANCA-associated vasculitis (AAV), ANCA should be requested for patients with the following clinical indications.
• Glomerulonephritis, especially rapidly progressive glomerulonephritis
• Pulmonary haemorrhage, especially pulmonary renal syndrome
• Cutaneous vasculitis with systemic features
• Multiple lung nodules
• Chronic destructive disease of the upper airways
• Long-standing sinusitis or otitis
• Subglottic tracheal stenoses
• Mononeuritis multiplex or other peripheral neuropathy
• Retro-orbital mass
• Scleritis
Reproduced and adapted with permissions from Judy Savige, et al. International consensus statement on testing and reporting of antineutrophil cytoplasmic antibodies (ANCA) (1999) American Journal of Clinical Pathology 111 (4); 507–513 (1999). Published online at: https://academic.oup.com/ajcp/article/111/4/507/1758310
C O N S E N S U S S TAT E M E N T
NATURE REVIEWS | RHEUMATOLOGY VOLUME 13 | NOVEMBER 2017 | 689
ǟɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ ǟ
ɥƐƎƏƗ
ɥ �!,(++�-
ɥ�4 +(2'#12
ɥ�(,(3#"Ʀ
ɥ/�13
ɥ.$ɥ�/1(-%#1
ɥ��341#ƥ
ɥ�++ɥ1(%'32
ɥ1#2#15#"ƥ
Bossuyt X et al. Nat. Rev. Rheumatol 2017

ANCA ELISAMPO and PR3
Atypical ANCAX-ANCA
Negative C-ANCA+ PR3+ p-ANCA+ MPA+
ANCA negativevasculitis
GPA
High suspicion
Churg-Strauss MPA
Low suspicion Biopsy
Other diagnostic
GPACS
MPA
Specific treatmentHigh suspicionClinical gravity
+-
Ingen-Housz-Oro S, et al. Ann Dermatol Venereol 2012;139:594-598.

Bosch X, et al Lancet 2006
Review
www.thelancet.com Vol 368 July 29, 2006 409
DPB1), and death-associated protein 6 (DAXX). Further analysis revealed a strong link between HLA-DPB1 0401 allele and Wegener’s granulomatosis. Certain HLA-DPB1 alleles are implicated in chronic beryllium disease, another granulomatous lung disorder. Furthermore, the researchers identifi ed an extended haplotype DPB1* 0401/RXRB03, which showed an even stronger asso-ciation with Wegener’s granulomatosis.
CTL4 plays an important part in T-cell activation downregulation. The frequency of the shortest allele (86) of an (AT)n microsatellite polymorphism of the CTLA4 gene is decreased in Wegener’s granulomatosis patients.57 This polymorphism might account for a hyperactive immune response.49 Another polymorphism in the promoter region of the CTLA 4 gene [C(–318)T] has been associated with Wegener’s granulomatosis, although it is unlikely to have functional importance. 58
Environmental factors Many case-control studies have shown an association between silica exposure and ANCA detection, ANCA-associated vasculitides, or both.59–62 In a series of 65 patients with ANCA-associated vasculitides, Hogan and associates61 showed that the odds ratio of silica dust exposure was 4·4 times greater in patients compared with controls. Lane and colleagues62 reported a substantial association between high occupational exposure to silica and Churg-Strauss syndrome (odds ratio 5·6) and ANCA positivity (4·9). Because silica particles are powerful stimulators of T cells and B cells, their inhalation by susceptible individuals might trigger production of autoantibodies including ANCA. Moreover, release of proteinase 3 or myeloperoxidase (and subsequent ANCA production) can be induced by activation of monocytes and macrophages by silica.61 Data from in-vitro and murine studies have shown that silica accelerates apoptosis.63,64 Silica might cause disturbances in normal apoptosis leading to cross-presentation of self-antigens by dendritic cells. In view of the growing evidence on the potential role of silica in ANCA-associated vasculitides pathogenesis, it seems reasonable to explicitly ask patients with these disorders about previous or current exposure to specifi c sources. Doctors can then consider whether such individuals who remain actively exposed to silica should be advised to move away from its source, which might improve their disease prognosis.
Other occupational factors associated with ANCA-associated vasculitides, ANCA positivity, or both (although to a lesser degree than silica) are farming (especially livestock), high occupational solvent exposure, allergy in general,62 asbestos,65 and pesticides.66
Cocaine-induced face midline destructive lesions have been linked to ANCA displaying double-specifi city for human neutrophil elastase and proteinase 3. This association helps to distinguish midline lesions arising as a result of sniffi ng cocaine from those in Wegener’s granulomatosis. In patients with this disorder, ANCA
Reference
Infections
Tuberculosis Flores-Suarez71
HIV/AIDS Klaassen72
Malaria Yahya73
Hepatitis C Wu74
Subacute endocarditis due to S aureus or streptococci Hellmich;75 Choi76
Parvovirus B19 Chou77
Leprosy Medina78
Pseudomonas (cystic fi brosis) Carlsson79
Aspergillosis Cho80
Histoplasmosis Mead81
Leptospirosis Constantin82
Amoebiasis Pudifi n15
Pulmonary sporotrichosis Byrd83
Digestive disorders
Infl ammatory bowel disease Saxon84
Primary sclerosing cholangitis Schwarze85
Autoimmune hepatitis Schwarze85
Primary biliary cirrhosis Sobajima86
Neoplasms
Carcinoma Vassilopoulos87
Lymphoma Savige88
Liebow’s disease Savige88
Chronic myelocytic leukaemia Chevailler89
Myelodysplasia Savige88
Monoclonal gammopathies Esnault90
Drugs
Propylthiouracil Slot69
Hydralazine Short91
Methimazole Guma92
Minocycline Elkayam93
Carbimazole Miller94
Allopurinol Choi95
Cocaine Wiesner67
D-penicillamine ten Holder70
Phenytoin ten Holder70
Levamisole ten Holder70
Pimagedine ten Holder70
Connective-tissue diseases
Systemic lupus erythematosus Schnabel96
Rheumatoid arthritis Bosch97
Felty’s syndrome Juby98
Systemic sclerosis Ruff atti99
Dermatomyositis Merkel100
Sjögren’s syndrome Font101
Mixed connective tissue disease Cooper102
Reactive arthritis Locht103
Ankylosing spondylitis Lotch103
Juvenile chronic arthritis Mulder104
Relapsing polychondritis Papo105
Eosinophilia myalgia syndrome Schnabel106
(Continues on next page)
Review
www.thelancet.com Vol 368 July 29, 2006 409
DPB1), and death-associated protein 6 (DAXX). Further analysis revealed a strong link between HLA-DPB1 0401 allele and Wegener’s granulomatosis. Certain HLA-DPB1 alleles are implicated in chronic beryllium disease, another granulomatous lung disorder. Furthermore, the researchers identifi ed an extended haplotype DPB1* 0401/RXRB03, which showed an even stronger asso-ciation with Wegener’s granulomatosis.
CTL4 plays an important part in T-cell activation downregulation. The frequency of the shortest allele (86) of an (AT)n microsatellite polymorphism of the CTLA4 gene is decreased in Wegener’s granulomatosis patients.57 This polymorphism might account for a hyperactive immune response.49 Another polymorphism in the promoter region of the CTLA 4 gene [C(–318)T] has been associated with Wegener’s granulomatosis, although it is unlikely to have functional importance. 58
Environmental factors Many case-control studies have shown an association between silica exposure and ANCA detection, ANCA-associated vasculitides, or both.59–62 In a series of 65 patients with ANCA-associated vasculitides, Hogan and associates61 showed that the odds ratio of silica dust exposure was 4·4 times greater in patients compared with controls. Lane and colleagues62 reported a substantial association between high occupational exposure to silica and Churg-Strauss syndrome (odds ratio 5·6) and ANCA positivity (4·9). Because silica particles are powerful stimulators of T cells and B cells, their inhalation by susceptible individuals might trigger production of autoantibodies including ANCA. Moreover, release of proteinase 3 or myeloperoxidase (and subsequent ANCA production) can be induced by activation of monocytes and macrophages by silica.61 Data from in-vitro and murine studies have shown that silica accelerates apoptosis.63,64 Silica might cause disturbances in normal apoptosis leading to cross-presentation of self-antigens by dendritic cells. In view of the growing evidence on the potential role of silica in ANCA-associated vasculitides pathogenesis, it seems reasonable to explicitly ask patients with these disorders about previous or current exposure to specifi c sources. Doctors can then consider whether such individuals who remain actively exposed to silica should be advised to move away from its source, which might improve their disease prognosis.
Other occupational factors associated with ANCA-associated vasculitides, ANCA positivity, or both (although to a lesser degree than silica) are farming (especially livestock), high occupational solvent exposure, allergy in general,62 asbestos,65 and pesticides.66
Cocaine-induced face midline destructive lesions have been linked to ANCA displaying double-specifi city for human neutrophil elastase and proteinase 3. This association helps to distinguish midline lesions arising as a result of sniffi ng cocaine from those in Wegener’s granulomatosis. In patients with this disorder, ANCA
Reference
Infections
Tuberculosis Flores-Suarez71
HIV/AIDS Klaassen72
Malaria Yahya73
Hepatitis C Wu74
Subacute endocarditis due to S aureus or streptococci Hellmich;75 Choi76
Parvovirus B19 Chou77
Leprosy Medina78
Pseudomonas (cystic fi brosis) Carlsson79
Aspergillosis Cho80
Histoplasmosis Mead81
Leptospirosis Constantin82
Amoebiasis Pudifi n15
Pulmonary sporotrichosis Byrd83
Digestive disorders
Infl ammatory bowel disease Saxon84
Primary sclerosing cholangitis Schwarze85
Autoimmune hepatitis Schwarze85
Primary biliary cirrhosis Sobajima86
Neoplasms
Carcinoma Vassilopoulos87
Lymphoma Savige88
Liebow’s disease Savige88
Chronic myelocytic leukaemia Chevailler89
Myelodysplasia Savige88
Monoclonal gammopathies Esnault90
Drugs
Propylthiouracil Slot69
Hydralazine Short91
Methimazole Guma92
Minocycline Elkayam93
Carbimazole Miller94
Allopurinol Choi95
Cocaine Wiesner67
D-penicillamine ten Holder70
Phenytoin ten Holder70
Levamisole ten Holder70
Pimagedine ten Holder70
Connective-tissue diseases
Systemic lupus erythematosus Schnabel96
Rheumatoid arthritis Bosch97
Felty’s syndrome Juby98
Systemic sclerosis Ruff atti99
Dermatomyositis Merkel100
Sjögren’s syndrome Font101
Mixed connective tissue disease Cooper102
Reactive arthritis Locht103
Ankylosing spondylitis Lotch103
Juvenile chronic arthritis Mulder104
Relapsing polychondritis Papo105
Eosinophilia myalgia syndrome Schnabel106
(Continues on next page)
Review
410 www.thelancet.com Vol 368 July 29, 2006
will react with proteinase 3 but not with neutrophil elastase.67 This double-reactivity suggests the existence of cocaine-induced polyclonal B-cell stimulation, an event noted also with other drugs (eg, allopurinol, D-penicillamine). The almost universal nasal carriage of S aureus in cocaine abusers might also account for the presence of ANCA in those with midline destructive lesions. Finally, bearing in mind the association between ANCA and infections, a persistent superinfected necrotic tissue in cocaine-induced lesions might account for the existence of ANCA in such cases.68
Among drug treatments, propylthiouracil, hydralazine, methimazole, carbimazole, D-penicillamine, and minocycline have mostly been implicated in the development of ANCA-associated vasculitides.69,70 Other uncommon reported agents are listed in table 1. Cases of drug-induced ANCA-associated vasculitides are not as severe as the primary forms of disease and withdrawal of the agent has generally resulted in a decrease in ANCA titres and disease resolution.123 The prevalence of ANCA in patients treated with propylthiouracil ranges between 33% and 64%. Yet clinical manifestations of vasculitis are uncommon.28 Of note, Slot and associates69 detected a higher frequency of ANCA, with or without vasculitis, in patients administered antithyroid drugs (compared with hyperthyroid patients who received other therapies) even after years of treatment. Most cases of drug-induced ANCA-associated vasculitides are associated not only with myeloperoxidase ANCA but also with elastase, proteinase 3, and lactoferrin. The detection of ANCA
against two or more antigens might hint at drug-induced disease.69,123 ANCA-associated vasculitides with drug-induced disease can show an atypical ANCA pattern along with a high concentration of myeloperoxidase ANCA;124 the pathogenesis is not well understood. Propylthiouracil can accumulate in neutrophils and is oxidised to reactive intermediates that bind to self-peptides and provoke T-cell sensitisation, potentially leading to ANCA production.28 After fi nding diff erences in epitope recognition, Ye and colleagues125 suggested that the mechanism of generation of ANCA in propylthiouracil-induced myeloperoxidase ANCA-asso-ciated vasculitis is dissimilar to that of idiopathic ANCA-associated vasculitides.
Methods for detection of ANCAIndirect immunofl uorescence and ELISA remain the most widely used techniques for ANCA detection, their combination being the most suitable approach.87,124,126–128 When positive results from indirect immunofl uorescence and ELISA are combined, specifi city for ANCA-associated vasculitides is 99% and sensitivity for Wegener’s granulomatosis and microscopic polyangiitis is 73% and 67%, respectively.126 Moreover, ANCA testing by both methods is highly useful to exclude pauci-immune necrotising and crescentic glomerulonephritis in patients with low pre-test likelihood (negative predictive value 99%); when there is high clinical suspicion, ANCA determination is most valuable to lend support to such a diagnosis (positive predictive value 95%).129
When searching for ANCA by indirect immuno-fl uorescence, four immunostaining patterns can be seen. The cytoplasmic pattern suggests the presence of serum proteinase 3 ANCA. The perinuclear pattern is defi ned as any perinuclear fl uorescence with or without nuclear extension. In a clinically suitable scenario, most perinuclear ANCA, usually with nuclear extension, will match myeloperoxidase ANCA. However, perinuclear ANCA, generally other than myeloperoxidase ANCA, can also be in disorders diff erent from ANCA-associated vasculitides, such as infl ammatory bowel disease and other autoimmune conditions. Atypical cytoplasmic ANCA (diff use fl at cytoplasmic staining without interlobular accentuation) has specifi city for bac-tericidal/permeability-increasing protein and is mainly linked to chronic infections.124 Any other ANCA staining makes up an atypical ANCA pattern, which is not typically associated with ANCA-associated vasculitides.
In clinical practice, ELISA will prove the presence of myeloperoxidase ANCA or proteinase 3 ANCA. Yet there might be sensitivity issues because of the quality of ELISA kits.130 Other techniques are being developed to overcome ELISA limitations (eg, capture ELISA).131
An international group of experts has produced guidelines on ANCA testing and reporting to minimise technical diffi culties and improve the homogeneity of results.124,128 They propose to screen ANCA by indirect
(Continued from previous page)
Systemic vasculitides other than ANCA-associated vasculitis
Polyarteritis nodosa Baranger107
Horton’s arteritis Bosch108
Takayasu’s arteritis Uppal109
Schönlein-Henoch purpura Saulsbury110
Kawasaki disease Rider111
Behçet’s disease Baleva112
Cryoglobulinemic vasculitis Lampretch113
Renal diseases
Poststreptococcal glomerulonephritis Ardiles114
IgA nephropathy van den Wall Bake115
Membranous nephropathy Dwyer116
Antiglomerular basement membrane disease Bosch117
Other disorders
Silica exposure Hogan61
Sarcoidosis Forde118
Sweet syndrome Burrows119
Idiopathic pulmonary haemosiderosis Attia120
Retroperitoneal fi brosis Sakemi121
Erythema elevatum diutinum Ayoub122
Table 1: Disorders other than ANCA-associated vasculitis, in which ANCA have been detected either by indirect immunofl uorescence or ELISA
Other causes of ANCA

ASSESSING THE ACTIVITY OF VASCULITISANCA associated vasculitides and Polyarteritis Nodosa

Birmingham Vasculitis Activity Score (BVAS)
• 9 sections– Persistent if all diseases
features have been present for > 1 month.
– If any of the features have started or deteriorated in the past month, please select New / Worse.
http://golem.ndorms.ox.ac.uk/calculators/bvas.htmlLuqmani et al, QJM 1994; Muhtyar te al. Ann Rheum Dis 2009; Stone et al. Arthritis Rheum 2001 (BVAS-WG)
BVAS/WG (adaptation française – GFEV) NOM : Prénom : BIRMINGHAM VASCULITIS ACTIVITY SCORE Date : FOR WEGENER’S GRANULOMATOSIS Médecin : EVALUATION FORM Les signes « récents » correspondent à des signes nouveaux survenus ou s’étant aggravés dans les 28 derniers jours au plus, et considérés en rapport avec l’activité de la vascularite. Les signes « persistants » correspondent à des manifestations témoignant d’une vascularite toujours active mais présents depuis plus de 28 jours. Les manifestations majeures sont en caractères gras et précédées d’un astérisque (*).
Récent / Persistant
1. Signes généraux Arthralgies / arthrites ◘ ○ Fièvre ≥ 38°C ◘ ○ 2. Signes cutanés Purpura ◘ ○ Ulcération(s) cutanées ◘ ○ * Gangrène ◘ ○ 3. Atteintes muqueuses et oculaires Ulcération buccale ◘ ○ Conjonctivite / épisclérite ◘ ○ Tumeur rétro-orbitaire / exophtalmie ◘ ○ Uvéite ◘ ○ * Sclérite ◘ ○ * Hémorragie rétinienne / exsudats rétiniens ◘ ○ 4. Signes ORL Epistaxis / croûtes nasales / ulcération des muqueuses nasales ◘ ○ Sinusite ◘ ○ Inflammation des glandes salivaires ◘ ○ Sténose / inflammation sous-glottique ◘ ○ Baisse d’audition de transmission (conduction) ◘ ○ * Baisse d’audition de perception (sensorielle) ◘ ○ 5. Signes cardiovasculaires Péricardite ◘ ○
Récent / Persistant
6. Signes digestifs * Ischémie mésentérique ◘ ○ 7. Signes pulmonaires Epanchement pleural ◘ ○ Nodule(s) / Nodule(s) excavé(s) ◘ ○ Infiltrat pulmonaire radiologique lié à la GW ◘ ○ Sténose / atteinte endobronchique ◘ ○ * Hémorragie intra-alvéolaire ◘ ○ * Détresse respiratoire ◘ ○ 8. Atteinte rénale Hématurie ≥10 GR/champ ou ≥1+ à la BU ◘ ○ * Hématurie avec cylindre (« RBC casts ») ◘ ○ * Augmentation de la créatininémie >30% ou diminution de la clairance de la créatinine >25% ◘ ○ 9. Atteinte neurologique * Méningite ◘ ○ * Atteinte médullaire (myélite) ◘ ○ * Accident vasculaire cérébral ◘ ○ * Atteinte de(s) paire(s) crânienne(s) ◘ ○ * Neuropathie périphérique sensitive ◘ ○ * Multinévrite avec atteinte motrice ◘ ○ 10. Autre atteinte spécifique Préciser :………………………………………… ◘ ○ Préciser :………………………………………… ◘ ○ Préciser :………………………………………… ◘ ○ Préciser :………………………………………… ◘ ○
Nombres de critères majeurs récents ◘ |__|__| (a), Nombre de critères majeurs persistants ○ |__|__| (c), Nombre de critères mineurs récents ◘ |__|__| (b), Nombre de critères mineurs persistants ○ |__|__| (d). BVAS/WG Total = (3 x a) + (1 x b) + (3 x c) + (1 x d) = |__|__| (maximum 68) EVALUATION GLOBALE DE L’ACTIVITE DE LA MALADIE : Poussée grave et systémique (≥ 1 critère majeur récent) ◘ Maladie persistante (critères persistants uniquement) ◘ Poussée limitée (≥ 1 critère mineur récent) ◘ Maladie en rémission (aucun critère) ◘ Indiquer d’un trait votre appréciation de l’activité de la maladie dans les 28 derniers jours (ne pas y inclure les séquelles) : Valeur de l’activité selon l’échelle visuelle analogue = |__|__| / 10 (distance du repère « 0 » au trait tracé, en millimètres)
0 10 Activité
maximale Rémission

Revised Five factor score (2011)Validated for PAN, MPA, CS and GPA/Wegener
Five Factor Score (FFS)Age > 65 yo
Renal failureStabilized peak creat > 150 micromol/L
GI involvementBowel perforation, bleeding, pancreatitis
Cardiac insufficiencyLack of ENT symptoms
FFS 5-year mortality0 9%
1 21%*
2 or more 40%**
*p < 0,005 et ** p < 0,0001 compared to patients FFS = 0.
Source : Guillevin et al. Medicine (Baltimore). 2011; 90:19-27, based in 1108 consecutive patients from the FVSG database
1 criteria = 1 point
FFS≥1
CS +
Immunosuppressive
treatment (CYC or
RTX)
Not applicable to IgA
vasculitis or Cryoglobulinemia
Assess the severity/mortalityrisk of the disease at diagnosis
of systemic necrotizing
vasculitis
Can be used to decide of the
first-line treatment

GRANULOMATOSIS WITH POLYANGIITIS(FORMER WEGENER’S)
ANCA associated vasculitides and Polyarteritis Nodosa

Main characteristics
Necrotizing small vessel-vasculitis with granulomas
C-ANCA 95% (IIF); PR3 >> MPO
Young patients (35-55 yo), white (90%), northern Europe
Prevalence 24-150/1 million
Relapsing disease +++

Extra-cutaneous manifestations
General signs (50%) Fever, asthenia, weight loss, arthritis, myalgias
ENT (70-100%) Rhinitis; epistaxis; otitis; sinusitis; dysphonia
Eye Episcleritis; exophalmia
Lung (50-75%) Cough; hemoptysis; IAH; NO ASTHMA
CNS/PNS (16-44%) Mononeuritis multiplex; headache; pachymeningitis
Kidney (45-90%) RP glomerulonephritis
Miscellaneous Pericarditis…; ileocolitis…
Karras et al. Presse Med 2012

Skin lesions N % / all patients % / all skin lesionsPalpable purpura 28 34,7% 74%
Oral ulcerations 16 21,3% 45,7%
Nodules 6 8% 17%
Skin ulcerations 5 6,7% 14%
Necrotic papules 5 6,7% 14%
Gingival hyperplasia
3 4% 8%
Pustules 2 2,7% 5,7%
Xanthoma 2 2,7% 5,7%
Livedo 1 1,3% 2,8%
Digital necrosis 1 1,3% 2,8%
Francès C et al. Arch Dermatol 1994; 130: 861-7.
Cutaneous manifestations
• 35-70%
• Inaugural in 10% of cases
• Exceptionallyisolated

Cutaneous histology
• Cutaneous vasculitis indistinguishable from MPA
Sunderkötter et al. Arthritis Rheum 2018.
Table 4. Systemic and cutaneous variants of small vessel vasculitis*
CHCC12vasculitis category, name
AbbreviatedCHCC2012 definition
Cutaneous component ofsystemic vasculitis
Skin-limited orskin-dominant variant
ANCA-associated vasculitis Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries);associated with ANCAs
Vasculitis of cutaneouspostcapillary venules, smallveins, arterioles, and smallarteries; associated with ANCAs
ANCA-associated vasculitislimited to the skin (not furtherspecified)
MPA Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,or arterioles)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), often withleukocytoclasia and withoutgranulomatous inflammation
Skin-limited MPA (includingdrug-induced skin-limitedMPA); vasculitis of small vesselsin the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), withoutcutaneous granulomatousinflammation and withoutsystemic vasculitis; associatedwith ANCAs
GPA Necrotizing granulomatousinflammation usually involvingthe upper and lower respiratorytracts, and necrotizing vasculitisaffecting predominantly small-to-medium vessels (e.g.,capillaries, venules, arterioles,arteries, and veins)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, small veins,or small arteries), often withleukocytoclasia andnonvasculitic extravasculardermal granulomatousinflammation
Skin-limited GPA (includingdrug-induced skin-limited GPA);vasculitis of small vessels in theskin (spectrum as in MPA), withnonvasculitic extravasculardermal granulomatousinflammation but withouteosinophilia, without a historyof asthma, and without systemicvasculitis; associated withANCAs
EGPA Eosinophil-rich and necrotizinggranulomatous inflammationoften involving the respiratorytract, and necrotizing vasculitispredominantly affecting small-to-medium vessels andassociated with a history ofasthma and eosinophilia
Eosinophil-rich vasculitis of small-to-medium vessels in the skin(postcapillary venules, arterioles,small venules, or small arteries),sometimes with leukocytoclasiaand, e.g., nonvasculiticextravascular dermalgranulomatous inflammation
Skin-limited EGPA (includingdrug-induced skin-limitedEGPA); eosinophil-richvasculitis of small vessels in theskin (spectrum as in MPA),with, e.g., nonvasculiticextravascular dermalgranulomatous inflammation,and with a history of asthma,but without systemic vasculitis;associated with ANCAs
Immune complex vasculitis Vasculitis with moderate-to-marked vessel wall deposits ofimmunoglobulin and/orcomplement components,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries)
Leukocytoclastic immune complexvasculitis of small vessels(mostly postcapillary venules,occasionally small veins orarterioles)
Skin-limited immune complexvasculitis
Anti–GBM disease Vasculitis affecting glomerularcapillaries, pulmonarycapillaries, or both, with GBMdeposition of anti-GBMautoantibodies
None None
CV Vasculitis with cryoglobulinimmune deposits affecting smallvessels (predominantlycapillaries, venules, orarterioles); associated withserum cryoglobulins
Leukocytoclastic vasculitis of smallvessels (postcapillary venules,small veins, or arterioles);associated with serumcryoglobulins (usually type IIand type III)
Skin-limited CV, without systemicvasculitis
IgA vasculitis(Henoch-Sch€onlein)
Vasculitis with IgA1-dominantimmune deposits, affecting smallvessels (predominantlycapillaries, venules, orarterioles)
Leukocytoclastic IgA1-dominantvasculitis of mostly postcapillaryvenules and also veins orarterioles in the skin, withvascular IgA deposits
Skin-limited IgA vasculitis, withoutsystemic vasculitis
176 SUNDERK€OTTER ET AL
Table 4. Systemic and cutaneous variants of small vessel vasculitis*
CHCC12vasculitis category, name
AbbreviatedCHCC2012 definition
Cutaneous component ofsystemic vasculitis
Skin-limited orskin-dominant variant
ANCA-associated vasculitis Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries);associated with ANCAs
Vasculitis of cutaneouspostcapillary venules, smallveins, arterioles, and smallarteries; associated with ANCAs
ANCA-associated vasculitislimited to the skin (not furtherspecified)
MPA Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,or arterioles)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), often withleukocytoclasia and withoutgranulomatous inflammation
Skin-limited MPA (includingdrug-induced skin-limitedMPA); vasculitis of small vesselsin the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), withoutcutaneous granulomatousinflammation and withoutsystemic vasculitis; associatedwith ANCAs
GPA Necrotizing granulomatousinflammation usually involvingthe upper and lower respiratorytracts, and necrotizing vasculitisaffecting predominantly small-to-medium vessels (e.g.,capillaries, venules, arterioles,arteries, and veins)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, small veins,or small arteries), often withleukocytoclasia andnonvasculitic extravasculardermal granulomatousinflammation
Skin-limited GPA (includingdrug-induced skin-limited GPA);vasculitis of small vessels in theskin (spectrum as in MPA), withnonvasculitic extravasculardermal granulomatousinflammation but withouteosinophilia, without a historyof asthma, and without systemicvasculitis; associated withANCAs
EGPA Eosinophil-rich and necrotizinggranulomatous inflammationoften involving the respiratorytract, and necrotizing vasculitispredominantly affecting small-to-medium vessels andassociated with a history ofasthma and eosinophilia
Eosinophil-rich vasculitis of small-to-medium vessels in the skin(postcapillary venules, arterioles,small venules, or small arteries),sometimes with leukocytoclasiaand, e.g., nonvasculiticextravascular dermalgranulomatous inflammation
Skin-limited EGPA (includingdrug-induced skin-limitedEGPA); eosinophil-richvasculitis of small vessels in theskin (spectrum as in MPA),with, e.g., nonvasculiticextravascular dermalgranulomatous inflammation,and with a history of asthma,but without systemic vasculitis;associated with ANCAs
Immune complex vasculitis Vasculitis with moderate-to-marked vessel wall deposits ofimmunoglobulin and/orcomplement components,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries)
Leukocytoclastic immune complexvasculitis of small vessels(mostly postcapillary venules,occasionally small veins orarterioles)
Skin-limited immune complexvasculitis
Anti–GBM disease Vasculitis affecting glomerularcapillaries, pulmonarycapillaries, or both, with GBMdeposition of anti-GBMautoantibodies
None None
CV Vasculitis with cryoglobulinimmune deposits affecting smallvessels (predominantlycapillaries, venules, orarterioles); associated withserum cryoglobulins
Leukocytoclastic vasculitis of smallvessels (postcapillary venules,small veins, or arterioles);associated with serumcryoglobulins (usually type IIand type III)
Skin-limited CV, without systemicvasculitis
IgA vasculitis(Henoch-Sch€onlein)
Vasculitis with IgA1-dominantimmune deposits, affecting smallvessels (predominantlycapillaries, venules, orarterioles)
Leukocytoclastic IgA1-dominantvasculitis of mostly postcapillaryvenules and also veins orarterioles in the skin, withvascular IgA deposits
Skin-limited IgA vasculitis, withoutsystemic vasculitis
176 SUNDERK€OTTER ET AL

Pyoderma gangrenosum-like lesions
• Histology: vasculitis, granuloma• Repeated biopsies
Cambourg, et al. Rev Med Int 2016

Localized form of GPA
• Limited expressions of GPA • ANCA less positive• Diagnosis more difficult• Not as easy to treat• Eye, ENT, lung or skin

5 years-survival with Five factor score
Revised FFS (2009) ScoreAge > 65 + 1
Renal failure (creatinine > 150 umol/L) + 1
Cardiac failure (clinical symptoms) + 1
Severe intestinal disorder (bleeding, bowel perforation,
pancreatitis)
+ 1
ENT (confirmed by ENT specialist + CT imaging) - 1
90%0
70%1
40%>1
Guillevin L, et al. Medicine 2011

Relapses
• 40% within 5 years, despite treatment• ANCA PR3+; titer increases• CYP > 10 g during the first 6 months; predisolon > 20 mg/d
during the first 3 months• Heart and lung initially affected

EOSINOPHILIC GRANULOMATOSIS WITHPOLYANGIITIS (CHURG AND STRAUSS)
ANCA associated vasculitides and Polyarteritis Nodosa

Main characteristics
Necrotizing small vessel-vasculitis with granulomas
The less common of ANCA vasculitis
P-ANCA 40% (IIF), MPO
Middle-aged patients (50 yo)
Prevalence: 11-13/million

Extra-cutaneous manifestations
General signs Fever, asthenia, weight loss, joint pain, myalgia
Lung Asthma +++; IAH
Eosinophilia >1500/mm3ENT Rhinitis; polyposis; sinusitis
Heart* Pericarditis; myocarditis
PNS Mononeuritis multiplex (fibula)Kidney (15%) GN
Gastro-intestinal (30-60%) Pain, nausea, vomiting, bleeding
*EGPA ANCA -
Montelukast, Omalizumab:
triggering or revealing factors?
Guillevin L. Presse Med 2012

Year N patients Dermatologic manifestations1977 20/30 (66%) Nodules, necrosis1984 11/16 (70%) Nodules, purpura, papules1991 11/16 (70%) Nodules, purpura, papules, Raynaud 1992 8/12 (67%) NA1997 36/90 (40%) NA1999 49/96 (51%) Purpura, nodules, papules, livedo2001 26/32 (81%) Purpura, papules, nodules, digital necrosisTotal 161/292 (55%)
Chumbley, LanHam, Haas, Abu Shakra, Guillevin, Solans
Cutaneous manifestations
40-75%; rarely inaugural (6%)

Cutaneous histology
C. Francès, Hôpital Tenon, FranceSunderkötter et al. Arthritis Rheum 2018.
Table 4. Systemic and cutaneous variants of small vessel vasculitis*
CHCC12vasculitis category, name
AbbreviatedCHCC2012 definition
Cutaneous component ofsystemic vasculitis
Skin-limited orskin-dominant variant
ANCA-associated vasculitis Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries);associated with ANCAs
Vasculitis of cutaneouspostcapillary venules, smallveins, arterioles, and smallarteries; associated with ANCAs
ANCA-associated vasculitislimited to the skin (not furtherspecified)
MPA Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,or arterioles)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), often withleukocytoclasia and withoutgranulomatous inflammation
Skin-limited MPA (includingdrug-induced skin-limitedMPA); vasculitis of small vesselsin the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), withoutcutaneous granulomatousinflammation and withoutsystemic vasculitis; associatedwith ANCAs
GPA Necrotizing granulomatousinflammation usually involvingthe upper and lower respiratorytracts, and necrotizing vasculitisaffecting predominantly small-to-medium vessels (e.g.,capillaries, venules, arterioles,arteries, and veins)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, small veins,or small arteries), often withleukocytoclasia andnonvasculitic extravasculardermal granulomatousinflammation
Skin-limited GPA (includingdrug-induced skin-limited GPA);vasculitis of small vessels in theskin (spectrum as in MPA), withnonvasculitic extravasculardermal granulomatousinflammation but withouteosinophilia, without a historyof asthma, and without systemicvasculitis; associated withANCAs
EGPA Eosinophil-rich and necrotizinggranulomatous inflammationoften involving the respiratorytract, and necrotizing vasculitispredominantly affecting small-to-medium vessels andassociated with a history ofasthma and eosinophilia
Eosinophil-rich vasculitis of small-to-medium vessels in the skin(postcapillary venules, arterioles,small venules, or small arteries),sometimes with leukocytoclasiaand, e.g., nonvasculiticextravascular dermalgranulomatous inflammation
Skin-limited EGPA (includingdrug-induced skin-limitedEGPA); eosinophil-richvasculitis of small vessels in theskin (spectrum as in MPA),with, e.g., nonvasculiticextravascular dermalgranulomatous inflammation,and with a history of asthma,but without systemic vasculitis;associated with ANCAs
Immune complex vasculitis Vasculitis with moderate-to-marked vessel wall deposits ofimmunoglobulin and/orcomplement components,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries)
Leukocytoclastic immune complexvasculitis of small vessels(mostly postcapillary venules,occasionally small veins orarterioles)
Skin-limited immune complexvasculitis
Anti–GBM disease Vasculitis affecting glomerularcapillaries, pulmonarycapillaries, or both, with GBMdeposition of anti-GBMautoantibodies
None None
CV Vasculitis with cryoglobulinimmune deposits affecting smallvessels (predominantlycapillaries, venules, orarterioles); associated withserum cryoglobulins
Leukocytoclastic vasculitis of smallvessels (postcapillary venules,small veins, or arterioles);associated with serumcryoglobulins (usually type IIand type III)
Skin-limited CV, without systemicvasculitis
IgA vasculitis(Henoch-Sch€onlein)
Vasculitis with IgA1-dominantimmune deposits, affecting smallvessels (predominantlycapillaries, venules, orarterioles)
Leukocytoclastic IgA1-dominantvasculitis of mostly postcapillaryvenules and also veins orarterioles in the skin, withvascular IgA deposits
Skin-limited IgA vasculitis, withoutsystemic vasculitis
176 SUNDERK€OTTER ET AL
Table 4. Systemic and cutaneous variants of small vessel vasculitis*
CHCC12vasculitis category, name
AbbreviatedCHCC2012 definition
Cutaneous component ofsystemic vasculitis
Skin-limited orskin-dominant variant
ANCA-associated vasculitis Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries);associated with ANCAs
Vasculitis of cutaneouspostcapillary venules, smallveins, arterioles, and smallarteries; associated with ANCAs
ANCA-associated vasculitislimited to the skin (not furtherspecified)
MPA Necrotizing vasculitis with few orno immune deposits,predominantly affecting smallvessels (i.e., capillaries, venules,or arterioles)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), often withleukocytoclasia and withoutgranulomatous inflammation
Skin-limited MPA (includingdrug-induced skin-limitedMPA); vasculitis of small vesselsin the skin (postcapillaryvenules, arterioles, venules, orsmall arteries), withoutcutaneous granulomatousinflammation and withoutsystemic vasculitis; associatedwith ANCAs
GPA Necrotizing granulomatousinflammation usually involvingthe upper and lower respiratorytracts, and necrotizing vasculitisaffecting predominantly small-to-medium vessels (e.g.,capillaries, venules, arterioles,arteries, and veins)
Vasculitis of small-to-mediumvessels in the skin (postcapillaryvenules, arterioles, small veins,or small arteries), often withleukocytoclasia andnonvasculitic extravasculardermal granulomatousinflammation
Skin-limited GPA (includingdrug-induced skin-limited GPA);vasculitis of small vessels in theskin (spectrum as in MPA), withnonvasculitic extravasculardermal granulomatousinflammation but withouteosinophilia, without a historyof asthma, and without systemicvasculitis; associated withANCAs
EGPA Eosinophil-rich and necrotizinggranulomatous inflammationoften involving the respiratorytract, and necrotizing vasculitispredominantly affecting small-to-medium vessels andassociated with a history ofasthma and eosinophilia
Eosinophil-rich vasculitis of small-to-medium vessels in the skin(postcapillary venules, arterioles,small venules, or small arteries),sometimes with leukocytoclasiaand, e.g., nonvasculiticextravascular dermalgranulomatous inflammation
Skin-limited EGPA (includingdrug-induced skin-limitedEGPA); eosinophil-richvasculitis of small vessels in theskin (spectrum as in MPA),with, e.g., nonvasculiticextravascular dermalgranulomatous inflammation,and with a history of asthma,but without systemic vasculitis;associated with ANCAs
Immune complex vasculitis Vasculitis with moderate-to-marked vessel wall deposits ofimmunoglobulin and/orcomplement components,predominantly affecting smallvessels (i.e., capillaries, venules,arterioles, and small arteries)
Leukocytoclastic immune complexvasculitis of small vessels(mostly postcapillary venules,occasionally small veins orarterioles)
Skin-limited immune complexvasculitis
Anti–GBM disease Vasculitis affecting glomerularcapillaries, pulmonarycapillaries, or both, with GBMdeposition of anti-GBMautoantibodies
None None
CV Vasculitis with cryoglobulinimmune deposits affecting smallvessels (predominantlycapillaries, venules, orarterioles); associated withserum cryoglobulins
Leukocytoclastic vasculitis of smallvessels (postcapillary venules,small veins, or arterioles);associated with serumcryoglobulins (usually type IIand type III)
Skin-limited CV, without systemicvasculitis
IgA vasculitis(Henoch-Sch€onlein)
Vasculitis with IgA1-dominantimmune deposits, affecting smallvessels (predominantlycapillaries, venules, orarterioles)
Leukocytoclastic IgA1-dominantvasculitis of mostly postcapillaryvenules and also veins orarterioles in the skin, withvascular IgA deposits
Skin-limited IgA vasculitis, withoutsystemic vasculitis
176 SUNDERK€OTTER ET AL

• Maximum 1 mg/kg/d• M3: 50% of the dose• M6 10 mg/day• Maintenance 5-10 mg/day
FFS=0
GCS
• CYC IV D0,14,21 and every 3 wk• Azathioprine 2 mg/kg/j 12-18 mo• MTX 0,3 mg/kg• MMF if failure of Aza/MTX• Rituximab• Mepolizumab (anti-IL5 Ab)
FFS≥1
GCS+IS
Guillevin L. Presse Med 2012Wechsler ME, et al. N Engl J Med 2017
Treatment

MPA AND PANANCA associated vasculitides and Polyarteritis Nodosa

33� --
Haugeberg, 1998
-�0,4-2-�2-3
Reinhold-Keller, 2005
31�-25 �-Mahr, 2004
31 � -94 � -
Mohammad, 2007
Prevalence�Incidence/1,000,000
PANMPA
2,6 �0,623,8 � 3,4
Romero-Gomez, 2015
-15 � 2,4
Pamuk, 2016
-�9,7-�8,4Watts, 2011
-�6,2-�11,6Watts, 2011
-� 10,2
Panagiotakis, 2009

Distinguishing PAN and MPA 1990 ACR Criteria for PAN• Weight loss > 4 kg
• Livedo reticularis
• Testicular pain or tenderness
• Myalgias, weakness
• Mononeuropathy or polyneuropathy
• Diastolic BP > 90 mm Hg
• Elevated BUN or creatininemia
• Hepatitis B virus
• Arteriographic abnormality
• Biopsy of small or medium-size artery containing
polymorphonuclear neutrophils
PAN if at least 3+ criteria have to be present (Se : 82.2%; Sp: 86.6%)
1994 Chapel Hill Consensus Conference nomenclature for PANNecrotizing inflammation of medium-size or small arteries without glomerulonephritis or vasculitis in arterioles,
capillaries or venules
ACR did not distinguish between PAN and MPA
1994 Chapel Hill Consensus Conference nomenclature for MPANecrotizing vasculitis, with few or no immune deposits, affecting small vessels (capillaries, venules or arterioles).
Necrotizing arteritis involving small and medium-size vessels may be present. Necrotizing glomerulonephritis is
very common. Pulmonary capillaritis often occurs.
CHCC 1994
distinguishes PAN and MPA
but disappointing for diagnostic
screening in routine clinical
conditions

European Medicines Agency (EMA) classification algorithm 2007
Clinical diagnosis of primary systemic vasculitis (PAN, Wegener’s granulomatosis, microscopic polyangiitis or Churg-Strauss syndrome) and non-fullfillment of classification criteria for entries other than PAN and histology compatible with the CHCC PAN or typical angiographic features
Diagnostic criteria for PAN (Henegar et al, 2008)
3 positive parameters: HBV infection, arteriographic anomalies, neuropathy5 negative parameters : ANCA, asthma, ENT, glomerulonephropathy, cryoglobulinemia
2012 Revised Chapel Hill Consensus Conference nomenclature for MPA = 1994 CHCC
Necrotizing vasculitis, with few or no immune deposits, affecting small vessels (capillaries, venules or arterioles). Necrotizing arteritis involving small and medium-size vessels may be present. Necrotizing glomerulonephritis isvery common. Pulmonary capillaritis often occurs.
2012 Revised Chapel Hill Consensus Conference nomenclature for PAN
Necrotizing arteritis of medium or small arteries without glomerulonephritis or vasculitis in arterioles, capillaries, or venules, and not associated with antineutrophil cytoplasmic antibodies (ANCAs).
Distinguishing PAN and MPA

Initial clinical manifestations of PAN and MPA
Agard C et al, Arthritis Rheum 2003
PAN (%, n = 36) MPA (%, n = 36)General signs/Poor condition• Only general signs• Fever• Weight loss• Asthenia
81-475042
6117*423325
Myalgias 44 42
Arthralgias 28 31
Peripheral neuropathy 33* 11GI symptoms 25* 3Skin 11 14
Kidney 3 -
Testicle 13 -
Heart 3 8
Initial manifestations are similar except for neuropathy and GI symptoms (PAN) or
isolated general signs (MPA)

Clinical manifestations of PAN and MPA, at diagnosis
PAN (%, n = 36) MPA (%, n = 36)General signs/Poor condition• Fever• Weight loss
815369
755664
Myalgias 56 56Arthralgias 44 56Peripheral neuropathy 75* 56Lung• Alveolar hemorrhage
6-
22*11
GI symptoms 53* 22Skin 28 53*Kidney 22 19Testicle 21 5Heart 17 17
Agard C et al, Arthritis Rheum 2003


Cutaneous manifestations are independant from lung manifestations,
GI tract manifestations, microaneurysms/stenosis (GI, kidney) for
PAN, ANCA for MPA, Prognosis (FFS)

Cutaneous small vessel involvement shouldnot rule out the diagnosis of PAN
Major interest for the confirmation of the systemic vasculitis (biopsy)
Low interest for distinction betweenPAN/MPA

PAN MPAVasculitis Necrotizing vasculitis, polymorphic
infiltrate, extravascular granulomaNecrotizing vasculitis, polymorphicinfiltrate, no extravasculargranuloma
Vessels MEDIUM-size +/- small arterioles SMALL (venules, capillaries, smallarteries) +/- medium-size vessels
Renal infarcts Yes NoGlomerulonephritis No FrequentAlveolar haemorrhage No YesMononevritis mult. 50 – 80% 10 – 20%Relapse Rare (lower than MPA) FrequentP-ANCA, MPO No FrequentHBV infection < 5-10% NoArteriography: aneurysms/stenoses Yes No

Corticosteroids protocol for ANCA vasculitisaccording to the FVSG
Day 1 – 3: methylprednisolon, bolus, 7,5-15 mg/kg (in the cases of severe forms)• Day 1 (or day 4) 1 mg/kg/d• Day 21: 0,75 mg/kg/d• Day 42: 0,5 mg/kg/d• Day 56 (wk 8): 0,4 mg/kg/d• Day 84 (wk 12): 0,33 mg/kg/d• Day 112 (wk 16): 0,25 mg/kg/d
During the first 4 months, prednisolon > 15 mg/d• Month 5: 15 mg/d• Month 6: 12,5 mg/d• Month 9 to 12: 10 mg/d• Then progressive tapering until withdrawal if possible at month 18 or before
Guillevin L et al. Presse Med 2007

Management of limited MPA and non-HBV PAN
FFS =0or
limited to theskin
Corticosteroidsalone
1 mg/kg/d
3-4 months15 mg/d
In case of failure, relapse, progression to
severity ordependance :
Aza, MTX
Makhzoum JP et al. Rev Rhum 2017

Management of severe MPA = (Wegener’s) GPA
INDUCTION MAINTENANCE
3-6 mo > 18 mo
Cyclophosphamide
Rituximab
375 mg/m2/semor 1 g day 1 – day 15
IV (bolus) 15 mg/kgD1, 15, 29 and
every 3 wks
po 2 mg/kg/d
+/- plasmapheresis?
500 mg every 6 mo or 1 g every 4 mo ?
Azathiorprine 2 mg/kg/d
Methotrexate 0,3 g/kg/sem
Leflunomide 20 mg/d
MFM 2 g/L
5 mg/d ?
Corticosteroids
Makhzoum JP et al. Rev Rhum 2017

• 10-year follow-up of 64 patients with PAN or MPA (FFS > 0) • Randomized trial for CS + CYC 6 or 12 times IV • 83% of remission (> 3 mo without symptoms) after induction– 46% had at least one relapse
• 10 years overall survival 57,4% and 10 year DFS 29,9%
Samson M, et al Clin Exp Rheumatol 2017

• Systemic necrotising vasculitides are chronic diseases that require long-lasting maintenance therapy because of their high relapse rates
• Impact of GC-related side effects remains high for all sequelae(osteoporosis, avascular osteonecrosis, cataract, hypertension and diabetes)
Samson M, et al Clin Exp Rheumatol 2017

PAN
Classicidiopathic
generalized
CutaneousPAN
ChildhoodPAN
HBV associated
Ozen S. Nat Rheu, Rev 2017
The expending concept of PAN

PAN
Classicidiopathic
generalized
CutaneousPAN
ChildhoodPAN
HBV associated
Severe / Life threatning• GCS + CYC (preferentially IV)• Switch from CYC to AZA or MTX for remission
maintenance
Non-severe• GCS alone• +/- GCS sparing IS (AZA or MTX)
De Menthon M, et al: Clin Exp Rheumatol 2011

• More frequent peripheral neuropathy, abdominal pain, cardiomyopathy, orchitis, HTA
• Less relapse• Better outcome
• Antiviral agents• Short term GCS• Plasma exchanges
• (vaccination)
PAN
Classicidiopathic
generalized
CutaneousPAN
ChildhoodPAN
HBV associated

PAN
Classicidiopathic
generalized
CutaneousPAN
ChildhoodPAN
HBV associated
• Subcutaneousnodules; ulcers; atrophie blanchescar, livedo
• Lower limbs• +/- neuropathy• +/- myalgias and
arthralgias
• NSAIDS• Colchicine• GCS• Dapsone• IS: Aza, MTX, MMF…
Macularlymphocytic arteritis

Atrophie blanche
Scaring process resulting from various types of injuries and not indicative of a specific
entity +++
Chronicvenous
insufficienyCutaneous
PANLivedoid
vasculopathyLupus
SclerodermaDegos
disease

Macular lymphocytic arteritis
Sadahira C, et al. J Am Acad Dermatol 2005; Al-Daraji W, et al. Am J Dermatopathol 2008; Buckthal-McCuin J, et al. Pediatr Dermatol 2009
• Described in 2003 • Skin limited small-vessel vasculitis• Erythematous or hyperpigmented, reticulated
patches and macules arising preferentially on the lower limbs without ulcerative evolution
• Chronic and indolent course• Lymphocytic arteritis at various stages

• Monocentric retrospective review of 35 cPAN
• 19/35 (54%) of the patients with cPAN have MLA lesions
• The results did not favor the classification of cPAN and MLA as distinct entities
• MLA may be the first manifestation of cPAN
Buffiere-Morgado A, et al. J Am Acad Dermatol 2015Taconet S, et al. Ann Dermatol Venereol 2015

• Histopathology of MLA
– Arteritis
– (1) Predominant (> 50%) lymphocytic
vessel wall infiltrate
– (2) the absence of neutrophils in the
vessel wall infiltrate
– (3) a typical hyalinized fibrin ring in the
vessel lumina, and
– (4) the absence of internal elastic
lamina disruption (assessed by an
orceine staining)
Taconet S, et al. Ann Dermatol Venereol 2015

PAN
Classicidiopathic
generalized
CutaneousPAN
ChildhoodPAN
HBV associated
Ozen S. Nat Rev Rheumatology 2017
Monogenetic diseases• SAVI• DADA2• FMF associated PAN• RAG deficiency• TAP deficiency

Childhood PAN
Ozen S, et al. Ann Rheum Dis 2010
Childhood-PAN EULAR/PRINTO/PRES Ankara 2008 classification
MANDATORY CRITERION Histopathology OR angiographic abnormalities+ 1 of the 5 following Skin involvement
Myalgia/muscle tendernessHypertensionPeripheral neuropathyRenal involvement
Livedo reticularis/racemosaSubcutaneous nodulesSuperficial skin ulcers or other minor ischaemic changes: nailbed infarctions, splinthaemorrhages, digital pulp necrosisDeep skin infarctions: ulcers, digital phalanx or other peripheral tissue (nose and ear tips) necrosis/gangrene
Se 89,6%, Sp 99,6%

ADA2 deficiency (DADA2): Early stroke + vasculopathy
• Autoinflammatory disease– AR, mutation CECR1 (LoF) – ↘ Adenosine deaminase-2
• Symptoms– Intermittent fevers + early-onset lacunar
strokes and other neurovascularmanifestations + vasculopathy + hypogammaglb
– ”PAN-like” presentation– Family history of PAN
• TNF alpha inhibition (etanercept, thalidomide)
Zhou Q, et al. N Engl J Med 2014Caorsi R, et al. Ann Rheum Dis 2017

ADA2 deficiency (DADA2): Early stroke + vasculopathy
Caorsi R, et al. Ann Rheum Dis 2017

• DADA2 in case of early childhood cPAN• Mutation of CERC1 in two siblings
Gonzalez Santiago, et al. JAMA Dermatol 2015

STING-Associated Vasculopathy with onset in Infancy(SAVI)
• Autoinflammatory disease (2014)– AD, mutation TMEM173 (GoF)– ↗ STING-interferon pathway– Interferonopathy
• Symptoms– Early in life (< 6 mo)– Low-grade fever + severe vasculopathy [vasculitis +
microthrombotic angiopathy] + lung inflammation + systemic inflammation
– Autoimmunity (ANA, ANCA)
• Blockade of interferon pathway (JAK inhibitors, anti-IFN Ab…) ?
Liu Y, et al. N Engl J Med 2014
STimulator of INterferon Genes

Familial Mediteranean Fever and vasculitis
• Autoinflammatory disease– AR, mutation MEFV (pyrin)– Fever + seritis (peritonitis, pleuritis) + arthritis + erysipela like attacks
• 1% of the patients with FMF – FMF precedes PAN– Occurs at a younger age– Less HBV , less PNS involvement– More myalgias, perirenal hematomas, CNS involement– Better prognosis
• Similar treatment as classic PAN + colchicine
Aksu K, et al. Rheumatol Int 2011

Conclusion
• PAN has become an even more uncommon form of vasculitis– Either a true change in PAN epidemiology (HBV vaccination, etc)– Or by a gradual narrowing of its place in the spectrum of systemic
vasculitis
• Cutaneous MPA and PAN treatments do not need to be as intense as the severe generalized forms
• Identification of autoinflammatory diseases with PAN like featuresenables the use of targeted therapies and help to understand the physiopathogeny of the disease

Necrotizing vasculitis (GFEV, EUVAS, VCRC)
PAN HBV - CS 1 mg/kg/j +/- MP bolus (1-3, 15 mg/kg/j)
EDX IV : 1) 3 bolus 0,6 g/m2 /14d, 2) 3 bolus 0,7g/m2/21 d.
No oral EDX (bladder K)
Azathioprine; MFM; MTX; IVIg only in children
MPA FFS = 0 : CS alone
FFS = 1 or + : cf WG
Wegener
(FFS > 1)
Induction by EDX (0,6 g/m2 D0, 14, 28 and 0,7 g/m2/21d
until remission: 6-9 maximum) or RTX (4x 375 mg/m2/wk).
RTX better than EDX in cases of relapes
Maintenance: Aza (2 mg/kg/d) or MTX (0,3 mg/kg/wk);
MFM (more relapse)
Anti-TNF alpha: ETC No, IFX possible but not long lasting
Churg/Strauss FFS = 0 : CS alone
FFS = 1 or + : EDX
Mepolizumab (anti-IL5, under trial), Omalizumab (anti-IgE,
NO), IFN-alpha
Guillevin L. How to treat systemic necrotizing vasculitides?. Presse Med 2012;41:1024-30.