Embed Size (px)
DESCRIPTION
anatomy
Citation preview

Name : Muhammad RamdhaniNPM : 130110110118Group : E5
Anatomy of Abdominal Wall
Although the abdominal wall is continuous, it is subdivided into the anterior wall, right and left lateral walls, and posterior wall for descriptive purposes. The wall is musculoaponeurotic, except for the posterior wall, which includes the lumbar region of the vertebral column. The boundary between the anterior and the lateral walls is indefinite, therefore the term anterolateral abdominal wall is often used. The anterolateral abdominal wall extends from the thoracic cage to the pelvis.
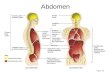
The anterolateral abdominal wall is bounded superiorly by the cartilages of the 7th-10th ribs and the xiphoid process of the sternum, and inferiorly by the inguinal ligament and the superior margins of the anterolateral aspects of the pelvic girdle (iliac crests, pubic crests, and pubic symphysis).
The anterolateral abdominal wall consists of skin and subcutaneous tissue (superficial fascia) composed mainly of fat, muscles and their aponeuroses and deep fascia, extraperitoneal fat, and parietal peritoneum. The skin attaches loosely to the subcutaneous tissue, except at the umbilicus, where it adheres firmly. Most of the anterolateral wall includes three musculotendinous layers; the fiber bundles of each layer run in different directions.
Fascia of the Anterolateral Abdominal WallThe subcutaneous tissue over most of the wall includes a variable amount
of fat. It is a major site of fat storage.Superior to the umbilicus, the subcutaneous tissue is consistent with that
found in most regions. Inferior to the umbilicus, the deepest part of the subcutaneous tissue is reinforced by many elastic and collagen fibers, so it has two layers: the superficial fatty layer (Camper fascia) and the deep membranous layer (Scarpa fascia) of subcutaneous tissue. The membranous layer continues inferiorly into the perineal region as the superficial perineal fascia (Colles fascia).
Superficial, intermediate, and deep layers of investing fascia cover the external aspects of the three muscle layers of the anterolateral abdominal wall and their aponeuroses (flat expanded tendons) and cannot be easily separated from them. The investing fascias here are extremely thin, being represented mostly by the epimysium (outer fibrous connective tissue layer surrounding all muscles) superficial to or between muscles. The internal aspect of the abdominal wall is lined with membranous and areolar sheets of varying thickness called the endoabdominal fascia. The glistening lining of the abdominal cavity, the parietal peritoneum, is formed by a single layer of epithelial cells and supporting connective tissue. The parietal peritoneum is internal to the transversalis fascia and is separated from it by a variable amount of extraperitoneal fat.
Muscles of Anterolateral Abdominal WallThere are five (bilaterally paired) muscles in the anterolateral abdominal
wall: three flat muscles and two vertical muscles. The three flat muscles are the external oblique, internal oblique, and transversus abdominis. All three flat

muscles are continued anteriorly and medially as strong, sheet-like aponeuroses. Between the midclavicular line (MCL) and the midline, the aponeuroses form the tough, aponeurotic, tendinous rectus sheath enclosing the rectus abdominis muscle. The aponeuroses then interweave with their fellows of the opposite side, forming a midline raphe (G. rhaphe, suture, seam), the linea alba (L. white line), which extends from the xiphoid process to the pubic symphysis. The two vertical muscles of the anterolateral abdominal wall, contained within the rectus sheath, are the large rectus abdominis and the small pyramidalis.
FUNCTIONS AND ACTIONS OF ANTEROLATERAL ABDOMINAL MUSCLESThe muscles of the anterolateral abdominal wall:
Form a strong expandable support for the anterolateral abdominal wall. Support the abdominal viscera and protect them from most injuries. Compress the abdominal contents to maintain or increase the intra-
abdominal pressure and, in so doing, oppose the diaphragm (increased intra-abdominal pressure facilitates expulsion).
Move the trunk and help to maintain posture.
The combined actions of the anterolateral muscles also produce the force required for defecation (discharge of feces), micturition (urination), vomiting, and parturition (childbirth). Increased intra-abdominal (and intrathoracic) pressure is also involved in heavy lifting, the resulting force sometimes producing a hernia.
Neurovasculature of Anterolateral Abdominal Wall
DERMATOMES OF ANTEROLATERAL ABDOMINAL WALLThe map of dermatomes of the anterolateral abdominal wall is almost identical to the map of peripheral nerve distribution. This is because the anterior rami of spinal nerves T7-T12, which supply most of the abdominal wall, do not
participate in plexus formation. Each dermatome begins posteriorly overlying the intervertebral foramen by which the spinal nerve exits the vertebral column and follows the slope of the ribs around the trunk. Dermatome T10 includes the umbilicus, whereas dermatome L1 includes the inguinal fold.

NERVES OF ANTEROLATERAL ABDOMINAL WALLThe skin and muscles of the anterolateral abdominal wall are supplied
mainly by the following nerves: Thoracoabdominal nerves: these are the distal, abdominal parts of the
anterior rami of the inferior six thoracic spinal nerves (T7-T11); they are the former inferior intercostal nerves distal to the costal margin.
Lateral (thoracic) cutaneous branches: of the thoracic spinal nerves T7-T9 or T10.
Subcostal nerve: the large anterior ramus of spinal nerve T12. Iliohypogastric and ilioinguinal nerves: terminal branches of the anterior
ramus of spinal nerve L1.
VESSELS OF ANTEROLATERAL ABDOMINAL WALLThe primary blood vessels
(arteries and veins) of the anterolateral abdominal wall are the
Superior epigastric vessels and branches of the musculophrenic vessels from the internal thoracic vessels.
Inferior epigastric and deep circumflex iliac vessels from the external iliac vessels.
Superficial circumflex iliac and superficial epigastric vessels from the femoral artery and greater saphenous vein,
respectively. Posterior intercostal vessels of the 11th intercostal space and the anterior
branches of subcostal vessels.
Lymphatic drainage of the anterolateral abdominal wall follows the following patterns:
Superficial lymphatic vessels accompany the subcutaneous veins; those superior to the transumbilical plane drain mainly to the axillary lymph nodes; however, a few drain to the parasternal lymph nodes. Superficial lymphatic vessels inferior to the transumbilical plane drain to the superficial inguinal lymph nodes.
Deep lymphatic vessels accompany the deep veins of the abdominal wall and drain to the external iliac, common iliac, and right and left lumbar (caval and aortic) lymph nodes.
Abdominal HerniasThe anterolateral abdominal wall may be the site of hernias. Most hernias
occur in the inguinal, umbilical, and epigastric regions Umbilical hernias are common in newborns because the anterior abdominal wall is relatively weak in the umbilical ring, especially in low-birth-weight infants. Umbilical hernias are usually small and result from increased intra-abdominal pressure in the presence of weakness and incomplete closure of the anterior abdominal wall after ligation of the umbilical cord at birth. Herniation occurs through the umbilical ring. Acquired umbilical hernias occur most commonly in women and obese people. Extraperitoneal fat and/or peritoneum protrude into the hernial sac. The lines along which the fibers of the abdominal aponeuroses interlace are also potential sites of herniation (see Fig. 2.6B). Occasionally, gaps exist where these fiber exchanges occur—for example, in the midline or in the transition from aponeurosis to rectus sheath. These gaps may be congenital, the result of the stresses of obesity and aging, or the consequence of surgical or traumatic wounds.
An epigastric hernia, a hernia in the epigastric region through the linea alba, occurs in the midline between the xiphoid process and the umbilicus. Spigelian hernias are those occurring along the semilunar lines (see Table 2.1B). These types of hernia tend to occur in people older than 40 years and are usually associated with obesity. The hernial sac, composed of peritoneum, is covered with only skin and fatty subcutaneous tissue.