-
02
| /
-
1
This lecture includes the slides that the doctor read and I
added the doctors words right in the boxes.
The doctor started by making a correction, which is the
additional slides on the website.
UreDers Muscular Tube Measuring About 25 Cm. Begin
at Renal Pevis, then descend retroperitoneally and anterior to
psoas muscle to posterior surface of Urinary bladder.
Then cross pelvic inlet into minor (true) pelvis where they are
still retroperitoneal and cross anterior to Common Iliac
Bifurcation And Anterior To Sacro-iliac Joint. Then it follows the
course of internal iliac artery (which goes to the pelvis).
Could Be Compromised By Aneurysm Of Common Iliac
End at ureterovesical and open into bladder and define upper
border of urinary bladder trigone.
3 Normal Constrictions (Kidney Stones Get Stuck): (1) At
Ureteropelvic( the beginning of the ureter
as it leaves the kidney) (2) Where Ureters Cross Pelvic Inlet
(Brim) (bending) (3) And At Ureterovesical (Intramural) (the end of
it)
Right Ureter Relations:
Anteriorly: Duodenum, ileum right testicular/ovarian vessels,
Right colic vessels, and mesentery of small
intestine. Posteriorly: Right Psoas muscle and bifurcation of
common iliac artery.
Left Ureter Relations: Anteriorly: Sigmoid colon and mesocolon
and left Colic vessels, Testicular/Ovarian artery. Posteriorly:
Left Psoas muscle and bifurcation of common iliac artery.
It is a muscular tube lined by surface epithelium, then we have
connective tissue, then we have the muscular layer, then the serosa
or adventitia.
The doctor said many times that the ureDer end at the SUPERIOR
POSTERIOR aspects of the urinary bladder.
-
2
Blood Supply of the ureter:
Upper Part: Renal Artery.
Mid-part: Ovarian/Testicular Artery. (branches
of aorta)
Lower/Pelvic Part: Superior Vesical artery.
Venous Blood Supply: Correspond to arteries.
Lymphatic drainage: Correspond to LN along
the course of arteries.
Nerve Supply:
Upper part: Renal nerve.
Mid-part: Ovarian/Testicular Nerve.
Lower/Pelvic Part: Hypogastric Plexus.
Afferent fibers enter spinal cord at L1-2 (thats why the
referred pain to that region during renal colic of
the ureter.)
Clinical Points
Long = 25 cm, Narrower and 3 constrictions:
Hence susceptible to renal stones lodgment at constriction
sites.
Renal Colic:
Severe pain experienced when renal stones are lodged.
Afferent fibers enter spinal cord at T 11-12 and L 1-2 (Skin of
Flank loin and
Groin Areas).
Renal stone arrest at Lower Part referred pain felt at Tip of
Penis/Testicles
or labia in case of females.
* Males: pass posterior to ductus deferens Females: pass
posterior & inferior to uterine artery. ***During hysterectomy
(surgical removal of the uterus) ureter can be ligated with uterine
artery. (it is posterior to artery near cervix).
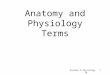
Ovarian and Testicular Artery are
branches from the aorta, because
during embryogenesis testicles
develop intra-abdominally (around
8th week), so testicles have to take
their blood supply form aorta and
after they develop they begin to
descend and exit through internal
ring of the inguinal canal then to the
external ring to the scrotal sac.
In a male infant you have to check
that both testicles are within the
scrotal sac and if there is
undescended testis , this mean it is
within higher a temperature than
the body because spermatogenesis
occur at lower temperature and this
will lead in the future to infertility
-
3
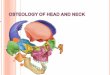
Organ Of Urine Storage (500 Ml). Lies behind Pubic symphysis and
is Pelvic Organ When Empty but rises into Hypogastric region of
abdominal cavity as it fills up.
It is Triangular and has an Apex, Base, A Superior Surface And
2-inferiolateral Surfaces.
Apex: Points Anteriorly and connected to Umblicus by Median
Umblical Ligament (remnant of Urachus).
The Posterior Surface; has Two -lateral angles where Ureters
join the bladder and 2-Vasa deferens run separating the Seminal
Vesicles fro each other.
Superior Surface: Is covered by peritoneum and related to Ileum
and Sigmoid Colon.
The Neck of Urinary bladder is Surrounded by Prostate Lobes
where Prostatic Urethra lies.
The Interior of Urinary bladder Presents Folds/Rugae when Empty.
But A triangular area joining the three openings; 2-ureters and one
internal sphincter is clear of Folds and called Trigone
During pregnancy there will be more
pressure on Urinary Bladder, so as
long as pregnancy on the first 3
months within pelvic there will
pressure symptoms on the urinary
bladder this will result in frequency
of Micturition in the first 3 months
The problem here, as male age (>45)
Prostate undergo Hypertrophic
changes and because prostate have
very dense capsule present at very
constricted anatomical position ,this
hypertrophy it does not extend
outward but also it push inward
where the urethrae pass and this will
lead to different degree of urinary
retention (complete or partial ).
-
4
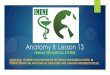
The interior of urinary bladder
The 2 ureters enter the urinary bladder at the 2 lateral angels
in the superior posterior region. The
area above the entrance of the 2 ureters is called the
fundus.
And notice in the picture the internal urethral orifice (which
is under the autonomic nervous
system) and the external (which is voluntary).
Now regarding the interior aspect of the urinary bladder, like
any organ in the body that is subjected
to distension (the stomach for e.g.). You can see that it's
folded to allow it to extend. These folds are
called "Rugae".
- still in the interior aspect we have a triangular area that
extend between the 2 upper lateral points
(which represent the opening of the 2 ureters) and the internal
urethral orifice. This area is called
the "trigon".
Trigone of the bladder is not folded, it smooth; the significant
of this is Because if its folded this will
affect the potency of the tube (ureter), that means the urine
will not pass easily from the ureter to
the bladder.
-
5
- At the neck of urinary bladder we have the prostatic urethra
and prostate (regarding males) while in females related to
urogenital diaphragm.
In females the UB and the urethra are
anterior to the uterus. There are 2 pouchs
(empty potential space) which are "Recto-
uterine" pouch behind the uterus
(between the uterus and the rectum) &
"viscero-uterine" pouch in front of the
uterus.
Regarding males as we said we have the prostate gland at the
neck of the bladder. And in the
urethra there is an opening for the vas deference which passes
within the substance of the prostate
gland carrying semen to the ejaculatory duct; this part of
urethra is called prostatic urethra. Then
the urethra pass through the urogenital diaphragm.
The blood supply and innervation of the Urinary
bladder:
- It's supplied by Superior and Inferior Vesical arteries which
are branches of Internal Iliac Artery.
- Regarding the venous drainage it's correspond to the arteries
and drain into the internal iliac vein.
- Nerve Supply via the Inferior Hypogastric Plexus from
Sympathetic fibers of L 1-2
The doctor scolded us for not
knowing what is the muscle tone -.-!
Anyone want to know the content,
refer to the record!
-
6
The urinary bladder relation:
Posterior surface (fundus/base):
- In males related to rectovesical pouch, rectum, seminal
vesicles, and ampulla of ductus
deferens
- In females related to anterior wall of vagina
Anterior surface:
Related to pubic symphysis and retropubic space of Retzius
Superior surface:
In males - peritoneal cavity
In females vesicouterine pouch (peritoneal cavity)
Apex:
related to median umbilical lig. or urachus
Neck:
in males related to prostatic urethra and prostate while in
females related to urogenital
diaphragm
Trigone of the bladder:
on posterior surface of bladder and defined superiorly by
ureters and inferiorly by urethra
(internal urethral meatus)
Bladder clinical:
1- In infants the empty bladder lies within the false abdominal
cavity. As it mature (in adults) it
shifts and move into the minor pelvis (true pelvis), but when
full can rise above pelvic inlet.
2- Prostatic Hypertrophy: Affects Males above 45 yrs. Hence
Pressure over Prostatic Urethra and cause Residual volume
and Urgency to Micturation and Possible Retention.
3- Incontinence (total, stress, urge, overflow types):
Uncontrolled passage of urine, it affects female more than
males, it happens due to the emotional
nature of the female (stress, anxiety, pregnancy . ) and due to
some anatomical (structural)
variation in female.
# Prostatic Hypertrophy: Sildenafil
(Viagra) is used as a TT by increasing
cGMP that cause Smooth muscle
relaxation said the doctor.
-
7
URETHRA :
Muscular Tube Carries urine from the Bladder to the outside of
the body
Internal Sphincter prevents urine from emptying; composed of
smooth muscle; involuntary
External Sphincter at the upper portion of the urethra allows
you to resist the urge to urinate; composed
of skeletal muscle; voluntary
Female Short and Wide opens to the outside at the urethral
meatus, subjected more to UTI
Male longer and narrow, passes through the prostate gland;
carries urine and sperm.
Hence Males more prone for Renal Stone arrest But Females more
susceptible to Urinary Tract Infection
Males (3 parts) 1. Prostatic post. wall has urethral crest that
contains 2 openings of ejaculatory ducts. Prostatic
ducts are lateral to urethral crest.
2. Membranous the narrowest crosses urogenital diaphragm and
surrounded by deep
transverse perineal m. and sphincter urethrae m. (external
sphincter)
-Both musc. by pudendal n.
- the place where lodgment of renal stone occur
3. Penile (spongy/cavernous) surrounded by corpus spongiosum,
enlarges into fossa navicularis,
and ends as external urethral meatus. Openings of bulbourethral
glands just below urogenital
diaphragm. (vulnerable to catheter penetration)
-
8
Females
- Courses through urogenital diaphragm and is surrounded by deep
transverse perineal m. and
sphincter urethrae m. (later muscles doesnt completely surround
urethra and is the reason for
high incidence of stress incontinence in women)
- Posterior surface fuses with anterior wall of vagina.
- External urethral orifice stratified Squamous epitheliumopens
into vestibule of vagina between
labia minora.
! ! !
Done by:
Anagreh
Obiedat
Zoubi
Shatnawi