Embed Size (px)
Citation preview

Anatomical M-mode: A novel technique for the quantitative evaluationof regional wall motion analysis during dobutamine echocardiography
Jonathan Chan, Sudhir Wahi, Peter Cain & Thomas H. MarwickUniversity of Queensland, Brisbane, Australia
Received 3 April 2000; accepted in revised form 2 July 2000
Key words: dobutamine echocardiography, M-mode echocardiography, quantitation
Abstract
Recognition of abnormal wall motion during dobutamine echocardiography requires an expert observer.Anatomical M-mode echocardiography may o�er a novel quantitative approach to interpretation, ame-nable to less expert readers. We studied the application of this new modality to 124 patients (80 with knowncoronary anatomy and 44 patients at low probability of coronary disease) who underwent dobutamineechocardiography, using a standard protocol. Wall motion was interpreted by an experienced reader, usingdigitally stored 2-dimensional echocardiographic images at rest and peak stress. Percentage of systolicthickening was measured o�ine using anatomical M-mode echocardiography in the basal and mid seg-ments at rest and peak dose, and compared with wall motion scores and coronary angiography. Of 729segments, wall motion was identi®ed as normal in 449, ischemic or viable in 171 and showed resting WMabnormalities only in 109 segments. After exclusion of the apex, anatomical M-mode measurements werefeasible in 729 of 960 possible basal- and mid-zone segments (76%). Measurement of systolic thickening atpeak dose was reproducible within (r2 � 0:83) and between observers (r2 � 0:93). Systolic thickening wassigni®cantly greater in segments with normal wall motion (37� 2%) compared with ischemic or viablesegments (30� 2%, p < 0:001), and scar segments (23� 3%, p < 0:001). There was an increment ofthickening from rest to stress in normal and viable segments, no change in scar, and a decrement in ischemicsegments. Signi®cant coronary artery disease (de®ned by stenoses >70% diameter) was present in 59patients. Systolic thickening showed signi®cant variation between segments interpreted by wall motionscoring and angiography as true and false positive and true and false negative (p < 0:05). Measurement ofsystolic thickening using anatomical M-mode echocardiography o�ers an objective method to quantifysystolic thickening at dobutamine echocardiography but has limited clinical feasibility.
Introduction
Stress echocardiography has become established asa standard clinical tool for the diagnosis of coro-nary heart disease. While wall motion abnormali-ties may not always re¯ect the severity of coronaryartery disease, qualitative evaluation of regionalfunction of each myocardial segment before, dur-ing and after stress, o�ers an accuracy of 80±85%for the diagnosis of coronary stenoses [1]. The
16 segment model of the American Society ofEchocardiography [2] is often used to derive asemi-quantitative wall motion score. However, thelimitations of wall motion analysis are that themeasurements made are subjective and depend onthe experience of the observer. Picano [3] hasdemonstrated that a learning curve is necessarybefore the acquisition of skills for accurate inter-pretation. Other studies [4] have shown that thereis a concordance of <80% between di�erent
International Journal of Cardiac Imaging 16: 247±255, 2000.Ó 2000 Kluwer Academic Publishers. Printed in the Netherlands.
247

centers with respect to the reproducibility of thisinterpretation.
Given the limitations of the qualitative wallmotion analysis, there is a need for a more objec-tive, quantitative technique for the assessment ofwall motion abnormalities. This quantitative pa-rameter should have greater reproducibility andmay require less skill for interpretation. StandardM-mode echocardiography has traditionally beenused to provide accurate measurement of leftventricular thickening but can only be applied inthe parasternal views. Anatomical M-mode is anovel post-processing technique, derived fromhigh-frame-rate 2-dimensional echocardiography,that permits the quantitative evaluation of wallmotion and thickening in multiple cardiac seg-ments [5]. Early experience has shown a highreproducibility of measurements by independentobservers [5±7]. We sought to evaluate the feasi-bility of using anatomical M-mode imaging toassess wall motion abnormalities during stressechocardiography in patients with known coro-nary anatomy.
Methods
Patient selection
Eighty patients (age 59� 8 years, 54 men) withknown coronary anatomy and 44 control patientswith a low probability of coronary artery disease[8] underwent dobutamine echocardiography,with standard interpretation and measurement ofsegmental wall thickening using anatomical M-mode. The clinical features of patients with cor-onary disease and control patients from the nor-malcy group are summarized in Table 1. Amongthe patients, chest pain was present in 71 (89%),of whom 54 had typical angina; the six patientswithout chest pain had exertional dyspnea thatwas considered to be a possible angina equiva-lent. Coronary disease was known to be presentin 28 patients with a previous myocardial in-farction. The patients' pre-test probability ofcoronary disease, based on symptoms, age andgender [8] was 55� 21%. Most patients (80%)had cardiac risk factors; 35 had hypertension,
13 had diabetes, 55 had hypercholesterolemia,and 17 were smoking.
Dobutamine echocardiography
Dobutamine echocardiography was performedusing a standard dobutamine-atropine protocol[9]. Patients were instructed to discontinue beta-blocking drugs on the day of the test. Undercontinuous clinical, electrocardiographic andechocardiographic monitoring, dobutamine wasinitially infused intravenously at a rate of 5 mc g/kg/min for 3 min and then the dose was sequen-tially titrated to 10, 20, 30 and up to a maximum of40 mc g/kg/min. If the chronotropic response wasinadequate, de®ned by the failure to reach 85% ofage predicted maximum heart rate [9], atropinewas administered to a maximum of 1 mg iv.Protocol completion was attempted in all patients,but the test was terminated prematurely in thepresence of severe ischemia or side-e�ects includ-ing hypertension, hypotension, dysrhythmias orpatient discomfort.
Standard 2-dimensional echocardiography wasobtained using a 3.5 MHz harmonic transducerand a standard commercial echocardiography ma-chine (Vingmed System FiVe, Horten, Norway).Images in the parasternal long- and short-axis,apical four-, three- and two-chamber views weresaved as digital ECG-triggered cine-loops and on
Table 1. Clinical characteristics in patients and controls.
Controls
(n = 44)
Patients
(n = 80)
Age 45 � 6 62 � 12
Male gender 33 (75%) 59 (74%)
Body mass index (kg/m2) 27 � 6 27 � 6
Risk factors
Smoking 2 (5%) 17 (21%)
Hypertension (>140/90) 9 (20%) 35 (44%)
Hypercholesterolemia 7 (16%) 55 (69%)
Diabetes 2 (5%) 13 (16%)
Previous myocardial infarction 0 (0%) 28 (35%)
Medical therapy
Betablockers 11 (25%) 42 (52%)
Calcium antagonists 4 (9%) 21 (26%)
Nitrates 5 (11%) 29 (36%)
248

video tape at rest, low-dose (5 and 10 mc g/kg/min) and peak dose.
Wall motion analysis
Wall motion was scored in each segment at rest,low- and peak-dose, by an experienced readerblinded to clinical, angiographic and anatomicalM-mode measurements. Segments showing aug-mentation with dobutamine were classi®ed asnormal. Ischemia was identi®ed in the presence ofa new or worsening wall motion abnormality [10].Viable segments were those with resting akinesisbut showed subsequent improvement duringstress. Scar was characterized by resting dyskinesisor akinesis.
Quantitative anatomical M-mode
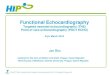
Anatomical M-mode images were obtained by dig-ital reconstruction from 2-dimensional cineloopimages at rest and peak stress (EchoPac 6.0, Ving-med, Horten, Norway) [5]. A freely mobile virtualM-mode line was positioned in the basal and mid-ventricular segments, at right angles to the longi-tudinal axis of the ventricle in the apical images.Apical segments were not included because theirwall motion was tangential to the longitudinal axisof the ventricle, di�cult to measure, and subject toforeshortening. Along this virtual M-mode line, the2-dimensional data were transformed into a tem-poral display similar to that seen in conventionalM-mode (Figure 1). Measurements were made of
Figure 1. Measurement of diastolic and systolic thickness and percent thickening in an apical 2-chamber view (left), using anatomic
M-mode echocardiography across the plane of the cursor on the 2-dimensional image. The anatomic M-mode image shows the motion
of the anterior wall (above) and inferior wall (below) throughout a single cardiac cycle, starting on the R wave. Measurements of the
thickness (thk) and percent systolic thickening (% sys thk) are recorded for the basal anterior (ant) and inferior (walls) as marked in
diastole and systole.
249

the thickness of each muscle segment during dias-tole and systole, and percent systolic thickening wasderived at rest and peak stress.
All measurements were made by a noviceobserver without expertise in stress echocardio-graphy, in order to minimize bias from wallmotion analysis. This reader was also blindedto wall motion analysis and angiographic data.A subset of these measurements (n � 20) wererepeated independently by an experienced observerblinded to the novice reader's measurements. Tocheck intra-observer reproducibility, the studieswere re-measured after an interval of several weeks.
Coronary angiography
Coronary angiography was performed using stan-dard Judkins technique. An independent readermeasured coronary stenoses using a quantitativemeasurement package (CAAS,PieMedical, Leiden,Netherlands). Stenoses >70% diameter in a majorepicardial artery were considered signi®cant.
Statistical analysis
These results were then compared to the wallmotion scores of the corresponding segments usingANOVA statistical package. A similar comparisonof the anatomical M-mode measurements weremade against those segments which had signi®cantcoronary artery disease, de®ned as >70% stenosisin any one vessel. All results were considered sta-tistically signi®cant if their p-values were less than0.05. Reproducibility of the measurements and theintra- and inter-observer correlation was testedusing the Cronbach's alpha statistic for continousvariables. An alpha >0.8 indicated a good corre-lation between the measurements. The intra- andinter-observer agreement was represented by theBland±Altman technique.
Results
Dobutamine echocardiography
The responses to stress in patients with coronarydisease and control patients from the normalcy
group are summarized in Table 2. Among thepatients, the protocol was completed in 64(80%), 16 (20%) had the protocol terminatedbecause of side-e�ects, including hypertension insix (8%), hypotension in one (1%), dysrhythmiasin one (1%), ischemia in six (8%) and otherdiscomfort in two patients. The heart-rate andblood pressure responses were greater in thecontrols, re¯ecting higher heart-rate targets dueto younger age as well as premature conclusionof fewer tests. Ischemic endpoints were identi-®ed in the majority of patients and almost nocontrols.
Anatomical M-mode analysis
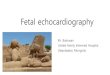
Wall motion was analyzed subjectively in allmyocardial segments. Anatomical M-mode wasattempted in all basal and mid-zone segments, butmeasurements could not be satisfactorily obtainedin 231 segments due to poor image quality. Thus,anatomical M-mode measurements were feasiblein 729 of 960 possible basal- and mid-zone seg-ments (76%). Quantitative measurements usinganatomical M-mode echocardiography showedgood intra-observer (Figure 2a) and inter-observer(Figure 2b) agreement. The Cronbach's alpha forre-test by the same observer was 0.95 and it was
Table 2. Dobutamine stress responses in patients and controls.
Controls Patients
Resting heart rate
(beats/min)
74 � 20 74 � 15
Resting systolic blood
pressure (mmHg)
134 � 36 123 � 30
Max heart rate
(beats/min)
147 � 18 134 � 23
% Age-predicted heart
rate
75% 77%
Peak systolic blood
pressure (mmHg)
158 � 66 151 � 41
Peak rate-pressure
product
23321 � 2500 21001 � 1687
Chest pain 1 (2%) 19 (24%)
ST segment depression
(>0.1 mV)
2 (4%) 14(17%)
Ischemia by Echo 0 (0%) 59 (74%)
Viability by Echo 0 (0%) 5 (6%)
Scar by Echo 0 (0%) 21 (26%)
250

0.98 for agreement between the measurementsmade by the two observers.
The mean values for regional systolic thicken-ing at rest and after stress are listed in Table 3.Although there were some regional variations,the average thickening was 50%. At peak stress,the percent systolic thickening measured by an-atomical M-mode was 37� 1% in normal seg-ments of patients that underwent angiography.This was signi®cantly greater than that in is-chemic segments (30� 2%, p < 0:001), and scarsegments (23� 3%, p < 0:001�. Despite this
relationship, signi®cant spread of the measuredvalues was detected in each group (Figure 3).Nonetheless, the progression of wall thickeningfrom rest to stress corresponded with the patternsobserved with conventional wall motion analysis(Figure 4). Normal segments showed incrementalthickening from a normal baseline, viable seg-ments showed an increment from reduced thick-ening at rest, ischemic segments showed adecrement, and scar segments showed reducedthickening at rest with no change followingstress.
Figure 2. Concordance and Bland±Altman plots showing inter-observer variability (2a) and intra-observer variability (2b).
251

Comparison with coronary angiography
Among patients undergoing coronary angiogra-phy, 21 had no signi®cant stenoses, 23 had singlevessel and 36 had multivessel disease. Wall motionanalysis identi®ed 449 (62%) segments as normal,171 (23%) as ischemic or viable, and 109 (15%)as scar. Wall motion analysis had a sensitivityof 93% (55/59), speci®city of 71% (15/21) andoverall accuracy of 88% for detection of coronaryartery disease.
Myocardial segments subtended by signi®cantcoronary stenoses had a lower percent systolic
thickening �30� 2%) compared to those with non-signi®cant coronary stenosis (35� 1%, p-value< 0:01). Figure 5 illustrates the systolic thickeningrecorded in segments classi®ed on the basis of wallmotion scoring and coronary angiography as trueand false positive, and true and false negative.Systolic thickening is more in false negative thantrue positive studies, implying that the resultsoccurred because the visual threshold for desig-nating wall motion as abnormal was not attained.Conversely, thickening was less in false positivethan true positive studies ± also explaining whysegments were `over-called'.
Table 3. Mean systolic thickening at rest and after stress in control patients.
Rest diast Rest syst Rest thick Peak diast Peak syst Peak thick
Base
Anteroseptum 1.1 � 0.2 1.6 � 0.3 0.4 � 0.2 1.2 � 0.2 1.2 � 0.3 0.5 � 0.2
Septum 1.2 � 0.2 1.7 � 0.2 0.5 � 0.2 1.2 � 0.2 1.8 � 0.3 0.5 � 0.2
Inferior 1.2 � 0.3 1.7 � 0.3 0.5 � 0.2 1.3 � 0.2 1.9 � 0.3 0.5 � 0.2
Lateral 1.1 � 0.2 1.7 � 0.2 0.6 � 0.2 1.1 � 0.1 1.8 � 0.3 0.7 � 0.2
Posterior 1.2 � 0.3 1.6 � 0.3 0.4 � 0.2 1.2 � 0.2 1.8 � 0.3 0.5 � 0.1
Anterior 1.0 � 0.1 1.7 � 0.2 0.6 � 0.2 1.2 � 0.2 1.8 � 0.3 0.6 � 0.2
Mid
Anteroseptum 1.1 � 0.2 1.6 � 0.3 0.5 � 0.2 1.2 � 0.2 1.8 � 0.3 0.5 � 0.2
Septum 1.2 � 0.3 1.6 � 0.3 0.4 � 0.1 1.2 � 0.3 1.8 � 0.4 0.5 � 0.2
Inferior 1.2 � 0.2 1.7 � 0.3 0.5 � 0.2 1.3 � 0.3 2.0 � 0.4 0.5 � 0.2
Lateral 1.1 � 0.2 1.7 � 0.3 0.6 � 0.3 1.2 � 0.2 1.8 � 0.3 0.6 � 0.2
Posterior 1.2 � 0.3 1.6 � 0.3 0.4 � 0.1 1.2 � 0.3 1.8 � 0.4 0.5 � 0.2
Anterior 1.1 � 0.1 1.7 � 0.2 0.6 � 0.2 1.2 � 0.1 1.8 � 0.2 0.5 � 0.1
All 1.1 � 0.2 1.6 � 0.3 0.5 � 0.3 1.2 � 0.2 1.8 � 0.3 0.5 � 0.2
Figure 3. Relationship between peak systolic thickening and
qualitative analysis of normal, ischemic or scar tissue.
Figure 4. Thickening response from rest to peak stress of
normal, ischemic, viable and scarred myocardium.
252

Discussion
Anatomical M-mode o�ers a new means of quan-tifying wall motion abnormalities during stressechocardiography. Although the modality isdependent on image quality, it is feasible in mostsegments. This robust technique is highly repro-ducible and its application does not requireexpertise in stress echocardiography. The results ofthis study indicate that anatomical M-modemeasurement of LV thickening is a useful quanti-tative parameter of regional function that can beapplied during stress echocardiography. Quantita-tive measurements of systolic thickening correlatewell with qualitative assessment of wall motionabnormalities; normal and ischemic segments showgreater thickening than viable and scar segments atrest. With stress, normal segments show improvedthickening, ischemic segments deteriorate, viablesegments improve and scar segments show nochange.While at present, this technique is limited intechnically di�cult studies, and is not equivalent toexpert interpretation, it may be of value in combi-nation with qualitative analysis.
Quantitative assessment of ischemia
When cardiac muscle is subject to ischemia, myo-cardial thickening is reduced almost immediately[11]. Subjective evaluation of regional functionusing wall motion analysis is often based on
assessment of wall motion, rather than thickeningbecause of di�culties in the delineation of theepicardium. Quantitation of systolic thickening,while providing a more objective and speci®c indexfor myocardial ischemia through a more systemicapproach to the measurement of thickening [11],remains limited by same challenges of detecting theappropriate edges.
The need for a less subjective approach toregional function analysis has been widely soughton the basis of improving reproducibility andreducing the need for expert interpretation.These methods have involved two separateapproaches ± various border-tracking techniquesfor the evaluation of radial or short-axis func-tion, and tissue Doppler measures of long axisfunction. Assessment of short-axis function byconventional M-mode echocardiography is lim-ited to cardiac segments that can be intersectedorthogonal to the ultrasonic beam. In contrast,the anatomical M-mode permits interrogation ofmultiple cardiac segments, potentially from theapical views. Reorientation of the axis ofthe anatomical M-mode line at various stages ofthe cardiac cycle reduces the e�ects of cardiactranslation [5], which is present in 2-dimensionalimages and limits quantitation using the center-line method [13], which until recently was themajor alternative for assessment of radial func-tion. The other alternative for quantitation ofregional function is color kinesis (derived fromacoustic quantitation techniques). The compari-son of anatomical M-mode with these othermodalities remains to be de®ned.
Limitations
Even with the development of harmonic imagingand other recent advances in transducer technol-ogy, the quality of transthoracic echocardio-graphic images is variable, depending onattenuation by overlying tissue, including ribs andlung. Suboptimal 2-dimensional images clearlycompromise the quality of anatomical M-modedata and measurements. Failure to include theepicardium of large hearts within the image pre-cludes thickening measurements in some segmentsin which endocardial motion is interpretable.
Figure 5. Systolic thickening in segments according to the
®ndings of 2-dimensional echocardiography and coronary
angiography. Segments are classi®ed as true (TP) and false
positive (FP) and true (TN) and false negative (FP), based on
correlation of wall motion and angiographic features.
253

Moreover, measurement of apical motion isproblematic, both because of fore-shortening andbecause of angulation between the apical segmentsand the ventricular axis used in this study. Evenafter exclusion of apical segments, fully 24% ofimages were of inadequate quality. Both of theseissues are signi®cant limitations on the feasibilityof the technique.
Recent in vitro data has documented that theaccurate measurement of anatomical M-mode datawas compromised with angle correction of >60degrees [5]. This measurement error was of theorder of 2±3 mm in the 75±90 degree range re-quired for anatomical M-mode reconstruction ofapical images, and may have in¯uenced our results.In particular, this likely contributed to the varia-tion of up to 20% around the mean measurements(Figure 2). Nonetheless, the data presented heresuggest that the tool may be of value as an adjunctto visual interpretation even in the apical views.
The variation of normal range values in thisstudy suggest that there may be fundamentallimitations in the application of this tool as ameans of fully quantifying the stress echo study.Anatomical M-mode may therefore be more of anadjuvant to standard visual analysis when imagesare of adequate quality.
A number of confounding factors are inherentto the comparison with angiography presentedhere. First, regional wall motion may remainnormal despite severe coronary stenoses, due tothe development of collateral circulation in thesetting of chronic ischemia. Second, in comparisonwith the extent of segments believed to be jeopar-dized based on coronary angiography ®ndings,stress echocardiography has a tendency to under-estimate the extent of coronary disease [15].Finally, the recognition of multivessel disease us-ing stress echocardiography in the absence of priormyocardial infarction (i.e. the majority of patientsin the study) is only about 50% [10]. This wouldinevitably compromise the sensitivity of both wallmotion and quantitative scoring of each vascularterritory independently.
This study does not address several issues thatmay be important applications of this new tech-nology. In viable myocardial segments, restingwall motion abnormalities improve in response to
low doses of dobutamine, and myocardium sup-plied by a stenosed infarct-related artery subse-quently deteriorates at peak dose [16]. Previousmyocardial infarction was present in about a thirdof patients but the number of viable segments wassmall and only a handful of segments were in pa-tients who proceeded to revascularization. Thus,we were unable to adequately characterize themerits of measuring percent thickening as amarker of viability, but clearly this may be animportant application in the future.
Conclusion
Measurement of systolic thickening using ana-tomical M-mode echocardiography o�ers anobjective method to quantify systolic thickeningat dobutamine echocardiography but has limitedclinical feasibility.
References
1. Geleijnse MR, Fioretti PM, Roelandt JRTC. Methodology,
feasibility, safety and diagnostic accuracy of dobutamine
stress echocardiography. J Am Coll Cardiol 1997; 30:
595±606.
2. Schiller NB, Shah PM, Crawford M, et al. Recom-
mendations for quantitation of the left ventricle by two-
dimensional echocardiography. American society of
echocardiography committee on standards, Subcommittee
on quantitation of two-dimensional echocardiograms. J Am
Soc Echocardiogr 1989; 2: 358±367.
3. Picano E, Lattanzi F, Orlandini A, et al. Stress echocardi-
ography and the human factor. The importance of being
expert. J Am Coll Cardiol 1991; 17: 666±669.
4. Ho�man R, Lethen H, Marwick TH, et al. Analysis of
interinstituitional observer agreement in interpretation of
dobutamine stress echocardiograms. J Am Coll Cardiol
1996; 27: 330±336.
5. Strotmann JM, Escobar Kvitting JP, Wilkensho� UM,
Wranne B, Hatle L, Sutherland GR. Anatomic M-mode
echocardiography: a new approach to assess regional
myocardial function ± a comparative in vivo and in vitro
study of both fundamental and second harmonic imaging
modes. J Am Soc Echocardiogr 1999; 12: 300±307.
6. Donato M, Igino P, Paolo A, Robert AL. Anatomical
M-mode: a new technique for quantitative assessment of
left ventricular size and function. Am J Cardiol 1998; 81:
82G±85G.
7. Pierard LA, Ashman JK, Olstad B, et al. Dimensional
quanti®cation of cardiac anatomy, utilizing anatomical
254

M-mode, a new post processing technique used on high
frame rate two-dimensional digitally stored cineloops. Eur
Heart J 1995; 16: P2885.
8. Diamond GA, Forrester DS. Analysis of probability as an
aid in the clinical diagnosis of coronary artery disease.
N Engl J Med 1979; 300: 1350±1358.
9. McNeil AJ, Fioretti PM, El-Said SM, et al. Enhanced sen-
sitivity for detection of coronary artery disease by addition
of atropine to dobutamine stress echocardiography. Am J
Cardiol 1992; 70: 41±61.
10. Marwick TH. Stress Echocardiography. In: Topol EJ,
editor Textbook of cardiovascular medicine. Philadelphia:
Lippincott±Raven Publishers, 1998: 1267±1300.
11. Kerber RE, Marcus ML, Ehrhardt J, et al. Correlation
between echocardiographically demonstrated segmental
dyskinesis and regional myocardial perfusion. Circulation
1975; 52: 1097±1102.
12. Torry RJ, Myers JH, Adler AL, et al. E�ects of nontrans-
mural ischemia on inner and outer wall thickening in the
canine left ventricle. Am Heart J 1991; 122: 1292±1297.
13. Ginzton LE, Laks MM, Brizendine M, et al. Noninvasive
measurement of the rest and exercise peak systolic pressure/
end systolic volume ratio: a sensitive two-dimensional
echocardiographic indicator of left ventricular function.
J Am Coll Cardiol 1984; 4: 509±516.
14. Lang RM, Vignon P, Weinart L, et al. Echocardiographic
quantitation of regional left ventricular wall motion with
color kinesis. Circulation 1996; 93: 1877±1885.
15. Marwick TH, Willemart B, D'Hondt AM, et al. Selection of
the optimal non exercise stress for the evaluation of ischemic
regional myocardial dysfunction and malperfusion:
Comparison of dobutamine and adenosine using echo-
cardiography and 99m Tc-MIBI single photon emission
tomography. Circulation 1993; 87: 345±354.
16. Pierard LA, De Landsheere CM, Berthe C, et al. Identi®-
cation of viable myocardium by echocardiography during
dobutamine infusion in patients with myocardial infarction
after thrombolytic therapy: Comparison with positron
emission tomography. J Am Coll Cardiol 1990; 15:
1021±1026.
Address for correspondence: Thomas H. Marwick, University
of Queensland, Department of Medicine, Princess Alexandra
Hospital, Ipswich Road, Brisbane, Qld 4102, Australia.
Phone: +61-7-3240-2111; Fax: +61-7-3240-5399;
E-mail: [email protected]
255