Embed Size (px)
Citation preview

USMLE WORLD STEP 1 ANATOMY
A. Testes B. Prostate C. Bladder D. Anal canal E. Sigmoid colon
Explanation:This patient has palpable firm superficial inguinal lymph nodes. The superficial inguinal lymph nodes drain all cutaneous lymph from the umbilicus to the feet, including the external genitalia and anus (up to the beginning of the rectum, the dentate line), but excluding the posterior calf which drains to the popliteal lymph nodes. The superficial inguinal lymph nodes lie in a region bounded by the inguinal ligament, sartorius muscle, and adductor longus muscle, and overlie the femoral nerve, artery and vein. (Choice A) In general, lymph vessels follow the paths of the arteries and veins supplying a particular structure. The testes receive their blood supply from the testicular arteries, which arise directly from the abdominal aorta just inferior to the renal arteries. The lymph vessels that drain the testes follow a path from the testes to the abdominal aortic lymph nodes. (Choice B) Lymph from the prostate drains primarily to the internal iliac nodes, but also to the external iliac nodes and sacral nodes (minor pathways). (Choice C) Lymph from the superior potion of the bladder drains to the external iliac nodes while lymph from the inferior portion of the bladder drains to the internal iliac nodes. (Choice E) Lymph from the sigmoid colon drains to the inferior mesenteric lymph nodes.
Educational Objective: All skin from the umbilicus down, including the anus (up to the dentate/pectinate line) but excluding the posterior calf, drains to the superficial inguinal lymph nodes.
66
Q NO 51: A 52-year-old male presents to your office with a painless mass in his groin. On physical examination, you palpate several hard lymph nodes in the right inguinal area. Lymph node biopsy reveals malignant cells that most likely originated from the:

USMLE WORLD STEP 1 ANATOMY
A. Surface ectoderm B. Neuroectoderm C. Neural crest D. Mesoderm E. Endoderm P. Notochord
Explanation:This patient has pigmented lesions that are most likely a café-au-lait macules, and headaches that could be due to a glioma—both of which are common presentations of Neurofibromatosis Type I. The tumors of interest in the question stem are neurofibromas. Neurofibromas are tumors of Schwann cells, which are derived from the neural crest. On exam, cutaneous neurofibromas are skin-colored or pink nodules with a rubbery texture that exhibit pathognomonic “buttonholing”. The latter refers to the examiner’s perception that these tumors “buttonhole” down through the skin with gentle pressure. (Choice A) The surface ectoderm gives rise to the skin and its appendages, the nasal and oral epithelium, the anal epithelium to the dentate line, and the lens and cornea. (Choice B)The neuroectoderm gives rise to all neurons of the CNSI the neurohypophysis, the retina, the pineal gland, preganglionic autonomic fibers, astrocytes, ependymal cells, and the choroid plexus. (Choice D) The mesoderm is divided into paraxial, intermediate, and lateral sections and gives rise to muscles, bones, blood, genital tissues, the dermis, and most organ systems. Notably, the mesoderm does not give rise to any epithelial surfaces. (Choice E)The endoderm gives rise to thyroid tissues (descendent from the base of the tongue) and the epithelial linings of the Gl tract, lung, urethra, bladder, and outer and middle ear. The endoderm also gives rise to the bulk of the liver, pancreas, and lungs, as these structures form from outpouchings of the primitive gut tube. (Choice F)The notochord almost completely regresses in humans. The only major vestige is the nucleus pulposus in the intervertebral disks. Vertebrae form from the paraxial mesoderm.
Educational Objective: Neurofibromatosis Type l (NF1, or von Recklinghausen’s disease) is a common autosomal-dominant disorder resulting from a defect in the NF-i gene on chromosome 17. Cutaneous and subcutaneous neurofibromas are common in this condition and are tumors of Schwann cells, which are embryologically derived from the neural crest.
67
Q NO 52: A 22-year-old male presents to your office complaining of occasional headaches. On exam, you note several pigmented spots on his trunk. You also discover a few rubbery cutaneous tumors on his neck. The cells composing these skin tumors most likely originated from which of the following structures?

USMLE WORLD STEP 1 ANATOMY
A. Ulnar B. Median C. Radial D. Musculocutaneous E. Axillary
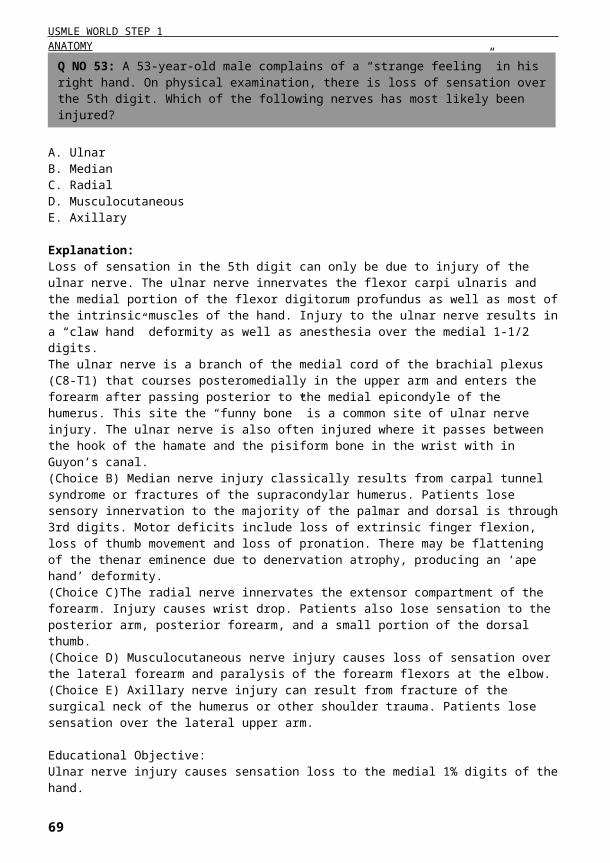
Explanation:Loss of sensation in the 5th digit can only be due to injury of the ulnar nerve. The ulnar nerve innervates the flexor carpi ulnaris and the medial portion of the flexor digitorum profundus as well as most of the intrinsic muscles of the hand. Injury to the ulnar nerve results in a “claw hand” deformity as well as anesthesia over the medial 1-1/2 digits. The ulnar nerve is a branch of the medial cord of the brachial plexus (C8-T1) that courses posteromedially in the upper arm and enters the forearm after passing posterior to the medial epicondyle of the humerus. This site the “funny bone” is a common site of ulnar nerve injury. The ulnar nerve is also often injured where it passes between the hook of the hamate and the pisiform bone in the wrist with in Guyon’s canal. (Choice B) Median nerve injury classically results from carpal tunnel syndrome or fractures of the supracondylar humerus. Patients lose sensory innervation to the majority of the palmar and dorsal is through 3rd digits. Motor deficits include loss of extrinsic finger flexion, loss of thumb movement and loss of pronation. There may be flattening of the thenar eminence due to denervation atrophy, producing an ‘ape hand’ deformity. (Choice C)The radial nerve innervates the extensor compartment of the forearm. Injury causes wrist drop. Patients also lose sensation to the posterior arm, posterior forearm, and a small portion of the dorsal thumb. (Choice D) Musculocutaneous nerve injury causes loss of sensation over the lateral forearm and paralysis of the forearm flexors at the elbow. (Choice E) Axillary nerve injury can result from fracture of the surgical neck of the humerus or other shoulder trauma. Patients lose sensation over the lateral upper arm.
Educational Objective: Ulnar nerve injury causes sensation loss to the medial 1% digits of the hand.
68
Q NO 53: A 53-year-old male complains of a “strange feeling” in his right hand. On physical examination, there is loss of sensation over the 5th digit. Which of the following nerves has most likely been injured?
USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
Explanation:The IVC filter is designed to prevent the travel of deep vein thrombosis from the legs to the lung vasculature. Inferior vena cava filter is used to prevent pulmonary embolism in patients who have contraindications to anticoagulation. This abdominal computed tomography (CT) scan is taken at the level of L2. The bilateral kidneys are viewed in section: the inferior pole of the right lobe of the liver is noted on the left side of the above image anterior to the right kidney and posterolateral to the large bowel. Choice A represents the lumen of the second part of the duodenum, which classically lies at the level of L2. Choice B is medial to the descending part of the duodenum and lies anterior to the right side of the vertebral body. This structure is the inferior vena cava. The right renal vein drains into the IVC near this plane of section. Choice C represents the abdominal aorta. The bifurcation of the abdominal aorta occurs at the level of L4. Choice D, if observed carefully, looks like a figure eight. This structure represents two segments of the ileum lying next to one another. Choice E represents the left renal vein. The left renal vein receives drainage from the left gonadal vein and courses anterior to the aorta, but posterior to the superior mesenteric artery, before draining into the inferior vena cava.
Educational Objective: The inferior vena cava courses through the abdomen and inferior thorax in a location anterior to the right half of the vertebral bodies. The renal veins join the IVC at the level of L1/L2, and the common iliac veins merge to become the IVC at the level of L4.
69
Q NO 54: A 63-year-old male with a history of gastrointestinal bleed has developed a sudden onset shortness of breath. Evaluation shows pulmonary embolism. A filter placement is planned to prevent further embolization. The filter will most likely be placed in which of the following structures?

USMLE WORLD STEP 1 ANATOMY
A. Biceps and coracobrachialis muscles B. Flexor carpi ulnaris and flexor digitorum profundus C. Flexor digitorum superficialis and flexor digitorum profundus D. Olecranon and the medial epicondyle of the humerus E. Supinator muscle and the head of the radius
Explanation:The median nerve receives contributions from the C5 through T1 spinal nerves and emerges as a distinct structure from a combination of fibers from the lateral and medial cords of the brachial plexus. From this location the median nerve courses with the brachial artery in the groove between the biceps brachii and the coracobrachialis / brachialis muscles. It gains access to the forearm in the medial aspect of the antecubital fossa and immediately courses between the humeral and ulnar heads of the pronator teres muscle. It then courses between the flexor digitorum superficialis and the flexor digitorum profundus muscles before entering the wrist and hand within the flexor retinaculum. Injury of the median nerve at the wrist can result from suicide attempts carpal tunnel syndrome, and other traumatic insults to the anterior wrist. Denervation atrophy leads to loss of the thenar eminence and an “ape hand” deformity. Sensation is also lost on the palmar surface of the first three and one-half fingers (including the thumb). (Choice A) The musculocutaneous nerve courses directly between the biceps brachii and the coracobrachialis muscles. Injury to this nerve leads to paralysis of the biceps and the brachialis, which results in an inability to flex the forearm. (Choice B) The ulnar nerve courses between the flexor carpi ulnaris and flexor digitorum profundus in the forearm. Injury to this nerve leads to a “clawhand” deformity due to paralysis of most of the intrinsic muscles of the hand. (Choice D) The ulnar nerve also courses between the olecranon and the medial epicondyle of the humerus. This is the location of the “funny bone” and is a common site of injury to the ulnar nerve due to the superficial location of the nerve in this region. (Choice E)The radial nerve courses through the supinator muscle near the head of the radius. Injury to this nerve causes “wrist drop” due to the fact that the radial nerve innervates the extensors of the hand at the forearm.
Educational Objective: The median nerve courses between the humeral and ulnar heads of the pronator teres muscle and then runs between the flexor digitorum superficialis and the flexor digitorum profundus muscles before entering the wrist and hand within the carpal tunnel.
70
Q NO 55: A 45-year-old Caucasian female presents to your office with numbness of the right palm. Alter taking a detailed history and doing a physical examination you suspect a median nerve lesion at the wrist. Before reaching the wrist the median nerve courses between the:

USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
Explanation:The vomiting that results from administration of systemic chemotherapy is believed to be triggered by the chemoreceptor trigger zone (CTZ) located on the dorsal surface of the medulla at the caudal end of the fourth ventricle (Choice D) in a region known as the area postrema. The area postrema receives blood from fenestrated vessels (absent blood-brain barrier), which allows it to sample chemicals circulating in the blood. (Choice A) This is the thalamus, which helps to coordinate the sensory and motor systems. (Choice B) This dorsal midbrain site is the location of the superior and inferior colliculi. The third ventricle is located dorsal to these structures. (Choice C) This is the ventral pons. Fibers of cranial nerves V-VIII, the corticospinal tract, the medial lemniscus, and the lateral spinothalamic tract course through this region. (Choice E) This is the site of the inferior cerebellar peduncle of the inferior medulla. Damage to this peduncle results in ipsilateral motor incoordination.
Educational Objective: Acute nausea following administration of systemic chemotherapy results from stimulation of the chemoreceptor trigger zone (CTZ), which lies in the area postrema of the dorsal medulla near the fourth ventricle.
71
Q NO 56: A 34-year-old male begins treatment with combination chemotherapy for Hodgkin’s lymphoma. Shortly there after, he experiences severe vomiting and requires intravenous fluid supplementation. Which of the following brain sites is responsible for his symptoms?

USMLE WORLD STEP 1 ANATOMY
Occlusion of the artery labeled ‘X’ would most likely result in an inability to:
A. Climb stairs B. Grip C. Whistle D. Swallow food
Explanation:This cerebral angiogram image is projected axially with the top of the image representing anterior regions and the bottom representing posterior regions. The yew large vessels seen bilaterally are the internal carotid arteries. Each gives off a middle cerebral artery to supply more lateral regions and an anterior cerebral artery, which extends medially. The above “X” marks an anterior cerebral artery. Each anterior cerebral artery supplies the medial region of the ipsilateral hemisphere from the frontal pole to the parietooccipital sulcus. Occlusion of the anterior cerebral artery would affect motor function of the contralateral leg and foot. (Choices B, C and D) Motor control of the hand head and neck would be affected by occlusion of the middle cerebral arteri.
Educational Objective: The anterior cerebral arteries supply the medial portions of the two hemispheres. Occlusion causes weakness of the contralateral legs and sensory deficits of the contralateral legs, trunk and genitals. There may also be behavior and mood changes due to injury of frontal lobe structures.
72
Q NO 57: Shown below are the cerebral arteriography findings from a 45-year-old patient.

USMLE WORLD STEP 1 ANATOMY
A. Inter ventricular foramina of Monro B. Cerebral aqueduct C. Medial foramen of Magendie D. Lateral foramina of Luschka E. Arachnoid villi
Explanation:This patient had findings consistent with noncommunicating hydrocephalus resulting from obstruction of cerebrospinal fluid (CSF) flow at the cerebral aqueduct. CSF is formed by the choroid plexus in each of the four ventricles. The choroid plexus is composed of ependymal cell- covered outgrowths of the pia mater blood vessels. The ependymal epithelium is a simple ciliated columnar layer. Choroid plexus capillaries are fenestrated unlike the other CNS capillaries. The ependymal cells form tight junctions with one another and selectively allow certain materials from the blood to enter the CSE. Once formed CSF flows from the lateral ventricles to the third ventricle via the interventricular foramina of Monro. It then circulates to the fourth ventricle through the cerebral aqueduct (of Sylvius). CSE then exits the fourth ventricle and enters the subarachnoid space via one of three foramina, the lateral foramina of Luschka or the medial foramen of Magendie. CSE is returned to the venous circulation via the arachnoid villi (granulations). Other forms of hydrocephalus are briefly as follows: 1. Communicating hydrocephalus: No blockage to CSF flow within the brain or brainstem. The blockage is in the subarachnoid space where flow may be restricted by fibrosis following inflammation. 2. Normal pressure hydrocephalus: CSF is not absorbed by the arachnoid villi. 3. Hydrocephalus ex vacuo: Increased CSF volume occurring in conditions of brain atrophy. 4. Pseudotumor cerebri: A condition that classically occurs in over weight young females and is related to decreased CSF outflow at the arachnoid villi.
Educational Objective: CSE flows from the third ventricle to the fourth ventricle via the cerebral aqueduct of Sylvius.
73
Q NO 58: A patient presents to the emergency room complaining of worsening headaches, confusion, and intermittent vomiting. She is admitted, but later dies in the hospital. Examination of the brain at autopsy shows enlargement of the lateral and third ventricles and a normal-sized fourth ventricle. Where is the most likely site of obstruction in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Globus pallidus B. Putamen C. Internal capsule D. Caudate nucleus E. Amygdala
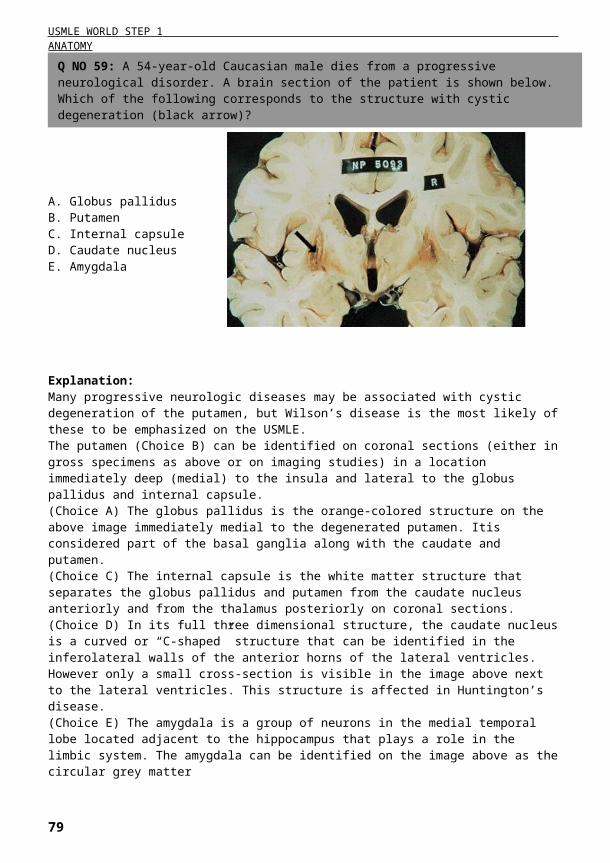
Explanation:Many progressive neurologic diseases may be associated with cystic degeneration of the putamen, but Wilson’s disease is the most likely of these to be emphasized on the USMLE. The putamen (Choice B) can be identified on coronal sections (either in gross specimens as above or on imaging studies) in a location immediately deep (medial) to the insula and lateral to the globus pallidus and internal capsule. (Choice A) The globus pallidus is the orange-colored structure on the above image immediately medial to the degenerated putamen. Itis considered part of the basal ganglia along with the caudate and putamen. (Choice C) The internal capsule is the white matter structure that separates the globus pallidus and putamen from the caudate nucleus anteriorly and from the thalamus posteriorly on coronal sections. (Choice D) In its full three dimensional structure, the caudate nucleus is a curved or “C-shaped” structure that can be identified in the inferolateral walls of the anterior horns of the lateral ventricles. However only a small cross-section is visible in the image above next to the lateral ventricles. This structure is affected in Huntington’s disease. (Choice E) The amygdala is a group of neurons in the medial temporal lobe located adjacent to the hippocampus that plays a role in the limbic system. The amygdala can be identified on the image above as the circular grey matter structures in the medial temporal lobe immediately inferior to the globus pallidus and putamen. The amygdala mediates fear and some sympathetic stimulation in humans.
Educational Objective: Wilson’s disease can cause cystic degeneration of the putamen as well as damage to other basal ganglia structures. The putamen is located medial to the insula and lateral to the globus pallidus on coronal sections.
74
Q NO 59: A 54-year-old Caucasian male dies from a progressive neurological disorder. A brain section of the patient is shown below. Which of the following corresponds to the structure with cystic degeneration (black arrow)?

USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
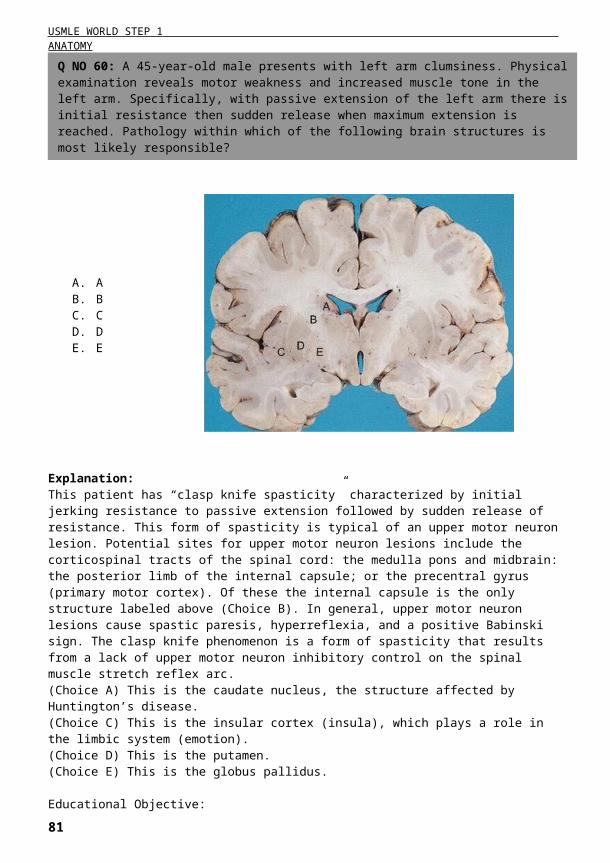
Explanation:This patient has “clasp knife spasticity” characterized by initial jerking resistance to passive extension followed by sudden release of resistance. This form of spasticity is typical of an upper motor neuron lesion. Potential sites for upper motor neuron lesions include the corticospinal tracts of the spinal cord: the medulla pons and midbrain: the posterior limb of the internal capsule; or the precentral gyrus (primary motor cortex). Of these the internal capsule is the only structure labeled above (Choice B). In general, upper motor neuron lesions cause spastic paresis, hyperreflexia, and a positive Babinski sign. The clasp knife phenomenon is a form of spasticity that results from a lack of upper motor neuron inhibitory control on the spinal muscle stretch reflex arc. (Choice A) This is the caudate nucleus, the structure affected by Huntington’s disease. (Choice C) This is the insular cortex (insula), which plays a role in the limbic system (emotion). (Choice D) This is the putamen. (Choice E) This is the globus pallidus.
Educational Objective: Upper motor neuron lesions cause spastic rigidity, hyperreflexia, and paresis. Corticospinal tract, internal capsule (Posterior limb), and primary motor cortex lesions can cause these symptoms.
75
Q NO 60: A 45-year-old male presents with left arm clumsiness. Physical examination reveals motor weakness and increased muscle tone in the left arm. Specifically, with passive extension of the left arm there is initial resistance then sudden release when maximum extension is reached. Pathology within which of the following brain structures is most likely responsible?

USMLE WORLD STEP 1 ANATOMY
A. Left anterior descending B. Left circumflex C. Left main D. Right E. Acute marginal
Explanation:The right and left main coronary arteries arise directly from the root of the aorta and provide the blood supply to the heart. The left main coronary artery divides into the left anterior descending (LAD) and circumflex coronary arteries, which supply most of the anterior and left lateral surfaces of the heart. In 85-90% of individuals, the right coronary artery gives rise to the posterior descending artery. These patients are said to have right dominant coronary circulation. In approximately 10% of patients the posterior descending artery arises from the circumflex branch of the left main coronary artery these patients have left dominant circulation. The posterior descending artery supplies most of the inferior wall of the left ventricle, which forms the diaphragmatic surface of the heart. The right coronary artery also gives rise to the SA and AV nodal arteries in most patients. (Choice A) The LAD coronary artery normally supplies the anterior 2/3 of the interventricular septum (septal branches), the anterior wall of the left ventricle (diagonal branches) and part of the anterior papillary muscle. (Choice B)The left circumflex coronary artery supplies the lateral and posterior superior walls of the left ventricle via obtuse marginal branches. (Choice C) The left main coronary artery gives rise to the LAD and left circumflex coronary arteries. It only gives rise to the posterior descending artery in about 10% of individuals and thus is not the artery most likely occluded here. (Choice E)The acute marginal branches arise from the right coronary artery to supply the wall of the right ventricle. They may provide collateral circulation in patients with LAD occlusion.
Educational Objective: The inferior wall of the left ventricle forms most of the diaphragmatic surface of the heart. The posterior descending artery supplies this area. In 85-90% of individuals the posterior descending artery derives from the right coronary artery.
76
Q NO 61: A 54-year-old male presents to your office complaining of periodic, tight, burning substernal chest pain. A thallium stress test shows hypoperfusion of the cardiac muscle forming the diaphragmatic surface of the heart. Which of the following coronary arteries is most likely occluded in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Left lung B. Left atrium C. Right ventricle D. Inferior vena cava E. Azygous vein
Explanation:Most of the volume of the thoracic cavity is occupied by the lungs. The apex of each lung extends into the neck approximately three to four centimeters above the first rib. The lung bases are in direct contact with diaphragm which separates the right lung from the right lobe of the liver and the left lung from the left lobe of the liver the stomach, and the spleen. The mediastinal surface of each lung has a cardiac impression that accommodates the heart. The heart is located behind the sternum and is partially covered by the lungs. The apex is formed by the left ventricle and is covered by the left lung. It lies behind the fifth left intercostal space on the level of left midclavicular line. The sternocostal (anterior) surface or the heart is formed chiefly by the right ventricle. The diaphragmatic (inferior) surface is formed by left and right ventricles, and is in contact with the central tendon of the diaphragm. The posterior surface of the heart is formed mainly by the left atrium. Penetrating injury in the fifth intercostal space at the left midclavicular line would most likely injure the left lung (Choice A). Penetration of the left lung in this location could lead to injury of the apex of the heart as well if the wound was deep enough. All other heart chambers lie medial to the left midclavicular line and would not be affected. (Choice B)The left atrium is located posterior to the left ventricle and forms the base of the heart. (Choice C) Right ventricle forms the anterior (sternal) surface of the heart and its inferior border. It lies medially to the left midclavicular line. (Choice D) The inferior vena cava is located in the mediastinum, lies to the right of midline and drains into the right atrium. (Choice E) The azygous vein lies in the posterior mediastinum immediately to the left of midline. It drains blood from the posterior intercostal veins into the superior vena cava.
Educational Objective: The left ventricle forms the apex of the heart and reaches as far as the fifth intercostal space in the left midclavicular line. The other chambers of the heart lie to the right of the left midclavicular line and would not be affected by penetrating injury in this location.
77
Q NO 62: A 23-year-old male who has been previously healthy is brought to the FR after a street fight. He has a stab wound at the fifth intercostal space along the left midclavicular line. Which of the following is most likely punctured in this patient?

USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
Explanation:The patient described in the question stem is likely suffering from alcoholic cirrhosis. Alcoholic cirrhosis is a form of micronodular cirrhosis associated with hepatocyte death followed by fine fibrosis of the liver. As cirrhosis worsens and the number of functioning hepatocytes decreases the functional ability of the liver diminishes. In advanced disease portal blood has an increasingly difficult time passing through the liver because the vasculature becomes compromised by the progressive fibrosis, causing “portal hypertension.” The effects of prolonged portal hypertension include varices at the four sites of portocaval anastomoses (esophagus, rectum umbilicus and retroperitoneal), as well as ascites. Of the structures identified on the image above only the portal vein (Choice C) is a part of the portal system. In this patient high pressure would be expected within the portal vein. (Choice A) The descending abdominal aorta will have elevated pressures in patients with systemic hypertension. (Choice B)The inferior vena cava experiences increased pressure in cases of heart failure. (Choice D)The celiac trunk emerges from the aorta at this level (T12/L1). (Choice E) The splenic artery pressure would increase under conditions of elevated systemic blood pressure. The splenic vein however would experience increased pressure with portal hypertension due to the fact that it drains directly into the portal vein (after receiving blood from the inferior mesenteric vein).
Educational Objective: The portal vein can be identified on cross-sectional scans lying in or near the right side of the liver and anterior to the inferior vena cava. The pressure in the portal system is elevated in liver cirrhosis.
78
Q NO 63: A patient with a long history of excessive alcohol consumption presents to your office with abdominal distention. The distension clears with a low-salt diet and spironolactone therapy. Which of the following structures labeled on the image below is expected to have an increased pressure in this patient?
USMLE WORLD STEP 1 ANATOMY
A. Trigeminal nerve B. Chorda tympani C. Glossopharyngeal nerve D. Hypoglossal nerve E. Vagus nerve
Explanation:The innervation of the tongue is complex because it involves motor, general somatic sensory and special sensory functions. Somatic sensation includes pain touch temperature and pressure; the same sensations felt by the skin. The lingual nerve, a branch of the mandibular division of the trigeminal nerve (CN V3) provides somatic sensory innervation to the anterior 2/3 of the tongue. CN V3 also provides somatic sensory innervation to the skin of the face. The glossopharyngeal (CN IX) nerve provides somatic sensory innervation to the posterior 1/3 of the tongue. (Choice B)The chorda tympani is a branch of the facial nerve that passes along the deep surface of the tympanic membrane and through the petrotympanic fissure before merging with the lingual nerve to deliver taste sensation to the anterior 2/3 of the tongue. (Choice C) The glossopharyngeal nerve (CN IX) delivers somatic sensory and taste innervation to the posterior 1/3 of the tongue. (Choice D)The hypoglossal nerve (CNXII) innervates all intrinsic muscles of the tongue except the palatoglossus muscle which is innervated by the vagus nerve (CN X). (Choice E) The vagus nerve (CN IX) innervates the palatoglossus muscle and carries taste signals from the pharynx and epiglottis. It does not carry taste signals from the tongue however.
Educational Objective: A branch of the mandibular division of the trigeminal nerve (CN V3) provides somatic sensory innervation to the anterior 2/3 of the tongue. The chorda tympani branch of the facial nerve provides taste sensation from the anterior 2/3 of the tongue. The glossopharyngeal nerve (CN IX) provides somatic sensory and taste innervation to the posterior portion of the tongue.
79
Q NO 64: A patient drinking hot tea at a restaurant experiences a burning sensation at the tip of his tongue. This sensation is transmitted by which of the following?

USMLE WORLD STEP 1 ANATOMY
A. Superior gluteal B. Inferior gluteal C. Obturator D. Femoral E. Sciatic
Explanation:This patient demonstrates a positive Trendelenburg sign. The Trendelenburg test involves observing a patient standing facing away from the examiner while lifting each foot off of the ground. The sign is positive when the hip dips downward when the ipsilateral leg is lifted off of the ground. This can occur due to weakness of the gluteus medius and gluteus minimus muscles because these muscles function to pull the pelvis down and abduct the thigh. These muscles are supplied by the superior gluteal nerve. Patients with injury of the superior gluteal nerve may exhibit a waddling gait ora characteristic limp known as the “gluteus medius limp.” The Trendelenburg sign and gluteus medius limp can also be seen in patients with injuries to the gluteus medius and gluteus minimus muscles themselves as well as in patients with injuries to the hip joint. (Choice B) The inferior gluteal nerve innervates the gluteus maximus muscle. This muscle is responsible for extension of the thigh at the hip and external rotation of the thigh. Injury of the inferior gluteal nerve causes difficulty rising from the seated position and climbing stairs. (Choice C) injury of the obturator nerve causes deficits of thigh adduction as well as medial thigh sensory loss. (Choice D)The femoral nerve innervates the muscles responsible for flexion of the thigh at the hip (iliacus and sartorius muscles) and extension of the leg at the knee (quadriceps femoris). It also supplies sensory innervation to the skin on the anterior thigh and medial leg. Injury results in loss of the knee reflex and anterior thigh sensory loss. (Choice E)The sciatic nerve innervates all of the knee flexors (hamstrings) except the short head of the biceps femoris. It subsequently divides into the tibial and common peroneal nerves, which each go on to provide motor and sensory innervation to the leg and foot.
Educational Objective: 1) Injury to the superior gluteal nerve causes weakness of the gluteus medius and gluteus minimus muscles, producing a positive Trendelenburg test. 2) The inferior gluteal nerve innervates the gluteus maximus muscle. Injury of the inferior gluteal nerve causes difficulty rising from the seated position and climbing stairs.
80
Q NO 65: A 43-year-old male presents to your office with difficulty walking. On gait examination you note that he leans to the right side while walking. When he is asked to stand on his left foot, his right hip tilts significantly downward. Which of the following nerves is most likely injured in this patient?
USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
Explanation:Inability to void despite sensation of a full bladder in the scenario presented in this vignette suggests urethral trauma. Urethral injuries are divided into trauma to the anterior or the posterior urethra. The posterior urethra is located above the urogenital diaphragm while the anterior urethra lies below it. Injury to the anterior urethra is the most common form of urinary tract trauma. This form of urinary tract injury most frequently occurs due to a saddle injury where the perineum is struck forcefully such as by falling on the crossbar of the bicycle or on the top of the fence. The symptoms of this form of trauma are difficulty with or inability to void in spite of a full bladder, and the presence of blood at the urethral meatus. Injury of the anterior urethra causes blood and urine to extravasate into the superficial perineal space of the penis, scrotum and anterior abdominal wall. This hematoma is called “butterfly-like”, as it does not extend to the thighs and anal triangle due to the firm attachment of the superficial perineal fascia with the fascia lata. Posterior urethral trauma most commonly occurs in association with pelvic fracture (choice C). Such injury commonly causes a hematoma below the prostate and upward displacement of that gland. It also causes rupture of the posterior urethra that is firmly connected to both the prostate and the pubic arch. Posterior urethral injury presents with inability to void despite a full bladder and an elevated (high riding) prostate on rectal examination. A typical presentation of posterior urethral trauma is described in this clinical vignette. If urethral trauma is suspected, placement of Foley catheter should be avoided and retrograde urethrogram should be preformed to demonstrate urethral injury. (Choice A) Anterior bladder wall rupture is associated with blunt abdominal trauma causing compression of a full bladder. It is associated with intraperitoneal extravasation of urine, abdominal pain and guarding, and inability to void. (Choice B) Superior bladder wall rupture also occurs in association with pelvic fracture. It manifests with difficulty with or inability to void, gross hematuria and suprapubic pain. Urine extravasates extra peritoneally with in the retropubic space of Retzius. (Choice D) Trauma to the urethra below the urogenital diaphragm results from saddle injuries. It presents with blood at the urethral meatus, a “butterfly” hematoma of the perineum, and an inability to void despite a full bladder.
81
Q NO 66: A 45-year-old male is brought to the ER after a motor vehicle accident. He is diagnosed with a left hemothorax and a pelvic fracture. The patient is unable to void and complains of a sensation of full bladder. Foley catheter placement does not produce any urine. The patient is likely to have an injury of which of the following labeled structures:

USMLE WORLD STEP 1 ANATOMY
(Choice E) injury to the penile urethra results from trauma to the erect penis. Symptoms include swelling and hematoma of the penis and perineum, inability to void and blood at the external urethral meatus.
Educational Objective: Injury to the posterior urethra is associated with pelvic fracture. It presents with inability to void despite a full bladder, and a high riding prostate on rectal examination.
82

USMLE WORLD STEP 1 ANATOMY
A. Common hepatic B. Right gastroepiploic C. Left gastric D. Gastroduodenal E. Inferior pancreaticoduodenal F. Splenic G. Superior mesenteric
Explanation:Duodenal ulcers are more common than gastric ulcers. Duodenal ulcers tend to occur anteriorly. Notably, ulcers located on the anterior wall of the duodenal bulb are more prone to perforation, while those on the posterior wall are more likely to cause hemorrhage. These complications are explained by the relationship of the duodenal bulb to adjacent organs. The bulb begins at the pylorus, ends at the neck of the gallbladder, and rests anterior to the gallbladder and liver. The gastroduodenal artery, common biliary duct, and vena porta lie behind the duodenal bulb; the head of the pancreas is located below. When an ulcer of the posterior wall of the duodenal bulb penetrates the posterior wall, the ulcer is likely to corrode the gastroduodenal artery. The gastroduodenal artery arises from the proper hepatic artery and perfuses both the pylorus and the proximal part of the duodenum. Damage to the gastroduodenal artery can cause significant upper gastrointestinal bleeding. (Choice A) The common hepatic artery arises from the celiac trunk bifurcates into the proper hepatic and gastroduodenal artery. It passes superiorly to the duodenal bulb and is not eroded by duodenal ulcers. (Choices B and C) The right gastroepiploic and left gastric arteries supply blood to the stomach. They don’t lie in close proximity to the duodenal bulb. (Choice E)The inferior pancreaticoduodenal artery is a branch of the superior mesenteric artery. It supplies blood to the lower duodenum and to the head of the pancreas. This artery does not have any close relation to the duodenal bulb. (Choice G) The superior mesenteric artery lies anterior to the transverse part of the duodenum. It arises from the anterior surface of the abdominal aorta and supplies the intestine from the duodenum to the left colic flexure. It also supplies the pancreas.
Educational Objective: The gastroduodenal artery lies along the posterior wall of the duodenal bulb and is likely to be eroded by posterior duodenal ulcers. Ulceration into the gastroduodenal artery can be a source of life-threatening hemorrhage.
83
Q NO 67: A 52-year-old Caucasian male is brought to the ER after repeated coffee-ground vomiting. After initial stabilization, endoscopy is performed revealing a deep, bleeding ulcer on the posterior wall of the duodenal bulb. This ulcer has most likely penetrated which of the following arteries?

USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
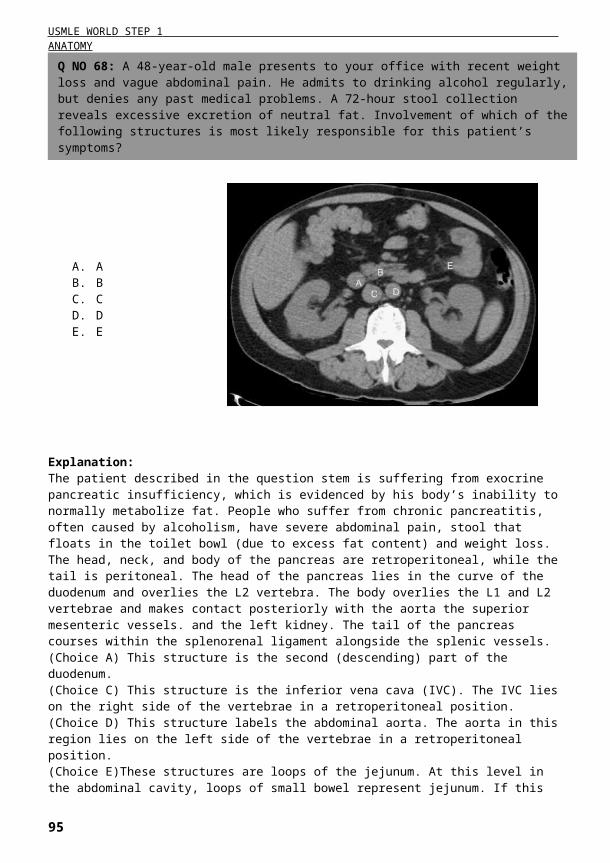
Explanation:The patient described in the question stem is suffering from exocrine pancreatic insufficiency, which is evidenced by his body’s inability to normally metabolize fat. People who suffer from chronic pancreatitis, often caused by alcoholism, have severe abdominal pain, stool that floats in the toilet bowl (due to excess fat content) and weight loss. The head, neck, and body of the pancreas are retroperitoneal, while the tail is peritoneal. The head of the pancreas lies in the curve of the duodenum and overlies the L2 vertebra. The body overlies the L1 and L2 vertebrae and makes contact posteriorly with the aorta the superior mesenteric vessels. and the left kidney. The tail of the pancreas courses within the splenorenal ligament alongside the splenic vessels. (Choice A) This structure is the second (descending) part of the duodenum. (Choice C) This structure is the inferior vena cava (IVC). The IVC lies on the right side of the vertebrae in a retroperitoneal position. (Choice D) This structure labels the abdominal aorta. The aorta in this region lies on the left side of the vertebrae in a retroperitoneal position. (Choice E)These structures are loops of the jejunum. At this level in the abdominal cavity, loops of small bowel represent jejunum. If this CT slice were of the inferior (lower) abdomen the small bowel would more likely be the ileum.
Educational Objective: On abdominal CT scans the pancreas can be identified by its head in close association with the second part of the duodenum: by its body overlying the left kidney aorta, IVC and superior mesenteric vessels: and also by the tail lying in the splenorenal ligament.
84
Q NO 68: A 48-year-old male presents to your office with recent weight loss and vague abdominal pain. He admits to drinking alcohol regularly, but denies any past medical problems. A 72-hour stool collection reveals excessive excretion of neutral fat. Involvement of which of the following structures is most likely responsible for this patient’s symptoms?

USMLE WORLD STEP 1 ANATOMY
A. Carpal tunnel B. Hook of the hamate C. Surgical neck of the humerus D. Head of the radius E. Coracobrachialis
85
Q NO 69: A patient presents to the emergency room with weak wrist extension. On physical examination, sensation to the arm is intact. The affected nerve was most likely injured at which of the following locations?

USMLE WORLD STEP 1 ANATOMY
Explanation:The radial nerve arises from the posterior cord of the brachial plexus. It innervates the muscles of the posterior (extensor) compartment of the arm. After innervating the extensor compartment of the upper arm, the radial nerve enters the forearm. At the lateral epicondyle of the humerus (where the humerus articulates with the radius), the radial nerve divides into superficial and deep branches. The superficial branch of the radial nerve is purely sensory it provides somatic sensory innervation to the radial half of the dorsal hand. (It does not, however, provide sensory innervation to the dorsal portions of the distal first through third digits. Sensory innervation of the palmar and dorsal surfaces of the distal 3 1/2 digits is provided by the lateral and medial branches of the median nerve.) Radial head subluxation (“nursemaid’s elbow”) is a common injury in children that can result from sudden outward pulling on an extended and pronated arm (e.g. when an adult attempts to pull a child upward by the arm). Radial head subluxation can damage the deep branch of the radial nerve, leading to weakness or paralysis of forearm extensor compartment muscles. “Wrist drop” commonly results from radial nerve injury. The deep branch of the radial nerve does not carry any somatic sensory innervation. (Choice A) Carpal tunnel syndrome can result from any factor (e.g. inflammation) that reduces the size of the carpal tunnel, compressing the median nerve. In addition to pain, patients classically experience difficulty with fine motor control of the thumb. (Choice B) In the wrist, the ulnar nerve passes between the hook of the hamate and the pisiform bone in a fibroosseous tunnel known as Guyon’s canal. Ulnar nerve injury at this site causes dysesthesias of the ulnar side of the hand and weakness of the intrinsic muscles of the hand. (Choice C) Fracture of the surgical neck of the humerus may cause axillary nerve injury leading to paralysis of the deltoid and teres minor muscles as well as loss of sensation on the lateral upper arm. (Choice E) The coracobrachialis muscle is an arm flexor that lies deep to the biceps brachii and overlies the median nerve and brachial artery. Itis innervated by the musculocutaneous nerve.
Educational Objective: The deep branch of the radial nerve arises near the lateral epicondyle of the humerus where the humerus articulates with the head of the radius. Radial head subluxation can damage the deep branch of the radial nerve, causing weakness of the forearm and hand extensors but no sensory deficits.
86

USMLE WORLD STEP 1 ANATOMY
A. Inferior epigastric vessels B. Cooper’s ligament C. Femoral vein D. Transversalis fascia E. Rectus muscle sheath P. Spermatic cord
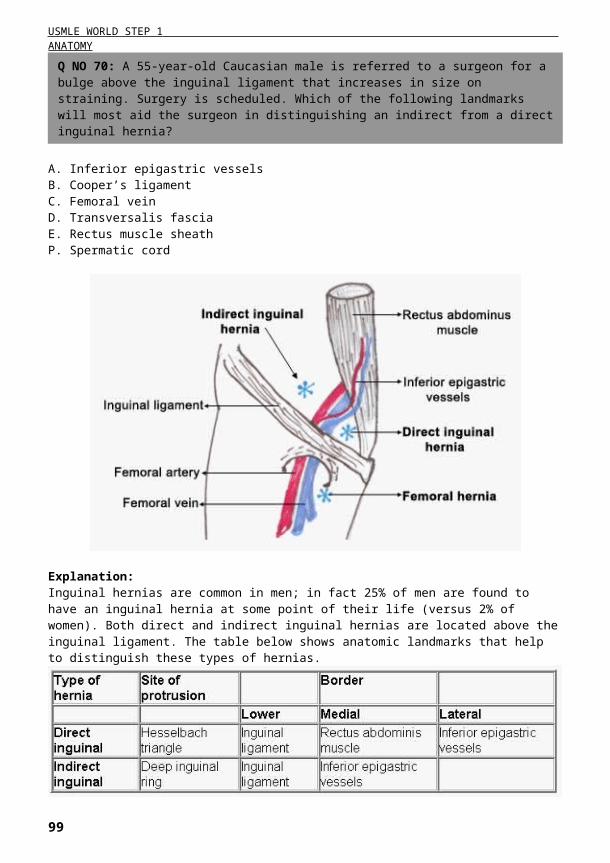
Explanation:Inguinal hernias are common in men; in fact 25% of men are found to have an inguinal hernia at some point of their life (versus 2% of women). Both direct and indirect inguinal hernias are located above the inguinal ligament. The table below shows anatomic landmarks that help to distinguish these types of hernias.
Indirect inguinal hernias are more common than direct. They occur in 213 cases of inguinal hernias, and tend to appear on the right side. Indirect inguinal hernias occur due to failure of the process us vaginal is to obliterate, allowing abdominal contents to protrude through the deep inguinal ring. Abdominal contents follow the path of the inguinal canal and may exit through the superficial inguinal ring into the scrotum. On
87
Q NO 70: A 55-year-old Caucasian male is referred to a surgeon for a bulge above the inguinal ligament that increases in size on straining. Surgery is scheduled. Which of the following landmarks will most aid the surgeon in distinguishing an indirect from a direct inguinal hernia?

USMLE WORLD STEP 1 ANATOMY
examination, these hernias can be detected by deep palpation at the tip of the finger. Direct inguinal hernias protrude through the Hesselbach triangle, which is a weak spot of the anterior abdominal wall. Hesselbach’s triangle is bounded by the rectus abdominis muscle medially, inferior epigastric vessels laterally, and inguinal ligament inferiorly. Direct inguinal hernias do not descend in to the scrotum. Direct inguinal hernias are felt with the pulp of the examiner’s finger on deep palpation. (Choice B) Cooper’s (pectineal) ligament will be posterior to a femoral hernia. (Choice C) The femoral vein will be laterally to a femoral hernia. (Choice D) The transversalis fascia lies posteriorly to indirect inguinal hernias. (Choice E) The rectus abdominis muscle sheath is medial to direct inguinal hernias. (Choice F) The spermatic cord passes through the inguinal canal and may be included in the indirect inguinal hernia sac.
Educational Objective: Indirect inguinal hernias are located laterally to the interior epigastric vessels. They can continue into the scrotum and are felt by deep palpation with the tip of the finger in the inguinal canal. On the contrary direct inguinal hernias are located medially to the interior epigastric vessels. They never protrude into the scrotum and are felt with the pulp of an examiner’s finger.
88

USMLE WORLD STEP 1 ANATOMY
A. External spermatic fascia B. Cremasteric fascia C. Internal spermatic fascia D. Tunica albuginea E. Tunica vaginalis
Explanation:This patient’s clinical presentation is consistent with hydrocele. Hydrocele occurs when serous fluid collects within the tunica vaginalis. During embryogenesis, the testis descends through the inguinal canal, drawing a diverticulum of peritoneum into the scrotum as it descends. This peritoneal tissue is known as the processus vaginalis. Normally, the communication between the processus vaginalis and the peritoneum is obliterated, and the tunica vaginalis is the tissue that remains overlying the testis and epididymis. Congenital hydrocele, as described in the question stem, results when the processus vaginalis remains patent, allowing fluid from the peritoneum to accumulate in the scrotum. (Choice A) The external spermatic fascia is derived from the aponeurosis of the external oblique abdominal muscle. This is the outermost layer of the spermatic cord and lies deep to the dartos muscle and scrotal fascia. (Choice B) The cremasteric fascia arises from the internal oblique abdominal muscle and aponeurosis. (Choice C) The internal spermatic fascia is derived from the transversalis fascia. This layer immediately overlies the spermatic cord and tunica vaginalis. (Choice D) The tunica albuginea is the fibrous tissue that overlies the corpus spongiosum and corpora cavernosa of the penis.
Educational Objective: Testicular hydrocele results when serous fluid accumulates within the tunica vaginalis. The tunica vaginalis is embryologically derived from the peritoneum; when it remains in communication with the peritoneum, a communicating hydrocele results.
89
Q NO 71: An 8-year-old male is brought to your office because of an enlarged right testicle. Transillumination reveals a fluid accumulation within the scrotum. This fluid accumulation is most likely confined to the:

USMLE WORLD STEP 1 ANATOMY
A. Abdominal aorta B. Transverse colon C. Liver D. Spleen E. Pancreas
Explanation:The retroperitoneum is the space located behind the peritoneal cavity. It includes the following structures: 1. Major vessels: abdominal aorta inferior vena cava and their branches. 2. Solid organs: pancreas (except the tail), kidneys, adrenal glands. 3. Hollow organs: parts 2 & 3 and a portion of part 4 of the duodenum the ascending and descending colon (secondarily retroperitoneal), rectum ureters and bladder. 4. Vertebral column and pelvic muscles. Retroperitoneal hematomas are commonly associated with abdominal and pelvic trauma: they develop in up to half of patients with blunt abdominal trauma. Pancreatic injury with formation of a retroperitoneal hematoma can occur due to severe blunt or penetrating abdominal trauma. It can frequently be caused by direct abdominal blows from malpositioned seat belts or by steering wheels during automobile collisions. Pancreatic injury can cause mild symptoms or be asymptomatic. An abdominal CT scan should be performed in stable patients with blunt abdominal trauma to exclude the possibility of retroperitoneal hematoma. (Choice A) Though the abdominal aorta is a retroperitoneal structure rupture of the abdominal aorta would most likely result in massive and rapid blood loss leading to hemorrhagic shock. (Choices B, C and D) The transverse colon, liver and spleen are intraperitoneal organs. Lacerations or rupture of these organs can occur in blunt abdominal trauma but these injuries would lead to hemoperitoneum (free blood in the peritoneal space) not retroperitoneal hematoma.
Educational Objective: Retroperitoneal hematoma in a stable patient is likely to occur due to pancreatic injury. Lt may present with mild symptoms be asymptomatic or be masked by symptoms from other injuries related to trauma. Abdominal CT is the diagnostic modality of choice. Frequently nonexpanding hematomas in this location will be treated conservatively (i.e. non-operatively).
90
Q NO 72: A 39-year-old female is brought to the emergency room after a motor vehicle collision. Upon arrival she is determined to be stable, but complains of mild abdominal pain. CT scan of the abdomen reveals a retroperitoneal hematoma. Trauma of which of the following anatomic structures is most likely responsible for this finding?

USMLE WORLD STEP 1 ANATOMY
A. Occipital B. MaxillaryC. Ophthalmic D. Middle cerebral E. Sphenopalatine F. Facial
Explanation:The patient described in the question stem has suffered a fracture where the frontal parietal, temporal, and sphenoid bones meet in the skull. This site is known as the pterion and is medically relevant due to the fact that the bone is thin in this region and the middle meningeal artery courses within the skull deep to this point. As such, fractures to this region of the skull are at risk of damaging the middle meningeal artery and causing an epidural hematoma. Epidural hematomas require prompt treatment because they are under systemic arterial pressure and can expand rapidly leading to transtentorial herniation and palsy of the oculomotor nerve. The middle meningeal artery is a branch of the maxillary artery, which itself is a branch of the external carotid artery. (Choice A) The occipital artery arises opposite the facial artery from the external carotid, coursing posteriorly instead of anteriorly. This vessel serves the posterior scalp and the stemocleidomastoids. (Choice C)The ophthalmic artery is the first branch of the internal carotid artery, serving the eye and orbital contents as well as the eyelids, forehead, nose, and nasal mucosa. The internal carotid artery has no branches in the neck. (Choice D)The middle cerebral artery is a branch of the internal carotid artery and supplies much of the parietal and temporal regions of the brain. Injury to this artery or its branches can cause a subarachnoid or intracerebral hemorrhage. (Choice E)The sphenopalatine artery is a branch of the third part of the maxillary artery that supplies much of the nasal mucosa. It anastomoses with branches of the ophthalmic and facial arteries within the anterior part of the nasal septum in a region known as Kiesselbach’s plexus — a frequent site of nosebleeds. (Choice F) The facial artery is a branch of the external carotid artery that courses over the mandible anterior to the insertion of the masseter muscle to supply the oral region and nose as well as the buccal region of the cheeks.
Educational Objective: The middle meningeal artery is a branch of the maxillary artery that enters the skull at the foramen spinosum and courses intracranially deep to the pterion. Skull fractures at this site may cause laceration of this vessel leading to an epidural hematoma.
91
Q NO 73: A 23-year-old Caucasian female is brought to the ER unconscious altera motor vehicle accident. A linear skull fracture in the area of junction of frontal parietal temporal, and sphenoid bones is seen on X-ray. A branch of which of the following arteries is most likely severed in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Loss of plantarflexion of the left foot B. Weakened inversion of the left foot C. Loss of sensation on the sole of the left foot D. Loss of sensation on the medial aspect of the left leg E. Loss of sensation on the dorsum of the left foot
Explanation:The common peroneal nerve is the most commonly injured nerve in the leg due to its superficial location where it courses laterally around the neck of the fibula. This location makes the common peroneal nerve susceptible to injury when a traumatic insult results in fracture of the neck of the fibula. The sciatic nerve branches into the common peroneal (fibular) nerve and the tibial nerve posteriorly on the thigh just proximal to the popliteal fossa. After coursing around the neck of the fibula the common peroneal nerve divides into superficial and deep branches. The superficial branch innervates the muscles of the lateral compartment of the leg which function primarily to evert the foot. The deep peroneal nerve innervates the anterior compartment of the leg whose muscles mainly act as dorsiflexors of the foot and toes, though they also participate in some inversion. The superficial peroneal nerve gives off branches that provide sensory innervation to the majority of the dorsum of the foot while the deep peroneal nerve provides sensory innervation only to the region between the first and second digits of the foot. Injury to the common peroneal nerve from a proximal fibula fracture would cause loss of sensation in both of these regions as well as motor deficits resulting in a clinical presentation with ‘toot drop”. (Choices A, B and C) Loss of plantarflexion of the left foot could result from injury of the tibial nerve as it courses through the middle of the popliteal fossa. Such an injury
92
Q NO 74: A 17-year-old football player comes to the ER hopping on his right foot. An X-ray of the left leg shows a fracture of the neck of the fibula. Which of the following findings do you most expect on physical examination?
USMLE WORLD STEP 1 ANATOMY
would also cause weakness of inversion of the foot as well as sensory loss on the sole. (Choice D) Loss of sensation on the medial aspect of the left leg would result from a lesion of the saphenous nerve. The saphenous nerve is the largest purely sensory branch of the femoral nerve.
Educational Objective: The common peroneal nerve is vulnerable to injury where it courses around the neck of the fibula. Fibular neck fractures can lesion this nerve, causing weakness of dorsiflexion (deep peroneal nerve) and eversion (superficial peroneal nerve) of the foot as well as loss of sensation over the dorsum of the foot. Inversion and plantarflexion would remain intact due to the action of the tibial nerve.
93

USMLE WORLD STEP 1 ANATOMY
A. Flexion of the humerus B. Extension of the humerus C. Adduction of the humerus D. Abduction of the humerus E. Medial rotation of the humerus
Explanation:The rotator cuff is made up of the tendons of the supraspinatus, infraspinatus, subscapularis, and teres minor muscles. These tendons along with the tendon of the long head of the biceps brachii muscle and the ligaments of the glenohumeral joint. contribute to the stability of the joint. In rotator cuff syndrome, the most commonly injured tendon is the supraspinatus because this tendon is prone to repeated impingement trauma between the humeral head and the acromion. The supraspinatus originates on the supraspinous fossa of the scapula and inserts on the superior portion of the head of the humerus and is primarily an abductor of the arm. Therefore, rotator cuff syndrome is most commonly associated with pain during abduction of the humerus. (Choice A) Flexion of the humerus at the shoulder is not accomplished by any of the rotator cuff muscles. The anterior segment of the deltoid is an important flexor of the humerus. (Choice B) Extension of the humerus is not accomplished by any of the rotator cuff muscles. (Choice C) Adduction of the humerus is not accomplished by any of the rotator cuff muscles. The main adductor of the humerus is the latissimus dorsi muscle. (Choice E) Medial rotation of the humerus is accomplished by the subscapularis muscle which originates on the subscapular fossa and inserts onto the lesser tubercle of the head of the humerus.
Educational Objective: The most commonly injured structure in rotator cuff syndrome is the tendon of the supraspinatus muscle. Because the supraspinatus is an abductor of the humerus injury to its tendon causes pain on abduction of the arm.
94
Q NO 75: A 52-year-old golfer presents to your office with right shoulder pain that has started to interfere with his daily activities, such as getting dressed. Imaging studies suggest calcification of the supraspinatus tendon. Which of the following is most likely to provoke pain in this patient?
USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
Explanation:This patient suffers from gastroesophageal reflux disease (GERD), a condition that affects the esophagus (labeled B above). In the thorax, the esophagus courses between the trachea and the vertebral bodies and is typically collapsed with no visible lumen. The trachea (Choice C) serves as a good landmark here because the radiolucency of the air in this structure allows one to differentiate it from the esophagus posteriorly and the great vessels anteriorly. (Choice A) This is the descending aorta. (Choice D)This is the arch of the azygous vein. (Choice E)This is a section of the right pulmonary artery.
Educational Objective: The esophagus is located between the trachea and the vertebral bodies in the superior thorax. It is typically collapsed with no visible lumen on CT images of the chest.
95
Q NO 76: A 47-year-old male with a long history of heartburn complains of feeling like food is “sticking in his throat.” He has changed his diet to accommodate this and now only consumes liquid foods. Which of the following structures in the computed tomography (CT) image below is responsible for this patient’s symptoms?

USMLE WORLD STEP 1 ANATOMY
A. Proprioception B. Pain C. Smell D. Vision E. Hearing E. Taste
Explanation:The thalamus is a part of diencephalon and has multiple functions. It translates information from all sensory pathways other than olfaction and selectively distributes those impulses to appropriate parts of the cortex (“relay” function). The following thalamic nuclei receive input from sensory pathways: 1. Ventral posterolateral nucleus (VPL) receives input from the spinothalamic tract (pain and temperature sensation) and medial lemniscus (position and proprioception). It transmits impulses to primary somatosensory cortex (Brodmann areas 3, 1 & 2). 2. Ventral posteromedial nucleus (VPM) receives inputs from the trigeminal and gustatory pathways and transmits them to the primary sensory cortex (Brodmann’s areas 3, 1 & 2). 3. Lateral geniculate body is a “relay” nucleus for the vision pathway. It receives impulses from the optic nerve and transmits them via the optic radiations to the visual cortex (calcarine sulcus). 4. Medial geniculate body is a part of the auditory pathway. It receives impulses from the superior olivary nucleus and the inferior colliculus of the pons, and projects them to the auditory cortex of the temporal lobe (Brodmann areas 41 & 42). The olfactory tract is the only sensory pathway where input is not processed through the thalamus.
Educational Objective: All sensory pathways except olfaction (smell) have relay nuclei in the thalamus. The VPL receives impulses from spinothalamic and medial lemniscus pathways, the VPM from the trigeminal and gustatory pathways, and the lateral and medial geniculate bodies are relay nuclei for the visual and auditory pathways respectively.
96
Q NO 77: A 54-year-old male undergoes evaluation for neurological symptoms. MRI scan shows bilateral infarcts in the thalami. Which of the following sensory pathways reaches the cortex without relay nuclei in the thalami?

USMLE WORLD STEP 1 ANATOMY
A. Vestibulocochlear B. Vagal C. Trigeminal D. Facial E. Accessory
Explanation:The patient described in the question has experienced a vasovagal syncope after stimulation of his posterior external auditory canal by an otoscope speculum. In this form of syncope, parasympathetic outflow via the vagus nerve (CNX) leads to decreased heart rate and blood pressure. The posterior part of the external auditory canal is innervated by the small auricular branch of the vagus nerve. Most of the remainder of the external auditory canal, including the external portion of the tympanic membrane, is innervated by the mandibular division of the trigeminal nerve via its auriculotemporal branch. The inner surface of the tympanic membrane is innervated by the glossopharyngeal nerve (CN IX) via its tympanic branch. (Choice A) The vestibulocochlear nerve (CN VIII) mediates hearing and vestibular proprioception. It does not mediate any cutaneous sensation. (Choice C)The mandibular branch of the trigeminal nerve (CN V3) does carry sensation to the majority of the external auditory meatus, except for the posterior wall. (Choice D) The facial nerve is represented in the middle ear by one of its branches, the chorda tympani nerve. The chorda tympani nerve carries the afferent taste fibers from the anterior two-thirds of the tongue as well as efferent parasympathetic preganglionic fibers that will ultimately innervate the submandibular and sublingual salivary glands. CN VII has a small motor component to the stapedius and behind the ear but does not carry cutaneous sensory information. (Choice E) The accessory nerve (CN Xl) provides voluntary motor innervation to the trapezius and the sternocleidomastoid.
Educational Objective: The vagus nerve provides some cutaneous sensation to the posterior external auditory canal via its small auricular branch. Sensation to the rest of the canal is from CN V3. A vasovagal syncopal episode results from stimulation of the vagus nerve, leading to a decrease in blood pressure and heart rate.
97
Q NO 78: A 34-year-old swimmer presents to your office with external ear infection. While inspecting the patient you insert a speculum in to the external auditory meat us in close contact with its posterior wall. The patient faints during the procedure. Irritation of which of the following nerves was most likely induced by the procedure?
USMLE WORLD STEP 1 ANATOMY
A. Left
kidney B. Spleen C. Liver D. Visceral pleura E. Pancreas
Explanation:The 12th rib overlies the parietal pleura medially and the kidney laterally. Recall that the 11th and 12th ribs are “floating” ribs, meaning that they are not bound to the anterior rib cage by cartilage as are the more superior “false” ribs. For this reason the distal tip of the left 12th rib can be displaced into the retroperitoneum when fractured lacerating the left kidney. (Choice B) The spleen lies in the posterior superior portion of the left abdominal cavity. The left 8th, 9th and 10th ribs overlie the spleen. (Choice C) The liver occupies much of the right upper quadrant of the abdominal cavity. The 8th, 9th 10th and 11th ribs over lie the liver’s posterior surface on the right. The positions of both the liver and spleen shift slightly with diaphragmatic movement during inhalation and exhalation. (Choice D)The visceral pleura envelop the lungs. At rest the inferior margin of the left lung lies at the level of the 10th rib in the mid scapular line. During maximal inhalation the lung may descend to the level of the most medial portion of the 12th rib but fractures of the 1st through 6th ribs have the greatest chance of damaging the visceral pleura. (Choice E) The pancreas is a partially retroperitoneal organ that overlies the body of the second lumbar vertebra. Classically crushing abdominal trauma is the injury that causes pancreatic damage.
Educational Objective: The left kidney lies immediately deep to the tip of the 12th rib on the left.
98
Q NO 79: A 21-year-oldfootball player is brought to the emergency room complaining of back pain. An X-ray shows a fractured 12th rib on the left side. Which of the following structures is most likely to be lacerated by the broken rib?
USMLE WORLD STEP 1 ANATOMY
A. Inferior thyroid artery B. Ansa cervicalis C. Lung pleura D. Accessory nerve E. Carotid body
Explanation:The patient likely has a tension pneumothorax, a condition where air enters the pleural cavity during inspiration but is not expelled during exhalation. An increasing volume of air accumulates within the pleural space, ultimately causing deviation of the lungs and mediastinum to the opposite side of the chest. The increased pressure within the chest cavity causes decreased systemic venous return to the heart leading to decreased cardiac output. Signs and symptoms of tension pneumothorax include tachycardia, hypotension, tachypnea, hypoxia, and absence of breath sounds and hyperresonance to percussion on the affected side. A chest X-ray will confirm the diagnosis; treatment is emergent needle thoracostomy or chest tube. In patients with neck injuries itis important to remember that the lung apices and cervical pleura extend above the clavicle and first rib through the superior thoracic aperture into the neck. As the above radiograph illustrates stab wounds immediately above the clavicle and lateral to the manubrium can puncture the pleura and cause pneumothorax, tension pneumothorax or hemothorax.
99
Q NO 80: A 22-year-old male is brought to the emergency room after being involved in a fight in a nearby bar. His blood pressure is 100/70 mmHg and his heart rate is 100/mm. Physical examination reveals a penetrating right-sided neck injury just above the clavicle and lateral to the manubrium sterni. Which of the following structures was most likely injured?

USMLE WORLD STEP 1 ANATOMY
(Choice A) The inferior thyroid artery arises from the thyrocervical trunk, which itself arises from the subclavian artery. The inferior thyroid artery courses posterior to the carotid artery and jugular vein and supplies the inferior pole of the thyroid gland. (Choice B) The ansa cervicalis arises from the C1, C2 and C3 nerve roots and innervates the sternohyoid, sternothyroid and omohyoid muscles of the anterior neck. Penetrating trauma to the neck superior to the cricoid cartilage might injure this nerve. (Choice D) The accessory nerve (CN XI) innervates the sternocleidomastoid and trapezius muscles. This nerve may be injured during surgery involving the posterior triangle of the neck (a region bounded by the sternocleidomastoid muscle trapezius muscle and clavicle). (Choice E)The carotid body which contains O2, CO2 and H+ chemoreceptors, lies at the bifurcation of the common carotid artery (just inferior to the hyoid bone).
Educational Objective: The lung apices extend above the level of the clavicle and first rib through the superior thoracic aperture. Penetrating injury in this area may lead to pneumothorax.
100

USMLE WORLD STEP 1 ANATOMY
A. Serratus anterior B. Latissimus dorsi C. Deltoid D. Rhomboid major E. Teres major
Explanation:Injury to the long thoracic nerve results in paralysis of the serratus anterior. This presents as a winged scapula which means that the medial border and inferior angle sticks out posteriorly like a bird’s wing when the patient presses anteriorly against a wall. (Choice B)The latissimus dorsi muscle is innervated by the thoracodorsal nerve and serves to adduct and extend the humerus. (Choice C)The deltoid is innervated by the axillary nerve and has three segments that act to flex extend, and abduct the arm. (Choice D)The rhomboid major is innervated by the dorsal scapular nerve and acts to draw the scapula medially at its medial border. (Choice E) The teres major is innervated by the subscapular nerve and acts to adduct and medially rotate the arm. This muscle is nota part of the rotator cuff.
Educational Objective: The serratus anterior muscle serves to fix the scapula against the posterior chest wall and rotate the scapula to allow abduction of the arm over the head. Paralysis of this muscle occurs with injury to the long thoracic nerve and results in winging of the scapula.
101
Q NO 81: A 24-year-old male complains of ‘clumsiness’ of his right arm. The patient is asked to face a wall and push against it with both hands. Abnormal prominence of the right inferior scapular angle is observed during the maneuver. Which of the following muscles is most likely denervated in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Esophageal varices B. Rectal varices C. Varicocele D. Left-sided ankle swelling E. Periumbilical venous distention
Explanation:A left-sided abdominal mass compressing the left renal vein would be expected to cause venous hypertension, varicosities, and edema in any upstream structures. In contrast to the right renal vein the left renal vein drains the left suprarenal gland and the left gonad in addition to the kidney. The renal veins do not participate in portal circulation. The patient described in the case above is a male, so venous hypertension due to obstruction of the left renal vein would eventually cause incompetence of the valves of the testicular veins and engorgement of the pampiniform plexus of veins around the testis. Leading to a left-sided varicocele. Varicocele is most common on the left side due to this anatomy. Varicocele arising from idiopathic failure of the valves of the testicular vein is generally left untreated unless it becomes symptomatic or is felt to be causing problems with fertility. (Choices A, B and E) Esophageal varices, rectal varices, and periumbilical venous distension are all signs of portal venous hypertension. The renal veins are nota part of the portal system. (Choice D) Unilateral left-sided ankle swelling can result from many causes including obstruction of the left common iliac vein, left external iliac vein, left femoral vein, or any of the other major veins of the left leg.
Educational Objective: The left gonadal (testicular or ovarian) vein drains into the left renal vein, commonly leading to left-sided varicoceles in males with obstructions of the left renal vein. The right gonadal vein drains directly into the inferior vena cava.
102
Q NO 82: A left-sided mass identified on an abdominal CT image in a 54-year-old male compresses the renal vein. Based on these CT scan findings, which of the following would you expect most in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Celiac trunk B. Superior mesenteric artery C. Inferior mesenteric artery D. Internal iliac artery E. External iliac artery
Explanation:This patient has a tumor in the descending colon. The distal 1/3 of the transverse colon, descending colon sigmoid colon, and rectum are all hindgut derivatives. Hindgut structures receive arterial blood from the inferior mesenteric artery (IMA), a branch of the aorta. These structures are drained by the inferior mesenteric vein (IMV)I which does not course with the IMA. The IMV drains blood from the hindgut into the splenic vein, which drains into the portal vein. (Choice A) The celiac trunk supplies blood to most foregut structures with the exception of the mouth pharynx and proximal esophagus. The foregut encompasses all structures from the mouth to the second part of the duodenum. Foregut derivatives include the liver pancreas gallbladder and spleen. (Choice B) The superior mesenteric artery supplies blood to the midgut which spans from the third part of the duodenum to the proximal 2/3 of the transverse colon. (Choice D)The internal iliac arte supplies portions of the gut through branches like the middle rectal artery and the inferior rectal artery (a branch of the pudendal artery, which arises from the internal iliac artery). (Choice E) Branches of the external iliac artery supply the lower extremity and anterior abdominal wall.
Educational Objective: The hindgut encompasses the distal 1/3 of the transverse colon the descending colon the sigmoid colon and the rectum. These structures receive their main arterial blood supply from the inferior mesenteric artery.
103
Q NO 83: A 56-year-old male is undergoing evaluation for fatigue, vague abdominal discomfort, and bloody stools. Colonoscopy reveals a mass in the descending colon. Surgical removal of the mass requires proper ligation of the:

USMLE WORLD STEP 1 ANATOMY
A. Popliteal fossa B. Fibular head C. Lateral compartment of the leg D. Anterior compartment of the leg E. Medial malleolus
Explanation:The common peroneal (fibular) nerve is the most commonly injured nerve in the leg due to its superficial location where it courses laterally around the neck of the fibula. This location makes this nerve susceptible to trauma resulting from lateral blows to the knee as well as from tightly applied plaster casts and other devices. The sciatic nerve branches into the common peroneal nerve and the tibial nerve posteriorly in the thigh just proximal to the popliteal fossa. After coursing around the neck of the fibula, the common peroneal nerve divides into superficial and deep branches. The superficial branch innervates the muscles of the lateral compartment of the leg, which function primarily to evert the foot. The deep peroneal nerve innervates the anterior compartment of the leg whose muscles act as dorsiflexors of the foot and toes. The superficial peroneal nerve gives oft branches that provide sensory innervation to the majority of the foot while the deep peroneal nerve provides sensory innervation only to the region between the first and second digits of the foot. Injury to the common peroneal nerve would cause a clinical presentation of foot drop due to weakness of the dorsiflexors. The foot would also be held in inversion due to weakness of the muscles of the lateral compartment. (Choice A) The popliteal artery and vein, as well as the tibial nerve, course through the middle of the popliteal fossa. The tibial nerve provides plantar flexi on and inversion: therefore injury to the tibial nerve would result in unopposed dorsiflexion and eversion of the foot. (Choices C and D)The lateral and anterior compartments of the leg are innervated by the superficial and deep peroneal nerves, respectively. These nerves lie deep within their respective compartments and are unlikely to be injured by superficial pressure. (Choice E) Several important structures course near the medial malleolus. The saphenous nerve and great saphenous vein lie anteriorly while the posterior tibial artery, the tibial nerve, and the tendons of the flexor digitorum longus, flexor hallucis longus, and tibialis posterior course posteriorly.
Educational Objective: Trauma or sustained pressure to the neck of the fibula can cause injury to the common peroneal nerve as it courses superficially and laterally to this structure.
104
Q NO 84: A 7-year-old male has a right leg cast alter a bicycle accident. After wearing the cast for some time he complains of pain and numbness of the dorsum of his right foot and cannot dorsiflex his right ankle. Which of the following is the most likely site of nerve compression in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Common iliac arteryB. Phrenic artery C. Internal iliac artery D. Renal artery E. Lumbar arteries F. Superior vesical artery
Explanation:In a kidney transplant operation the native kidneys are typically left in place, and the donor kidney is placed retroperitoneally in the right iliac fossa. Blood supply to the donor organ is typically established by anastomosing the donor renal artery with the recipient’s external iliac artery. Similarly the donor renal vein is connected to the recipient’s external iliac vein. The proximal 1/3 of the donor ureter is preserved and used to establish continuity from the collecting system of the kidney to the recipient’s bladder. This portion of the ureter receives its blood supply from branches of the renal artery. (More distally, the ureters are supplied by branches from the aorta and iliac, gonadal and vesical arteries.) Ureteric ischemia occurs in approximately 2% of renal transplant patients. (Choice A) Small branches from the common iliac artery may supply the ureter’s midportion. (Choice B)The inferior phrenic arteries are branches of the aorta that supply the diaphragm and provide branches to the suprarenal glands. These arteries do not supply the ureters. (Choice C) An alternate method of providing blood supply to a transplanted kidney is end-to-end anastomosis with the internal iliac artery. The internal iliac artery does not directly contribute to the blood supply of the ureter. (Choice E) The lumbar arteries like the intercostal arteries arise directly from the aorta to supply the lumbar vertebrae and surrounding structures. They do not supply the ureters. (Choice F) The superior vesical artery is a branch of the internal iliac artery that supplies blood to the superior portion of the urinary bladder. It also provides branches to the distal ureter.
Educational Objective: The proximal 1/3 of the ureter receives its blood supply from branches of the renal artery. For this reason this portion of the donor ureter is typically viable after renal transplantation.
105
Q NO 85: A surgeon transplants a donor kidney into a 45-year-old patient with end-stage renal disease. The upper 1/3 of the ureter of the transplanted kidney is retained and attached to the recipient patient’s bladder. However, soon after transplantation, the ureter becomes necrotic. Which of the following arteries is the major source of blood supply to the upper ureter?

USMLE WORLD STEP 1 ANATOMY
A. Common bile duct B. Ureter C. Superior mesenteric artery D. Portal vein F. Gastroduodenal artery
Explanation:The first part of the duodenum, the portion emerging from the pylorus of the stomach, is horizontally oriented and overlies the first lumbar vertebra. It is the only part of the duodenum that is not retroperitoneal. The second part of the duodenum courses inferiorly from the level of Li to L3. This part of the duodenum is in close relation to the head of the pancreas. The ampulla of Vater, the site where the pancreatic and common bile ducts provide their secretions, is in the second part of the duodenum. The third part of the duodenum courses horizontally over the third lumbar vertebra, abdominal aorta, and inferior vena cava. Itis in close association with the uncinate process of the pancreas and the superior mesenteric artery and vein, which puts these structures at high risk for direct invasion by a tumor in the third part of the duodenum. The fourth part of the duodenum courses superiorly and to the left of the L2 and L3 vertebrae and becomes the jejunum past the ligament of Treitz. (Choice A) The common bile duct is formed when the common hepatic bile duct and the cystic duct join in the porta hepatis region of the hepatogastric ligament. This common bile duct courses interiorly posterior to the pylorus and within the head of the pancreas to drain into the second part of the duodenum. (Choice B)The left ureter has no relation to the duodenum. The right ureter courses retroperitoneally posterior to the second part of the duodenum for a short length. (Choice D) The portal vein is formed retroperitoneally, posterior to the pancreas at the level of the first lumbar vertebra, by the fusion of the superior mesenteric and splenic veins. The portal vein is not in contact with the duodenum at any point. (Choice E)The gastroduodenal artery arises from the common hepatic artery and courses inferiorly, posterior to the first part of the duodenum where it then splits into the anterior superior pancreaticoduodenal artery and the right gastroepiploic artery.
Educational Objective: The third part of the duodenum courses horizontally across the abdominal aorta and inferior vena cava at the level of the third lumbar vertebra. Here itis in close association with the uncinate process of the pancreas and the superior mesenteric vessels.
106
Q NO 86: A 56-year-old male with recent recurrent vomiting and weight loss is found to have a malignancy originating from the third part of the duodenum. Which of the following structures is at greatest risk for direct penetration by tumor?

USMLE WORLD STEP 1 ANATOMY
A. T12 B. L2 C. L4 D. L5 E. S1E. S4
Explanation:In the adult, the spinal cord terminates in a tapering fashion at the conus medullaris at approximately the L2 vertebral level. After this point, spinal nerves course from the conus medullaris inferiorly to exit through their respective intervertebral foramina. This collection of spinal nerves, which at this point are considered peripheral nerves, is referred to as the cauda equina (horse’s tail). Cauda equina syndrome typically results from a massive rupture of an intervertebral disc that is capable of causing compression of many or all of the spinal nerves of the cauda equina, but it can also occur due to any trauma or space- occupying lesion of the lower vertebral column. Symptoms classic of cauda equina syndrome include saddle anesthesia and loss of the anocutaneous reflex as described in the question, as well as bowel and bladder dysfunction and symptoms of sciatica. Of the spinal nerves potentially involved, a lesion of S2 through S4 will specifically result in the symptoms described in the question stem as they reflect impairment of the pudendal nerve that innervates the perineum. (Choice A) Compression atTl2would result in impingement of the spinal cord itself in the region of origin of the lumbar spinal nerves. (Choice B) L2 lesions would cause anesthesia or paresthesias posteriorly in the gluteal region inferior to the iliac crests and anteriorly on the thigh inferior to the femoral triangle and inguinal ligament. (Choice C) The L3 and L4 spinal levels contribute to the femoral nerve and mediate the quadriceps (knee-jerk, patellar) reflex. A lesion to these levels would cause loss of this reflex as well as paresthesias and weakness over the anterior thigh. (Choice D) L5 lesions would cause a loss of sensation or paresthesias over the anterior leg. (Choice E) S1 and S2 mediate the Achilles (ankle-jerk) reflex, which tests for the integrity of the sciatic nerve. A lesion of these roots would cause sensory loss or paresthesias over the posterior leg and thigh.
Educational Objective: Saddle anesthesia and loss of the anocutaneous reflex are symptoms of the cauda equina syndrome, associated with damage to the S2 through S4 nerve roots.
107
Q NO 87: A 53-year-old Caucasian male comes to the ER with severe low back pain of sudden onset. Pinprick in the perianal area does not cause rapid contraction of the anal sphincter in this patient. This finding indicates involvement of which of the following nerve roots?

USMLE WORLD STEP 1 ANATOMY
A. AB. BC. CD. DE. E
Explanation:A fall on an outstretched, dorsiflexed hand is the classic injury that causes lunate dislocation. The lunate (Choice D) is one of the proximal carpal bones. It can be identified on an X-ray of the hand as the more medial of the two bones that articulate with the radius. The scaphoid is the other (more lateral) bone that articulates with the radius (Choice C). Injuries that cause lunate dislocation also often cause fracture of the scaphoid. A potential late sequela of such an injury is avascular necrosis of the proximal scaphoid fracture fragment. (Choice A) The trapezium is the most lateral of the distal carpal bones. Recall that the “thumb swings on the trapezium.” (Choice B)The capitate bone lies in the center of the wrist. (Choice E) The triquetrum bone is located in the proximal medial wrist and together with the lunate forms the small articular surface between the distal ulna and the carpal bones.
Educational Objective: The lunate bone can be identified on a hand X-ray as the more medial of the two carpal bones that articulate with the radius. It lies immediately medial to the scaphoid bone.
108
Q NO 88: A 34-year-old female presents to the emergency room after falling in the bathroom. She complains of wrist pain and numbness in her right palm. Based on her symptoms. you suspect that she has dislocated the lunate bone in the wrist. Identify the lunate bone on the X-ray below.
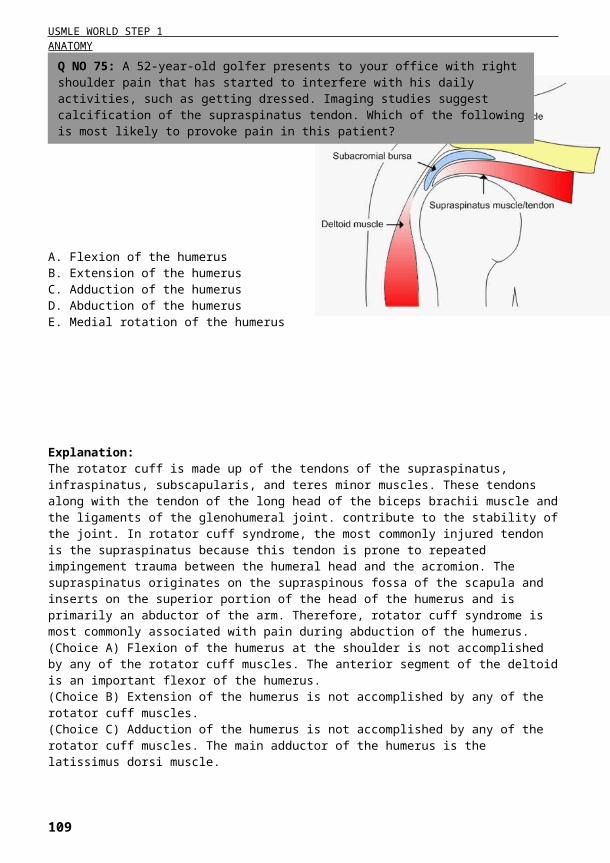
USMLE WORLD STEP 1 ANATOMY
A. Rhomboid muscles B. Sternocleidomastoid muscle C. Pectoralis minor muscle D. Serratus anterior muscle E. Subclavius muscle P. Sternoclavicular ligaments
Explanation:Several muscles insert on the clavicle, including the pectoralis major muscle on the inferior medial aspect, the deltoid muscle on the inferior lateral aspect, the subclavius muscle on the inferior lateral aspect, the trapezius muscle on the superior lateral aspect, and the sternocleidomastoid muscle on the superior medial aspect. The sternocleidomastoid muscle is responsible for the upward traction on the medial section of the fractured clavicle described above. Recall that the sternocleidomastoid muscle has three points of insertion (described in its name): “sterno—the muscle inserts inferiorly on the manubrium of the sternum “cleido”—the muscle inserts inferiorly on the medial part of the clavicle, “mastoid—the muscle inserts on the mastoid process of the skull. (Choice A) Both the major and the minor rhomboid muscles originate on the vertebral bodies/spines and insert on the scapular spine. (Choice C)The pectoralis minor muscle originates on the coracoid process of the scapula and inserts on the 34th and 5th ribs. (Choice D)The serratus anterior muscle originates laterally on the through 8th ribs and inserts onto the medial border of the scapula. This muscle is innervated by the long thoracic nerve injury to which causes winging of the scapula. (Choice E)The subclavius muscle originates on the 1st rib and inserts on the inferior lateral aspect of the clavicle. (Choice F)The sternoclavicular ligaments join the clavicle to the manubrium. These ligaments would tend to hold the medial fragment of the clavicle in place.
Educational Objective: The sternocleidomastoid muscle originates on the medial clavicle and manubrium and inserts on the mastoid process of the skull. Itis innervated by CN Xl and functions to turn the head in the opposite direction.
109
Q NO 89: A 34-year-old male presents to the emergency room complaining of severe right shoulder pain after falling from a tree. X-ray reveals a fracture in the middle third of the right clavicle. The medial end of the fractured clavicle is displaced upward due to traction by the:

USMLE WORLD STEP 1 ANATOMY
A. Superomedial quadrant of the buttock B. Superolateral quadrant of the buttock C. Inferomedial quadrant of the buttock D. Inferolateral quadrant of the buttock E. Posterior thigh
Explanation:All injections into the gluteal region should target the superolateral quadrant to avoid damage to the gluteal nerves and sciatic nerve. This patient is exhibiting the classic “gluteus medius gait” i.e. the hip dips downward when the ipsilateral foot is lifted off of the ground. This gait is observed when there is injury to the superior gluteal nerve or to the gluteus medius muscle itself. The superior gluteal nerve is derived from the L4-S1 ventral rami and leaves the pelvis through the greater sciatic foramen above the level of the piriformis. Injection in the superomedial quadrant of the buttock is likely to injure this nerve. (Choice B)The superolateral quadrant of the buttock is a safe site for intramuscular injections. (Choice C) The sciatic nerve courses through the inferomedial quadrant of the buttock, thus nerve damage can occur with injections to this site. (Choice D)The inferolateral quadrant of the buttock is the site where many of the muscles of the gluteal region have their tendinous insertions. (Choice E) The sciatic nerve courses just below the biceps femoris muscle in the posterior thigh. The sciatic nerve innervates all of the knee flexors (hamstrings) with the exception of the short head of the biceps femoris.
Educational Objective: Injections given in the superomedial part of the buttock risk injury to the gluteal nerves, Injections given in the inferomedial part of the buttock risk injury to the sciatic nerve. The superolateral quadrant of the buttock is a safe site for intramuscular injections.
110
Q NO 90: A 43-year-old male received a deep intramuscular injection two days ago and now presents with difficulty walking. You note that his right hip drops every time he raises his right foot. At which location did this patient most likely receive his injection?
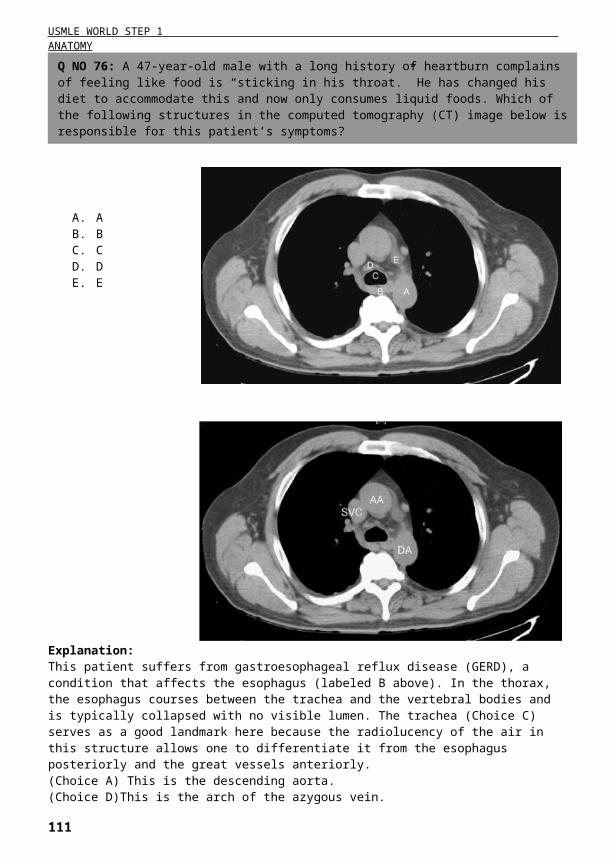
USMLE WORLD STEP 1 ANATOMY
A. Posterior arm B. Posterior forearm C. Lateral forearm D. Medial forearm E. Thenar eminence
Explanation:This patient has symptoms suggestive of injury the musculocutaneous nerve. The musculocutaneous nerve is derived from the C5-C7 ventral rami. As its name implies the musculocutaneous nerve provides both motor innervation and somatic sensory innervation to the arm. It innervates the major upper arm flexors including the biceps brachii, coracobrachialis, and brachialis muscles. After innervating these muscles, the remaining fibers continue as the lateral cutaneous nerve of the forearm, providing sensory innervation to the skin of the lateral forearm. (Choice A) The posterior arm is innervated by a branch of the radial nerve (posterior cutaneous nerve of the arm). (Choice B)The posterior forearm is innervated by a branch of the radial nerve (posterior cutaneous nerve of the forearm). (Choice D)The medial forearm is innervated by a branch of the ulnar nerve (medial cutaneous nerve of the forearm).(Choice E) The thenar eminence is innervated by the superficial branch of the radial nerve.
Educational Objective: The musculocutaneous nerve innervates the flexor muscles of the upper arm and provides sensory innervation to the lateral forearm. The musculocutaneous nerve is derived from the upper trunk of the brachial plexus and can be injured by forceful injuries that cause separation of the neck and shoulder.
111
Q NO 91: A young athlete presents to your office after sustaining an injury to the right upper extremity. Physical examination reveals weak right forearm flexion and an absent biceps reflex. Given these findings, sensation loss in which of the following areas is most likely to be found in this patient?

USMLE WORLD STEP 1 ANATOMY
A. Common hepatic B. Right gastroepiploic C. Left gastric D. Gastroduodenal E. Inferior pancreaticoduodenal F. Splenic G. Superior mesenteric
Explanation:The majority of gastric ulcers arise at the lesser curvature of the stomach. They are usually located at the transitional zone between the acid-secreting epithelium of the body of the stomach and gastrin-producing epithelium of the antrum. Glands in the body of the stomach contain parietal cells that produce HCI and intrinsic factor; mucosal glands in the antrum contain G-cells that secrete gastrin. A number of arteries supply the stomach. They are summarized in the table below:
112
Q NO 92: A 55-year-old Caucasian male is brought to the ER with profuse upper gastrointestinal bleeding. His past medical history is non-contributory. His blood pressure is 70/40 mmHg, and his heart rate is 120/mm. The patient dies one hour after admission, despite resuscitation efforts. Autopsy shows a deep peptic ulcer in the lesser curvature of the stomach. The ulcer most likely penetrated which of the following arteries?

USMLE WORLD STEP 1 ANATOMY
Left and right gastric arteries perfuse the lesser curvature of the stomach the most common site of gastric ulcers. These arteries run along the lesser curvature and are likely to be penetrated by ulcers, leading to hemorrhage. (Choice A) The common hepatic artery perfuses the liver, pylorus, duodenum, and pancreas. It arises from the celiac trunk and ends when it bifurcates in the hepatic proper and gastroduodenal arteries. (Choice B) The right gastroepiploic artery arises from gastroduodenal artery and perfuses the distal greater curvature of the stomach. Gastric ulcers don’t commonly occur in the greater curvature. (Choice D)The gastroduodenal artery supplies blood to the pylorus and the proximal part of the duodenum. It arises from the common hepatic artery. (Choice F) The splenic artery arises from the celiac trunk and supplies blood to the spleen. It gives rise to the left gastroepiploic artery and a number of short gastric arteries that perfuse proximal greater curvature of the stomach. (Choices E and G) The superior mesenteric and the inferior pancreaticoduodenal arteries do not perfuse the stomach.
Educational Objective: The great majority of gastric ulcers occur at the lesser curvature, at the border between acid-secreting and gastrin secreting mucosa. Left and right gastric arteries run along the lesser curvature and are likely to be damaged, causing gastric bleeding.
113