Embed Size (px)
Citation preview

AaEJ
FH
Bpspdnp
Otm
Micu
IDtactithtLbto
etIrai
fMrAGm2
1
nalysis of the left atrial appendage by magnetic resonancengiography in patients with atrial fibrillation. Kevin Heist, MD, PhD,* Marwan Refaat, MD,† Stephan B. Danik, MD,* Godtfred Holmvang, MD,‡
eremy N. Ruskin, MD,* Moussa Mansour, MD*
rom the *Cardiac Arrhythmia Service, †Department of Medicine, and ‡Cardiology Division, Massachusetts General
ospital, Harvard Medical School, Boston, Massachusetts.Rd1(ri
Cdss
Ka
(
ACKGROUND Recent interest has focused on the left atrial ap-endage (LAA) in the setting of atrial fibrillation as a potentialource of thromboembolism and stroke, which may be amenable toermanent occlusion by a variety of investigational catheter-elivered devices. Precise anatomic characterization of the LAA isecessary to determine the suitability of a patient for devicelacement and for device selection and sizing.
BJECTIVES The purpose of this study was to perform detailedhree-dimensional characterization of LAA size and geometry byagnetic resonance angiography.
ETHODS Fifty patients with chronic atrial fibrillation undergo-ng cardiac magnetic resonance angiography in preparation foratheter ablation of atrial fibrillation were analyzed for LAA vol-
tap
spppodov
MSTwMwfdAct
CM(w006.)
547-5271/$ -see front matter © 2006 Heart Rhythm Society. All rights reserved
ESULTS The average LAA volume was 17.3 � 6.7 mL, with aepth of 26.6 � 4.9 mm and a “neck” diameter of 20.0 � 5.3 mm �4.1 � 4.7 mm. The average number of LAA lobes was 1.4 � 0.7range 1–4). Substantial interpatient variability was present in theelative dimensions and morphology of the LAA. There was a signif-cant correlation between left atrial size and LAA neck dimensions.
ONCLUSION There is significant heterogeneity in LAA size andimensions among patients with atrial fibrillation. Device occlu-ion of the LAA may require devices that are available in multipleizes/shapes or that can adapt to this heterogeneity.
EYWORDS Atrial fibrillation; Cardiac anatomy; Left atrial append-ge; Magnetic resonance imaging; Occlusion device
Heart Rhythm 2006;3:1313–1318) © 2006 Heart Rhythm Society.
me, neck size, depth, and overall geometry. All rights reserved.ntroductionetailed analysis of cardiac anatomy based on high-resolu-
ion imaging studies is increasingly utilized by cardiologistsnd cardiac electrophysiologists to guide interventional pro-edures. Precise characterization of left atrial (LA) struc-ures, particularly the pulmonary veins, has been importantn the evolution of the ablation procedure for atrial fibrilla-ion (AF).1,2 Until recently, the left atrial appendage (LAA)as been considered primarily as a potential source ofhromboembolus and stroke. For this reason, imaging of theAA has primarily been directed at the presence of throm-us, spontaneous echo contrast, and other risk factors forhromboembolism by echocardiography,3,4 with less focusn detailed LAA dimensions and geometry.
The recent development of percutaneous, catheter-deliv-red LAA closure devices may allow for the direct preven-ion of strokes associated with LAA thromboembolism.5,6
n order for such a device to fully occlude and be safelyetained within the LAA, either it must be a reasonable sizend shape to match a particular patient’s LAA anatomy, ort must be able to adapt to a variety of LAA dimensions. For
Dr. Heist is a speaker for Guidant Corp. and receives research supportrom Guidant Corp. and St. Jude Medical. Dr. Ruskin is a consultant for
edtronic. Dr. Mansour is a consultant for Biosense-Webster. Addresseprint requests and correspondence: Dr. Moussa Mansour, Cardiacrrhythmia Service and Cardiac Unit, Massachusetts General Hospital,ray 109, 55 Fruit Street, Boston, Massachusetts 02114. E-mail address:[email protected]. (Received June 17, 2006; accepted July 17,
his reason, a detailed description of the range of LAA sizesnd anatomic variations present in patients with AF is im-ortant.
The aim of this study was to analyze the three-dimen-ional geometry and dimensions of the LAA in a series ofatients with chronic AF by magnetic resonance angiogra-hy (MRA), with a focus on measurements likely to bearticularly important with regard to the selection and sizingf occlusion devices. These dimensions include LAA neckiameter (short and long axis), depth, volume, and numberf lobes. In addition, a comparison was made betweenarious patient characteristics and LAA dimensions.
ethodstudy populationhe study population consists of 50 consecutive patientsith chronic AF undergoing gadolinium-enhanced cardiacRA in preparation for catheter ablation procedures for AFith adequate imaging of the entire LAA. MRA was per-
ormed in all patients prior to the ablation procedure. AFuration was measured from the first documented episode ofF until the MRA was performed. Body surface area was
alculated based on the Mosteller formula. Patient charac-eristics are given in Table 1.
ardiac MRARA was performed using a 1.5-T Signa CVi MR scanner
GE Healthcare, Milwaukee, Wisconsin) with Excite-2 soft-
are and with an eight-channel phased-array receiver coil.. doi:10.1016/j.hrthm.2006.07.022
Aigetm
pSec2t
dhlpeka
Gweem“rta
tTawa(dl
ETddo
T
V
AAGHDLLCBAAASC
t
Fde
1314 Heart Rhythm, Vol 3, No 11, November 2006
fter initial cardiac localization with multislice SSFP sag-ttal and axial scans, a single-slice multiphase fast spoiledradient echo image series was acquired during held end-xpiration using an oblique coronal view of the LA. An LAime-intensity curve was defined with a test bolus of 8 to 10L of intravenous gadopentetate dimeglumine.MRA focused on the LA and surrounding structures was
erformed with a three-dimensional (3D) fast time-of-flightPGR pulse sequence and sagittal slab volume during heldnd-expiration (average 40 seconds). The LA slab typicallyontained 56 to 64 slice locations with partition thickness of.4 to 2.6 mm and a matrix size of 256 � 192 interpolatedo a 512 matrix with zero-fill interpolation �2 in the z-
able 1 Patient characteristics (n � 50)
ariable Result
ge (yr) 62.2 � 9.6trial fibrillation duration (yr) 5.4 � 4.8ender (male) 88%ypertension 62%iabetes 8%eft ventricular ejection fraction 58.1 � 11.4eft atrial size (mm) 45.9 � 5.7reatinine 1.03 � 0.23eta-blocker 46%ngiotensin-converting enzyme inhibitor 36%ngiotensin receptor blocker 10%miodarone 42%otalol 36%lass I antiarrhythmic drug 16%
Values are given as mean � SD or percent.All drugs listed are based on what the patient was prescribed at the
ime of the procedure.
A
LAA
LPV
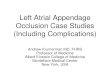
igure 1 Measurements of the left atrial appendage (LAA) by three-iameter short and long axis from an endoluminal view of the left atrium
ndoluminal surface of the LAA, digitally transected from the left atrium at the Lirection. The scan was timed to coincide with peak en-ancement of the LA from IV injection of 40 mL of gado-inium at 4 mL/s, followed by saline flush. Typical scanarameters included field of view 28 cm, time to fractionalcho 1.1 ms, repetition time 4.6 ms, receiver bandwidth 62.5Hz, flip angle 4°, number of excitations 1, and parallelcquisition phase acceleration factor 1.3.
The standard 3D volume analysis tools available on theeneral Electric Advantage Windows workstation equippedith software versions 3.1 and 4.0 was used to generate
ndoluminal “navigator” and volume-filled views of thendoluminal surfaces and internal volume of the LA, pul-onary veins, and LAA. The rendering mode was set to
smooth,” with the threshold set to an intensity level cor-esponding to the vascular boundaries. Fine adjustments tohresholding were made to refine the structures of the LAnd the LAA.
The “neck” of the LAA was defined as the site of reflec-ion of this structure with the surrounding LA (Figure 1).his neck was digitally transected, and endoluminal volumenalysis of the entire LAA was performed. Measurementsere made with electronic calipers of the short- and long-
xis measurements of the LAA neck, as well as its depthdefined from the center of the neck to the deepest directimension of the LAA; Figure 1). The number of majorobes of the appendage was defined.
chocardiographyransthoracic echocardiography was performed using stan-ard techniques. LA size as well as LV diastolic and systolicimensions were measured by two-dimensional echocardi-graphy in the parasternal long-axis view. Left ventricular
B
LAA Neck
ional magnetic resonance angiography. Measurement of the LAA neckd the LAA depth from a three-dimensional volume reconstruction of the
dimens(A) an
AA neck (B). LPV � left-sided pulmonary vein.
(m
SDwC
RLDptlotnasdnddtmmd
RIrpaaPtllrdti
l(oFhd
wna
T
DR
A) nec
FSsv
1315Heist et al MRA Analysis of the LAA
LV) ejection fraction was measured by the Simpsonethod.
tatistical analysisata are reported as mean � SD. Statistical correlationsere performed with Statview software (SAS Institute,ary, NC, USA). P �.05 was considered significant.
esultsAA dimensions and neckata for LAA volumetric analysis were available for all 50atients examined. The LAA is composed of an LAA bodyhat is separated from the LA by an oval-shaped “neck.” Theong axis of the LAA neck is generally in the superoinferiorrientation, and the short axis is directly perpendicular tohe long axis within the two-dimensional plane of the LAAeck. Delineation of the LAA neck (with short- and long-xis measurements of the neck) and the LAA depth arehown in Figure 1. The LAA endoluminal volume (withigital transaction of the LAA from the LA at the LAAeck) was determined to be 17.3 � 6.7 mL. The long-axisiameter of the neck was 20.0 � 5.3 mm, and the short-axisiameter was 14.1 � 4.7 mm. The LAA depth from the necko the deepest direct dimension of the LAA was 26.6 � 4.9
m. There was a large range between smallest and largesteasurements for LAA volume, neck dimensions, and
epth (Table 2).
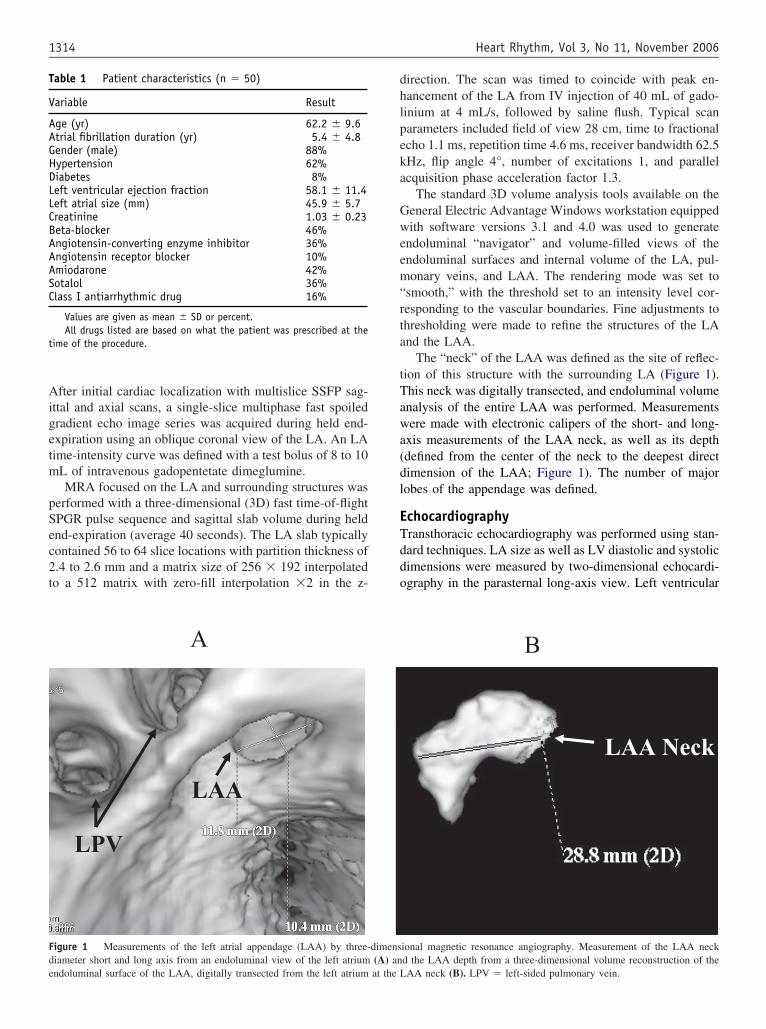
elationships between LAA dimensionst is important to determine whether there is a consistentelationship between the LAA size in one dimension com-ared with its size in its other major dimensions. There wassignificant correlation between the long-axis diameter
nd the short-axis diameter of the LAA neck (r � 0.72,�.0001; Figure 2). Despite this correlation, however,
here was great variability in the relative ratio of the short vsong axis of the neck, with some necks forming a relativelyong and narrow oval, whereas others were nearly perfectlyound. The average ratio of the short axis of the LAA neckivided by the long axis of the neck was 0.70 � 0.16, buthe range of this ratio was great (0.23–0.98) in the patientsn this study.
There were also significant correlations between theong-axis diameter of the LAA neck and the LAA depthr � 0.49, P � .0003) and between the short-axis diameterf the LAA neck and the LAA depth (r � 0.36, P � .01;igure 2). Similar to the variable shapes of the LAA neck,owever, there was also substantial variability in the relative
able 2 Dimensions of the left atrial appendage (n � 50)
Volume (mL) Depth (mm)
imension 17.3 � 6.7 26.6 � 4.9ange 5.0–35.7 14.3–37.2
All dimensions are expressed as mean � standard deviation.Neck-L � largest long-axis dimension of the left atrial appendage (LA
epth of the LAA in comparison to the neck dimensions, L
ith some LAA being relatively shallow compared with theeck dimensions and others being comparatively deep. Theverage ratio of the long axis of the LAA neck divided by
Neck-L (mm) Neck-S (mm) No. lobes
20.0 � 5.3 14.1 � 4.7 1.4 � 0.79.5–29.9 3.1–24.1 1–4
k; Neck-S � largest short-axis dimension of the LAA neck.
0
5
10
15
20
25
30
0 5 10 15 20 25 30 35
LAA Neck-Long Axis (mm)
LA
AN
eck-
Sh
ort
Axi
s (m
m)
Ar=0.72p<0.0001
0
5
10
15
20
25
30
35
40
0 5 10 15 20 25 30 35
LAA Neck-Long Axis (mm)
LA
A D
epth
(m
m)
Br=0.49p=0.0003
0
5
10
15
20
25
30
35
40
0 5 10 15 20 25 30
LAA Neck-Short Axis (mm)
LA
A D
epth
(m
m)
C r=0.36p=0.01
igure 2 Correlations between left atrial appendage (LAA) dimensions.catter plots of LAA neck long axis-dimension (x-axis) vs LAA neckhort-axis dimension (y-axis) (A), LAA neck long-axis dimension (x-axis)s LAA depth (y-axis) (B), and LAA neck short-axis dimension (x-axis) vs
AA depth (y-axis) (C). n � 50 for all plots.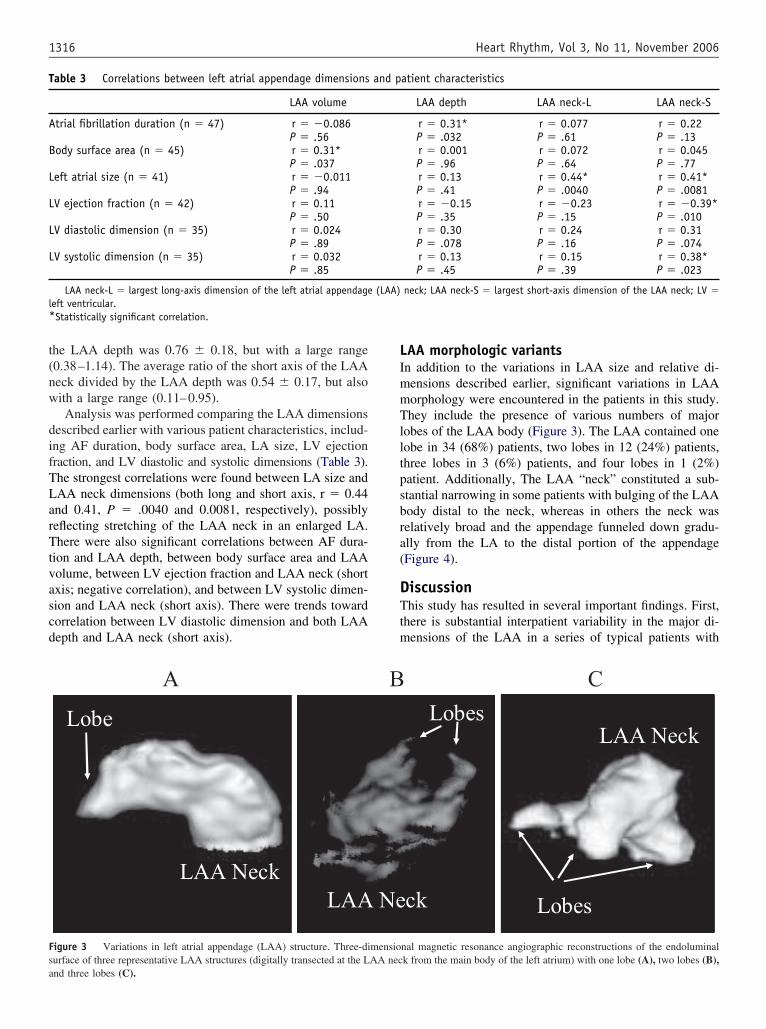
t(nw
difTLarTtvascd
LImmTlltpsbra(
DTtm
T
A
B
L
L
L
L
l*
Fsa
1316 Heart Rhythm, Vol 3, No 11, November 2006
he LAA depth was 0.76 � 0.18, but with a large range0.38–1.14). The average ratio of the short axis of the LAAeck divided by the LAA depth was 0.54 � 0.17, but alsoith a large range (0.11–0.95).Analysis was performed comparing the LAA dimensions
escribed earlier with various patient characteristics, includ-ng AF duration, body surface area, LA size, LV ejectionraction, and LV diastolic and systolic dimensions (Table 3).he strongest correlations were found between LA size andAA neck dimensions (both long and short axis, r � 0.44nd 0.41, P � .0040 and 0.0081, respectively), possiblyeflecting stretching of the LAA neck in an enlarged LA.here were also significant correlations between AF dura-
ion and LAA depth, between body surface area and LAAolume, between LV ejection fraction and LAA neck (shortxis; negative correlation), and between LV systolic dimen-ion and LAA neck (short axis). There were trends towardorrelation between LV diastolic dimension and both LAAepth and LAA neck (short axis).
able 3 Correlations between left atrial appendage dimensions
LAA volume
trial fibrillation duration (n � 47) r � �0.086P � .56
ody surface area (n � 45) r � 0.31*P � .037
eft atrial size (n � 41) r � �0.011P � .94
V ejection fraction (n � 42) r � 0.11P � .50
V diastolic dimension (n � 35) r � 0.024P � .89
V systolic dimension (n � 35) r � 0.032P � .85
LAA neck-L � largest long-axis dimension of the left atrial appendageeft ventricular.Statistically significant correlation.
Lobe
A
LAA NeckLAA
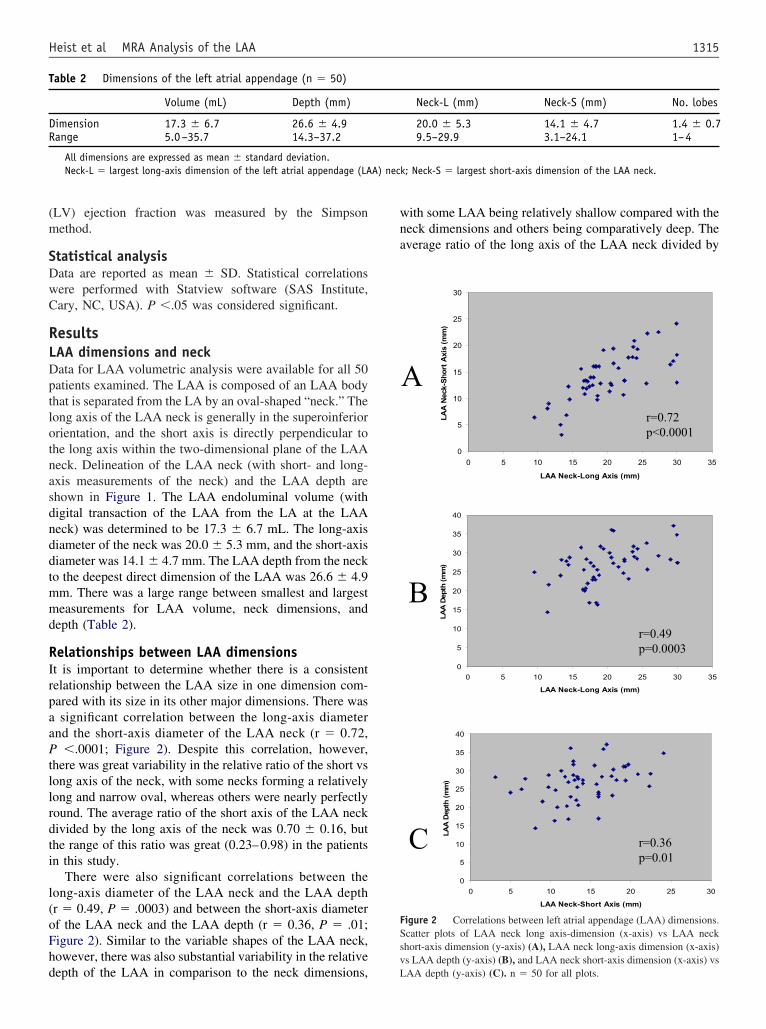
igure 3 Variations in left atrial appendage (LAA) structure. Three-diurface of three representative LAA structures (digitally transected at the L
nd three lobes (C).AA morphologic variantsn addition to the variations in LAA size and relative di-ensions described earlier, significant variations in LAAorphology were encountered in the patients in this study.hey include the presence of various numbers of major
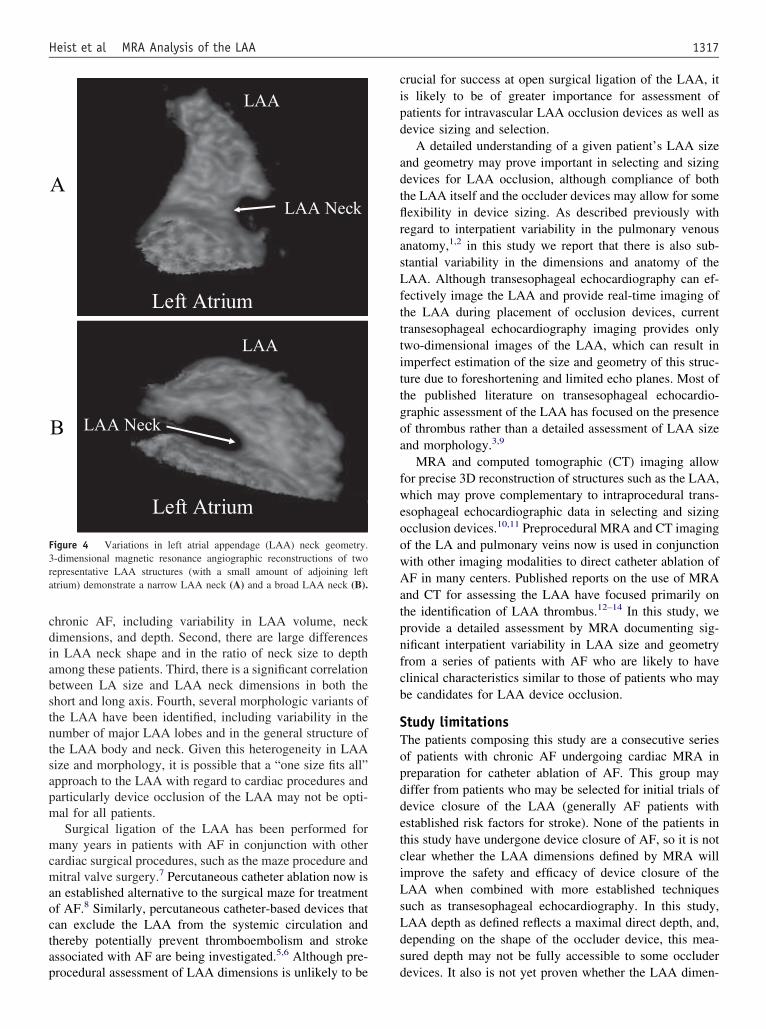
obes of the LAA body (Figure 3). The LAA contained oneobe in 34 (68%) patients, two lobes in 12 (24%) patients,hree lobes in 3 (6%) patients, and four lobes in 1 (2%)atient. Additionally, The LAA “neck” constituted a sub-tantial narrowing in some patients with bulging of the LAAody distal to the neck, whereas in others the neck waselatively broad and the appendage funneled down gradu-lly from the LA to the distal portion of the appendageFigure 4).
iscussionhis study has resulted in several important findings. First,
here is substantial interpatient variability in the major di-ensions of the LAA in a series of typical patients with
atient characteristics
LAA depth LAA neck-L LAA neck-S
r � 0.31* r � 0.077 r � 0.22P � .032 P � .61 P � .13r � 0.001 r � 0.072 r � 0.045P � .96 P � .64 P � .77r � 0.13 r � 0.44* r � 0.41*P � .41 P � .0040 P � .0081r � �0.15 r � �0.23 r � �0.39*P � .35 P � .15 P � .010r � 0.30 r � 0.24 r � 0.31P � .078 P � .16 P � .074r � 0.13 r � 0.15 r � 0.38*P � .45 P � .39 P � .023
neck; LAA neck-S � largest short-axis dimension of the LAA neck; LV �
Lobes
LAA Neck
LAA Neck
Lobes
Lobes
ck
C
nal magnetic resonance angiographic reconstructions of the endoluminalk from the main body of the left atrium) with one lobe (A), two lobes (B),
and p
(LAA)
Ne
B
mensioAA nec
cdiabstntsapm
mcmaoctap
cipd
adtflrasLftttittgoa
fweoowAatpnfcb
STopddetciLsLds
F3ra
1317Heist et al MRA Analysis of the LAA
hronic AF, including variability in LAA volume, neckimensions, and depth. Second, there are large differencesn LAA neck shape and in the ratio of neck size to depthmong these patients. Third, there is a significant correlationetween LA size and LAA neck dimensions in both thehort and long axis. Fourth, several morphologic variants ofhe LAA have been identified, including variability in theumber of major LAA lobes and in the general structure ofhe LAA body and neck. Given this heterogeneity in LAAize and morphology, it is possible that a “one size fits all”pproach to the LAA with regard to cardiac procedures andarticularly device occlusion of the LAA may not be opti-al for all patients.Surgical ligation of the LAA has been performed for
any years in patients with AF in conjunction with otherardiac surgical procedures, such as the maze procedure anditral valve surgery.7 Percutaneous catheter ablation now is
n established alternative to the surgical maze for treatmentf AF.8 Similarly, percutaneous catheter-based devices thatan exclude the LAA from the systemic circulation andhereby potentially prevent thromboembolism and strokessociated with AF are being investigated.5,6 Although pre-
A
Left Atrium
LAA
Left Atrium
LAA
LAA Neck
LAA Neck
B
igure 4 Variations in left atrial appendage (LAA) neck geometry.-dimensional magnetic resonance angiographic reconstructions of twoepresentative LAA structures (with a small amount of adjoining lefttrium) demonstrate a narrow LAA neck (A) and a broad LAA neck (B).
rocedural assessment of LAA dimensions is unlikely to be d
rucial for success at open surgical ligation of the LAA, its likely to be of greater importance for assessment ofatients for intravascular LAA occlusion devices as well asevice sizing and selection.
A detailed understanding of a given patient’s LAA sizend geometry may prove important in selecting and sizingevices for LAA occlusion, although compliance of bothhe LAA itself and the occluder devices may allow for someexibility in device sizing. As described previously withegard to interpatient variability in the pulmonary venousnatomy,1,2 in this study we report that there is also sub-tantial variability in the dimensions and anatomy of theAA. Although transesophageal echocardiography can ef-
ectively image the LAA and provide real-time imaging ofhe LAA during placement of occlusion devices, currentransesophageal echocardiography imaging provides onlywo-dimensional images of the LAA, which can result inmperfect estimation of the size and geometry of this struc-ure due to foreshortening and limited echo planes. Most ofhe published literature on transesophageal echocardio-raphic assessment of the LAA has focused on the presencef thrombus rather than a detailed assessment of LAA sizend morphology.3,9
MRA and computed tomographic (CT) imaging allowor precise 3D reconstruction of structures such as the LAA,hich may prove complementary to intraprocedural trans-
sophageal echocardiographic data in selecting and sizingcclusion devices.10,11 Preprocedural MRA and CT imagingf the LA and pulmonary veins now is used in conjunctionith other imaging modalities to direct catheter ablation ofF in many centers. Published reports on the use of MRA
nd CT for assessing the LAA have focused primarily onhe identification of LAA thrombus.12–14 In this study, werovide a detailed assessment by MRA documenting sig-ificant interpatient variability in LAA size and geometryrom a series of patients with AF who are likely to havelinical characteristics similar to those of patients who maye candidates for LAA device occlusion.
tudy limitationshe patients composing this study are a consecutive seriesf patients with chronic AF undergoing cardiac MRA inreparation for catheter ablation of AF. This group mayiffer from patients who may be selected for initial trials ofevice closure of the LAA (generally AF patients withstablished risk factors for stroke). None of the patients inhis study have undergone device closure of AF, so it is notlear whether the LAA dimensions defined by MRA willmprove the safety and efficacy of device closure of theAA when combined with more established techniquesuch as transesophageal echocardiography. In this study,AA depth as defined reflects a maximal direct depth, and,epending on the shape of the occluder device, this mea-ured depth may not be fully accessible to some occluder
evices. It also is not yet proven whether the LAA dimen-
scv
CTwmiMii
R 1
1
1
1
1
1318 Heart Rhythm, Vol 3, No 11, November 2006
ions described in this study are static or whether they mayhange substantially over time and with changes in intra-ascular volume and LA filling pressure.
onclusionhere are significant differences in LAA size and geometryith regard to LAA volume, neck dimensions, depth, andorphology among the patients in this study. Given the
ncreasing interest in device occlusion of the LAA, 3DRA analysis of LAA structure may prove useful for guid-
ng the appropriate selection and sizing of occlusion devicesn the preprocedural setting.
eferences1. Wittkampf FH, Vonken EJ, Derksen R, Loh P, Velthuis B, Wever EF, Boersma
LV, Rensing BJ, Cramer MJ. Pulmonary vein ostium geometry: analysis bymagnetic resonance angiography. Circulation 2003;107:21–23.
2. Mansour M, Holmvang G, Sosnovik D, Migrino R, Abbara S, Ruskin J, KeaneD. Assessment of pulmonary vein anatomic variability by magnetic resonanceimaging: implications for catheter ablation techniques for atrial fibrillation.J Cardiovasc Electrophysiol 2004;15:387–393.
3. Zabalgoitia M, Halperin JL, Pearce LA, Blackshear JL, Asinger RW, Hart RG.Transesophageal echocardiographic correlates of clinical risk of thromboembo-lism in nonvalvular atrial fibrillation. Stroke Prevention in Atrial Fibrillation IIIInvestigators. J Am Coll Cardiol 1998;31:1622–1626.
4. Shinokawa N, Hirai T, Takashima S, Kameyama T, Nakagawa K, Asanoi H,Inoue H. A transesophageal echocardiographic study on risk factors for stroke in
elderly patients with atrial fibrillation: a comparison with younger patients.Chest 2001;120:840–846.5. Sievert H, Lesh MD, Trepels T, Omran H, Bartorelli A, Della Bella P, Nakai T,Reisman M, DiMario C, Block P, Kramer P, Fleschenberg D, Krumsdorf U,Scherer D. Percutaneous left atrial appendage transcatheter occlusion to preventstroke in high-risk patients with atrial fibrillation: early clinical experience.Circulation 2002;105:1887–1889.
6. Nakai T, Lesh MD, Gerstenfeld EP, Virmani R, Jones R, Lee RJ. Percutaneousleft atrial appendage occlusion (PLAATO) for preventing cardioembolism: firstexperience in canine model. Circulation 2002;105:2217–2222.
7. Gillinov AM, Wolf RK. Surgical ablation of atrial fibrillation. Prog CardiovascDis 2006;48:169–177.
8. Oral H, Pappone C, Chugh A, Good E, Bogun F, Pelosi F, Bates ER, LehmannMH, Vicedomini G, Augello G, Agricola E, Sala S, Santinelli V, Morady F.Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N EnglJ Med 2006;354:934–941.
9. Donal E, Yamada H, Leclercq C, Herpin D. The left atrial appendage, a small,blind-ended structure: a review of its echocardiographic evaluation and itsclinical role. Chest 2005;128:1853–1862.
0. Beygui F, Cluzel P, Montalescot G. Multimodality imaging of percutaneousclosure of the left atrial appendage. Eur Heart J 2005;EHI:527.
1. Mohrs OK, Schraeder R, Petersen SE, et al. Percutaneous left atrial appendagetranscatheter occlusion (PLAATO): planning and follow-up using contrast-enhanced MRI. AJR Am J Roentgenol 2006;186:361–364.
2. Ohyama H, Hosomi N, Takahashi T, Mizushige K, Osaka K, Kohno M, KoziolJA. Comparison of magnetic resonance imaging and transesophageal echocar-diography in detection of thrombus in the left atrial appendage. Stroke 2003;34:2436–2439.
3. Jaber WA, White RD, Kuzmiak SA, Boyle JM, Natale A, Apperson-Hansen C,Thomas JD, Asher CR. Comparison of ability to identify left atrial thrombus bythree-dimensional tomography versus transesophageal echocardiography in pa-tients with atrial fibrillation. Am J Cardiol 2004;93:486–489.
4. Mohrs OK, Nowak B, Petersen SE, Welsner M, Rubel C, Magedanz A, Kauczor
HU, Voigtlaender T. Thrombus detection in the left atrial appendage using contrast-enhanced MRI: a pilot study. AJR Am J Roentgenol 2006;186:198–205.