-
ANALGESIA PRESCRIBINGYear 4 Prescribing Tutorial 2019 – 2020
Disclaimer: All cases are fictional for teaching purposes
-
ResourcesGolden rules of prescription
writinghttp://intranet.lothian.scot.nhs.uk/NHSLothian/Healthcare/ClinicalGu
idance/Documents/Golden%20rules%20for%20prescribing.pdf
BNF http://www.bnf.org/ Also BNF App
Lothian Joint Formulary Also LJF
Apphttp://www.ljf.scot.nhs.uk/Pages/default.aspx
NHS Lothian pain medicine
guidancehttp://intranet.lothian.scot.nhs.uk/NHSLothian/Healthcare/A-
Z/PainMedicine/Pain%20management/Pages/default.aspx
http://intranet.lothian.scot.nhs.uk/NHSLothian/Healthcare/ClinicalGuidance/Documents/Golden%20rules%20for%20prescribing.pdfhttp://www.bnf.org/http://www.ljf.scot.nhs.uk/Pages/default.aspxhttp://intranet.lothian.scot.nhs.uk/NHSLothian/Healthcare/A-Z/PainMedicine/Pain%20management/Pages/default.aspx
-
GOLDEN RULES OF PRESCRIBING (I)
Select correct prescription chart (14 day ± warfarin chart)
Write clearly in block CAPITALS using a black ballpoint pen
Complete all the required patient details on the front
Use generic names for drugs where possible and appropriate
Write drug dose clearly; remember only g, mg and ml are
acceptable abbreviations
Select route of administration
-
GOLDEN RULES OF PRESCRIBING (II)
Enter correct start date (use original start date when
rewriting)
Remember the once only section
Sign and print your name
Enter supplementary charts in use
Never alter prescriptions (cancel and rewrite)
Discontinue prescriptions correctly
-
LEARNING OUTCOMES
Describe the mode of action of common pain medicines.
List the factors to consider when managing pain.
Describe the WHO pain ladder and apply it to clinical
scenarios.
List side effects of common pain medications.
-
WHAT IS PAIN?
“An unpleasant sensory and emotional experience associated with
actual or potential tissue damage, or described in terms of such
damage”
Pain management is one of the most commonly encountered
prescribing scenarios for the junior doctor.
-
PAIN PATHWAY
Tissue injury
Sensitising prostaglandins
Nocioceptoractivation
Peripheral nerves
-
WHAT ANALGESICS CAN YOU THINK OF?
Common:ParacetamolIbuprofenCodeineMorphine
Less common, but still used :
Nefopam
Tramadol
Co-dydramol
Buprenorphine
Diamorphine
Dihydrocodeine
Methadone
Fentanyl
Oxycodone
-
COMMON ANALGESICS
Paracetamol
NSAIDs (e.g. aspirin, ibuprofen)
Morphine (and other opiates)
Local anaesthetic (e.g. lidocaine)
-
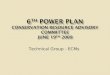
PAIN PATHWAY
Tissue injury
Sensitisingprostaglandins
Nocioceptoractivation
Peripheral nerves
NSAIDsLocal
AnaestheticsOpiates Paracetamol
Opiates
-
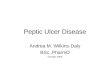
PAIN LADDER
-
Acute Pain Assessment
Verbal numeric rating scale
0----------------------10
No pain-----worst pain
Verbal descriptor scale
0 =no pain 1=mild pain undistressing 2=moderate pain,
distressing 3= severe pain, very
distressing
-
Pain Assessment--Treatment
Mild pain0-3
Moderate pain3-6
Severe pain6-10
No interventionParacetamolMild opioid eg codeine
Give rescue analgesiaParacetamol +/-NSAIDStrong opioid regular
and as reqd.
Urgent rescue analgesia (iv morphine)
Paracetamol +/-NSAIDStrong opioid regular and as reqd.
-
CASE 1A 30 year old male comes into A&E and you are the FY
doctor who sees him first. He had been playing football, but fell
awkwardly and his right ankle is now swollen and painful.
What is your initial management plan?
-
CASE 1Analgesia
Whilst examination and investigations are important in reaching
a diagnosis, the most important issue at the moment is pain
relief.
What do you need to know before you prescribe?o Drug Allergieso
Has he taken any medication at homeo Past Medical History (esp.
asthma, PUD, liver disease,
renal failure) and regular medicationso Any vomiting?
-
CASE 1
Oral therapy is usually the preferred choice if adequate
analgesia can be achieved via this route.
IV access is not risk-free, so risks should be balanced against
benefits.
Some analgesics can be given IM – removing the need for a
cannula in someone who is not going to be admitted to hospital.
-
CASE 1The patient has an x-ray which does not demonstrate any
fracture, however 6 months later is still suffering from some joint
pain around his ankle.
He is still regularly taking paracetamol and ibuprofen, which he
is buying over the counter.
He presents to A&E once more, this time with epigastricpain
and vomiting.
o What is the most likely diagnosis?
o What could have been prescribed to prevent this happening?
-
NSAIDSGood for MSK pain as they act in the tissue to limit the
production of PGs which sensitise nocioceptors; they also serve as
anti-inflammatory agents.
However, side effects include gastritis and peptic ulceration,
and therefore it is important to be careful when using them long
term.
They should be taken after food to prevent GI upset, and
consideration could be given to co-prescription of a
gastro-protective drug (e.g. PPI).
A topical NSAID may be an option
-
CASE 2A 60 year old man on the orthopaedic ward develops
abdominal pain. It is shearing in nature and radiates through to
his back. It is very severe – pain 9/10.He had a MI 2 years
ago.
What do you do?
-
CASE 2Observations:o Hypotensive 90/60 mmHgo HR 140 bpmo RR 28o
O2 sats 95% on air.o Temp 37.5 oC
HS I+II+0, chest clear. Radial pulse thready in character.
Peripheral pulses not palpable.
Abdomen is peritonitic.
What would you like to do?
-
CASE 2GET HELP!
ABCDE
Oxygen
IV access (2 large gauge cannulae)
Urgent bloods, including crossmatch
Analgesia
-
CASE 2 Pain can be an important indicator that something is
going wrong.
It is especially important to assess the patient who complains
of a new type of pain in hospital, rather than blindly prescribing
analgesia and waiting until the ward round the next day to discover
that they’ve ruptured their aorta...
-
CASE 3You are the FY1 on HAN and have just been called to see a
60 year old woman was admitted for an elective laparoscopic
cholecystectomy. The procedure proceeded without any problems.
However, she is now complaining of abdominal pain.
What do you do?
-
CASE 3She is now 8 hours post-op and has a history of gallstones
and cholecystitis.
Her abdomen is soft, and is only tender around the
RUQ/epigastrium. Observations are stable, and she does not look
acutely unwell.
You look at her Prescription chart and note that she has had 1g
of paracetamol and 50mg of tramadol in the last 3 hours.
What do you do?
-
CASE 3You prescribe IV morphine.
The nursing staff are busy, so you have to give it yourself.
Sadly while you are documenting in the prescription chart that
you’ve given the drug, the patient starts to feel sick. She then
proceeds to vomit, covering both herself and you.
What should you have done?
-
CASE 3Nausea and vomiting is a major side effect of opiates, and
is a particular problem post-operatively.
Always ensure that you prescribe an antiemetic when giving
morphine for the first time to a patient.
-
ANTIEMETICSCyclizine (Antihistamine)o Good in GI obstruction
& post-operative nausea and vomitingo Side-effects include
tachycardia and constipation
Metoclopramide (Prokinetic, D2 agonist)o Good for GI causes of
vomiting, migraine and nausea in
response to drugs (e.g. opiates).o AVOID IN OBSTRUCTION.o
MHRA/CHM advice in BNF
Ondansetron (5HT3 antagonist)o Good for severe/resistant nausea
post-operatively or related
to chemotherapy.o Particular use in nausea related to
chemotherapy
-
CASE 3 Different patients will have different levels of pain
following the same procedure and therefore will require
differing levels of analgesia.
It is important to assess each patient in order to ensure that
they are not becoming acutely unwell, and then to ensure that they
have adequate analgesia.
-
CASE 3It is now several hours since you first saw the 60 year
old lady, but again the nursing staff call you with a problem. Now
she has become unresponsive.
What are you thinking about as you walk to the ward?
-
CASE 3You find the patient slumped in her bed. She does not
respond to pain. Her RR is 5 and her pupils are pinpoint.
You look at her prescription chart and realisethat you
accidentally prescribed the IV morphine without a frequency and the
patient has been getting IV morphine every hour.
What’s going on?
-
SIGNS OF OPIATE TOXICITYMild-moderate:o Hypotensiono
Bradycardiao Altered consciousness levelo Myoclonus
Severe:o Respiratory depressiono Pupillary constriction
“pin-point pupils”o Coma
Treatment?
-
CASE 3You give naloxone and the patient comes round. You
document this in the notes, and stop the regular morphine on the
prescription chart.
However, 45 min later, you are called again by nursing staff as
the patient has once again become unresponsive...
Why?
-
CASE 3Naloxone has a shorter half-life than morphine. Therefore,
depending on how much morphine the patient has onboard, one dose of
naloxone may not be enough.
Treatment of opiate toxicity may require a naloxone
infusion.
-
OTHER SIDE EFFECTS OF OPIATES
Constipation
Dependence
Tolerance
Difficult with micturition/urinary retention
-
OTHER DOS AND DONTS!DO!Prescribe regular analgesia and
break-thoughStart low and titrate upwards, particularly with
morphineBe aware that analgesics can precipitate deliriumSeek
advice from the Acute/Chronic Pain Teams
DO NOT!Prescribe NSAIDs to anyone on an ACEi/ARB, or
AKI/CKDPrescribe metoclopramide for young femalesPrescribe tramadol
for patients with dementia Prescribe nefopam to anyone with normal
renal function
-
THE END
Any questions?
We would appreciate if you could take the time to complete a
feedback form, this will help us to ensure that the tutorials are
worthwhile, and allow us to improve them for future year
groups.
Thank you!
Analgesia PrescribingResourcesGOLDEN RULES OF PRESCRIBING
(I)GOLDEN RULES OF PRESCRIBING (II)LEARNING OUTCOMESWhat is
Pain?Pain pathwayWhat analgesics can you think of?Common
AnalgesicsPain pathwayPain ladderAcute Pain AssessmentPain
Assessment--TreatmentCase 1Case 1Case 1Slide Number 17Case 1Slide
Number 19NSAIDsCase 2Case 2Case 2Case 2Case 3Case 3Slide Number
27Case 3Slide Number 29Case 3AntiemeticsCase 3Case 3Case 3Signs of
opiate toxicityCase 3Case 3Other side effects of opiatesOther Dos
and DONTs!The End