Embed Size (px)
Citation preview
Pharmacology of analgesiapain :An unpleasant sensory or emotional experience associated with actual
or potential tissue damage, or described in terms of such damage. Pain is
always subjective. Each individual learns the application of the word
through experiences related to injury in early life. It is unquestionably a
sensation in a part of the body, but it is also unpleasant, and therefore
also an emotional experience. Many people report pain in the absence of
tissue damage or any likely pathophysiological cause; usually this happens
for psychological reasons. There is no way to distinguish their experience
from that due to tissue damage, if we take this subjective report……
• Universal, complex, subjective experience
• Number one reason people take medication
• Generally is related to some type of tissue damage and serves as a warning signal
Scope of the Problem• Increases as Baby Boomers age• 25 million people suffer acute pain related to surgery or
injury• Chronic pain affects 250 million Americans• Is a multibillion dollar industry• Much ignorance exists about this complaint
Gate control theory of pain is the idea that physical pain is not a direct result of
activation of pain receptor neurons, but rather, its perception is modulated by interaction between different neurons
Nerve fibers (A delta (fast channels)) and C fibers (slow channels) transmit pain impulses from the periphery
Gate Control Theory of Pain
• Gate control theory of pain is the idea that physical pain is not a direct result of activation of pain receptor neurons, but rather, its perception is modulated by interaction between different neurons
• Impulses are intercepted in the dorsal horns of the spinal cord, the substantia gelatinosa.In this region, cells can be inhibited or facilitated to the T-cells (trigger cells)
• Similar gating mechanisms exist in the nerve fibers descending from the thalamus and the cortex. These areas of the brain regulate thoughts and emotions. Thus, with a pain stimulus, one’s thoughts and emotions can actually modify the pain experience.
• Nociceptive—free nerve endings that receive painful stimuli• Neuropathic –damaged nerves
Pathophysiological Response
• Tissue damage activates free nerve endings (nociceptors) of peripheral nerves
• Pain signal is transmitted to the spinal cord, hypothalamus, and cerebral cortex
• Pain is transmitted to spinal cord by A-delta fibers and C fibers
• A-delta fibers transmit fast, sharp, well-localized pain signals
• C fibers conduct the pain signal slowly and produce poorly localized, dull, or burning type of pain
• Thalamus is the relay station for incoming stimuli, incl. pain
Pain Fibers and Pathways
• A delta fibers found in the skin and muscle, myelinated, respond to mechanical stimuli. Produce intermittent pain.
• C fibers distributed in the muscle as well as the periosteum and the viscera. These fibers are unmyelinated, conduct thermal, chemical and strong mechanical stimuli. Produce persistent pain.
Inhibitory and Facilitatory Mechanisms
• Neurotransmitters—chemicals that exert inhibitory or excitatory activity at post-synaptic nerve cell membranes. Examples include: acetylcholine, norepinehprine, epinephrine, dopamin, and serotonin.
• Neuromodulators—endogenous opiates. Hormones in brain. Alpha endorphins, beta endorphins and enkephalins. Help to relieve pain.
• Physiology of analgesiaPain sensation
First pain:sharp, pricking, well defined,A fibers
Second pain:dull, aching, poorly localized, C fibers
Types and reasonsNeuropathic painInflammatory painBone cancer painFibromyalgiaMigrainePsychogenic pain
• NSAIDs and other anti-inflammatory drugs• Opiates and morphinomimetics• Some tricyclic antidepressants• Some antiepileptic drugs• Local anesthetics• Others: ketamine, mexiletine, etc
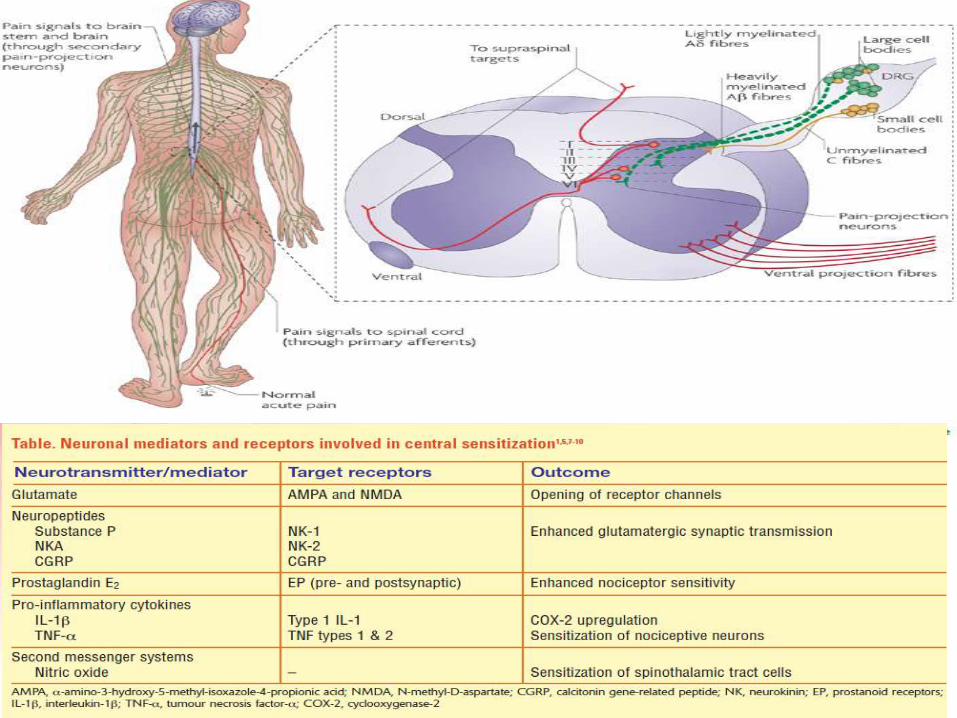
Milligan et al, 2009
• Pharmacologic classes and agents for analgeisa
Types and reasonsNeuropathic painInflammatory painBone cancer painFibromyalgiaMigrainePsychogenic pain
• NSAIDs and other anti-inflammatory drugs• Opiates and morphinomimetics• Some tricyclic antidepressants• Some antiepileptic drugs• Local anesthetics• Others: ketamine, mexiletine, etc
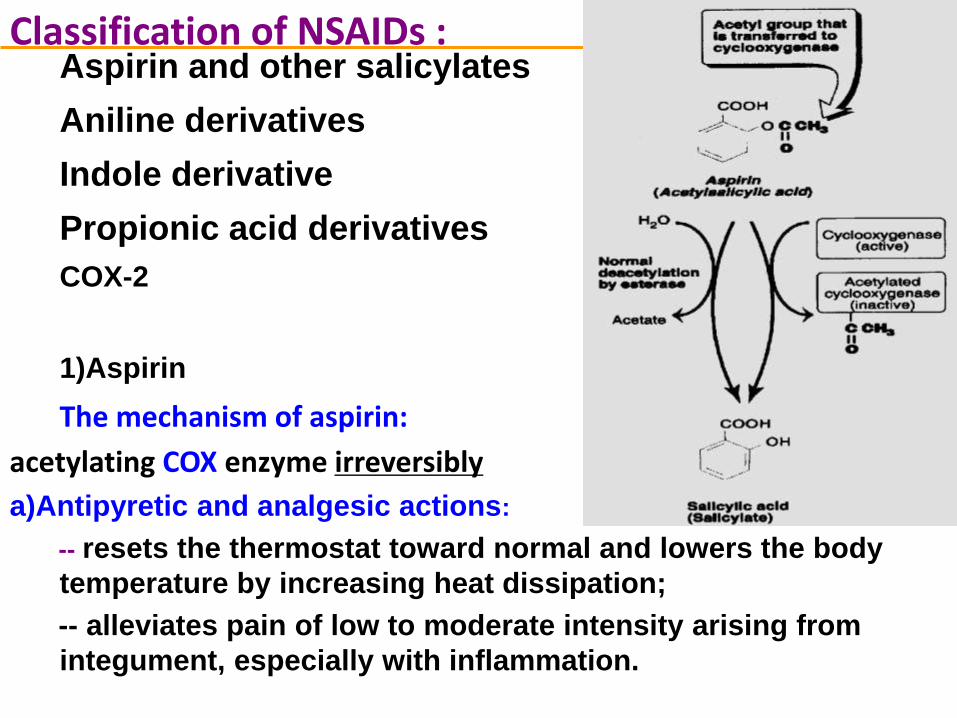
Aspirin and other salicylates
Aniline derivatives
Indole derivative
Propionic acid derivatives
COX-2
1)Aspirin
The mechanism of aspirin:
acetylating COX enzyme irreversibly
a)Antipyretic and analgesic actions:
-- resets the thermostat toward normal and lowers the body
temperature by increasing heat dissipation;
-- alleviates pain of low to moderate intensity arising from
integument, especially with inflammation.
Classification of NSAIDs :
B Anti-rheumatic actions: at large dose (4-6 g/d).
C Anti-aggregation of platelets and
vasoconstriction: at small dose (~100 mg/d),
irreversibly inhibits thromboxane production in
platelets without markedly affecting PGI2 in the
endothelial cells of the blood vessel.
Indications for Use
• Treat mild to moderate pain or inflammation
• Musculoskeletal disorders; HA; dysmenorrhea, minor trauma and surgery
• Low dose ASA for risk of MI or stroke
• Celebrex is indicated for familial polyposis
1. Aspirin :Actions and therapeutic uses continued:
Adverse effects:
Gastrointestinal effects: epigastric distress, nausea and
vomiting, bleeding, ulcer. Allergic effects: Urticaria
Bronchoconstriction (aspirin asthma), angioneurotic edema
Prolonged bleeding time
Excessive ventilation: respiratory alkalosis
Salicylism :toxicity in the CNS (headache, dizziness, nausea,
vomiting, tinnitus)
Reye’s syndrome: liver and brain injury in children with
virus infection
Acetaminophen:Slow and prolonged antipyretic and
analgesic effects.No obvious anti-inflammation effect
• Less stimulation to gastrointestinal tract
Damage of liver and kidney if used for a long time and at high
dose
Acetaminophen• Equal in effectiveness to ASA in analgesic and antipyretic
effects• Lacks anti-inflammatory actions• Ethanol induces drug-metabolizing enzymes in liver. Resulting
rapid metabolism of acetaminophen produces enough toxic metabolite to exceed glutathione. Need glutathione to inactivate toxic metabolites.
• Toxicity occurs with 20g or more. • Creates toxic metabolite that is inactivated by glutathione.• OD supply of glutathione is depleted and toxic metabolite
damages liver cells• Not to exceed 4g/day• Treatment—gastric lavage, charcoal, antidote is Mucomyst
(acetylcysteine). Provides cysteine, a precursor to glutethione.
Indomethacin• Used for ankylosing spondylitis ,
• Osteoarthritis and gout
• Effective in treating patent ductus arteriosus
• High incidence of adverse effects like:
central nervous system effect
gastrointestinal complaints
allergic reactions
hematopoietic reactions
• Sulindac and Etodolac are less toxic and used for OA, RA,
SA and acute gout.
Propionic acid derivatives
• Anti-inflammatory, analgesic and antipyretic activity
• Less gastrointestinal effects
• Change platelet function and prolong bleeding time
• Used for the treatment of various arthritis and
dysmenorrhea
Inhibitors of TNF-
• TNF- is the predominant factor in inflammatory
reaction.
• Include infliximab, adalimumab and IgG1
• Used for the treatment of rheumatoid arthritis,
spondylitis ankylosans and other autoimmune
diseases.
Drugs used in Gout and Hyperuricemia
• Zyloprim (allopurinol)—prevents or treats hyperuricemia• Uric acid is formed by purine metabolism and an enzyme xanthine
oxidase. Allopurinol prevents formation by inhibiting xanthineoxidase.
• Colchicine—used to treat or prevent acute attacks of gout. Drug of choice for acute attacks. Decreases inflammation by affecting leukocytes.
• Benemid (probenecid) increases urinary excretion of uric acid. Not effective in acute attacks.
• Anturane (sulfinpyrazone) uricosuric similar to Benemid. Not for acute attacks.
Guidelines for Treating Gout• Maintenance drugs are Zyloprim, Benemid and Anturane• Colchicine needed for several weeks to prevent acute attacks while
serum levels are being lowered• Need high fluid intake, alkaline urine to prevent renal calculi
Drugs Used for Migraines• Selective serotonin 5-HT1 receptor agonists• Increase serotonin in the brain• Constrict blood vessels• Contraindicated in patient’s with history of MI,, angina,
uncontrolled htn.
• Drugs vary in onset with sub q sumatriptan acting the most rapidly and starting within 10 minutes; most clients get relief within 1-2 hours
• Drugs are metabolized in the liver by monoamine oxidase or by cytochrome p450 enzymes; sub q administrations causes more adverse effects than the oral drugs
• Ergotamine tartrate—ergot alkaloid used only in tx of migraine• Work by constricting blood vessels• Most effective when given sublingual or by inhalation• Contraindicated in pregnancy, htn, PVD, CAD, renal or hepatic
disease and even in severe infections
Guidelines for Treating Migraine• Start out with acetaminophen, aspirin, or other
NSAIDs
• Moderate to severe migraines, sumatriptan or other related drugs are useful
• For severe and frequent migraines, prophylaxis is indicated. Use ASA and NSAIDs.
• For menstrual migraines, start tx one week before and during menses
• Other drugs indicated for tx include beta adrenergic blocking agents such as Inderal
Guidelines for Treating Arthritis• Control pain and inflammation
• Rest, exercise,and PT
• Osteoarthritis—COX1, COX2, glucosamine, intraarticular injections of corticosteroids or hyaluronic acid (Synvisc) to act as shock absorber
Rheumatoid Arthritis
• NSAIDs
• Corticosteroids
• Immunosuppressants—methotrexate
• Enbrel, Remicade and Arava. Affect tumor necrosis factor and other cytokines.
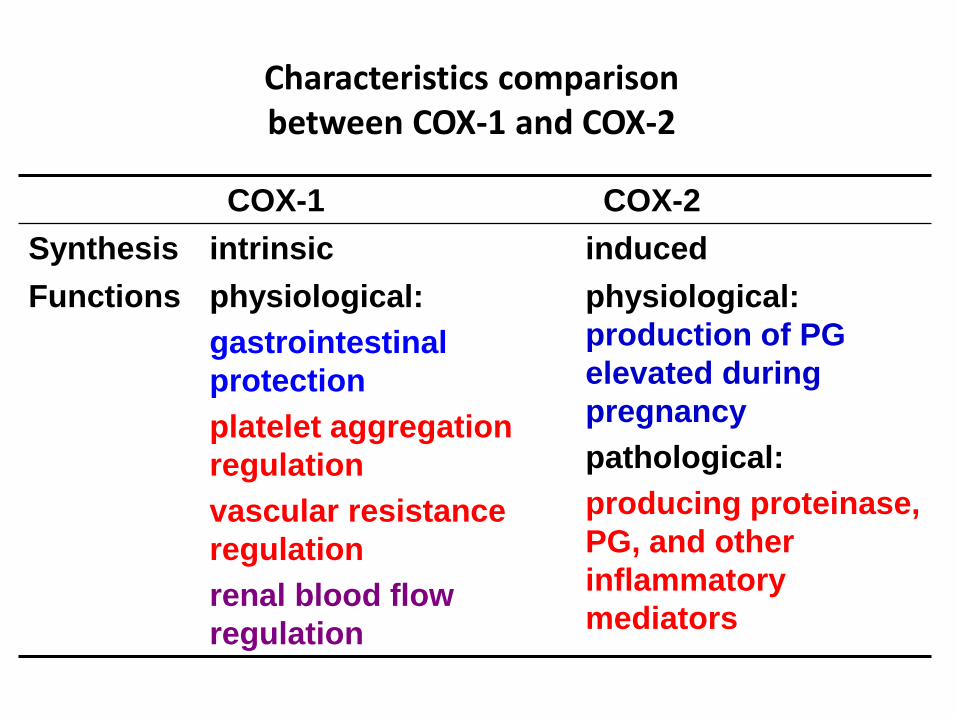
COX-1 COX-2
Synthesis intrinsic induced
Functions physiological:
gastrointestinal
protection
platelet aggregation
regulation
vascular resistance
regulation
renal blood flow
regulation
physiological:
production of PG
elevated during
pregnancy
pathological:
producing proteinase,
PG, and other
inflammatory
mediators
Characteristics comparison between COX-1 and COX-2
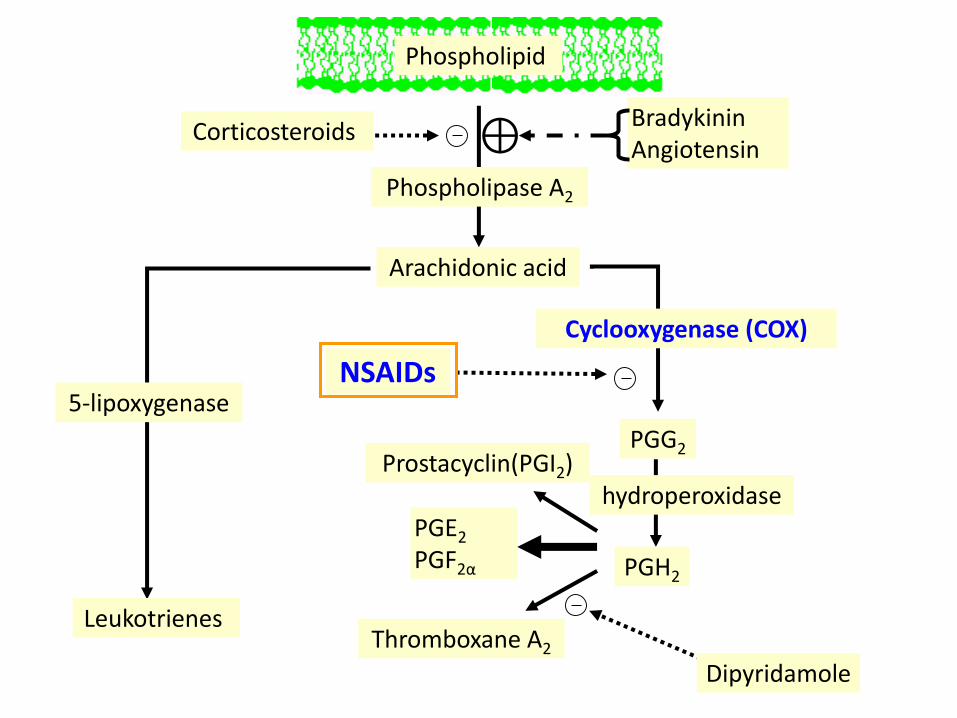
Arachidonic acid
Phospholipase A2
Corticosteroids ⊕BradykininAngiotensin
Cyclooxygenase (COX)
PGG2Prostacyclin(PGI2)
PGE2
PGF2α
Thromboxane A2
Dipyridamole
hydroperoxidase
NSAIDs
Leukotrienes
5-lipoxygenase
Phospholipid
PGH2
Contraindications to Use• PUD
• GI or bleeding disorders
• Hypersensitivity reactions
• Impaired renal function
• If allergic to ASA
• In children, ASA contraindicated in presence of viruses=Reye’s syndrome
• Celebrex if allergic to sulfonamides
Reye’s
• Seen in children under 15 after an acute viral illness
• Results in encephalopathy, fatty infiltration of the liver, pancreas, kidneys, spleen, and lymph nodes
• Toradol not used in labor & delivery/during any major surgery
• OTC preps contraindicated in alcoholics due to possible liver damage
Aspirin (ASA)• Home remedy for headaches, colds, influenza and other
respiratory infections• For fever,For inflammation• ASA and COX 2 are ok, COX 2 have little effect on platelet function
• Poisoning can occur with large doses. Saturate the metabolic pathway, slow elimination and cause drug accumulation
• If overdose, measure serum levels• Recognize s/s: N/V, fever, fluid and lyte deficiencies, tinnitus,
decreased hearing, hyperventilation, confusion, visual changes>>>>delirium, stupor and coma
ASA salicylism• Gastric lavage• Activated charcoal• IV bicarbonate so more rapid excretion• hemodialysis
NSAIDS• Propionic acid derivatives such as ibuprofen,
ketoprofen (Orudis), naproxen and fenoprofen(Nalfon)
Acetic acid derivatives include indomethacin (Indocin), sulindac (Clinoril) and tolmetin(Tolectin)---these drugs have more severe adverse reactions than the proprionic acid derivatives
Prostaglandins important in:
1. Protection of kidneys and stomach
2. Regulate vascular tone and platelets in CV system
NSAIDS• IV indomethacin is approved for the tx of patent ductus arteriosus
in premature infants.• Remember: patent ductus is a communication between the
pulmonary artery and the aorta
• Toradol (ketoralac) is used only for pain. Is the only NSAID that can be given by injection. Use limited to 5 days as can cause bleeding.
• Oxicam drugs include Mobic (meloxacam) and Feldene (piroxicam)• Celebrex (celecoxib)• Affect bleeding only while drug is still in the system
Effects of Nonsteroidals on Other Drugs• Decrease effects of ACEI, beta blockers and diuretics• Affect sodium and water retention• Inhibit renal prostaglandin synthesis
Natural opiates: morphine, codeine, papaverine and thebaine;
Semi-synthetic opiates: hydromorphone, hydrocodone, oxycodone,
oxymorphone, desomorphine, diacetylmorphine (Heroin),
nicomorphine, dipropanoylmorphine, benzylmorphine and
ethylmorphine;
Fully synthetic opioids: fentanyl, pethidine, methadone, tramadol
and propoxyphene;
Endogenous opioid peptides: endorphins, enkephalins,
dynorphins, and endomorphins.
Classification of opiates
Opioid receptors
Distribution and physiological effects:
Certain cells in the CNS:
Brainstem: mediate respiration, cough, nausea and vomiting, maintain blood pressure, pupillarydiameter and control of stomach secretions.
Medial thalamus: modulate deep pain that is poorly localized and emotionally influenced.
Spinal cord: involved in the reception and integration of incoming sensory information and attenuate painful afferent stimulation.
Hypothalamus: affect neuroendocrine secretion.
Limbic system: influence emotional behavior.
Distribution and physiological effects:
Periphery:
--- Inhibit the release of excitatory, proinflammatorysubstances from nerve endings, which contribute to the anti-inflammatory effect of opioids.
Immune cells: immune depression
Morphine and most other clinically used opioid agonists exert their effects through m opioid receptors. These drugs affect a wide range of physiological systems. They produce analgesia, affect mood and rewarding behavior , and alter respiratory, cardiovascular, gastrointestinal, and neuroendocrine function. d Opioid receptor agonists also are potent analgesics in animals, and in some cases they have proved useful in humans
Opioid receptors
• Opioids have been the mainstay of pain treatment for thousands of years, and they remain so today. Opioids such as heroin and morphine exert their effects by mimicking naturally occurring substances, called endogenous opioid peptides or endorphins.
Much now is known about the basic biology of the endogenous opioidsystem and its molecular and biochemical complexity, widespread anatomy, and diversity.
The diverse functions of this system include the best known sensory role, prominent in inhibiting responses to painful stimuli; a modulatory role in gastrointestinal, endocrine, and autonomic functions; an emotional role, evident in the powerful rewarding and addicting properties of opioids; and a cognitive role in the modulation of learning and memory
The word opium is derived from opos, the Greek word for "juice," the drug being derived from the juice of the opium poppy, Papaversomniferum.
• Three distinct families of classical opioid peptides have been identified: the enkephalins, endorphins, and dynorphins.
• Each family derives from a distinct precursor protein and has a characteristic anatomical distribution. These precursors, prepro-opiomelanocortin (POMC), preproenkephalin, and preprodynorphin, respectively, are encoded by three corresponding genes.
• The major opioid peptide derived from POMC is b-endorphin. Although b-endorphin contains the sequence for met-enkephalinat its amino terminus, it is not converted to this peptide; met-enkephalin is derived from the processing of preproenkephalin.
• In addition to b-endorphin, the POMC precursor also is processed into the nonopioid peptides adrenocorticotropic hormone (ACTH), melanocyte-stimulating hormone (a-MSH), and b-lipotropin (b-LPH). Previous biochemical work had suggested a common precursor for the stress hormone ACTH and the opioid peptide b-endorphin.
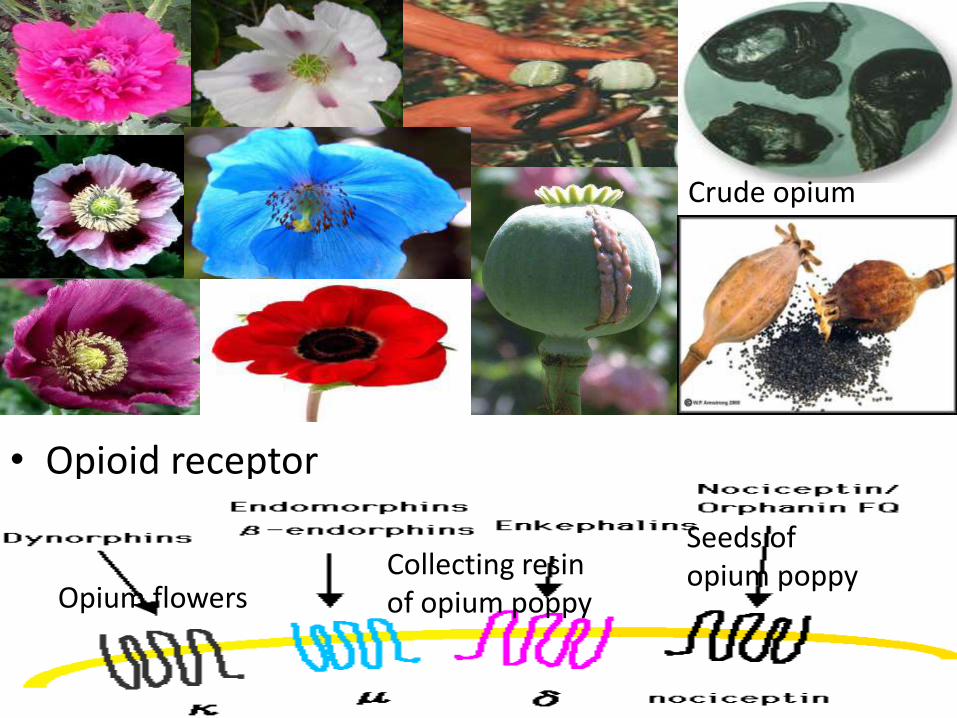
• Opioid receptor
Collecting resin of opium poppy
Crude opium
Opium flowers
Seeds of opium poppy
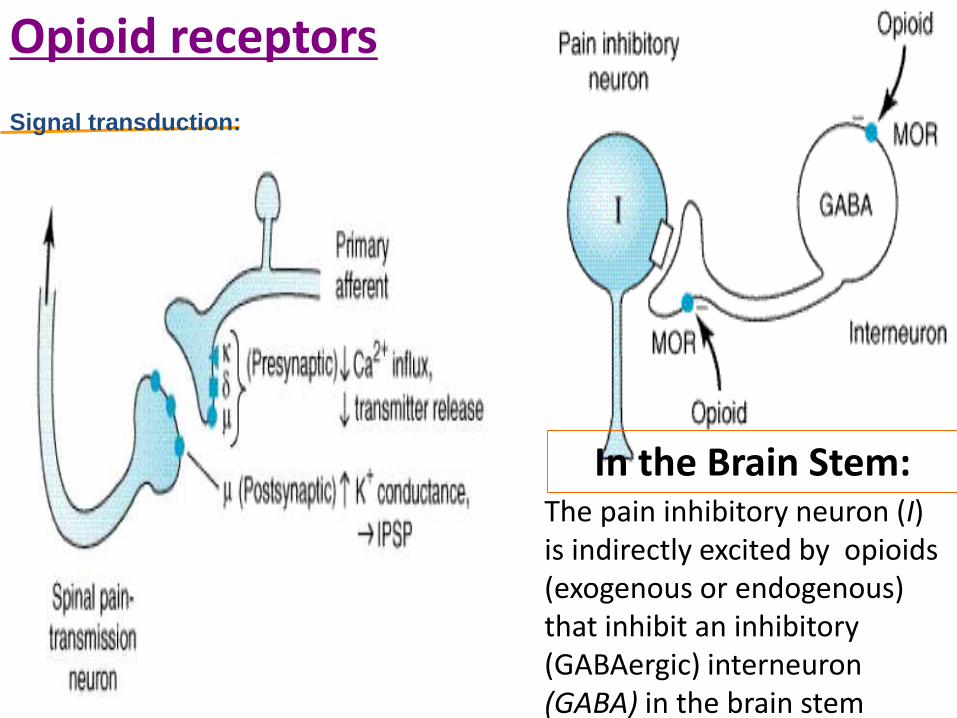
In the Brain Stem:
Opioid receptors
Signal transduction:
The pain inhibitory neuron (I) is indirectly excited by opioids(exogenous or endogenous) that inhibit an inhibitory (GABAergic) interneuron (GABA) in the brain stem
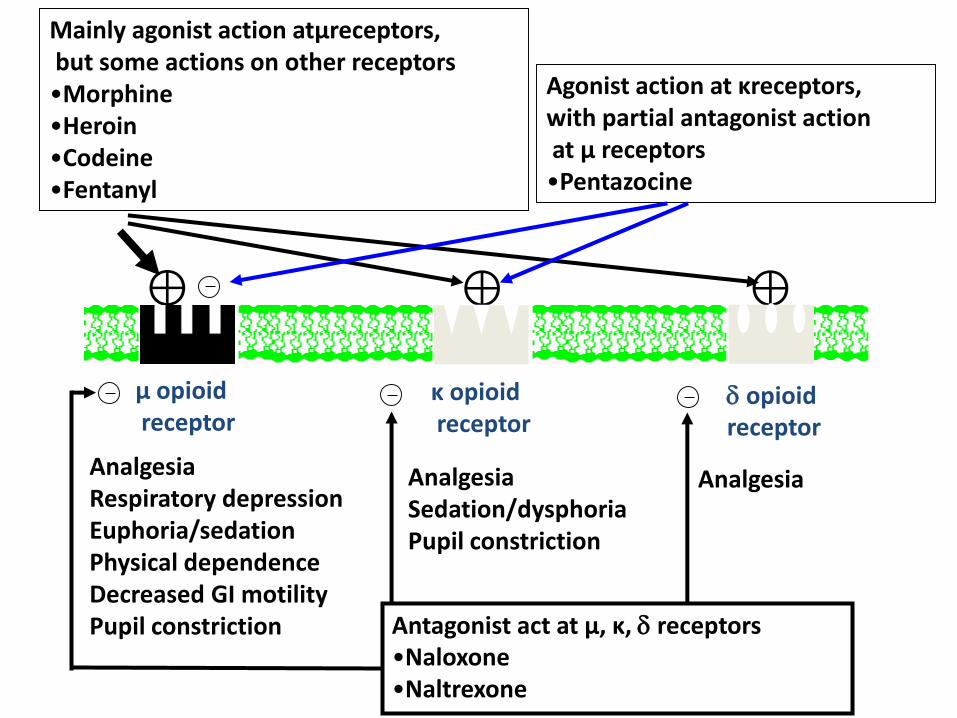
Mainly agonist action atμreceptors,but some actions on other receptors•Morphine•Heroin•Codeine•Fentanyl
⊕
Agonist action at κreceptors,with partial antagonist actionat μ receptors•Pentazocine
⊕⊕
μ opioidreceptor
κ opioidreceptor
opioidreceptor
AnalgesiaRespiratory depressionEuphoria/sedationPhysical dependenceDecreased GI motilityPupil constriction
AnalgesiaSedation/dysphoriaPupil constriction
Analgesia
Antagonist act at μ, κ, receptors•Naloxone•Naltrexone
•Molecular Basis for Opioid Receptor Selectivity and Affinity. Previous studies of other peptide receptors suggested that peptides and small molecules may bind to GPCRs differently. Mutagenesis studies of small-ligand receptors (e.g., adrenergic and dopamine receptors) showed that charged amino acid residues in the transmembrane domains were important in receptor binding and activation.
•Receptor Desensitization, Internalization, and Sequestration after Chronic Exposure to Opioids. Transient administration of opioids leads to a phenomenon called acute tolerance, whereas sustained administration leads to the development of classical or chronic tolerance. Tolerance simply refers to a decrease in effectiveness of a drug with its repeated administration
•An "Apparent Paradox". A paradox in evaluating the function of endogenous opioid systems is that a large number of endogenous ligands activate a small number of opioid receptors. This pattern is different from that of many other neurotransmitter systems, where a single ligand interacts with a large number of receptors having different structures and second messengers.
MorphinePharmacological effects:
A Analgesia:
- Raises the pain threshold at the spinal cord level, alters nociception in the brain.
- Relieves anxiety and fear
B Euphoria:
- Produces a powerful sense of contentment and well-being by stimulation of the ventral tegmentum.
Respiration:
- Causes respiration depression by reduction of the sensitivity of respiratory center neurons to carbon dioxide.
D Depression of cough reflex:
- May allow accumulation of secretions and thus lead to airway obstruction and atelectasis .
-Replaced by other safer antitussives .
Miosis: - The pinpoint pupil is the characteristic of morphine
use, little tolerance. Emesis: - Causes vomiting by
stimulating the CTZ in the medulla but with no
unpleasant sensations. Sedation: - Causes drowsiness
and clouding of mentation, even disrupting sleep
Gastrointestinal effect: - Decreases motility of smooth
muscle and increases tone, which causes constipation
and increases pressure in the biliary tract (worsens
abdominal colic, eg. Sphincter oddi contraction).
Cardiovascular : - Has no major effects on the
cardiovascular system. - Is usually contraindicated in
individuals with severe brain injury (because that
increased PCO2 induced by respiration depression leads
to cerebral vasodilation and consequential increase in
cerebral blood flow and intracranial pressure).
- Causes postural hypotension sometimes.
J Histamine release:
- Causes pruritus, urticaria, sweating, vasodilation and bronchoconstriction.
K Hormonal actions:
- Inhibits release of LH .
- Increases GRH , ADH , PRL
M Immune depression
Therapeutic uses:
A Analgesia:
- Used for various pain, especially acute, obstinate constant pain (e.g. burn, cancer pain);
- Fixed interval of administration reduces tolerance and dependence;
- Severe pain of renal and biliary colic + MR blockers.
Pharmacodynamics- morphine
B Treatment of diarrhea: synthetic surrogates
C Cardiac asthma:
- Acute left ventricular heart failure induces pulmonary
edema
- Reduces anxiety, cardiac preload and afterload.
- Particularly useful for painful myocardial ischemia with
pulmonary edema.
D Relief of cough: synthetic antitussives
E Premeditate drugs before anesthesia : sedative,
anxiolytic, and analgesic properties. For high-risk
surgery administered systemically; for local (epidural)
anesthesia.
Caution: respiratory suppression
Adverse effects:
- Respiratory depression
- Vomiting, constipation, biliary colic
- Dysphoria
- Allergy-enhanced or postural hypotensive effects
- Urinary retention (prostatic hypertrophy)
- Elevation of intracranial pressure (head injury)
-Immune depression
Tolerance and Physical Dependence
• Repeated use produces tolerance to the respiratory depression,
analgesic, euphoric and sedative effects, but not to pupil-
constricting and constipating effects.
• Physical and psychologic dependence readily occur for strong
μagonists, especially used on necessities.
Contraindications:
• Women during labor or lactation
• New-born infants
• Chronic obstructive pulmonary disease (COPD)
• Asthma
• PETHIDINE (meperidine)
Actions and mechanisms:
• Binds to opioid receptors, particularly receptor.
• Actions similar to but less potent than morphine.
----Transient decrease of gastro-intestinal motility and increase of the tone
---- Indistinctly central depression of cough reflex.
`
Therapeutic uses:
• Analgesia: various severe pain, including during obstetric
labor (less depression of respiration in newborn infants)
• Cardiac asthma
• Administration before anesthesia and artificial hibernation,
combined with chlorpromazine and promethazine
Pentazocine
• An agonist on receptor, but a weak antagonist at and
receptors (partial agonist).
• Actions (less potent compared with morphine): analgesia and
respiratory depression, indistinct euphoria and dependence.
Dysphoria, hallucinations and hypertension in high dose
• Used for moderate or chronic pain.
Narcotic Analgesics• Relieve moderate to severe pain by inhibiting release of Substance
P in central and peripheral nerves; reducing the perception of pain sensation in brain, producting sedation and decreasing emotional upsets associated with pain
• Can be given orally, IM, sub q, IV or even transdermally• Orally are metabolized by liver, excreted by kidney—caution if
compromised• Morphine and meperidine produce metabolites• Widespread effects: CNS, Resp., GI• Bind to opioid receptors in brain and SC and even in peripheryIndicationsBefore and during surgeryBefore and during invasive diagnostic proceduresDuring labor and deliveryTx acute pulmonary edemaTreating severe, nonproductive cough
Contraindications to Use• Respiratory depression
• Chronic lung disease
• Chronic liver or kidney disease
• BPH
• Increased intracranial pressure
• Hypersensitivity reactions
Management Considerations
• age-specific considerations
• Morphine often drug of choice—non-ceiling. Other nonceilingdrugs include: hydromorphone, levorphanol and methadone
• Use non-narcotic when able
• Combinations may work by different mechanisms thus greater efficacy (e.g. Tylenol w/codeine)
Dosage• Dosages of narcotic analgesics should be reduced
for clients receiving other CNS depressants such as other sedative-type drugs, antihistamines or sedating antianxiety medications
• Give narcotics before encouraging turning, coughing and deep breathing in post-surgical patients
• Automatic stop orders after 72h
• In acute pain, narcotic analgesics are most effective when given parenterally and at start of pain
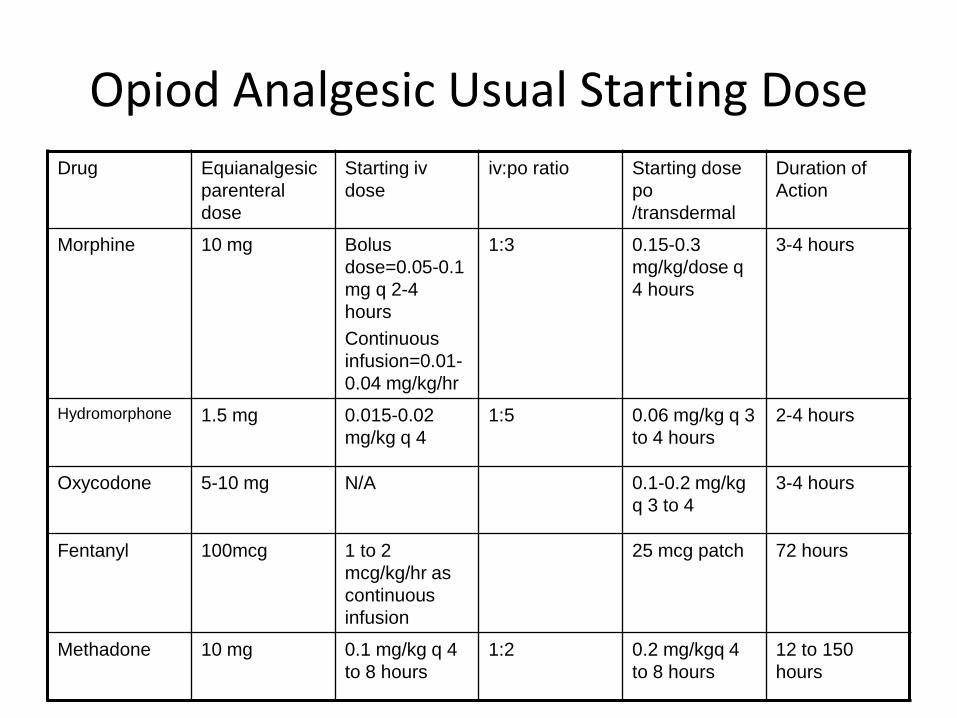
Opiod Analgesic Usual Starting Dose
Drug Equianalgesic
parenteral
dose
Starting iv
dose
iv:po ratio Starting dose
po
/transdermal
Duration of
Action
Morphine 10 mg Bolus
dose=0.05-0.1
mg q 2-4
hours
Continuous
infusion=0.01-
0.04 mg/kg/hr
1:3 0.15-0.3
mg/kg/dose q
4 hours
3-4 hours
Hydromorphone 1.5 mg 0.015-0.02
mg/kg q 4
1:5 0.06 mg/kg q 3
to 4 hours
2-4 hours
Oxycodone 5-10 mg N/A 0.1-0.2 mg/kg
q 3 to 4
3-4 hours
Fentanyl 100mcg 1 to 2
mcg/kg/hr as
continuous
infusion
25 mcg patch 72 hours
Methadone 10 mg 0.1 mg/kg q 4
to 8 hours
1:2 0.2 mg/kgq 4
to 8 hours
12 to 150
hours
Individual Drugs
• Agonists have activity on mu and kappa opioid receptors
• Agonist/antagonists have agonist activity in some receptors; antagonists in others. Have lower abuse potential than pure agonists; because of antagonism—can produce withdrawal symptoms
• Antagonists are antidote drugs
Agonists• Alfenta (alfentanil)—short duration• Codeine • Sublimaze or Duragesic (Fentanyl)—short duration• Dilaudid (hydromorphone)• Demerol (meperidine)—preferred in urinary and biliary colic, less
resp. depression newborns• Morphine• OxyContin
• Darvon (propoxyphene)• Ultram (tramadol)• MethadoneHave lower abuse potential than pure agonists• Buprenex (buprenorphine)• Nubain (nalbuphine)• Talwin (pentazocine)• Stadol (butohanol)—also in nasal spray
Antagonists
• Revex (nalmefene)—longer duration of action than Narcan
• Narcan (naloxone)
• ReVia (naltrexone)-used in maintenance of opiate-free states in opiate addicts
• Zostrix (capsaicin)—from cayenne peppers; topical indicated for post-herpetic neuralgia, neuropathic pain=Substance P
Management of Withdrawal Symptoms• Methadone
• Clonidine (norepinephrine)
• Gradually decrease dosing so not to cause withdrawal s/s
Naloxone• Competitive blocker of opioid receptor, with ten-fold
higher affinity for receptor than for .
• Actions:
--- precipitates withdrawal symptoms;
---reverses the coma and respiratory depression of
opioid overdose (short action duration! Naltrexone with
much longer action duration);
--- eliminates some adverse effects with opioids
Other analgesic
Tramadol: weak receptor agonist, inhibits uptake of NA and
5-HT, effective on moderate to severe acute and chronic
pain.
Tetrahydropalmatine : effective on persistent blunt pain
Neuropathic Pain Syndromes Trigeminal neuralgia Post-herpetic neuralgia Diabetic neuropathy Chemotherapy-induced neuropathy Plexopathies Phantom limb pain Complex regional pain syndrome Central post-stroke (damage to thalamus, cortical
or subcortical structures) Syringomyelia Sympathetically maintained pain syndrome (RSD)
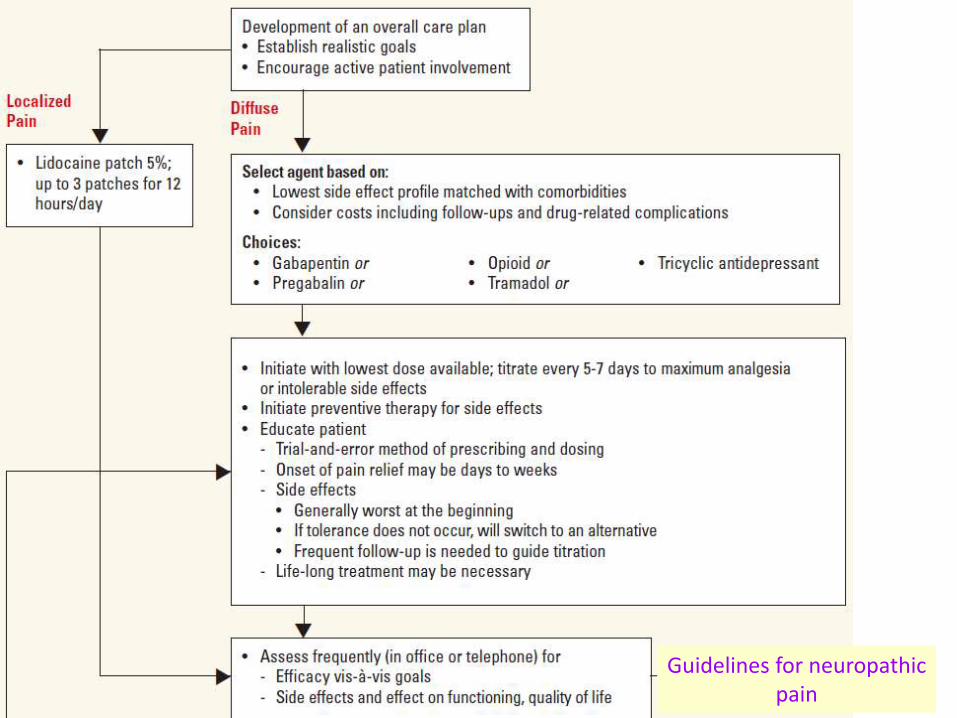
Guidelines for neuropathic pain
Adjuvant Analgesics• Tricyclic Anti-depressants
• Inhibit reuptake of norepinephrine and serotonin in nerve endings in the spinal cord and in the brain
• NMDA antagonism
• Tricyclic Antidepressants• Tertiary amines:
• amitriptyline
• doxepin
• imipramine
• clomipramine
• Secondary amines:• desipramine
• nortriptyline
Antidepressants• Serotoninergic agents
• Fluoxetine
• Paroxetine
• Sertraline
• Citalopram
• Escitalopram
• SNRI’s (serotonin / norepinephrine reuptake inhibitors)
• Venlafaxine
• Desvenlafaxine
• Duloxetine
Antidepressants• Used for:
• Analgesia• Depression• Insomnia• (even pruritis)
• Mechanism of action is inhibition of reuptake of neurotransmitters (serotonin, norepinephrine and dopamine)
• Only tricyclic antidepressants have analgesic properties independent of their antidepressant activity
Antidepressants:Side Effects
• Nausea
• Sedation
• Confusion
• Xerostomia
• Tachycardia
• Drug interactions
• (Anticholinergic )
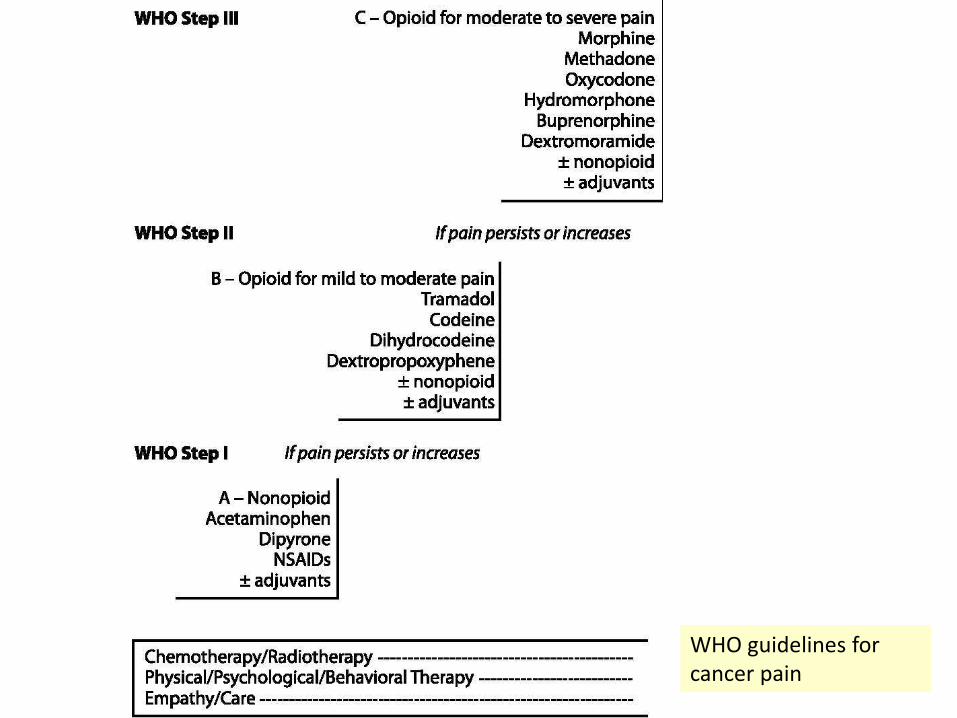
WHO guidelines for cancer pain





























