Embed Size (px)
DESCRIPTION
Anesthesia for closed heart procedure
Citation preview
ANAESTHESIA FOR
CLOSED HEART
PROCEDURE
CLOSED HEART PROCEDURES
•LESIONS CORRECTED WITH CLOSED PROCEDURES
•CLOSED PALLIATIVE PROCEDURES
LESIONS CORRECTED WITH CLOSED PROCEDURES
Patent ductus arteriousus Co-arctation of aorta
CLOSED PALLIATIVE PROCEDURES
o PA Banding o Blalock - Taussig shunto Balloon atrial septostomies (Rashkind
Procedures)
PATENT DUCTUS ARTERIOUSUS
1 in 2500live , full term births 10 % of all congenital heart defects Girls are affected twice than boys Prenatal exposure to rubella virus during first
trimester of pregnancy
ANATOMY PDA extends from the post. Descending aorta
near the origin of left sub clavian artery to the anterior surface of the main pulmonary artery
It is the remnant of sixth branchial arch A bilateral PDA is possible
STRUCTURAL DIFFERENCE BETWEEN PDA& AORTA + PULMONARY ARTERY Aorta & pulmonary artery`s internal media is
composed of elastic fibers Internal media of PDA is composed of smooth
muscle in both longitudinal & circumferential arrangementsThe muscle constrict when exposed to increased Pao2 This response becomes more dramatic as the fetus
matures
PATHOPHYSIOLOGY In the fetus blood flow from the RV is diverted
from the high resistance pulmonary bed via the ductus to the descending aorta
Hemodynamics of a PDA is similar to VSD- left to right shunt flow is determind by the capacity of the ductus to impede flow from the aorta to the PA
If the ductus is large,stunted blood flow is determined by the pulm. Vasculature resistance to systemic vascular resistance
NATURAL COURSE o Functional closure of ductus is due to vas o
Constriction after term
o Anatomic closure is due to intimal proliferation
and fibrosis which is complete at one month
CATEGORIZATION OF PDA
Done on the degree of left to right shunt,which is determined by both the size and the length of the duct and the diff. bet. the SVR and PVR
SILENT: tiny PDA detected by echocardiographySMALL: continuous murmer common;Qp/Qs of
1.5to2.2:1MODERATE: continous murmer
present;Qp/Qs>2.2:1EISSNMENGER:continous murmer
absent;substantial pulm.HT,differential hypoxemia;and differential cyanosis(pink fingers,blue toes)
DIAGNOSIS Signs
tachypneadiaphoresisdecreased exercise tolerance failure to thrive recurrent respiratory infection lobar emphysema / collapsecardiac failurecardiac enlargementbacterial endocarditis irreversible pulmonary vascular disease
PHYSICAL EXAMINATION continuous machine murmur which gets louder through
out systole with a peak at the 2nd heart sound & gets softer through out diastole
Murmur is loudest at 1st or 2nd inter costal space at left sternal border
Pulse pressure- wide- prominent or bounding pulse Pulse biferiens-two distinct peaks seprated by a deep
cleft, noted on the intra-arterial wave form is a specific & sensitive indicator of PDA with Left to right shunting in the neonate
ECG- usually normalwith large L-R flow- LVH or Lt arterial enlargement
o RVH- if PDA has caused pulmonary occlusive diseaseo Chest x-rayo small PDA – normal X-rayo as flow increases- prominent pulmonary
-prominent aortic knobo further increase in flow
- left heart enlargement
- increase in pulmonary vascular marking
( indicative of failure)
o Echocardiographyo main diagnostic procedure for PDAo 2D Echo- can identify the aortic end of the ductuso Continuous wave Doppler – can detect abnormal flow in PAo Color flow Doppler- can visualize the jet of abnormal flow &
determine more information about the size and shape of the ductus
INDICATION FOR INTERVENTION
Unnecessary in an asymptomatic infant with a small left to right shunt
Necessary for those who have signs of a significant ductal left –to- right shunt during the course of the respiratory distress syndrome
Surgical ligation is required in the infants who are unresponsive to Indomethacin
C.I TO DUCTAL CLOSURE Irreversible pulmonary HT Active endarteritis
PREOPERATIVE PREPARATION Prophylactic antibiotics Vit. K (preterm infants)
INTRA-OPERATIVE MONITERING ECG B .P – invasive Capnography Pulse oximeter (two) – Rt hand & one on
lower extrimity Temperature monitering Esophageal stethoscope – to listen to murmur
PREMEDICATION
Usually not recquired ORAL PREMEDICANT COMBINATIONS Mepridine – 1.5 mg/kg(max. 100mg) Atropine -0.02mg/kg(max.0.4mg) Diazepam 0.15mg/kg(10mg)
or Mepridine – 2- 3mg/kg(max.100 mg) Diazepam -0.1 mg/kg(max.10mg) Fentanyl(oral/transmucosal) – 15 – 20 micro gram/kg
or Midazolam -0.5 – 0.75 mg/kg(max.5mg) INTRAMUSCULAR PREMIDICANT COMBINATIONS Morphine 0.2 mg /kg(max.10mg)
oro Midazolam -0.08mg/kg(max5mg)
(recommended for children over 1 year of age)
INDUCTION Fentanyl – 2microg/kg body wt. Sleep dose of thiopentone Succinyl choline – 1mg/kg Ventilation Larynx sprayed with 2% ligocaine Maintenance with N2O & O2 mixture( 60:40) Halothane and non depolarising agents Other supplemental drugs used are
ketamine,isoflurane and midazolam
MAINTENANCE N2O +O2+ Halothane + non depolarising agents Sodium Nitropruside – 1 vial in 5% of 500 ml of
dextrose in micro drip set started when the ductus is dissected out and the systolic pressure is brought down to 60 mm Hg
Once the ligation is complete the SNP is stopped and continued if the pressure rises post -operatively
FOLL. LIGATION OF PDA Diastolic pressure rises in the typical PDA pt. In selected pt`s – PA pressure monitoring m/b
carried out In typical PDA pt`s with no change in PA
pressure after occlusion If PA pressure falls in pt`s with pulmonary HT,
then the degree of increased resistance is minimal & the ductus m/b ligated safely
If PA pressure increases with severe pulmonary HT – then ligation carries a high mortality
ON THE CLOSURE OF DUCTUS The diastolic component of the murmur will
disappear Systolic component persist but without
significance
SERIOUS COMPLICATION A serious complication is increased PVR with
severe Pulmonary hypertension- reversal of flow –RHF
• If ligation of the ductus is performed at this stage death may occur promptly owing to the closure of the escape route of the pulmonary circuit
o Damage to the laryngeal nerve
INTERVENTIONAL TECHNIQUES
TRANSCATHTER TREATMENT -for ducts smaller than 8mm have been establised
SURGICAL TREATMENT -either by ligation or by putting clips
-greater morbidity and mortality
-immediate closure in more than 95%of patients
-surgical mortality in adults is 1%to 3.5% and is due to pulmonary art. Hypertension and difficult ductal morphology
-reserved for those in whom PDA is too large for device closure
VIDEO ASSISTED THORACOSCOPIC SURGERY
-costly
-experience is required
CO –ARCTATION OF AORTA Etiology and risk of occurrence -1 in 2000 live births Sixth most common congenital heart disease Narrowing of aortic lumen from protrusion from within
posterior and lateral aortic media Mortality is associated with - cardiac failure (25%)
-Aortic rupture(21%)
-Endocarditis (18%)
-Cerebrovascular hemorrhage(11.5%)
-Others –HT
-CAD
ANATOMY Classification of co-arctation is based on the
relationship with the ductus arteriosus Preductal – proximal to the ductus , infantile
type Postductal – distal to the fibrosed ductus,adult
type
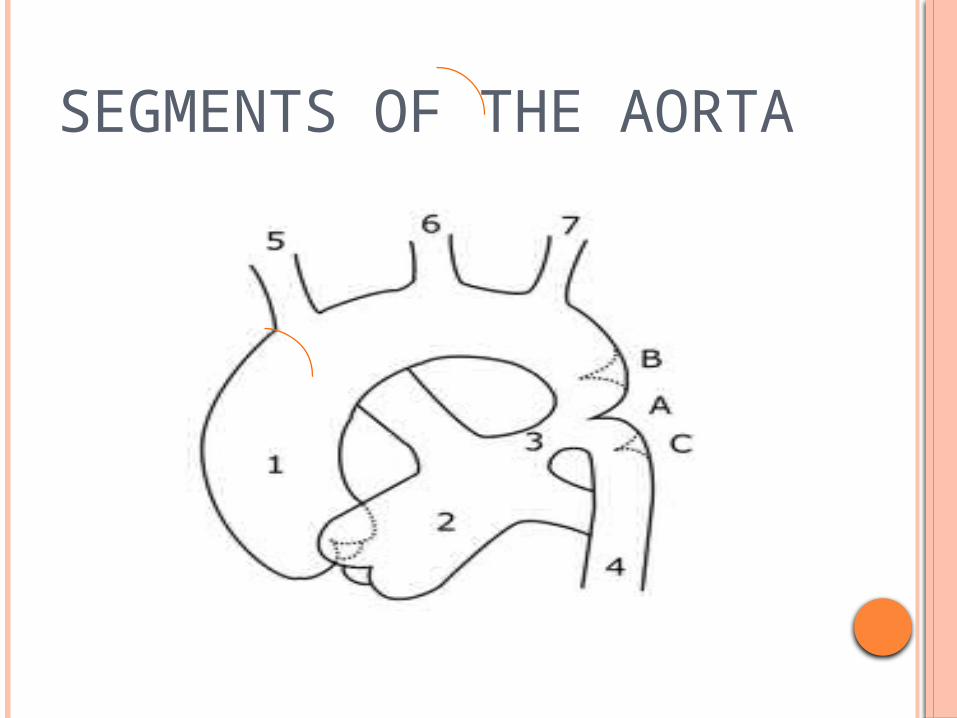
SEGMENTS OF THE AORTA
SEGMENTS OF THE AORTA Ascending aorta to innominate to artery proximal arch from innominate to left carotid Distal arch from left carotid to left subclavian
artery Isthmus from left subclavian to co –arctation Aorta at the level of the diaphragm
PRE – DUCTAL CO ARC TATION Morphology -Localised shellf in the postero lateral aortic wall
opposite the ductus More assoc. with neonates CLINICAL FEATURES More in males Associated with –gonadal dysgenesis (Turner syndrome
-Biscuspid aortic valve
-VSD
-MS/MR
NEONATES Left ventricular failure –
increase in left ventricular wall stress after closure of arterial duct
Systemic hypo perfusionLeft to right shunting across patent foramen ovale
(PFO) and pulmonary venous hyper tension secondary to heart failure cause pulmonary arterial hypertension
Peripheral pulse are weak If L.V function is improved with medical
management, a significant pressure difference then develops between the arms & the legs, allowing detection of a pulse discrepancy
LAB INVESTIGATION ECG –RAD &RVH Chest x- ray
Cardiomeagalypulmonary arterial & venous engorgementEchocardiographyDemonstrates the posterior shelf & the degree of
associated isthmic or transverse arch hyopoplasia Doppler echo cardiography -is helpful if ductus is closed
- it demonstrates a high velocity jet during systole & diastole
MANAGEMENT Prostaglandin therapy
PGE1 infusion to dilate the ductus arteriosus, the pressure difference may be obliterated across the site of co-arctation because the fetal flow pattern is re-established
This also improves the renal perfusion, which in turn reverses the associated metabolic acidosis
INTERVENTIONSurgical- excision of the area of co-arctation and
extended end to end repair or end to side anastomosis with absorbable
sutures to allow remodeling of the aorta with time
Subclavian flap aortoplasty- Less popular now days
Balloon dialation – does not have in management in this age group
Early surgery – lower incidence of long term hypertension
INFANTS & CHILDRENPRESENTATION Reduced femoral pulses Hypertension Heart failure is uncommon because, the L.V has
a chance to become hypertrophied Complaints of headache, cold extremities and
claudication with exercise is noted in older child & adolescent age group
Midsystolic murmur over the anterior chest, back is most frequent
Lab investigation ECG
-LVH with co-existing RVHo CHEST-X RAY
pre –stenotic & post stenotic dilatation of the proximal descending thoracic aorta
Rib notching – unilateral or bilateral in 50% of caseECHO cardiography
- Demonstrates a post. Shelf
-A well expanded isthmus and trasverse aortic arch
-High velocity continuous jet through the co-arctation site
INTERVENTION Balloon dilation Surgery reserved for arch hypoplasia
Extended end to end anastomosis is the currently favored surgical approach with patch augmentation
COMPLICATIONS Paradoxical HT in immediate post. Op ( not seen
with balloon dilation ) Becoz of HT – cerebral aneurysm & hemorrage
Hypertensive encephalopathyRupture of aortaL V F Infective endocarditis
ADULT PRESENTATION Presents with simple co-arctation Associated anomalies –
bicuspid aortic valve(80 %)Intracranial aneurysms (2-10%)
CLINICAL FEATURES Asymptomatic Epistaxis Headache Leg weakness on exertion C H F Angina Aortic stenosis Aortic dissection Un explained intracerebral hemorrhage Leg claudication ( pain)
CLINICAL EXAMINATION Upper limb HT Differential systolic blood pressure of atleast
10mm Hg(brachial>popliteal) Radial-femoral pulse delay Auscultation- interscapular systolic murmur Fundoscopic examination-corkscrew tortuosity
of retinal arterioles
INTERVENTION Surgical Balloon dilatation
ANAESTHETIC MANAGEMENT PRE-OP PREPARATION
Prophylatic antibioticsControl of BPBETA-blockerso Intra Operative Monitoring
Invasive arterial pressure monitoring in right radial artery and femoral artery
o CVP Monitoringo Capnographyo Pulse Oximitryo Spinal Cord Monitoring -
ANAESTHETIC INDUCTION G.A with controlled ventilation is the
technique of choice Epidural anaesthesia avoided as it may mask
paraplegia Total IV Anaesthesia with opiates is useful in
neonates with cardiac failure or cardiovascular instabilty
Avoid ketamine Isoflurane preffered becoz of its effect on
afterload
MAINTENANCE
Monitor lower body pressure closely-pressure should not fall 45mmHg
Provide analgesia for intra&postop Epidural analgesia technique+/-; Intercostal nerve blocks not recommended
becoz of collaterals Volatile agents make blood pressure control
easy Start antihypertensive control early after
cross clamp has been removed,using beta –blockade,then nitroprusside
THANK YOU