Embed Size (px)
Citation preview

CASE REPORT
Anabolic steroid related abscess–—A riskworth taking?
C.P. Marquis *, N. Maffulli
Injury Extra (2006) 37, 451—454
www.elsevier.com/locate/inext
Orthopaedics and Trauma, University Hospital of North Staffordshire, Royal Infirmary,Princes Road, Hartshill, Stoke-on-Trent ST4 7LN, United Kingdom
Accepted 5 June 2006
Introduction
Anabolic steroid use in the sporting arena is wellrecognised,10 however, there appears to be increas-ing numbers of people using these drugs for aes-thetic reasons. Worryingly, the profile of the usersnot only crosses social boundaries, but also agegroups, with children as young as 14 reporting thereuse.5
As well as the side effects of the drugs,8 there arethe associated risks of infection associated withneedle sharing and poor injection technique. Thedrugs themselves may be contaminated,2,12 theillegal nature of there use necessitating illicit meansto obtain a supply.
We report on a case of bilateral deltoid abscessessecondary to anabolic steroid use and the subse-quent treatment. The literature pertaining to theuse of steroids and the reported clinical cases arediscussed.
Case
A 36-year-old male body builder presented withbilateral deltoid abscesses associated with pyrexia
* Corresponding author. Tel.: +44 77 200 76909;fax: +44 1782 714817.
E-mail address: [email protected] (C.P. Marquis).
1572-3461# 2006 Elsevier Ltd.doi:10.1016/j.injury.2006.06.011
Open access under the Elsevier OA license.
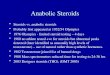
and marked local erythema (Fig. 1). Both abscesseswere fluctuant and exquisitely tender, measuring4 cm � 5 cm. The patient readily admitted to intra-muscular steroid use, giving details of a 10-daycycle, over which he took:
� 1
00 mg Viramone (testosterone propionate); � 3 00 mg Enathate (testosterone enathate); � 3 00 mg Deca–—duarabolin (nandrolone).The patient was taken to theatre and bothabscesses incised and drained (Fig. 2). The woundswere packed and antibiotics commenced consistingof flucloxacillin (1 g QDS) and benzylpenicillin (1.2 gQDS). Subsequent cultures showed a growth of Sta-phylococcus aureus sensitive to flucloxacillin andantibiotic therapy was therefore restricted to flu-cloxacillin only.
The patient was followed up over a period of 2months whilst dressing management was dealt withby both district and clinic nursing staff. During hisfollow-up the patient persisted in weight training,altering his regime to accommodate his reduceddeltoid function. At discharge his wounds hadhealed well and an agreed lifting strategy of lowweights and high reps was being utilised by thepatient. At no stage did the patient admit to eitherneedle or vial sharing, like wise the clinical incidenthad not served to altered his intentions regardsfurther anabolic use.

452 C.P. Marquis, N. Maffulli
Figure 1 Pre-operative clinical appearance.

Anabolic steroid related abscess–—A risk worth taking? 453
Figure 2 Intra-operative drainage.
Discussion
Anabolic steroid use for performance enhancing iswell recognised, and tested for by sporting bodies.10
With the increasing emphasis on the ‘body beauti-ful’ concept, an increasing number of people areturning to such drugs for aesthetic reasons.4,5 Thereare no exact figures available on the scale of use,but needle exchange programmes in many cities arenoticing that often the largest single group visitingare intra-muscular steroid injectors,6 overtakingopiate users. In some cases up to 60% of the clientbase are anabolic steroid users.6 The Home Officealso estimates that as many as 42,000 people use thedrugs in the UK.1
Aworrying trend is the change in the profile of theusers. Steroid use is increasing among children andadolescents as young as 14.5 Social groups are alsono boundary, with teachers, police officers andoffice workers all admitting to anabolic abuse.Schools are also noting usage among pupils.6 In astudy from the Children’s Hospital Boston, Massa-chusetts4 they looked at a population of 6212 girlsand 4237 boys aged from 12 to 18 years old. 4.7% ofboys and 1.6% of girls used protein powders, crea-tine, amino acids, beta-hydroxy-beta-methylbuty-
rate, dehydroepiandrosterone, growth hormone oranabolic/injectable steroids at least weekly. Boysreading fashion or health and fitness magazines, andgirls who were trying to look like women in themedia, were significantly more likely than theirpeers to use products to improve appearance orstrength.
There have been several reports of abscessesrelated toanabolic steroid injection.2,7,9,11,12,13 Nee-dle and vial sharing is commonplace and has oftenbeen the attributed cause. Grace, Barker and Daviesreported needle sharing in a sample of 170 cases.5
Staphylococcal infections have been reported occur-ring from needle sharing, or reusing,11 as well asStreptococcus and atypical Mycobacteria.13
Another potential source of infection are thedrugs themselves. Steroids are banned under thesame Misuse of Drugs act that controls the supply ofrestricted drugs such as heroin, cannabis andcocaine. Users thus have to resort to illicit meansto obtain their supplies. As a result there are limitedguarantees that the product purchased is what itsays on the bottle. On the Internet there are avariety of forums and resources where usersexchange information and advice to improve theirchances of success. Despite this, infections from

454 C.P. Marquis, N. Maffulli
contaminated sources still occur. Mycobacteriumsmegmatis has been cultured from a veterinarygrade stanozolol that caused thigh abscesses intwo body builders.12 Likewise there has been areport of a gluteal abscess caused by a drug con-taminated with Pseudomonas.2
Conclusion
Like most habits with associated risk, cessation ofthe activity is the best way of reducing this risk. Aswell as the associated side effects of testicularatrophy, baldness and gynaecomastia,8 seriousinfections can occur. These infections are oftensecondary to needle sharing, contaminated productand poor injection technique, and they shouldtherefore be preventable. Needle exchanges helpwith this, and further patient education would alsobe of benefit. The behaviour of anabolic drug users isstill open to further investigation. Having engaged inan illegal activity they may be less inclined to seekmedical advice or aid, with potentially serious out-comes. Also ‘muscle dysmorphia’ is accepted as apsychological disorder, although it is still debatedwhether it is a sub-category of body dysmorphicdisorders (such as anorexia nervosa), or more con-sistent with an obsessive—compulsive disorder.3
Whilst not all steroid users will fall into this cate-gory, some inevitably will, and as will require appro-priate treatment for their condition. An abscess isunlikely to be sufficient deterrent for such a patient.
References
1. Aust R, Sharp C, Goulden C. Prevalence of drug use: keyfindings from the 2001/2002 British Crime Study. http://www.homeoffice.gov.uk/.
2. Bergman RT. Contaminated drug supply. Phys Sportsmed1993;21:8.
3. Chung B. Muscle dysmorphia: a critical review of the pro-posed criteria. Perspect Biol Med 2001;44(4):565—74.
4. Field AE, Austin SB, Camargo Jr CA, Taylor CB, Striegel-MooreRH, Loud KJ, et al. Exposure to the mass media, body shapeconcerns, and use of supplements to improve weight andshape among male and female adolescents. Pediatrics2005;116(2):214—20.
5. Grace F, Baker J, Davies B. Anabolic androgenic steroid use inrecreational gym users: a regional sample of the mid-Gla-morgan area. J Subst Use 2001;6(3):189—95.
6. Kelso P, Mackay D, Taylor M. From gym to club to school: theshock spread of steroid abuse. The Guardian, 14 November2003.
7. Krauss MD, Van Meter CD, Robertson DW. Be alert for ‘spotshot’ complications. Your Patient Fitness 1995;9:12—4.
8. Maravelias C, Dona A, Stefanidou M, Spiliopoulou C. Adverseeffects of anabolic steroids in athletes. A constant threat.Toxicol Lett 2005;158(3):167—75.
9. Maropis C, Yesalis CE. Intramuscular abscess: another ana-bolic steroid danger. Phys Sportsmed 1994;22:105—10.
10. Noakes TD. Tainted glory–—doping and athletic performance.N Eng J Med 2004;351(9):847—9.
11. Plaus WJ, Hermann G. The surgical management of super-ficial infections caused by atypical mycobacteria. Surgery1991;110:99—105.
12. Rastad J, Jorborn H, Ljunghall S, Akerstrom G. Glutealinfection hos styrkelyftare efer injectktion av anabola ster-oider. Lakartidningen 1985;82:3407.
13. Rich JD, Dickinson BP, Flanigan TP, Valone SE. Abscess relatedto anabolic-androgenic steroid injection. Med Sci SportsExerc 1999;31(2):207—9.