Embed Size (px)
Citation preview

ELSEVIER Clinical Neurology and Neurosurgery 97 (1995) 23-27
Clinical Neurology and Neurosurgery
An unusual case of central nervous system cryptococcosis
S t e p h a n S c h m i d t a'*, I n g r i d R e i t e r - O w o n a b, M i c h a e l H o t z a, J o a c h i m M e w e s a, R o l f B i n i e k a
"Department of Neurology, RLK Bonn, Bonn, Germany bDepartment of Parasitology, University of Bonn, Bonn, Germany
Received 8 August 1994; revised 5 October 1994; accepted 17 October 1994
Abstract
Opportunistic infections of the central nervous system (CNS) in immunocompromised patients often represent a diagnostic and therapeutic challenge due to the variety of possible infectious agents causing CNS disease. We report the case of a severely immunocompromised 43-year-old woman presenting with headache, confusion, abnormal CSF findings (cell count 237/mm 3 with 50% eosinophils and clew.ted protein), multiple contrast enhancing lesions on CT and MRI in the basal ganglia, and serologic findings compatible with latent or reactivated toxoplasmosis with high IgA and IgG antibody titers against Toxoplasma gondii in whom a final diagnosis of CNS cryptococcosis was made. This case illustrates the considerable difficulties in the differential diagnosis of opportunistic CNS infection in the immunocompromised host. We conclude from our report that (1) the diagnosis of toxoplasma encephalitis should not be based on serological findings but rather be proven by either PCR, mouse inoculation or brain biopsy, (2) CNS cryptococcosis can be associated with marked CSF eosinophilia and multiple cryptococcomas, and (3) cryptococcomas can persist on CT and MRI despite successful antifungal treatment.
Keywords." Cryptococcus neoformans; Cryptococcomas; CSF eosinophilia
1. Introduction
Opportunistic infections of the CNS represent life threatening complications of immunosuppression. In the past decade the incidence of opportunistic CNS infec- tions has increased dramatically, mainly due to the out- break of the acquired immunodeficiency syndrome (AIDS) epidemic. The spectrum of opportunistic CNS infection is broad including viruses, bacteria, fungi and parasites. Toxoplasmic e.ncephalitis and CNS cryptococ- cosis rank second and third after HIV on the list of infectious agents causing CNS disease in AIDS [1]. Up to 28% of patients with AIDS develop cerebral toxoplas- mosis [1] and up to 111% CNS cryptococcosis in the course of the disease [2]. The differential diagnosis in the
*Corresponding author. At: Department of Neuroimmunology, Max Planck Institute of Psychiatry, Am Klopferspitz 18a, D-82152 Martinsried, Germany. Tel.: (+49-89) 8578 3585; Fax: (+49-89) 8578 3790.
0303-8467/95/$9.50 © 1995 Elsevier Science B.V. All rights reserved SSDI 0303-8467(94)00063-8
immunosuppressed host presenting with headache, con- fusion, lethargy or a focal neurologic deficit remains challenging, however. Cerebrospinal fluid (CSF) find- ings in opportunistic CNS disease are usually nonspe- cific, revealing a mild mononuclear pleocytosis with slight elevation of protein or hypoglycorrhachia. Still, in about 50% of patients with CNS cryptococcosis the CSF cell count remains normal [3]. Neuroimaging by com- puted tomography (CT) and magnetic resonance imag- ing (MRI) can help to detect intracranial mass lesions, but no pathognomonic features exist that could establish a specific diagnosis on the basis of CT or MRI alone [4-6]. Serologic studies are useful in the diagnosis of CNS cryptococcosis [7] but can be confusing in Toxoplasma encephalitis [8]. We report the case of a 43 year old female with severe immunosuppression follow- ing thymectomy and multiple courses of combined irra- diation and chemotherapy who presented with multiple contrast enhancing mass lesions on CT and marked CSF eosinophilia. A final diagnosis of CNS cryptococcosis

24 S. Schmidt et al. /Clinical Neurology and Neurosurgery 97 (1995) 2 3 ~ 7
Fig. 1. Noncontrast- and contrast-enhanced CT of the brain obtained 3 days after admission showing asymmetrical iso- or hyperdense lesions in the basal ganglia and in proximity of the corticomedullary junction (a) with strong postcontrast enhancement (b).
was made, although the serologic studies indicated reac- tivated CNS toxoplasmosis. We discuss the clinical and diagnostic features of CNS cryptococcosis and toxoplas- mic encephalitis, the differential diagnosis of contrast enhancing mass lesions on CT and MRI and CSF eosin- ophilia.
2. Case report
A 43-year-old woman was admitted to our clinic be- cause of progressive waste, headache, dysphagia and confusion. At the age of 35 well differentiated thymic carcinoma had been removed. Combined mediastinal ir- radiation and chemotherapy had been performed for local metastases to the mediastinum and the left lateral thoracic wall. One year after thymectomy paraneoplastic myasthenia gravis developed. Six months prior to admis- sion a course of chemotherapy with doxorubicin and carboplatin had to be interrupted because of pancy- topenia. On examination the patient was cachectic with arterial hypotension of 80/60 mm Hg; the temperature was 37.5°C, the pulse rate 100/min. Neurologic examina- tion revealed weakness of the left lateral rectus muscle and minimal facial asymmetry on the same side. The
patient was unable to swallow and there was general muscle wasting without focal weakness. The tendon re- flexes were ++ and equal, the plantar responses were flexor. The patient was alert, easily fatigued and disori- ented in time and place. Laboratory abnormalities included transient normochromic anemia with 9.3 g/dl hemoglobin and a MCH of 98.9 ft. Leucocytes were 6500//21 with 3.6% lymphocytes. The CD4+ and CD8+ lymphocyte counts were 20//21 and 100//21, respectively. The CD4+/CD8+ ratio was 0.2. ELISA, polymerase chain reaction (PCR) and Western blot testing for HIV- 1/2 was negative. CT scan revealed multiple bilateral iso- or hyperdense lesions in the basal ganglia (Fig. 1 a) which strongly enhanced after i.v. injection of contrast material (Fig. lb). On MRI these lesions were hyperintense on T2-weighted images and enhancing on postcontrast T1- weighted images (Fig. 2). Lumbar puncture yielded 237/ mm 3 white cells with approximately 50% eosinophils. CSF protein was 173 mg/dl, CSF glucose 38 mg/dl (blood glucose 105 mg/dl). Culture and serological test- ing for helminthic parasites, mycobacteria, leptospirosis and brucellosis were negative. Dye test (DT) for specific anti-Toxoplasma IgG antibodies showed persistently ele- vated IgG antibody titers in blood (1:4000 to 1:16 000) and CSF (1:256). IgA antibody titers as measured by

s. Schmidt et al. / Clinical Neurology and Neurosurgery 97 (1995) 23-27 25
unchanged and there was a pleocytosis of 23/mm 3 white cells with about 20% eosinophils, the cryptococcal anti- gen in the CSF had dropped to 1:16. After 11 months CT scan revealed a markedly diminished number of le- sions with less contrast enhancement (Fig. 3a,b). CSF was normal except for persisting intrathecal IgG produc- tion. CSF cultures for Cryptococcus neoformans were negative after 6 weeks of treatment and remained nega- tive after 3, 5 and 11 months. Clinically, the patient was well without neurologic or psychopathologic deficit. Leucocytes were 3680//A with 13,6% lymphocytes. The CD4+ and CD8+ lymphocyte counts were 90//~1 and 240//zl with a CD4+/CD8+ ratio of 0.4.
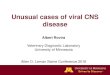
Fig. 2. Coronal Tl-weighted MRI of the brain after gadolinium injec- tion obtained 6 weeks after admission showing disseminated contrast- enhancing nodules in the basal ganglia and in proximity of the corti- comedullary junction with predilection of the right hemisphere.
immunosorbent agglutination assay (ISAGA) were largely elevated in blood (> 1 : 16 000) and borderline in CSF (1:64). Toxoplasma-specific IgG-avidity as meas- ured by ELISA was >30%. Specific anti-Toxoplasma IgM antibodies could not be demonstrated by ISAGA or by indirect immunofluorescent test (IgM-IFT). A mouse inoculation test and PCR failed to detect Toxoplasma parasites. Treatment with oral pyri- methamine (75 mg/d), sulfadiazine (4000 mg/d) and fo- linic acid (15 mg/d) was begun for suspected toxoplasmic encephalitis. CSF pleocytosis dropped to 59/mm 3 after 4 days of treatment, but rose again to 180/mm 3 after 1 week. CT scan after 1 month of therapy was un- changed but Cryptococcus neoformans could be detected by India ink stain. CSF at that time showed 79/mm 3 white cells with an unchanged high percentage of eosino- phils, CSF protein was 93 mg/dl, CSF glucose 41 mg/dl (blood glucose 91 mg/dl). The cryptococcal antigen was 1:4200 in the CSF. Treatment with intravenous flucon- azole at 400 mg/d was begun and continued with an oral maintenance dose of 400 mg/d after 2 weeks. Recurrent tonic-clonic seizures could be controlled by administra- tion of 600 mg carbamazepine daily. The patient was dismissed on 400 mg fluconazole per day. CT scan was
3. Discussion
Toxoplasma encephalitis is a condition almost un- known in immunocompetent hosts [9]. Among the pa- tients immunocompromised by malignancies, collagen- vascular disease or among transplant recipients toxoplasmic encephalitis is the most common manifesta- tion of organ-specific toxoplasmosis [10]. Moreover, toxoplasmic encephalitis has become the most important differential diagnosis in suspected opportunistic CNS disease after the outbreak of the AIDS epidemic [1,11]. Toxoplasma serology had not been performed in our patient before the onset of the clinical symptoms. How- ever, the serological findings were compatible with chronic toxoplasmosis when CNS disease developed. Al- though HIV negative the rather selective T-cell defi- ciency in our patient resulted in a condition closely re- sembling AIDS. In these patients CNS toxoplasmosis rather represents a reactivation of a latent infection than a manifestation of an acute, acquired infection [12]. Un- fortunately, conventional anti-Toxoplasma serology often fails to differentiate conclusively between chronic latent and reactivated toxoplasmosis [8,13]. Therefore it is recommended to use alternative methods such as mi- croscopy, PCR and mouse inoculation test for the defin- itive diagnosis of reactivated toxoplasmosis [8,13].
Clinically, Toxoplasma gondii causes an acute or suba- cute meningoencephalitis presenting with focal neurol- ogic deficits superimposed on mental status changes [12,14].
On CT and MRI toxoplasmic encephalitis usually pre- sents as multifocal, contrast enhancing process with a predilection for the basal ganglia, the frontoparietal lobes and the cerebellar hemispheres often associated with surrounding edema and considerable mass effect [4,5]. In our patient the CT and MRI distribution of the contrast enhancing lesions was compatible with toxoplasmic encephalitis, although there was no mass effect and almost no perifocal edema.
CSF examination in Toxoplasma encephalitis usually reveals a mononuclear pleocytosis of < 100/mm 3, eleva-

26 S. Schmidt et al. I Clinical Neurology and Neurosurgery 97 (1995) 23~7
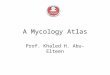
Fig. 3. a and b: noncontrast- and contrast-enhanced CT of the brain obtained after 11 months of follow-up. The lesions shown in Fig. la and b are still detectable but diminished in number and postcontrast enhancement.
tion of CSF protein and mild hypoglycorrhachia [12,14]. CSF eosinophilia is not a prominent feature of Toxoplasma encephalitis [15].
The clinical findings in our patient were compatible with CNS cryptococcosis. Headache is almost univer- sally noted in patients with CNS cryptococcosis followed by focal neurologic deficits, mental status changes, sei- zures and cranial nerve palsies [2,3].
CSF studies in CNS cryptococcosis usually reveal a moderate mononuclear pleocytosis of 20-500/mm 3 [2,3] but can be normal in over 50% of patients with AIDS [2,3]. Assays of the cryptococcal antigen in serum and CSF reach a sensitivity and specificity of over 90% [16]. Cryptococci can be cultured from the CSF in about 70-90% and India ink studies are positive in about 70% [2,3,16,17].
Marked CSF eosinophilia is an extremely rare finding in CNS cryptococcosis [15]. The association between Coccidioides immitis infection and CSF eosinophilia has been documented more frequently [15,18]. In most cases, however, it is either caused by helminthic parasites or by an allergic reaction following the application of nonster- oidal anti-inflammatory agents, antibiotics or myelogra- phy contrast agents [15]. Other rare conditions associ- ated with CSF eosinophilia include sarcoidosis and
central eosinophilic granuloma [15], but none of those could be verified in our patient.
Pathologically, Cryptococcus neoformans causes a bas- ilar, chronic meningitis spreading along the subarach- noid space [19]. Cryptococci can form cystic lesions in the Virchow-Robin spaces adjacent to the basal ganglia and the corticomedullary junction, consisting of budding yeast with little surrounding inflammation [19]. Invasion of the CNS leads to intraparenchymal mass lesions, called cryptococcomas. In our patient the CT and MRI findings opened a broad spectrum of differential diagno- ses. The most common causes of focal intracranial mass lesions in AIDS patients are toxoplasmic encephalitis and primary CNS lymphoma [4,5]. Radiological abnor- malities associated with CNS cryptococcosis include dif- fuse atrophy, hydrocephalus and widening of the basal cisterns [20]. Cryptococcomas occur in 4-11% of patients with cryptococcal meningitis [20-25]. They can either present as solitary mass lesion or as disseminated lesions predominantly in the basal ganglia and the midbrain [6,20-25]. Cryptococcomas typically exhibit a strong en- hancement of contrast material [20]. The CNS pathology of cryptococcal infection can be classified according to MRI criteria. The most common patterns described are parenchymal cryptococcomas, dilated Virchow-Robin

S. Schmidt et al. /Clinical Neurology and Neurosurgery 97 (1995) 23-27 27
spaces and multiple parenchymal and leptomeningeal nodules [25]. In our patient the distribution of the CT and MRI lesions was indicative of dilated Virchow- Robin spaces that typically present as nonenhancing, hypodense 'soap bubble~';' on CT [4,5]. Our patient, how- ever, exhibited massive contrast enhancement. Pathol- ogically, cryptococcoma~; and dilated perivascular spaces are usually present in the same areas [6]. We conclude that the contrast enhancing lesions in our patient repre- sent cryptococcomas in a distribution otherwise typical for dilated perivascular spaces.
Finally, we would like: to emphasize that the cryptoc- comas visualized on CT and MRI persisted over a fol- low-up period of 11 months although the patient was clinically asymptomatic and CSF cultures for Cryptococ- cus neoformans had relx~ained negative for almost 9 months.
Acknowledgements
We would like to thartk Uwe Gross (Wiirzburg, Ger- many) for screening the specimen for Toxoplasma infec- tion by PCR and Klaus Hedman (Helsinki, Finland) for testing the sera by IgG-avidity ELISA.
References
[1] Levy, R.M., Bredesen, D.E. and Rosenblum, M.L. (1985) Neuro- logical manifestations of the acquired immunodeficiency syn- drome (AIDS): experience at UCSF and review of the literature. J. Neurosurg., 62: 475-49:5.
[2] Zuger, A., Louie, E., Holzman, R.S., Simberkoff, M. and Rahal, J. (1986) Cryptococcal disease in patients with the acquired immu- nodeficiency syndrome. A:an. Intern. Med., 104: 234-240.
[3] Pons, V.G., Jacobs, R.A. and Hollander, H. (1988) Nonviral infec- tions of the central nervous system in patients with acquired immu- nodeficiency syndrome. In: M.L. Rosenblum, R.M. Levy and D.E. Bredesen (Eds.), AIDS and the Central Nervous System, Raven Press, New York, pp. 263- 283.
[4] Post, M.J.D., Berger, J.R. and Hensley C.T. (1986) The radiology of central nervous system disease in acquired immunodeficiency syndrome. In: J.M. Taveras and J.T. Ferucci (Eds.), Radiology: Diagnosis-Imaging-Interve.ntion, Vol, 3, J.B. Lippincott, Philadel- phia, PA, pp. 1-26.
[5] Post, M.J.D. (1993) Neuroimaging of AIDS. In: A.L. Belman (Ed.), AIDS and the Nervous System, Annual Meeting of the American Academy of Neurology, New York, pp. 65-132.
[6] Mathews, V.P., Alo, P.L., ]~umar, A.J. and McArthur J.C. (1992) AIDS-related CNS cryptococcosis: Radiologic-pathologic correla- tion. AJNR, 13: 1477-1486.
[7] Perfect, J.R. (1991) Diagnosis and treatment of fungal meningitis.
In: W.M. Scheld, R.J. Whitley and D.T. Durack (Eds.), Infections of the central nervous system, Raven Press, New York, NY, pp. 729-739.
[8] Sulahian, A., Nugues, C., Garin, Y.J.F., Pelloux, H., Longuet, P., Slizewicz, B. and Derouin F. (1992) Serodiagnosis of toxoplas- mosis in patients with acquired or reactivating Toxoplasmosis and analysis of the specific IgA antibody response by ELISA, aggluti- nation and immunoblotting. Immun. Infect. Dis., 3: 63-69.
[9] Krick, J.A. and Remington, J.S. (1978) Current concepts in para- sitology Toxoplasmosis in the adult-an overview. New Engl. J. Med., 298: 550-553.
[10] Ruskin, J. and Remington, J.S. (1976) Toxoplasmosis in the Com- promised Host. Ann. Intern. Med., 84: 193-199.
[11] Luft, B.J., Conley, F., Remington, J.S., Laverdiere, M., Wagner, K.F., Levine, J.F., Craven, P.C., Stanberg, D.A., File, T.M., Rice, N., Meunier-Carpentier, F. (1983) Outbreak of central nervous system toxoplasmosis in Western Europe and North America. Lancet, 1: 781-784.
[12] Luft, B.J. and Remington J.S. (1987) Toxoplasmic encephalitis. J. Infect. Dis., 157: 1-6.
[13] Janitschke, K., Hummel, M., Roth, A., Roth, B., E1 Khalifa, M. (1993) Probleme bei der Laboratoriumsdiagnostik der Toxoplas- mose bei einem Herztransplantationspatienten. Klin. Lab., 39: 581-586.
[14] Navia, B.A., Petito, C.K., Gold, J.W.M., Cho, E.S., Jordan B.D. and Price R.W. (1986) Cerebral toxoplasmosis complicating the acquired immune deficiency syndrome: clinical and neuropathol- ogical findings in 27 patients. Ann. Neurol., 19: 224-238.
[15] Weller, P.F. and Liu, L.X. (1993) Eosinophilic meningitis. Sem. Neurol., 13:161 168.
[16] Dismukes, W.E. (1988) Cryptococcal meningitis in patients with AIDS. Infect. Dis., 157: 624-628.
[17] Waterson, J.A. and Gilligan, B.S. 0987) Cryptococcal infections of the central nervous system: a ten year experience. Clin. Exp. Neurol., 23:127 137.
[18] Schermoly, M.J. and Hinterhorn, D.R. (1988) Eosinophilia in coccidioidomycosis. Arch. Intern. Med., 148:895 896.
[19] Perfect, J.R. and Durack, D.T. (1991) Pathogenesis and pa- thophysiology of fungal infection of the central nervous system. In: W.M. Scheld, R.J. Whitley and D.T. Durack (Eds.), Infections of the Central Nervous System, Raven Press, New York, NY, pp. 693-702.
[20] Wehn, S.M., Heinz, E.R., Burger, P.C. and Boyko O.B. (1989) Dilated Virchow-Robin spaces in cryptococcal meningitis associ- ated with AIDS: CT and MR findings. J. Comput. Assist. To- mogr., 13:756 762.
[21] Arumugasamy, N. (1985) Intracerebral cryptococcomas. Ann. Acad. Med., 14: 16-21.
[22] Harper, C.G., Wright, D.M., Parry, G. and O'Connor, M.J. (1979) Cryptococcal granuloma presenting as intracerebral mass. Surg. Neurol., 11:425-429.
[23] Vijahan, N., Bhatt, G.P. and Dreyfuss, P.M. (1971) Intraventricu- lar cryptococcal granuloma. Neurology, 21: 728-734.
[24] Popovich, M.J., Arthur, R.H. and Heimer, E. (1990) CT ofintrac- ranial cryptococcosis: AJNR, 154: 603~506.
[25] Tien, R.D., Chu, P.K., Hesselink, J.R., Duberg, A. and Wiley, C. (1991) Intracranial cryptococcosis in immunocompromised pa- tients: CT and MR findings in 29 cases. AJNR, 12: 283-289.