Embed Size (px)
Citation preview

An Interdisciplinary Health Team Training Program for School Staff in Minnesota Betty Lia-Hoagberg, Paula Nelson, Richard A. Chase
ABSTRACT: This paper describes an interdisciplinary health team training program for school-based clinic staff in Minnesota. The project sought to improve team functioning, level of practice, and health care services at the school sites. Participants were inferdisci- plinary staff members,from clinics in senior high, middle, and elementary schools. The program consisted offurther development in team training knowledge and skills and educational sessions on issues identified by participants. Evaluations indicated participants reported greater knowledge and improved team functioning experiences from the team training. Gains also were shown in knowledge and skills in specific school topic areas such as violence, resiliency, working with resistant families, and self-care. The program could serve as a model for other interdisciplinary school health team training. (J Sch Health. 1997;67(3):94-97)
chools are faced with increasing numbers of children S that suffer from health care problems and lack of access to health care services.'.2 These problems often are signifi- cant and affect children's ability to perform well academi- cally.-' To address these needs, schools increased the number of health professionals and developed programs and services to work with the children and their fa mi lie^.^ Examples of these services and staffs included school- based health centers, child study teams, and others. These special programs of services are composed of interdiscipli- nary and interagency teams that include various health and other school professionals. The primary goal of these teams is to provide expanded access to health services for high- risk student pop~lations.~ A recent statewide institute for school health personnel in Massachusetts indicated that professional development programs are valued by partici- pants and add to their knowledge, skills, and work with children.6
There is greater recognition that school districts and school-linked services must change the ways they interact with families and community agencies.' Professionals also would be more willing to work and could be more effective with high-risk children if their training gave them skills and relevant experiences, and the setting rewarded them.* In addition, existing professional education programs often fail to teach professionals to work co l l ab~ra t ive ly .~ Although school interdisciplinary teams have existed for years, little information is available on their training for effective functioning.
Minnesota developed one of the first school-based clin- ics in the country in 1973. Currently, 16 clinics operate in the Minneapolis and St. Paul metropolitan school districts.'" Although the school systems have long-standing involve- ment in school-based health care, little interdisciplinary training has been offered to the diverse staff in these programs. This article describes the Minnesota Interdisciplinary Staff Development Project for selected school-based clinic staff in these two cities.
Betty Lia-Hoagberg, RN, PhD, Associate Professor, University of Minnesota, School of Nursing, 308 Harvard St. SE, Minneapolis, MN 55455; Paula Nelson, RN, MS, Project Coordinator, Minnesota Dept. of Health. 71 7 Delaware St. SE, Minneapolis, M N 55455; and Richard A. Chase, PhD, Senior Research Consultant, Wilder Research Center, 1295 Bandana Blvd. N. Suite 210, St. Paul, MN 55108. This project was funded by Maternul und Child Health Bureau grant #4 MCJ 27-SHOI-01-01, This article was submitted August 5, 1996, and revised and accepted for publi- cation December 23. 1996.
PROGRAM BACKGROUND Program Coals and Objectives
A Healthy Schools, Healthy Communities School Health Initiative grant was awarded through the federal Maternal and Child Health Bureau to the Minnesota Dept. of Health and the University of Minnesota School of Nursing in October 1994. The grant was used to develop a model to train school-based teams for interdisciplinary team function and improved delivery of care. The premise of the grant was that improved level of knowledge and skills would enhance the quality of care offered to students. Specific project goals were:
1) to design and implement a model interdisciplinary team training curriculum for school-based and school- linked clinics to improve the level of practice at such sites,
2) to improve health care services provided in school- based and school-linked clinics, and
3) to improve the functioning of interdisciplinary and interagency teams as they provided health care services in school settings.
Theoretical Basis Several theoretical components were used as a basis for
planning the foundation of the program. First, information was used on interdisciplinary team building since this theo- retical base was central to the training project."-12 These strategies included team-building, developmental transition characteristics of teams, dynamics of problem-solving and decision-making in interdisciplinary groups, practice in team decision-making, role socialization, role overlap, and role conflict.
Second, modern adult learning theory identified by KnowlesL4 was used to work with the professional interdis- ciplinary teams. Basic principles from the work suggest that adults come into the learning setting with specific learning needs, that adult's orientation to learning is life- centered, and that experience is the richest resource for adults' learning. The third theoretical component was the use of Prochaska and DiClemente's model of behavior change.'s,'6 Information on behavior change was included in the curriculum because the interdisciplinary teams conduct numerous assessments and interventions with students and families to promote health behaviors. Knowledge and application of the six stages of behavior change - precon- templation, contemplation, preparation, action, mainte- nance, and termination - were discussed to assist team
94 Journal of School Health March 1997, Vol. 67, No. 3

members with integrating the information into their prac- tice and services.
PROGRAM DEVELOPMENT The one-year project officially began in January 1995,
with the hiring of the project coordinator and selection of the project advisory committee. With input from the committee, plans were made that included a needs assess- ment, team participation, curriculum/program implementa- tion, and selection of faculty.
Needs Assessment A needs assessment of the staffs of school-based health
centers was conducted in the Minneapolis and St. Paul public schools. Of the 122 school health staff who received the needs assessment, 55 (45%) responded. Respondents included nurse practitioners, social workers, school nurses, clinic managers, nutritionists, health educators, medical assistants, and receptionists. Respondent experience in a school-based or school-linked clinic ranged from three months to 22 years. Respondents were asked to identify how the needs of students had changed since they began working in a school setting. Responses noted increased family disruption, decreased parental involvement, increased poverty, conflict, violence, earlier sexual activity, increased risk-taking behavior, and more racialkultural diversity. The school-based health staff also identified major issues they wanted addressed in the curriculum of the training sessions.
Team Participants The original intent was to design a team selection
process and accept applications from teams interested in participating. However, due to the tight timeline imposed by the grant, that approach was not possible. Administrators from the Minneapolis and St. Paul school districts identified two teams from each city who were interested in participating in the project. Two teams were from health centers in senior high schools, one team was from a middle school, and the other was in an elementary school. Approximately 10% of participants were part of the first school-based clinics established in St. Paul in the early 1970s. Altogether, 24% had worked for 11 years or more in school-based clinics. Forty-eight persons participated in the project, and the four teams each consisted of 8-14 members. Attendance at the sessions varied, and approxi- mately 25 participants regularly attended all the sessions. Ten participants attended only the team-building sessions. The schools or sponsoring agency were reimbursed for the time participants attended the training sessions and were away from their jobs.
Curriculum/Program Design/Faculty The cumculum for the training sessions focused on 1)
interdisciplinary team-building process and analysis and 2) major educational areas identified by respondents that would provide additional information and skills to address the changing needs of students.
Interdisciplinary team-building training and analysis were conducted in two full-day sessions halfway through the project. Sessions were planned by the project coordina-
tor and a team-training specialist with a doctoral degree and extensive team-building experience in educational environ- ments. Session content consisted of assessing team effec- tiveness, team development, shared mission and goals, group norms, effective communication, and problems-solv- ing skills. Content was presented by the trainer through brief lectures. Following the lectures, participants generated ideas specific to their school settings through brainstorming and discussion. Practical exercises allowed teams to apply the knowledge, identify problem areas, and receive feed- back from other participants.
The second part of the cumculum included nine three- hour educational sessions to improve knowledge, skills, and intervention strategies, and to assist staff in dealing with students changing needs. Topic areas identified on the needs assessment and incorporated into the curriculum included behavior change theory, family centered services in schools, violence prevention, conflict resolution, resiliency models and application, cultural competence, working with difficult families, mental health and referral, and self-care strategies for professionals working with high-risk youth and families. All workshop sessions were videotaped and made available to the participating schools and other schools.
Faculty were selected from academic and private prac- tice settings based on level of expertise in the topic area and familiarity with school-based health care. Faculty were requested to present current information that incorporated adult learning principles and used innovative, multi-media teaching strategies such as case studies, role-playing, brain- storming, and video presentations.
Scheduling sessions at a time when most team members could attend presented a major challenge. Scheduling the sessions from 1-4 pm allowed participants to fulfill their school responsibilities and still be available for evening commitments.
cost Major program costs included salary for the project
director, stipends for participants which were paid to the employing schools, faculty salaries, a subcontract for the evaluation, and additional funds for rental of classroom space, food for the sessions, and paper. The grant covered program costs. However, a great deal of negotiation was needed to keep expenditures within the budget.
PROGRAM EVALUATION The evaluation was conducted by Wilder Research
Center of St. Paul under a subcontract with the Minnesota Dept. of Health. Purposes of the evaluation were 1) to determine the effectiveness of the interdisciplinary team training, 2) to determine the knowledge and skills gained by participants from the nine educational sessions, and 3) to identify how participants expected to use the information in their future work, and how they felt the training would affect student health services.
Two pretraining and nine post-training questionnaires were developed to assess participants knowledge, skills, and responses. The first pretraining questionnaire focused on objectives of sessions one-four, and the second covered team-building and education sessions five-nine. The post-
Journal of School Health * March 1997, Vol. 67, No. 3 * 95

training questionnaires examined change in participant knowledge and skills on the objectives, ways they could use what they learned, and their assessment of the instruc- tor and session content. Post-training questionnaires were administered at the end of each session.
Thirty-three participants completed pretraining question- naires and estimated their own level of competence in the various topic areas. Highest areas of competence were in mental health intervention and conflict management and areas of least competence were in cultural competence, resiliency, and behavior change.
Team-Building Competencies Prior to training. When asked to define characteristics
of a good team, nearly all participants mentioned open communication as a key. Shared vision, respect, and valu- ing other team members roles also were mentioned by approximately half the group. Forty-five percent estimated their competence on the team-building issues of communi- cation and team roles as four or five on a six-point scale. The most positive experience identified by participants was their own commitment to the team approach and the extent of shared commitment to their own clinic school health teams. Seventy-one percent said staff in their setting gener- ally functioned as a team at a four on a six-point scale, Lower ratings were given to items such as the adequacy of time to hold meetings, and the adequacy of space and facil- ities. Very low ratings were given to the availability of technological links such as e-mail to facilitate team communication.
Participants were asked to name specific improvements they would like in their own team process. One-third said they would like to see communication skills improved; another one-third said they would like to have more time together at regular meetings; and other comments addressed the need for role clarification, more structure in the team process, and greater accountability.
Post-training. Participants reported their experiences as a team member improved as a result of the team-building training. Comparison of pretest and post-test results of experiences as a team member indicated marked improve- ment in level of trust, increased feelings of respect and support, greater understanding of their own and others’ roles, and higher shared commitment to their clinic. Eighty- five percent also reported they increased their understand- ing of characteristics of an effective team, their ability to give positive affirmations and constructive requests for change, and improved team-building skills. One key
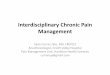
Table 1 Participant Learning in Educational Sessions
Topics Four-Point Scale Behavior change 3.2 Family-centered services 3.0 Violence preventionheduction 3.5 Cultural competence 3.3
Working with resistant families 3.4 Resiliency in children and youth self-care for team members Mental health needs of students’
Conflict management’ 2.9
3 - 4 3- 4 2.1
* Competencies were rated highest prior to fraining
achievement by team members was to articulate a mission and purpose statement for their own team.
Knowledge and Ski l ls in Educational Sessions
For each educational sessions, participants were asked to rate their response to various aspects of the session on a four-point Likert-type scale. The following results reflect participant responses and indicate that their highest learn- ing occurred in sessions dealing with violence and resiliency (Table 1).
Behavior change. Participants rated learning from the training on behavior change as 3.2 on a four-point scale. Almost all (97%) said they increased their knowledge of the six stages of behavior change. Health care professionals reported higher learning than health education or mental health professionals.
family centered services. Overall, participants rated their learning as three of four on this topic. All respondents reported improving their ability to explain the concept of family centered services which was presented as a holistic approach of actively doing outreach to involve parents in their children’s lives and the school.
Violence. The highest ratings (3.5) were given to learn- ing to define violence beyond physical violence, under- standing the impact on children of growing up in a violent home, and the relevance to adolescent health.
Cultural competence. More than 90% of participants rated this topic 3.3 of four. The highest rated objective was improvement in their ability to define cultural complemen- tarity and its importance in a therapeutic alliance.
Conflict management. Learning scores were low (2.9) but were rated among the highest prior to the training.
Working with resistant families. More than half of respondents reported a 4.0 on each objectives with an aver- age of 3.4 of four. The objectives included learning to define resistance within a family system, intervention strategies to increase collaboration and cooperation with families, and how professionals who work with these fami- lies can stay solution-focused and positive.
Resiliency. Resiliency was defined as the characteristic that helps children succeed despite adversity in their lives. The highest average learning was reported for this session; 95% to 100% of participants reported learning at three or four on four of five objectives. All said they had increased their ability to define resiliency and identify characteristics of a resilient child.
Self-care. The focus was on self-care of team members. Eighty-nine percent reported they increased their under- standing of how burnout, stress, and grief are related, and rated as three or four how to identify problems for them- selves and their coworkers.
Mental health. Participants reported the highest pretraining competencies on assessing and dealing with mental health needs of students. Scores for amount of skills, knowledge, and abilities were lowest (2.7) of all the training sessions.
In summary, participants’ satisfaction level with the workshop content, instructors, and usefulness of training were highly related to the level of learning they experi- enced from the training. The most helpful teaching strate- gies used by the instructors were use of stories, examples,
96 Journal of School Health March 1997, Vol. 67, No. 3

analogies, and metaphors which made the information more relevant. Participants appreciated the instructors’ knowl- edge and depth in the subject area, their responses to ques- tions, honesty about issues, humor, and handouts. Overall, the ratings for instructors averaged between three and four on a four-point scale.
Expected Use of New Knowledge and Skills and Effect on Services
The funded project was limited to one year. Therefore, participants were asked to rate the extent to which they expected to be able to use or apply the interdisciplinary team training and the knowledge or skills gained in each educational session.
In the interdisciplinary team-building area, participants indicated they would be able to use or apply most of the training “somewhat” or “a great deal.” They expected to use what they learned about characteristics of an effective team, their improved team-building skills, their increased ability to give positive affirmations and constructive requests for change, their understanding about the roles of other team members, and how values and norms affect teamwork.
Expected use of information from the nine educational sessions also was rated highly. Application of resiliency training was rated highest, and most reported they would be able to apply the information “a great deal.” Other sessions with future high application ratings were understanding and dealing with violence, working with resistant families, and cultural competence.
Participants were asked how and in what ways they expected to use the information and how their work with students would be different as a result of the training. Overall, a third of participants said they would use their increased knowledge of the content areas in their work with students such as doing violence prevention efforts, and reinforcing strengths for resilience. Almost one-third said that their face-to-face contact with students and resistant families would improve as a result of the training. An addi- tional third reported they would be more sensitive to students as a result of the training.
CONCLUSION Although the interdisciplinary health team training
included a small number of participants, evaluation results are encouraging. By participating in the training, team members from established school-based teams gained addi- tional team functioning knowledge and skills. The training also provided information and increased skills to work with children and families with highly complex problems. The training structure and content especially were beneficial to new team members who had been on an interdisciplinary team for five years or less. Unanswered questions are the extent to which these improvements last over time and their relationship to improved health outcomes for students.
The training model could be improved and extended through a number of changes. The scheduling problems could be reduced by conducting a two- or three-day train- ing workshop in a retreat format. Expenditures could be
controlled by charging for the workshop but offering continuing education credits. In addition, speakers could be used from within the school district, standard evaluations done rather than use professionals, and school staff do conference planning rather than use a consultant. The eval- uation process could be adjusted so evaluations were conducted at six months or one year after the project to measure actual team member behavior and selected student health outcomes.
The training focus on communication and team-building was appropriate and worthwhile for participants. Communication skills are of key importance for effective team functioning and may warrant expended attention in future trainings. Overall, the training participants were opti- mistic about their own potential to use or apply their new knowledge and skills gained through the training, and the
H project should be replicated in other settings.
References 1. Kleinman JC. Health status indicators for school-age children. In
Wallace H, Patrick K, Parcel G, Igoe J, eds. Principles and Practices of Student Health. Oakland, Calif Third Party Publishing Co; 1992: 1-9.
2. Rogers CC, Bianchi SM. The socioeconomic status of America’s children and youth. In Wallace H, Patrick K, Parcel G, Igoe J , eds. Principles and Practices of Student Health. Oakland, Calif Third Party Publishing Co; 1992:lO-29.
3. Girouard SA, Igoe JB. A primary health care perspective on comprehensive children’s services. In Levin RA, ed. Greater than the Sum: Professionals in a Comprehensive Services Model. Washington, DC: ERIC Clearinghouse on Teacher Education monograph 17; 1994: 167- 178.
4. US Dept of Health and Human Services, Public Health Service. Healthy People 2000: National Health Promotion and Disease Prevention Objectives. Washington, DC: US Dept of Health and Human Services publication PHS 91-50213; 1991.
5 . Juszczak L, Fisher M, Lear JG, Friedman SB. Back to school: Training opportunities in school-based health centers. Develop Behav Pediatr. 1995; 16(2): 101-104.
6. Piessens PW. King MC, Ryan J, Millette B, Sheetz A, Douglas IB, et al. A statewide institute to deliver professional development programs to school health personnel in Massachusetts. J Sch Health.
7. Jehl J, Yirst M. Getting ready to provide school-linked services: What schools must do. The Future of Children. Los Altos, Calif The David and Lucille Packard Foundation. 1992;2( 1):95-106.
8. Schoor E. Within Our Reach: Breaking the Cycle of Disadvantage. Garden City, NY: Anchor PresslDoubleday; 1989.
9. Bearinger LH, Gephart J. Interdisciplinary education in adolescent health. J Paediatric Child Health. 1993;29(suppl l):SlO-S15.
10. Zimmerman D, Reif CJ. School-based health centers and managed care health plans: Partners in primary care. J Public Health Manage Pract.
11. lvey SL, Brown KS, Teske Y, Silverman D. A model for teaching about interdisciplinary practice in health care settings. J Allied Healrh.
12. Parker GM. Team Players and Teamwork. San Francisco, Calif Jossey-Bass Publishers; 1990
13. Quick TL. Successful Teambuilding. New York, NY: American Management Association; 1992.
14. Knowles M. The Adult Learner: A Neglected Species. Houston, Texas: Gulf Publishing; 1978.
15. Prochaska JO, DiClemente CC. The Transtheoretical Approach: Crossing the Traditional Boundaries of Therapy. Homewood, 111: Dow Jones Irwin; 1984.
16. Prochaska JO. Assessing how people change. Cancer.
1995;65(5): 176-180.
1995;1:33-39.
1988; 17(3): 189-195.
I991 ;67:805-807.
Journal of School Health March 1997, Vol. 67, No. 3 9 7