Embed Size (px)
Citation preview

Research PaperHead and Neck Oncology
Int. J. Oral Maxillofac. Surg. 2007; 36: 533–540doi:10.1016/j.ijom.2007.03.003, available online at http://www.sciencedirect.com
An experimental study of theuse of hyperbaric oxygen toreduce the side effects ofradiation treatment formalignant disease
R. A. Williamson: An experimental study of the use of hyperbaric oxygen to reduce theside effects of radiation treatment for malignant disease. Int. J. Oral Maxillofac. Surg.2007; 36: 533–540. # 2007 International Association of Oral and MaxillofacialSurgeons. Published by Elsevier Ltd. All rights reserved.0901-5027/060533 + 08 $30.00/0 # 2007 Interna
tional Association of Oral and Maxillofacial SurgeoR. A. WilliamsonFaculty of Medicine and Dentistry, Universityof Western Australia, 17 Monash Avenue,PERTH WA 6000, Australia
Abstract. Hyperbaric oxygen (HBO) has been used for more than 20 years to assistwound healing in the treatment of the more severe complications associated with theside effects of therapeutic radiation treatment. A prospective study was performedin an irradiated rat model to determine whether HBO is effective in reducing thelong-term side effects of therapeutic radiation treatment on normal tissue, whengiven 1 week after the completion of the radiation treatment. The experimentalmodel was designed to simulate a fractionated course of therapeutic radiation that iscommonly used in the treatment of cancer of the mandible. One week followingcompletion of the radiotherapy, the animals underwent a 4-week course of HBOtreatment, and two animals from each group were killed at 8-week intervals until theend of the experiment at 36 weeks. Histological sections of tissue clearly showedcontinued growth of teeth and maintenance of specialized tissues, such as salivarygland and bone, in the treated group compared to the non-treated group. Thisexperimental model demonstrated that HBO is effective in reducing the long-termside effects of therapeutic radiation treatment in normal tissue, when given 1 weekafter the completion of the radiation treatment.
Key words: hyperbaric oxygen; therapeuticradiation; tooth growth; salivary gland; bone.
Accepted for publication 5 March 2007
Therapeutic radiation has been used forthe treatment of cancer and other diseasesfor nearly a century. Over the past 20years, hyperbaric oxygen (HBO) has beenused to assist wound healing in the pre-vention and treatment of the more severecomplications associated with the side
effects of therapeutic radiation treatment(TRT). The use of HBO treatment(HBOT) is based on the premise thatincreased oxygen tissue tension aidswound healing by increasing the hypoxicgradient and stimulating angiogenesis andfibroblast differentiation. As it takes up to
6 months for a hypoxic state to develop intreated tissue, following radiation treat-ment, current recommendations for HBOstate that it is not effective until after thistime. During this 6-month period, imme-diately following TRT, many specializedtissues in or adjacent to the field of irra-
ns. Published by Elsevier Ltd. All rights reserved.

534 Williamson
diation, such as salivary glands and bone,are damaged due to a progressive thicken-ing of arteries and fibrosis, and these tissuesare never replaced. Currently, HBO is usedto treat the complications of TRT, but itwould be far better if they could be pre-vented. With this in mind a prospectivestudy was performed in an irradiated ratmodel to determine if HBO is effective inreducing the long-term side effects of ther-apeutic radiation treatment on normal tis-sue, when given 1 week after thecompletion of the radiation treatment.
Materials and methods
Experimental animals
For the purpose of this research project,the Animal House at Royal Perth Hospitalsupplied and supervised the well being of30 male Wistar rats (250–300 g). The ratswere held under a 12-h light–dark cycle at22 � 2 8C. All experimental surgical pro-cedures were carried out under licencefrom the Animal Ethics Committees ofRoyal Perth Hospital and The Universityof Western Australia in accordance withNational Health & Medical ResearchCouncil of Australia guidelines.
The rats were divided into four groups:
(1) a
ir-breathing control group (Control)– no treatment (six rats);(2) H
BOT only group (HBO) – (six rats); (3) T RT only group (Rx) – (eight rats); (4) T RT plus HBOT group (Rx + HBO) –(10 rats).
Experimental time table
The experiment ran for 253 days (36weeks). Day 1 was nominated as the firstday of radiation treatment. The experi-mental time table was as follows.
(a) A
simulated therapeutic course ofradiotherapy was given to the mand-ible of Groups 3 and 4 animals over 15days.(b) O
ne week recovery time for animals. (c) F our weeks of HBO for Groups 2 and4.
(d) T wo animals from each group werethen killed at 85 days, 141 days and253 days.
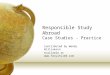
Fig. 1. Tetracycline staining (magnification 17.5�).
Irradiation protocol
A 42-Gy fractionated course of simulatedtherapeutic radiotherapy was given to theanimals in Groups 3 and 4 over 15 dayswith 6 Gy being given on each of days 1, 3,
5, 8, 10, 12, 15 of the experiment. A 250-kVp Siemens Stabilipan DXRT Orthovol-tage Therapy machine was used with thefollowing specifications:
� d
istance from source to animal skinsurface – 25 cm;� k
Vp – 250; � m A – 10; � fi lter – half value layer of 0.5-cm cop-per;
� m easured dose rate – 1.30; � p rescribed dose – 6.0 Gy; � ti me to achieve dose – 4 min 37 s.Hyperbaric oxygenation
One week post radiotherapy, to allowrecovery time for the experimental animals,Groups 2 and 4 underwent a 4-week courseof HBO, similar to that used by MARX
19,20
to treat human subjects with osteoradione-crosis. This treatment course was carriedout in a specially built HBO chamber,supplied by the Royal Australian Navy,for experimental HBO treatment of smallanimals. The course involved the ratsundergoing 20 treatments of HBO. Ahyperbaric treatment is defined as breathing100% oxygen for 90 min at 2.4 ATA19,20. AHBOT, also called a dive, consists of:
(1) d
escent time – 15 min; (2) b ottom time – 90 min of HBO under2.4 ATA pressure;
(3) a ssent time – 15 min.As the animals in this experiment didnot undergo a surgical procedure andtherefore did not need postoperativeHBO, only 20 treatments were given to
initiate a wound healing response, as sug-gested by DAVIDSON & MUSTOE
7.
Tetracycline
The use of low-dose tetracycline as ahistological hard-tissue marker has beenwell established and allows clear evidenceof continued hard-tissue growth in experi-mental animals10. A veterinarian-approved tetracycline was administeredto all rats as a marker of tooth growth.The tetracycline is taken up by growingteeth and can be seen histologically asbands of growth, like growth rings in atree section. Tetracycline is available, as aVeterinary Approved Drug (Alamycin), invials of 200 mg/ml for intravenous/intra-muscular/intraperitoneal use in Australia.Three treatments of 5 mg/rat/day (20 mg/kg)10 of Alamycin (oxytetracycline) wereadministered as an i.p. dose every 4 weeks,beginning on Day 22, the same day asHBOT commenced, and continued for thelength of the experiment. The dosage of20 mg/kg of tetracycline for animal usehas been reported by FROST
10.
Removal of mandible and preparation of
samples
At necropsy, the mandibles were resecteden bloc, then hemi-sected through thefibrous symphysis, and the lower incisorteeth removed. The specimens were storedin formalin and then embedded in waxblocks, prior to sectioning and then stain-ing. Two slides of consecutive tissue slicesfrom each specimen group, which bestrepresented each tissue type, were selectedfor specific analysis. One of the slides hadbeen stained with haematoxylin and eosin

HBO on side effects of radiotherapy 535
Fig. 3. Examples of salivary gland tissue from Group 3 to 6 (Rx), stained with (a) H&E and (b)LFB, showing the reduction in volume of salivary gland tissue and thickening of arterial wall,253 days after TRT. Note that (a) the H&E stain does not demonstrate fibrosed salivary glandclearly; (b) the LFB stain clearly demonstrates the residual fibrosed salivary gland.
Fig. 2. Growth rate of teeth comparing the four groups. SDs are shown. The growth rate ofGroup 4 is more than twice that of Group 3.
(H&E) and a second consecutive slice oftissue was stained with Luxol Fast Blue/Cresyl Fast Violet (LFB). The LFB wasparticularly useful in demonstrating thepresence of salivary gland tissue, espe-cially in those sections where the salivarytissue was undergoing radiation fibrosisand was very difficult to see in H&Esections.
An incisor tooth from each dead animalwas imbedded in an epoxy resin. Eachembedded tooth was then ground to halfits thickness and the ground side of thetooth glued to a glass slide. Each slide-mounted half tooth was then furtherground down to achieve a tooth slice30 mm thick. The mounted tooth sectionswere viewed at 17.5 magnification usingfluorescence microscopy with a narrow-band, blue-light filter block (450–490 nm). After image acquisition, the fileswere analysed by Metamorph Imaging 6.0Software System by the IAAF, and used tocarry out both histomorphological analy-sis and histomorphometric quantificationof the images.
Results
Teeth
Sections of teeth were viewed under UVlight and clearly showed continued growthrings of tetracycline in Groups 1, 2 and 4,with little growth shown in Group 3.Figure 1 shows an example of the tetra-cycline staining and measurement of thebanding. As the tetracycline was givenover 3 days, every 4 weeks, the distancebetween the bands represents 25 days’tooth growth. Figure 2 compares thegrowth rate of teeth between the fourgroups. The positive effect of HBO ongrowth rate can be seen in Group 4(Rx + HBOT), being twice the growth rateof the non-treated Group 3 (Rx) teeth.
Salivary gland
Histological sections of tissue taken fromthe angle of the mandible clearly showedmaintenance of specialized tissues, suchas salivary glands and osteoblasts, in thetreated group compared to the non-treatedgroup of animals at the end of the experi-ment. Figure 3a shows an example ofsalivary gland tissue from Group 3 (Rx)stained with H&E taken from a rat killed atDay 253 (36 weeks), and Fig. 3b shows aconsecutive slice from the same animalstained with LFB. Figure 4a shows anexample of salivary gland tissue fromGroup 4 (Rx + HBOT) stained with H&Etaken from a rat killed at Day 253

536 Williamson
Fig. 4. Examples of salivary gland tissue from Group 4 to 9 (Rx + HBOT), stained with (a) H&Eand (b) LFB, showing the retention in volume of salivary gland tissue, 253 days after TRT andHBOT. H&E and LFB clearly demonstrate healthy salivary gland tissue.
Fig. 5. Number of salivary gland acini at Day 253. SDs are shown. Group 4 is comparable to thecontrols, in contrast to Group 3.
(36 weeks), and Fig. 4b shows a consecu-tive slice from the same animal stainedwith LFB. To analyse the salivary glandtissue, this study employed a point-count-ing technique called the Multipurpose TestSystem, which is based on the stereologi-cal principles originally described byBOLENDER & WEIBEL
4. Figure 5 tablesthe number of salivary gland acini atDay 253 (36 weeks). The presence andquantity of salivary gland acini in Group4 (Rx + HBO) were seen to be comparableto those of Groups 1 (Control) and 2 (HBO),whereas Group 3 (Rx) had less than 50% ofthe quantity of salivary gland acini. Group 3(Rx) had significantly less than the otherthree groups (p < 0.05, ANOVA).
Bone
Figures 6 and 7 show an example of bonefrom Group 3 (Rx) and Group 4(Rx + HBO), respectively, taken from arat killed at Day 253 (36 weeks) andstained with H&E. In this study the per-centage of lacunae occupied by osteo-blasts was used to quantify the vitalityof the bone over the time frame of theexperiment. It is immediately clear thatthere are far fewer lacunae occupied byosteoblasts in Group 3 (Rx) compared tothe other three groups. Group 4(Rx + HBOT) exhibits areas of new bonegrowth (reversal lines), whereas Group 3(Rx) has no areas of new bone growth.Figure 8 shows the percentage of lacunaeoccupied by osteoblasts in each group atDay 253. The percentage of lacunae occu-pied by osteoblasts in Group 4(Rx + HBOT) (87.5%) is comparable tothat of Groups 1 (Control) (96.3%) and2 (HBOT) (96.3%). In Group 3 (Rx), thepercentage of lacunae occupied by osteo-blasts is only 47% of that of Group 4(Rx + HBO) and only 43% of the controlgroup.
Discussion
Current HBO protocols are designed tomanage some of the complications ofTRT, particularly osteoradionecrosis(ORN). Prior to the introduction of HBOT,conditions such as ORN were difficult totreat surgically as operating on exposedbone lead to further soft-tissue breakdownand exposure of more irradiated bone.Most treatment regimes consisted of tetra-cycline mouthwash and a conservativeapproach to sequestrectomies. The intro-duction of HBOT to manage ORN byauthors such as MARX
19 gave surgeonsthe ability to operate on patients withexposed ORN bone and to remove teeth

HBO on side effects of radiotherapy 537
Fig. 6. Example of bone from Group 3 to 8 (Rx) (H&E) showing most of the lacunae are empty,with few osteoblasts present, 253 days after TRT. Group 3 (Rx) has no areas of new bone growth.
with a reduced risk of developing ORN.HBOT has been shown to induce angio-genesis and fibroblast differentiation17
with resulting revascularization of thehypoxic tissues. But HBO does notretrieve dead or dying tissue such as sali-vary gland and bone that lies within thefield of radiation; it simply revascularizesfibrous hypoxic, hypocellular and hypo-vascular tissue. Once the specialized tis-sues are lost, they are lost forever. WhileHBOT gives surgeons the ability to treatORN, using current protocols where
Fig. 7. Example of bone from Group 4 to 9 (Rx +occupied by osteoblasts, 253 days after TRT and Hnew bone growth (reversal lines) compared to Fibone growth.
patients wait at least 6 months beforethe HBOT, it does not prevent the com-plications associated with TRT and sub-sequent permanent loss of specializedtissues such as salivary gland and bone.
The MARX HBO18 protocols for thetreatment of ORN have been in use forover two decades. Although there havebeen many articles reporting the successof this treatment protocol over this time19,from the start there has been controversyover its efficacy, with a number of alter-native treatment protocols offered for
HBOT) (H&E) showing that all the lacunae areBOT. Group 4 (Rx + HBOT) exhibits areas of
g. 6, Group 3 (Rx), which has no areas of new
ORN. In 1989, BALOGH & SUTHERLAND3
reviewed the then current treatmentregimes for ORN and reported that therole of hyperbaric oxygen remained con-troversial, with this treatment being com-plex and time-consuming with results thatare confounded by the concurrent use oflocal antiseptic/antibiotic measures andsurgery. Although the pathogenesis ofORN may often involve vascularhypoxia20, ORN was recently suggestedto be triggered by a predominantly fibro-atrophic mechanism1,6,8. DELANIAN &LEFAIX
8 reported the complete healing ofsevere ORN for the first time using anantifibrotic treatment with combined pen-toxifylline, tocopherol and clodronate in12 patients. They considered that thereduction of microscopic radiation-induced fibrosis, which is always asso-ciated with the necrotic process, mayallow tissue restoration. This, in turn,may reverse defective osteoblastic heal-ing, with clodronate, a well known bispho-sphonate, inhibiting osteoclastic bonedestruction22. GAL et al.11 reported thatmicrovascular reconstruction of mandib-ular ORN can be successfully achievedwithout the use of perioperative HBOtherapy. In 2004, in a double-blind trialwhich had to be stopped for potentiallyworse outcomes in the HBO arm, ANNANE
et al.2 concluded that patients with overtmandibular ORN did not benefit fromhyperbaric oxygenation. Clearly, furtherstudies, such as this one, are needed toassess the efficacy and safety of HBO inORN.
Since we know that HBOT inducesendothelial proliferation and angiogen-esis, there has been a real concern thatit may accelerate the development orgrowth rate of mitotic cells. The possibi-lity of tumour cell stimulation has beenraised but has never been proven. Wellcontrolled studies involving animals andhumans with various malignancies,including cancer models, have shownno difference between HBOT and non-HBOT groups with respect to tumour size,metastasis and long-term survival14,16,21.The most comprehensive review of thissubject was given in a presentation byProfessor FELDMEIER, in 20019. He listed73 papers from the literature, dating from1966 to 2001, including both animal stu-dies and human follow-up studies. Heconcluded that ‘The available publishedevidence strongly suggests that intermit-tent HBOT has no enhancing effect oncancer primary or metastatic growth.Likewise, there is no credible evidencethat HBOT is an initiator or promoter ofcancer de novo.’

538 Williamson
Fig. 8. Percentage of lacunae occupied by osteoblasts at Day 253. SDs are shown. Group 4 iscomparable to the controls, in contrast to Group 3.
The mechanism by which HBOachieves angiogenesis and fibroplasia inirradiated tissue has now been eluci-dated18,19, and found to be stimulated bya similar oxygen-gradient phenomenon tothat which KNIGHTON et al. and SILVER
reported to be central in the angiogenesisand fibroplasia of normal wound heal-ing17,25. The HBO creates an oxygen gra-dient that is steep across a short distancebetween irradiated and normal tissue.Such steep oxygen gradients are the phy-sio-chemotactic factor attracting wound-regulating macrophages to a wound17,25.Steep oxygen gradients, along with thelactate, iron and low pH inherent inwounds, stimulate macrophage-derivedangiogenesis factor and macrophage-derived growth factor, which in turn pro-mote the capillary budding and collagensynthesis of wound healing16. Some otherpossible suggestions for the mechanism ofHBO in wound healing were made byZHAO et al.26 in 1994, who noted a100% reversal of the healing deficitinduced by ischaemia in experimental ani-mals when wounds were treated with HBOand growth factors simultaneously.Clearly, this synergistic response sug-gested a direct interaction between oxygenand growth factors rather than theresponse expected from restoring ade-quate nutrition to compromised cells.The nature of this interaction was deducedby BONOMO et al.5 who reported a statis-tically significant rise in the production ofplatelet-derived growth factor (PDGF)receptor protein I in ischaemic woundsthat were treated simultaneously with bothHBO and PDGF. DAVIDSON & MUSTOE
7
have stated that this finding leads strongsupport to the concept that HBO functionsas an intracellular signalling transducerand thus is a modulator of gene function.SIDDIQUI et al.24, who documented thatHBO treatment produces hyperoxic (notphysiologic) concentrations in ischaemic
wounds and that oxygen concentrationfalls promptly to pre-treatment levels inischaemic tissue, also demonstrated a pro-gressive increase in the real oxygen con-centration in ischaemic tissue when it waschallenged with 100% oxygen at 1 atm aswell as a more rapid washout of oxygenfrom tissue after serial HBO treatments.The magnitude of these changes was pro-portional to the number of HBO treat-ments. DAVIDSON & MUSTOE
7 attributedthese acute changes in the responsivenessof ischaemic tissue to serial HBO treat-ments, and suggested prompt but transientproduction of a potent local vasodilator.
It is now becoming increasingly appar-ent that hyperoxia, as well as hypoxia,induces a distinct set of cellular responses.As HBO has been shown to modify theexpression of vascular endothelial growthfactor (VEGF) and PDGF receptors, it hasbeen suggested by DAVIDSON & MUSTOE
7,and HUNT et al.15 that hyperoxia may actvia an oxygen-sensing transduction path-way to impact on other important regula-tors of cell growth and metabolism. Therecent papers by HUNT et al.15 and GOR-
DILLO & SEN13 suggest further mechanisms
by which oxygen exerts its vital actions inwound healing. They state that reactiveoxygen species are a constructive force inwound healing. In the right quantity andplace, they promote angiogenesis and col-lagen synthesis. GIBSON et al.12 confirmedthat HBO can be angiogenic and added,because the effect was inhibited by anti-VEGF antibody, that it is mediated byVEGF. Since current doctrine is thathypoxia is a key trigger of VEGF expres-sion, and the data that hypoxia does insti-gate VEGF production must be accepted,it fell to SHEIKH et al.23 to show that VEGFprotein levels in actual wounds are raisedby HBO. HUNT et al.15 have thereforeconcluded that both hypoxia and hyper-oxia can promote VEGF activity orrelease. It logically follows that HBO in
normal tissues produces hyperoxia whichin turn promotes VEGF. The experimentaldata mentioned above support the hypoth-esis that transient hyperoxia, when given 1week after completion of TRT, functionsas an intracellular signal transductionagent or modulator of gene function viamore than one signalling pathway, in addi-tion to supplying the critical element forcellular respiration, and reduces some ofthe side effects of radiotherapy. Thishypothesis is summarized in Fig. 9. Theimplications of being able to prevent thecomplications of TRT, rather than treatingthem as is currently practiced, are farreaching. Prevention of the complicationsof TRT will go a long way to improvingthe quality of life of patients who undergothis form of cancer treatment. Thesepatients will therefore not lose specializedtissues such as salivary gland and bone,and this will impact on their ability toretain their teeth and salivary gland func-tion. The patients may then be treated in anormal fashion by dentists and not have toundergo removal of all teeth as a preven-tive measure. In addition, the implicationof the continued growth of teeth in irra-diated animals, when treated early withHBO, as found in this study, suggests aprotective mechanism which may beextrapolated to other tissues such as mus-cle, and will need further investigation.Children receiving TRT, for conditionssuch as rhabdomyosarcoma, may be curedby the treatment but are left with loss ofcontinued growth of all tissues in thetreatment area. Early treatment withHBO, as found in this study with teeth,may well benefit these children with con-tinued growth of normal tissues in thetreated area. Obviously much furtherresearch needs to be done in this area,but this study has certainly indicated thattreatment with HBO reduces the acuteinflammatory damage caused by TRTand thereby increases the preservation ofspecialized tissues, which in turn leads to areduction in the long-term complicationsassociated with TRT.
In summary, this experimental modelhas fulfilled its prime objective of demon-strating that HBO is effective in reducingsome of the long-term side effects of TRTin normal tissue, when given 1 week afterthe completion of the radiation treatment.
Acknowledgements. I would like to thankmy supervisors, Professor John McGea-chie and A/Professor Marc Tennant, fortheir encouragement, guidance, friendshipand support throughout this seeminglyinterminable project.

HBO on side effects of radiotherapy 539
Fig. 9. Wound healing pathway elicited by HBO. This diagram outlines the author’s hypothesis of the molecular pathway of wound healingelicited by HBOT, when given 1 week after TRT, in irradiated tissue. MDAF, macrophage-derived angiogenesis factor; MDGF, macrophage-derived growth factor; PDGF, platelet-derived growth factor; ROS, reactive oxygen species; TGF, transforming growth factor; VEGF, vascularendothelial growth factor.
I would like to thank the followingorganizations for their financial supportof this project:
Australian Dental Research FoundationAustralian and New Zealand Associa-
tion of Oral and Maxillofacial SurgeonsRankine Memorial Foundation
References
1. Aitasalo K, Aro H. Irradiation-inducedhypoxia in bones and soft tissues: anexperimental study. Plast ReconstructSurg 1986: 77: 256–265.
2. Annane D, Depondt J, Aubert P, Vil-
lart M, Gehanno P, Gajdos P, Chev-
ret S. Hyperbaric oxygen therapy forradionecrosis of the jaw: a randomized,placebo-controlled, double-blind trialfrom the ORN96 study group. J ClinOncol 2004: 22: 4893–4900.
3. Balogh JM, Sutherland SE. Osteora-dionecrosis of the mandible: a review. JOtolaryngol 1989: 18: 245–250.

540 Williamson
4. Bolender RP, Weibel ER. A morpho-metric study of the removal of phenobar-bital-induced membranes fromhepatocytes after cessation of treatment.J Cell Biol 1973: 56: 746–761.
5. Bonomo S, Davidson JD, Yu Y, Xia Y,Lin X, Mustoe TA. Hyperbaric oxygen asa signal transducer; upregulation of plate-let derived growth factor-beta receptor inthe presence of HBO2 and PDGF. Under-sea Hyperb Med 1998: 25: 211–216.
6. Dambrain R. Pathogenesis of osteora-dionecrosis. Rev Stomatol Chir Maxillo-fac 1993: 94: 140–147.
7. Davidson JD, Mustoe TA. Oxygen inwound healing, more than just a nutrient.Wound Repair Regen 2001: 9: 175–177.
8. Delanian S, Lefaix JL. Complete heal-ing of severe osteoradionecrosis withtreatment combining pentoxifylline, toco-pherol and clodronate. Br J Radiol 2002:75: 467–469.
9. Feldmeier J. Hyperbaric oxygen: does ithave a cancer causing or growth enhan-cing effect? Proceedings of the EuropeanSociety for Therapeutic Radiology andOncology, Consensus Conference. Lis-bon, Portugal, 2001: 129–146.
10. Frost MH. Tetracycline-based histologi-cal analysis of bone remodelling. CalcifTissue Res 1969: 3: 211–237.
11. Gal TJ, Yueh B, Futran ND. Influenceof prior hyperbaric oxygen therapy incomplications following microvascularreconstruction for advanced osteoradio-necrosis. Arch Otolaryngol Head NeckSurg 2003: 129: 72–76.
12. Gibson JJ, Sheikh AY, Rollins MD,Hopf H, Hunt TO. Increased oxygentension and wound fluid vascularendothelial growth factor levels. SurgForum 1998: 89: 607–610.
13. Gordillo GM, Sen CK. Reactive deri-vatives of oxygen support healing: a newhorizon. Am J Surg 2003: 186: 259–263.
14. Headley DB, Gapany M, Dawson DE,Kruse GD, Robinson RA, McCabe BF.The effect of hyperbaric oxygen ongrowth of human squamous cell carci-noma xenografts. Arch Otolaryngol HeadNeck Surg 1991: 117: 1269.
15. Hunt TK, Hussain MZ, Sen CK. Giveme ROS or give me death. Pressure 2001:30: 10–11.
16. Johnson RE, Kagan AR, Bryant TL.Hyperbaric oxygen effect on experimentaltumour growth. Radiology 1967: 88: 775.
17. Knighton DR, Hunt TK, Scheuen-
stuhl H, Halliday BJ, Werb Z, Banda
MJ. Oxygen tension regulated the expres-sion of angiogenesis factor by macro-phages. Science 1983: 221: 1283–1285.
18. Marx RE. A new concept in the treat-ment of osteoradionecrosis. J Oral Max-illofac Surg 1983: 41: 351–357.
19. Marx RE. Problem wounds in oral andmaxillofacial surgery. In: Davis JC,Hunt TK, eds: Problem Wounds TheRole of Oxygen, 4. New York: ElsevierScience Publications Co. 1988: 65–123.
20. Marx RE. Radiation Injury to tissue. In:Kindwall EP, ed: Hyperbaric MedicinePractice Revised edn. Flagstaff: Best Pub-lishing Co. 2002: 665–723.
21. Nemiroff PM. Effects of hyperbaric oxy-gen in growth and metastases on Lewislung tumours in mice. J HBO 1988: 93:485.
22. Rodan G, Fleisch H. Biphosphonates:mechanisms of action. J Clin Invest 1996:97: 2692–2696.
23. Sheikh AY, Gibson JJ, Rollins MD,Hopf HW, Hussain Z, Hunt TO. Effectsof hyperoxia on vascular endothelialgrowth factor in a wound model. ArchSurg 2000: 135: 1293– 1297.
24. Siddiqui A, Davidson JD, Mustoe TA.Ischemic tissue oxygen capacitance afterhyperbaric oxygen therapy: a new phy-siologic concept. Plast Reconstr Surg1977: 99: 148–155.
25. Silver IA. Cellular microenvironment inhealing and non-healing wounds. In:Hunt TK, Heppenstall RB, Pines E,eds: Soft and Hard Tissue Repair. NewYork: Praeger 1984: 50–66.
26. Zhao L, Davidson JD, Sang CW, Roth
SI, Mustoe TA. Effect of hyperbaricoxygen and growth factors on rabbit earischemic ulcers. Arch Surg 1994: 129:1043–1049.
Address:Raymond Allan WilliamsonFaculty of Medicine and DentistryUniversity of Western Australia17 Monash AvenuePERTH WA 6000 AustraliaTel: +61 8 93467622Fax: +61 8 93467623E-mail: [email protected]