Embed Size (px)
Citation preview
An electromyographic analysis of theupper extremity in pitching
Nick M . DiGiovine, MD, Frank W . Jobe, MD, Marilyn Pink, MS, PT, andJacquelin Perry, MD, Inglewood, Calif.
The upper extremity is vulnerable to in;ury during the baseball pitch because ofthe repetitious nature of the action, the extremes in range of motion, and thehigh angular velocities and torques generated at the shoulder and elbow. Hencethis study was designed to describe the muscle-firing patterns through fine-wireelectromyography in 29 muscle bellies in the upper extremities of skilled pitchersduring the fastball pitch. The results demonstrated that the muscles functionedwith precise timing for [oint stabilization to prevent injury, [oint activation totransfer forces to the ball, and [oint deceleration to dissipate forces after ballrelease. The synchrony of reciprocal and sequential muscle contractionnecessary to accomplish these functions was clearly evident. This study providesa better understanding of the coordinated sequence of muscle activity during thethrowing motion; this understanding is crucial to the development of exerciseprotocols and surgical procedures used for treatment and prevention of shoulderand elbow iniuries in the throwing athlete. (J SHOULDER ELBOW SURG 7992; 7:75-25.)
Pitching is a complex sequence of body movements that result in the rapid propulsion of aprojectile, the ball. Four parameters determinethe effectiveness of a pitcher. These are the abilities to generate velocity, ma inta in accuracy,apply spin, and sustain endurance. Coordinating the integration of these parameters is a highlevel of neuromuscular control. Synchrony ofmuscle contraction is vital to the motion. Effectiveness also requires performance at a levelthat maximally stresses the anatomic elementsinvolved. At work is a delicate balance betweenmobility and stability. The fine line that separates maximum performance and injury is oftencrossed, and shoulder and elbow injuries inpitchers are not uncommon.* Understanding thebiomechanics of pitching is important to preventand treat these injuries.
For the past 12 years the Biomechanics Laboratory at Centinela Hospital and the KerlanJobe Clinic have collected electromyographicdata on muscular activity during the throwingmotion in athletes. The early reports were on
f rom the Biomechani cs Lab oratory, Centinela Ho spital Medical Center, Inglewo od , Colif.
Reprint requests: Marilyn Pink, MS, PT, Centinela HospitalMedical Center , Biomechanics Laboratory, 555 E. HardySt., Inglewood, CA 90301.
' References 7, 8, 10-12, 16, 23-26.32/1136032
selected muscles in a lim ited number of sub[ects.": 13, 14 Also, the instrumentation to quantify the data as an integ rated signal was notinitially available. This study was designed todescribe a comprehensive, integrated, andquantified data base of electromyographic activ ity in 29 muscles of the shoulder girdle andupper extremity in a large sample of uninjured,skilled pitchers during the fastball pitchingmotion.
SUBJECTS AND METHODSFifty-six uninjured, skilled pitchers, who were
active at the college or professional level, wereevaluated at the Biomechanics Laboratory ofCentinela Hospital in Inglewood, California. Indwelling electromyography was used to recordact ivity in 29 separate muscles or muscle belliesof the shoulder girdle and dominant upper extremity during the fastball pitch. These includedmuscles responsible for scapular rotation (7muscles), glenohumeral motion (10 muscles),and elbow, forearm, wrist, and finger motion(12 muscles). Technical limitations of the electromyography and telemetry unit allowed monitoring of only eight muscles for each pitcherduring a single pitching session . Occasionallypitchers volunteered to come back for a secondsession, but none came back for a third session.Different pitchers had different combinations ofthe eight muscles monitored. No pitcher had all
15
16 DiGiovine et 01. J. Shoulder Elbow Surg.January /February 1992
FINISHFOOT
DOWNMAXIMAL BALLEXTERNAL RELEASEROTATION
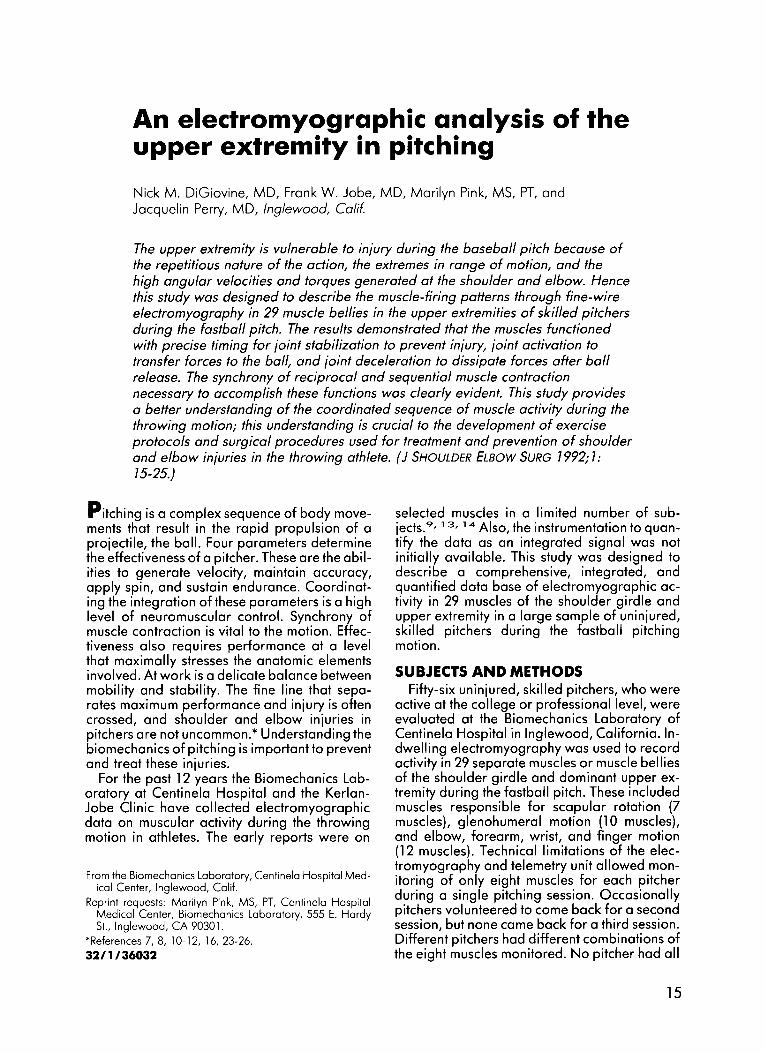
Figure 1 Six phases of pitching.
HANDSAPART
START
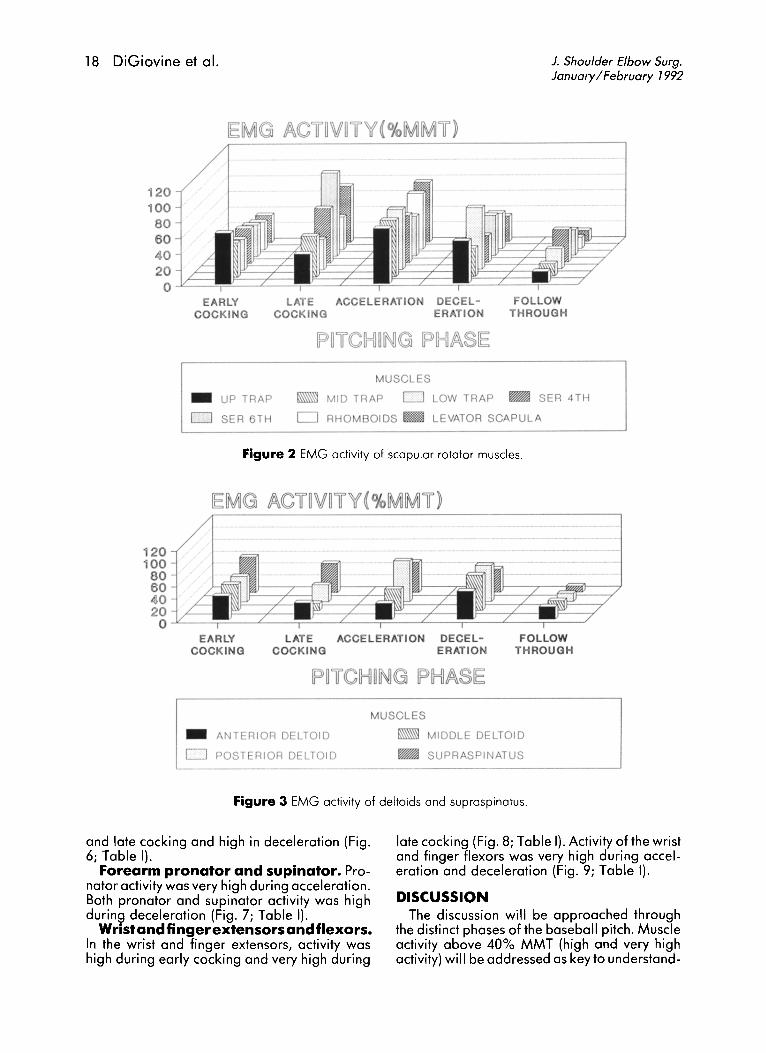
29 muscle bellies monitored. Recordings foreach muscle were obta ined in an average of 13pitchers (range, 10 to 18) (Table I).
Fifty-micran dual-wire electrodes were inserted intramuscularly by means of the singleneedle technique of Basmajian and Deluco."Manual muscle testing or electrical stimulationwas then performed to confirm placement,while muscle activity wos observed on an oscilloscope. The electrodes were connected to abaHery-powered transmiHer belt pack to prevent restrictions in body movements. To correlate electromyograph ic act ivity with specificmovements in the pitching sequence, a 16 mmmotion picture camera was used to film eachpitch at the rate of 400 or 450 frames persecond.
The electromyographic signals were telemetered to a computer for conversion to digitalformat and quantified by integration of 2500samples every second . Excluding noise, thepeak 1-second signal during a maximal manualmuscle test (MMT) was selected as 100% activity. All other muscular activity was assessedevery 20 msec and expressed as a relative percentage of the MMT. To facilitate generalizedcomparisons a range of 0% to 20% was considered low activity; 21% to 40%, moderate activity; 41% to 60%, high act ivity; and greaterthan 60%, very high activity.
The film was reviewed on a stop-action projector. Single-frame viewing allowed each pitchto be accurately d ivided into six phases:windup, early cacking, late cocking, acceleration, deceleration, and follow-through (Fig. 1).As previously defined, follow-through beganwhen the ball left the fingers and continued untilmotian in the pitching arm ceosed.P- 14.26 Deceleration now describes the first one third ofthis phase, and follow-through is defined asthe second two thirds of this phase. Synchronization between the pitching phases and the
electromyographic data was achieved by useof electronic markers, wh ich were placed onboth the motion picture film and the electromyographic recording . Electromyographic activity was averaged with in each phase of thepitch for each muscle and each pitcher. Recorded measurements of the act iv ities for everyphase in each muscle were averaged amongpitchers and expressed as a mean and standarddeviation.
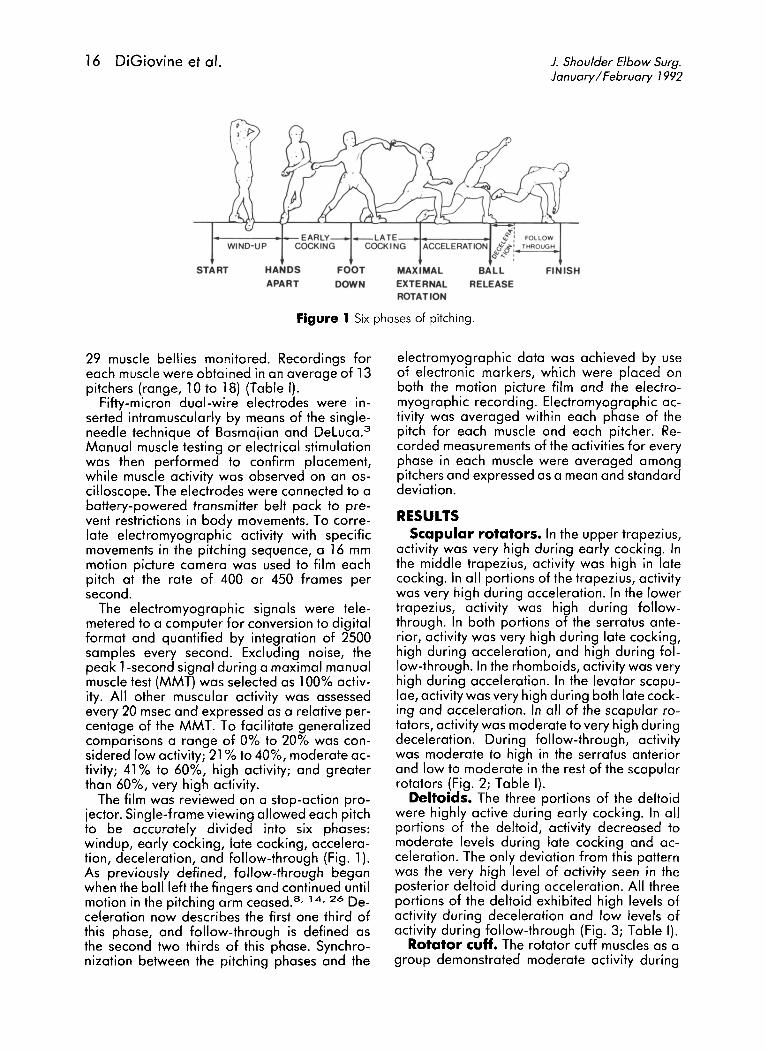
RESULTSScapular rotators. In the upper trapezius,
activity was very high during early cocking. Inthe middle trapezius, act ivity was high in latecocking . In all portions of the trapez ius, activitywas very high during acceleration. In the lowertrapezius, activity was high during followthrough. In both portions of the serratus anterior, activity was very high during late cocking,high during acceleration, and high during follow-through. In the rhomboids, activity was veryhigh during acceleration. In the levator scapulae, activity was very high during both late cocking and acceleration. In all of the scapular rotators, act ivity was moderate to very high duringdeceleration. During follow-through, activitywas moderate to high in the serratus anteriorand low to moderate in the rest of the scapularrotators (Fig. 2; Table I).
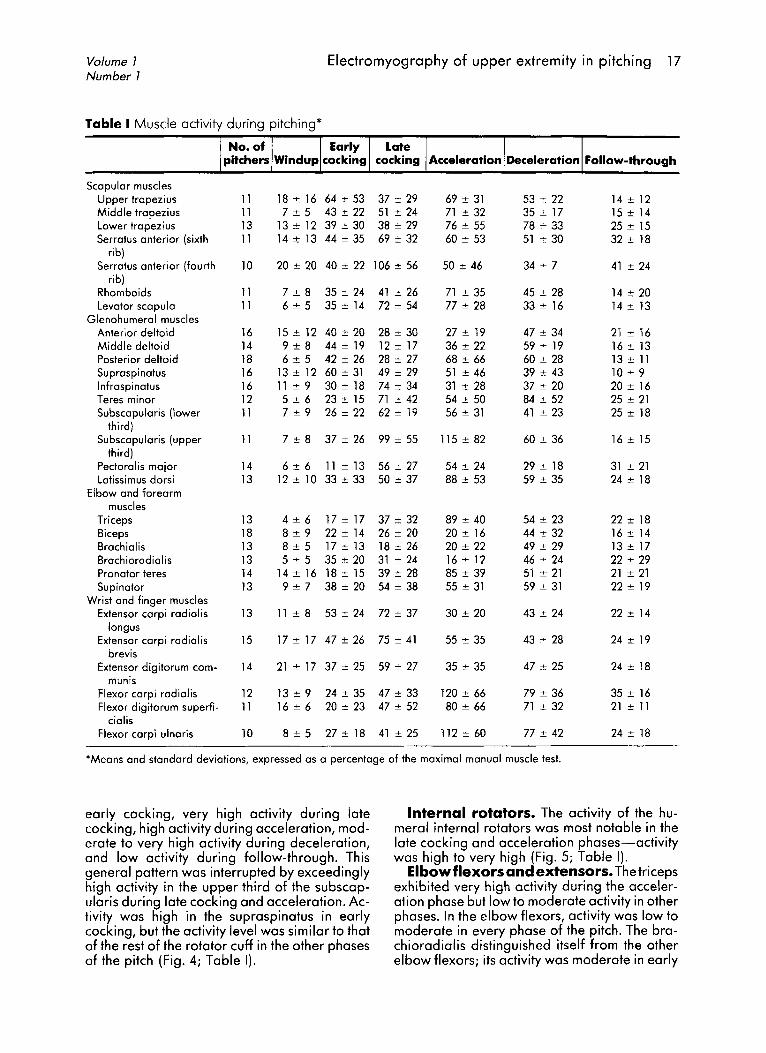
Deltoids. The three portions of the deltoidwere highly active during early cocking. In allportions of the deltoid, act ivity decreased tomoderate levels during late cocking and acceleration. The only deviation from this paHernwas the very high level of activity seen in theposterior deltoid during acceleration . All threeportions of the deltoid exhibited high levels ofact ivity during deceleration and low levels ofactivity during follow-through (Fig. 3; Table I).
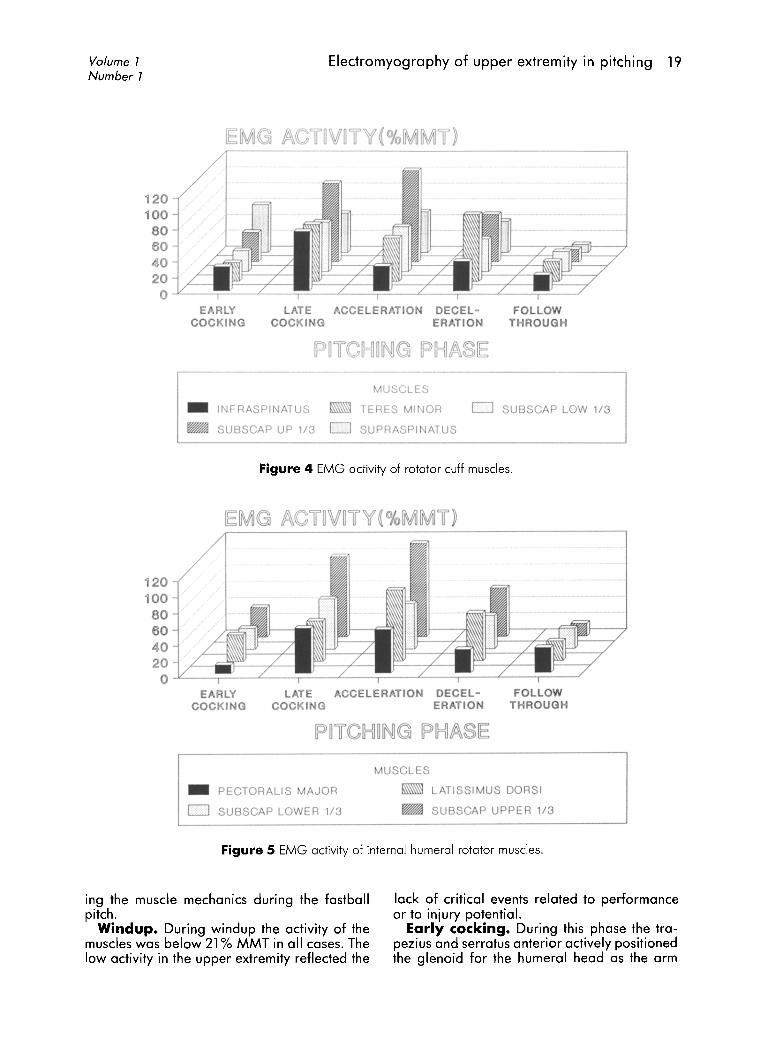
Rotator cuff. The rotator cuff muscles as agroup demonstrated moderate activity during
Volume 7Number 7
Electromyography of upper extremity in pitching 17
Acceleration Deceleration Follow-through
Scapular musclesUpper trapezius 11 18:!: 16 64 ::!: 53 37 ::!: 29 69 ::!: 31 53::!: 22 14 ::!: 12Middle trapezius 11 7:!: 5 43 ::!: 22 51 ::!: 24 71 ::!: 32 35:!: 17 15 ::!: 14Lower trapezius 13 13 ± 12 39 ± 30 38 ::!: 29 76 ± 55 78 ± 33 25 ± 15Serratus anterior (sixth 11 14 ± 13 44 ::!: 35 69 ± 32 60 ± 53 51 ± 30 32 ± 18
rib)Serratus anterior (fourth 10 20 ± 20 40 ± 22 106 ::!: 56 50 ± 46 34 ± 7 41 ± 24
rib)Rhomboids 11 7 ± 8 35 ± 24 41 ± 26 71 ± 35 45 ± 28 14 ± 20Levator scapula 11 6 ± 5 35 ± 14 72 ± 54 77 ± 28 33 ± 16 14 ± 13
Glenohumeral musclesAnterior deltoid 16 15 ± 12 40 ± 20 28 ::!: 30 27 ± 19 47 ± 34 21 ± 16Middle deltoid 14 9 ± 8 44 ± 19 12 ± 17 36 ± 22 59 ± 19 16 ± 13Posterior deltoid 18 6 ± 5 42 ± 26 28 ± 27 68 ± 66 60 ± 28 13 ± 11Supraspinatus 16 13 ± 12 60 ± 31 49 ± 29 51 ± 46 39 ± 43 10 ± 9Infraspinatus 16 11 ::!: 9 30 ± 18 74 ± 34 31 ± 28 37 ± 20 20 ± 16Teres minor 12 5 ::!: 6 23 ± 15 71 ± 42 54 ± 50 84 ± 52 25 ± 21Subscapularis (lower 11 7 ± 9 26 ± 22 62 ::!: 19 56 ± 31 41 ± 23 25 ± 18
third)Subscapularis (upper 11 7 ± 8 37 ± 26 99 ± 55 115 ± 82 60 ± 36 16 ± 15
third)Pectoralis major 14 6 ± 6 11 ± 13 56 ± 27 54 ± 24 29 ± 18 31 ± 21Latissimus dorsi 13 12 ::!: 10 33 ± 33 50 ± 37 88 ± 53 59 ± 35 24 ± 18
Elbow and forearmmuscles
Triceps 13 4 ± 6 17 ± 17 37 ± 32 89 ::!: 40 54 ± 23 22 ± 18Biceps 18 8 ± 9 22 ± 14 26 ± 20 20 ± 16 44 ± 32 16:!: 14Brachialis 13 8 ± 5 17 ± 13 18 ± 26 20 ± 22 49 ± 29 13 ± 17Brachioradialis 13 5 ± 5 35 ± 20 31 ::!: 24 16 ± 12 46 ± 24 22 ± 29Pronator teres 14 14 ± 16 18 ± 15 39 ::!: 28 85 ± 39 51 :+: 21 21 ± 21Supinator 13 9 ± 7 38 ± 20 54 ± 38 55 ± 31 59 :+: 31 22 ± 19
Wrist and finger musclesExtensor carpi radialis 13 11 ± 8 53 ± 24 72 ± 37 30 ± 20 43 ± 24 22 ::!: 14
longusExtensor carpi radialis 15 17 ± 17 47 ± 26 75 ::!: 41 55 ± 35 43 :+: 28 24 ± 19
brevisExtensor digitorum com- 14 21 ± 17 37 ± 25 59 ± 27 35 ± 35 47 ::!: 25 24 ± 18
munisFlexor carpi radialis 12 13 ± 9 24 ± 35 47 ± 33 120 ± 66 79 :+: 36 35 ± 16Flexor digitorum superfi- 11 16 ± 6 20 ± 23 47 ± 52 80 ± 66 71 :+: 32 21 ± 11
cialisFlexor carpi ulnaris 10 8 ± 5 27 ± 18 41 ± 25 112 ± 60 77 ± 42 24 ± 18
'Means and standard deviations, expressed as a percentage of the maximal manual muscle test.
early cocking, very high activity during latecocking, high activity during acceleration, moderate to very high activity during deceleration,and low activity during follow-through. Thisgeneral pattern was interrupted by exceedinglyhigh activity in the upper third of the subscapularis during late cocking and acceleration. Activity was high in the supraspinatus in earlycocking, but the activity level was similar to thatof the rest of the rotator cuff in the other phasesof the pitch (Fig. 4; Table I).
Internal rotators. The activity of the humeral internal rotators was most notable in thelate cocking and acceleration phases-activitywas high to very high (Fig. 5; Table I).
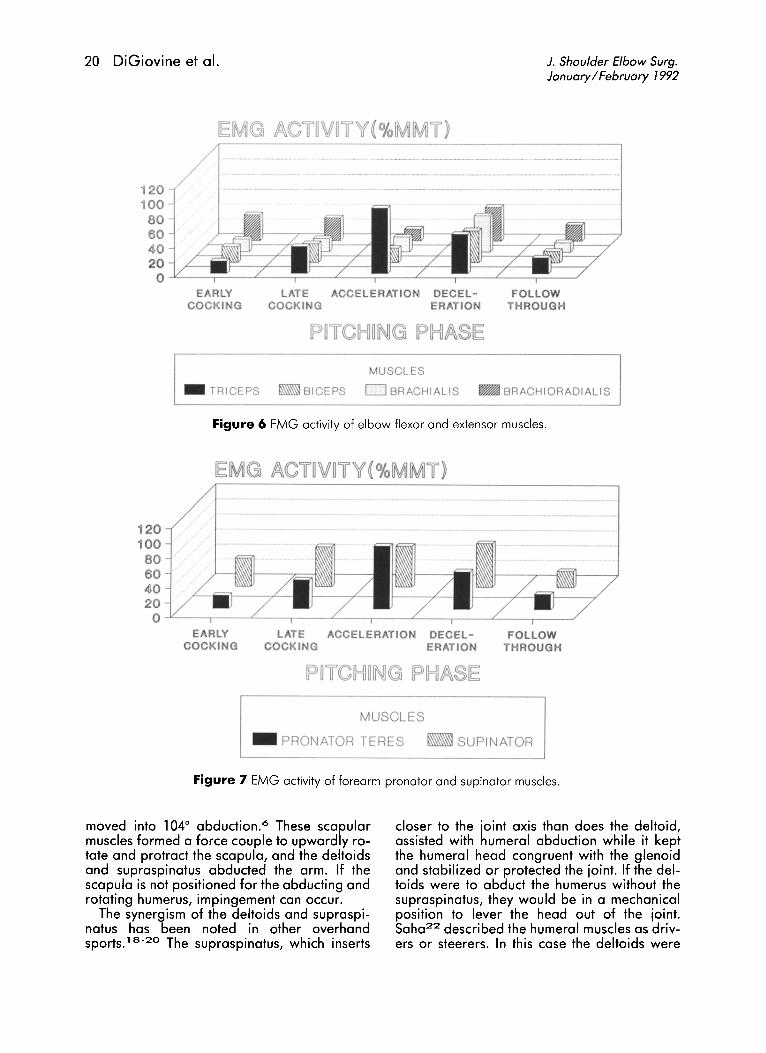
Elbowflexors and extensors. Thetricepsexhibited very high activity during the acceleration phase but low to moderate activity in otherphases. In the elbow flexors, activity was low tomoderate in every phase of the pitch. The brachioradialis distinguished itself from the otherelbow flexors; its activity was moderate in early
18 DiGiovine et 01. J. Shoulder Elbow Surg.January / February 1992
OllOWTH ROUGH
LATECOCKING
12010080
60 ldJ~_~4020
0 -
_ UP TRAP
o SER 6T H
MU SCL ES
_ MID TRAP 0 LOW TRAP _ SER 4TH
o RHO MBO IDS _ LE VATOR SCAP UL A
Figure 2 EMG activity of scapular rotator muscles.
12010080604020
O --lL-- ......::;==-- ..L-- ---=;==--- ..L----=;==--- L..-- -=r==---- L.-- -=;==------/EARLY
COCKINGL AT E ACCEL ERATION DECE L-
COCKING ERAT IONFOL LOW
TH ROUGH
_ ANTER IOR DELTOID
o POSTERIOR DELTOI D
MUSCL ES
_ MIDDL E DELTO ID
_ SUPRASPINATUS
Figure 3 EMG activity of deltoids and supraspinatus.
and late cocking and high in deceleration (Fig.6; Table I).
Forearm pronator and supinator. Pronator activity was very high during acceleration.Both pronator and supinator activity was highduring deceleration (Fig. 7; Table I).
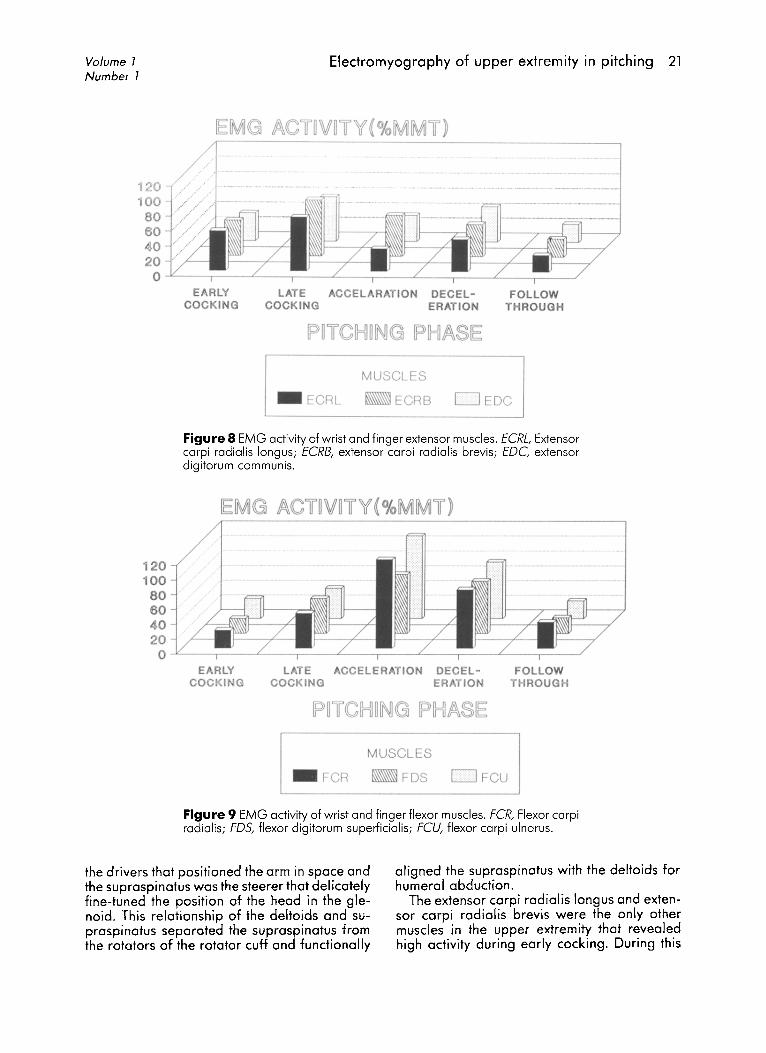
Wrist and fingerextensorsandflexors.In the wrist and finger extensors, activity washigh during early cocking and very high during
late cocking (Fig. 8; Table I). Activity of the wristand finger flexors was very high during acceleration and deceleration (Fig. 9; Table I).
DISCUSSIONThe discussion will be approached through
the distinct phases of the baseball pitch. Muscleactivity above 40% MMT (high and very highactivity) will be addressed as key to understand-
Volume 7Number 7
Electromyography of upper extremity in pitching 19
12010080604020o J'-----=r=--"--.::y=--L_---=;=-_-L-_....:;::=-~C__..:::;=--/
EA RLYCOCKING
L ATE ACCELERATION DECEL-COCKIN G ERATI ON
FOLLOWTHROUGH
r--------- - - ----------- - - - - - - --,
MUS CLE S
_ INFRASPINATUS TERES MINOR 0 SUBSCAP LOW 1/3
_ SUBSCAP UP 1/3 0 SUPRASPINATUS
Figure 4 EMG activity of rotator cuff muscles.
12010080604020
O JL_ -.:;:.. L...-_-.-_-----L_-,,--_-L-_-,.--__c__--,--_-----'
EARLYCOCK ING
_ PECTOR ALIS MA J OR
o SUBSCAP LO WER 1/3
MUS CL ES
_ L ATISSIMUS DORSI
_ SUBSCAP UPPER 1/ 3
Figure 5 EMG activity of internal humeral rotator muscles.
ing the muscle mechanics during the fastballpitch.
Windup. During windup the activity of themuscles was below 21% MMT in all cases. Thelow activity in the upper extremity reflected the
lack of critical events related to performanceor to injury potential.
Early cocking. During this phase the trapezius and serratus anterior actively positionedthe glenoid for the humeral head as the arm
20 DiGiovine et 01. 1. Shoulder Elbow Surg.January / February 1992
12010080604020
O --"-- ---,- - "--- -.--- --L- ----,r-- -L-- ---,- - "--- -.--- -J
MUSCL ES
_ TRICEPS _ BI CEPS 0 BRACH IALI S _ BRA CHIORADI ALIS
Figure 6 EMG activity of elbow flexor and extensor muscles.
120100
80604020
O --"-- -,-- --'::....-- ,-- ...L.-- -,-- --''--- .-_ -L.._ ---.-_ -----'EARLY
COC KINGLAT E ACCELERATION DECEL-
COC KING ERATIONFOLL OW
THROUGH
MUSCL ES
- PRONATOR TERES _ SUPINATOR
Figure 7 EMG activity of forearm pronator and supinator muscles.
moved into 104° obduction." These scapularmuscles formed a force couple to upwardly rotate and protract the scapula, and the deltoidsand supraspinatus abducted the arm. If thescapula is not positioned for the abducting androtating humerus, impingement can occur.
The synergism of the deltoids and supraspinatus has been noted in other overhandsportS.1 8
-2 0 The supraspinatus, which inserts
closer to the joint axis than does the deltoid,assisted with humeral abduction while it keptthe humeral head congruent with the glenoidand stabilized or protected the joint. If the deltoids were to abduct the humerus without thesupraspinatus, they would be in a mechanicalposition to lever the head out of the joint.Saha2 2 described the humeral muscles as drivers or steerers. In this case the deltoids were
Volume 7Number 7
Electromyography of upper extremity in pitching 21
LATECOCKING
--If-+----.
EMG ACf~VrrY'( ¥oMMf )---------------,
EARLYCOCKING
120 ....100 80604020O -"'---,---L.---,-----L.--r--L-_,--_.L-_-:;=~_/
- ECRL
MUSCLES
ECRB 0 EDC
Figure 8 EMG act ivity of wrist and finger extensor muscles. fCRL, Extensorcarpi radialis longus ; fCRB, extensor carpi rad ial is brevis; f OC, extensordig itorum commun is.
12010080604020o -¥----r--..L.----r--L----,---~e.--.---_----L:....__ _._---./
FOLLOWTHROUGH
_ FCR
MUSCLES
FDS DFCU
Figure 9 EMG activity of wrist and finger flexor muscles. FCR, Flexor carpiradial is; F05, flexor digitorum superficialis; FCU, flexor carpi ulnarus.
the drivers that positioned the arm in space andthe supraspinatus was the steerer that delicatelyfine-tuned the position of the head in the gleno id. This relationship of the deltoids and supraspinatus separated the supraspinatus fromthe rotators of the rotator cuff and functionally
aligned the supraspinatus with the deltoids forhumeral abduction.
The extensor carpi radial is longus and extensor carpi radial is brevis were the only othermuscles in the upper extremity that revealedhigh activity during early cocking . During this
22 DiGiovine et 01.
Supr••pl atus
T. r••minor
T.r ••major
SGHl
Su bacapul.r I.
J. Shoulder Elbow Surg.January / February 1992
IGHl
Peel.m.jor
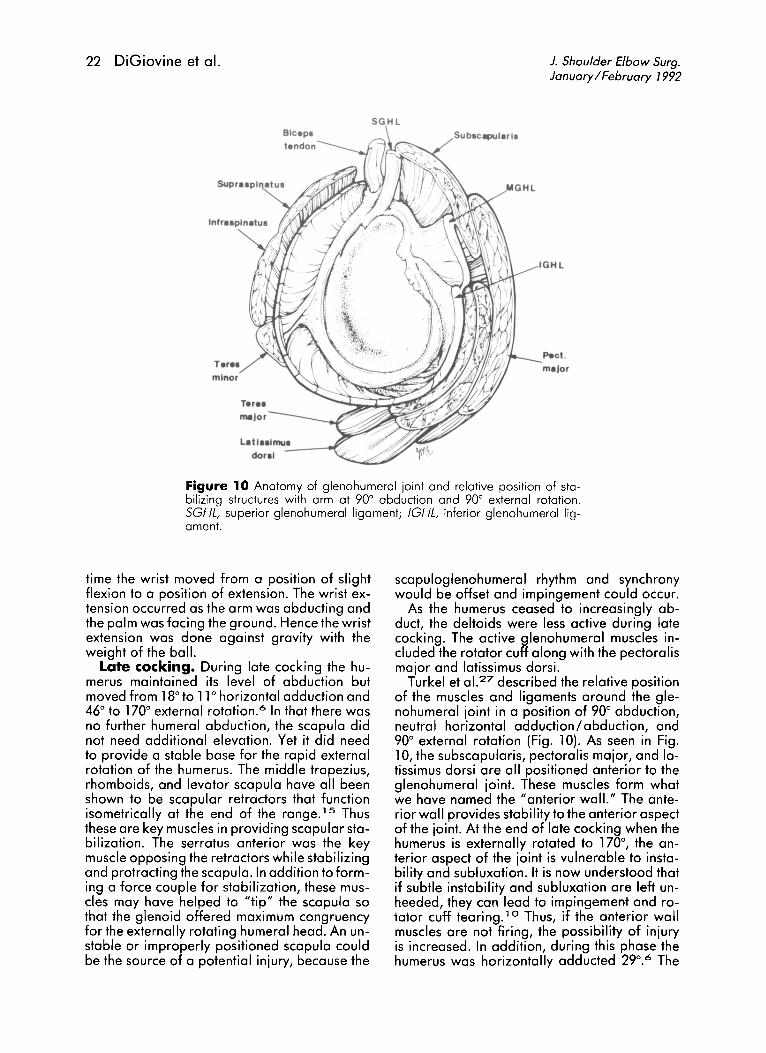
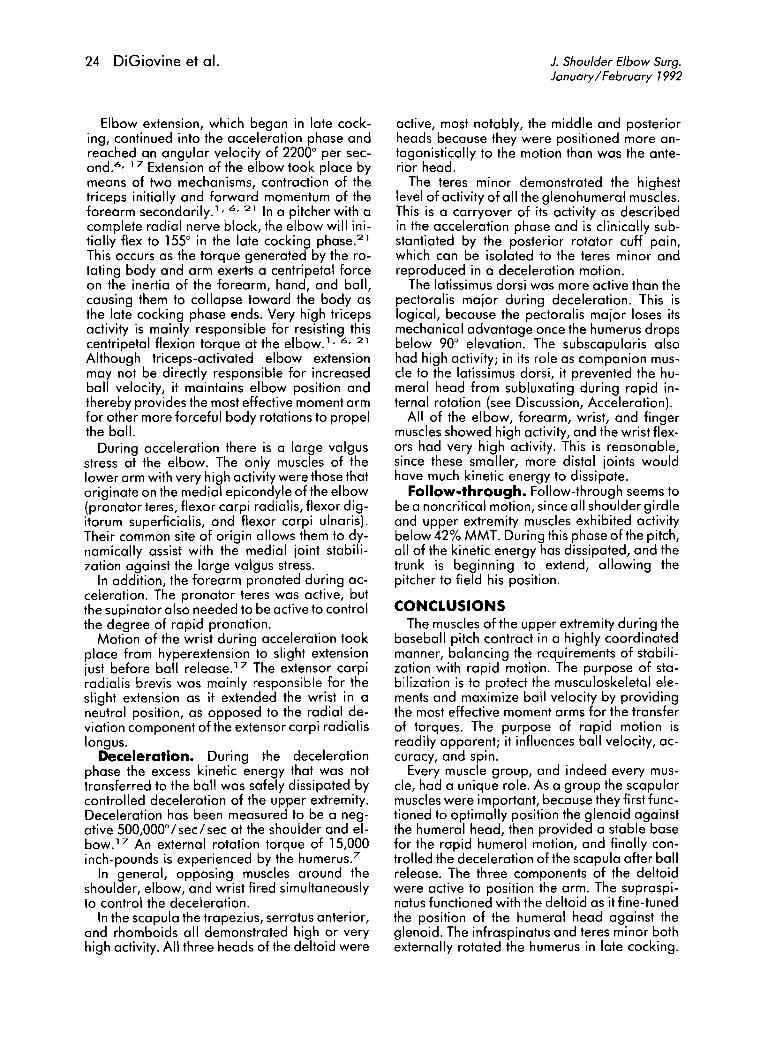
Figure 10 Anatomy of glenohumeral joint and relative position of stabilizing structures with arm at 90° abduction and 90° external rotation.SGHL, superior glenohumeral ligament; IGHL, inferior glenohumeral ligament.
time the wrist moved from a position of slightflexion to a position of extension. The wrist extension occurred as the arm was abducting andthe palm was facing the ground. Hence the wristextension was done against gravity with theweight of the ball.
Late cocking. During late cocking the humerus maintained its level of abduction butmoved from 18° to 11° horizontal adduction and46° to 170° external rototion.? In that there wasno further humeral abduction, the scapula didnot need additional elevation. Yet it did needto provide a stable base for the rapid externalrotation of the humerus. The middle trapezius,rhomboids, and levator scapula have all beenshown to be scapular retractors that functionisometrically at the end of the rcnqe.!? Thusthese are key muscles in providing scapular stabilization. The serratus anterior was the keymuscle opposing the retractors while stabilizingand protracting the scapula. In addition to forming a force couple for stabilization, these muscles may have helped to "tip" the scapula sothat the glenoid offered maximum congruencyfor the externally rotating humeral head. An unstable or improperly positioned scapula couldbe the source of a potential injury, because the
scapuloglenohumeral rhythm and synchronywould be offset and impingement could occur.
As the humerus ceased to increasingly abduct, the deltoids were less active during latecocking. The active glenohumeral muscles included the rotator cuff along with the pectoralismajor and latissimus dorsi.
Turkel et al. 2 7 described the relative positionof the muscles and ligaments around the glenohumeral joint in a position of 90° abduction,neutral horizontal adduction/abduction, and90° external rotation (Fig. 10). As seen in Fig.10, the subscapularis, pectoralis major, and latissimus dorsi are all positioned anterior to theglenohumeral joint. These muscles form whatwe have named the"anterior wall." The anterior wall provides stability to the anterior aspectof the joint. At the end of late cocking when thehumerus is externally rotated to 170°, the anterior aspect of the joint is vulnerable to instability and subluxation. It is now understood thatif subtle instability and subluxation are left unheeded, they can lead to impingement and rotator cuff tearing.' 0 Thus, if the anterior wallmuscles are not firing, the possibility of injuryis increased. In addition, during this phase thehumerus was horizontally adducted 29°.6 The
Volume 7Number 7
Electromyography of upper extremity in pitching 23
pectoralis major undoubtedly contributed tothat motion.
The posterior ratator cuff muscles were alsoquite active during late cocking. The infraspinatus and teres minor were actively externallyrotating the humerus. Their posterior placementalso offered a posterior restraint to the anteriorsubluxation. A weakness of either of these muscles would diminish the posterior restraint.
The supraspinatus was the least active of therotator cuff muscles. As mentioned previously,the supraspinatus has demonstrated a synergywith the deltoid. During this phase the armmaintained rather than increased its level of elevation. Hence activity of the supraspinatus waslower in late cocking than in early cocking butstill high. Also, in the position of extreme external rotation, the supraspinatus was rotatedposteriorly. At this point the supraspinatuswould be in a relatively ineffective position withless superior compressive force.
The superior compressive force, which wasabdicated by the supraspinatus, may have beenin part provided by the subscapularis. The upper portion of the subscapularis was more active than the lower portion. At the point of 170°humeral external rotation with 102° abduction,the upper portion of the subscapularis was rotated superiorly and was able to offer somecompression and support for the superior portion of the anterior wall.
The only elbow/ forearm muscle that was active during late cocking was the supinator. Theliterature has shown that during this phase theforearm is in supination. Pronation does not begin until 10 msec before ball releose." Thus thefunction of the supinator is to appropriately position the forearm.
All of the wrist and finger muscles demonstrated high or very high activity at this time. Bycocontracting these muscles the pitchers wereable to have a stable base from which they subsequently launched the ball.
Acceleration. During acceleration the humerus internally rotated approximately 100° in0.05 second and the elbow extended an average of 54°.6 Angular velocities of 6100° persecond'v 17 created a humeral internal rotationtorque of 14,000 inch-pounds." The highestshoulder joint compression force (860 Newtonmeters}? was observed at this time.
A stable scapula is needed as a fulcrum forthe high angular velocities and torques. All ofthe scapular muscles demonstrated very highactivity as they filled this function.
As the humerus was internally rotating, theposterior deltoid was optimally positioned to bethe primary humeral horizontal abductor, as
noted by its very high electrical activity. The supraspinatus was also highly active as it againdemonstrated its relationship to the deltoid.
At this point the teres minor and the infraspinatus had differing levels of activity-highin the teres minor and moderate in the infraspinatus. This may have clinical relevance, because in our experience posterior cuff tenderness in baseball pitchers can frequently be isolated to the teres minor. Also, our experiencewith the electromyographic manual muscle testing has revealed higher levels of activity in theteres minor when the humerus is abducted orextended. In addition, electromyographic investigations in other sports have shown separate functions for the infraspinatus and teresminor. 1 8 - 2 o
The activity in the teres minor is similar to theactivity in the pectoralis major. These two muscles appear to form a force couple. As the pectoralis major forcefully contracts at the relatively high elevations for adduction and internalrotation, the teres minor provides a stabilizingposterior restraint. The direction of the fibers ofthe teres minor give it an extension component,which may be the reason it performs thisfunction.
The large angular velocity during acceleration is the result of energy that is transferredfrom the trunk, with augmentation by the latissimus dorsi and pectoralis major. Bassett et ol."have shown that although both the latissimusdorsi and the pectoralis major can potentiallygenerate large internal rotation torques aboutthe shoulder, the latissimus dorsi is anatomically positioned to generate the greater torque.This is consistent with the relative electromyographic activities in these two muscles during this phase; the latissimus dorsi has thegreater activity. The pectoralis major and latissimus dorsi were the main upper extremity muscles that actively contributed velocity to the ball.A clinical study indicated that these muscleswere the only ones in the upper extremity tohave a positive correlation between peaktorque developed in isokinetic testing and pitching velocity."
The subscapularis, especially the upper portion, also exhibited very high activity during thisphase and functioned with the latissimus dorsiand the pectoralis major. The subscapularis apparently functioned as the steering muscle toprecisely position the humeral head in the glenoid; this is similar to the relationship of thesupraspinatus with the deltoid. This alignmentof the subscapularis with the latissimus dorsihas been observed in other sports activities. 1 8 - 2 o
24 DiGiovine et 01.
Elbow extension, which began in late cocking, continued into the acceleration phase andreached an angular velocity of 22000 per second."- 17 Extension of the elbow took place bymeans of two mechanisms, contraction of thetriceps initially and forward momentum of theforearm secondarily.": 6, 21 In a pitcher with acomplete radial nerve block, the elbow will initially flex to 1550 in the late cocking phase. 2 1
This occurs as the torque generated by the rotating body and arm exerts a centripetal forceon the inertia of the forearm, hand, and ball,causing them to collapse toward the body asthe late cocking phase ends. Very high tricepsactivity is mainly responsible for resisting thiscentripetal flexion torque at the elbow,"- 6, 21
Although triceps-activated elbow extensionmay not be directly responsible for increasedball velocity, it maintains elbow position andthereby provides the most effective moment armfor other more forceful body rotations to propelthe ball.
During acceleration there is a large valgusstress at the elbow. The only muscles of thelower arm with very high activity were those thatoriginate on the medial epicondyle of the elbow(pronator teres, flexor carpi radialis, flexor digitorum superficialis, and flexor carpi ulnaris).Their common site of origin allows them to dynamically assist with the medial joint stabilization against the large valgus stress.
In addition, the forearm pronated during acceleration. The pronator teres was active, butthe supinator also needed to be active to controlthe degree of rapid pronation.
Motion of the wrist during acceleration tookplace from hyperextension to slight extensionjust before ball relecse.!? The extensor carpiradialis brevis was mainly responsible for theslight extension as it extended the wrist in aneutral position, as opposed to the radial deviation component of the extensor carpi radialislongus.
Deceleration. During the decelerationphase the excess kinetic energy that was nottransferred to the ball was safely dissipated bycontrolled deceleration of the upper extremity.Deceleration has been measured to be a negative 500,000 0
/ sec/ sec at the shoulder and elbow."" An external rotation torque of 15,000inch-pounds is experienced by the humerus."
In general, opposing muscles around theshoulder, elbow, and wrist fired simultaneouslyto control the deceleration.
In the scapula the trapezius, serratus anterior,and rhomboids all demonstrated high or veryhigh activity. All three heads of the deltoid were
J. Shoulder Elbow Surg.January / February 7992
active, most notably, the middle and posteriorheads because they were positioned more antagonistically to the motion than was the anterior head.
The teres minor demonstrated the highestlevel of activity of all the glenohumeral muscles.This is a carryover of its activity as describedin the acceleration phase and is clinically substantiated by the posterior rotator cuff pain,which can be isolated to the teres minor andreproduced in a deceleration motion.
The latissimus dorsi was more active than thepectoralis major during deceleration. This islogical, because the pectoralis major loses itsmechanical advantage once the humerus dropsbelow 900 elevation. The subscapularis alsohad high activity; in its role as companion muscle to the latissimus dorsi, it prevented the humeral head from subluxating during rapid internal rotation (see Discussion, Acceleration).
All of the elbow, forearm, wrist, and fingermuscles showed high activity, and the wristflexors had very high activity. This is reasonable,since these smaller, more distal joints wouldhave much kinetic energy to dissipate.
Follow-through. Follow-through seems tobe a noncritical motion, since all shoulder girdleand upper extremity muscles exhibited activitybelow 42% MMT. During this phase of the pitch,all of the kinetic energy has dissipated, and thetrunk is beginning to extend, allowing thepitcher to field his position.
CONCLUSIONSThe muscles of the upper extremity during the
baseball pitch contract in a highly coordinatedmanner, balancing the requirements of stabilization with rapid motion. The purpose of stabilization is to protect the musculoskeletal elements and maximize ball velocity by providingthe most effective moment arms for the transferof torques. The purpose of rapid motion isreadily apparent; it influences ball velocity, accuracy, and spin.
Every muscle group, and indeed every muscle, had a unique role. As a group the scapularmuscles were important, because they first functioned to optimally position the glenoid againstthe humeral head, then provided a stable basefor the rapid humeral motion, and finally controlled the deceleration of the scapula after ballrelease. The three components of the deltoidwere active to position the arm. The supraspinatus functioned with the deltoid as it fine-tunedthe position of the humeral head against theglenoid. The infraspinatus and teres minor bothexternally rotated the humerus in late cocking.

Volume 7Number 7
Electromyography of upper extremity in pitching 25
During acceleration and deceleration they haddiffering activities. The teres minor, unlike theinfraspinatus, maintained a high level of activity, providing a posterior restraint to limit humeral head translation. This may have clinicalrelevance, because posterior cuff pain in baseball pitchers can frequently be isolated to theteres minor. The subscapularis, pectoralis major, and latissimus dorsi were part of the components of the" anterior wall," which affordedanterior stability during the time of maximal humeral external rotation. All musclesof the lowerarm, which originate on the medial epicondyleof the humerus, demonstrated very high activityduring the time of valgus stress to the elbow.They were likely adding a dynamic componentto elbow stability.
The critical role of the deceleration phase tohelp dissipate the kinetic energy that was notimparted to the ball is now evident; a lack ofmuscular control at this time would undoubtedlylead to injury. On the other hand, the windupand follow-through phases demonstrated alack of consequential events in the upper extremity.
This study has provided information on boththe coordinated sequence of muscular eventsand their relative magnitudes in the upper extremity during pitching. This knowledge is critical to the development of exercise protocolsand surgical procedures that are used for theprevention and treatment of shoulder and elbow injuries resulting from throwing motions inathletes.
REFERENCES1. Atwater AE. Biomechanics of overarm throwing move
ments and of throwing injuries. Exerc Sport Sci Rev1979;7:43-85.
2. Bartlett lR, Storey MD, Simons BD. Measurement of upper extremity torque production and its relationship tothrowing speed in the competitive athlete. Am J SportsMed 1989;17:89-91.
3. Basmajian JV, Deluca DJ. Muscles alive: their functionsrevealed by electromyography. Baltimore: Williams andWilkins, 1985:265-89.
4. Bassett RW, Browne AO, Morrey BF, An KN. Glenohumeral muscle force and moment mechanics in a position of shoulder instability. J Biomech 1990;23:405-15.
5. Elliott B, Grove JR, Gibson B, Thurston B. A three-dimensional cinematographic analysis of the fastball andcurveball pitches in baseball. Int J Sports Biomech1986;2:20-8.
6. Feltner M, Dapena J. Dynamics of the shoulder andelbow joints of the throwing arm during a baseball pitch.lnt J Sports Biomech 1986;2:235-59.
7. Gainor BJ, Piotrowski F, Puhl J, Allen We, Hagen R. Thethrow: biomechanics and acute injury. Am J Sports Med1980;8: 114-8.
8. Glousman R, Jobe FW, Tibone JE,Moynes DR,AntonelliD, Perry J. Dynamic electromyographic analysis of thethrowing shoulder with glenohumeral instability. J BoneJoint Surg [Am] 1988;70A:220-6.
9. Gowan ID, Jobe FW, Tibone JE, Perry J, Maynes DR. Acomparative electramyagraphic analysis of the shoulderduring pitching: professionol versus amateur pitchers.Am J Sports Med 1987;15:586-90.
10. Jobe FW, Bradley JP. Rotator cuff injuries in baseball:prevention and rehabilitation. Sports Med 1988;6:37887.
11. Jobe FW, Maynes DR. Delineation of diagnostic criteriaand a rehabilitation program for rotator cuff injuries. AmJ Sports Med 1982;10:336-9.
12. Jobe FW, Moynes DR, Brewster CEo Rehabilitation ofshoulder joint instabilities. Orthop Clin North Am1987; 18:473-82.
13. Jobe FW, Moynes DR,Tibone JE, PerryJ. An EMG analysis of the shoulder in pitching: a second report. Am JSports Med 1984;12:218-20.
14. Jobe FW, Tibone JE,Maynes DR, PerryJ. An EMG analysis of the shoulder in throwing and pitching: a preliminary report. Am J Sports Med 1983;11:3-5.
15. Moseley JB, Jobe FW, Pink M, Perry J, Tibone JE. EMGanalysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med (in press).
16. Pappas AM, Zawacki RM, McCarthy CF. Rehabilitationof the pitching shoulder. Am J Sports Med 1985;13:22335.
17. Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics ofbaseball pitching: a preliminary report. Am J Sports Med1985;13:216-22.
18. Pink M, Jobe FW, Perry J, Kerrigan J, Browne A, Scovazzo ML. The normal shoulder during the backstroke: anEMG and cinematographic analysis of twelve muscles.Clin J Sports Med 1992;2:6-12.
19. Pink M, Jobe FW, Perry J, Kerrigan J, Browne A, Scovazzo Ml. The normal shoulder during the butterfly swimstroke: an EMG and cinematographic analysis of twelvemuscles. Clin Orthop (in press).
20. Pink M, Perry J, Jobe FW, Browne A, Scovazzo Ml, Kerrigan J. The normal shoulder during freestyle swimming:an EMG and cinematographic analysis of twelve muscles. Am J Sports Med 1991;19:569-75.
21. Roberts EM. Cinematography in biomechanical investigation. In: Cooper JM, ed. Committee on InstitutionalCooperation Symposium on Biomechanics, Indiano University, 1970. Chicago: Athletic Institute, 1971.
22. Saha AK. Mechanics of elevation of glenohumeral joint.Acta Orthop Scand 1973;44:668-78.
23. Sisto DJ, Jobe FW. The operative treatment of scopulothoracic bursitis in professional pitchers. Am J SportsMed 1986;14:192-4.
24. Sisto DJ, Jobe FW, Moynes DR, Antonelli DJ. An electromyographic analysis of the elbow in pitching. Am JSports Med 1987;15:260-3.
25. Stacey E. Pitching injuries to the shoulder. Athletic J1984;64:44-7.
26. Tullos HS, King JW. Throwing mechanism in sports. Orthop Clin North Am 1973;4:709-20.
27. Turkel SJ, Panio MW, Marshall Jl, Girgis FG. Stabilizingmechanisms preventing anterior dislocation of the glenohumeral joint. J Bone Joint Surg [Am] 1981;63A: 120817.





























