Embed Size (px)
Citation preview

Page 18
IntroductionPregnancy affects essentially all aspects of kidney and systemic hemodynamics physiology marked by significant volume expansion and vasodilatation. Glomerular filtration rate (GFR) increases 50%, the kidneys are larger during pregnancy because of fluid retention, and physiological hydronephrosis is common and it is more prevalent with advancing trimester (1). The dilated collecting system can hold 200 to 300mL of urine, leading to urinary stasis and advanced increase of kidneys volume (2). The growth is attributed to increased kidney vascular and interstitial volume rather than any changes in the number of nephrons (3, 4). The use of Doppler ultrasound is to improve the anatomical diagnosis of renal calyceal dilation or hydronephrosis by providing functional evidence of acute or chronic obstruction, principally by measuring the resistive index (RI). The differentiation between obstructive and unobstructive hydronephrosis in pregnancy remains a challenging task for the gynecologist. Finally, although collecting system dilatation is reliably detected, it is often not possible to
Research Article Open Access
American Research Journal of GynaecologyVolume 1, Issue 1, pp: 18-30
www.arjonline.org
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
Maja Avramovska1, Goran Dimitrov1, Marija Hadzi Lega1, Elena Dzikova1 Gligor Tofoski1, Ana Daneva Markova1
1University Clinic of Gynecology and Obstetrics, Medical University, St. Cyril and Methodius, SkopjeRepublic of Macedonia.
Background/Aims: Doppler ultrasonography is used in clinical gynecologic practice to detect the renal macroscopic vascular abnormalities and changes in blood flow at the micro vascular level. The aim of the study was to find the differences between renal flow parameters in pregnant and nonpregnat participants, and to find the associative connection of those Doppler parameters with certain stages of gestation period.
Methods: Doppler ultrasonography evaluations of both kidneys were performed in 65 pregnant women and 35 healthy volonteers from control group (CG). We measured resistive index (RI) at the level of the arcuate or interlobar arteries, peak systolic velocity (PSV) and end diastolic velocity (EDV) in pregnant and CG.
Results: We found statistically high significance in renal RI (0.648±0.017 vs. 0.616±0.035 in pregnant and CG, p < 0.0001) and in RI between three gestational age subgroups (0.645±0.027, 0.659±0.013 and 0.644±0.011 for first, second and third group, respectively). The mean PSV and EDV results for pregnant and CG were: 60.09±3.87 and 21.15±1.57 vs. 52.99±12.32 and 20.28±4.51. The PSV and EDV results among subgroups were: 58.29±3.25, 60.93±4.40 and 60.65±3.39 for PSV and 20.38±1.57, 21.28±1.55 and 21.62±1.42 for EDV, according first, second and third group, respectively). There is a high statistical significance between PSVs and renal RIs in pregnant and CG (P < 0.0001), but not between the EDVs (p = 0.162). By linear regression analysis (y = 19.4009 + 0.06813∙x) we found strong positive correlation between EDV and gestational age, only.
Conclusions: We conclude that pregnancy reduces renal vascular resistance (RI) and increases renal flow according statistically high significance between the mean renal RI in pregnant and CG. The EDV changes during gestational age are more than two and a half time bigger than changes in PSV. The EDV value has a greater diagnostic significance for assessing the renal function in pregnancy than PSV and RI.
Keywords: Doppler, Resistive index, pregnancy, renal flow.

Page 19
differentiate obstructive and nonobstructive pelvicaliectasis on gray-scale sonography alone (5). Initial studies which examined vasoconstrictive response to a high pressure in the renal collecting system suggested that the renal RI increase is primarily generated by influence of mechanical factors, and secondly as a result of the release of humoral factors which are in favor of vasoconstriction of the renal arteries (5, 6, 7, 8, 9).
Doppler ultrasonography is a noninvasive method widely used in clinical gynecologic practice and for pregnancy monitoring. It can detect renal macroabnormalities and changes in the renal vasculature blood flow. The RI is commonly used as an index of intrarenal arterial resistance (7). It is calculated with the following formula:
or [PSV (peak systolic velocity) - EDV (end diastolic velocity)]/ PSV (peak systolic velocity) (8, 9). Almost all modern ultrasound scanners have software for automatic calculation of the Doppler parameters including the RI. Doppler ultrasonography detects not only the renal macroscopic vascular abnormalities; it also identifies changes in blood flow at the microvascular level (10, 11, 12). Unlike conventional B-mode renal ultrasonography which assess renal and collecting system morphology (providing valuable information on anatomic features including kidney size, parenchyma thickness, echogenicity of the parenchyma, cortex and medulla, presence of the stone, calcifications, cysts or solid mass), renal Doppler is valuable for assessing large arterial or venous abnormalities and has been suggested for evaluating changes in intrarenal perfusion due to diseases of the renal parenchyma (11, 12, 13, 14).
The aims of this study were: first, to establish the differences in Doppler renal blood flow parameters (RI, PSV and EDV) in 65 pregnant women between 10 to 37 weeks gestational age and 35 age-matched nonpregnant healthy volunteers; second, to find the associative connection of those Doppler parameters with certain stages of the gestation period.
Methods
Patients
During 18 months period, from March 2016 to August 2017, color and pulsed Doppler ultrasonography evaluations were performed in 35 healthy nonpregnant volunteers and 65 women with normal pregnancies (ranging in age from 20 to 36 years) followed at the low-risk prenatal care unit of our department between 10 to 37 weeks of gestational age. The pregnant patients were recruited from the gynecological ambulance where their gestational age was determined by sonographic measurement of fetal parameters by measuring mean sac diameter (MSD), Crown-rump length (CRL), biparietal diameter (BPD), head circumference (HC), femoral length (FL) or abdominal circumference (AC) depending on the trimester of pregnancy.
After that, they were sent to Doppler ultrasound department for measuring their renal RI. The mean maternal age was 29.4±5.4 years and well matched with control group age (29.±5.6 years, p = 0.794). A more detailed comparative overview of demographic data is presented in Table 1. All of the 100 participants had no history of hypertension or urinary tract disease. Informed consent was obtained from all patients and the ethics committee of our institution approved the study.
Assessment
We used pulsed color Doppler ultrasound scanner Toshiba SSA 340-A with convex array 3.5 MHz abdominal probe (Toshiba SSA-340A, Toshiba Medical System Co., Tokyo, Japan). Each patient from the control and pregnant group underwent B-mode and Doppler ultrasound examination of the urinary tract, including the kidneys (renal parenchyma and renal pelvis) proximal and distal segments of the left and right ureter. Since changes in heart rate (HR) may affect Doppler renal artery velocimetry, measurements of the HR were obtained before each evaluation in all patients (15). An experienced clinician ultrasonographer with over 30 year of experience performed the measurements. Renal artery flow was detected and recorded by positioning the sample volume at the renal hilum. As resistance to blood flow progressively increases from the hilar arteries toward the more
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 20
peripheral parenchymal vessels, it is generally recommended that sampling for renal RI should be done at the level of the arcuate or interlobar arteries, adjacent to medullary pyramids (7).
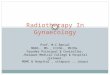
Fig1. Renal RI measurement technique
A sample volume (green parallel line in the right bottom part of the Figure 1) was placed within an intrarenal artery (an arcuate or interlobar one) under Color Doppler guidance and spectral analysis of vascular signals was obtained. In order to maximize waveform size, we used the lowest pulse repetition frequency without aliasing (PRF = 4KHz), the highest possible gain (Gain = 70) without noise and the lowest wall filter (233Hz). The base-line (a green line in the bottom of the spectral analysis diagram) is deliberately lowered down so that the peaks of the spectrum can be displayed without aliasing. We set the flow area to the minimal size to explored vascular vessels so we can get the maximal frame rate of the screen monitor. Sometimes, for better visualization of small renal vessels, we switched on colour enhacement mode with colour persistence, color angio and color capture mode in our sonograph (16, 17).
All of the measurements were preferentially repeated in different anatomic parts of both kidneys (superior, median and lower). At least six reproducible spectral waveforms have been obtained, and the mean of all 6 measurements were accepted for the renal RI. The renal RI was calculated with the following formula:
. The mean of the renal RI was calculated as an average value of the sum of the left renal RI and right renal RI divided by two, or mean .
Statistical Analysis
Statistical analysis was performed using MedCalc Statistical Software version 17.2 (MedCalc Software bvba, Ostend, Belgium). Results are expressed as mean ± SD. Student’s t-test for unpaired data (two-sided) was used to compare the results from demographic and Doppler data between two groups and subgroups. Simple linear regression analysis data and appropriate scatter plots were presented to assess the associations between dependent and independent variables. Appropriate comparative diagram called forest plot was created to show and compare the essential information and results of another studies with our study.
Results
Demographic and Clinical Data
During the eighteen-month period we estimated the both renal artery RI in 65 pregnant women and 35 young women as control group (age and height matched). The demographic and clinical characteristics of the patients are presented in Table 1.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 21
Table1. Demographic and Doppler characteristics of the patients
There is statistically high significance between the mean renal RI in pregnant participants and mean renal RI in control group (0.648±0.017 vs. 0.616±0.035, p < 0.0001, respectively). The highest value for renal RI (0.651±0.011) was measured in patients belonging to the second group (20 to 29 weeks), and smaller value for renal RI (0.644±0.009) was measured for the third group (30 to 37 weeks). The results for PSV and EDV for all three groups of pregnant women are presented in the Table 1, too. The paired t-test shows no statistical significance between PSVs in the first and second group (P = 0.118) and between PSVs in second and third group (P = 0.758). The highest statistical significance (P = 0.024) is shown with the paired t-test between PSVs in first and third group. The paired t-test show no statistical significance between EDVs in the first and second group (P = 0.301) and between EDVs in second and third group (P = 0.423). The highest statistical significance (P = 0.041) is shown with the paired t-test between EDVs in first and third group. There is a high statistical significance between PSVs and renal RIs in pregnant and control group (P < 0.0001), but not between the EDVs (0.162). The mean PSV to EDV ratio (PSV/EDV) in pregnant group was = 2.846±0.137. There is statistically significant inverse correlation between PSV/EDV and gestational age: r = - 273, P = 0.0292.
T-test Results
Test for unpaired data between renal RI in control and pregnant group shows these results: sample size: 35 vs. 64; arithmetic mean: 0.616 vs. 0.648; 95 confidence (CI) for the mean: 0.6037 to 0.6277 vs. 0.6435 to 0.6521; standard deviation (SD): 0.035 vs. 0.017; standard error of the mean: 0.005913 vs. 0.002162; variance: 0.001224 vs. 0.0002993 and test statistic t(d) (Welch-test assuming unequal variances: t(d) = 5.101 and P < 0.0001) for control and pregnant group, respectively. A graphic presentation of the most important results is shown on the Figure 2.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 22
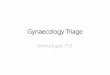
Fig2. Notched Box-and-whisker plots of statistical data for both studied groups
There is a statistically high significance between the mean renal RI in pregnant women and mean renal RI in control group (0.648±0.017 and 0.616±0.035, respectively, p < 0.0001).
The test for unpaired data between renal RI among pregnant group, according gestational age showed these results: 1th group (gestational age 10 - 19 weeks, mean gestational age = 15.3±3.3 weeks), p - value between first and second group is p = 0.002, RI = 0.457±0.027; 2nd group (gestational age 20 - 29 weeks, mean gestational age = 25.3±2.9 weeks), p - value between second and third group is p = 0.0041, RI = 0.659±0.013; 3rd group (gestational age 31 - 37weeks, mean gestational age = 34.1±1.9 weeks), p - value between first and third group is p < 0.001, RI = 0.644±0.011. A graphic presentation of the most important results among pregnant groups is shown on the Figure 3.
Fig3. Box-and-whisker plots of the mean Renal Resistive Index in pregnancy according gestational age
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 23
There is statistically high significant p - value between renal RIs in all subgroups of pregnant women participants (p < 0.05).
Linear Regression and Scatter Plots Data
Resistive Index
The results of linear regression, which are an approach for modeling the relationship between scalar dependent variable Y (mean renal RI) and an explanatory variable denoted X (gestational age, week) were presented as follows: coefficients of determination (R2
1 = 0.01645, R22 = 0.00296 and R2
3 = 0.1603) and appropriate P - values (P1 = 0.612, P2 = 0.805, P3 = 0.058) for each one of the individual three groups, respectively). There is no statistical significant correlation between gestational age and the mean renal RI in all three gestational periods. Only P3 value which belongs to the third gestational group is approaching statistically significant (0.058 ~ 0.050).
Three separate scatter plots in Figure 4 show the trend of dependence of the mean renal RI correlation on the gestation period.
Fig4. Correlation between renal resistive index and gestational age according predefined pregnant group (three - segmental scatter plot).
The thickened light blue, dark blue and red lines are linear regression lines but purple dashed line presents 95% confidence interval (CI). The coefficient of determination R2 (0.1603) in third pregnant group showed that 16.03% of the total variability was explained with the linear relation between mean renal RI and gestational age, or that 16.03% from mean renal RI was dependent on gestational age, measured in third pregnant group. Only 16.03% of the changes from the mean renal RI were a result of gestational age value changes, and the remaining of the total variability between them were not explained (83.97% of renal RI were dependent on other factors, which were not covered with the regression model). The results for linear relation calculated for first and second gestational period are negligible small (1.645% and 0.296%, respectively).
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 24
Fig5. The summary scatter plot shows inverse correlation between mean renal resistive index and gestational age.
The summary results of negative association between mean renal RI and gestational age are presented by linear regression line in Figure 5. We calculated correlation coefficient r = - 0.2282, coefficient of determination R2 = 0.05207 and P = 0.00698 (CI = - 0.4488 to 0.0186). The correlation coefficient, P - value (0.0698) and coefficient of determination showed (R2 = 0.05207) negative association between mean renal RI and gestational age, but not enough statistically significant (0.0698 > 0.05). Only 5.207% (based on R2) of the changes in mean renal RI were a result of gestational age value changes, and the remaining from the total variability (94.793%) between them were not explained. The data of each of 65 female pregnant participants was displayed as a collection of colored points (blue circles for the first, red squares for the second and green triangles for the third gestational period) which determined the mean renal RI. Each point had the value of one variable determining the position on the horizontal axis and the value of the other variable determining the position on the vertical axis.
Renal Artery Velocity
The strong positive correlation between two variables (EDV and gestational age) is presented by the linear regression equation y = 19.4009 + 0.06813∙x. Another results of linear regression were presented as follows: coefficient of determination R2 = 0.1212, regression parameter b0 = 19.4009, regression parameter b1 = 0.06813, residual standard deviation = 1.4799, P = 0.0048, t =2.9246 (slope) and P < 0.0001, t =30.9755 (intercept). The regression parameter b1 = 0.06813 signified that with each increase of one unit (month) in gestational age, the EDV score (cm/s) increased by 0.06813 cm/s.
The Figure 6 shows a scatter plot of linear regression between renal artery velocity and gestational age, for both PSV and EDV.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 25
Fig6. The summary scatter plot shows positive correlation between renal artery velocity (PSV and EDV) with gestational age.
Despite its higher inclination, the red line of PSV does not show a statistically significant correlation (R = 0.2164, R2 = 0.04683 and P = 0.0859). The great congregation of the blue circles around the blue solid line shows strong positive significant (p = 0.0048) correlation between EDV and gestational age. The brown dashed line beside blue solid line presents the CI = 0.1119 to 0.5472. Comparing the R2 results for EDV and PSV (0.1212 vs. 0.04683, respectively) and their coefficient 0.1212/0.04683 which is equal to 2.588, we conclude that changes in EDV as a results of gestational age value changes are more than two and a half time pronounced than changes in PSV.
Comparison with Other Studies
The diagram called a forest plot (Figure 7) summarizes almost all of the essential information of a meta-analysis (the name of corresponding author, year of publication, mean value of renal RI in both groups, number of participants and P-value of statistical significance). The horizontal lines represent each study. The blue horizontal lines with vertical red lines represent the mean renal RI in control group, vs. green horizontal lines with vertical red lines which represent the mean renal RI in pregnant group. The number of participants is presented beside every group.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 26
Fig7. A forest plot presentation (blobbogram) of Renal Resistive analysis in control and pregnant studied population.
A serial independent t-tests were made between the renal RI results of every mentioned study with our study: Kurjak A (18) and Avramovska M, 0.689±0.028 vs. 0.648±0.17, P < 0.0001; Hertzberg BS (19) and Avramovska M, RI = 0.611±0.24 vs. 0.648±0.17, P < 0.001; Dib FR (20) and Avramovska, RI = 0.650±0.02 vs. 0.648±0.17, P = 0.484). The results of our study are closest to the results of Dib FR 2003 study, only. The statistical significance expressed by P-value (P < 0.05) indicates that the results of other studies are significantly differed from the results in our study.
DiscussionTo our knowledge, this kind of studies are quite rare, and perhaps the only longitudinal cross-sectional study which evaluates renal Doppler flow parameters (RI, PSV, EDV) in pregnancy and compare them with renal Doppler flow parameters in young women of the same age in the general population. By reading and analyzing a larger number of studies that measured renal flow parameters and indexes we concluded that there are not enough studies that have integrally measured RI, PSV and EDV and compare them with the same flow parameters in the women general population (9, 18, 19, 20, 21, 22). Some of the mentioned studies examined only RI in pregnant, some of them measured RI and pulsatility index (PI) (23), or PI only, some measured PSV and EDV or their Systolic/Diastolic ratio (24), with or without comparing with the young women from the general population, but none of them have studied integrally all the essential Doppler parameters and their associations as in our study. The aim of the study was to find the differences between renal flow parameters in two women population (pregnant and nonpregnat) and to find the associative connection of those Doppler parameters with certain stages of the gestation period.
We found statistically high significance between the mean RI in pregnant and control group participants. Renal RI in pregnant patients is greater than renal RI in the control group. This difference is reasonable for an explanation because the kidneys are larger during pregnancy, maternal blood volume and cardiac output increase
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 27
with pronounced fall in peripheral vascular resistance due to systemic vasodilatation (1, 25). Hemodynamic changes in the kidneys of pregnant women are so progressive and dramatic that initial renal RI changes and differences are occurring in early gestational age. These differences in the renal vascular resistance expressed by the renal RI are evident between pregnant and control group, but also between pregnant patients from each gestational group during pregnancy. The renal RI estimation in our study deliberately excluded the pregnant women under 10 weeks of gestation, to avoid early mechanism of hemodynamic adaptation, so-called normal circulatory adaptation to pregnancy (26). The elevation of renal RI according gestational age is evident in our and many clinical studies that investigated the renal RI (18, 19, 20). Evidently higher renal RI values were measured in the second group (20 to 29 weeks) than the RI in the first group (10 to 19 group, p = 0.002). In the third gestational group (30 to 37 weeks) we registered a small but still significant (p = 0.041) decreases of renal RI. The decrease of renal artery RI in last trimester of pregnancy is induced by mechanisms responsible for mediating the changes in systemic hemodynamics which have not yet been completely elucidated: nitric oxide (NO) production is elevated in normal pregnancy and that these increases appear to play important role in the vasodilatation especially in the last period of pregnancy; hormonal factors such as estrogen and relaxin are thought to be important in stimulating of NO production during pregnancy (25, 26). A greater value of RI in right than in left renal artery and high statistically significant difference between left and right renal artery RI was found in both examined groups (pregnant and control group, p < 0.0001). A greater value of RI in right renal artery than left renal artery RI during pregnancy, but also in the control group, in their studies found Kurjak et al, 1992 (18), Hertzber et al, 1993 (19) and Dibb FR et al, 2003, too (20). Hertzberg et al 1993, concluded that an elevated resistivity index during pregnancy should not be attributed to the normal physiologic changes of pregnancy (19).
The results of our study are closest to the results of Dib FR 2003 study (20), only (p = 0.484). The results of other studies (18, 19) are significantly differed from the results in our study. The relatively small number of participants, the different criteria for including patients with or without physiologic pelvicaliectasis of pregnancy, the different start-point and gestational interval while authors formed gestational groups, are part of possibilities from which the possible differences in renal RI may arise between our and above studies. This predisposing occurrence of higher RI in right kidney is explained with a right sided preponderance of hydronephrosis or calyceal dilation in up to 86% of pregnant women and anatomical positioning of the right ureter which crosses the iliac and ovarian vessels at an angle before entering the pelvis, whereas the left ureter travels at less acute an angle, travelling in parallel with the ovarian vein. This asymmetry has an equal importance to both pregnant and general population and could not be explained by a hormonal effect during pregnancy (1, 27).
Although some studies (18, 19, 20, 27) and our study too showed a slightly increase of the renal RI during second trimester of the pregnancy, the general trend of linear regression line which presents inverse correlation between RI and gestational age, showed a linear decline, but such changes were not statistically significant (p = 0.0698). We believe that this inverse correlation with statistical value close to 0.05 would be statistically significant if the number of patients examined increases. Only Kurjak et al, 1992 (18) found a significant correlation between RI of left renal artery and gestational age (P < 0.050).
The relatively small number of respondents in each gestational period subgroups (n = 18, 23, 24) does not allow us to present enough statistically significant data so that we can conclude there is strong correlation between the renal RI and the gestational age. A greater hope for the possible existence of a correlative relationship between Doppler haemodynamic parameters and gestational age, gave us the possibility to make linear
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 28
regression analysis between PSV and EDV with gestational age. By the equation of linear regression analysis we found strong positive correlation between EDV and gestational age (p = 0.0048), but not between PSV and gestational age. We found a rise in diastolic speed of approx. 0.7 cm/s for every ten months of gestational age. Based on their coefficient of determination (R2), EDV changes in dependent of gestational age are more than two and a half time pronounced than changes in PSV. This described alteration in diastolic flow, more pronounced than systolic flow, are consequence of renal vasodilatation, renal plasma flow and glomerular filtration rate (GFR) both increase compared to non-pregnant levels. Vascular resistance decreases in both renal afferent and efferent arterioles and therefore, despite the massive increase in renal plasma flow, glomerular hydrostatic pressure remains stable, avoiding the development of glomerular hypertension. These changes are continuously increasing until the end of pregnancy as a compensatory mechanism to avoid the development of glomerular hypertension (29, 30).
Even if we express the perfusion parameters of the kidney as quotient (PSV/EDV ratio), instead PSV or EDV only, the summary changes in systolic and diastolic flow still remain in strong inverse correlative association with the gestational age, statistically significant of course (P = 0.0292). Continuous increase of EDV during pregnancy, compared with PSV, reduces the PSV/EDV quotient resulting in an inverse correlation of this ratio with gestational age.
In conclusion, our analysis shows that pregnancy reduces renal vascular resistance (RI) and increases renal flow. We found statistically high significance between the mean renal RI in pregnant and RI in the control group, with significant differences between left and right sides; between the mean RI among every groups according gestational age; a small rise of renal RI during first to second trimester with a decline of renal RI in the last trimester of pregnancy, although on the basis of the various transformations caused by pregnancy in renal physiology and hemodynamics we would expect a reduction of the RI. This reduction is confirmed with inverse correlation of renal RI and gestational age with statistical significance very close to p = 0.05. The EDV value changes according gestational age are a more than two and a half time bigger than changes in PSV. The EDV value has a greater diagnostic significance for assessing the renal function in pregnancy than PSV and RI.
ReferencesCheung KL, Lafayette RA. Renal Physiology of Pregnancy. Adv Chronic Kidney Dis. 2013; 20(3): 209-214.1.
Rasmussen PE, Nielson FR. Hydronephrosis in pregnancy: a literature survey. Eur J Obstet Gynecol Reprod 2. Biol. 1988; 27(3):249–259.
Beydoun SN. Morphologic changes in the renal tract in pregnancy. Clin Obstet Gynecol. 1985; 28(2): 249. 3.
Strevens H, Wide-Swensson D, Hansen A, Horn T, Ingemarsson I, Larsen S. Glomerular endotheliosis in 4. normal pregnancy and pre-eclampsia. BJOG. 2003; 110(9): 831–836.
Tublin ME, Bude RO, Platt JF. The resistive index in renal Doppler sonography: where do we stand? AJR Am 5. J Roentgeneol. 2003; 180(4): 885-892.
Klahr S. Pathophysiology of obstructive nephropathy: a 1991 update. Semin Nephrol. 1991; 11: 156 –168.6.
Viazzi F, Leoncini G, Derchi LE, Pontremoli R. Ultrasound Doppler renal resistive index: a useful tool for the 7. management of the hypertensive patient. Journal of Hypertension. 2014; 32(1): 149-153.
McDermott RA, Teefey S A, Middleton W D, Windus DW, Hildebolt CF. The resistive index in renal parenchymal 8. disease: no correlation with histopathologic findings. Radiology. 2000; 217: 560.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 29
Ogunmoroti O A, Ayoola O O, Makinde O.N, Idowu BM. Maternal renal artery Doppler sonographic changes 9. in pregnancy-induced hypertension in South West Nigeria. Niger Med J: J Nigeria Med Assoc 2015; 56(3): 190–193.
Samoni S, Nalesso F, Meola M, Villa G, De Cal M, De Rosa S et al. Intra-Parenchymal Renal Resistive Index 10. Variation (IRRIV) Describes Renal Functional Reserve (RFR): Pilot Study in Healthy Volunteers. Frontiers in Physiology. 2016; 7: 286.
Darmon M, Schnell D, Zeni F. Doppler-Based Renal Resistive Index: A Comprehensive Review. Yearbook of 11. Intensive Care and Emergency Medicine 2010; 331-338.
Krumme B, Blum U, Schwertfeger E, Flügel P, Höllstin F, Schollmeyer P et al. Diagnosis of renovascular 12. disease by intra and extrarenal Doppler scanning. Kidney Int. 1996; 50: 1288-1292.
Lerolle N, Guerot E, Faisy C, Bornstain C, Diehl JL, Fagon JY. Renal failure in septic shock: predictive value of 13. Doppler-based renal arterial resistive index. Intensive Care Med. 2006; 32: 1553–1559.
Keogan MT, Kliewer MA, Hertzberg BS, DeLong DM, Tupler RH, Carroll BA. Renal resistive indexes: variability 14. in Doppler US measurement in a healthy population. Radiology. 1996; 199 (1): 165-169.
Mostbeck GH, Gössinger HD, Mallek R, Siostrzonek P, Schneider B, Tscholakoff D. Effect of heart rate on 15. Doppler measurements of resistive index in renal arteries. Radiology. 1990; 175(2): 511-513.
Avramovski P. Value of Ultrasound Machine Settings Optimization for Better Diagnosis of Focal Liver 16. Lesions. Open Access Maced J Med. 2009; 15(22): 149-152.
Boddi M, Bonizzoli M, Chiostri M, Begliomini D, Molinaro A, Tadini Buoninsegni L et al. Renal Resistive 17. Index and mortality in critical patients with acute kidney injury. Eur J Clin Invest. 2016; 46(3): 242-251.
Kurjak A, Vidovic MI, Velemir D, Zalud I. Renal arterial Resistance Index in pregnant and nonpregnat women: 18. evaluation with color and pulse Doppler ultrasound. J Perinat Med. 1992; 20(1): 11-14.
Hertzberg BS, Carroll BA, Bowie JD, Paine SS, Kliewer MA, Paulson EK et al. Doppler US assessment of maternal 19. kidneys: analysis of intrarenal resistivity indexes in normal pregnancy and physiologic pelvicaliectasis. Radiology. 1993; 186(3): 689-692.
Dib FR, Duarte G, Sala MM, Ferriani RA, Berezowski AT. Prospective evaluation of renal resistance and 20. pulsatility indices in normal pregnant women. Ultrasound Obstet Gynecol. 2003; 22(5): 515-519.
Miyake H, Nakai A, Koshino T, Araki T. Doppler velocimetry of maternal renal circulation in pregnancy-21. induced hypertension. J Clin Ultrasound. 2001; 29(8): 449-455.
Boemi G, Bruno MT, La Ferrera G, Butera L, Pulvirenti G, Lanzone A et al. Maternal renal and interlobar 22. arteries waveforms evaluation with color Doppler ultrasound in pregnancy-induced hypertension. Fetal Diagn Ther. 1996; 11(2): 132-136.
Sturgiss SN, Martin K, Whittingham A, Davison JM. Assessment of the renal circulation during pregnancy 23. with color Doppler ultrasonography. Am J Obstetr Gynecol. 1992; 167(5): 1250-1254.
Hata T, Hata K, Aoki S, Takamiya O, Murao F, Kitao M. Renal arterial blood flow velocity waveforms in 24. pregnant women. Am J Obstet Gynecol. 1987. 157 (5): 1269-1271.
Michael EH, Eric MG, Joey PG. The heart during pregnancy. Rev Esp Cardiol. 2011; 64(11): 1045-1050.25.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology

Page 30
Sladek SM, Magness RR, Conrad KP. Nitric oxide and pregnancy. Am J Physiol. 1997; 272 (2): 441-463.26.
Ansarin K, Bavil A.S, Ghabili K, Shoja MM, Khosroshahi HT, Hajipour B et al. Are Doppler ultrasonography 27. parameters symmetric between the right and left kidney? Int J Gen Med. 2010; 3: 371–373.
Andriani G, Persico A, Tursini S, Ballone E, Cirotti D, Lelli Chiesa P. The renal-resistive index from the last 3 28. months of pregnancy to 6 months old. BJU Int. 2001; 87(6): 562-564.
Priya Soma-Pillay, Nelson-Piercy Catherine, Heli Tolppanen, Alexandre Mebazaa, Heli Tolppanen, Alexandre 29. Mebazaa. Physiological changes in pregnancy. Cardiovasc J Afr. 2016; 27(2): 89-94.
Kirk P. Conrad, John M. Davison. The renal circulation in normal pregnancy and preeclampsia: is there a 30. place for relaxin? Am J Physiol Renal Physiol. 2014; 306(10): 1121–1135.
Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population
American Research Journal of Gynaecology
Citation: Maja Avramovska, Goran Dimitrov, Marija Hadzi Lega, Elena Dzikova, Gligor Tofoski, Ana Daneva Markova, “Changing of Doppler Renal Flow Parameter in Pregnancy Compared with General Population”. American Research Journal of Gynaecology, 1(1): 18-30.
Copyright © Maja Avramovska, Goran Dimitrov, Marija Hadzi Lega, Elena Dzikova, Gligor Tofoski, Ana Daneva Markova, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.