Embed Size (px)
Citation preview

Molecular and Cellular Pathobiology
Alterations of Choline Phospholipid Metabolism inEndometrial Cancer Are Caused by Choline Kinase AlphaOverexpression and a Hyperactivated Deacylation Pathway
Sebastian Trousil1, Patrizia Lee2,3, David J. Pinato3, James K. Ellis2, Roberto Dina4, Eric O. Aboagye1,Hector C. Keun2, and Rohini Sharma3
AbstractMetabolic rearrangements subsequent to malignant transformation are not well characterized in
endometrial cancer. Identification of altered metabolites could facilitate imaging-guided diagnosis,treatment surveillance, and help to identify new therapeutic options. Here, we used high-resolution magicangle spinning magnetic resonance mass spectroscopy on endometrial cancer surgical specimens andnormal endometrial tissue to investigate the key modulators that might explain metabolic changes,incorporating additional investigations using qRT-PCR, Western blotting, tissue microarrays (TMA), anduptake assays of [3H]-labeled choline. Lipid metabolism was severely dysregulated in endometrial cancerwith various amino acids, inositols, nucleobases, and glutathione also altered. Among the most importantlipid-related alterations were increased phosphocholine levels (increased 70% in endometrial cancer).Mechanistic investigations revealed that changes were not due to altered choline transporter expression,but rather due to increased expression of choline kinase a (CHKA) and an activated deacylation pathway,as indicated by upregulated expression of the catabolic enzymes LYPLA1, LYPLA2, and GPCPD1. Weconfirmed the significance of CHKA overexpression on a TMA, including a large series of endometrialhyperplasia, atypical hyperplasia, and adenocarcinoma tissues, supporting a role for CHKA in malignanttransformation. Finally, we documented several-fold increases in the uptake of [3H]choline in endometrialcancer cell lines compared with normal endometrial stromal cells. Our results validate deregulated cholinebiochemistry as an important source of noninvasive imaging biomarkers for endometrial cancer. CancerRes; 74(23); 6867–77. �2014 AACR.
IntroductionEndometrial cancer (EC) is the most common gynecologic
malignancy in North America and Europe, and despiteresearch efforts, the 5-year overall survival in patients withmetastatic disease remains less than 20%. Themain risk factorin the development of endometrial cancer is unopposed estro-gen, a complication of obesity, hence the incidence of endo-metrial cancer is projected to dramatically increase in the nextdecade (1).
Early-stage endometrial cancer can be effectively managedwith surgery with a 5-year survival of >80%. Although surgery iscurative in patients with disease confined to the uterus,lymphovascular invasion and spread to the regional lymphnodes are most important prognostic factors in endometrialcancer, and will dictate the choice of adjuvant therapy (2).Currently, patients deemed to be at "high risk" of extrauterinespread undergo staging pelvic lymphadenoectomy such that acertain number of patients will undergo an unnecessary sur-gery, whereas others will be undertreated. Reliable staging,therefore, is critical to both the management and prognosticstratification of patients. Conventional imaging techniqueshave limited sensitivity in the assessment of lymph node statusandmore effective imaging modalities are urgently needed (3).Understanding the metabolic and biochemical changes thatunderlie the malignant progression of the disease would allowutilization of noninvasive molecular imaging techniques forclinical staging and follow-up. Furthermore, as an increasingnumber of novel targeted therapies are entering clinical trial,more effective imaging can facilitate drug development effortsin this tumor type, aid patient stratification, and therebyimproving clinical outcome.
Choline (Cho) is an essential nutrient that is phosphorylatedto phosphocholine (PCho) by choline kinase (CHK) and then
1Comprehensive Cancer Imaging Centre at Imperial College, Faculty ofMedicine, Imperial College London, London, United Kingdom. 2Depart-ment of Surgery and Cancer, Imperial College London, London, UnitedKingdom. 3Department of Experimental Medicine, Imperial College Lon-don, London,UnitedKingdom. 4Department of Pathology, Imperial CollegeNHS Trust, London, United Kingdom.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Author: Rohini Sharma, Senior Lecturer Medical Oncol-ogy and Clinical Pharmacology, Imperial College London, HammersmithCampus, Du Cane Road, W12 0HS London, United Kingdom. Phone: 077-26403043; Fax: 020-83833720; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-13-2409
�2014 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 6867
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

incorporated into the cell membrane via the Kennedy pathway(4). CHK exists in at least three isoforms, a1, a2 (CHKA), and b(CHKB), of which the alpha but not beta isoforms have beenassociated with malignancy (5). CHKA overexpression, elevat-ed Cho uptake, and PCho formation have been shown in a widearray of human cancers, including breast, ovarian, lung, andprostate cancer (6–10). These changes in choline handling havemost commonly been studied using magnetic resonance spec-troscopy (MRS). 1H MRS studies report alterations in thespectral profile in the region of 3.20 to 3.24 ppm that areindicative of PCho, glycerophosphocholine (GPC), and freeCho. In the majority of tumor models, an increased PCho:GPCratio has been reported compared with normal tissues (11).More recently, the enzyme endometrial differential 3 has beenidentified as cleaving GPC to form glycerol-3-phosphate andcholine, whichmay also contribute to the increased PCho:GPCratio (12). Mechanisms of PCho accumulation within tumorcells can occur via a number of mechanisms includingenhanced choline transport, CHKA dedicated phosphoryla-tion, and activation of phosphatidylcholine-specific phospho-lipases. Furthermore, overexpression of CHKA (6–8) and abun-dance of choline metabolites (13–15) have been shown to beprognostic in a number of cancers including prostate, breast,lung, and ovarian cancer. More recently inhibition of CHKA,both by shRNA and small-molecule inhibitors, has been shownto have both an antimitogenic and antiproliferative effectsin vitro and in vivo (16–21).
Celik and colleagues identified an abnormal choline signal inproliferating endometrium comparedwith endometrial cancerby spectroscopy (7). However, neither alterations in cholinephospholipid metabolism in the development of endometrialcancer nor alterations in CHKA expression and activity havebeen considered in endometrial cancer, and may representboth a novel therapeutic target and imaging strategy. The aimof this study was therefore to confirm an altered choline profilein endometrial cancer compared with normal endometrialtissue from patients using high-resolution magic angle spin-ning (HR-MAS) 1H nuclear magnetic resonance (NMR) tech-nique. We then further investigated alterations in the enzymesresponsible for choline homeostasis and choline uptake inendometrial cancer using comparative mRNA analysis ofrelevant genes. We then considered whether the expressionof CHKA correlates with progressive histologic changes from anormal endometrial tissue, hyperplasia, and endometrial can-cer using a tissue microarray (TMA) approach. Furthermore,we investigated differential activity of CHKA using radioactiv-ity uptake studies.
Materials and MethodsClinical specimens
Fresh-frozen endometrial tissue (�5 mm3) was obtainedfollowing approval from the Hammersmith Hospital tissuebank (London, United Kingdom). Informed consent to useleftover biologic material for investigative purposes wasobtained from all patients. Samples were taken at the time ofinitial surgery from 20 patients, 10 with histologically con-firmed grade III endometrioid endometrial cancer and 10 with
normal endometrium. The median age of the sample set withnormal tissue was 47.8 years, whereas with the cancer set was65.8 years. Samples were immediately frozen in liquid nitrogenand stored within the tissue bank at �80�C until use. Thenatural morphology in this tumor type is that of discretelesions rather than diffuse infiltrate; contamination by non-tumor tissue is deemed negligible.
1H NMR spectral acquisition and analysisTissue preparation and NMR acquisition were undertaken
as per previously published (22, 23). Briefly, for HR-MAS,approximately 5 mm3 (5–18.5 mg) endometrial tissue wasthawed and rinsed with a small volume of 0.9% saline (90 mgNaCl in 10 mL D2O) before being placed into a zirconia rotor(Bruker Biospin). Before spectral acquisition using the BrukerDRX600 spectrometer operating at 600.13-MHz 1H NMR,sufficient time was allowed for the rotor to reach a steadyspin rate of 5 kHz and a temperature of 283 K. Standard 1DNuclear Overhauser Effect Spectroscopy (NOESY)-presatura-tion pulse sequence (RD-90�-t1-90�-tm-90�-AQ) was usedto manually determine the receiver gain, water saturationpower, 90� pulse length, and shimming for each sample. Eachspectrum was acquired with eight dummy scans (to allowsufficient time for the nuclei spin to reach steady state) and32 scans (2.73 seconds per scan). Field homogeneity wasoptimized by measuring the n1/2 (�1.5–2.2 Hz) for L-lactate(d1.33) before the final acquisition and manual adjustment ofthe shim coils (24). To suppress signals arising from macro-molecules, 1D Carr-Purcell-Meiboom-Gill (CPMG) spin-echopulse sequence [RD-90�-{t-180�-t)n-AQ] was used witht ¼ 400 ms and n ¼ 300. For 1D CPMG experiments, 16dummy scans followed by 256 transients were collected. Aline-broadening factor of 0.3 Hz was multiplied to all freeinduction decays before Fourier transformation. For peakassignment, 2D J-Resolved and correlation spectroscopyexperiments were also performed on a selected sample.Spectra were calibrated to the L-alanine resonance (d1.48),phasing and baseline correction were done manually usingTopSpin software (v.3.1, Bruker Biospin). Subsequent dataprocessing was carried out using in-house scripts written inMATLAB (R2011a, Mathworks) by Drs. T.M.D. Ebbels, H.C.Keun, J.T. Pearce, K. Veselkov, and O. Cloarec (Department ofSurgery and Cancer, Imperial College London, London, Unit-ed Kingdom). Ethanol resonances (d1.06–1.31, d3.56–3.75),introduced during sample collection, and the residual waterresonance (d4.68–d5.16) were removed. Regions at d < 0.6and d > 9.0 were also removed to reduce effects of noise atbaseline. Median fold-change normalization was performedon all reduced spectra to compensate for effects arising fromvariation in tissue weight or any systematic preparation error(25). Multivariate analysis (Principal Component Analysisand Partial Least Squares Discriminant Analysis; PLS-DA)was applied to the reduced and normalized data usingSIMCA Pþ software (v.12.0.1, Umetrics). Seven-fold cross-validation and permutation tests were carried out to validatethe robustness of our models and to assess their predict-ability (26). ROC curve analysis was used to indicate themodel's ability to accurately discriminate the presence of
Trousil et al.
Cancer Res; 74(23) December 1, 2014 Cancer Research6868
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

disease. Nonparametric Mann–Whitney U test and Wilcoxonsigned-rank tests were performed using Excel (Microsoft).The Benjamini–Hochberg multiple testing correction (27)was used to assess FDR and counteract multiple hypothesistesting. Specifically for more accurate estimation of ratiosbetween PCho, GPC, and choline, the relative abundance ofthese metabolites was estimated using manual spectraldeconvolution via Profiler (Chenomx) software. The in vitrocell samples were collected and the aqueous metabolitesextracted as previously described (28). Briefly, cold methanolwas used to quench metabolism and lysates extracted in adual-phase process. Chloroform/methanol (300 mL, 2:1, v/v)was added to the dried methanol quenched samples, vor-texed (30 seconds) and centrifuged (16,000�g, 10 minutes).Ultrapure water (300 mL) was added and samples vortexedand centrifuged as before, the aqueous and organic phaseswere then aspirated to fresh sample tubes. To maximizemetabolite recovery, the extraction was repeated and thesamples pooled and dried. Blank samples were also generatedto account for any contamination from the extraction sol-vents. All 1D CPMG experiments were conducted in solutionstate at 600 MHz 1H and 300K using a Bruker AVANCEDRX600C spectrometer fitted with a 5-mm broadband-inverse tube probehead (Bruker Biospin). The spectral datawere processed, digitized, and imported into MATLAB usingin-house scripts (see above). The area under the peak wasmeasured for the PCho and Cho resonances at approximately3.2 ppm and the ratio calculated for each of the threeendometrial cancer cell lines.
Tissue microarray and IHCThree types of TMAs were constructed comprising normal
endometrium (n ¼ 17), endometrial hyperplasia (n ¼ 15), andendometrial cancer (n ¼ 28). Briefly, formalin-fixed, paraffin-embedded specimen and corresponding hematoxylin andeosin (H&E) slides were retrieved from the local pathologyarchive. After review of H&E-stained sections, three 1-mmcores were identified from themost representative areas of thetumor tissue, then re-embedded into recipient TMA blocksusing an MTA-1 Manual Tissue Microarrayer (Beecher Instru-ments). Consecutive 4-mm thick sections of the TMA blockswere cut and stained for CHKA using an automated protocolon a Bond Max Autostainer (Leica Microsystems) using thePolymer-HRP system (BioGenex) with subsequent develop-ment in diaminobenzidine and Mayer's Hematoxylin counter-staining. CHKA rabbit polyclonal antibody (Sigma-Aldrich,HPA024153) was used at a 1:25 dilution in Dako REAL antibodydiluent (Dako) and the Dako EnVisionþ System- Peroxidase/DABþ Rabbit kit (Dako) secondary antibody was used tovisualize antibody binding. Slides were counterstained withhematoxylin. Normal bronchial tissue was used as positivecontrol to confirm reaction specificity. Omission of the pri-mary antibody was used as negative control reaction. Tissuesamples were scored manually using the immunohistochem-ical score method (IHS), as described previously (29). Briefly,each sample was assigned an IHS ranging between 0 and 300,based on the product of the percentage of cells showing IHCexpression (0–100) and the intensity of the signal (graded 1–3).
Every core was assessed individually. A composite score of0 to 300 was generated from the product of intensity andpercentage. A final score on a scale of 0 to 3 was obtained; 0, noexpression; 1, weak expression (composite score <100); 2,moderate expression (composite score 101–200), and 3, strongexpression (composite score 201–300). For statistical purposes,immunoexpression patterns were divided into two groups:reduced phenotype with a staining scored 0 or 1 and preservedphenotype with a staining scored 2 or 3. The pattern of stain-ing (cytoplasmic, membranous, nuclear, or diffuse) was alsodescribed in each case. Two observers (R. Dina and R. Sharma)scored all the cases independently, blindly from clinical dataand results were found to be consistent.
Real-time PCRRNA was extracted from cells using RNeasy Mini Kit (Qia-
gen) according to manufacturer's instructions and 1 mg totalRNA reverse-transcribed using QuantiTect Reverse Transcrip-tion Kit (Qiagen). Gene expression was analyzed by qRT-PCRusing SYBR green method and Platinum SYBR Green qPCRSuperMixUDG (Invitrogen) master mix according to manu-facturer's instructions. The reaction was run in a total volumeof 20 mL using 25 ng cDNA at a final primer concentration of400 nmol/L. The following custom designed primers weresupplied by Invitrogen: CHKA (Fwd. CGGAAGTATCCCACCA-AGAA; Rev. TCCCCAGAGGAAATGAGATG), CHKB (Fwd. TG-GTGCTAGAAAGCGTGATG; Rev. GCCGACTTGGGATGTACT-GT), PCYT1A (Fwd. GCAACCAGCTCCTTTTTCTG; Rev. GCAA-ACTCCCACAATGAGGT). The following primers were customdesigned by PrimerDesign Ltd: PCYT1B (Fwd. TCTAAGTGT-TCCTGCTGAGTTG; Rev. CATACCCATACAATAACCCAAA-GAG), CHPT1 (Fwd. TCTGCTCTTTTATTGGGATGTTTG; Rev.CAACACAAAGACAATCACTAAAGC), SLC44A4 (Fwd. GGCA-TACGGCATCTACTACTG; Rev. TGGTAGGCACTGAGGTTGG),SLC22A3 (Fwd. TAGGACTTCTCGGCTCTGC; Rev. CATGCT-CTTTGTTCACTCCAC), GPCPD1 (Fwd. CCCTGGACTTC-CTCTCTGTC; Rev. GAAGTTTCCACAAGGGCTCAG), LYPLA1(Fwd. AGAAACTGGCAGGTGTCAC; Rev. GTGGCACTGGA-GAATAGAAATATC), LYPLA2 (Fwd. AAGAAGGCAGCAGA-GAACATC; Rev. CTCCCAGGACGATTCGATTG), SLC5A7 (Fwd.CCCTCAGCTCAACTTTCACC; Rev. GATGGGGTCACTGTAA-ATTATCTTC), PLD1 (Fwd. CTCTGCTGCTGATTGGTCTG;Rev. GATATAGATATAGTGGCCTGCTGTTC).
Gene expression assays were performed on an ABI 7900HTFast Real-Time PCR machine (Applied Biosystems) under thefollowing conditions: 50�C for 2minutes, 95�C for 2minutes, 40cycles of 95�C for 3 seconds, and 60�C for 30 seconds. Datawereanalyzed using comparative Ct method as previously describedwith PPIA (Fwd. CTGCACTGCCAAGACTGA; Rev. CATT-CCTGGACCCAAA) as an internal control (30).
Western blotting in tissuesTissue samples were homogenized in RIPA buffer contain-
ing protease and phosphatase inhibitors (all Sigma-Aldrich)using a Precellys 24 homogenizer with CK14 beads. Homo-genates were cleared of debris by centrifugation at 5,000 � gat 4�C for 5 minutes. Supernatants were recovered and 20 mgprotein was resolved on a 4% to 15%Mini-PROTEAN TGX gel
Choline Metabolism in Endometrial Cancer
www.aacrjournals.org Cancer Res; 74(23) December 1, 2014 6869
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

(Bio-Rad) and transferred to a polyvinylidene difluoridemembrane using Trans-Blot Turbo Transfer Pack (Bio-Rad).Membranes were blocked for 1 hour in 5% milk in TBScontaining 0.1% v/v tween (Cell Signaling Technology) andincubated with the following antibodies in 5%milk overnightat 4�C: CHKA (Sigma-Aldrich, HPA024153) and b-actin(Abcam, ab6276). Secondary horseradish peroxidase(HRP)-conjugated rabbit and mouse antibodies (Santa CruzBiotechnology; sc-2004 and sc-2005) were applied for onehour at room temperature. Signals were visualized usingAmersham ECL Western Blotting Detection Reagent (GEHealthcare) and Amersham Hyperfilm (GE Healthcare).
Cell cultureIshikawa (Health Protection Agency Culture Collections) and
HEC-1B (ATCC) were maintained in DMEM (Invitrogen). Endo-metrial stromal cells, St-T1B, were a kind gift of Professor JanBrosens (University ofWarwick, Coventry, United Kingdom) andcultured in DMEM/F12. All media were supplemented with 10%FCS, glutamine, penicillin, and streptomycin. Cells were incu-bated at 37�C in a humidified atmosphere containing 5% CO2.Commercially available cell lines were authenticated by providerby short-tandem repeat analysis and immediately expanded.Low-passage stocks were used for studies.
[3H]-choline uptake assaySt-T1B, HEC-1B and Ishikawa cells were plated into 6-well
plates at a density of 5 � 105 cells per well. The following day,
cells were pulsed with 0.1 mCi/mL [3H]choline (PerkinElmer)for one hour then washed once with PBS, trypsinized, andcentrifuged. The cell pellet was washed three times with PBSand lysed in RIPA buffer (Sigma-Aldrich). Radioactivity wasmeasured on a scintillation counter after addition Ultima Goldscintillation cocktail (PerkinElmer). Counts were normalizedto protein content as determined by BCA assay (Pierce).
Statistical analysisUnless stated otherwise, data were analyzed using either
GraphPad Prism software version 5.01 or SPSS version 5.01.Statistical significance of differences was determined as spec-ified and a P value of <0.05 deemed significant.
ResultsMAS analysis illustrates unique endometrial cancerspectra compared with normal endometrial tissue andincreased levels of choline-containing metabolites inendometrial cancer tissue
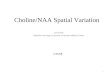
CPMG-derived 1H NMR spectra analysis of the tissue sam-ples revealed prominent differences in concentration of mul-tiple metabolites (Fig. 1A). In total 18 samples (10 normalendometrial tissue and 8 endometrial cancer) were analyzed.Two samples were excluded from further analysis due to poorspectral quality. To model all these differences, a total of68 spectral regions covering most distinguishable resonancesacross the spectra were integrated for multivariate analysis.
×10–4
12
A
B C D
10
8
6
Rel
ativ
e in
tens
ity (
a.u.
)
4
2
04.5 4 3.5 3
1H Chemical shift (ppm)
2.5 2 1.5 1
Glucose
myo-inositol
Taurine
Creatine
Glutathione
GlutamineGlutamate
Alanine
Lactate
BCAAsInosine/adenosine
10
5
0PC
2
PC1
–5
Control
Cancer
–10
–10 –5 0 5
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
–0.1
–0.1
–0.2
–0.3
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7
R2Y=0.950Q2Y=0.757
0.8 0.9 1.0
1
0.9
0.8
0.7
True
pos
itive
rat
e
False positive rate
0.6
0.5
0.4
0.3
0.2
0.1
00 0.2 0.4 0.6
AUC = 0.98750.8 110
Figure1. 1HHRMASNMRspectralanalysis of endometrial tissuereveals metabolic perturbations inendometrial cancer. A, meanspectra (1D-CPMG experiments)for tumor (n¼ 8) and normal tissue(n ¼ 10); BCAA, branched chainamino acids. B–D, multivariateanalysis of endometrial tissuebased on integrals of metabolitedata extracted from 1H HR MASNMR CPMG spectra. B,unsupervisedPCAscores plot (UVscaled) of the first two principalcomponents reveal discriminationbetween control (black squares)and cancer (red diamonds)groups, with each pointrepresenting a patient's metabolicprofile. C, validation of the two-component PLS-DA model bypermuting 999 randomcombinations of the class matrix,giving P ¼ 0.001. R2Y and Q2Yrepresent cumulative values forthe two-component model,measuring "goodness of fit" and"goodness of prediction,"respectively. D, the ROC curvesummarizes the diagnosticaccuracy in classifyingendometrial cancer and controls.
Trousil et al.
Cancer Res; 74(23) December 1, 2014 Cancer Research6870
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

Unsupervised principal component analysis (PCA) with unitvariance scaling was initially used to look for visible separationbetween the metabolic profiles of different classes. Thisrevealed a clear division between the normal endometrialtissue and cancer groups inmodel scores (Fig. 1B). To examinefurther the relationships between cancer and normal endo-metrial tissue, PLS-DA was exploited to model specifically thecovariance between the class membership of the samples andspectral variables. The resulting two-component modelexplained 95% of the class variance (R2Y), which fell to75.7% with cross-validation (Q2Y). A permutation test wheremodels were generated on randomly classified data indicatedthat these model statistics were significant (Fig. 1C). The ROCcurve, based on fitted Y values, gave an AUC of 0.9875 indica-tive of the ability of themodel to positively identify endometrialcancer from normal endometrial tissue (Fig. 1D).Following the establishment of a valid and significant
model, we began to deconvolute the metabolic fingerprintof endometrial cancer to identify the metabolites contrib-uting to the classification of normal endometrial tissue andendometrial cancer observed in the PLS-DA model. Figure 2illustrates a variable importance for the projection (VIP)plot, which summarizes in order of the overall importanceindividual metabolite/regions that correlates to our model.The metabolites observed to be contributing most to theclassification model were PCho, myo-inositol, nucleosides,glutathione, several amino acids, lipids, and glucose, sug-gesting generally deregulated metabolism in endometrialcancer. To confirm which metabolite changes were statis-tically significant, we compared the integrals of individualmetabolites of cancer against control using Mann–WhitneyU test, which provided a semiquantitative analysis in termsof relative metabolite concentration change. In the casewhere one metabolite has more than one signal across thespectrum, the one with the least signal overlapping wasselected; for metabolites of low abundance (e.g., phenylal-anine), the signal with the highest contrast from the baseline
was selected on the basis of visual inspection, otherwise themetabolites with negative integrals were excluded (e.g.,uracil), as signal-to-noise ratio tends to be relatively poorupfield of the NMR spectrum. Out of the 44 metabolitestested, metabolites showing statistical significance weresimilar to those observed from our multivariate model(Table 1; a list of all metabolites is summarized in Supple-mentary Table S1). In endometrial cancer, significantlyelevated metabolites included a number of amino acids,leucine, valine, alanine, proline, tyrosine, in addition to PChoglutathione, inositols, inosine/adenosine, and unsaturatedlipids and triglycerides. Importantly, on superimposingspectra from normal endometrial tissue and endometrialcancer, a significantly increased PCho:Cho ratio (1.59-fold)was detected in endometrial cancer compared with normalendometrial tissue, indicative of activated CHK (Fig. 3). Nosignificant differences were observed in GPC and Cho con-tent, whereas an increase in the PCho:GPC ratio (1.29-fold)approached but did not reach significance (P ¼ 0.08).
Expression of enzymes responsible for phosphocholinesynthesis is increased in endometrial cancer
Increased levels of PCho can be attributed to increasedCho uptake and CHKA activity or increased activity ofphospholipid catabolic pathways. To establish which aspectsof the choline biochemistry are deregulated in endometrialcancer, we investigated the mRNA expression of enzymesinvolved in differing aspects of choline metabolism usingtissues from normal endometrial tissue (n ¼ 10) and gradeIII endometrioid endometrial cancer (n ¼ 10, Fig. 4A). Weobserved a significant increase in the expression of CHKA(P ¼ 0.02), GPCPD1 (P ¼ 0.01), LYPLA1 (P < 0.01), andLYPLA2 (P ¼ 0.01) in endometrial cancer compared withnormal endometrial tissue, but found no alterations inexpression of the organic cation transporters or cholinetransporter-like proteins. These results suggest that thedeacylation pathway may be activated in clinical specimens
Figure 2. VIP plot for PLS-DAmodel discriminating endometrial cancer from normal endometrial tissue. Error bars are computed as the 'jack-knife' estimate ofthe 95% confidence intervals. X, unassigned resonance.
Choline Metabolism in Endometrial Cancer
www.aacrjournals.org Cancer Res; 74(23) December 1, 2014 6871
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

of endometrial cancer and the generated Cho is consequent-ly converted by CHKA to PCho, which results in the highPCho accumulation in the metabolic profile.
Choline kinase is overexpressed in endometrial cancercompared with normal endometrial tissue andendometrial hyperplasia
Because of the high intracellular accumulation of PCho, wehypothesized that CHKA is a key driver for deregulated cholinebiochemistry and further investigated the role of CHKA inendometrial cancer. In an initial study, we performedWesternblot analysis on the same sample set we used for mRNAanalysis and found an increased expression of CHKA in endo-metrial cancer compared with normal endometrial tissue(P < 0.001, Fig. 4B and C). To confirm this, we used a TMAapproach to assess whether the IHC expression of CHKAchanges between normal endometrial tissue, typical and atyp-ical hyperplasia of endometrium and endometrial cancer. Theexpression of CHKA was cytoplasmic in all samples, and asignificantly increased CHKA expression was observed inendometrial cancer and atypical hyperplasia compared withnormal endometrial tissue (c2 test, P < 0.02). However, nodifference was observed between atypical endometrial hyper-plasia and endometrial cancer (Fig. 5A).
Choline kinase activity in endometrial cell linesFinally, to investigate whether upregulated CHKA expres-
sion and activity would allow utilization of choline-based PETexaminations, wemeasured [3H]choline uptake in HEC-1B andIshikawa endometrial cancer cells compared with that of St-T1b endometrial stromal cells. Incorporated radioactivity wasincreased 7- and 12-fold in the two endometrial cancer celllines, respectively, which indicates good differential uptake tostromal tissue (P < 0.001, Fig. 5B). Increased CHKA activity wasfurther confirmed by MRS as denoted by increased PCho/Choratios in cancer cell lines versus normal control (Fig. 5C).Elevated flux was caused by higher baseline expression ofcholine transporters SLC44A, SLC22A3, andCHKA. In addition,we found that, comparably to the patient-derived samples,
× 10-4
12
10 GPC
PCho
Cho8
6
4
2
0
3.24 3.22
Control
PCho:GPC
PCho:choline
GPC:choline 1.63 ± 1.18
2.25 ± 0.83
1.69 ± 0.53
1.73 ± 0.89
3.57 ± 1.65
2.18 ± 0.57
0.8
0.04
0.08
EC P value
1H Chemical shift (ppm)
3.2
Figure 3. Superimposition of mean HR MAS 1H NMR spectra forendometrial cancer and normal endometrial tissue revealing regions forcholine-containing metabolites (3.20–3.24 ppm). Black line, controls(n¼10); gray line, endometrial cancer (n¼8). Table below indicates ratiosof different choline metabolites.
Table 1. Metabolic alterations in endometrial cancer detected by HR MAS 1H NMR
MetaboliteIntegral region(ppm) Multiplicity
Direction ofchange
% Changeto Control P
Valine 0.98–1.00 d " 58.88 0.0019Leucine 0.95–0.98 dd " 44.63 0.0059Alanine 1.47–1.49 d " 40.26 0.0077Proline 1.97–2.03 m " 54.97 0.0019Glutathione 2.51–2.61 m # �43.86 0.0019PCho 3.22–3.23 s " 69.99 0.0100Scyllo-inositol 3.34–3.35 s # �60.12 0.0019Myo-inositol 3.52–3.55 dd # �57.82 0.0005Tyrosine 6.87–6.92 d " 79.09 0.0077Inosine/adenosine 8.23–8.25 s # �54.04 0.0025Lipids 5.26–5.39 m " 3419.99 0.0034
NOTE:Statistically significantmetabolites after Benjamini–Hochbergmultiple testing correction (FDRof 5%);P values are derived fromMann–WhitneyU test. The integral region indicates the signal that was selected for univariate testing. Fold changes are basedonmeanvalues in each tissue type.Abbreviations: s, singlet; d, doublet; dd, double doublet; m, multiplet.
Trousil et al.
Cancer Res; 74(23) December 1, 2014 Cancer Research6872
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

PCYT1B and LYPLA1 and 2 were significantly higher express-ed in cancer-derived cell lines compared with St-T1b (Fig. 5D).
DiscussionAbnormal NMR-detectable metabolic profiles have been
reported in a number of tumor types, including breast, cervical,and colorectal cancers (9, 31–34). However, this has not beenstudied in endometrial cancer. In this study, we investigatedmetabolic alterations in endometrial cancer using comple-mentary approaches with the aim of identifying novel potentialtherapeutic and molecular imaging targets. We reveal anincrease in the PCho pool in endometrial cancer comparedwith normal endometrial tissue that can be attributed to anincrease in CHKA activity and upregulation of enzymesinvolved in the deacylation pathway. Alterations in cholinehandling directly impacts radiolabeled choline uptake allowingPET imaging to be used to assess tumor stage. Furthermore, ascholine biochemistry is intimately involved with cellular pro-liferation, deregulated transporters or enzymes involved incholine handling may act as potential therapeutic targets. Toour knowledge, this is the first study to show altered cholinehandling in endometrial cancer, and moreover this study usesthe novel technique of HR-MAS MRS to illustrate specificalterations in choline metabolites in primary tissue specimensof endometrial carcinoma.A number of studies have investigated the utility of
HR-MAS MRS in cancer where the metabonomic phenotypewas correlated with recognized prognostic features (13, 33,35, 36). Overall these studies illustrate increased total Choresonance signal at approximately 3.2 ppm in cancer com-pared with normal tissue consistent with our findings. PCho,GPC, and Cho all contribute to the total choline resonanceand we report relative levels of PCho, GPC, and Cho con-sistent with previously reported values, with PCho being the
main contributor to the total choline resonance. We re-ported an approximately 70% increase in PCho concentra-tion in cancer compared with normal tissue. Consistent withprevious publications in ovarian and breast cancer, wereport a significant increase in the PCho:Cho ratio(11, 37) and nonsignificant increase in the PCho:GPC ratioin endometrial cancer. We hypothesize that the lack of adistinct PCho:GPC switch, which is associated with onco-genic transformation in breast cancer (11), may not occurin endometrial cancer and that overexpression of GPCPD1identified in endometrial cancer converts GPC via the dea-cylation pathway into free choline, which is again convertedto PCho by CHKA (38, 39).
Considering the changes observed by MAS MRS, we inves-tigated the gene expression of enzymes responsible for phos-phatidylcholine anabolism (Kennedy pathway), catabolism(deacylation pathway), and choline substrate transporters toascertain whether the changes in the choline peak in endo-metrial cancer observed onMAS resulted from the deregulatedintracellular metabolism of choline or transport of exogenouscholine into the cells. Choline flux can only be measuredaccurately in vitro, and as we utilized clinical samples, qRT-PCR was used to assess the expression of transporters. Thechanges in relative gene expression of enzymes involved incholine handling have been studied in a number of tumor typesincluding breast and ovarian cancer, and these studies areconsistent in reporting an increase in the expression andactivity of CHKA in cancer cells compared with normal epi-thelial cells (9, 38). Activation of CHKA results in an increase inthe product, PCho, and product:substrate ratio, PCho:Cho.Furthermore, we report an increase in the expression of CHKAin endometrial cancer compared with normal endometrialtissue by IHC. Of interest, we noted increase in CHKA expres-sion not only in endometrial cancer, but also in hyperplasticendometrial tissue. Our TMA included both simple and
2520
30
1512
10
Fol
d ch
ange
in E
C c
ompa
red
with
nor
mal
8
6
4
2
0
Kennedy pathway Catabolic pathway Transporter
1.0BA
C
0.8
0.6
OD
CH
KA
/ O
D β
-act
in
0.4
0.2
0.0Normal
NormalEEC
CHKA
β-Actin
NormalEEC
ECCHKACHKB
PCYT1APCYT1BCHPT1
GPCPD1LY
PLA1
LYPLA
2PLD
1SLC
44A
SLC22
A3SLC
5A7
Figure 4. Determinants ofderegulated choline metabolism.A, relative fold difference in mRNAexpression of enzymes inendometrial cancer samples(n ¼ 10) compared with controltissue (n ¼ 10). Bar graphrepresents mean of threeindependent qRT-PCRexperiments. For each gene, themean value � SD of the analyzedsamples is reported, Student t test,�, P < 0.05. B and C, Western blotanalysis of same endometrialcancer samples against CHKA andcorresponding densitometryresults (P ¼ 0.0025). ��, P < 0.01.
Choline Metabolism in Endometrial Cancer
www.aacrjournals.org Cancer Res; 74(23) December 1, 2014 6873
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

complex atypical hyperplasia, the latter being premalignantand this may account for the increase in CHKA in thesespecimens. Although our approach illustrates tissue heteroge-neity, the use ofmicrodissection techniques and larger samplessize may reduce the variation observed in the presentedresults. In a number of studies, CHKA has been shown tomediate cellular proliferation, transformation, and carcino-genesis, and mediation of this target using siRNA and small-molecule inhibitors suggests inhibition of tumor growth(11, 16, 18, 40, 41).
As indicated, we further observed in clinical samples andendometrial cancer cell lines, a significant increase in themRNA expression of enzymes of the phosphatidylcholinedeacylation pathway; GPCPD1, LYPLA1, and LYPLA2. Altera-tions of the deacylation pathway have been previously inves-
tigated for its contribution to the relative PCho pool (38, 42).Iorio and colleagues reported a 2- to 4-fold increased levels ofGPC in a number of ovarian cell lines (38), but found no changein the activity of LYPLA1 and 2. Gene expression analysisconducted in breast cancer cell lines illustrated a reductionin the expression of LYPLA1 in cancerous cell lines comparedwith normal controls (9). Discrepancies may arise from the useof whole tissue extracts of endometrial tissue rather than celllines. Furthermore, as we used whole tissue, we were only ableto consider gene expression rather than enzyme activity. It isunclear from the literature whether any posttranslationalmodifications occur for these enzymes and in future studies,it would be important to assess the functional alterations ofthese enzymes in endometrial cancer. Nonetheless, on MAS,the levels of GPC were not significantly altered, despite the
Normal Hyperplasia EC
15
A
B C
D
60
40
20PC
ho:C
ho r
atio
0
10
Rel
ativ
e no
rmal
ized
[3 H]c
holin
e up
take
5
0
30
25
20
15
10
8
mR
NA
rel
ativ
e ex
pre
ssio
n
6
4
2
0
CHKA
Kennedy pathway Catabolic pathway Transporter
CHKB PCYT1A PCYT1B CHPT1 GPCPD1 LYPLA1 LYPLA2 PLD1 SLC44A SLC22A3
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-
T1b
HE
C-1
BIs
hika
wa
St-T1b HEC-1B Ishikawa St-T1b HEC-1B Ishikawa
Figure5. CHKA isoverexpressed inendometrial cancer and causesincreased uptake of radiolabeledcholine. A, representative sectionsof TMAshowingCHKA expressionin normal, hyperplastic, orendometrial cancer samples. Bar,100 mm. B, cells were pulsed with[3H]choline for 1 hour and retainedactivity measured. Uptake of[3H]choline in human endometrialcancer cell lines HEC-1B andIshikawa was compared withthe human endometrial stromacell line St-T1b (error, SEM;��, P < 0.01; ���, P < 0.001). C, theaqueous metabolites wereextracted from the threeendometrial cancer cell lines,analyzed by MRS, and the cholinemetabolites measured. Dataexpressed as PCho/Choratio � SEM and significantdifferences to the St-T1b cell lineindicated (�, P < 0.05; ��, P < 0.01).D, relative mRNA expression ofindicated enzymes involved incholine handling. Expression isshown relative to normal cell line(St-T1b) and statisticalsignificance was determined bycomparison of the cancer cell linesto St-T1b (error, SD; �, P < 0.05;��, P < 0.01).
Trousil et al.
Cancer Res; 74(23) December 1, 2014 Cancer Research6874
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

increased expression of enzymes in the catabolic arm ofcholine handling the complementary activities of cholinephosphorylation, and deacylation could contribute to theunique NMR profile observed in endometrial cancer.The increase in the expression of CHKA in human endo-
metrial cancer compared with normal endometrial tissueprovides further support for the use of choline radiotracersin the staging of endometrial cancer, particularly in patientsat high risk of lymph node involvement where the use ofcholine PET imaging may alleviate the need for staginglymphadenectomy and its accompanied adverse effects. Anumber of studies have investigated the utility of2[18F]fluoro-2-deoxy-D-glucose (FDG) PET in endometrialcancer (3, 43). These studies are limited by poor sensitivitybecause of the rapid excretion and accumulation of FDGwithin the bladder, the largest study reporting 74% sensi-tivity in detecting lymph node involvement (3). The use ofMRS in assessing endometrial cancer is limited by poorspectral signal to noise ratio (7, 44). We have recently shownthe feasibility of imaging using [11C]choline PET-CT indetecting lymph node involvement in high-risk prostatecancer. Furthermore, we suggest a correlation between theexpression of CHKA within prostate cancer specimens with[11C]Choline uptake (6). To this end, we showed differentialuptake of [3H]choline by endometrial cancer cells comparedwith normal stromal by 7- to 12-fold, highlighting thepotential utility of choline radiotracers in imaging endome-trial cancer. The utility of [11C]choline PET/CT was dem-onstrated in a small study of 22 patients, where the accuracyof detecting lymph node involvement was 86%, increasing to96% with both [11C]choline PET/CT and MRI. However, theuse of [11C]choline is limited to institutions with onsitecyclotron given the short half-life of 11C (20.38 minutes).The use of 18F-labeled choline tracers is felt to be limited bybladder uptake; however, this could be alleviated throughthe use of delayed phase imaging, with the novel, moremetabolically stable [18F]Fluoromethyl-[1,2-2H4]-choline orthrough the application of filtering techniques (45). Cholineimaging by PET or MRS has become an established tool ofpreclinical and clinical research and small-molecule inhibi-tors of CHKA are currently in development.Using an unbiased HR-MAS MRS approach, we identified
additional metabolic patterns that illustrate a severelyaltered phenotype in endometrial cancer. The majority ofthese metabolites can be classed into proliferation-asso-ciated markers (e.g., various amino acids and the nucleo-base uracil, which are indicative of high transcriptional andproliferative activity), maintenance of intracellular redoxhomeostasis (glutathione), osmoregulation (inositols, tau-rine), and glucose and lipid metabolism (lactate, acetate,free Cho, PCho, GPC, fatty acids, and unsaturated lipids;ref. 46). Glucose and lipid metabolisms are tightly con-
nected in cancer. Because of the Warburg effect, lessglucose-derived metabolites are fed into the TCA cycle.Consequently, the required intermediates for generation oflipids need to be restored, and acetate, lactate, ketonebodies, and glutamine serve as substitutes (47). Interest-ingly, these metabolites were not increased in our dataset,but the end products, unsaturated lipids and fatty acids(summarized as lipids in Table 1), were among the mostseverely upregulated metabolites.
A limitation of this study is that themenopausal status of thepatients studiedwas not known; however, based on themedianage of the patients in the control cohort and those in the cancercohort, it can be inferred that patients in the control cohortwere likely to be partially premenopausal, whereas those in thecancer cohort were likely to be predominately postmenopaus-al. Changes in MRS spectra caused by cyclical changes of theendometrial tissue or with menopause remain an importantquestion for further investigation.
In conclusion, using a multimodality approach, we haveshown that the expression and activity of CHKA areincreased in human endometrial cancer specimens com-pared with normal endometrium. These findings suggestthat deregulated choline metabolism may represent a sourceof molecular targets with important diagnostic and thera-peutic implications for the management of patients withendometrial cancer.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: S. Trousil, P. Lee, E.O. Aboagye, H.C. Keun, R. SharmaDevelopment of methodology: S. Trousil, P. Lee, E.O. Aboagye, H.C. Keun,R. SharmaAcquisition of data (provided animals, acquired and managed pati-ents, provided facilities, etc.): S. Trousil, P. Lee, D.J. Pinato, J.K. Ellis, H.C.Keun, R. SharmaAnalysis and interpretation of data (e.g., statistical analysis, biostati-stics, computational analysis): S. Trousil, P. Lee, D.J. Pinato, J.K. Ellis, R. Dina,H.C. Keun, R. SharmaWriting, review, and/or revision of the manuscript: S. Trousil, D.J. Pinato,J.K. Ellis, E.O. Aboagye, H.C. Keun, R. SharmaStudy supervision: E.O. Aboagye, R. SharmaOther (histopathology and immunohistochemistry): R. Dina
Grant SupportThis work was funded by Cancer Research UK - Engineering and Physical
Sciences Research Council grant (in association with the Medical ResearchCouncil and Department of Health; England) C2536/A10337. E.O. Aboagye'slaboratory receives core funding from the UK Medical Research Council(MC_US_A652_0030). J.K. Ellis was supported by Cancer Research UK programgrant A15115.
The costs of publication of this article were defrayed in part by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received August 21, 2013; revised August 5, 2014; accepted August 12, 2014;published OnlineFirst September 29, 2014.
References1. Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass
index and incidence of cancer: a systematic review andmeta-analysisof prospective observational studies. Lancet 2008;371:569–78.
2. Wright JD, Barrena Medel NI, Sehouli J, Fujiwara K, Herzog TJ.Contemporary management of endometrial cancer. Lancet 2012;379:1352–60.
Choline Metabolism in Endometrial Cancer
www.aacrjournals.org Cancer Res; 74(23) December 1, 2014 6875
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

3. AntonsenSL, Jensen LN, Loft A, Berthelsen AK,Costa J, Tabor A, et al.MRI, PET/CTandultrasound in thepreoperative staging of endometrialcancer - a multicenter prospective comparative study. Gynecol Oncol2013;128:300–8.
4. Glunde K, Bhujwalla ZM. Metabolic tumor imaging using magneticresonance spectroscopy. Semin Oncol 2011;38:26–41.
5. Gruber J, See Too WC, Wong MT, Lavie A, McSorley T, Konrad M.Balance of human choline kinase isoforms is critical for cell cycleregulation: implications for the development of choline kinase-tar-geted cancer therapy. FEBS J 2012;279:1915–28.
6. Contractor K, Challapalli A, Barwick T, Winkler M, Hellawell G,Hazell S, et al. Use of [11C]choline PET-CT as a noninvasive methodfor detecting pelvic lymph node status from prostate cancer andrelationship with choline kinase expression. Clin Cancer Res 2011;17:7673–83.
7. Celik O, Hascalik S, Sarac K, Meydanli MM, Alkan A, Mizrak B.Magnetic resonance spectroscopy of premalignant and malignantendometrial disorders: a feasibility of in vivo study. Eur J ObstetGynecol Reprod Biol 2005;118:241–5.
8. Ramirez deMolina A, Sarmentero-Estrada J, Belda-IniestaC, TaronM,Ramirez deMolina V, Cejas P, et al. Expression of choline kinase alphato predict outcome in patients with early-stage non-small-cell lungcancer: a retrospective study. Lancet Oncol 2007;8:889–97.
9. Glunde K, Jie C, Bhujwalla ZM. Molecular causes of the aberrantcholine phospholipid metabolism in breast cancer. Cancer Res2004;64:4270–6.
10. Ramirez de Molina A, Rodriguez-Gonzalez A, Gutierrez R, Martinez-Pineiro L, Sanchez J, Bonilla F, et al. Overexpression of choline kinaseis a frequent feature in human tumor-derived cell lines and in lung,prostate, and colorectal human cancers. Biochem Biophys Res Com-mun 2002;296:580–3.
11. Aboagye EO, Bhujwalla ZM. Malignant transformation alters mem-brane choline phospholipid metabolism of humanmammary epithelialcells. Cancer Res 1999;59:80–4.
12. Stewart JD, Marchan R, Lesjak MS, Lambert J, Hergenroeder R, EllisJK, et al. Choline-releasing glycerophosphodiesterase EDI3 drivestumor cell migration and metastasis. Proc Natl Acad Sci 2012;109:8155–60.
13. Jim�enez B, Mirnezami R, Kinross J, Cloarec O, Keun HC, Holmes E,et al. 1H HR-MAS NMR spectroscopy of tumor-induced local meta-bolic "field-effects" enables colorectal cancer staging and prognos-tication. J Proteome Res 2013;12:959–68.
14. Cao MD, Giskeodegard GF, Bathen TF, Sitter B, Bofin A, Lonning PE,et al. Prognostic value of metabolic response in breast cancer patientsreceiving neoadjuvant chemotherapy. BMC Cancer 2012;12:39.
15. Choi JS, Baek H-M, Kim S, KimMJ, Youk JH, Moon HJ, et al. HR-MASMR spectroscopy of breast cancer tissue obtained with core needlebiopsy: correlationwith prognostic factors. PLoSONE2012;7:e51712.
16. Krishnamachary B, Glunde K, Wildes F, Mori N, Takagi T, Raman V,et al. Noninvasive detection of lentiviral-mediated choline kinasetargeting in a human breast cancer xenograft. Cancer Res 2009;69:3464–71.
17. Hernandez-Alcoceba R, Fernandez F, Lacal JC. In vivo antitumoractivity of choline kinase inhibitors: a novel target for anticancer drugdiscovery. Cancer Res 1999;59:3112–8.
18. Trousil S, Carroll L, Kalusa A, Aberg O, Kaliszczak M, Aboagye EO.Design of symmetrical and nonsymmetrical N,N-dimethylaminopyr-idine derivatives as highly potent choline kinase alpha inhibitors.MedChemComm 2013;4:693–6.
19. Sanchez-Lopez E, Zimmerman T, Gomez del Pulgar T, Moyer MP,Lacal Sanjuan JC, Cebrian A. Choline kinase inhibition induces exac-erbated endoplasmic reticulum stress and triggers apoptosis viaCHOP in cancer cells. Cell Death Dis 2013;4:e933.
20. Ramirez de Molina A, de la Cueva A, Machado-Pinilla R, Rodriguez-Fanjul V, Gomez del Pulgar T, Cebrian A, et al. Acid ceramidase as achemotherapeutic target to overcome resistance to the antitumoraleffect of choline kinase alpha inhibition. Curr Cancer Drug Targets2012;12:617–24.
21. Rubio-RuizB,Conejo-Garcia A, Rios-Marco P,Carrasco-JimenezMP,Segovia J, Marco C, et al. Design, synthesis, theoretical calculations
and biological evaluation of new non-symmetrical choline kinaseinhibitors. Eur J Med Chem 2012;50:154–62.
22. Beckonert O, Coen M, Keun HC, Wang Y, Ebbels TM, Holmes E, et al.High-resolution magic-angle-spinning NMR spectroscopy for meta-bolic profiling of intact tissues. Nat Protoc 2010;5:1019–32.
23. Yakoub D, Keun HC, Goldin R, Hanna GB. Metabolic profiling detectsfield effects in nondysplastic tissue from esophageal cancer patients.Cancer Res 2010;70:9129–36.
24. Piotto M, Elbayed K, Wieruszeski JM, Lippens G. Practical aspects ofshimming a high resolutionmagic angle spinning probe. JMagnReson2005;173:84–9.
25. Dieterle F, Ross A, Schlotterbeck G, Senn H. Probabilistic quotientnormalization as robust method to account for dilution of complexbiologicalmixtures. Application in 1HNMRmetabonomics. Anal Chem2006;78:4281–90.
26. Westerhuis J, Hoefsloot HJ, Smit S, Vis D, Smilde A, Velzen EJ, et al.Assessment of PLSDA cross validation. Metabolomics 2008;4:81–9.
27. Benjamini Y, Hochberg Y. Controlling the false discovery rate: apractical and powerful approach to multiple testing. J Roy Stat SocSer B (Stat Method) 1995;57:289–300.
28. Keun HC, Athersuch TJ. Nuclear magnetic resonance (NMR)-basedmetabolomics. Methods Mol Biol 2011;708:321–34.
29. Pinato DJ, Ramachandran R, Toussi ST, Vergine M, Ngo N, Sharma R,et al. Immunohistochemical markers of the hypoxic response canidentifymalignancy in phaeochromocytomasandparagangliomas andoptimize the detection of tumours with VHL germline mutations. Br JCancer 2013;108:429–37.
30. Schmittgen TD, Livak KJ. Analyzing real-time PCR data by the com-parative C(T) method. Nat Protoc 2008;3:1101–8.
31. Backshall A, Sharma R, Clarke SJ, Keun HC. Pharmacometabo-nomic profiling as a predictor of toxicity in patients with inoperablecolorectal cancer treated with capecitabine. Clin Cancer Res 2011;17:3019–28.
32. Cheng LL, Chang IW, Smith BL, Gonzalez RG. Evaluating humanbreast ductal carcinomas with high-resolution magic-angle spinningproton magnetic resonance spectroscopy. J Magn Reson 1998;135:194–202.
33. Sitter B, Bathen T, Hagen Bø, Arentz C, Skjeldestad FE, Gribbestad IS.Cervical cancer tissue characterized by high-resolution magic anglespinning MR spectroscopy. Magn Reson Mater Biol Phys Med 2004;16:174–81.
34. Hasim A, Ali M, Mamtimin B, Ma JQ, Li QZ, Abudula A. Metabo-nomic signature analysis of cervical carcinoma and precancerouslesions in women by (1)H NMR spectroscopy. Exp Ther Med 2012;3:945–51.
35. Chan EC, Koh PK, Mal M, Cheah PY, Eu KW, Backshall A, et al.Metabolic profiling of human colorectal cancer using high-resolutionmagic angle spinning nuclear magnetic resonance (HR-MAS NMR)spectroscopy and gas chromatography mass spectrometry (GC/MS).J Proteome Res 2009;8:352–61.
36. Zietkowski D, Davidson RL, Eykyn TR, De Silva SS, Desouza NM,Payne GS. Detection of cancer in cervical tissue biopsies usingmobilelipid resonances measured with diffusion-weighted (1)H magneticresonance spectroscopy. NMR Biomed 2010;23:382–90.
37. Iorio E,MezzanzanicaD, Alberti P, Spadaro F, Ramoni C,D'AscenzoS,et al. Alterations of choline phospholipid metabolism in ovarian tumorprogression. Cancer Res 2005;65:9369–76.
38. Iorio E, Ricci A, Bagnoli M, Pisanu ME, Castellano G, Di Vito M, et al.Activation of phosphatidylcholine cycle enzymes in human epithelialovarian cancer cells. Cancer Res 2010;70:2126–35.
39. Gallazzini M, Ferraris JD, Burg MB. GDPD5 is a glycerophospho-choline phosphodiesterase that osmotically regulates the osmo-protective organic osmolyte GPC. Proc Natl Acad Sci U S A 2008;105:11026–31.
40. Gallego-Ortega D, Ramirez de Molina A, Ramos MA, Valdes-Mora F,Barderas MG, Sarmentero-Estrada J, et al. Differential role of humancholine kinase alpha and beta enzymes in lipid metabolism: implica-tions in cancer onset and treatment. PLoS ONE 2009;4:e7819.
41. Glunde K, Raman V, Mori N, Bhujwalla ZM. RNA interference-mediated choline kinase suppression in breast cancer cells
Trousil et al.
Cancer Res; 74(23) December 1, 2014 Cancer Research6876
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

induces differentiation and reduces proliferation. Cancer Res 2005;65:11034–43.
42. Eliyahu G, Kreizman T, Degani H. Phosphocholine as a biomarker ofbreast cancer: molecular and biochemical studies. Int J Cancer2007;120:1721–30.
43. Signorelli M, Guerra L, Buda A, Picchio M, Mangili G, Dell'Anna T,et al. Role of the integrated FDG PET/CT in the surgical manage-ment of patients with high risk clinical early stage endometrialcancer: detection of pelvic nodal metastases. Gynecol Oncol2009;115:231–5.
44. SaracK,CelikO,Hascalik S, AlkanA,MizrakB. In vivoprotonmagneticresonance spectroscopy in the evaluation of the endometrium. ActaObstet Gynecol Scand 2004;83:751–7.
45. Gray KR, Contractor KB, Kenny LM, Al-Nahhas A, Shousha S, Steb-bing J, et al. Kinetic filtering of [(18)F]Fluorothymidine in positronemission tomography studies. Phys Med Biol 2010;55:695–709.
46. Griffin JL, Shockcor JP. Metabolic profiles of cancer cells. Nat RevCancer 2004;4:551–61.
47. FrezzaC,PollardPJ,GottliebE. Inborn andacquiredmetabolic defectsin cancer. J Mol Med 2011;89:213–20.
www.aacrjournals.org Cancer Res; 74(23) December 1, 2014 6877
Choline Metabolism in Endometrial Cancer
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409

2014;74:6867-6877. Published OnlineFirst September 29, 2014.Cancer Res Sebastian Trousil, Patrizia Lee, David J. Pinato, et al. Hyperactivated Deacylation PathwayCancer Are Caused by Choline Kinase Alpha Overexpression and a Alterations of Choline Phospholipid Metabolism in Endometrial
Updated version
10.1158/0008-5472.CAN-13-2409doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2014/09/27/0008-5472.CAN-13-2409.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/74/23/6867.full#ref-list-1
This article cites 47 articles, 12 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/74/23/6867.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/74/23/6867To request permission to re-use all or part of this article, use this link
on May 9, 2020. © 2014 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 29, 2014; DOI: 10.1158/0008-5472.CAN-13-2409