-
7/31/2019 ALS and Medical Emergencies in Psychiatry
1/29
ALS and Medical Emergencies in
Psychiatry
John Corish2012
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
2/29
ALS why do I need to know this?
4-fold increase in risk of acute cardiac eventsin people with
schizophrenia
Sudden death
Ventricular arrhythmias
Accelerated atherosclerotic change
Main causes are
Direct pro-arrhythmic effects of antipsychotics Endocrine
changes and obesity rates
Sedentary lifestyle, smoking, poor general health
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
3/29
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
4/29
Basic Life Support (ARC, 2011)
The mnemonic is now D (check for danger before starting)
R (responsiveness is the person rousable or
breathing normally)
S ( send someone for help)
A (airway; clear obstruction, head tilt / jaw thrust)
B
(is the person breathing effectively) C (start chest
compressions; 30 then 2 breaths)
D (attach defibrillator ASAP; follow AED prompts)
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
5/29
Basic Life Support new features
Guidelines now indicate thatunconsciousness and abnormal
breathing are
sufficient to warrant CPR.
Attempting to palpate a pulse not
recommended for lay people.
Clinicians should spend
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
6/29
Advanced Life Support (ARC, 2011)
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
7/29
ALS Step 1 attach the defibrillator
While attaching defibrillator, follow BLS
protocol of 30 compressions followed by 2
breaths.
Place pads on front and back of left side of
thorax; ensure optimal skin contact.
Ensure sync switch is OFF.
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
8/29
Types of defibrillators - monophasic
Older, less commonly used. All shocks delivered at 360J.
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
9/29
Types of defibrillators - biphasic
Widely used in all Hospitals. All shocks delivered at 200J.
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
10/29
Types of defibrillatorsAEDs
Found in public places, non-acute Hospitals(e.g. Greenwich
Hospital)
Shocks delivered automatically and audible
instructions provided know where the
manual over-ride button is.
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
11/29
ALS Step 2 Assess the rhythm strip
Shockable rhythms ventricular fibrillation (VF)
ventricular tachycardia (VT)
Non-shockable rhythms
sinus rhythm with insufficient output (PEA)
Asystole
Bradycardia (
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
12/29
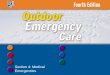
Shockable rhythms VF and VT
VF
VT
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
13/29
ALS Step 3 (shockable) deliver shock
Biphasic immediate 200J shock, thenassess cardiac output, if no
pulse detectable
and no indication of respiratory effort or
consciousness continue CPR (30 comp : 2
breaths) for 2 minutes.
Monophasic immediate 360J shock, then
follow the same procedure.
AED will assess rhythm and shock ifappropriate, follow spoken
instructions.
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
14/29
ALS Step 3 (shockable) subsequently
If there is no output, and after 2 minutes ofCPR
Shock again at 200J (biphasic) / 360J (mono) and
assess cardiac output
If no output, give adrenaline 1mg (or 10mcg/kg)then continue CPR
for a further 2 minutes
On the next cycle, shock/assess then give one
dose of amiodarone 300mg followed by CPR for a
further 2 minutes Continue to shock/assess/CPR giving 1mg of
adrenaline every 2nd cycle
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
15/29
ALS Step 3 (non-shockable)
Asystole give adrenaline 1mg immediately followed by CPR
for 2 minutes
Assess after 2 minutes, shock if VF/VT, otherwise
continue CPR for a further 2 minutes, givingadrenaline 1mg at
every second cycle (i.e. 0, 4, 8,
mins)
Sinus rhythm (with no output) - PEA
Hs (hypoxia, hypo/hyperthermia,
hypo/hyperkalaemia, hypovolemia)
Ts (tamponade, tension pneumothorax, thrombus,
toxins)
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
16/29
ALS Step 3 (non-shockable)
Bradycardia (with inadequate output)
Not common
Initially, 1mg atropine every 3 minutes to total of
3mg
If no improvement, most defibrillators will have a
Pacing button/mode that, when engaged, can
transcutaneously pace while the patient is
awaiting PPM insertion
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
17/29
ALS Step 4 - Post-resuscitation care
Oxygenate to get sats > 95%
Monitor airway patency
Assess for other injuries (spinal, abdominal,
head)
12-lead ECG
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
18/29
Things that are new
In BLS CPR starts if unconscious and breathing
abnormally, checking pulse not recommended
Chest compressions (30) before first 2 breaths are
given Compressions pause only for breaths/assessment
Compressions still effective even if first aid
provider can not / does not want to give rescue
breaths
AEDs should be used even if staff not trained in
their use
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
19/29
Things that are new
In ALS Chest compressions continue during defibrillator
charging
All shocks at 200J (biphasic) or 360J (mono)
Atropine is no longer recommended for asystole orPEA
routinely
Intubation not prioritised over cardiac status
No precordial thump unless patient develops
VT/VF while monitored
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
20/29
Other things to keep in mind
take your own pulse Try to stay calm, walk the last 10m as you
get to
the arrest
Clearly identify you are in charge and allocate
roles to the others present Send away any non-involved staff,
visitors, family
and other patients
Remember that your tone and demeanour will
inevitably reduce or exacerbate the anxiety of theother people
present
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
21/29
Medical Emergencies in Psychiatry
Neuroleptic Malignant Syndrome (NMS)
Serotonin Syndrome (SS)
Status epilepticus
Acute dystonia
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
22/29
Neuroleptic Malignant Syndrome
Physiology Dopaminergic antagonism resulting in sympathetic
hyperactivity
Possible contribution from elevated NAd and 5HT
levels
Risk factors
Onset of AP, increase in dose, IM route of
administration, cessation of DA agents, high-
potency and typical APs
Pre-existing structural brain lesions
Genetic loading
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
23/29
Neuroleptic Malignant Syndrome
Diagnosis History, deteriorating mental state, hypertonia
and
lead-pipe rigidity, autonomic disregulation
Bloods usually show CK level, WCC and ARF
in severe cases
Treatment
Cease DA-antagonist or re-start DA-agonist,
lorazepam (agitation), correct fluid/electrolyte
imbalances
In HDU, dantrolene (mm relaxant) and
bromocriptine (DA agonist) may be helpful
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
24/29
Serotonin Syndrome
Physiology Excessive 5HT activity on 5HT1A and 5HT2
receptors; increased NAd activity also likely to be
a factor
Risk factors Serotonergic agents (incl SSRIs. Li, synthetic
opioids, MAOIs, amphetamines, St Johns Wort),
genetic predisposition, drugs with multiple
serotonin-increasing actions often responsible
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
25/29
Serotonin Syndrome
Diagnosis History, clonus, hypereflexia, autonomic
disregulation, deterioration in mental state with
pronounced agitation, headache
May mimic encephalitis, meningitis, toxinexposure,
anticholinergic delirium
Treatment
Mild cease agent, diazepam 10mg q1h and
(debatably) stat dose 6mg cyproheptadine
Severe cease agent, consider early ICU
admission for sedation/intubation
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
26/29
Status Epilepticus (SE)
Definition continuous seizure activity (+/- convulsions)
with
no intervening recovery of consciousness or, for
complex partial seizures, continuous EEG seizure
activity Treatment
Convulsive SE treated with airway/circulatory
support, IV lorazepam/diazepam, IV phenytoin
and, if no resolution, intubation and induced-paralysis with
midazolam/propofol
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
27/29
Acute dystonia
Pathpohysiology Likely due to decreased DA in basal
ganglia/motor
cortex with decreased motor inhibition
Risks
Use of any D2- receptor antagonist (although
typical APs much greater problem), Li, SSRIs
Genetic predisposition significant risk factor
Previous problem with other drugs in same class
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
28/29
Acute dystonia
Features Typically affects 3-5% of all patients on APs and
up to 10% on typical APs
Most commonly in muscles of neck (30%), tongue
(17%), jaw, occular movements
Treatment
Stat dose 2mg IVI benztropine, diazepam 10mg;
symptoms usually resolve in 3-5 mins
-
7/31/2019 ALS and Medical Emergencies in Psychiatry
29/29
Final thoughts
Attending an arrest is confronting, no matterhow many times
youve done it before
You really cant make things worse, so doingsomething (even if
youre unsure) will always
be better than doing nothing
If you cant remember anything else, goodCPR with some
ventilation will buy you the
10-15mins it generally takes for help to arrive