Embed Size (px)
Citation preview

APPENDIX 1
LOGISTICS & KEY DATA ON: PATIENT, DIAGNOSIS, THERAPY,
OUTCOME & TOXICITY
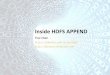
1.0 Logistics
1.1 Baseline-Data & Initial-Response Form
1.2 Follow-up Form
1.3 Variables in ALL IC-BFM 2002 Database
1.3.a Baseline Data
1.3.b Therapy
1.3.c Therapy Realization & Toxicity
1.3.d FU
1.3.e SCT
1.3 Add. Code List Cytogenetics
1.4 SAE Form

Dia
gnos
tics
in A
LL IC
-BFM
200
2Ap
pend
ix 1
.0
Man
dato
ryAt
dia
gnos
isD
ay 8
Day
15
Day
33
Day
52
Day
bef
ore
Prot
. m
M/M
/1.H
R´' b
lock
Mon
th 2
4
Ref
eren
ce c
ente
r:M
orph
olog
y (P
B/B
M/L
P)
Th
erap
y R
espo
nse
&
Rem
issi
on S
tatu
s
6 P
B sm
ears
6
BM
sm
ears
2
cyt
ospi
n sm
ears
6 P
B
6
BM
*
6
PB
6
BM
6 B
M
6 B
M+
6
BM
++
6
BM
*
Imm
unop
heno
typi
ng
(DN
A in
dex,
MR
D)
1 PB
+ 1
BM
sm
ear
2 m
l ED
TA B
M
5
ml E
DTA
PB
2 m
l PB
+BM
* 2
ml B
M2
ml
BM_
2 m
l BM
_
_2
ml B
M_
2 m
l BM
_
Cyt
ogen
etic
s1
PB +
1 B
M s
mea
r 3
ml h
epar
in. B
M
3
ml h
epar
in. P
B
__
__
__
* O
ptio
nal
+ NR
D+3
3 ++
NR
D
+52
Mol
ecul
ar G
enet
ics
+MR
D D
iagn
ostic
s
1 PB
+ 1
BM
sm
ear
2 m
l ED
TA B
M
5
ml E
DTA
PB
_
10 m
l ED
TA B
M if
WBC
< 2
,000
/µL
in P
B

ALL IC-BFM 2002 Appendix 1.1
ALL IC � BFM 2002 Baseline-Data & Initial-Response Form
National Study Coordinator: Address: Tel.: Fax:
Initials (Family name/First name) UPN Center Sex (M/F) Date of Birth dd/mm/yyyy)
/ HISTORY: Pre-existing disease: no yes Previous treatment with corticosteroids or cytostatic agents: no yes Previous treatment timing: within 4 weeks before diagnosis more than 4 weeks before diagnosis not known ALL � treatment started at another department: no yes , in
(place) DIAGNOSIS: Date of diagnosis: (dd/mm/yyyy)
Type of diagnosis: Primary disease Secondary malignancy Relapse BM at diagnosis: central review in local review (to be confirmed by reference lab)
Blasts in BM (%): Comments:
CBC at diagnosis: WBC / µL:
Platelets / µL:
Blasts (%):
Hb (g/dL): . Weight: . kg Height: cm BSA: . m2 Date of 1. prednisone dose: (dd/mm/yyyy) 1/3

ALL IC-BFM 2002 Appendix 1.1 CNS LEUKEMIA (initial): no yes Cerebral mass: no yes Blasts in CSF: no yes Retinal involvement: no yes CSF contaminated with blood: no yes Cells in CSF / µL: Cranial nerve palsy: no yes Blasts in CSF (%): CNS status at diagnosis: 1 2 3 ORGAN INVOLVEMENT (initial): Hepatomegaly: no yes: cm below costal margin Splenomegaly: no yes: cm below costal margin Thymus / Mediastinum: no yes Testicles / Ovaries: no yes Other organ involvement: DIAGNOSTICS: Immunology: no yes, central in Result: yes, local (please add copy) DNA index: no yes, central in DNA index: . yes, local (please add copy) Cytogenetics: no yes, central in Result: yes, local (please add copy) Molecular (cyto)genetics:
BCR/ABL no pos. neg. non-evaluable yes, performed in Result:
TEL/AML1 no yes, performed in Result:
MLL/AF4 no yes, performed in Result: 2/3

ALL IC-BFM 2002 Initial-Response Form Appendix 1.1 DAY 8 � prednisone response: Date: (dd/mm/yyyy)
PB: no (not performed), reason: yes, central review in yes, local review (to be confirmed by reference lab)
WBC / µL: Blast cell count / µL:
Blasts in PB (%):
Pre-phase cumulative dose of prednisone (7 days): mg/m2
BM (optional): no (not performed)
yes, central review in yes, local review (to be confirmed by reference lab)
BM cellularity: Normal Blasts in BM (%): Hypoplastic Comments: Aplastic DAY 15: Date: (dd/mm/yyyy)
PB + BM: no (not performed), reason: yes, central review in yes, local review (to be confirmed by reference lab)
WBC / µL: Blast cell count / µL: BM cellularity: Normal Blasts in BM (%):
Hypoplastic Comments: Aplastic DAY 33: Date: (dd/mm/yyyy)
PB + BM: no (not performed), reason: yes, central review in yes, local review (to be confirmed by reference lab)
Blast cell count / µL: BM cellularity: Normal Blasts in BM (%):
Hypoplastic Comments: Aplastic
CR 1 achieved: yes no If no, date of CR 1: (dd/mm/yyyy)
Comments: Patient alive Patient dead Physician Date (dd/mm/yyyy) Signature Please send copy to National Study Coordinator 3/3

ALL IC-BFM 2002 Appendix 1.2
ALL IC � BFM 2002 Follow-up Form
National Study Coordinator: Address: Tel.: Fax:
Initials (Family name/First name) UPN Center Sex (M/F) Date of Birth (dd/mm/yyyy) / Risk group: SR-1 IR-1 HR-1 SR-2 IR-2 HR-2A
HR-2B RELAPSE: 1. 2. 3. Relapse Date: (dd/mm/yyyy)
Site of relapse: BM CNS Testicles Other:
Remission achieved: no yes Date: (dd/mm/yyyy) SECONDARY MALIGNANCY: Date: (dd/mm/yyyy) Type of secondary malignancy: ALL B-ALL AML NHL HD CNS tumor other tumor Other: LATE TOXICITY: Date: (dd/mm/yyyy) Site/Type: Skeleton Psychologic GIT Heart Sense organ Skin CNS Lungs Osteonecrosis Kidney Endocrine Osteoporosis Liver Hematologic Other: Patient dead: Date of death: (dd/mm/yyyy) Autopsy: no yes
Cause of death: Death in induction Relapse Death in CR Secondary malignancy SCT Other: Follow - up: Date of last follow-up: (dd/mm/yyyy)
Phase of protocol: Comments: Physician Date (dd/mm/yyyy) Signature Please send copy to National Study Coordinator

Appendix 1.3
VARIABLES IN ALL IC-BFM 2002 DATABASE In this database the data of all children diagnosed with ALL and entered into the ALL IC-BFM 2002 trial will be pooled regardless of whether they are observed or protocol patients. Each group will provide the data according to the variable names and codes listed bellow, and the Trial Statistics Center will produce, based on them, the pooled database. The type of file can be SAS, ACCESS or DBF. Appendix 1.3 is composed of 5 parts: Appendix 1.3.a through Appendix 1.3.e: Appendix 1.3.a Baseline Data 1. Baseline Variables VAR. NAME Code UPN UPN Use your own UPN Group GROUP 1-Chile, 2-Argentina, 3-Uruguay,
4-Czech Republic, 5-Hungary, 6-Poland, 7-Israel, 8-Hong Kong, 9-Croatia, 10-Yugoslavia, 11-Turkey, 12-Ukraine, 13-Cuba
Initials INIT First letter Family name, First name Sex SEX 1=male, 2=female Date of birth DOB day/month/year Date of diagnosis DOD day/month/year Eligible for study ELIG no=1(observed pt), yes=2(protocol pt) Reason for ELIG=No CONOELIG 1=conditions for participation in study
not fulfilled (e.g. age of the patient) 2=preexisting disease/ALL is second malignancy 3=significant previous treatment 4=essential data missing (no safe diagnosis a./o. therapy branch stratification possible)
Weight WEIGHT (kg) Height HEIGHT (cm) Body surface BS (m2) Previous treatment with Corticosteroids or cytostatic agents
PRETX 1=no, 2=yes
Previous treatment timing PRETIME 1=within 4 weeks before diagnosis 2=more than 4 weeks before diagnosis 9= not known
WBC at diagnosis (/µL) WBC % blasts (PB) BLA % BM blasts at diagnosis BM Platelets (/µL) PLT Hb (g/dl) HB CNS status CNS 1=CNS status 1 2=CNS status 2
3=CNS status 3 Cells in CSF (/µL) CSF_CELL Blasts in CSF (%) BLA_CSF CSF contaminated with blood 1=no, 2=yes, 9=no data Cerebral mass CM_INV 1=no, 2=yes, 9=no data Cranial nerve palsy CNP_INV 1=no, 2=yes, 9=no data

Splenomegaly SPL_INV 1=no, 2=yes, 9=no data Splenomegaly MEA_SPLE cm below costal margin Hepatomegaly HEP_INV 1=no, 2=yes, 9=no data Hepatomegaly MEA_LIV cm below costal margin Mediastinal mass MED_INV 1=no, 2=yes, 9=no data Testicular involvement GON_INV 1=no, 2=yes, 9=no data Karyotype t(4;11) T411 1=negative, 2=positive, 9=no data Karyotype t(9;22) T922 1=negative, 2=positive, 9=no data Other karyotypes 1 KARYO1 See code list cytogenetics Other karyotypes 2 KARYO2 See code list cytogenetics Hyper-/Hypodiploidy HYPDIP 1= <45 2=>50 BCR/ABL BCR 1=negative, 2=positive, 9=no data MLL/AF4 MLL 1=negative, 2=positive, 9=no data TEL/AML1 TEL 1=negative, 2=positive, 9=no data Immunophenotype IMMPHEN 1=Pro-T
2=Pre-T 3=Intermediate (cortical) T 4=Mature T 5=T-lineage not classified 6= Pro-B 7= Common 8=Pre-B 9=Mature B 10=B-lineage not classified 11=AUL 12=AHL 99=no data
TCR alpha/beta (required only if IMMPHEN = 4 or 5)
TCRA 1=negative, 2=positive 9=no data
TCR gamma/delta (required only if IMMPHEN = 4 or 5)
TCRB
1=negative, 2=positive 9=no data
AHL-Type (required only if IMMPHEN = 12)
AHLT 1=b-lineage, 2=t-lineage
Markers (percent positive cells in blast gate)
CD7 CD7 % CD2 CD2 % CyCD3 CYCD3 % Surface CD3 CD3 % CD19 CD19 % CD10 CD10 % CD33 CD33 % CD66c CD66C % DNA index DNAI WBC/µL on day 8 WBC_8 Blast cell count/µL on day 8 COBLA_8 WBC/µL on day 15 WBC_15 Blast cell count/µL on day 15 COBLA_15 BM day 8, % blasts BLA_8 BM day 15, % blasts BLA_15 BM day 33, % blasts BLA_33

Appendix 1.3.b Therapy 2. Therapy Data VAR. NAME Code Date of start of treatment DOSTR day/month/year Pre-phase cumulative dose of prednisone (mg/m2)
PDN_DOSE
Date of first IT-MTX DOMTX day/month/year Dose of HD-MTX HD_MTX 1=2g/m2, 2=5g/m2 CR1 achieved CR1 1=no, 2=yes Date of first complete remission DOCR1 day/month/year Timing of CR1 CR_PHASE 1=early (day 33), 2=late (>day 33) Date of start of maintenance DOSM day/month/year Date of end of treatment CHTEND day/month/year Radiotherapy RT 1=no, 2=yes Risk group RG 1=SR, 2=IR, 3=HR Date of randomization DORAND day/month/year Treatment assigned R_ASS 1=SR-1, 2=SR-2, 3=IR-1, 4=IR-2,
5=HR-1, 6=HR-2A, 7=HR-2B Treatment administered R_ADM 1=SR-1, 2=SR-2, 3=IR-1, 4=IR-2,
5=HR-1, 6=HR-2A, 7=HR-2B Cause of non-randomization CONORAN 1=clinical decision, 2=parent's refusal
of random, 3=error, 9=not known Cause of shift (if treatment administered differs from assigned)
COSHIFT 1=doctor refuses the arm, 2=parents refuse the arm, 9=not known
Appendix 1.3.c Therapy Realization & Toxicity 3. Therapy-Flow & Toxicity Data VAR. NAME Code UPN UPN use your own UPN Group GROUP 1 � Chile, 2 � Argentina, 3-Uruguay,
4-Czech Republic, 5-Hungary, 6-Poland, 7-Israel, 8-Hong Kong, 9-Croatia, 10-Yugoslavia, 11-Turkey, 12-Ukraine, 13-Cuba
Treatment element
ID_ELE 1=Protocol I, 2= Protocol I', 3=Protocol mM, 4=Protokol M, 5=Protocol II, 6= Protocol III, 7= HR-1', 8=HR-2', 9=HR-3'
Element no ELE_NO Prot- II/III 1=1., 2= 2. 3=3. HR: 1=Block no 1 ...6=Block no 6
Element phase ELE_PH Prot I/II/III 1=phase 1, 2=phase 2 Prot M. 1 = 1.MTX, 2 = 2.MTX, ...
First day of the element ELESTART day/month/year Last day of the element ELEEND day/month/year Body surface (m2) BS Deviations in timing DEV_TIM 1=no, 2=yes Deviations in medication (replacement of drugs)
DEV_MED 1=no, 2=yes
Deviation in dosages DEV_DOS 1=no, 2=yes

Deviation: cause DEV_CAU 1=initial complications, 2=allergic reaction3=other toxicity, 4=relapse/death 4=other
Deviation: Description and cause DEV_NOTE General condition TX_GC NCI Grade 0-4, 9 = no data Infection TX_INF NCI Grade 0-4, 9 = no data Fever TX_FEV NCI Grade 0-4, 9 = no data Nausea TX_NAUS NCI Grade 0-4, 9 = no data Vomiting TX_VOM NCI Grade 0-4, 9 = no data Stomatitis TX_STOM NCI Grade 0-4, 9 = no data Diarrhea TX_DIAR NCI Grade 0-4, 9 = no data S- bilirubin TX_BILI NCI Grade 0-4, 9 = no data S- ALT/ S- AST TX_ALT NCI Grade 0-4, 9 = no data Creatinine TX_CREA NCI Grade 0-4, 9 = no data Proteinuria TX_PROT NCI Grade 0-4, 9 = no data Hematuria TX_HEMA NCI Grade 0-4, 9 = no data Creatinine clearance TX_CRCL NCI Grade 0-4, 9 = no data Arrhythmia TX_ARRH NCI Grade 0-4, 9 = no data Cardiac function TX_CARD NCI Grade 0-4, 9 = no data Echocardio: LV-SF TX_SG NCI Grade 0-4, 9 = no data Central neurotoxicity TX_CNEU NCI Grade 0-4, 9 = no data Peripheral neurotoxicity TX_PNEU NCI Grade 0-4, 9 = no data Osteonecrosis TX_OST NCI Grade 0-4, 9 = no data Other toxicity TX_OTH 1=no, 2=yes Notes/other complications TX_NOTE Other toxicity, description; Notes Appendix 1.3.d FU 4. FU Data VAR. NAME Code Date of first relapse DOREL day/month/year Site of relapse: BM R_BM 1=no, 2=yes Site of relapse: CNS R_CNS 1=no, 2=yes Site of relapse: Testis R_TESTIS 1=no, 2=yes Site of relapse: Other R_OTHER 1=no, 2=yes Date of death DODEAD day/month/year Cause of death CODEAD 1=progressive ALL, 2=SCT-related,
3=2nd tumor, 4=sepsis, 5=pneumonia, 6=other infection, 7=hemorrhage, 8=MOF, 9=other (specify), 99=not known
Phase of death PH_DEAD 1=before start of therapy, 2=in induction before CR, 3=in first CR, 4=after relapse, 5=after 2nd tumor
Date of 2nd malignancy DOSMN day/month/year Type of 2nd malignancy T_SMN Text (C 20) Date of last follow-up DOLFU day/month/year

Appendix 1.3.e SCT 5. SCT Data VAR. NAME Code Eligible for SCT ELBMT 1=no, 2=yes, 9=not known Search for donor DONOR 1=no, 2=yes, 9=not known No of siblings SIBL Histocompatibility HISTO 1=no, 2=yes, 9=not known Date of HLA typing DOHLA day/month/year Date of SCT DOBMT day/month/year Phase of disease at Tx PBMT 1=in CR1, 2=not in CR (e.g. non-
responder) Type of SCT TBMT 1=matched sibling donor
2=matched family donor other than sibling 3=mismatched family donor 4=matched unrelated donor 5=mismatched unrelated donor 6=syngeneic 9=not known
Source of the graft SBMT 1=BM, 2=PBSC, 3=cord blood, 9=not known

Addendum 1.3
CODE LIST CYTOGENETICS
a la J. Harbott (Some codes are relevant only for AML or lymphoma)
-1 no data 0 no result 1 normal 2 t(9;22)(q34;11) 3 11q23 aberrations except t(4;11),t(11;19), t(9;11) 9 der(1q)
10 single-cell aberrations 11 t(1;19)(q23;p13) 12 t(4;11)(q21;q23) 13 t(8;14)(q24;q32), t(2;8), t(8;22) 14 14q11 aberrations 15 del(6q) 16 del(9p) 17 der(12p) 18 >50 19 t(11;19)(q23;p13) 20 t(12;21)(p13;q22) 21 t(8;21)(q22;q22) 22 t(15;17)(q22;q11) 23 inv(16)/t(16;16) 24 t(9;11)(p22;q23) 25 t(6;9)(p23;q34) 26 der(3q) 27 +4 28 +8 29 -5/5q- 31 -X/-Y 32 +12 33 i(17q) 34 t(1;22)(p13;q13) 35 complex >=3 aberrations 36 7p- 37 +21 50 7 (in general) 51 -7 (only) 52 -7 (+ additional) 53 7q- (only) 54 7q- (+ additional) 55 -7 unclear; e.g. +mar 60 1p 61 2p12 62 t(2;5)

63 der(3)(q27) 64 +7 65 der(7)(p22) 66 der(7)(q34~35) 67 8q24 other than code 13 68 del(10q) 69 t(11;14)(q13;q32) / der(11)(q13) 70 t(11;18) 71 Dup(12q) 72 del(13q) 73 del(14q) 74 t(14;18)(q32;q21) 75 der(14q32) 76 der(15q) 77 der(17p) 78 der(17q) 79 +18 80 der(18q) 81 der(22)(q11) except Ph+ 82 +X 83 der(2)(p23) except t(2;5) 84 der(5)(q35) except t(2;5) 85 t(5;14)(q35;q32) 99 random aberration not in this list

Appendix 1.4
ALL IC-BFM 2002 Severe-Adverse-Event Form
Report every unexpected toxic event of grade 3 and 4 except hematologic toxicity, infection and mucositis
Pt Initials: Surname:____________ Name:___________ Date of birth:____________ Event and related measures description: ___________________________________________________________________________ ___________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________ Grade of toxicity according to NCI Common Toxicity Criteria: 4 ڤ 3 ڤ Event: onset: __________ end: __________ or continuation ڤ Cause of event Is the initial status of the patient or other disease responsible for this event? impossible to consider ڤ no ڤ improbably ڤ possibly ڤ probably ڤ yes ڤ Is there any relation between the event and a study medication? impossible to consider ڤ no ڤ improbably ڤ possibly ڤ probably ڤ yes ڤ Course of event no ڤ yes ڤ Death Autopsy performed ڤ Cause of death: ڤ primary disease ڤ complications of treatment ڤ other _____________ life-threatening event ڤ persistent or severe sequels ڤ necessity or prolongation of hospitalization ڤ Send this form by fax to your national study coordinator & national data manager. Fax: Fax: Notes: Date:________________ Signature:________________

APPENDIX 2
PATIENT / PARENT INFORMATION & CONSENT
2.0 Patient & Parent Information
2.1 Informed Consent
2.2 Discussion Protocol on Therapy According to ALL IC-BFM 2002
2.3 Informed Consent with Randomization to Arm SR-1 & SR-2
2.4 Informed Consent with Randomization to Arm IR-1 & IR-2
2.5 Informed Consent with Randomization to Arm HR-1 & HR-2A
2.6 Informed Consent with randomization to Arm HR-1 & HR-2B

Appendix 2.0 PATIENT & PARENT INFORMATION
The treatment and its side effects must be explained to the patient and his/her parents or legal representatives prior to starting it. This study requires to inform on its meaning and the scientific progress achieved in the field of treatment of childhood leukemia. It is also required that the patient (whenever possible) and/or parents/legal guardians be informed on their right to refuse the study, withdraw from it at any time or select themselves the randomization arm during the course of therapy, and that they can do so without giving any cause, and be assured their decision is free, will not negatively affect the attitude of the staff to them, nor it will influence their right to opt for an alternative treatment. The previous study ALL-BFM 95, which, compared with other international studies, achieved a high percentage of first remission without significant increase in toxicity can serve as an alternative. The long-term results as well as the possible late side effects of that study are not yet known, however. The radiation oncologist clarifies radiation therapy and its side effects. With regard to any possible surgical intervention the responsibility to inform lies with the surgeon and the anesthesiologist performing the procedure. According to the World Medical Association (WMA) Declaration of Helsinki, first adopted by the 18th WMA General Assembly (GA) in Helsinki, Finland, June 1964, and amended by 5 subsequent WMA GAs, last by the 52nd WMA GA in Edinburgh, Scotland, October 2000, it is required that younger patients be informed and asked permission to treat, so far as they are able to understand the meaning, purpose and risks of the proposed therapy, and to make their will clear. This requirement holds also for this study. Whether this step is appropriate, must be judged in each individual case. The same approach should be used with adolescent patients between 14 and 18 years of age who are informed on their disease. The treating physician upon discussion with the parent(s)/legal representative(s) will decide as to whether explanation of the study to their adolescent child is appropriate, and if an informed consent should/could be obtained from him/her. Informing a child should be done in a manner corresponding to his/her age and in the presence of the parent(s)/legal guardian(s). If the patient reaches the age of 18 years in the course of the study, his/her consent to continue on it should be obtained. The study recommends the patient (if deemed competent) and legal representative(s) sign the consent, in which the content of the informing discussion is documented. In addition, it is recommended to give them a copy of the whole protocol they have just signed. It is however recognized that these issues will depend on the national conditions, i.e. culture, traditions, legislation, etc. Therefore, informed verbal consent is also acceptable, provided it is clearly and adequately documented and signed by the physician in charge and two witnesses. A copy of the signed written informed consent or a statement regarding a verbally obtained informed consent must be sent to the national data manager. All personal data necessary for central documentation, analysis and reporting of the results will be blinded by the use of numbers. Following an in-depth discussion, the members of the Trial Management Committee (TMC) and Trial Steering Committee (TSC) approved the therapeutic protocol ALL IC-BFM 2002, and expressed their readiness to perform all the tasks required by this study. The Ethics Committees (Institutional Review Boards) of the participating countries/centers examined the ethical and legal issues related to the study and raised no objection against the concept and conduct of the trial or the current form of the protocol.

Appendix 2.1 INFORMED CONSENT
with therapy of acute lymphoblastic leukemia according to ALL IC-BFM 2002 Study
Patient:������������� Date of birth:���������..
(Name) Date of informing discussion:��������� Informing physician:������������..
(Name and appointment) I confirm that the above named physician has informed me today on my/my child's illness and of the proposed therapy. I know that without appropriate therapy this disease cannot be controlled. I am informed on the chances for success with the proposed therapy and on other formerly proven therapies for this disease. Treatment should proceed according to the study ALL IC-BFM 2002, in which more than 10 countries participate. Approximately 1,000 patients are treated according to this study annually, with the total number of patients reaching 4,000 by the end of accrual. The goal of the study is to increase the cure rate by adjusting treatment to the risk of relapse in each patient. The risk of treatment failure, when the disease cannot be controlled with available therapy, as well as the risk of relapse, i.e. recurrence after initial disappearance of the disease (remission) are determined by different biologic properties of the leukemic cells and their response to therapy. In this study, the early treatment response as evaluated in blood on day 8 and in bone marrow on day 15 and ≈33 serves to divide patients into risk groups requiring different therapy. I understand that in this way the intensity of therapy can be adjusted to the individual risk of relapse. The difference from other therapeutic trials and the basis of modern clinical research has been explained to me. The treatment is primarily based on the use of medications that kill leukemic cells, i.e. chemotherapy. A small number of patients should also receive radiation therapy to the brain and/or testicles, which are involved by leukemia, or if the risk of relapse within the central nervous system is considered to be high. Chemotherapy is divided into sequential therapeutic blocks, each using a combination of drugs with different antileukemic properties. Combining a number of different chemotherapeutic agents (cytostatics) should decrease the risk of developing resistance to therapy by leukemic cells. The side effects and risks of therapy were explained to me in detail. These include nausea and vomiting, transient hair loss, damage to mucous membranes, suppressed bone marrow function and blood-forming elements with increased risk of infection or bleeding, and possible delayed side effects such as damage to organs, possible infertility, need for control of childbearing and risk of late-appearing serious illnesses including, among others, second malignant tumors. The reason for radiation therapy in a small number of patients is destruction of leukemic cells in the central nervous system and the testicles. Possible late side effects of this therapeutic modality were explained to me. The radiation therapist will provide more detailed information on radiation therapy to me before starting that treatment. If the initial response to therapy is inadequate, the intensity of therapy must be increased. In a small number of patients with a high risk of relapse, bone marrow transplantation is indicated, so far as a suitable donor is available. If this is a case with me/my child, further information regarding the risks and chances of this procedure and of alternative methods will be provided to me/my child. I will then have the opportunity to decide on that option.

Patients will be assigned to one of three risk groups based on the results of risk assessment, i.e. response to prednisone; response to multi-agent chemotherapy and biologic markers, as these become known during the first one to three months of therapy: SR = standard risk; IR = intermediate risk; HR = high risk. In the SR & IR groups, during the last intensive part of therapy (reinduction), Protocol III will be tested in a random manner in some patients (experimental arm) against Protocol II in others (control arm). In the HR group, Protocol III will be similarly tested either against Protocol II (option HR-2A, as known from the AIEOP LLA-95 trial) or against so-called HR therapy blocks plus Protocol II (option HR-2B, which is essentially the same as in the ALL-BFM 95 study). Protocol III is a shortened version of Protocol II. Allocation of the patients into one or the other arm will be done by randomization, i.e. by chance and anonymous selection, which will be performed by the national study center following my agreement with this manner of patient selection. Randomization is necessary to ensure equal numbers of patients be assigned in each arm for valid scientific analysis. I will be informed about the result of randomization for me/my child. I also have the right to refuse this result and choose myself one of the alternative therapeutic arms or opt for another established treatment. The ALL IC-BFM 2002 study contains two research projects that will assess minimal residual disease (MRD). A small amount of blood (5 ml) and/or bone marrow (2 ml or exceptionally 10 ml) will be obtained for this purpose from me/my child on day 8, day 15 and ≈33 in Protocol I/I', before consolidation and possibly two years following the diagnosis. Evaluation of MRD will be performed in the national reference laboratories, where only samples of blood and/or bone marrow will be submitted. The research results will not be disclosed to the treating center or to the patient/legal representative(s), as the meaning of these results for each individual patient will be evaluated only during the course of the study, and hence cannot have direct implications with regard to the treatment being given to him/her. I know that at the same time bone marrow smears are looked at in the microscope in order to assess the rate at which malignant cells are cleared by counting their percentage, thus providing a precise estimate of the efficiency of the already delivered chemotherapy. The morphologic findings of bone marrow smears worked out day 15, day ≈33 of Protocol I/I', and before consolidation do have direct therapeutic implications and prognostic value for me/my child. On the other hand, I know that although bone marrow smears from day 8, and 2 years following diagnosis (if any) will be also evaluated similarly, the morphologic findings at those time points will have no impact on decision-making with regard to treatment, and these specimens will serve solely for scientific research on MRD. However, I will be free to make the decision as to whether I/my child will participate in these research projects. I/my child will be acknowledged of any important new findings, changes or amendments related to me/my child by the physician in charge who will be notified in a written form by the TMC/TSC of this study or be informed at a meeting of the I-BFM-SG. The treating physician is responsible for informing me/my child on these issues in a way I/my child can understand. I am aware that progress in the management of leukemia is possible only through co-operation of many dedicated pediatric hematology/oncology centers. This requires transmission of patients' data to the national data management center, the Trial Statistics Center (central database) and the national reference and research labs involved in this trial. I understand that I can refuse transmission of any personal data or data related to me/my child without stating the reason and without consequences to my child or me. Publication of the results of this study will employ anonymous data only. Therefore it is not possible to identify any individual patient retrospectively. I understand that treatment will proceed according to ALL IC-BFM 2002 study, which was explained to me/my child. I also understand that I can recall my consent to this study or

certain parts of it at any time and select a different type of therapy of proven efficacy. The recall of my agreement can be done informally. I feel I was adequately informed and have no further questions. _______________________ Place _______________________ ____________________________ Patient Name Signature Date _______________________ ____________________________ Name of legal representative Signature Date _______________________ ____________________________ Name of physician Signature Date _______________________ ____________________________ Name of a witness Signature Date A copy of this Informed Consent and a scheme of the planned therapy should be given to the patient and/or parent(s)/guardian(s). A copy of this Informed Consent is attached to the patient's file at the treating center. Another copy should be sent to the national data manager, but no copy is required by the Trial Statistics Center (central database).

Appendix 2.2
DISCUSSION PROTOCOL ON THERAPY ACCORDING TO ALL IC-BFM 2002
Treatment of Acute Lymphoblastic Leukemia in Children & Adolescents According to ALL IC-BFM 2002 Therapy Plan
(to remain in the patient's file)
_______________________________ _____________________ Patient's name Date of birth Informing discussion was held at________________________________________
Participants: ( ) Legal representative(s)____________________________ ( ) Patient_________________________________________ ( ) Physician_______________________________________ ( ) Witness________________________________________
Information given includes: ( ) Diagnosis ( ) Prognosis without appropriate therapy ( ) Expected prognosis with therapy according to ALL IC-BFM 2002 study ( ) Prognosis with alternative therapy (for example ALL-BFM 95, ALL-BFM 90) ( ) Effects of chemotherapy:
Destruction of leukemic cells with subsequent restoration of normal function of bone marrow, need for intensive combined therapy with multiple cytotoxic drugs, need for repetition of therapeutic blocks in certain risk groups
( ) Side effects of chemotherapy:
Nausea and vomiting, temporary hair loss, transient damage to mucous membranes, tissue necrosis (especially following DOX, DNR, VCR, VDS), temporary impairment or failure of normal production of blood elements, increased susceptibility to infection, organ dysfunction and possible organ damage (liver, pancreas, stomach and bowels, kidneys, urinary tract, heart, lungs, nervous system, etc), possibility of infertility, bone necrosis, risk of second malignancy
( ) Effects of radiation therapy:
Destruction of leukemic cells dwelling in the brain and meninges with subsequent decrease in the risk of relapse in certain subgroups of patients

Destruction of leukemic cells within the testicles that may persist in spite of delivered or ongoing chemotherapy
( ) Side effects of radiation therapy:
Apathy/somnolence syndrome, headache, transient increase in intracranial pressure, possible intellectual deficits and other late side effects
( ) Adjuvant studies:
Research projects on MRD, exchange of data from adjuvant studies
Aims, basis & structure of the study: ( ) Meaning of the study:
Improvement in prognosis for children with acute lymphoblastic leukemia, especially for those with inadequate response to initial therapy
( ) Knowledge based on scientific progress ( ) Randomization in all three risk groups (SR, IR, HR) ( ) Anonymous and confidential storage, sharing and analysis of patient data ( ) Freedom to choose randomization arm or other proven therapy by patient/legal
representative(s)
Points not crossed were not discussed for the following reason: ( ) Refusal by patient ( ) Refusal by legal representative(s) ( ) Risk to patient
Decision: ( ) Participate in study ( ) Not participate in study Date: ____________________________ Informing physician: ________________________________________ Witness: __________________________________________________ Patient/Legal representative(s): ________________________________

Appendix 2.3
INFORMED CONSENT WITH RANDOMIZATION TO ARM SR-1 & SR-2
for patients in the standard-risk group: SR
Patient: ���������������� Date of birth: �������������������... Progress in treatment of malignant diseases of childhood has been made predominantly through so-called randomized clinical trials/studies. Randomized study means that a certain part of therapy or the entire therapy is provided in two different versions (A and B), whereby one half of the patients receive therapy A and the other half therapy B. Which therapy will be assigned to each individual patient is decided by a computer program in the study center on the basis of chance selection (randomization). In order to determine whether therapies A and B are equivalent or whether one of them offers some advantage it is essential to compare a large number of patients, who have similar baseline characteristics and conditions. Patients in the SR group will be randomized to receive either one of two therapeutic approaches that differ as follows: In the SR-1 arm Protocol II will be given only once, while in the SR-2 arm Protocol III will be used twice with a 12-week interval in between. In Protocol III dexamethasone is used for 23 days instead of 30 days in Protocol II. By repeating Protocol III (SR-2) the total dose of dexamethasone will increase by more than 40%. Three drugs (vincristine, doxorubicin and asparaginase) are used from day 1 in Protocol III, and from day 8 in Protocol II. This means it will take 28 days for Protocol III to complete against 49 days for Protocol II. Only two doses each of vincristine and doxorubicin are used in Protocol III. Through repeating Protocol III, patients assigned to SR-2 arm will receive twice the total dose of asparaginase, cytarabine and thioguanine, compared to those allocated to SR-1 arm, but the total dose of vincristine, doxorubicin and cyclophosphamide will remain the same in both arms. Between the first and second Protocol III there is an interval of 12 weeks, during which the patients will receive a 10-week course of daily 6-mercaptopurine and weekly methotrexate, both by mouth. This course of so-called interim maintenance therapy begins 1 week after the first Protocol III and ends up also 1 week before the second one. Maintenance therapy follows the second Protocol III in SR-2 arm and the single Protocol II in SR-1 arm and lasts for both arms until week 104 from diagnosis (start of treatment). With this longer and more intensive therapy in SR-2 arm it is hoped to improve the chances for cure, but an increase in complications is also expected. However, whether this is indeed the case can be definitively determined only on final evaluation of the study. Based on the current state of knowledge a substantial difference in management risks between these two therapeutic alternatives is not expected. According to the general principles valid for the conduct of such studies like ALL IC-BFM 2002, the legal representative(s) and/or the patient must be informed about randomization and their consent obtained. By your signature you confirm you were informed about:
1. Purpose and goal of randomization 2. Therapeutic approach assigned to your child/yourself by randomization 3. Possibility to refuse randomization and select an alternative therapy yourself
( ) Consent for randomization given ( ) Consent for randomization not given Place ________________________________________ Date ________________________________________ Signatures ______________________________ ________________ ________________ Legal representative(s) and/or patient Informing physician Witness (This form should be kept in the patient's file at the treating center. The national data manager should be only notified of the consent, using the form enclosed with a letter from him/her telling the result of randomization, i.e. the arm assigned to the patient)

Appendix 2.4
INFORMED CONSENT WITH RANDOMIZATION TO ARM IR-1 & IR-2
for patients in the intermediate-risk group: IR
Patient: ���������������� Date of birth: �������������������... Progress in treatment of malignant diseases of childhood has been made predominantly through so-called randomized clinical trials/studies. Randomized study means that a certain part of therapy or the entire therapy is provided in two different versions (A and B), whereby one half of the patients receive therapy A and the other half therapy B. Which therapy will be assigned to each individual patient is decided by a computer program in the study center on the basis of chance selection (randomization). In order to determine whether therapies A and B are equivalent or whether one of them offers some advantage it is essential to compare a large number of patients, who have similar baseline characteristics and conditions. Patients in the IR group will be randomized to receive either one of two therapeutic approaches that differ as follows: In the IR-1 arm Protocol II will be given only once, while in the IR-2 arm Protocol III will be used thrice with 6-week intervals in between. In Protocol III dexamethasone is used for 23 days instead of 30 days in Protocol II. By repeating Protocol III (IR-2) the total dose of dexamethasone will increase by about 111%. Three drugs (vincristine, doxorubicin and asparaginase) are used from day 1 in Protocol III, and from day 8 in Protocol II. This means it will take 28 days for Protocol III to complete against 49 days for Protocol II. Only two doses each of vincristine and doxorubicin are used in Protocol III. Through repeating Protocol III, patients assigned to IR-2 arm will receive 3-fold the total dose of asparaginase, cytarabine and thioguanine, and 1.5-fold the total dose of vincristine, doxorubicin and cyclophosphamide, compared to those allocated to IR-1 arm. Between the individual Protocols III there is an interval of 6 weeks, during which the patients will receive a 4-week course of daily 6-mercaptopurine and weekly methotrexate, both by mouth. This course of so-called interim maintenance therapy begins 1 week after the previous Protocol III and ends up also 1 week before the subsequent one. Two courses of interim maintenance therapy will be given to patients in IR-2 arm. Maintenance therapy follows the third Protocol III in IR-2 arm and the single Protocol II in IR-1 arm and lasts for both arms until week 104 from diagnosis (start of treatment). With this longer and more intensive therapy in IR-2 arm it is hoped to improve the chances for cure, but an increase in complications is also expected. However, whether this is indeed the case can be definitively determined only on final evaluation of the study. Based on the current state of knowledge a substantial difference in management risks between these two therapeutic alternatives is not expected. According to the general principles valid for the conduct of such studies like ALL IC-BFM 2002, the legal representative(s) and/or the patient must be informed about randomization and their consent obtained. By your signature you confirm you were informed about:
1. Purpose and goal of randomization 2. Therapeutic approach assigned to your child/yourself by randomization 3. Possibility to refuse randomization and select an alternative therapy yourself
( ) Consent for randomization given ( ) Consent for randomization not given Place ________________________________________ Date ________________________________________ Signatures ______________________________ ________________ ________________ Legal representative(s) and/or patient Informing physician Witness (This form should be kept in the patient's file at the treating center. The national data manager should be only notified of the consent, using the form enclosed with a letter from him/her telling the result of randomization, i.e. the arm assigned to the patient)

Appendix 2.5
INFORMED CONSENT WITH RANDOMIZATION TO ARM HR-1 & HR-2A for patients in the high-risk group: HR
Patient: ���������������� Date of birth: �������������������... Progress in treatment of malignant diseases of childhood has been made predominantly through so-called randomized clinical trials/studies. Randomized study means that a certain part of therapy or the entire therapy is provided in two different versions (A and B), whereby one half of the patients receive therapy A and the other half therapy B. Which therapy will be assigned to each individual patient is decided by a computer program in the study center on the basis of chance selection (randomization). In order to determine whether therapies A and B are equivalent or whether one of them offers some advantage it is essential to compare a large number of patients, who have similar baseline characteristics and conditions. For patients in the HR group, two reinduction approaches of comparable efficacy are available: the AIEOP (Italian) option and the BFM (German) option. Either may serve as the control arm designated HR-2A and HR-2B, respectively. Each national group/center participating in this trial is free to choose one of those options according to its previous experience, i.e. this is not done by randomization. Our national study group/center has opted for HR-2A as the control arm, against which the experimental arm (HR-1) will be tested in a randomized manner. Patients in the HR group will be randomized to receive one of two therapeutic approaches: either triple Protocol III and two 4-week phases of so-called interim maintenance therapy for HR-1, or double Protocol II and a single 4-week phase of interim maintenance therapy for HR-2A. Protocol II & Protocol III are intensive therapy elements, between which 1-week rest periods and courses of less intensive interim maintenance treatment with daily 6-mercaptopurine and weekly methotrexate, both given by mouth, are inserted. The overall duration of reinduction therapy including the rest breaks necessary for recovery of bone marrow function is 24 weeks in arm HR-1 and 20 weeks in arm HR-2A. The same drugs are employed in both arms, however over somewhat different time schedules and/or at variable dosages with regard to the number of doses, the length of treatment and exceptionally the dose size (cyclophosphamide). HR-1 differs from HR-2A in that it contains 25% less vincristine, doxorubicin and cyclophosphamide, but approximately 25 mg/m2 more dexamethasone, 50% more asparaginase, 6-thioguanine and cytarabine, and 100% more 6-mercaptopurine and methotrexate. In addition, depending on whether the central nervous system was/was not involved by leukemia at the beginning, i.e. at the time of initial diagnosis, patients allocated to arm HR-1 will receive 9 or 6 doses of intrathecal methotrexate, whereas those in HR-2A will get 8 or 4 such doses of the drug. However, there is no difference in cranial radiotherapy between the two arms. Two weeks following reinduction therapy, all patients from both arms are put on maintenance therapy that continues until week 104 from diagnosis (start of treatment). With the changes in dosage, schedule and duration of late reintensification (reinduction) therapy introduced in HR-1 arm it is hoped to improve the chances for cure, but an increase in complications is also expected. However, whether this is indeed the case can be definitively determined only on final evaluation of the study. Based on the current state of knowledge a substantial difference in management risks between these two therapeutic alternatives is not expected, as all therapeutic elements used in this study have been employed in previous trials. According to the general principles valid for the conduct of such studies like ALL IC-BFM 2002, the legal representative(s) and/or the patient must be informed about randomization and their consent obtained. By your signature you confirm that you were informed about:
1. Purpose and goal of randomization 2. Therapeutic approach assigned to your child/yourself by randomization 3. Possibility to refuse randomization and select an alternative therapy yourself
( ) Consent for randomization given ( ) Consent for randomization not given Place ________________________________________ Date ________________________________________ Signatures ______________________________ ________________ ________________ Legal representative(s) and/or patient Informing physician Witness (This form should be kept in the patient's file at the treating center. The national data manager should be only notified of the consent, using the form enclosed with a letter from him/her telling the result of randomization, i.e. the arm assigned to the patient)

Appendix 2.6
INFORMED CONSENT WITH RANDOMIZATION TO ARM HR-1 & HR-2B for patients in the high-risk group: HR
Patient: ���������������� Date of birth: �������������������... Progress in treatment of malignant diseases of childhood has been made predominantly through so-called randomized clinical trials/studies. Randomized study means that a certain part of therapy or the entire therapy is provided in two different versions (A and B), whereby one half of the patients receive therapy A and the other half therapy B. Which therapy will be assigned to each individual patient is decided by a computer program in the study center on the basis of chance selection (randomization). In order to determine whether therapies A and B are equivalent or whether one of them offers some advantage it is essential to compare a large number of patients, who have similar baseline characteristics and conditions. For patients in the HR group, two reinduction approaches of comparable efficacy are available: the AIEOP (Italian) option and the BFM (German) option. Either may serve as the control arm designated HR-2A and HR-2B, respectively. Each national group/center participating in this trial is free to choose one of those options according to its previous experience, i.e. this is not done by randomization. Our national study group/center has opted for HR-2B as the control arm, against which the experimental arm (HR-1) will be tested in a randomized manner. Patients allotted to arm HR-1 will receive x3 an intensive therapy element (Protocol III) over 4 weeks each and two 4-week courses of less intensive treatment (so-called interim maintenance therapy) with daily 6-mercaptopurine and weekly methotrexate, both by mouth, during the 6-week intervals between Protocols III. The overall duration of reinduction therapy including the four 1-week rest periods separating Protocols III and phases of interim maintenance treatment is 24 weeks. Patients assigned to the control arm (HR-2B) will sequentially receive 3 short, but very intensive blocks in the same composition and order as was the case during consolidation, i.e. HR-1', HR-2' & HR-3', with recovery periods of about 2 weeks each interposing those blocks. Following an additional rest break of 3 weeks, these patients will receive once Protocol II over 7 weeks. Interim maintenance treatment is not a part of the reinduction therapy in arm HR-2B. To facilitate rapid recovery of bone marrow function and to maintain the concept of dose intensity, i.e. larger doses of cytostatic drugs delivered per unit of time, a growth factor for granulocytes (G-CSF) will be given during the rest period following each HR block. The overall duration of reinduction therapy in HR-2B including the rest pauses is 17 weeks. Furthermore, there are differences between Protocol II and Protocol III. In the former vincristine, doxorubicin and asparaginase are given x4 each beginning by day 8, whereas in the latter vincristine and doxorubicin 2 doses each, and asparaginase in 4 doses are used beginning by day 1. Dexamethasone is administered full-dose for 21 days and 14 days in Protocol II and Protocol III, respectively, then tapered over 9 days in both. Cyclophosphamide is given at 1 g/m2 (Protocol II), but at 0.5 g/m2 (Protocol III). Finally, depending on whether the central nervous system was/was not involved at the time of initial diagnosis, patients randomized to arm HR-1 will receive 3 or 2 doses of intrathecal methotrexate per each Protocol III, i.e. a total of 9 or 6 injections. On the other hand, those patient randomized to arm HR-2B will go to get 4 or 3 triple-drug doses of intrathecal methotrexate, cytarabine and prednisone during the HR blocks, and 4 or 2 doses of intrathecal methotrexate during Protocol II, i.e. a total of 8 or 5 injections. However, with regard to cranial radiotherapy, the only difference lies in timing: while it is delivered after the first intensive therapy element (first Protocol III) in arm HR-1, it follows the last one (single Protocol II) in arm HR-2B. Two weeks after the end of all intensive chemotherapy, patients of either arm are started on maintenance therapy, which is continued until week 104 from diagnosis (start of treatment). With this prolonged intensive therapy in HR-1 arm it is hoped to improve the chances for cure, but an increase in complications is also expected. However, whether this is indeed the case can be definitively determined only on final evaluation of the study. Based on the current state of knowledge a substantial difference in management risks between these two therapeutic alternatives is not expected, as all the therapeutic elements used in this study have been already employed in previous trials. According to the general principles valid for the conduct of such studies like ALL IC-BFM 2002, the legal representative(s) and/or the patient must be informed about randomization and their consent obtained. By your signature you confirm that you were informed about:
1. Purpose and goal of randomization 2. Therapeutic approach assigned to your child/yourself by randomization 3. Possibility to refuse randomization and select an alternative therapy yourself

( ) Consent for randomization given ( ) Consent for randomization not given Place ________________________________________ Date ________________________________________ Signatures ______________________________ ________________ ________________ Legal representative(s) and/or patient Informing physician Witness (This form should be kept in the patient's file at the treating center. The national data manager should be only notified of the consent, using the form enclosed with a letter from him/her telling the result of randomization, i.e. the arm assigned to the patient)

APPENDIX 3 3.0 Therapy Flow Sheets 3.0.a Global Therapy Scheme 3.0.b 1 Protocol I 3.0.b 1/1 Protocol I � Infusion Plan / Phase 1 3.0.b 2 Protocol I' 3.0.b 2/1 Protocol I' � Infusion Plan / Phase 1 3.0.b 1/2+2/2 Protocol I/I' � Infusion Plan / Phase 2 3.0.c 1 Protocol mM 3.0.c 1.1 Protocol mM � Infusion Plan 3.0.c 2 Protocol M 3.0.c 2.1 Protocol M � Infusion Plan 3.0.d Protocol II 3.0.d 1 Protocol II � Infusion Plan / Phase 1 3.0.d 2 Protocol II � Infusion Plan / Phase 2 3.0.e Protocol III 3.0.e 1 Protocol III � Infusion Plan / Phase 1 3.0.e 2 Protocol III � Infusion Plan / Phase 2 3.0.f Block HR-1' 3.0.f 1 Block HR-1' � Infusion Plan 3.0.g Block HR-2' 3.0.g 1 Block HR-2' � Infusion Plan 3.0.h Block HR-3' 3.0.h 1 Block HR-3' � Infusion Plan 3.0.i Maintenance Therapy
3.1 Leucovorin-Rescue Plan
3.2 Therapy � Toxicity Documentation 3.2.a Acute-Toxicity Form 3.2.b Acute-Toxicity Instructions
3.3 Late-Effects Follow-Up Form

APPENDIX 3.0
THERAPY FLOW SHEETS

0
mM
$
1012
R
H R
1'
H R
2'
H
R
3'
BM s
ampl
ing
12G
y*
* C
NS
statu
s 1/2
: pC
RT =
12
Gy
q 1.
5 G
y pe
r fra
ctio
n
CN
S sta
tus 3
: tC
RT: 1
2/18
Gy
q 1.
5 pe
r fra
ctio
n �
dosa
ge b
y ag
e at
trea
tmen
t del
iver
y
Infa
nts <
1 y
r of a
ge: n
eith
er p
CRT
nor
tCRT
See
text
for d
efin
ition
of C
NS
stat
us, i
ndic
atio
ns, t
imin
g &
tech
niqu
e of
CRT
# S
elec
ted
indi
catio
ns fo
r allo
gene
ic S
CT in
all
strat
a of
HR
(See
text
) § N
o ra
ndom
izat
ion
of A
IEO
P vs
. BFM
but
cho
ice
by g
roup
acc
ordi
ng to
pre
viou
s e
xper
ienc
e w
ith o
ne o
f the
two
high
-risk
stra
tegi
es in
tria
l 95
II
HR
: PR
ED-P
R IR
, M3
d15
t(9;2
2)
t(4;1
1)
NR d
33
BFM
Allo
-SC
T#
III
12 G
y* o
nly
for T
-ALL
III
III
III
III
II
II12
Gy*
IIAI
EOP
I/I'
**
d15
104
W
52
10-w
k in
terim
mai
nten
ance
with
6-
MP
/ MT
X
H
R
1'
H
R
2'
H R 3'
R
6-M
P/M
TX4
wks
6-
MP/
MTX
4 w
ks
d33
SR IR
R
IT M
TX in
mai
nten
ance
ther
apy
** P
rot.
I' (D
NR
30m
g/m
2x2
onl
y fo
r SR
pat
ient
s with
BC
P-A
LL
)
dx
§ §
AL
L IC
-BFM
200
2
w12
II
$ BC
P-A
LL
: MT
X 2
g/m
2 /24h
x4;
T-A
LL
: MT
X 5
g/m
2 /24h
x4
12 G
y* o
nly
for T
-ALL
12
Gy*
6-M
P/M
TX4
wks
A
LL IC
-BFM
200
2
App
endi
x 3.
0.a
6-M
P/M
TX
6-M
P/M
TX
6-M
P/M
TX
6-
MP/
MTX
6-M
P/M
TX
6-M
P/M
TX

AL
L IC
-BFM
200
2
Ap
pend
ix 3
.0.b
1
BM
AL
L IC
- BFM
200
2:Pr
otoc
ol I
Day
18
1522
2936
4350
PRED
p.o
. 60
mg/
m 2 /d
=
VCR
i.v
. 1.
5 m
g/m
2 /d =
(m
axim
um: 2
.0 m
g/SD
)
CPM
p.
i. (1h
)1,
000
mg/
m 2 /d
=
(+ M
ESN
A: 4
00 m
g/m
2i.v
. x3
at 0
, 4, 8
h )
DN
R p
.i. (
1h)
30
mg/
m 2 /d
=
L-AS
P p
.i. (
1h)
5,00
0 U
/m 2 /d
=
(E.c
oli-
MED
AC/K
YOW
A)
ARA -
C
i.v.
75 m
g/m
2 /d =
6-M
P p.
o. (2
8 d)
60 m
g/m
2 /d =
( (
)*
)*
5764
MTX
I.T.
= D
ose
age -
adap
ted:
<1
1
2
≥3Y
M
T X IT
(mg)
6
8
10
12
* if C
NS
-2 o
r CN
S-3
stat
us, o
r tra
umat
ic L
P:
add
ition
al M
TX IT
on d
18/
27
DO
B:
Nam
e:
Cen
ter:
18
1522
2936
4350
5764
Star
t Pha
se 1
W
eigh
t =
kg
Hei
ght
=
cm
BSA
=
m2
Wei
ght =
kg
Hei
ght
= cm
BSA
=
m2
Star
t Pha
se 2
Fill
in a
dditi
onal
toxi
city
form
s fo
r Pha
se 1
& 2
!
Si
gnat
ure
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
Dat
e of
Sta
rt:
Dat
e of
End
:
Date
mg
mg
U
mg
mg
. m
g
.m
g
. m
g
Dat
e of
Sta
rt:
Dat
e of
End
:
3333
Day
33:
Rem
issi
on?
yes
no ≥
5% b
last
s in
BM
Bla
sts i
n C
SF
Med
iast
inal
tum
or
≥30
% o
f ini
tial s
ize
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
YE
S �
NO
Des
cri p
tion
of m
odifi
catio
n(s)
& re
ason
(s):

ALL IC-BFM 2002 Appendix 3.0.b 1/1 Protocol I/Phase 1
Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Day 1: LP mg Methotrexate IT at age-adjusted dosage (see below) ( _________ ) Day 8: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Daunorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% Diagnostics (obligatory): CBC+Diff+ABC, liver & spleen size. (optional): BMP
Day 12: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9% LP mg Methotrexate IT at age-adjusted dosage (see below) Day 15: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Daunorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h in 50 ml NaCl 0.9% Diagnostics (obligatory): BMP, CBC+Diff+ABC
Day 18: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9% LP ( if CNS � 2 or CNS � 3 status or traumatic LP ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 21: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9%
Day 22: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Daunorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 24: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9%
Day 27: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9% LP ( if CNS � 2 or CNS � 3 status or traumatic LP ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 29: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Daunorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 30: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9%
Day 33: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9% LP mg Methotrexate IT at age-adjusted dosage (see below) Diagnostics (obligatory): BMP, CBC+Diff+ABC
Day 1 � 28: mg Prednisone (60 mg/m2/d) p.o./i.v. (Cave: hyperleukocytosis & risk of ( - ) tumor lysis syndrome � cautious dosage over first few days; see text) mg mg mg p.o. Prednisone � taper: Day 29-31: ( - ): mg mg mg p.o. Day 32-34: ( - ): mg mg mg p.o. Day 35-37: ( - ): mg mg mg p.o.
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________


ALL
IC-B
FM 2
002
Appe
ndix
3.0
.b 2
BM
Day
18
1522
2936
4350
PRED
p.o
. 60
mg/
m 2 /d
=
VCR
i.v
. 1.
5 m
g/m
2 /d =
(m
axim
um: 2
.0 m
g/SD
)
CPM
p.
i. (1h
)1,
000
mg/
m 2 /d
=
(+ M
ESN
A: 4
00 m
g/m
2i.v
. x3
at 0
, 4, 8
h )
DN
R p
.i. (
1h)
30
mg/
m 2 /d
=
L-AS
P p
.i. (
1h)
5,00
0 U
/m 2 /d
=
(E.c
oli-
MED
AC/K
YOW
A)
ARA -
C
i.v.
75 m
g/m
2 /d =
6-M
P p.
o. (2
8 d)
60
mg/
m 2 /d
=
( (
)*
)*
5764
MTX
I .T.
= D
ose
age -
adap
ted:
<1
1
2
≥3Y
M
TX IT
(mg)
6
8
10
12
* if C
NS-
2 or
CN
S-3
stat
us, o
r tra
umat
ic L
P:
add
ition
al M
TX IT
on
day
18/2
7
DO
B:
Nam
e:
Cen
ter:
18
1522
2936
4350
5764
Star
t Pha
se 1
Wei
ght =
kg
Hei
ght
=
cm
BSA
=
m 2
W
eigh
t =
kg
Hei
ght
=
cm
BSA
=
m2
Star
t Pha
se 2
Fill
in a
dditi
onal
toxi
city
form
s fo
r Pha
se 1
& 2
!
Sign
atur
e Se
nd c
opy
on c
ompl
etio
n to
nat
iona
l stu
dy c
oord
inat
or
Dat
e of
Sta
rt:
Dat
e of
End
:
Date
mg
mg
U
mg
mg
. m
g
.m
g
. m
g
Dat
e of
Sta
rt:
Dat
e of
End
:
3333
Day
33:
Rem
issi
on ?
yes
no ≥
5% b
last
s in
BM
Blas
ts in
CSF
Med
iast
inal
tum
o r ≥
30%
of i
nitia
l siz
e
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
YE
S �
NO
Des
cri p
tion
of m
odifi
catio
n(s)
and
reas
on(s
):
AL
L IC
-BFM
200
2 : P
roto
col I
'R
isk
grou
p: S
R B
CP
- AL
L

ALL IC-BFM 2002 Appendix 3.0.b 2/1 Protocol I'/Phase 1
Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Day 1: LP mg Methotrexate IT at age-adjusted dosage (see below) ( _________ ) Day 8: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Daunorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% Diagnostics (obligatory): CBC+Diff+ABC, liver & spleen size. (optional): BMP
Day 12: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 % LP mg Methotrexate IT at age-adjusted dosage (see below) Day 15: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD)
( ) mg Daunorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9 % U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h in 50 ml NaCl 0.9 % Diagnostics (obligatory): BMP, CBC+Diff+ABC
Day 18: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 % LP ( if CNS � 2 or CNS � 3 status or traumatic LP ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 21: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 %
Day 22: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( )
Day 24: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 %
Day 27: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 % LP ( if CNS � 2 or CNS � 3 status or traumatic LP ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 29: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( )
Day 30: U L-Asparaginase (E. coli, native, Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 %
Day 33: L-Asparaginase (Fa. Medac) (5,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9 % LP mg Methotrexate IT at age-adjusted dosage (see below) Diagnostics (obligatory): BMP, CBC+Diff+ABC
Day 1 � 28: mg Prednisone (60 mg/m2/d) p.o./i.v. (Cave: hyperleukocytosis & risk of ( - ) tumor lysis syndrome � cautious dosage over first few days; see text) mg mg mg p.o. Prednisone � taper: Day 29-31: ( - ): mg mg mg p.o. Day 32-34: ( - ): mg mg mg p.o. Day 35-37: ( - ): mg mg mg p.o.
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________

ALL IC-BFM 2002 Appendix 3.0.b 1/2+2/2
Protocol I/I'/Phase 2 Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Lab tests: CBC, electrolytes, creatinine, urea, G, U/S-osmolality, alb, ALT, AST, bilirubin, urinalysis
Day 36: mg Cyclophosphamide (1,000 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% ( ) mg Mesna (400 mg/m2/SD) i.v. at 0, 4 & 8 h
ml i.v. crystalloids (3,000 ml/m2/24h: 5% G / 0.45% NaCl aa + 90 mmol/m2/24h 7.45% KCl) p.i. for 24 h from end of CPM infusion
Fluid balance: I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: ____________ ml/m2/12h ____________ ml/m2/12h Furosemide: ____________ mg i.v. ____________ mg i.v.
Day 38 � 41: mg Cytarabine (75 mg/m2/d) i.v.
( - )
Day 45: ( )LP mg Methotrexate IT at age-adjusted dosage (see below) Day 45 � 48: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Day 52: BMP (in case of NR day 33) ( ) Day 52 � 55: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Day 59: ( )LP mg Methotrexate IT at age-adjusted dosage (see below)
Day 59 � 62: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Lab tests: CBC, electrolytes, creatinine, urea, G, U/S-osmolality, alb, ALT, AST, bilirubin, urinalysis
Day 64: mg Cyclophosphamide (1,000 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% ( ) mg Mesna (400 mg/m2/SD) i.v. at 0, 4 & 8 h
ml i.v. crystalloids (3,000 ml/m2/24h: 5% G / 0.45% NaCl aa + 90 mmol/m2/24h 7.45% KCl) p.i. for 24 h from end of CPM infusion
Fluid balance: I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: ____________ ml/m2/12h ____________ ml/m2/12h Furosemide: ____________ mg i.v. ____________ mg i.v.
Day 36 � 63: mg 6-Mercaptopurine (60 mg/m2/d) p.o.
( - )
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________


ALL
IC-B
FM 2
002
A
ppen
dix
3.0.
c 1
BM
AL
L IC
- BFM
200
2: P
roto
col m
M
R
isk
grou
p:
SR
BC
P�
AL
L
IR B
CP
�A
LL
Day
18
1522
2936
4350
MTX
p.
i. (2
4h)
2
, 000
mg/
m2
=(1
0% in
0.5
h, 9
0% in
23.
5 h)
MTX
I.T
. (1h
afte
r sta
rt of
MTX
inf.)
=
Dos
e ag
e -ad
apte
d:
<1y:
6 m
g;
1y:
8 m
g;
2y:
10
mg;
>
=3y:
12
mg
6- M
P p.
o. (5
6 d)
25
mg/
m 2 /d
=
(in e
veni
ng, o
n em
pty
stom
ach,
w/o
milk
)
56
LCV
- Res
cue
15
mg/
m 2 i
.v. a
t h:
42,
48,
54
Wei
ght =
Hei
ght
=
BSA
=
kg
cm
m2
DO
B:
Nam
e:
Cen
ter:
.m
g/d
mg/
SD
mg
Date
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
Si
gnat
ure
Fill
in a
dditi
onal
toxi
city
form
per
eac
h M
D M
TX !
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
Y
ES �
NO
D
escr
iptio
n of
mod
ifica
tion(
s) &
reas
on(s
):

ALL IC-BFM 2002 Appendix 3.0.c 1.1 Protocol mM
SR BCP-ALL IR BCP-ALL
1. MTX 2. MTX 3.MTX 4. MTX
Name: Weight: kg Height: cm BSA: m2
DOB: d/m/y CLcr: ml/min/m2 Start: ___/___/___ d/m/y
Prior to each MD MTX Lab tests: CBC, electrolytes, G, creatinine, urea, U/S-osmolality, albumin, ALT, AST, ALP, bilirubin, urinalysis
Day 1 pre � MTX hydration:
ml NaHCO3 (2 mmol/kg) + ml aqua pro inj. (2 ml/kg) p.i. (1 h) Thereafter: 500 ml (NaCl 0.45% / G 5% aa) + 40 mmol NaHCO3 + 10 ml KCl 7.45%
Day 1 (1400) mg Methotrexate (2,000 mg/m2/d) p.i. (24 h) urine pH ≥ 7 mg Methotrexate (1/10) loading dose p.i. (30 min)
mg Methotrexate (9/10) p.i. (23.5 h)
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) ml/h + mmol NaHCO3 (180 mmol/m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 1 (1500) LP: mg MTX IT Dosage: <1 1 2 ≥ 3 Age (yr) 6 8 10 12 mg MTX IT
Day 2 + 3 + post - MTX hydration:
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) + mmol NaHCO3 (180 mmol/ m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 2 + 3 + Leucovorin rescue:
mg LCV (15 mg/m2/SD) i.v. at: _______42 h, _______48 h, _______54 h
Day 1 � 3 - mg 6-Mercaptopurine (25 mg/m2/d) p.o. in evening on empty stomach w/o milk
Day 1 � 3 - Monitoring of U-pH (every portion with dipstick) If U-pH < 7 ⇒ 20 mmol NaHCO3 / 20 ml aqua pro inj. p.i. over 30 min _______ ∑ № of extra alkali infusions Fluid balance: If I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: _____ _____ _____ _____ _____ ml/m2/12h Furosemide: _____ _____ _____ _____ _____ mg i.v.
Supportive: Drug Date 1. _____________________ 2. _____________________ 3. _____________________ 4. _____________________
Date:________ Signature: Physician 1_______________ Physician 2 _______________


ALL
IC-B
FM 2
002
App
endi
x 3.
0.c
2
BM
AL
L IC
- BFM
200
2: Pr
otoc
ol M
R
isk
grou
p:
SR
T�
AL
L
IR T
� A
LL
Day
18
1522
2936
4350
MTX
p.
i. (2
4h)
5
, 000
mg/
m2 =
(10%
in 0
.5 h
, 90%
in 2
3.5
h)
MTX
I.T. (
1h a
fter s
tart
of M
TX in
f.) =
Dos
e ag
e -a
dapt
ed:
<1y:
6 m
g;
1y:
8 m
g;
2y:
10
mg;
>
=3y:
12
mg
6-M
Pp.
o. (5
6 d)
25
mg/
m 2 /d
=
(in e
veni
ng, o
n em
pty
stom
ach,
w/o
milk
)
56
LCV
- Res
cue
15
mg/
m 2 i
.v. a
t h:
42,
48,
54
Wei
ght =
Hei
ght
=
BSA
=
kg
cm
m2
DO
B:
Nam
e:
Cen
ter:
.m
g/d
mg/
SD
mg
MTX
(µ m
ol/l)
CF
- Res
cue
(
mg)
24
h
36 h
42
h
48 h
54
h
2.M
TX
M
TX (
µ mol
/l)
C
F - R
escu
e
(
mg)
24
h
36 h
42
h
48 h
54
h
3.M
TX
MTX
(µ m
ol/l)
CF
- Res
cue
(m
g)
24 h
36
h
42 h
48
h
54 h
4.M
TX
MTX
(µ m
ol/l)
CF
- Res
cue
(
mg)
24
h
36 h
42
h
48 h
54
h
1.M
TXDate
Fill
in a
dditi
onal
to
xici
ty fo
rm fo
r eac
h H
D M
TX !
Si
gnat
ure
Ex
tend
ed R
escu
e
Yes
No
until
hou
r
Exte
nded
Res
cue
Ye
s
N
o un
til h
our
Exte
nded
Res
cue
Yes
No
until
hou
r
Exte
nded
Res
cue
Yes
No
until
hou
r
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
Dos
e m
odifi
catio
n?
C
ytos
tatic
age
nts
adde
d or
om
itted
?
YES
� N
O
Des
crip
tion
of m
odifi
catio
n(s)
/reas
on(s
):

ALL IC-BFM 2002 Appendix 3.0.c 2.1 Protocol M
1. MTX 2. MTX 3.MTX 4. MTX
Name: Weight: kg Height: cm BSA: m2
DOB: d/m/y CLcr: ml/min/m2 Start: ___/___/___ d/m/y
Prior to each HD MTX Lab tests: CBC, MTX level, electrolytes, G, creatinine, urea, U/S-osmolality, alb, ALT, AST, ALP, bilirubin, urinalysis, (baseline MTX level in all but first HD MTX) Day 1 pre � MTX hydration:
ml NaHCO3 (2 mmol/kg) + ml aqua pro inj. (2 ml/kg) p.i. (1 h) Thereafter: 500 ml (NaCl 0.45% / G 5% aa) + 40 mmol NaHCO3 + 10 ml KCl 7.45%
Day 1 (1400) mg Methotrexate (5,000 mg/m2/d) p.i. (24 h) urine pH ≥ 7 mg Methotrexate (1/10) loading dose p.i. (30 min)
mg Methotrexate (9/10) p.i. (23.5 h)
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) ml/h + mmol NaHCO3 (180 mmol/m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 1 (1500) LP: mg MTX IT Dosage: <1 1 2 ≥ 3 Age (yr) 6 8 10 12 mg MTX IT
Day 2 + 3 + post - MTX hydration:
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) + mmol NaHCO3 (180 mmol/ m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 2 + 3 + Leucovorin rescue:
mg LCV (15 mg/m2/SD) i.v. at: _______42 h, _______48 h, _______54 h See also text [section 2.2.3.2 (p 58); section 3.10 (p 135)] & Appendix 3.1 [Leucovorin Rescue Plan].
Day 1 � 3 - mg 6-Mercaptopurine (25 mg/m2/d) p.o. in evening on empty stomach w/o milk
Day 1 � 3 - Monitoring of U-pH (every portion with dipstick) If U-pH < 7 ⇒ 20 mmol NaHCO3 / 20 ml aqua pro inj. p.i. over 30 min _______ ∑ № of extra alkali infusions Fluid balance: If I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: _____ _____ _____ _____ _____ ml/m2/12h Furosemide: _____ _____ _____ _____ _____ mg i.v.
Supportive: Drug Date 1. _____________________ 2. _____________________ 3. _____________________ 4. _____________________
Date:________ Signature: Physician 1_______________ Physician 2 _______________


ALL
IC-B
FM 2
002
A
ppen
dix
3.0.
d
Day
18
1522
29
3643
49
BM
CPM
p .i .
(1h)
1,
000
mg/
m 2 /d
=
(+M
ESN
A: 4
00 m
g/m
2i.v
. x3
at 0
, 4, 8
h)
ARA -
C i
.v .
7
5 m
g/m
2 /d =
6-TG
p .o .
(14
d) 6
0 m
g/m
2 /d =
L-AS
P p
.i . (1
h) 1
0,00
0 U
/m 2 /d
=
(E.c
oli-
MED
AC/K
YOW
A)
DEX
A p
.o ./i
.v .
10 m
g/m
2 /d =
VCR
i.v
.
1.5
mg/
m2 /d
=
(max
imu m
: 2.0
mg/
SD)
DO
X p .
i . (1
h)
30 m
g/m
2 /d =
MTX
I .T
. =
Dos
e ag
e-ad
apte
d:
<1
1
2
≥ 3
Y
M
T X I T
(mg)
6
8
10
12
* If C
NS-
posi
tive:
add
ition
al M
TX IT
on
day
1 &
18
Star
t Pha
se 1
W
eigh
t =
kg
Hei
ght
= cm
BSA
=
m2
mg
. m
g
. m
g
U
W
eigh
t =
kg
Hei
ght
= cm
BSA
=
m2
Star
t Pha
se 2
mg
mg
mg
. m
g
Date
Start of 6- MP/MTX:
DO
B:
Nam
e:
Cen
ter:
Cra
nial
radi
othe
rapy
:
No
Yes
, fro
m
till
Tota
l dos
e:
.
G
y
Frac
tions
(n):
18
1522
29
3643
49
()*
)*
(
AL
L IC
- BFM
200
2 : P
roto
col I
I T
hera
py a
rm:
SR
-1
I
R-1
H
R- 2
A
H
R- 2
BH
R- 2
A
1
.
2
.
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
Si
gnat
ure
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
YE
S �
NO
Des
crip
tion
of m
odifi
catio
n(s)
and
reas
on(s
):
Fill
in a
dditi
onal
toxi
city
form
s for
Pha
se 1
& 2
!

ALL IC-BFM 2002 Appendix 3.0.d 1 Protocol II/Phase 1
SR-1 IR-1 HR-2A 1. 2. HR-2B
Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Day 1: ( ) Diagnostics: BMP (optional)
LP ( if CNS � 3 status ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 8: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Doxorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 11: U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9%
Day 15: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Doxorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 18: U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9% LP ( if CNS � 3 status ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 22: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Doxorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 29: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Doxorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 1 � 21: mg Dexamethasone (10 mg/m2/d) p.o./i.v. ( - ) mg mg mg p.o./i.v. Dexamethasone � taper: Day 22-24: ( - ): mg mg mg p.o./i.v. Day 25-27: ( - ): mg mg mg p.o./i.v. Day 28-30: ( - ): mg mg mg p.o./i.v.
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Cave: Allergic reactions to L-ASP are frequent at this stage of treatment. See text for
alternative therapy.
Supportive therapy: See text for SDD, PCP prophylaxis, prevention/therapy of ulcer disease, etc.
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________

ALL IC-BFM 2002 Appendix 3.0.d 2 Protocol II/Phase 2
SR-1 IR-1 HR-2A 1. 2. HR-2B
Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Lab tests: CBC, electrolytes, creatinine, urea, G, U/S-osmolality, alb, ALT, AST, bilirubin, urinalysis
Day 36: mg Cyclophosphamide (1,000 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% ( ) mg Mesna (400 mg/m2/SD) i.v. at 0, 4 & 8 h
ml i.v. crystalloids (3,000 ml/m2/24h: 5% G / 0.45% NaCl aa + 90 mmol/m2/24h 7.45% KCl) p.i. for 24 h from end of CPM infusion
Fluid balance: I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: ____________ ml/m2/12h ____________ ml/m2/12h Furosemide: ____________ mg i.v. ____________ mg i.v.
Day 38: ( )LP mg Methotrexate IT at age-adjusted dosage (see below)
Day 38 � 41: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Day 45: ( )LP mg Methotrexate IT at age-adjusted dosage (see below)
Day 45 � 48: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Day 36 � 49: mg 6-Thioguanine (60 mg/m2/d) p.o.
( - )
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Supportive therapy: See text for SDD, PCP prophylaxis, prevention/therapy of ulcer disease, etc.
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________

ALL
IC-B
FM 2
002
Ap
pend
ix 3
.0.e
CPM
p .i.
(1h)
5
00 m
g/m
2 /d =
(+
MES
NA:
200
mg/
m2i.v
. x3
at 0
, 4, 8
h)
ARA -
C i.v
.
75
mg/
m2 /d
=
6-TG
p .o .
(14
d) 6
0 m
g/m
2 /d =
L-AS
P p
.i. (1
h) 1
0,00
0 U
/m 2 /d
=
(E.c
oli-
MED
AC/K
YOW
A)
DEX
A p
.o ./i
.v .
10 m
g/m
2 /d =
VCR
i .v.
1.5
mg/
m2 /d =
(m
axim
um: 2
.0 m
g/SD
)
DO
X p .
i . (1
h)
30
mg/
m2 /d
=
BM
Day
18
1522
29
()*
MTX
I.T
.
=
D
ose
age
-ada
pted
: <1
1
2
≥ 3
Y
M
T XIT
(mg)
6
8
1
0
1
2 * I
f CN
S po
sitiv
e: a
dditi
onal
MTX
IT o
n da
y 1
AL
L IC
-BFM
200
2:Pr
otoc
ol II
I
The
rapy
arm
SR
-2
IR-2
HR
-1SR
-2
1.
2
.
IR- 2
/HR
-1
1.
2.
3.
Star
t Pha
se 1
W
eigh
t =
kgH
eigh
t =
cm
BSA
=
m2
mg
. m
g
. m
g U
18
1522
29
W
eigh
t =
kgH
eigh
t =
cm
BSA
=
m2
Star
t Pha
se 2
mg
mg
mg
. m
g
Date
Start of 6- MP/MTX:
DO
B:
Nam
e:
Cen
ter:
Cra
nial
radi
othe
rapy
:
No
Yes
, fro
m
till
Tota
l dos
e:
.
G
y
Frac
tions
(n):
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
Si
gnat
ure
Fi
ll in
add
ition
al to
xici
ty fo
rms f
or P
hase
1 &
2 !
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
YE
S �
NO
Des
cri p
tion
of m
odifi
catio
n(s)
& re
ason
(s):

ALL IC-BFM 2002 Appendix 3.0.e 1 Protocol III/Phase 1
SR-2 1. 2. IR-2/HR-1 1. 2. 3.
Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Day 1: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Doxorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h in 50 ml NaCl 0.9% Diagnostics: BMP (optional)
LP ( if CNS � 3 status ) mg Methotrexate IT at age-adjusted dosage (see below)
Day 4: U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9%
Day 8: mg Vincristine (1.5 mg/m2/d) i.v. (max. 2.0 mg/SD) ( ) mg Doxorubicin (30 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h in 50 ml NaCl 0.9%
Day 11: U L-Asparaginase (E. coli, native, Fa. Medac) (10,000 U/m2/d) p.i. over 1h ( ) in 50 ml NaCl 0.9%
Day 1 � 14: mg Dexamethasone (10 mg/m2/d) p.o./i.v. ( - ) mg mg mg p.o./i.v. Dexamethasone � taper: Day 15-17: ( - ): mg mg mg p.o./i.v Day 18-20: ( - ): mg mg mg p.o./i.v. Day 21-23: ( - ): mg mg mg p.o./i.v.
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Cave: Allergic reactions to L-ASP are frequent at this stage of treatment. See text for
alternative therapy.
Supportive therapy: See text for SDD, PCP prophylaxis, prevention/therapy of ulcer disease, etc.
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________

ALL IC-BFM 2002 Appendix 3.0.e 2 Protocol III/Phase 2
SR-2 1. 2. IR-2/HR-1 1. 2. 3.
Name: Weight: kg Height: cm BSA: m2 DOB: d/m/y Start: ___/___/___ End: ___/___ /___ Lab tests: CBC, electrolytes, creatinine, urea, G, U/S-osmolality, alb, ALT, AST, bilirubin, urinalysis Day 15: mg Cyclophosphamide (500 mg/m2/d) p.i. over 1h in 50 ml NaCl 0.9% ( ) mg Mesna (200 mg/m2/SD) i.v. at 0, 4 and 8 h
ml i.v. crystalloids (1,500 ml/m2/12h: 5% G / 0.45% NaCl aa + 45 mmol/m2/12h 7.45% KCl) p.i. for 12 h from end of CPM infusion
Fluid balance: I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: ____________ ml/m2/12h Furosemide: ____________ mg i.v.
Day 17: ( )LP mg Methotrexate IT at age-adjusted dosage (see below)
Day 17 � 20: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Day 24: ( )LP mg Methotrexate IT at age-adjusted dosage (see below)
Day 24 � 27: mg Cytarabine (75 mg/m2/d) i.v. ( - )
Day 15 � 28: mg 6-Thioguanine (60 mg/m2/d) p.o.
( - )
Dosage of Methotrexate IT: <1 1 2 ≥3 Age (yr) 6 8 10 12 mg Methotrexate IT
Supportive therapy: See text for SDD, PCP prophylaxis, prevention/therapy of ulcer disease, etc.
Date:_____________ Signature: Physician 1___________________Physician 2 ___________________

ALL
IC-B
FM 2
002
Appe
ndix
3.0
.f
AL
L IC
- BFM
200
2 :B
lock
HR
-1�
1.
2
.
HR
- 1' b
lock
T
hera
py a
rm:
H
R -
1
H
R -
2A
HR
- 2
B
DEX
A p
.o./i
.v.
20 m
g/m
2 /d
=
VCR
i.v
. 1
.5m
g/m
2 /d
=(m
axim
um:2
.0 m
g/SD
)
HD A
RA
- C p
.i. (3
h)2,
000
mg/
m2
x2 =
HD M
TX p
.i.(2
4h)
5,00
0 m
g/m
2
=
MTX
/AR
A- C
/PR
EDI.T
. =
/
/
m
g
d
ose
by a
ge 12
30
1
0 m
g=>
3 Y
10
26
8
mg
=>
2 <
3 Y
1h a
fter s
tart
HD
-MTX
8
20
6 m
g
=
> 1
< 2
Y
6
16
4 m
g
< 1
Y
L-AS
Pp.
i.(2
h)
25,
000
U/m
2 /d=
(E.c
oli- M
EDAC
/KYO
WA)
CF-
Res
cue
i.v.
15m
g/m
2
= x3
(h: 4
2,48
,54)
CPM
p.
i. (1
h) 2
00 m
g/m 2
x5 (q
12h
) =(+
MES
NA
70 m
g/m
2 i.v.
x3
at 0
, 4, 8
h)
Day
1
2
3
4
5
6
11
BM
Wei
ght =
Hei
ght
=
BSA
=
kg
cm
m2
DO
B:
Nam
e:
.
.
U
mg/
SD
mg/
SD
mg/
SD
mg/
SD m
g
mg/
d
Dat
e
Da
ta b
efor
e st
art o
f blo
ck:
Patie
nt in
rem
issi
on ?
Y
es
No
M
TX (
µ mol
/l)
CF -
Res
cue
24
h
36 h
42
h
48 h
54
h
Cen
ter:
(mg)
Yes
No
until
hou
r
Exte
nded
Resc
ueFi
ll in
add
ition
al
to
xici
ty fo
rm !
Si
gnat
ure
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
Y
ES �
NO
D
escr
iptio
n of
mod
ifica
tion(
s) &
reas
on(s
):
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
(
q 12
h)

ALL IC-BFM 2002 Appendix 3.0.f 1 BLOCK HR � 1' Name: Weight: kg Height: cm BSA: m2
DOB: d/m/y CLcr: ml/min/m2 Start: / / d/m/y Lab tests prior to start: CBC, electrolytes, creatinine, urea, U/S-osmolality, G, alb, ALT, AST, ALP, bilirubin, urinalysis; in addition TC O2
Lab tests on day 2 + 3: electrolytes, creatinine, urea, G, ALT, AST, ALP, bilirubin
Day 1 � 5 - mg Dexamethasone p.o./i.v. (20 mg/m2/d): mg, mg, mg
Day 1 pre � MTX hydration:
ml NaHCO3 (2 mmol/kg) + ml aqua pro inj. (2 ml/kg) p.i. (1 h) Thereafter: 500 ml (NaCl 0.45% / G 5% aa) + 40 mmol NaHCO3 + 10 ml KCl 7.45%
Day 1 + mg Vincristine (1.5 mg/m2/d) slowly i.v. (max. 2.0 mg/SD), at least 1h before MTX Day 1 (1400) mg Methotrexate (5,000 mg/m2/d) p.i. (24 h)
urine pH ≥ 7 mg Methotrexate (1/10) loading dose p.i. (30 min)
mg Methotrexate (9/10) p.i. (23.5 h)
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24) ml/h + mmol NaHCO3 (180 mmol/m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 1 (1500) LP: mg MTX IT, mg ARA-C IT, mg Prednisone IT
Day 1 � 3 - Monitoring of U-pH (every portion with dipstick) If U-pH < 7 ⇒ 20 mmol NaHCO3 / 20 ml aqua pro inj. p.i. over 30 min _______ ∑ № of extra alkali infusions Day 2 + 3 + post - MTX hydration:
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) + mmol NaHCO3 (180 mmol/ m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 2 + 3 + Leucovorin rescue:
mg LCV (15 mg/m2/SD) i.v. at: _______42 h, _______48 h, _______54 h See also text [section 2.2.3.2 (p 58); section 3.10 (p 135)] & Appendix 3.1 [Leucovorin Rescue Plan]
Day 2 � 4 - mg Cyclophosphamide (200 mg/m2/SD) p.i. (1 h) 5 doses q 12 h: 1. dose on day 2 (2100), 5. dose on day 4 (2100) mg Mesna (70 mg/m2/SD) i.v. at 0, 4 & 8 h from start of each CPM infusion
Day 4 - 6 - INFUSION ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) +
ml KCl 7.45% (90 ml/m2/24h)
Day 5 mg Cytarabine (2,000 mg/m2/SD) in 250 ml G 5%, p.i. (3 h) 900 + 2100 2 doses 12 h apart (900 + 2100); close monitoring; Cave: ataxia, nystagmus Day 5 � 8 - Dexamethasone eye drops: tid; B6: 150 mg/m2 i.v./p.o. q 12h for 2 � 3 days
Day 6 + mg Vincristine (1.5 mg/m2/d) slowly i.v. (max. 2.0 mg/SD), 10 � 12h before L-ASP Day 6 + ___________ U E. coli L-asparaginase (25,000 U/m2/d) in 250 ml NaCl 0.9%, p.i. (2 h) Day 11 ___________ U E. coli L-asparaginase (25,000 U/m2/d) in 250 ml NaCl 0.9%, p.i. (2 h)
Day 11 + µg G-CSF (5 µg/kg/d s.c.) until ANC > 5,000/µL
Fluid balance: q 12h, if I > O + 400 ml/m2 /12h ⇒ mg furosemide i.v. (0.5 mg/kg/SD, max. 20 mg)
Date: Supportive therapy: HT3 blocker & other indispensable medications pro re nata Signature: Physician 1 Physician 2

ALL
IC-B
FM 2
002
A
ppen
dix
3.0.
g
DEX
Ap.
o /i.
v.
.
20m
g/m
2 /d
=
VDS
i.v
.
3
mg/
m2 /d
=
(max
imum
: 5.0
mg/
SD)
DNR
p.i.
(24h
) 3
0 m
g/m
2
=
HD M
TXp.
i. (2
4h)
5,00
0 m
g/m
2 =
IFO
p.i.
(1h)
800
mg/
m2
x 5=
(+ M
ESN
A: 3
00 m
g/m2
i.v. x
3 at
0, 4
, 8h)
L-AS
P p
.i.(2
h)25
, 000
U/m
2 /d =
(E.c
oli- M
EDAC
/KYO
WA )
*
CF-
Res
cue
i.v.
1
5 m
g/m
2
=
x3 (h
: 42,
48,5
4)
* O
nly
in C
NS-
posi
tive
pts
Day
1
2
3
4
5
6
11
BM
W
eigh
t =
Hei
ght
=
BSA
=
kg cm m2
MTX
/AR
A- C
/PR
EDI.T
.=
/
/
mg
dose
by
age
12
30
1
0m
g=>
3 Y
10
2
6
8 m
g
=>
2 <
3 Y
1h
afte
r sta
rt H
DM
TX
8
2
0 6
mg
=
> 1
< 2
Y
6
16
4
mg
< 1
Y
Dat
e
DO
B:
Nam
e:
D
ata
befo
re s
tart
of b
lock
: Pa
tient
in re
mis
sion
?
Y
es
N
o
.
U
mg/
SD
mg/
SD
mg
mg/
d .
mg/
SD
mg/
SD
.
Cen
ter:
AL
LIC
- BFM
200
2 : B
lock
HR
- 2 �
1.
2
.
HR
- 2' b
lock
T
hera
py a
rm:
H
R -
1
H
R- 2
A
H
R -
2B
M
TX (
µ mol
/l)
CF -
Res
cue
24
h
36 h
42
h
48 h
54
h
(mg)
Yes
No
until
hou
r
Exte
nded
Res
cue
Fill
in a
dditi
onal
toxi
city
form
!
Si
gnat
ure
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ato r
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
Y
ES �
NO
D
escr
iptio
n of
mod
ifica
tion(
s) &
reas
on(s
):

ALL IC-BFM 2002 Appendix 3.0.g 1 BLOCK HR � 2'
Name: Weight: kg Height: cm BSA: m2
DOB: d/m/y CLcr: ml/min/m2 Start: / / d/m/y Lab tests prior to start: CBC, MTX level, electrolytes, creatinine, urea, U/S-osmolality, G, alb, ALT, AST, ALP, bilirubin, urinalysis; in addition TC O2
Lab tests on day 2 + 3: electrolytes, creatinine, urea, G, ALT, AST, ALP, bilirubin
Day 1 � 5 - mg Dexamethasone p.o./i.v. (20 mg/m2/d): mg, mg, mg
Day 1 pre � MTX hydration:
ml NaHCO3 (2 mmol/kg) + ml aqua pro inj. (2ml/kg) p.i. (1 h) Thereafter 500 ml (NaCl 0.45% / G 5%) + 40 mmol NaHCO3 + 10 ml KCl 7.45%
Day 1 + mg Vindesine (3 mg/m2/d) slowly i.v. (max. 5.0 mg/SD), at least 1 h before MTX Day 1 (1400) mg Methotrexate (5,000 mg/m2/d) p.i. (24 h) urine pH ≥ 7 mg Methotrexate (1/10) loading dose p.i. (30 min)
mg Methotrexate (9/10) p.i. (23.5 h)
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) ml/h + mmol NaHCO3 (180 mmol/m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 1 (1500) LP: mg MTX IT, mg ARA-C IT, mg Prednisone IT +Day 5: CNS + ditto ditto ditto
Day 1 � 3 - Monitoring of U-pH (every portion with dipstick) If U-pH < 7 ⇒ 20 mmol NaHCO3 / 20 ml aqua pro inj. p.i. over 30 min : _______ ∑ № of extra alkali infusions Fluid balance: q 12h, if I > O + 400 ml/m2 /12h ⇒ mg furosemide i.v. (0.5 mg/kg/SD, max. 20 mg) Day 2 + 3 + post - MTX hydration:
ml G 5% / NaCl 0,45% aa (3,000 ml/m2/24h) + mmol NaHCO3 (180 mmol/ m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 2 + 3 + Leucovorin rescue: mg LCV (15 mg/m2/SD) i.v. at: __ 42 h, __ 48 h, __ 54 h
See also text [section 2.2.3.2 (p 58); section 3.10 (p 135)] & Appendix 3.1 [Leucovorin Rescue Plan]
Day 2 � 4 - mg Ifosfamide (800 mg/m2/SD) p.i. (1 h) 5 doses q 12 h: 1. dose on day 2 (2100), 5. dose on day 4 (2100) mg Mesna (300 mg/m2/SD) i.v. at 0, 4 & 8 h from start of each IFO infusion Day 4 - 6 - INFUSION: ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) + ml KCl 7.45% (90 ml/m2/24h) Day 1 - 6 - Fluid balance: q 12 h
If I > O + 400 ml/m2 /12h ⇒ mg furosemide i.v. (0.5 mg/kg/SD, max. 20 mg)
Day 5 mg Daunorubicin (30 mg/m2/SD) in ml NaCl 0.9%, p.i. (24 h) Day 6 + mg Vindesine (3 mg/m2/d) slowly i.v. (max. 5.0 mg/SD), 10 � 12 h before L-ASP Day 6 + U E. coli L-asparaginase (25,000 U/m2/d) in 250 ml NaCl 0.9%, p.i. (2 h) Day 11 U E. coli L-asparaginase (25,000 U/m2/d) in 250 ml NaCl 0.9%, p.i. (2 h) Day 11 + µg G-CSF (5 µg/kg/d s.c.) until ANC > 5,000/µL
Date: Supportive therapy: HT3 blocker & other indispensable medications pro re nata Signature: Physician 1 Physician 2

A
LL IC
-BFM
200
2
App
endi
x 3.
0.h
DEX
A p.
o./i.
v.
20m
g/m
2 /d =
VP - 1
6 p.
i.(1
h)
100
mg/
m2
x5 =
(q
12
h)
Day
1
2
3
4
5
6
1
1
L-AS
P p
.i.(2
h)
25, 0
00 U
/m2 /d
=
(E.c
oli-
MED
AC/K
YOW
A)
HD
ARA-
Cp.
i. (3
h)2,
000
mg/
m2
x4 =
(q
12
h)
DO
B:
Nam
e:
Cen
ter:
W
eigh
t =
Hei
ght
=
BSA
=
kg
cm m2
MTX
/AR
A-C
/PR
EDI.T
. =
/
/
m
g
dos
e by
age
12
30
1
0m
g =>
3 Y
10
26
8
mg
=
> 2
< 3
Y 8
20
6
mg
=
> 1
< 2
Y 6
16
4 m
g
<
1 Y
Dat
e
D
ata
befo
re s
tart
of b
lock
: Pa
tient
in re
mis
sion
?
Y
es
N
o
U
mg/
SD
mg /
SD
. m
g/d
AL
L IC
- BFM
200
2 : B
lock
HR
- 3 �
1.
2
.
HR
- 3'
blo
ck
The
rapy
arm
:
H
R -
1
H
R -
2A
H
R- 2
B
Fill
in a
dditi
onal
toxi
city
form
!
Si
gnat
ure
Send
cop
y on
com
plet
ion
to n
atio
nal s
tudy
coo
rdin
ator
Dos
e m
odifi
catio
n?
Cyt
osta
tic a
gent
s ad
ded
or o
mitt
ed?
YE
S �
NO
Des
cri p
tion
of m
odifi
catio
n(s)
& re
ason
(s):

ALL IC-BFM 2002 Appendix 3.0.h 1 BLOCK HR � 3'
Name: Weight: kg Height: cm BSA: m2
DOB: d/m/y CLcr: ml/min/m2 Start: / / d/m/y Lab tests prior to start: CBC, electrolytes, creatinine, urea, U/S-osmolality, G, alb, ALT, AST, ALP, bilirubin, urinalysis; in addition TC O2
Lab tests on day 2 + 3: electrolytes, creatinine, urea, G, ALT, AST, ALP, bilirubin
Day 1 � 5 - mg Dexamethasone p.o./i.v. (20 mg/m2/d): mg, mg, mg
Day 1 � 2 - mg Cytarabine (2,000 mg/m2/SD) p.i. (3 h)
• 4 doses 12 h apart • 1,000 mg in 50 ml G 5% • Cave: ataxia, nystagmus • Dexamethasone eye drops: tid Day 1 � 3 - • B6: 150 mg/m2 i.v./p.o. q 12 h Day 1 � 3 -
Day 1 - 6 - INFUSION
ml G 5% / NaCl 0.45% aa (3,000 ml/m2/24h) + ml KCl 7.45% (90 ml/m2/24h)
Day 3 � 5 - mg Etoposide (100 mg/m2/SD) // Etopophos (113 mg/m2/SD) p.i. (1 h)
• in ml NaCl 0.9% (400 ml/m2)
• 5 doses 12 h apart
• 1. dose on day 3 at 2100 h; 5. dose on day 5 at 2100 h
• ECG monitor during & for 5 h after infusion
• Cave: dysrhythmia, hypotension, allergic reactions,
anaphylaxis
• Be prepared with (methyl)prednisolone 5 mg/kg &
clemastine (dosage by age: 0.25 � 2 mg slowly i.v. q 6 � 8
h) or promethazine (dosage by age: 0.25 � 1 mg/kg slowly
i.v. q 8 h) for case of serious allergic event
Day 5 LP: mg MTX IT, mg ARA-C IT, mg Prednisone IT
Day 6 + U E. coli L-asparaginase (25,000 U/m2/d) in 250 ml NaCl 0.9%, p.i. (2 h) Day 11 U E. coli L-asparaginase (25,000 U/m2/d) in 250 ml NaCl 0.9%, p.i. (2 h)
Day 11 + µg G-CSF (5 µg/kg/d s.c.) until ANC > 5,000/µL
Day 1 - 6 - Fluid balance: I > O + 400 ml/m2/12h ⇒ 0.5 mg/kg (max. 20 mg) furosemide i.v.
+ ∆ fluid balance: _____ _____ _____ _____ _____ _____ _____ _____ _____ ml/m2/12h Furosemide: _____ _____ _____ _____ _____ _____ _____ _____ _____ mg i.v.
Date: ________ Supportive: Drug Date Signature: Physician 1_______________ Physician 2 _______________ 1. _______________________
2. _______________________ 3. _______________________ 4. _______________________


A
LL IC
-BFM
200
2
App
endi
x 3.
0.i
MTX
p.o
. 20
mg/
m 2 /w
k
6-M
P p.
o. 5
0 m
g/m
2 /d
(day
: 1 �
70)
Wee
k 1
2 3
4 5
6 7
8 9
10
Dat
e
MTX
mg/
wk
6-M
P m
g/d
WBC
/ µL
Hg
g/
dL
* Blo
od c
hem
istr
y:
PLT
/µL
ALT
U
/LAS
T
U/L
i.v. A
TB
Bili
µm
ol/L
(n d
ays)
AL
P
U/L
R
BC tr
ansf
.(n)
Cre
a µ
mol
/L
PL
T tra
nsf.
(n)
Frac
ture
(? w
k)
Ost
eone
cros
is
(y
es/n
o)
BC
*
Sign
atur
e
AL
L IC
- BFM
200
2 : M
aint
enan
ce T
hera
py
Cyc
le №
:
Nam
e:
D
OB
:
Wei
ght:
k
g H
eigh
t:
cm
BSA
:
m 2
TMP/
SMZ
5/25
mg/
kg p
.o.
3 co
nsec
utiv
e da
ys p
er w
k D
ose:
___
___
/___
___
mg
Day
: ___
__ /_
____
/ __
___

ALL IC-BFM 2002 Appendix 3.1
Leucovorin � Rescue Plan
Principles: • Immediate MTX24 / 42 / 48 level measurement.
Table 1: Regular Plasma MTX Levels & Standard LCV Rescue MTXhour µmol/L Rescue at: [h] Leucovorin i.v. [mg/m2] MTX24 < 150 MTX36 < 3.0 MTX42 ≤ 1.0 42 15
MTX48 ≤ 0.4 48 15
54 15
Management guidelines for non-regular MTX elimination • Forced diuresis up to 4,500 ml/m2/24h. • Strict fluid balance control q 6 h � (q 3 h); Cave: fluid overload (furosemide i.v. as needed). • MTX level q 6 h. • Immediate MTX36 level measurement only if MTX24 > 150 µmol/L or when impaired MTX elimination is clinically
suspected, otherwise together with MTX42.
• Start of LCV rescue: as soon as increased MTX36 /42 level is available (Tab. 2).
Table 2: LCV Rescue in Case of Disproportionately High Plasma MTX Levels • MTX42 1 to < 5.0 µmol/L or • MTX48 > 0.4 µmol/L
• LCV i.v. q 6 h until MTX ≤ 0.25 µmol/L • Dosage: according to Diagram for LCV Dosage by MTX Level (Fig. 1)- vide infra, corresponding to MTX value assessed 6 h earlier
• MTX42 > 5.0 µmol/L See section 2.2.3.2 (p 58) & section 3.10 (p 135)
• LCV i.v. q 6 h until MTX ≤ 5.0 µmol/L • Dosage: LCV [mg] = MTX [µmol/L] x weight [kg], corresponding to MTX value assessed 6 h earlier
• Cave: Because of calcium content, a single LCV dose > 20 mg/kg should be administered via i.v. infusion over 1 h. • Salvage with carboxypeptidase G2 (CPD G2): by availability. See section 2.2.3.2 (p 58) & section 3.10 (p 135). Fig. 1: Diagram for LCV Dosage by MTX Level
MTX [µmol/L] 5
75 mg / m2
4 60 mg / m2
3 45 mg / m2
2 30 mg / m2
1 15 mg / m2
0.25
NO RESCUE
0 24 36 42 48 54 60 66 72 78 84 90 96 Time after start of MTX [h]

APPENDIX 3.2
THERAPY-TOXICITY DOCUMENTATION

ALL IC-BFM 2002 Acute - Toxicity Form Appendix 3.2.a Pt Initials (Surname / Name): ______ DOB: ___/___/___d/m/y UPN: RG: SR IR HR 1 2 2A 2B
Acute Toxicity During / After ALL IC- BFM 2002 Protocol I: Phase 1 Phase 2 Protocol I': Phase 1 Phase 2
Protocol mM: 1.MTX 2.MTX 3.MTX 4.MTX Protocol M: 1.MTX 2.MTX 3.MTX 4.MTX
1. 2. HR-1' Block 1. 2. HR-2' Block 1. 2. HR-3' Block
1. 2. Protocol II: Phase 1 Phase 2 1. 2. 3. Protocol III: Phase 1 Phase 2
Start of therapy block/phase: __ __ . __ __ . __ __ d/m/y End of therapy block/phase: __ __ . __ __ . __ __ d/m/y
Please check off appropriate box for each parameter (maximal toxicity during & after block until start of next phase) Classification According To NCI CTC, Modified By GPOH
Grade 0 1 2 3 4 General condition
normal activity
mild impairment
age-related activities strongly limited
bedridden, in need for nursing
intensive care, very sick
Infection Infection none mild pathogen not identified,
IV antibiotics pathogen identified
IV antibiotics septic shock
Fever (°C) < 38 38 � 39 > 39 � 40 > 40 < 24 h > 40 ≥ 24 h Gastrointestinal toxicity Nausea none adequate food
intake markedly decreased food
intake almost no food
intake TPN necessary
Vomiting (in 24 h) 0 1 2 � 5 6 - 10 > 10/TPN necessary Stomatitis none painless ulceration,
erythema painful ulceration, can still
eat painful ulceration,
cannot eat TPN required due to
stomatitis Diarrhea (stool frequency/day)
none 2 - 3 4 � 6 or night stools or light cramps
7 � 9 or incontinence or strong cramps
? 10 or bloody diarrhea or TPN required
Liver toxicity S- bilirubin normal for age > N � 1.5 x N > 1.5 � 3.0 x N > 3.0 � 10.0 x N > 10.0 x N S- ALT/ S- AST normal for age > N � 2.5 x N > 2.5 � 5.0 x N > 5.0 � 20.0 x N > 20.0 x N Renal toxicity: Creatinine normal for age > N � 1.5 x N > 1.5 � 3.0 x N > 3.0 � 6.0 x N > 6.0 x N Proteinuria (g/L) none < 3.0 3.0 � 10.0 > 10.0 nephrotic syndrome Hematuria none microscopic macroscopic w/o clots macroscopic with clots transfusion required Creatinine clearance (ml/min/1,73m2)
≥ 90 60 - 89 40 � 59 20 - 39 ≤ 19
Cardiac toxicity Arrhythmia none asymptomatic,
no therapy recurrent / persistent,
no therapy therapy required hypotension, ventr.
arrhyth., defibrillation Cardiac function normal for age EF ↓ < 20% from
baseline value EF ↓ ≥ 20% from
baseline value mild cardiac insuff.,
therapeutically compensated
severe / refractory cardiac insufficiency
Echo-CG: LVSF ≥ 30% ≥ 24% - < 30% ≥ 20% - < 24% > 15% - < 20% ≤ 15% Neurologic toxicity Central neurotoxicity none transient lethargy somnolence < 50% of the
day, moderate disorientation
somnolence ≥ 50% of the day,
disorientation, hallucinations
coma, seizures
Peripheral neurotoxicity, Myopathy
none paresthesias and/or decreased tendon
reflexes
severe paresthesias and/or mild weakness
unbearable paresthesias,
marked motor deficits
paralysis
Skeletal toxicity: acute & delayed
Osteonecrosis none asymptomatic and detectable only by
imagining techniques
symptomatic with decreased function, but
no limitations in everyday living
symptomatic and restrictions in everyday
living
symptomatic, crippling
Other toxicity: _______________________________________________________________________________________________ Abbreviations: N normal for age Stamp: EF ejection fraction LVSF left-ventricle shortening fraction Date: _____/_____/_____ d/m/y Signature: _____________ Please send copy to National Study Coordinator & National Data Manager
Notes/other complications: (severe & life-threatening complications as well as extraordinary accidents & toxic deaths must be notified within 24 � 72 h to National Study Coordinator, and reported without delay to him/her and National Data Manager on the SAE Form)

ALL IC BFM-2002 Acute-toxicity Instructions Appendix 3.2.b
Instructions for Filling the Acute-Toxicity Form One Toxicity Form should be filled for each therapeutic part: Phase 1 & 2 of Protocol I/I'/II/III, each MD/HD MTX in Protocol mM/M, every HR block (HR-1', HR-2', HR-3') & its repetition. The part in question must be ticked in the Toxicity Form. The first day of treatment according to a specific part of a protocol is considered as the date of start of that part. Similarly, the end-of-therapy date of a specific part of a protocol is the same as the last day of treatment with that part. However, all toxicities occurring until the start of the next therapy element/part thereof must be added to the debit of the just outgoing one. For example: The first day of therapy according to I/1 is 01.11.2002 = Date of start of I/1 = 01.11.2002. The last day of therapy according to I/1 is 04.12.2002 = Date of end of I/1 = 04.12.2002. The first day of therapy according to I/2 is 07.12.2002 = Date of start of I/2 = 07.12.2002. On the Toxicity Form for I/1 all reportable toxicities seen through 06.12.2002 should be recorded. In each observation period the highest degree of toxicity observed for a given parameter should be recorded (reported). Only results of investigations carried out during the observation period will be reported. Earlier or later observations whatsoever will not be included. The table in Appendix 3.2.a is a shortened version of selected parameters of non-hematologic toxicity derived from the National Cancer Institute Common Toxicity Criteria (NCI CTC) as adopted by SIOP and modified by the German Society of Pediatric Oncology/Hematology (GPOH). For other parameters not listed in the table one can refer to the widely accessible original document. However, not all parameters will be reported. For example, acute hematologic toxicity is routinely recorded in the patient's file, and serves for steering chemotherapy (entry criteria for commencing a therapy element or its part, dosage modification of 6-MP/MTX during interim maintenance and post-intensive long-term maintenance therapy, etc). It may also determine supportive therapy, first of all substitution with blood components, or guide the need for and duration of antimicrobial therapy, and so forth. Acute hematologic toxicity is therefore not liable to notification in this trial, except for drug-induced irreversible SAA. On the other hand, complications consequent on chemotherapy-induced BM failure, e.g. infection or hemorrhage, should be reported. This is done on the Acute-Toxicity Form (Appendix 3.2.a) as appropriate, i.e. either in the body or the footnote of that Form. Other acute non-hematologic adverse events that are serious, life threatening or that interfere with the fluent flow and structure of the basic treatment, e.g. acute pancreatitis, anaphylaxis, ARDS, etc, must be immediately notified to the national study coordinator and properly reported in the footnote of the Acute-Toxicity Form. In addition, if severe (grade 3/4) or fatal they should be also reported on the SAE Form (Appendix 1.4). Secondary leukemia or MDS is a matter of late effects, and should be reported as such on the Follow-up Form (Appendix 1.3.d) & Late-Effects Follow-up Form (Appendix 3.3). It is recognized that the reference values (so-called normal range) may vary between labs for different populations, techniques, equipment and reagents. It is recommended to employ standard lab methods. For the purpose of toxicity grading however, an absolute value falling outside the normal range must be compared with the upper or lower limit of normal as appropriate, i.e. depending on whether the usual pathology of a given parameter is that of increase or decrease, respectively. The result is then expressed as a ratio of the measured absolute value and the ULN or LLN, thus giving a relative value to be used for the assessment of the degree of toxicity.

SELECTED PARAMETERS General Condition See table- Appendix 3.2.a. Infection All infections (bacterial, viral, fungal & protozoan) regardless of the pathogen are included. Fever See table- Appendix 3.2.a. Nausea / Vomiting / Diarrhea See table- Appendix 3.2.a. Stomatitis Stomatitis means any damage to oral mucosa as a result of chemotherapy. Pain in the mouth, ulcerations of and even bleeding from mucous membranes are also included in this category. Bilirubin For the first month of life special guidelines apply. Refer to a textbook of
pediatrics for reference values. For children > 1 month of age and adults: < 17 µmol/L (< 1 mg/dL). N = ULN = Upper Limit of Normal = 17 µmol/L
GOT = AST / GPT = ALT For assessment of the grade of toxicity both parameters should be considered separately. The higher value of GOT or GPT determines the toxicity grade. Table 3: Normal Range of GOT (AST) & GPT (ALT) by Age
Newborn Children & Adults GOT = AST [U/L] 15 � 60 8 � 20 GPT = ALT [U/L] 5 � 25 8 � 20
N = ULN = Upper Limit of Normal Creatinine Table 4: ULN of Plasma Creatinine by Age
[µmol/L] (mg/dL) Newborn < 106 < 1.2 Till end of 5th yr < 44 < 0.5 Till end of 10th yr < 88 < 1.0 > 10 yr < 106 < 1.2
N = ULN = Upper Limit of Normal Proteinuria / Hematuria See table- Appendix 3.2.a. Creatinine clearance (CLcr) This corresponds essentially to glomerular filtration rate (GFR). It can be assessed either by the classic technique of CLcr requiring 24h-urine collection or by radionuclide scans using 51Cr-EDTA/99mTc-DTPA. Alternatively, it is practical to estimate CLcr (GFR) from body height (length) and plasma creatinine according to the formula of Schwartz et al., which was originally proposed for children > 6 months of age (Schwartz GJ et

al. 1976)(84), and later (1984, 1985) developed by the same investigators for full-term newborns and infants, as well as for adolescents: K1 x Height [cm] K2 x Height [cm]
CLcr [ml/min/1.73 m2] = = Plasma Creatinine [mg/dL] Plasma Creatinine [µmol/L]
The constant of proportionality in the numerator is related to creatinine excretion per unit body size, and depends on age, reflecting changes in muscle mass that occur during childhood.
Table 5: Constant of Proportionality by Age (Schwartz Formula)
Age [yr] K1 K2 = 88.18 x K1 Full-term neonates & infants < 1 0.45 39.7 Children 1 � 13 0.55 48.5 M adolescents 14 � 21 0.70 61.7 F adolescents 14 � 21 0.57 50.3
Arrhythmia Grade 1 Isolated remarkable ECG findings not requiring therapy, e.g. extrasystoles Grade 2 Recurrent remarkable ECG findings not requiring therapy, e.g. repetitive
premature systoles Grade 3 Serious arrhythmia necessitating therapy, e.g. atrial fibrillation or flatter Grade 4 Severe arrhythmia involving the ventricles or leading to hypotension Cardiac Function LVEF = Left-Ventricle Ejection Fraction (value derived from echocardiogram) LVSF = Left-Ventricle Shortening Fraction (value derived from echocardiogram) CHF = congestive heart failure Grade 1 EF decreased by < 20% from pre-treatment value Grade 2 EF decreased by > 20% from pre-treatment value Grade 3 Cardiac insufficiency requiring therapy and responding to it Grade 4 Heart failure refractory to treatment Central & Peripheral Neurotoxicity See table- Appendix 3.2.a. Osteonecrosis Grade 1 Incidental finding Grade 2 Remarkable difficulties are apparent, with only slightly limited function, e.g. in
sport, but without restrictions in routine activities of daily living Grade 3 Remarkable problems significantly limiting daily activities Grade 4 Significantly impaired joint or limb function that may require joint
replacement, crutches, wheel chair etc.

ALL IC-BFM 2002 Appendix 3.3
Late-Effects Follow-up Form First Proposal for FU of Patients with ALL
Elaborated in cooperation between leadership of ALL-BFM 2000 trial, LESS,
ELTEC (I-BFM-SG) & Quality-of-Life-&-Late-Effects Project
Pt's Initials (Surname / Name): ____________________
Date___.___.___ After End Of Treatment End of
Treatment (Maintenance)
1. yr 20__
2. yr 20__
3. yr 20__
4. yr 20__
5. yr 20__
- 10. yr -20__
Diagnostics to rule out recurrence Complete physical exam.+ testicles
x monthly q 3 months q 3 months q 4 months q 6 months x
Neurology x monthly q 3 months q 3 months q 4 months q 6 months x CBC + diff. LDH
x monthly q 3 months q 3 months q 4 months q 6 months x
FU & late-effects diagnostics Blood chemistry1 x x Renal function2 x q 4 months q 6 months Viral serology3 x x Ab titers4 x x Endocrinology Percentiles5 x x x x x x x Tanner / breast abnorm. / volume of testicles
x q 6 months q 6 months x x x x
Serum parameters6 in case of remarkable deviations in pubertal development Spermiogram once after 18. yr Ophthalmology x x US � thyroid fT3, fT4, TSH7
x x x
ECG/ (stress)-Echo-CG x q 2 yr BMD x x Neuropsychologic tests (motor, coordination, cognitive domain): from 6. yr of age
x
FU after radiotherapy q 1 yr according to APRO guidelines Second Malignancies
(increased risk for developing brain tumors) the most common second malignancy in ALL: brain tumors 6 � 10 yr after Dx of ALL
1 CRP, ESR, bilirubin, AST, ALT, γ-GT, ALP, LDH, α-amylase, ferritin, immunoglobulins 2 Blood: phosphate, calcium, magnesium, sodium, potassium, creatinine, bicarbonate
Urine: urinalysis, phosphate, calcium, creatinine
3 HBV, HCV, CMV, HIV 4 Diphtheria, tetanus 5 X-ray of left hand/wrist (bone age) 6 LH, FSH, Prolactin, Estradiol, (stimulation tests, if need be) 7 Only after cranial radiotherapy

APPENDIX 4
4.0 IMMUNOPHENOTYPIC CLASSIFICATION OF
ACUTE LEUKEMIAS

ALL IC-BFM 2002 Appendix 4.0
Immunophenotypic Classification of Acute Leukemias
General points, conventions & definitions Surface expression is considered, unless the prefix intra is added. If expression in the membrane or intracellular or both is considered for the definition, the prefix intra is in parentheses. Examples: CD3pos means surface positivity regardless of the intracellular expression; intraIgM means intracellular expression regardless the membrane; (intra)CD79a means expression of CD79a on the membrane, intracellularly or both. The positivity cut-off is 20% of blasts. Cytometry gates are set at the optimal population of cells using optical scatter properties (FSc & SSc).
Acute lymphoblastic leukemia Category Definition Typical findings
proB ALL CD10neg CD20neg c ALL CD10pos intraIgMneg B
precursor preB ALL intraIgMpos CD10pos
B precursor (shared features)
• 2 or 3 of: CD19pos, (intra)CD79apos, CD22pos
• CD3neg, intraCD3neg, κneg and λneg
HLADRpos, intraTdTpos, CD7neg
mature B either κpos or λpos aberrant My Agsneg,
CD20pos, intraTdTneg, may be CD10pos
• Mature B ALL has characteristically L3 morphology. True mature B ALL cases with L1 or L2 are rare but do occur � typical mature B translocations [t(8;14), t(8;22), t(2;8)] are found in these blasts, and genetics should be solicited before the final decision is made.
• Simultaneous positivity of both κ and λ usually indicates improper handling of the specimen, mostly low transport temperature.
• Intracellular κ or λ expression is not considered for classification in ALL IC-BFM 2002. proT ALL CD2neg CD5neg CD8neg preT ALL CD2pos and/or CD5pos and/or CD8pos
intermediate T ALL CD1apos CD4pos & CD8pos,
[Some cases may be CD3pos ]
mature T ALL CD3pos CD1aneg TCRαβpos T ALL TCRαβpos
T lineage
TCRγδpos T ALL TCRγδpos T lineage (shared features)
(intra)CD3pos , CD7pos
Acute biphenotypic (hybrid) leukemia (AHL) Definition: AHL is an acute leukemia with blasts scoring > 2 points (according to the scoring table below) for myeloid lineage and simultaneously >2 points for B or T lineage.

Scoring points
B lineage T lineage My lineage
2 (intra)CD79a, intraIgM, (intra)CD22
(intra)CD3, TCRαβ, TCRγδ intraMPO
1 CD19, CD10, CD20 CD2, CD5, CD8, CD10 CD13, CD33, CD65, CD1170.5 intraTdT, CD24 intraTdT, CD7, CD1a CD14, CD15, CD64
Notes: • EGIL scoring is adopted in its modified version (Bene, Castoldi et al. 1995; Bene, Bernier
et al. 1998). • This scoring system is not intended for the diagnostic distinction between ALL and AML.
In doubtful cases, look at the definitions first and see if the necessary criteria are met; don't compare the absolute score values.
• Frequently, the cells clearly belong to one lineage, based on the pattern of expression of multiple antigens, but the case is assigned to AHL, because the aberrant antigens reach a score of > 2.0. In such cases, the cytometrist should always include the primary lineage of the blasts and the respective reasoning.
• In accordance with the AIEOP LLA-2000/ALL-BFM2000, true AHL cases should be adequately reported and can receive the ALL-focused treatment within ALL IC-BFM 2002 as study-patients.
Acute undifferentiated leukemia (AUL) Definition: Acute leukemia that is unclassifiable using morphology, immunophenotyping and cytochemistry. Note: This is an extremely rare entity. Non-hematologic malignancies must be considered and ruled out.
Acute myeloid leukemia (AML) Definition • At least 2 of the following: intraMPOpos, CD13pos, CD33pos, CD65pos and/or CD117pos • (intra)CD3neg, (intra)CD22neg, (intra)CD79aneg
Diagnostic delineation of ALL vs. Non-Hodgkin Lymphoma Cases with lymphoblasts >=25% in BM qualify for ALL, and should be managed within ALL IC-BFM 2002, except for mature B-ALL, which must be treated as such. Cases with blasts < 25% in BM are considered as NHL, and must be handled as such outside ALL IC-BFM 2002.
I-BFM mini-mini Project Participants and observers are asked to use the set of combinations following the I-BFM mini-mini guidelines http://clip.webpark.cz/minimini.html These combinations, in addition to the goals of I-BFM mini-mini Project, are also helpful in differential diagnostics. You may also use the email conference of the I-BFM mini-mini Project http://clip.webpark.cz/minimini/conference.html to get an insight of other colleagues.

References ALL-BFM 2000: Immunologische Klassifizierung der akuter Leukämien (Anhang 4.0). Bene M C., Bernier M et al.: Blood 92 (2): 596-9; 1998. Bene MC., Castoldi G et al.: Leukemia 9 (10): 1783-6; 1995.
Questions & consulting You can consult individual cases with the national reference lab or you can email your question or comment to the author of these guidelines ([email protected]).

APPENDIX 5
5.0 PARTICIPATING COOPERATIVE / NATIONAL GROUPS


Stat
e
Arg
enti
na
FAX
+54-
11-4
784
4115
!+5
4-11
-478
4 41
15FA
X+5
4-11
-480
6 84
57FA
X+5
4-11
-430
8 53
25FA
X+5
4-11
-495
8 40
93E-
mai
l:m
cric
cher
i@in
tram
ed.n
et.a
r!
!+5
4-11
-430
8 43
00!
+54-
11-4
658
6923
E-m
ail:
webm
aste
r@ga
tla.o
rg.a
rE-
mai
l:jo
rro9
8@ho
tmai
l.com
E-m
ail:
edua
rdo.
diba
r@ho
spita
lital
iano
.org
.ar
FAX
+54-
11-4
308
5325
!+5
4-11
-430
8 43
00 (I
nt 1
301;
1597
;141
7)E-
mai
l:m
felic
e@dd
.com
.ar
Chi
le
FAX
+56-
2-73
5 07
25FA
X+5
6-2-
556
8840
FAX
+56-
2-73
5 07
25FA
X+5
6-2-
225
2031
!+5
6-2-
239
2765
!+5
6-2-
242
1140
!+5
6-2-
239
2765
!+5
6-2-
211
9246
E-m
ail:
fsfe
rrei
@vt
r.net
E-m
ail:
csal
gado
@m
annq
uehu
e.ne
tE-
mai
l:fs
ferr
ei@
vtr.n
etE-
mai
l:m
cabr
era@
mi-m
ail.c
l
Cro
atia
FAX
+385
-1-4
92 0
017
FAX
+385
-51-
623
126
FAX
+385
-1-4
92 0
017
FAX
!+3
85-1
-492
001
7/38
5-99
-424
691
!+3
85-5
1-65
9 11
1!
+385
-1-4
55 2
333
(ext
371
)!
+385
-1-2
38 8
888
E-m
ail:
josip
.kon
ja@
zg.te
l.hr
E-m
ail:
milj
enko
.smok
vina
@ri.
tel.h
rE-
mai
l:ra
nka.
fem
enic
-kes
@zg
.hin
et.h
rE-
mai
l:dr
ago.
batin
ic@
zg.te
l.hr
Arg
entin
a11
81 C
ap.F
ed.-
Buen
os A
ires
Gasc
on 4
50
Uni
vers
idad
de
Chile
, Rob
erto
del
Rio
Hos
pita
l
Sant
iago
Prof
. Dr.
Josip
Kon
ja
Sala
ta 4
Croa
tia
Part
icip
atin
g C
oope
rativ
e / N
atio
nal G
roup
sALL IC-BFM 2002
Nat
iona
l Coo
rdin
ator
s, D
ata
Man
ager
s an
d R
efer
ence
Lab
orat
orie
s
Nat
iona
l Coo
rdin
ator
:V
ice-
Coo
rdin
ator
:D
ata
Man
ager
:N
atio
nal R
efer
ence
Lab
orat
ory
for I
mm
uno p
heno
typi
ng:
Hos
pita
l de
Pedi
atria
Juan
P. G
arra
han
Dr.
Jorg
e G.
Ros
i
Pedi
atric
Hem
atol
ogy-
Onc
olog
y D
iv.
Hos
pita
l Ita
liano
de
Buen
os A
ires
(CP
1428
) Cap
ital F
eder
al-B
ueno
s Aire
sO
´Hig
gins
200
8 Pi
so 5
0
Dr.
Ceci
lia R
icch
eri
12 4
5 Bu
enos
Aire
sIm
mun
olog
y D
epar
tmen
t
Arg
entin
aA
rgen
tina
Arg
entin
a
Dr.
Edua
rdo
A. D
ibar
Dr.
Fran
cisc
o Ja
vier
Las
tiri
(CP
1425
) Cap
. Fed
eral
Pach
eco
de M
elo
3081
Stat
istic
Dep
artm
ent o
f GA
TLA
Prof
. Dr.
Myr
iam
Cam
pbel
lPr
of. D
r. Ca
rmen
Sal
gado
Prof
. Dr.
Myr
iam
Cam
pbel
lD
r. M
aria
Ele
na C
abre
ra
Avd
a La
Esc
uela
930
, Las
Con
des
Dr.
Mar
ia S
ara
Felic
e
Uni
v. d
e Ch
ile, H
ospi
tal E
xequ
iel G
onal
ez C
orte
sU
nive
rsid
ad d
e Ch
ile, R
ober
to d
el R
io H
ospi
tal
Uni
vers
idad
de
Chile
Hos
pita
l del
Sal
vado
r
Hos
pita
l de
Pedi
atria
Juan
P. G
arra
han
Hem
atol
ogy
and
Onc
olog
y D
epar
tmen
t12
45
Buen
os A
ires
Arg
entin
a
Hem
ato-
Onc
olog
y D
ivisi
onH
emat
o-O
ncol
ogy
Div
ision
Hem
ato-
Onc
olog
y D
ivisi
on
Sant
iago
Sant
iago
Gral
Ped
ro D
artn
ell 1
526,
Nun
oaCo
pan
1803
, Vita
cura
Gral
Ped
ro D
artn
ell 1
526,
Nun
oaSa
ntia
goCh
ileCh
ileCh
ileCh
ile
Child
ren´
s Clin
ic S
alat
aCh
ildre
n´s C
linic
Kan
trid
aCh
ildre
n´s C
linic
Sal
ata
Clin
ical
Hos
pita
l Cen
ter R
ebro
HR-
1000
0 Za
greb
HR-
5100
0 Ri
jeka
HR-
1000
0 Za
greb
HR-
1000
0 Za
greb
Croa
tiaCr
oatia
Croa
tia
Appendix 5.0
Ista
rska
43
Sala
ta 4
K
ispat
icev
a 12
Dr.
Milj
enka
Sm
okvi
naD
r. Ra
nka
Fem
enic
Doc
. Dr.
Dra
go B
atin
ic

Stat
e
FAX
+385
-21-
556
590
!+3
85-2
1-55
6 11
1E-
mai
l:sr
djan
a.cu
lic@
st.te
l.hr
Cze
ch R
epub
lic
Inst
itute
of I
mm
unol
ogy
Labo
rato
ry fo
r Flo
w Cy
tom
etry
FAX
+420
-2-2
443
2220
FAX
+420
-38-
787
6302
FAX
+420
-2-2
443
2220
Czec
h Re
publ
ic!
+420
-2-2
443
2201
!+4
20-3
8-78
7 63
76!
+420
-2-2
443
2201
FAX
+420
-2-2
443
2084
E-m
ail:
jan.
star
y@lfm
otol
.cun
i.cz
E-m
ail:
jaba
li@ne
mcb
.cz
E-m
ail:
alen
a.vr
zalo
va@
lfmot
ol.c
uni.c
z!
+420
-2-2
443
5969
E-m
ail:
ondr
ej.h
rusa
k@lfm
otol
.cun
i.cz
Hon
g K
ong
Dr.
Shau
-Yin
HA
Que
en M
ary
Hos
pita
l
FAX
+852
-285
5 48
49!
+852
-285
5 34
53FA
X+8
52-2
649
7859
E-m
ail:
syha
@hk
ucc.
hku.
hkFA
X+8
52-2
649
7859
!+8
52-2
632
1029
!+8
52-2
632
1029
FAX
+852
-260
2 31
85E-
mai
l:ck
li@cu
hk.e
du.h
kE-
mai
l:he
idiw
ong2
001@
yaho
o.co
m.h
k!
+852
-263
2 21
79E-
mai
l:m
arga
retn
g@cu
hk.e
du.h
k
Hun
gary
FAX
+36-
1-45
9 91
54FA
X+3
6-1-
303
6022
FAX
+36-
1-21
7 44
04FA
X+3
6-52
-417
631
!+3
6-1-
459
9108
!+3
6-1-
334
3186
!+3
6-1-
215
1380
!+3
6-52
-431
956
E-m
ail:
tapo
lcai
@sz
taki
.hu
E-m
ail:
beny
o@gy
er1.
sote
.hu
E-m
ail:
jaka
b@gy
er2.
sote
.hu
E-m
ail:
Dr.
Srda
na C
ulic
Child
ren´
s Clin
ic S
plit
Spin
cice
va1
HR-
2100
0 Sp
litCr
oatia
B.Něm
cové
54
Dep
t. of
Ped
iatr
ics
Regi
onal
Hos
pita
lD
r. Y
ahia
Jaba
li
Hei
m P
al C
hild
ren´
s Hos
pita
l
2nd
Dep
t. of
Ped
iatr
ics
Hun
gary
1089
Bud
apes
tÜ
lloi u
. 86
Hem
ato-
Onc
olog
y D
epar
tmen
t
Hon
g K
ong
Hon
g K
ong
Uni
vers
ity H
ospi
tal M
otol
Dr.
Ond
rej H
rusa
k
V úv
alu
8415
0 06
Pra
ha 5
Appendix 5.0N
atio
nal C
oord
inat
or:
Vic
e-C
oord
inat
or:
Dat
a M
anag
er:
Nat
iona
l Ref
eren
ce L
abor
ator
y
fo
r Im
mun
ophe
noty
ping
:
ALL IC-BFM 2002
Dr.
Jan
Star
ýA
lena
Vrz
alov
á, M
ScU
nive
rsity
Hos
pita
l Mot
olU
nive
rsity
Hos
pita
l Mot
ol2n
d D
ept.
of P
edia
tric
sV
úval
u 84
V úv
alu
8415
0 06
Pra
ha 5
150
06 P
raha
5Cz
ech
Repu
blic
Czec
h Re
publ
icCz
ech
Repu
blic
370
87 Č
eské
Buděj
ovic
e
Dr.
Chi-K
ong
LIM
s Hei
di W
ong
Dr.
Mar
gare
t NG
Prin
ce o
f Wal
es H
ospi
tal
Prin
ce o
f Wal
es H
ospi
tal
Prin
ce o
f Wal
es H
ospi
tal
The
Chi
nese
Uni
vers
ity o
f Hon
g K
ong
The
Chi
nese
Uni
vers
ity o
f Hon
g K
ong
The
Chi
nese
Uni
vers
ity o
f Hon
g K
ong
Dep
artm
ent o
f Ped
iatr
ics
Canc
er C
entr
e, R
oom
G17
Dep
artm
ent o
f Ana
tom
ical
and
Cel
lula
r Pat
holo
gyD
epar
tmen
t of P
edia
tric
s
Shat
inSh
atin
Hae
mat
olog
y La
bora
tory
Hon
g K
ong
Hon
g K
ong
Shat
in
Dr.
Edin
a M
agya
rosy
Dr.
Gábo
r Ben
yóD
r. Zs
uzsa
nna
Jaka
bD
r. La
szlo
Mus
zbek
Deb
rece
n M
edic
al U
nive
rsity
4032
Deb
rece
n
1st D
epar
tmen
t of P
edia
tric
sBó
kay
J. u.
53
Sem
mel
weis
Med
ical
Uni
vers
ity
1083
Bud
apes
t
Sem
mel
weis
Med
ical
Uni
vers
ity2n
d D
epar
tmen
t of P
edia
tric
s
1094
Bud
apes
tT
uzol
tó u
. 7-9
Nag
yerd
ei k
rt. 9
8
Hun
gary
Hun
gary
Hun
gary

Stat
e
Isra
el
FAX
+972
-3-9
25 3
042
FAX
+972
-3-9
25 3
042
FAX
+972
-3-9
25 3
042
FAX
!+9
72-3
-925
366
9!
+972
-3-9
25 3
669
!+9
72-3
-925
366
9!
E-m
ail:
dnao
mi@
clal
it.or
g.il
E-m
ail:
dnao
mi@
clal
it.or
g.il
E-m
ail:
dnao
mi@
clal
it.or
g.il
E-m
ail:
e-ro
sent
@sh
eba.
heal
th.g
ov.il
Stat
isti
cs:
FAX
+972
-3-5
30 2
377
!+9
72-3
-530
232
7FA
X+9
72-3
-640
935
7E-
mai
l:siz
rael
i@po
st.ta
u.ac
.il!
+972
-3-6
40 8
035
FAX
+972
-3-9
25 3
042
E-m
ail:
dms@
post
.tau.
ac.il
!+9
72-3
-925
366
9E-
mai
l:dn
aom
i@cl
alit.
org.
il
Pola
nd
FAX
+48-
81-7
47 7
220
FAX
+48-
61-8
47 4
356
FAX
+48-
81-7
47 7
220
FAX
+48-
12-6
58 9
730
!+4
8-81
-718
552
0!
+48-
61-8
47 4
356
!+4
8-81
-718
553
0!
+48-
12-6
58 9
730
E-m
ail:
jkow
alcz
@ds
k.lu
blin
.pl
E-m
ail:
bmt5
641@
sk5.
usom
s.poz
nan.
plE-
mai
l:dk
rasn
@ds
k.lu
blin
.pl
E-m
ail:
mip
ituch
a@cy
f-kr
.edu
.pl
Uru
guay
FAX
+598
-2-7
08 3
095
FAX
+598
-2-7
08 3
095
FAX
+598
-2-4
08 7
588
!+5
98-2
-708
309
5!
+598
-2-7
08 3
095
!+5
98-2
-408
742
7E-
mai
l:lc
ast@
adin
et.c
om.u
yE-
mai
l:nb
rock
@ad
inet
.com
.uy
E-m
ail:
hgio
rdan
o@as
esp.
com
.uy
fpgh
op@
adin
et.c
om.u
yfp
ghop
@ad
inet
.com
.uy
gior
dano
@m
onte
vide
o.co
m.u
y
Nat
iona
l Coo
rdin
ator
:V
ice-
Coo
rdin
ator
:D
ata
Man
ager
:N
atio
nal R
efer
ence
Lab
orat
ory
for I
mm
uno p
heno
typi
ng:
ALL IC-BFM 2002
Dr.
Batia
Sta
rkPr
of. R
ina
Zaiz
ovM
s Din
a K
ugel
Dr.
Eti R
osen
thal
Schn
eide
r Chi
ldre
n´s M
edic
al C
ente
r of I
srae
lSc
hnei
der C
hild
ren´
s Med
ical
Cen
ter o
f Isr
ael
Schn
eide
r Chi
ldre
n´s M
edic
al C
ente
r of I
srae
lSh
eba
Med
ical
Cen
ter
Pedi
atric
Hem
atol
ogy
Onc
olog
yPe
diat
ric H
emat
olog
y O
ncol
ogy
Pedi
atric
Hem
atol
ogy
Onc
olog
yH
emat
olog
ical
Inst
itute
, FA
CS la
bora
tory
Peta
h-T
ikva
492
02Pe
tah-
Tik
va 4
9202
Peta
h-T
ikva
492
02T
el H
asho
mer
526
21Is
rael
Isra
elIs
rael
Isra
el
Dr.
Shai
Izra
eli
Dr.
Dro
rit L
uria
, PhD
Sheb
a M
edic
al C
ente
rPr
of. D
avid
M. S
tein
berg
Schn
eide
r Chi
ldre
n´s M
edic
al C
ente
r of I
srae
lPe
diat
ric H
emat
olog
y O
ncol
ogy
Tel
Avi
v U
nive
rsity
Pedi
atric
Hem
atol
ogy
Onc
olog
yT
el H
asho
mer
526
21D
ept.
of S
tatis
tics a
nd O
RIm
mun
ophe
noty
ping
Lab
orat
ory
Isra
elT
el A
viv
6997
8K
apla
n 14
Isra
elPe
tah-
Tik
va 4
9202
Isra
el
Prof
. Dr.
med
. Jer
zy K
owal
czyk
Dr.
Mal
gorz
ata
Kac
zmar
ek-K
anol
dD
ariu
sz K
rasn
odeb
ski
Dr.
Ann
a Pi
tuch
-Now
orol
ska
Dep
artm
ent o
f Ped
iatr
ic H
emat
olog
y D
epar
tmen
t of P
edia
tric
Hem
atol
ogy
Dep
artm
ent o
f Ped
iatr
ic H
emat
olog
y U
nive
rsity
Chi
ldre
n´s H
ospi
tal
and
Onc
olog
yan
d O
ncol
ogy
and
Onc
olog
yD
epar
tmen
t of C
linic
al Im
mun
olog
yul
. Cho
dzki
2ul
. Szp
italn
a 27
/33
ul. C
hodz
ki 2
ul. W
ielic
ka 2
6520
-093
Lub
lin60
-572
Poz
nan
20-0
93 L
ublin
30-6
63 K
rakó
wPo
land
Pola
ndPo
land
Pola
nd
Dr.
Luis
Cast
illo
Dr.
Nic
ole
Broc
khor
stD
r. H
ugo
Gior
dano
Appendix 5.0
Fund
ació
n Pe
luff
o Gu
igue
sFu
ndac
ión
Pelu
ffo
Guig
ues
Aso
ciac
ion
Espańo
laBu
leva
r Art
igas
155
6 Bu
leva
r Art
igas
155
6 Bu
leva
r Art
igas
146
5CP
: 160
0, M
onte
vide
oCP
: 160
0, M
onte
vide
oM
onte
vide
oU
rugu
ayU
rugu
ayU
rugu
ay

Stat
e
Cub
a
FAX
+53-
7-44
334
FAX
+53-
7-44
334
FAX
+53-
7-44
334
FAX
+53-
7-44
334
!+5
3-7-
578
268
!+5
3-7-
578
268
!+5
3-7-
578
268
!+5
3-7-
578
268
E-m
ail:
agon
zale
z@he
mat
o.sld
.cu
E-m
ail:
esva
rch@
hem
ato.
sld.c
uE-
mai
l:sm
achi
n@he
mat
o.sld
.cu
E-m
ail:
cmac
ias@
hem
ato.
sld.c
uot
ero@
info
med
.sld.
cuev
a_sv
arch
@ho
tmai
lcom
Turk
ey
FAX
+90-
212-
418
8834
FAX
+90-
232-
362
4990
FAX
!+9
0-21
2-53
0 03
31!
+90-
232-
388
1858
!
E-m
ail:
lebr
izy@
turk
.net
E-m
ail:
cetin
gul@
med
.ege
.edu
.trE-
mai
l:
Ukr
aine
FAX
+380
-44-
213
1646
FAX
FAX
+380
-44-
213
1646
FAX
+380
-44-
213
1646
!+3
80-4
4-21
9 49
82!
+380
-652
-27
0477
!+3
80-4
4-21
9 49
82!
+380
-44-
219
4982
E-m
ail:
ped.
onco
l@uk
rnet
.net
E-m
ail:
E-m
ail:
ped.
onco
l@uk
rnet
.net
E-m
ail:
ped.
onco
l@uk
rnet
.net
Yug
osla
via
FAX
+381
-11-
684
672/
629
273
FAX
+381
-11-
697
232
FAX
+381
-11-
684
672
FAX
+381
-11-
697
232
!+3
81-1
1-62
9 27
3!
+381
-11-
310
8245
!+3
81-1
1-68
8 54
1!
+381
-11-
310
8177
E-m
ail:
dr.ja
nic@
eune
t.yu
E-m
ail:
dr.m
icic
@eu
net.y
uE-
mai
l:dr
.jani
c@eu
net.y
uE-
mai
l:bo
naka
2001
@ya
hoo.
com
Dr.
Svitl
ana
Don
ska
Ukr
aine
Dr.
Vale
ntin
Usa
tche
nko
9500
0 Sy
mph
erop
ilT
ytov
a-St
r. 77
Hem
atol
ogy
Dep
artm
ent i
n K
rym
Repu
blic
an C
hild
ren´
s Hos
pita
l
0410
7 K
yiv
Ukr
aine
Serg
ey D
yma
Regi
onal
Onc
olog
ic H
ospi
tal
Ped.
Onc
olog
y-H
emat
olog
y D
ep. i
n K
iev
Bagg
ovut
ovsk
a-St
r. 1a
0410
7 K
yiv
Ukr
aine
Dr.
Elen
a K
rem
insk
aRe
gion
al O
ncol
ogic
Hos
pita
l Re
gion
al O
ncol
ogic
Hos
pita
l Pe
d. O
ncol
ogy-
Hem
atol
ogy
Dep
. in
Kie
vBa
ggov
utov
ska-
Str.
1a
Ukr
aine
0410
7 K
yiv
Bagg
ovut
ovsk
a-St
r. 1a
Ped.
Onc
olog
y-H
emat
olog
y D
ep. i
n K
iev
Nat
iona
l Coo
rdin
ator
:V
ice-
Coo
rdin
ator
:D
ata
Man
ager
:N
atio
nal R
efer
ence
Lab
orat
ory
for I
mm
uno p
heno
typi
ng:
ALL IC-BFM 2002
Dr.
Ale
jand
ro G
onzá
lez
Dr.
Eva
G. S
varc
hSe
rgio
Mac
hin
Dr.
Cons
uelo
Mac
ías
Inst
ituto
de
Hem
atol
ogia
e Im
mun
olog
iaIn
stitu
to d
e H
emat
olog
ia e
Imm
unol
ogia
Inst
ituto
de
Hem
atol
ogia
e Im
mun
olog
iaIn
stitu
to d
e H
emat
olog
ia e
Imm
unol
ogia
Ave
San
Fra
ncisc
o y
calle
E A
ltaha
bana
Ave
San
Fra
ncisc
o y
calle
E A
ltaha
bana
Ave
San
Fra
ncisc
o y
calle
E A
ltaha
bana
Ave
San
Fra
ncisc
o y
calle
E A
ltaha
bana
10 8
00 L
a H
aban
a10
800
La
Hab
ana
10 8
00 L
a H
aban
a10
800
La
Hab
ana
Cuba
Cuba
Cuba
Cuba
Prof
. Dr.
Lebr
iz Y
ukse
l Soy
can
Prof
. Dr.
Naz
an C
etin
gul
Dr.
Hilm
i Apa
kU
nive
rsity
of I
stan
bul,
Cerr
ahpa
sa M
edic
al S
choo
lEg
e U
nive
rsity
Med
ical
Sch
ool
Uni
vers
ity o
f Ist
anbu
l, Ce
rrah
pasa
Med
ical
Sch
ool
Tur
key
Tur
key
Tur
key
Dep
artm
ent o
f Ped
iatr
ic H
emat
olog
y/O
ncol
ogy
Dep
t. of
Ped
iatr
ic O
ncol
ogy
Dep
artm
ent o
f Ped
iatr
ic H
emat
olog
y/O
ncol
ogy
3430
3 A
ksar
ay -
Ista
nbul
3510
0 Bo
rnov
a - I
zmir
3430
3 A
ksar
ay -
Ista
nbul
Dr.
Dra
gana
Jani
cD
r. D
raga
n M
icic
Jele
na L
azic
Dr.
Boja
na S
lavk
ovic
Uni
vers
ity C
hild
ren´
s Hos
pita
lIn
stitu
te fo
r Mot
her a
nd C
hild
Uni
vers
ity C
hild
ren´
s Hos
pita
lIn
stitu
te fo
r Mot
her a
nd C
hild
Appendix 5.0
Dep
t. H
emat
olog
y/O
ncol
ogy
Dep
t. H
emat
olog
yD
ept.
Hem
atol
ogy/
Onc
olog
yLa
bora
tory
for I
mm
unop
heno
typi
ngT
irsov
a 10
Rado
ja D
akic
a 6-
8T
irsov
a 10
Rado
ja D
akic
a 6-
811
000
Belg
rade
1107
0 Be
lgra
de11
000
Belg
rade
1107
0 Be
lgra
deY
ugos
lavi
aY
ugos
lavi
aY
ugos
lavi
aY
ugos
lavi
a