Embed Size (px)
Citation preview


Alexander Dubček University of Trenčín
Izhevsk State Technical University
Publishing House:Alexander Dubček University of TrenčínIzhevsk State Technical University

(The international scientific journal founded by two universities from the Slovak Republic and Russian Federation)
This journal originated with kindly support of Ministry of Education of the Slovak Republic
Editor-in-Chief
Kneppo Ivan, Prof., Ing., DrSc., Alexander Dubček University of Trenčín
Science Editor
Dubovská Rozmarína, Prof., Ing., DrSc., Alexander Dubček University of Trenčín
Honorary Editors
Kneppo Ivan, Prof., Ing., DrSc.rector, Alexander Dubček University of Trenčín, Slovakia
Jakimovič Boris Anatoľjevič, Prof., DrSc. rector, Izhevsk State Technical University, Russian Federation
Members
Barborák Oto, Assoc. prof., Ing., CSc.Bielik Ján, Assoc. prof., MUDr., PhD.Kurty Ján, Prof., Ing., PhD.Lipták Peter, Assoc. prof., Ing., CSc.Meluš Vladimír, RNDr., PhD.Pajtášová Mariana, Assoc. prof., RNDr., PhD.Strunz Herbert, Prof., Dr.Tkáč Jozef, Assoc. prof., Ing., PhD.Vavro Ján, Prof., Ing., PhD. Vojtovič Sergej, Assoc. prof., Mgr., DrSc.
Jakimovič Boris Anatoľjevič, Prof., DrSc. Alijev Ali Vejsovič, Prof., DrSc. Turygin Jurij Vasiľjevič, Prof., DrSc. Ščenjatskij Aleksej Valerjevič, Prof., DrSc. Kuznecov Andrej Leonidovič, Prof., DrSc. Fiľkin Nikolaj Michajlovič, Prof., DrSc. Sivcev Nikolaj Sergejevič, Prof., DrSc. Senilov Michail Andrejevič, Prof., DrSc. Klekovkin Viktor Sergejevič, Prof., DrSc.Trubačev Jevgenij Semenovič, Prof., DrSc.
Alexander Dubček University of Trenčín Slovak Republic
Izhevsk State Technical UniversityRussian Federation
Editorial Office
Študentská 1, 911 50 Trenčín, Tel.: +421 (0) 32 7 400 279, +421 (0) 32 7 400 [email protected], [email protected]

Macharová Nikola, Mgr., Alexander Dubček University of Trenčín
Redaction
Publishing House
University Review Vol. 4, No. 4Trenčín: Alexander Dubček University of Trenčín2010, 54 p.ISSN 1337-6047EV 3723/09
Alexander Dubček University of Trenčín, Študentská 2911 50 Trenčín, Slovak Republic
Izhevsk State Technical University, Russian Federation
Slezáková Zuzana, Mgr.
Graphic Design
Technical Information
© 2010 All rights reserved.Alexander Dubček University of Trenčín, Slovak Republic

1
Contributors
contents
23
28
42
36
49
20
15
2
7
3
Eva Červeňanová, Gabriela OpršalováNursing Standards and Intensive Care
Eva ČerveňanováStudy of Nursing The University Igbinedion Okada, Benin City in Nigeria
Miriama Záhumenská, Zdenka Krajčovičová, Vladimír Meluš
Ján Bielik, Milan Hlista, Slavomír Černok, Miroslav Šorf
Jana Slobodníková
Nikoleta Poliaková
Gabriela Rozvadský Gugová
Effectiveness of PSA Assay in Prostate Cancer Screening
Crohn´s Disease and Quality of Life
Ultrasound Guided Biopsy and Cytology During Differential Diagnosis and Therapy of Postoperative Changes After Conserving Treatment of Breast Cancer
Involment of Nurses In Promoting Health Child Poulation
Coping Strategies In Conflict Situations (Anxiety and Avoidance)
Vladimír Meluš, Zdenka Krajčovičová, Erika Štrbavá, Jana SlobodníkováCardiac Markers: Practical Limitations in Routine Laboratory Analyses
11 Vladimír Meluš, Zdenka Krajčovičová, Ľubica PieseckáInfectious Agens: Underrated Factors in Human Nutrigenomics?
Iveta Matišáková, Katarína Gerlichová, Eva ČerveňanováEducation in Nursing – New Trends

2
Vladimír Meluš, Zdenka Krajčovičová, Jana Slobodníková, Iveta Matišáková, Katarína Gerlichová, Eva Červeňanová, Ján Bielik, Nikoleta Poliaková Faculty of Healthcare, Alexander Dubček University of Trenčín, Trenčín, Slovak Republice-mail: [email protected]: [email protected]: [email protected]: [email protected]: [email protected]: [email protected]: [email protected]: [email protected]
Milan Hlista, Slavomír Černok, Miroslav ŠorfOffice of Gastroenterology and Dept. of Gen. Medicine, Hospital with Outpatient Department, Trenčín/Nové Mesto nad Váhom, Slovakiae-mail: [email protected]: [email protected]
Gabriela Opršalová, Faculty Hospital in Trenčín, Slovak Republice-mail: [email protected]
Erika Štrbavá, Ľubica Piesecká, Faculty Hospital in Nitra, Slovak Republice-mail: [email protected]: [email protected]
Miriama Záhumenská, Dpt. of Clinical Biochemistry, NsP Nové Mesto nad Váhom, Slovakia
e-mail: [email protected]
Gabriela Rozvadský Gugová, Faculty of Social and Economic Relations, Alexander Dubček University of Trenčín, Trenčín, Slovak Republice-mail: [email protected]
contributors
Eva Červeňanová, Gabriela Opršalová
Eva Červeňanová
Miriama Záhumenská, Zdenka Krajčovičová, Vladimír Meluš
Ján Bielik, Milan Hlista, Slavomír Černok, Miroslav Šorf
Jana Slobodníková
Nikoleta Poliaková
Gabriela Rozvadský Gugová
Vladimír Meluš, Zdenka Krajčovičová, Erika Štrbavá, Jana Slobodníková
Iveta Matišáková, Katarína Gerlichová, Eva Červeňanová
Reviewers
Bielik Ján, assoc. prof., MUDr., CSc.Červeňanová Eva, PhDr., PhD.Meluš Vladimír, RNDr., PhD.Krajčovičová Zdenka, RNDr., PhD.Slobodníková Jana, assoc. prof., MUDr., CSc.Botíková Andrea, assoc. prof., PhDr., PhD.Herman Oto, MUDr.
Kozics Katarína, RNDr., PhD.Nemcová Jana, PhDr., PhD.Novodvorská Michaela, RNDr., PhD.Porubský Ján, assoc. prof., MUDr., CSc.Strmeň Jura, MUDr., PhD., FAOIHeretik Anton, assoc. prof., Mgr., PhD.Iljevová Ľubica, assoc. prof., PhDr., PhD.

3
Vladimír Meluš, Zdenka KrajčoVičoVá, erika štrbaVá, jana SlobodníKoVá
The rapid evaluation of patients with symptoms of an acute coronary syndrome is of great clinical relevance. The reliability of cardiac markers routinely used in the diagnostics of cardiovascular dis-eases (AST, CK, CK-MB and troponin T) are significantly influenced by their biological and analytical variability. The goal of our study was therefore to verify their actual clinical value, sensitivity and specificity in routine laboratory settings. In 80 randomly selected patients (45 with ischemic heart disease and 35 with hypertensive heart disease) were analysed and the concentrations of AST, CK, CK-MB and troponin T were recorded as an integral part of standard diagnostics. Troponin T and CK-MB showed equal sensitivity (0.31; 95% CI: 0.18 – 0.47), whereas the test specificity was higher in troponin T (0.97; 95% CI: 0.85 – 0.99) compared to CK-MB isoenzyme (0.86; 95% CI: 0.70 – 0.95). In respect of genders, none of analytes had outright diagnostic value. The utilization of these cardiac markers in laboratory diagnostics is therefore limited. Further research is needed to determine if a multimarker strategy of established and newer biomarkers is a feasible approach for better risk stratification and therapeutic choice in patients with suspected acute coronary syndrome.
Abstract
cardiac markers, variability, diagnostic value
Key words
Over the past two decades, the development and implementation of cardiac markers
have fundamentally improved the laboratory diagnostics of cardiovascular diseases (1). While the individual’s risk factors genotyping is an im-portant tool in prevention of cardiovascular dis-eases, the use of biochemical markers is essen-
tial, especially in the acute phase of diseases (2). Laboratory testing of heart function began with “classical“ enzymes such as: aspartate transami-nase (AST), lactate dehydrogenase (LDH), creat-ine kinase (CK), and creatine kinase isoenzyme CK-MB. However, of these enzymes only CK-MB is relatively specific for ischemic heart disease
cardiac markers: practical limitations in routine laboratory analyses

4
(IHD). AST is also specific for liver tissue damage and LDH levels can be elevated due to infections or malignancy.
Nowadays, measurement of circulating car-diac troponins (cTn) plays a fundamental role in the diagnosis and management of acute coro-nary syndromes (3). Cardiac troponin I and T are not enzymes, but the proteins binding to the tropomyosin. They are released from the myocytes cytosol after myocardial injury and have increased specificity compared with the enzyme CK-MB. Currently, there are three oth-er markers (apart from the classic risk factors), which have sufficient evidence of clinical utility to be recommended for regular clinical use: B-type natriuretic peptides, C-reactive protein and D-dimer. B-type natriuretic peptides (BNP and NT-proBNP) aid in the diagnosis of chronic as well as acute heart failures, provide prognos-tic information, and might help in the targeting of therapies. C-reactive protein (CRP) is a bi-omarker associated with increased cardiovascu-lar risk that demonstrated an important role in identifying apparently healthy individuals who could benefit from intensive statin therapy. D-dimer has proven clinically useful in ruling-out deep-vein thrombosis and pulmonary embolism (4). Also promising in this regard are ischemia modified albumin (IMA) and heart-type fatty acid binding protein (4-7).
More recently, novel or improved analytical methods for myoglobin, CRP, CK-MB or cardiac troponin assays have been developed that are more sensitive than currently used assays (4, 8).
However, the present situation is still far from ideal. There are three factors negatively influencing the precision and accuracy of labo-ratory results. Specific markers can be analysed with kits from different manufacturers, which are often based on different biochemical princi-ples. A second issue is the lack of harmonization (or rather synchronization) in different assays produced by various companies (9). Third key factor in the analytical process is the measure-ment uncertainty (U). Laboratories undergoing the certification and accreditation process are
bound to disclose U in their public issues (10). For example, CK-MB shows usually U= 6-10%, for troponin T it is often the case that U= 10-15%. In other words, the obtained numerical re-sult of individual could theoretically deviate by ± 6% or ± 15% of the given value. This is critical especially in cases of numerical results, which are near to upper limiting values.
The aim of our work was to confirm the real sensitivity and specificity of routinely used car-diac markers and their diagnostic values.
material and methodsIn our study we evaluated the data of 80 pa-tients. 35 patients had hypertensive heart dis-ease (HHD) and 45 patients had ischemic heart disease (IHD). All data were obtained during the same time period and we de-identified them to ensure the anonymity of patients.
AST, CK and CK-MB were tested with the AU640 (Olympus) analyzer (kinetic UV-test), levels of troponin T were tested using the Elec-sys 2010 (Roche) system (sandwich ECLIA). All samples were measured according to standard operating procedures of the laboratory. In all samples no additional parameters were tested except of those ordered by physicians.
Categorical data were evaluated with the Fischer’s exact test, while numerical values were tested with the non-parametrical Mann-Whitney test, since the data showed non-nor-mal distribution. Due to the lack of normality, basic statistical parameters are given as arith-metical mean, standard deviation together with median.
results and discussionThe first remarkable finding relates to gender. The mean age of tested group was 63.8 years (n = 80, SD = 12.74). Male patients had signifi-cantly lower mean age (mean = 59.3; n = 38; SD = 10.45) compared to female patients (mean = 68.7; n = 42; SD = 13.05; Mann-Whitney test p < 0.001). The obtained results showed evidence of a close relationship between the incidence of

5
cardiovascular diseases and the life expectancy in our population (11), because this types of di-agnoses are the leading cause of mortality of the population (12).
Upper reference limits for cardiac markers were: AST 0.62 μkat/L for male patients and 0.52 μkat/L for female patients; CK 2.87 µkat/L for male patients and 2.48 µkat/L for female pa-tients; CK-MB 0.42 µkat/L and troponin T 0.10 ng/ml. Only CK-MB and troponin T were com-pared in both groups of patients with ischemic and hypertensive heart disease, because of their acceptable sensitivity and specificity as found in common literature sources (13-15).
Our results show that CK-MB isoenzyme had lower sensitivity (0.31; 95% CI: 0.18 – 0.47) than specificity (0.86; 95% CI: 0.70 – 0.95) with a negative predictive value of 0.49 (95% CI: 0.36 – 0.63). Troponin T showed slightly better specif-
ity (0.97; 95% CI: 0.85 – 0.99) but almost identi-cal sensitivity (0.311; 95% CI: 0.18 – 0.47), with a negative predictive value of 0.52 (95% CI: 0.40 – 0.65).
The Fischer’s exact test revealed that only troponin T is able to differentiate significantly between both groups with IHD and HHD (p = 0.001). Isoenzyme CK-MB exceeded reference ranges in only 14 of 45 patients with IHD, but in 5 of 35 individuals suffering from HHD (Fischer’s exact test p = 0.11).
The next question was about the normality of the obtained numerical data. Lower numbers of individuals could be problematic for para-metrical statistical tests. Therefore we used the non-parametrical Mann-Whitney U test for as-sessing whether IHD and HHD in both genders have equally large numerical values of tested cardiac markers (table 1).
PARAMETER GENDER DIAGNOSES N X SD M P
AST
men IHD 23 0.71 0.87 0.47 0.16
HHD 19 0.47 0.27 0.41
women IHD 22 0.59 0.50 0.44 0.37
HHD 16 0.49 0.29 1.56
CK
men IHD 23 4.93 8.86 2.88 0.77
HHD 19 3.12 3.12 1.77
women IHD 22 4.29 5.92 2.12 0.31
HHD 16 1.99 1.22 0.24
CK-MB
men IHD 23 0.50 0.77 0.32 0.23
HHD 19 0.30 0.10 0.27
women IHD 22 0.55 0.60 0.39 0.07
HHD 16 0.31 0.17 0.24
Trop Tmen IHD 23 0.24 0.61 0.06 0.01
HHD 19 0.02 0.02 0.01
women IHD 22 0.25 0.71 0.01 0.28
HHD 16 0.06 0.19 0.01
Tab. 1: Cardiac markers in particular groups of gender and diagnosis
Legend: n - number of patients, X - arithmetical mean (bold values were over reference limits), SD – standard deviation, M – median, p – significance values of Mann-Whitney test results, IHD – ischemic heart disease, HHD - hypertensive heart disease, AST - aspartate transaminase, CK - creatine kinase, CK-MB – creatine kinase isoenzyme, Trop T - cardiac troponin T
6
Our results showed a large variability in numeri-cal values, which excessively increased stand-ard deviation values. That is the reason of list-ing median values together with arithmetical means and standard deviations. We can see from Table 1 that of all categories tested, only troponin T levels in male patients showed statis-tically significant differences between IHD and HHD patients.
conclusionIn our examination of the cardiac markers com-monly used in routine laboratory diagnostics in the Slovak Republic, we found a broad range of concentrations. This variability is not only the consequence of intraindividual and interindi-vidual differences, biological, seasonal and cir-
cadian rhythms, but also the result of impreci-sion and inaccuracy of the different analytical methods. The utilization of these cardiac mark-ers in laboratory diagnostics is therefore limit-ed. Further research is needed to determine if a multimarker strategy of established and newer biomarkers is a feasible approach for better risk stratification and therapeutic choice in patients with suspected acute coronary syndrome. We believe that all these factors together with the considerably longer time of work flow in labo-ratory can make point-of care testing advanta-geous for routine applications. In the nearer fu-ture we expect that “classical” laboratories will be more effective rather in special analyses such as genotyping and proteotyping in personalized medicine and nutrigenomics.
PEETZ D, SCHWEIGERT R, JACHMANN N, et al. Method comparison of cardiac marker assays 1. on PATHFAST, StratusCS, AxSYM, Immulite2000, triage, elecsys and cardiac reader. Clin Lab 2006;52:605-614.MELUS V, KIRICOVA G, SIMEK M. Laboratory testing of hereditary trombophilia: Previous data in 2. the face of verification. Bratisl. Lek. Listy 2009;110:18-20.KOCIOL RD, PANG PS, GHEORGHIADE M, FONAROW GC, O’CONNOR CM, FELKER GM. Troponin 3. elevation in heart failure prevalence, mechanisms, and clinical implications. J Am Coll Cardiol. 2010;56(14):1071-1078.HOCHHOLZER W, MORROW DA, GIUGLIANO RP. Novel biomarkers in cardiovascular disease: 4. update 2010. Am Heart J. 2010;160(4):583-594.DEKKER MS, MOSTERD A, VAN´T HOF AW, et al. Novel biochemical markers in suspected acute 5. coronary syndrome: systematic review and critical appraisal. Heart 2010;96:1001-1010.KIM Y, KIM H, KIM SY, et al. Automated heart-type fatty acid binding protein assay for the early 6. diagnosis of acute myocardial infarction. Am J Clin Pathol 2010;134:157-162.VASILE VC, SAENGER AK, KRONING JM. Biological and analytical variability of a novel high-sensi-7. tivity cardiac troponin T assay. Clin Chem 2010;56:1086-1090.VIKENES K, MELBERG T, FARSTAD M, et al. Elevated CK-MB values after routine angioplasty pre-8. dicts worse long-term prognosis in low risk patients. Scand Cardiovasc J 2000;2:69-75.PENTTILÄ IM, LAATIKAINEN A, PENTTILÄ K, et al. Imprecision of cardiac marker analyses among 9. laboratories on the basis of external quality assurance results: Finnish experience. Scandinavian Journal of Clinical and Laboratory Investigation 2007;67:507-518.Slovak national accreditation service: Medical laboratories. Available on website: http://www.10. snas.sk/e/index.php?page=4&ts=1&id_druh=10GINTER E, HULANSKA A. Social determinants of health in Slovakia. Bratisl Lek Listy 2007;10-11-11. :477-479.
Literature

7
PISKOVA T, GAVORNIK P. Epidemiology of vascular disease. Vnitr. Lek 2010;1:53-58.12. TZIVONI D, KOUKOUI D, GUETTA V, et al. Comparison of Troponin T to creatine kinase and to 13. radionuclide cardiac imaging infarct size in patients with ST- elevation myocardial infarction un-dergoing primary angioplasty. Am J Cardiol 2008;101:753-757.INNES G, CHRISTENSON J, WEAVER WD, et al. Diagnostic parameters of CK-MB and myoglobin 14. related to chest pain duration. Canadian Journal of Emergency Medicine 2002;5:322-330.NAGAHARA D, NAKATA T, HASHIMOTO A, et al. Early positive biomarker in relation to myocardial 15. necrosis and impaired fatty acid metabolism in patients presenting with acute chest pain at an emergency room. Circ J 2006;70:419-425.
iveta MatišáKoVá, Katarína GerlichoVá, eva čerVeňanoVá
education in nursing – new trends
The authors focused on the significance and future of education in nursing and on stressing of the role of nurse-educator. The aim of the education is to increase the health consciousness of the population – healthy and ill at the same time. Thereby we can reach better cooperation with the doctor, following the treatment, physiotherapy and ordering mainly at long-term treatment. It is important to teach the patient to decide correctly in the matters of health, to create life attitudes, values and to teach him some skills. Therefore, it becomes one of the most important tasks of the nurse, despite the fact that her competences do not include it.
Abstract
Nursing, as science branch, has certain re-lation towards other sciences; interferes
into diagnostics, prevention, therapy, health fortifying, and also into social and education area. Pedagogy helps the nursing to manage the education techniques of effects on person, with
the aim to reach changes in attitudes, behavior, acting, and lifestyle of healthy and ill person (Farkašová, 2005).

8
Education is one of the most difficult tasks of nursing. It creates space for new knowledge, skills or creation of emotional, value, motion structures of the personality and for reaching of positive change in behavior (Magurová, 2009). It has a significant role at reaching changes in patient’s behavior and is considered as part of standard care, which is provided by nurses. Edu-cation in nursing is a process, which influences the behavior of patient, family, community with the aim to make changes in the area of knowl-edge, skills and attitudes.
„Since half of 1800, when nursing was acknowl-edged as a unique discipline, the responsibility for education of patients has become a natural com-ponent of nurses’ endeavor as the care provider“ (Nemcová et al., 2010, p. 17).
Since the times of Florence Nightingale, the work of nurses was traditionally perceived as ap-prentice, often realized in religious orders by young women. However, there was a part of nurses – men. In 1860, Florence Nightingale founded first training school for nurses in St Thomas’ Hospital in London. Nightingale’s teaching schedules were based on nurse practice, and with instructions fo-cused on hygienic needs and task competence. Her methods are described in her publication “Notes on Nursing” from 1898.
Florence Nightingale stressed the importance of education of patients in need of fresh air, proper nutrition, exercise and personal hygiene (Nemcová et. al., 2010).
According to regulation of Ministry of Health of Slovak Republic No. 364/2005 Coll., which de-termines the volume of nursing practice provided by the nurse individually and in cooperation with the doctor and the volume of practice of midwife assistance provided by a midwife individually and in cooperation with a doctor, as later amended is a constituent of nursing care of patients, when the nurse educates the person, the family or the com-munity about the nursing practice with stress on self-sufficiency.
Education can help the patient to adapt to a new life situation caused by change of health state. It enables the patient to get to know his
disease and thereby prevent from deteriora-tion of health. It helps the patient and his family to overcome the obstacles, fear, anguish, and, what is most important – it helps him to keep or reinstate his self-sufficiency and independence and thereby the quality of life.
By means of education, we integrate the pa-tient deeper into medical and nursing processes; we support prevention and prevent from deterio-ration of the illness. It is important to proceed con-sistently according to the educational plans in or-der to educate the patient successfully (Gerlichová et. al., 2008).
Education role of the nurse belongs to the ba-sic competences of registered nurses. The role of the nurse as an educator consists in her active sup-port of learning and creating conditions for learn-ing. She is at the head of the education team, she thinks about how the individual team members (doctor, physiotherapist, nutrition assistant) can help the family. It is necessary, that during creation and realization of education process she has the knowledge and skills; she should be able to moti-vate the patients into learning, know the education techniques and organizational forms of education, and provide tools needed and cooperate with oth-er team members.
the need of the role of the nurse as an educator mirrors in following areas:
Nurses actively educate individuals, fami-1. lies, communities, so that they would take over the responsibility for their healthNurses provide professional care2. Their role, status, credibility is projected 3. into their educationNurses help by providing, reaching physical, 4. mental and social potential within the con-text of the environment, in which their work (Magurová, 2009).
Education process in nursing was often com-pared with nursing process. Even though the steps might be similar, the aims remain differ-ent. Education depends on the phase of illness, in which it is realized.

9
Credibility Competency Communicativeness Accuracy
Nurse:Chooses what the pa-
tient should learn
Nurse:Decides, what is impor-
tant to learn
Nurse:Provides clear information
Nurse:Respects patient’s fears
Prepares appropriate educational plan
and material
Teaches house manage-ment of special troubles
Uses simple pictures and models
Show sensibility towards patient’s mood
Reduces patient’s anguish
Provides safety to the patient
Speaks patient’s language
Is emphatic, supports the patient
Provides accurate educa-tional environment
Provides customized written instructions
Chooses time appropri-ate for education
Tab. 1: Characteristics of nurse responsible for education (Nemcová et. al., 2010)
Education initial (preparation of patient to per-manent colostomy)
Education supplementary – (we supple-ment the knowledge about care of colostomy, practice of skills)
Education continuous – (after release into home care – adaptation to life in home and pro-fessional life)
Reeducation – if the desired behavior of pa-tient is not reached
education has 5 phases:Judgment1. – before the education starts, it is important to know the patient, his family members, their ability to learn, their motiva-tion to learn, agents influencing the learnig, obstacles at learning, sources of support from the side of the family.Educational diagnosis2. – based on judgment, it is necessary to determine the diagnosis, which relate to deficit in knowledge, skills or patient’s attitudes. Plan of education 3. – originates in the priori-ties of education – what the patient needs to learn at first, what will be the subject of further education, one educational unit = education. An essential part of this phase is target de-termination: Cognitive – focused on the area of knowl-edge, intellectual skills and cognitive abili-ties
Emotional (attitude) – include mainly emo-tional area, opinions, attitudes, values. Their reaching is the main aim of education – edu-cational aimsBehavioral (psycho-motive, skill) – focused on obtaining motive skills and adopting hab-its.Realization of educational plan4. Motivational – preparation of the educated for learningExpositional – first contact of student with new study topicsFixation – primary repetition and fixation of study topicsEvaluating – control of learned knowledge, abilities, skills and habitsEvaluation5. – is a process, when the nurse and the patient (family, community) evalu-ate, what they learned. Intentions and tar-gets of education are evaluated as well.
Factors, which help the education:Compliance, motivation, readiness, feedback, repetition of key words and notions, logically set leaning material.
Factors interrupting the education:Physical state of the patient, cultural barriers
the attitude in education includes following rules:Continuity, reversibility, exactness, uncontradic-tion, accuracy, resolution, connection of theory

10
and practice, positive evaluation, seriousness and honor towards client’s personality, individ-ual approach, activeness (Závodná, 2006).
The result of the education, which is real-ized on time, comprehensibly, by an accurately learned educator, is that a well educated patient trusts us, cooperates better and will take over responsibility for his health sooner (Magurová, 2009)
The use of education in practice is nowadays deficient; often it is only formal – in the form of submission of little information to patient or his family. It is important to realize, that the impact of the nurse in cooperation with other member of health-care team (doctor, physiotherapist, nutrition assistant, speech therapist, psycholo-gist and other members) on the patient can be crucial for faster process of healing of patient, for shortening his stay at hospital and thereby decreasing the risk of repeated illnesses and numerous complications (Matišáková, et. al., 2008).
Health concerns the whole man and his environ-ment that affect their people behavior and life-time care for your body and soul. It should start right from early childhood to The acquisition habits, skills and attitudes to promote health as soon as possible. Based on these patterns are already in childhood creates a healthy lifestyle. (Červeňanová, 2008)
Concerning gaining positive attitude of an individual towards his own health, the struggle for realization of education activity of the nurse is stressed. For the future, it will be necessary to work out the competences of nurses for the area of education, so that they might fully apply the requirements resulting from the education process in practice. Nurse, who would be fully devoted to education of patients, would take full responsibility for her activity. To the fore comes education not in the form of information and instructions, but in the form of an education process focused on individual and his family, his problems and needs. The aim of the education is to improve the quality of their lives.
ČERVEŇANOVÁ, E. 2008 Výchova k zdraviu - edukačný projekt pre deti v predškolskom ob-1. dobí. [CD ROM ] In: Výchova a vzdelávanie v ošetrovateľstve , Zborník z II. vedeckej konferencie pedagogických pracovníkov v ošetrovateľstve. Trenčín: 2008, ISBN: 978-80-8075-265-1 , EAN: 9788080752651 , s.187-196 FARKAŠOVÁ, D. 2005. Teória ošetrovateľstva. Martin: Osveta, 2005. 212s. ISBN 80-8063-227-8. 2. GERLICHOVÁ, K., MATIŠÁKOVÁ, I., MIŠINOVÁ, M. Úloha sestry v podpore zdravia u pacienta po 3. prekonanom infarkte myokardu. [CD-ROM]: In Úlohy pedagogických pracovníkov v sústavnom vzdelávaní zdravotníckych pracovníkov: Vedecké práce z medzinárodnej interdisciplinárnej kon-ferencie. Trenčín : 2007. ISBN 978-80-8075-218-7, s.172-182.MAGUROVÁ, D., MAJERNÍKOVÁ, Ľ. 2009. Edukácia a edukačný proces v ošetrovateľstve. 1. vyd. 4. Martin: Osveta, 2009. 155 s. ISBN 978-80-8063-326-4.MATIŠÁKOVÁ, I., KVASNICOVÁ, Z., POLIAKOVÁ, N. Návrh edukačného plánu u geriatrického 5. pacienta v prevencii vzniku dekubitu v domácej ošetrovateľskej starostlivosti. [CD-ROM]: In Ošetrovateľstvo a zdravie II. Trenčín : TnUAD, 2008. ISBN 978-80-8075-322-1, s.209-215.NEMCOVÁ, J., HLINKOVÁ, E. 2010. Moderná edukácia v ošetrovateľstve. 1. vyd. Martin: Osveta, 6. 2010. 260 s. ISBN 978-80-8063-321-9.ZÁVODNÁ, V. 2006. Pedagogika v ošetrovateľstve. Martin: Osveta, 2006. 117 s. ISBN 80-8063-7. 193-X.
Literature

11
Vladimír Meluš, Zdenka KrajčoVičoVá, Ľubica PieSecKá
inFectious agens: underrated Factors in human nutrigenomics?
During the past years human nutrition has proved to be very important player in the biomedical research and all facilities of the nutritional genomics (or nutrigenomics) allow us to understand its processes on the molecular level. The new era of nutrition research translates empirical knowl-edge to evidence-based molecular science. Modern nutrition research is focused on preventing or delaying the onset of diseases, on health improving, and assessing risk factors. Infectious agents represent along with the nutrition another very important epigenetical factor, which could mark-edly influence the human metabolism. The aim of the article is to briefly advise of current trends in today s human nutrigenomics. In the present minireview, we have summarized important tasks of today s human nutrigenomics. In addition, examples of the factors complexly affecting the liver function (hereditary hemochromatosis, HCV and nutrition) and their relative interactions are also discussed.
Abstract
nutrition, hereditary hemochromatosis, HCV
Key words
Nutrigenomics (or nutritional genomic) is relatively new branch of nutrition science,
which aim is to study the impact of the foods we eat on the function of our genes (1, 2). To-day there is already clear that the diet is more than the merely food intake. The traditional nu-trition research has been focused on providing nutrients to nourish populations and preventing specific nutrient deficiencies (3). Nutrigenom-ics explores health-related aspects of individual
bioactive components as well as entire diets and this at group rather than population level (3-6). All recognized epigenetic factors (includ-ing DNA methylation, histone modification, and microRNA expression) are influenced by envi-ronmental exposures, including diet, tobacco, alcohol, physical activity, stress, environmen-tal carcinogens, genetic factors, and infectious agents which play important roles in the etiol-ogy of cancer. Some of these epigenetic modi-

12
fications change the expression of tumor sup-pressor genes and oncogenes and, therefore, may be causal for tumorigenesis (7).
The role of nutrigenomics is to investigated and analysed nutrients with the aid of the cut-ting-edge techniques, facilitating the latest find-ings in transcriptomics, metabolomics and pro-teomics areas of the functional nutrigenomics (8). On the opposite site, the nutrigenetics ex-amines the influence of genetic variation on nu-trient requirements and interactions between metabolic diseases and diet.
Nowadays, the role of nutrition and nutri-ents in “metabolic programming“ taking place during very early period of human life, is the most discussed question. It has an important effect on development of organism and pre-determination of metabolic diseases further in adulthood (9, 10). Identifying of nutritionally regulated genes (mostly by DNA methylation) involved in regulatory pathways of metabolism, could lead to personal-unique diet used in the so-called “personalized nutrigenomics“ (11-14).
Personalized nutrition is a conceptual ana-logue to personalized medicine and means adapting food to individual needs. Nutrigenom-ics and nutrigenetics build the science foun-dation for understanding human variability in preferences, requirements, and responses to diet and may become the future tools for con-sumer assessment motivated by personalized nutritional counseling for health maintenance and disease prevention (9). However, there is still dubious area of interactions like: pathogen → genome ← nutrient, which must be carefuly illuminated from the both sides of nutrigenom-ics and nutrigenetics, respectively. In liver oc-curring interactions HBV/HCV → hereditary he-mochromatosis ← iron uptake could be a typical example.
liver and single nucleotide polymorphismsHereditary hemochromatosis (HH) is an exam-ple of inherited disorder of iron metabolism, leading to its accumulation in various organs.
HH cause tissue damages of variable intensity, especially in the liver, which plays major role in the metabolism. As a result, liver cirrhosis and malignant hepatoma can be diagnosed (15).
The most frequently HH-associated human hemochromatosis (HFE) gene-mutations (Cy-s282Tyr and His63Asp) revealed merely statis-tical association with the disease. Lower HH-penetrance in the presence of the mutations (approximately 5% developing clinical symp-toms for Cys282Tyr) indicates, that there are necessary, but not sufficient causes of its clini-cal manifestation (16). It is not surprising, that multigene-ground (together with other non-HFE genes) with supposed apheliotropic effect and environmental factors are assumed in the mechanism of HH clinical manifestation (17).
Among non-HFE genes we can find trans-ferrin-receptor 2 (TFR2 or HFE3), hemojuvelin (HJV or HFE2), hepcidin (HAMP-hepcidin anti-microbial peptide or HFE2B) and ferroportin-1 (SLC11A3) (18, 19).
liver and hepacivirusesOf course, the term “environmental factors“ leads us back to dietary effect of the food and supporting nutritional therapy. Trouble is, that there might be another hidden, but more im-portant and stronger epigenetic factor, chroni-cal hepatitis. It is often asymptomatic, caused by hepatitis B virus (HBV), but more frequently by hepatitis C virus (HCV). HBV and HCV particles are transmitted by blood-to-blood contact, and especially HCV tends to chronic form of disease. HCV belongs to Flaviviridae family, with genetic information stored in single-stranded positive sense RNA. We know six major genotypes of HCV (marked 1-6) (20). It is well documented, that HCV can directly alter host cell lipid me-tabolism through nuclear transcription factors. To date, only a limited number of studies have been on the effect of human foods on the nucle-ar transcription factors of HCV-induced hepato-steatosis (1).

13
Even in acute phase of the hepatitis C the ma-jority of infected people do not manifest any syndromes (21). The actual risk of HCV rests just in its ability for affecting the processes of metabolic pathways in liver cells, which influ-ences the whole human metabolism. The con-sequences are serious, leading in some cases to hepatosteatosis, cirrhosis and liver cancer. HCV treatment is time consuming (approx. 24 - 48 weeks, depending upon particular genotype), and used preparates (e.g. pegylated interferon alpha combinated with ribavirin) have uncom-fortable side-effects (e.g. anemia, psychiatric problems) (1, 22).
Some previous population studies have in-dicated higher sensitivity to HCV in the case of H63D heterozygous females (23). A recent pro-spective clinical trial suggests that patients with chronic hepatitis C may benefit from strict di-etary instructions. Increasing evidence suggest that some crucial nuclear transcription factors related to HCV-associated hepatosteatosis and HCV RNA itself can be controlled by specific anti-HCV nutrition (1, 24). In another study only three nutrients, selected among 46 different nu-trients: beta-carotene, vitamin D2, and linoleic acid were found in a cell culture system to inhib-it HCV RNA replication. In addition, polyunsatu-rated fatty acids (PUFAs) especially arachidonic acid, docosahexaenoic acid, and eicosapentae-noic acid have been demonstrated to diminish HCV RNA replication. These PUFAs, in particular the highly unsaturated n-3 fatty acids change the gene expression of PPARa and SREBP, sup-press the expression of mRNAs encoding key metabolic enzymes and hereby suppress hepat-ic lipogenesis and triglyceride synthesis, as well as secretion and accumulation in tissues (1).
It seems important that these findings are taken into account. Specific nutritional supple-ments should be used in combination with in-terferons as adjunctive therapy with the aim to improve both the early as well as the sustained virological response (1). On the other side, we don’t have enough information about the inter-actions at the molecular level. The modifying ef-fect of pharmaceuticals on the metabolism dur-ing the long-term therapy is still unexplained.
liver and nutrientsIn clinical and pharmaceutical populations´ studies the attention is often focused on the vi-rological aspect of chronicle hepatitis (22, 25). Understanding of its effect on the whole (iron) metabolism through the interaction of the vi-rus multiplication cycle with the given host’s genotype configuration, bearing unique genetic constitution, is crucial for right interpretation (24). Nowadays dominate clinical studies, taking into account mostly mis-nutritives (mainly alco-hol abuse) or another alimentary abnormalities (26). Such an approaches are not probatory for understanding of „standard“ interactions and cross-influencing among individual patient’s genotype, pathogen and nutrients.
Even more substantial premise is the fact, that also common human nutrition resources (crops and livestock) have certain degree of in-trinsic variability in their genetic information, which influences concentrations of broad com-pounds ranging from micronutrients to unsatu-rated fatty acids (27). This genetic diversity also effects on final human metabolical processes.
conclusionNutrigenomics investigates the genome-com-plex influences of nutrition and represents today one of the most developing branches of the medicine and life sciences. Nowadays, high expectations are still outmatching the real outcomes however; the results from the past decade have increased considerably our under-standing of the nutrients role in metabolic path-ways and regulation.
In the future, if we desire ever to think over medical applications of personalized nu-trigenomics, we must systematically focus our attitude from population studies of nutrition - genome interactions towards research based on the molecular basis, followed with potential modulating effect of infection agents within an organism having specific SNPs-configuration and normal nutritional habitudes. Only than the research of mis-nutrition influence can be worthwhile, and could give us relevant and reli-able data for successful medical praxis.

14
LIU Q, BENGMARK S, QU S. Nutrigenomics therapy of hepatisis C virus induced-hepatosteatosis. 1. BMC Gastroenterol. 2010; 10: 49.MÜLLER M, KERSTEN S. Nutrigenomics: goals and strategies. Nature Rev. Genet 2003; 4: 315-2. 322.KUSSMANN M, PANCHAUD A, AFFOLTER M. Proteomics in nutrition: status quo and outlook for 3. biomarkers and bioactives. J Proteome Res. 2010; 9 (10): 4876-4887.FARDET A. New hypotheses for the health-protective mechanisms of whole-grain cereals: what 4. is beyond fibre? Nutr Res Rev. 2010; 23 (1): 65-134.SIMOPOULOS AP. Genetic variants in the metabolism of omega-6 and omega-3 fatty acids: their 5. role in the determination of nutritional requirements and chronic disease risk.Exp Biol Med (Maywood). 2010; 235 (7): 785-795.CHAKRABARTI S, FREEDMAN JE. Review: Nutriceuticals as antithrombotic agents. Cardiovasc 6. Ther. 2010; 28 (4): 227-235.MATHERS JC, STRATHDEE G, RELTON CL. Induction of epigenetic alterations by dietary and other 7. environmental factors. Adv Genet. 2010; 71: 3-39.IZAR MCO. Nutrigenomics and nutrigenetics: Future perspectives for disease prevention. Int J 8. Atheroscler 2007; 2 (3): 203-206.DE MOURA EG, LISBOA PC, PASSOS MC. Neonatal programing of neuroimmunomodulation - 9. role of adipocyokines and neuropeptides. Neuroimmunomodulation 2008; 15 (3): 176-188.BUDGE GC, LILLYCROP KA, JACKSON AA. Nutrition in early life, and risk of cancer and metabolic 10. disease: alternative endings in an epigentic tale? Br J Nutr 2009; 101 (5): 619- 630.MCKAY JA, ADRIAENS ME, FORD D, RELTON CL, EVELO CT, MATHERS JC. Bioinformatic interroga-11. tion of expression array data to identify nutritionally regulated genes potentially modulated by DNA methylation. Genes Nutr 2008; 3 (3-4): 167-171.WANG J, WU G, ZHOU H, WANG F. Emerging technologies for amino acid nutrition research in 12. the post genome area. Amino Acids 2009; 37 (1): 177-186.MC-CABE-SELLERS B, LOVERA D, NUSS H, et al. Personalizing nutrigenomics research through 13. community based participatory research and omics technologies. OMICS 2008; 12 (4): 263-272.SACHIDANAMDAN R, WEISSMAN D, SCHMIDT SC, et al. A map of human genome sequence vari-14. ation containing 1.42 million single nucleotide polymorpisms. Nature 2001; 409: 928-933.LEHMANN U, WINGEN LU, BRAKENSIEK K, WEDEMEYER H, BECKER T et al. Epigenetic defects 15. of hepatocellular carcinoma are already found in non-neoplastic liver cells from patients with hereditary haemochromatosis. Hum Mol Genet. 2007; 16 (11): 1335-1342.BEUTLER E. The HFE Cys282Tyr mutation as a necessary but not sufficient cause of clinical he-16. reditary hemochromatosis. Blood 2003; 101 (9): 3347-3350.Rossi E, Jeffrey GP. Clinical penetrance of C282Y homozygous HFE haemochromatosis. Clin Bio-17. chem Rev 2004; 25 (3): 183-190.LEE P, RICE L, MCCARTHY JJ, BEUTLER E. Severe iron overload with a novel aminolevulate syn-18. thase mutation and hepatitis C ifection. A case report. Blood Cells Mol Dis 2009; 42 (1): 1-4.Jones DC, Young NT, Pigott C, Fuggle SV, Barnardo MC et al. Comperhensive hereditary hemo-19. chromatosis genotyping. Tissue Antigens 2002; 60 (6): 481-488.
Literature
15
KANG KH, YAMAMURA Y, CARLOS MP, KARVELAS N, KIM IS et al. Synthetic antigens representing 20. the antigenic variation of uman hepatitis C virus. Viral Immunol 2010; 23 (5): 497-508.Sersté T, Nkuize M, Moucari R, Van Gossum M, Reynders M et al. Metabolic disorders associated 21. with chronic hepatitis C: impact of genotype and ethnicity. Liver Int 2010; 30 (8): 1131-1136.HOOFNAGLE JH, WAHED AS, BROWN JR RS, HOWELL CD, BELLE SH, VIRAHEP-C STUDY GROUP. 22. Early changes in hepatitis C virus (HCV) levels in response to peginterferon and ribavirin treat-ment in patients with chronic HCV genotype 1 infection. J Infect Dis 2009; 199 (8): 1112-1120.FRACANZANI AL, FARGION S, STAZI MA, et al. Association between heterozygosity for HFE gene 23. mutations and hepatitis viruses in hepatocellular carcinoma. Blood Cells Mol Dis 2005; 35 (1): 27-32.VALENTI L, PULIXI EA, AROSIO P, et al. Relative contribution of iron genes, dysmetabolism and 24. hepatitis C virus (HCV) in the pathogenesis of altered iron regulation in HCV chronic hepatitis. Haematologica 2007; 92 (8): 1037-1042.PÁCAL L, HUSA P, ZNOJIL V, KANKOVÁ K. HFE C282Y gene variant is a risk factor for the progres-25. sion to decompensated liver disease in chronic viral hepatitis C subjects in the Czech population. Hepatol Res 2007; 37 (9): 740-747. SPANAGEL R, BARTSCH D, BRORS B, DAHMEN N, DEUSSING J et al. An integrated genome re-26. search network for studying the genetics of alcohol addiction. Addict Biol 2010; 15 (4): 369-379.TANIGUCHI M, UTSUGI T, OYAMA K, et al. Genotype of stearoyl- CoA desaturase si associated 27. with fatty acid composition in Japanese Black cattle. Mammalian genome 2004; 14: 142-148.
eva čerVeňanoVá, Gabriela oPršaloVá
nursing standards and intensive care
Standard is expertly, professionally agreed level of quality performance in nursing practice. The standard is determining the necessary standard, base level, which must be observed and provided in nursing practice. Intensive care is the highest form of care in a differentiated system of care. Its filling is the care of critically ill patients, in whom there is failure, failing or failed to feature one or more organ systems.
Abstract

16
Nursing Standard is an agreed level of profe- ssional quality, mandatory standards for
quality nursing care and provides an objec-tive assessment of the nursing care. (Kontrová, Záčeková, Block et al., 2005)
Understand, difficult theoretical training in nursing standards and at the same time the gradual implementation in nursing practice re-quires a creative team of nurses at each site.
SR National Quality Program for the years 2004 - 2008, the Slovak government adopted in its resolution no. 90/2003 of 24 September 2003, included in the main roles and the intro-duction of standardization in health care. For nursing as a distinct scientific discipline and for nurses in all positions to create a very challeng-ing task to develop and put into practice nurs-ing standards. Article Riadiacim become expert of the Ministry of Health nursing and working groups to individual departments, to develop individual procedures and submit them to the public on the application of nursing practice.
Gradually since 2003 in professional medical press had the opportunity to nurse throughout Slovakia to follow the basic theory of nursing standards, but also the framework due process standards of nursing performance.
Creative team led by Dr.. V. Block, PhDr. Ľ. Kontrová and Mgr. M. Záčeková issued in the 2005 publication of standards in nursing, which became the basic document for nurses in all clinical nursing specialties. Based on the pub-lished standards have gradually started to due process standards to implement in practice. The initial way is a difficult, thorny and not always find a positive response.
Education, permanent education of nurses, a prudent attitude, acquired skills and profes-sional skills manager at individual workplaces and brought their effect on the development of standards in nursing practice.
department intensive care – oaimAnaesthesiology and Intensive Medicine is an interdisciplinary department of health care. Ex-amines and provides anesthetic and intensive care. Cooperates with non-operational and op-erational departments of health care, in provid-ing comprehensive health care in the diagnosis and intensive care, the failure of vital organs or systems. (Concept). It deals with the diag-nosis, continuous monitoring and treatment of potentially curable patients, life threatening conditions, which require intensive and contin-uous medical and nursing care, which can not provide for standard units. Intensive Medicine focuses on the most serious respiratory and cardiovascular diseases. Intensive Care Medi-cine has evolved from the need of special care for patients with failing ventilation, based on the experience of post-operative ward. (Zadák, Havel, et al., 2007, p.2).
Intensive Care Medicine has enabled the survival and return to life to patients with re-versible impairment of vital functions. Intensive care units should be in a hospital located close to all acute-oriented workplaces - Operation Salam, emergency reception, coronary units, delivery room, X-ray work, given that any trans-port of critically ill is high risk.
nursing, standard, intensive care, quality
Key words

17
Intensive care is the highest form of care in a dif-ferentiated system of care. Its filling is the care of critically ill patients, in whom there is failure, failing or failed to feature one or more organ systems. To ensure intensive care is urgently needed the continued presence of a physician specialist in the department premises. Intensive care is a continuation of acute resuscitation, emergency hospital care or continuation of the previous standard of care in other disciplines.
Intensive care is
continuous monitoring of critically ill pa- J
tients at risk of organ system failurecontinuous monitoring and instrumental J
support of some organ systems until return of consciousness and protective reflexesintensive care and the risk of pathological J
newborns.
Acute intensive care be exercised in patients who are proven end-stage incurable disease. For admission of patients to pay certain criteria - “can not accept patients for too few patients this level of care or those who are terminally ill, that too much to them to help sebalepšia inten-sive care” (Black, Vítovec et al., 2000 , p.3).
Adoption should be directed to those pa-tients who can be expected to benefit intensive care provided to bridge the critical state.
Indications for hospitalization in intensive care wards:
patients who experienced failure of one or J
more of vitally important organs or systemspatients who have experienced chronic fail- J
ure to stabilize an acute deterioration, which threatens to acute failure or a failure has oc-curredpatients who are likely to further develop- J
ment of the disease leads to failure or failure of the body or bodies, or organ systempatients who are referred to as procedures, J
methods, technical equipment used in inten-sive care possible to prevent deterioration and failure of vital organs or systems
patients who experienced complications J
during the anesthesia, which may lead to the failure of important vital organs or systems, and thus a potential threat to their life or healthpatients who need specialized preoperative J
preparation necessary, to prevent the de-velopment of per and postoperative compli-cationspatients enrolled in the transplant program J
Reasons for termination of hospitalization in in-tensive care wards:
Improvement and stabilization of the pa- J
tientfinding goes out irreversible brain functions J
- the so-called brain death /for inclusion in the transplant program/. (Koncepcia zdra-vot-nej starostlivosti v odbore anestéziológia a intenzívna medicína, číslo 29589-1/2006 – OZSO)
Qualified nursing care:
“Intensive care provides detailed observation and treatment of patients with potentially cur-able conditions involving multiple organ failure or requiring mechanical ventilation is provided 24 - hours a day.” (Moore, 2004, p.7)
Since nurses are expected to follow training, assessment, identification of nursing diagnoses, goals, outcome criteria, interventions, imple-mentation and evaluation of nursing plan. Sister intensively monitor the patient’s condition, his behavior, do physical examinations and moni-toring instrumentation. Based on the findings, draws conclusions, assess the situation in which itself has to intervene and when to inform a doctor about an altered state. (Vörösová, 2005) Nursing care is focused on patient needs.
The role of nurses is:
make decisions quickly, accurately, often in- J
dependentlymake decisions that prevent complications J
perform accurately, skillfully intervention in J
case of sudden deterioration in conditionrespond quickly in a variety of emergencies J

18
carefully monitor every detail of patient J
careduring his practice to acquire specific train- J
ing for critically illwork with team J
work effectively in potentially stressful envi- J
ronmentsto provide holistic care with family members J
and relatives. (Moore, 2004, p.7)
standards in nursing“Nursing Standard is valid and agreed defini-tion of acceptable nursing care. The standard is the standard by which they can assess whether nursing care corresponds to the required level. Determines what is necessary and essential to the basic form desirable to provide quality nurs-ing care. “(Farkašová, 2005, s.196)
Quality of nursing care is the result of the creation and implementation of standards in practice. Štandard the sisters prijatá level of nursing care for a particular procedure or group that may be valid without set the criteria for the evaluation of effectiveness and quality. Before starting work as a nurse with the standards, they must understand they have a right atti-tude, and monitor its effectiveness. Not all nurs-es have the same procedure in use in nursing interventions, improvisation often departs from the quality and also the important role played by knowledge, attitudes and skills of nurses ob-tained permanent education, level of education and nursing practice.
History has been known since the first indi-cations of the standards of nursing founder Flor-ence Nightingale of 1859, from the book “Notes on Nursing, which focuses on environmental cleanliness, infection prevention and observa-tion of nursing care.
According Farkašová (2005) as important aspects of nursing care considered noise, air and clean environment, on time of administra-tion and quality of food. The issue focused on bedding bedding types and their distribution in space stations, the mattress and bed linen, other aspects were focused on personnel,
compliance with hygiene and infection control. Theoretically developed and practically tested standards first emerged in the U.S. later in the developed Western countries. American Nurses Association in 1973 prepared and adopted, the standards, which in turn affect the level of nurs-ing care.
American Nurses Association in 1975, in a model of quality assurance, quality assurance describes the process as beginning with steps to identify values and define standards based on social, professional and scientific assumptions. (Schroeder, 1991) According to Terry Fulmer, standards reflect a vision of professional prac-tice, not simply the identification of tasks, steps and goals. Can not be copied from the text and applied to any organization, group of nurses and patient populations. Reflect the unique needs of groups of patients, providing nursing care, possibilities and resources of professionals, who work with them.
Standards reflect the values and respect. The practice carried out by professional nurses, must play a major role in creating a view, so that patients can achieve positive results. Standards of nursing practice, describes the arrangement between the mechanisms that support nursing care (structural standards), process and con-tent of nursing care (due process standards), or patient outcomes resulting in nursing care (standard result), or any combination of those. (Fulmer, T. et al.2001, p.2)
Creating standards is a first step in the con-figuration standards and quality management system. (Stevens, 1995) Standards must be de-termined as a method for inplementáciu levied, collected and analyzed information and feed-back continuous change must be made if the results differ from those objectives. (Stevens Barnum, 1995)
Standards of care are detailed directive, which show the predicted care, which is indicat-ed in a specific situation, they would display care, entitlement to which nurses are responsible and not the ideal level of care. (Moyet, 2008)

19
High quality in the system of nursing can be achieved by influencing thinking and behavior of all those who provide nursing care and to ensure the provision of nursing care methods and procedures in accordance with current and credible (scientifically) a source of knowledge. This is the main reason for the standardization of entry into the Slovak health care. (National Quality Program of the Slovak Republic, 2004-2008, Ministry of Health)
conclusionNursing standards should be developed, change to form an integrated system that ensures quality services. Be based on common results of science, research, technology and nursing practice.Certified nursing standards in practice at the department of anesthesia and intensive care nurses to help in the continuous practice, showing how to properly proceed with individ-ual performance to achieve the desired quality and effect.
CARPENITO-MOYET, L.J. 2008. Nursing care plans & documentation: nursing diagnoses 1. and collaborative problems, Nursing Care Plans and Documentation, Lippincott Williams & Wilkins, 2008, s. 814, ISBN 0781770645, 9780781770644ČERNÝ, V., VÍTOVEC, J. et al. 2000. Intenzivní medicína. Galen. 2000. ISBN 80-7262-042-82. FARKAŠOVÁ, D. 2005. Ošetrovateľstvo – teória. Martin, Osveta, 2005.215 s. ISBN 80-8063-3. 182-4FULMER, T. T., FOREMAN, M. D., WALKER, M. K. 2001. Critical care nursing of the elderly, 4. Springer series on geriatric nursing, Mactips Series, Springer Publishing Company, 2001, ISBN 0826114091, 9780826114099Koncepcia zdravotnej starostlivosti v odbore anestéziológia a intenzívna medicína, číslo 5. 29589-1/2006 –OZSOKONTROVÁ,Ľ., BORBÉLYOVÁ,V. et al.:2006. Ošetrovateľské štandardy v nefrológii, , Osveta, 6. Martin, 2006, 1.vyd., 215 s. ISBN 80-8063-237-5MOORE, T., WOODROW, P. 2004. High dependancy nursing care. Observation Intervention 7. Support. Routledge, 2004. 400s., ISBN 04- 152- 6755- 2Národný program kvality Slovenskej republiky na roky 2004-2008, MZ SR8. SCHROEDER, P. S.1991 Approaches to nursing standards, The Encyclopedia of nurs-9. ing care quality – zväzok 2, Jones & Bartlett Publishers, 1991, s.208 , ISBN 083420214X, 9780834202146STEVENS BARNUM, B., KERFOOT, K. M. 1995, The nurse as executive Jones & Bartlett Publish-10. ers, s. 356 , ISBN 0834205718, 9780834205710VÖRÖSOVÁ, G. 2005. Interné ošetrovateľstvo. Martin: Osveta, 2005. 198 s. ISBN 80-8063-11. 192-1ZADÁK,Z., HAVEL, E. et al. 2007. Intenzivní medicína na principech vnitřního lékařství. Grada 12. Publishing. 2007. ISBN 978-80-247-2099-9.
Literature

20
eva čerVeňanoVá
study oF nursing the university igbinedion okada, benin city in nigeria
Nursing is as old as human existence as mother cared for their babies and people
cared for their sick and injured ones. But, pro-fessional nursing practice began with the Lady with the lamp-the legendary of nursing – Flor-ence Nightingale. She initiated the need for formal education for nurses and started the first school of nursing. In fact , Florence Night-ingale once stated, “any system that does not march shall not endure “Nursing education all over the world and in Nigeria had experienced phenomenal development and today in Nigeria, University – based education for nurses is the acceptable and approved trend by both the Na-tional Universities Commission and the Nursing
and Midwifery Counsil of Nigeria. Therefore, for nursing to remain relevant on the globally advancing medical technology, knowledge ex-plosion, university-based nursing education is imperative. In response to this challenge and in consonance with the vision of Igbinedion Uni-versity (Academic Excellence) this department was started in 2005/2006 session. (Oba Okun-ade Sijuwade, 2007/2008, 3)
By the major majority of the population lives in Africa is Nigeria’s daily struggle for survival. Nursing and Nursing also has an irreplaceable role in the hospital, but also community care. During his private residence on the African con-
Nursing is a young scientific discipline of education and unification of people in this field of study is currently the main focus of the Heads of Department in the world.
Nursing education is also made to this country after graduating from high schools to state and pri-vate schools for nurses, but also on the university campus.
university, nursing, nursing education, Nigeria
Key words
Abstract

21
tinent, I had the opportunity to compare nursing education in Nigeria and for us. (Červenanová, E.,2010)
nigeriaThe State situated on the African continent, full name for the Federal Republic of Nigeria - Federal Republic of Nigeria. The total area is 923,768 km ².
The largest city is the former capital Lagos. The capital city is Abuja. Population of the coun-try in 2009 assumed 149 million. The official lan-guage is English and other languages are harm Hauls, Yoruba, Ibovia, Fulani and Kanuri, ie lan-guages according to racial and ethnic composi-tion.
Benin-City is a modern city located in the southwestern part of the country, the Niger es-tuary into the Gulf of Guinea. High speed grows and becomes a bustling city. Falls within the ad-ministrative region of Edo. The tradition of cast-ing bronze sculptures are preserved in “street artists”. The museum, which was restored by UNESCO, unfortunately, keeps only a fraction of the artistic treasures that during the turbulent political twists in the country lost in all corners of the world. Here is the Igbinedion University Okada, the first private university in Nigeria. (Červenanová, E., 2010)
igbinedion university, okada, benin cityIgbinedion University Okada (IUO) is the first private university with a long tradition in the city of Benin City, Nigeria. 16. May 1999 Federal Government of Nigeria granted a “Certificate No.001”, namely a certificate of competency and so became a fully fledged University in Ni-geria.
Founded as a center of excellence and qual-ity. Its vision is to become the leading hub for knowledge production and human capital.
Located in Okada, Wonderland, and togeth-er with the world’s academics, support staff, re-search institutions, teaching hospital business,
information technology center for solutions applicable in telemedicine and teleconferenc-ing. Together with the students spontaneously organized IUO offers the right atmosphere for human development, as well as innovation, pro-ductivity and sustained scholarship.
IUO is truly cosmopolitan university employ-ees and students from 36 states (states) of Ni-geria, but also other parts of the world. The Uni-versity currently attracts prospective students to its 7 faculties:
Arts and Social Sciences J
Business and Management Studies J
Oba Erediauwa Collage of Law J
Oba Okunade Sijuwade Collage of Health Sci- J
encesNatural and Applied Sciences J
School of Diplomacy & Interantional Secu- J
rity StudiesGeneral Abdulsalami Abubakar Collage of J
Engineering
Igbinedion University Okada is recognized as one of the leading, scientific research and edu-cational institutions not only in Africa but also worldwide.
philosophyThe philosophy of the Department of Nursing Science, of School of Clinical Medicine of Igbin-edion University, Okada, is in consonance with the philosophy of education in Nigeria and that of Igbinedion University:
The nursing faculty believes that the De-1. partment of Nursing Science should have the greatest concern for service through high standards of scholarship and personal character. The ultimate purpose being the advancement of public welfare and culture through wider and deeper knowledge, finer skills, and broader appreciation of human values and the African cultural heritage.The faculty believes that preparation for 2. Professional nursing should consist of lib-eral and Professional education leading to a bachelor’s degree, and should take place

22
within a university setting. Such a nursing program should be an integral part of the university education programs, utilizing and supporting all the facilities and activities of the institution.The Nursing profession believes that man is 3. a biopsychosocial being and his needs are the focus of all Nursing activists. Man is a member of family and families make up the the communities.The faculty believes nursing is a process 4. of interaction, which aims to assist the in-dividual, family and community in main-taining or establishing an optimal level of healthy living. The nurse is an inherent part of the transaction, which helps the individ-ual, family and community to modify their patterns of daily living according to their requirement. The nurse does this through the use of the analytic-synthetic process, the applicant of technical skills and feeling responses, and in cooperation with other disciplines. The faculty believes that a health team in 5. which the individual, the family and the community play significant roles is the most effective approach to promotion, mainte-nance and restoration of health.It is believed that a professional nursing pro-6. gramme should incorporate knowledge from the arts, sciences, humanities and nursing in order to ensure sound Professional train-ing, to stimulate research and continued acquisition of new knowledge, to promote individual self development and to advance public welfare. Therefore, there should be an orderly progression in learning. Professional Nursing education is built upon 7. the theoretical base that seeks to develop continually self-directed practitioners who will advance and test knowledge on which practice is based. Current health care de-mands require and innovative approach in professional preparation and a curriculum that is responsive to the needs of the so-ciety. (Oba Okunade Sijuwade, 2007/2008, 3-5)
curriculum objectives:By the end of the academic programme in Nurs-ing, the undergraduate is expected to:
Integrate concepts and principles form the 1. biological, social, physical and nursing sci-ences in the provision of comprehensive nursing care.Function effectively independently and in 2. collaboration with other members of health and related sectors.Utilize the nursing process and other tools of 3. nursing in assisting individuals, families and groups adapt to changing health needs.Formulate a theoretical framework that is 4. applicable to the nursing care of clients at the three levels of health care by using ten-ets from relevant sciences.Incorporate the medical plan of care into 5. nursing activities to achieve the objectives of the dependent, interdependent and in-dependent functions of the nurse.Contribute to the improvement of nursing 6. practice by participating in interdisciplinary research, utilizing the research process and publishing research findings in nursing prac-tice situations.Appreciate the influence of culture and hab-7. its on the health status of clients and utilize this knowledge in developing clinical skills and teaching.
Utilize the principles of management in the ad-ministration of health care facilities and person-nel. (Oba Okunade Sijuwade, 2007/2008, 6-7)
conclusionVisiting the University and meeting with heads of universities will forever remain an unforget-table experience. The possibility to exchange knowledge and experience is a great enrich-ment for everyone, without distinction of color, status or nationality. Education in Nursing, or Af-rica or Europe prepares nurses for their future, and challenging profession, which for many be-comes a life mission.

23
OBA OKUNADE SIJUWADE1. , 2007/2008, Bachelor of nursing science [B.N.SC.] College of health sciences, School of clinical medicine, Departmental of nursing, Departmental handbook, Hand book for 2007/2008 academic sessionČERVENANOVÁ, 2. E., 2010, Sestry a bratia z Nigérie In.: Sestra a lekár v praxi, Journal for nurses, doctors and other health workers, roč.IX, č.9-10/2010, ISSN 1335-9444ČERVENANOVÁ,E3. .,2010, Nigéria, In.: TnU Trendy, Journal about the life of students and teach-ers Trencin University of A. Dubcek, roč.8./č.2
Literature
Miriama ZáhuMenSKá, Zdenka KrajčoVičoVá, Vladimír Meluš
eFFectiveness oF psa assay in prostate cancer screening
Prostatic specific antigen (PSA) is a laboratory parameter widely used in the screening of prostate carcinoma (PCA) and to differentiate PCA from benign prostatic hyperplasia (BPH). We examined 16 patients with PCA and 105 patients with BPH and compared these to 24 controls. Our results indicated relatively high test specificity (0.83; 95% CI: 0.62 – 0.95) for both diagnoses, but low sen-sitivity (0.25 for PCA; 95% CI: 0.07-0.52 and 0.15 for BPH 95% CI: 0.09-0.23). Differences in the age of the groups were statistically significant (controls: M = 57.16; SD = 11.04; BPH patients: M = 63.13; SD = 10.53; PCA patients: M = 74.94; SD = 8.24; Kruskal-Wallis analysis p < 0.001), but the concentrations of PSA showed high variability. For this reason, the differences within groups were non-significant (Kruskal-Wallis analysis p = 0.83). Large variability of the PSA concentrations in our examined groups suggest a reduced effectiveness of the actual diagnostic system.
Abstract

24
Together with the human life extending and steadily rising of life expectancy we can
see an increasing frequency of diseases asso-ciated with higher age. Prostate diseases such benign prostatic hyperplasia (BPH) or prostate carcinoma (PCA) are typical examples of diag-noses among aging men (1, 2). For this reason, PCA screening has become an important test for men over 55 years of age (3). The benefits of population-based prostate cancer screening are the detection of clinically significant pros-tate cancers at an early (still curable) stage and the subsequent reduction of prostate cancer-specific mortality (4).
Prostate specific antigen (PSA) is a serine protease that is exclusively produced in the prostate, and its detection is the only labora-tory test available for the screening of men for PCA (5). PSA is a polypeptide comprised of 240 amino acids with a molecular weight of 34 kDA. Its enzymatic activity is similar to that of chy-motrypsin. PSA is mainly inactivated in the body by binding to alpha-1-antichymotrypsin, and the half-life of PSA is approximately two days. Phys-iologically PSA is present in the semen plasma and serves to facilitate the movement of sper-matozoa (6). The ratio of free to total PSA can be used to discriminate between cases of BPH and PCA, with ratios greater than 0.15 being in-dicative of BPH. However, the PSA ratio is only a reliable indicator in older individuals presenting symptoms of or having a predisposition to PCA, and it is not a reliable indicator in asymptomatic individuals (7).
aimThe objective of our study was to verify the ef-fectiveness of the PSA assay in the local Cau-casian population of the laboratory’s tributary area.
material and methodsThe data of 145 male patients, examined for PSA within a period of six months, were extracted from the laboratory database. Of these, 105 pa-tients had been diagnosed with BPH, and 24 had been diagnosed with PCA. A control group was formed from 24 healthy individuals. All items obtained from patients were de-identified to ensure their anonymity.
PSA was routinely analysed using the ECLIA method according to the standard operating procedure of the laboratory. Reference range was 0.00 – 3.00 μg/L. Physicians were required to obtain informed consent from all patients. Potential sources of false results (obstipation, catheterization, prostate examination, etc.) were also taken into account.
Descriptive statistics is given by the arith-metical mean, standard deviation, number of individuals and median. The non-parametrical Kruskal-Wallis analysis was used for compar-ing the three groups. The differences between individual pairs of groups were tested with the Dunn’s post test. Individual categories were compared with the contingency tables, based on the Fisher’s exact test, followed by the calcu-lation of sensitivity and specificity.
prostatic specific antigen, benign prostatic hyperplasia, prostate cancer, assay effectivity
Key words
25
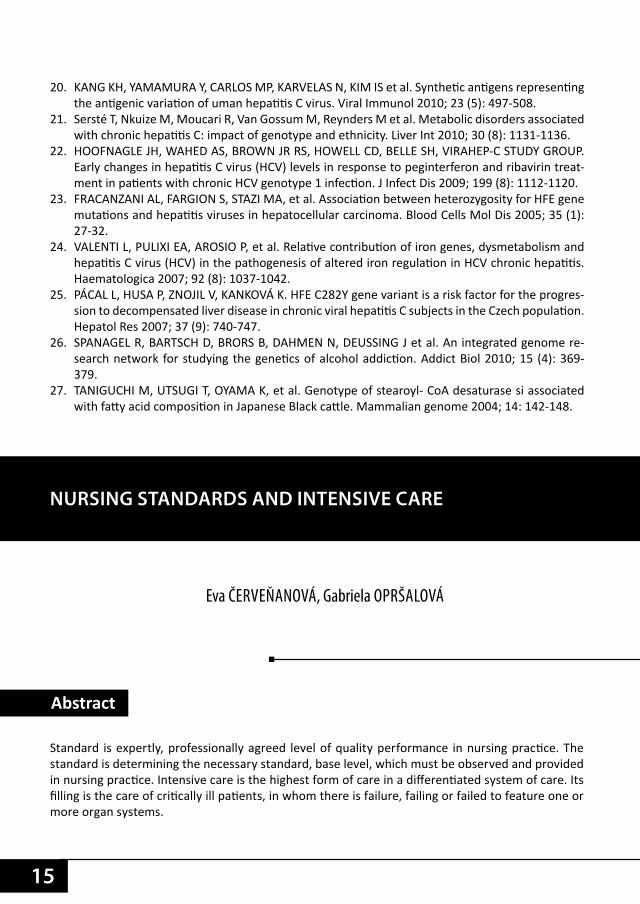
results and discussionTable 1 shows the basic characteristics of the three tested groups of male patients: age and PSA. We can see statistically significant differ-ences between the mean ages of individual groups (p < 0.001).
Dunn’s post test revealed significant differ-ences in age between controls and BPH patients (p < 0.05). Even more significant were the differ-ences between controls and PCA patients (p < 0.001; Dunn’s test) as well as that between PCA and BPH patients (p < 0.01; Dunn’s test) (Table 1, Graph 1). We can conclude, that average age with higher incidency of BPH is around 65th year of age. For man in our population it needs next ten years to reach the average age of patients with PCA.
Although BPH and PCA patients with appear to have elevated PSA values compared to con-trols (Table 1), these differences were found to
be not statistically significant (p = 0.83) due to large variability in PSA values. When reading the PSA values in Table 1, we can see that only controls have a SD less than the mean; both BPH and PCA patients have a SD greater than the mean. PCA patients have a mean PSA concen-tration of 8.67 μg/L but with a SD of 24.82 μg/L because this group is the most heterogenous and contains individuals before treatment, as well as those after surgical and oncological ther-apy (Graph 2).
We also tried to assess the sensitivity and specificity of the PSA testing. As can ben seen in Table 2, there are no significant differences be-tween PCA patients and controls in individuals with a PSA > 3 μg/L (p = 0.69). The sensitivity is low with the value of 0.25 (95% CI: 0.07 – 0.52), specificity is higher (0.83; 95% CI: 0.62 – 0.95). The positive predictive value was 0.5 (95% CI: 0.16-0.84) while the negative predictive value was 0.63 (95% CI: 0.44 - 0.79).
Parameter Descriptive Statistics
Controls BPH patients PCA patients p
AGE n 24 105 16 <0.001
M 57.16 64.16 74.94
SD 11.04 10.53 8.24
median 55.50 65.00 77.00
PSA n 24 105 16 0.83
M 1.61 2.1 8.67
SD 1.39 2.75 24.82
median 0.98 1.16 1.38
Legend: n - number of individuals, M - arithmetical mean, SD - standard deviation, p - significance value of the Kruskal-Wallis analysis results, BPH - benign prostatic hyperplasia, PCA – prostate carcinoma, PSA - prostate specific antigen.
Tab. 1: Examined parameters in male patients
Tab. 2: Comparison of PCA patients with control group
Parameters PCA patients Controls Total
PSA>3μg/L 4 4 8
PSA<3μg/L 12 20 32
Total 16 24 40
Fisher’s exact test p = 0.69

26
Graph 1: Mean age of tested groups
Graph 2: PSA in tested groups

27
WEI JT, CALHOUN E, JACOBSEN SJ. Urologic diseases in America project: benign prostatic neo-1. plasia. J Urol 2005; 173: 1256-1261GAT Y, GORNISH M, HEIBLUM M, JOSHUA J. Reversal of benign prostate hyperplasia by selec-2. tive occlusion of impaired venous drainage in the male reproductive system: novel mecha-nism, new treatment. Andrologia 2008; 40 (5): 273 -281SLOBODNÍKOVÁ J. Prevencia onkologických ochorení. In Kaušitz J, Altaner Č. Onkológia. Veda, 3. SAV, 2003; 51–57.VAN VUGT HA, BANGMA CH, ROOBOL MJ. Should prostate-specific antigen screening be of-4. fered to asymptomatic men? Expert Rev Anticancer Ther. 2010;10(7):1043-1053.
Literature
Tab. 3: Comparison of BPH patients with control group
Parameters PCA patients Controls Total
PSA>3μg/L 16 4 20
PSA<3μg/L 90 20 110
Total 106 24 130
Fisher’s exact test p = 0.76
In the case of comparison between BPH patients and controls are results similar (Table 3). The sensitivity of the PSA test was even lower than that shown the in previous table, with a value of 0.15 (95% CI: 0.09-0.23), while test specificity was almost equal (0.83; 95% CI: 0.63 – 0.95). The positive predictive value was 0.80 (95% CI: 0.56 - 0.94) while the negative predictive value was 0.18 (95% CI: 0.11-0.27).
conclusionMeasurement of serum PSA levels is useful in detecting early prostate cancer but the inter-pretation of the laboratory assay is difficult since it is specific for prostate tissue and cellular growth, but not for PCA (5). Large variability of PSA concentrations in our examinated groups suggest a reduced effectiveness of the actual diagnostic system.
PSA screening has impacted the detection of PCA and is directly responsible for a dramatic decrease in stage at diagnosis. In the absence of
more accurate and reliable tissue or blood bi-omarkers, Gleason score and stage at the time of diagnosis remain the main methods of pre-dictive prognosis. Despite extensive research ef-forts, to date very few biomarkers of PCA have been introduced in clinical practice. Even screen-ing with PSA has recently been questioned (8). Our results confirmed that PSA screening is as-sociated with a high rate of overdiagnosis and overtreatment (9). To improve the detection of clinically significant cancers, several auxiliary clinical and imaging tools can be used. The ab-solute PSA value can be complemented with pa-rameters such as PSA velocity, PSA density and free/total PSA (4, 10). Further improvement can be achieved with the digitalization of patients’ data and increasing their online accessibility in the future e-health projects.

28
MENER DJ. Prostate specific antigen reduction following statin therapy: Mechanism of action 5. and review of the literature. IUBMB Life. 2010;62(8):584-590.TOSOIAN J, LOEB S. PSA and beyond: the past, present, and future of investigative biomarkers 6. for prostate cancer. ScientificWorldJournal. 2010;10:1919-1931.KELL JS. Prostate-specific antigen tests and prostate cancer screening: an update for primary 7. care physicians. Can J Urol. 2010;17 Suppl 1:18-25.FIORENTINO M, CAPIZZI E, LODA M. Blood and tissue biomarkers in prostate cancer: state of 8. the art. Urol Clin North Am. 2010;37(1):131-1411HUMPHREY PA, ANDRIOLE GL. Prostate cancer diagnosis. Mo Med. 2010;107(2):107-112. 9. DE VISSCHERE P, OOSTERLINCK W, DE MEERLEER G, VILLEIRS G. Clinical and imaging tools in 10. the early diagnosis of prostate cancer, a review. JBR-BTR. 2010;93(2):62-70.
ján bieliK, Milan hliSta, Slavomír černoK, Miroslav šorF
crohn´s disease and Quality oF liFe
A survey of the available literature showed that no paper focusing on the health related quality of life of patients with Crohn s disease from Central and Eastern Europe has been published as yet. Methods: Health related quality of life was studied in a group of 60 patients with Crohn s disease using the „Inflammatory Bowel Disease Questionnaire“ (IBDQ, Guyatt,1989). The following para-metres were evaluated with regard to quality of life: Age, - Marital status, - Religion, - Duration of disease, - Course of disease, - Extraintestinal symptoms, - Histological evidence, - Locality, - Drug treatment, - Surgery, - CDAI, - Socioeconomic status, - Disability, - Future expectations. Results: The average value of IBDQ-measured health related quality of life for the group was 174.4 points (170.5 and 179.1 points for females and males, respectively). The most important results were ducement-ed in these parametres: Duration of the disase: a, up to 3 y. – 181.2; b, between 3 and 6 y. – 182.6; c, more than 6 y. – 160.9. CDAI: a, up to 150 (average 55.7) – 179.4; b, 151 and more (average 213) – 152.1. Surgery: a, no surgery – 179.8; b, undergoing surgery – 165.6; ba, one surgery – 178.1; bb, two and more interventions – 137.3. Faith: a, non-believers – 191.1; b, believers – 170.2; ba, mild believers – 182.9; bb, moderate believers – 163.4; bc, strong believers – 169.5. Conclusions: The following parameters were found to have a significant (at the p<0.05 level) impact on the health related quality of life: duration of the disease, - multiple surgical interventions, - CDAI and faith.
Abstract

29
Crohn s disease, quality of life, inflammatory bowel diseases, health-related quality of life
Key words
Quality assessment of the health condition of human individuals started to get increas-
ingly to the foreground since the 1980s. This was due on the one hand to longer duration of chronic diseases connected with extended average life expectancy (1). In spite of the ini-tial problems concerning the application of ap-propriate and reliable measurement methods quality of life started to be used as an aspect of the assessment of the health care under vari-ous health care programmes (2). The focus was shifting towards specific illnesses in the subse-quent years. Among the diseases of the diges-tive tract, non-specific inflammatory diseases, and in particular Crohn s disease and ulcerative colitis, gastro-oesophageal reflux disease, ma-lignant diseases of the digestive tract and liver diseases got into the centre of attention (3).
Attention has been paid to quality of life of patients with Crohn s disease since effectively the early days of this trend becoming apparent. One of the first papers in this respect studied the quality of life in patients with Crohn s dis-ease who underwent surgery (4). The aim of the present work has been to identify the overall level of quality of life of patients in Slovakia suf-fering from Crohn s disease, identification of the relationships of the various factors to quality of life, and last but not least, verification of the use of IBDQ in the conditions of Slovakia.
patients and methodspatientsThe group of patients comprised 60 (81%) out of the total 74 patients with Crohn s disease regis-tered with 2 offices of gastroenterology in Dis-
trict Trenčín (population 115,000) and District Nové Mesto nad Váhom (population 65,000). Fourteen patients could not be included into the study because of time constraints on the part of the gastro-enterologist who registered and followed up the patients. There were 33 males (average age 44.9 years) and 27 females (average age 48.6 years). The average duration of the disease was 8.7 years - 7.5 and 10.1 years for females and males, respectively. In 45 cases (75%), Crohn s disease was confirmed histologi-cally; the histological diagnosis was non-spe-cific in 11 cases (18.3%). One case (1.7%) was associated with a negative finding. No histology was performed in 3 cases (5%). In all the cases, the clinical picture and the course of the disease suggested Crohn s disease. The sites involved were as follows: ileum- 40x, caecum 18x, as-cendent colon- 10x, hepatic flexure- 7x, trans-versal colon - 19x, lienal flexure- 9x, descendent colon- 10x, sigma- 29x, rectum- 17x. The phar-macotherapeutical profile of the patients was as follows: a, causal monotherapy (5- ASA) - 21 patients; b, combination causal therapy (5-ASA + corticosteroids, 5-ASA + corticosteroids + en-tizol, 5- ASA + corticosteroids + entizol + immu-nosuppressants, 5-ASA + immunosuppressants; 5-ASA + corticosteroids + immunosuppres-sants, corticosteroids + entizol) – 27 patients; c, combination causal and adjuvant therapy – 7 patients; d, adjuvant or no therapy- 5 patients. There were 21 patients in the group with a mild course of the disease, 13 in the group of moder-ate course and 26 patients with a severe course of the disease. Extraintestinal symptoms were experienced by 23 patients. Twenty-three pa-tients underwent surgery, 7 patients underwent

30
multiple surgical interventions. Table 1 shows an overview of the patient group by parameters studied.
methodsA specific questionnaire focusing on the evalu-ation of quality of life in patients with inflam-matory bowel diseases, IBDQ, was used in the original form comprising 32 items. The replies were evaluated using the 7-point Likert scale (5). IBDQ is oriented towards the evaluation of the perceived quality of life in 4 areas: intestinal symptoms – 10 items, general symptoms- items, emotional functions – 12 items, and social func-tions- 5 items. IBDQ was chosen because its translations have proven useful (sometimes with negligible modifications) in various coun-tries, including the Netherlands (6), Germany (7), the United Kingdom (8), Greece (9,) as well as South Korea (10).
The patients received information from their doctor on the purpose of the study. Af-ter giving their consent with the inclusion in the study, the patients received explanation as to how to work with the questionnaire. Complet-ed questionnaires were checked by the doctor. If s ome items in the questionnaire were miss-ing, the doctor asked the patient and filled in the respective answers if the patient agreed. Patient s opinion was respected if refusing to fill in certain items. A total of 1,824 replies went into the evaluation stage (99.0 %).
The clinical disease activity index, CDAI, was evaluated using the questionnaire according to Best (11).
Quality of life was evaluated with respect to the following parameters: A.- Group of ba-sic data: - sex, - age, -marital status. B. Group of clinical data: - duration of disease – course of disease – clinical disease activity index – site of involvement – histological finding – extrain-testinal symptoms – type of health care – char-acter of pharmacotherapy. C. Group of socio-economic data: - ability to undertake working activities - socio-economic status. D. Group of
mental data: - faith – nature of future expecta-tions. The above mentioned structure and the respective results IBDQ of CDAI are shown in Table 2.
The non-parametric Kruskal-Wallis´ test was used for statistical evaluation. Two-sample test was used in some cases. The Kruskall-Wallis´ test was based on comparison of median val-ues. Average, minimum and maximum values, top and bottom quartils and standard devia-tions were calculated for the various levels of the factors studied. The value of p < 0.05 was taken as the significance level of differences.
The study followed the recommendations of the Helsinki II Declaration. Both the study design and the protocol were approved by the Hospital Ethics Commission.
resultsThe average value of quality of life for the whole group was 174.4 points, the corresponding values for females and males being 170.5 and 179.1 points respectively. The average value of CDAI for the whole group was 84.5 points; for patients showing up to 150 points, the aver-age value was 55.7, and for those with values exceeding 150.0 points the average value was 213.0 points. Table 1 shows the results ob-tained for all the parameters studied.
The overall evaluation confirmed the logi-cal assumption that there is a certain indirect correlation between CDAI and quality of life (p –0.008), and that among the other parameters it is repeated surgical interventions only that have a significant effect on the quality of life (p -0.0146). From among the other parame-ters studied, duration of disease of more than 6 years and faith were under the significance level of p < 0.05 (p- 0.038 and p- 0.0163, respec-tively). Faith was only evaluated with respect to claiming no faith, because of the low numbers of respondents in the group of so-called strong believers (2).
As a certain surprise came the observation that neither the course of the disease, the pres-ence of extraintestinal symptoms or the meth-

31
od of conservative therapy showed any signifi-cant effect on the quality of life. Neither the site of involvement, even in the case of pancolitic involvement, had any effect. These results in-directly suggest that the patients were receiv-ing adequate therapy in dependence upon their clinical condition. There was no significant dif-ference between cases in whom the histological finding specifically confirmed Crohn s disease and those whose histological finding was non-specific or those who had no report in their doc-umentation on such an examination or those in whom no such examination had ever been per-formed.
The socio-economic status, the degree of the limitation of working activities or the char-acter of future expectations showed no impact on the quality of life.
discussionEpidemiologic data characterize Crohn s disease as a disease with annual incidencies ranging between 1 and 10 per 100,000, depending on the geographical localisation (12). The values for European countries are as follows: Belgium 5.5 (13), France (14), Norway 5.3 (15), Sweden between 5 and 7 (16), Italy between 1.9 and 6.6 (17), and/or 2.8 after gender- and age-ad-justments (18). The incidencies show a relative long-term stability (16). In Slovakia, the approx-imative incidence of Crohn s disease is 7.4 per 100,000 per year (19).
As a rule, health-related quality of life (HR-QoL) studies use standardized questionnaries. MOS 36 and/or its abbreviated version MOS SF-36 are examples of generally oriented ac-cepted questionnaire that have proven accept-able under a variety of conditions as well as for the general population (20). The above men-tioned Guyatt s IBDQ is an example of a ques-tionnaire specifically focusing on non-specific inflammatory bowel diseases; it seems to be the most frequently used specific questionnaire at present (5). Using IBDQ, the range of values assigned to quality of life is between 32 and 224
points; the scores for patients in remission usu-ally reach more than 170 points (5). IBDQ is a valid, reliable method to evaluate significant changes in the health condition of patients. It measures the treatment efficacy and can also be used in clinical trials (21). The reliability of the method could also be confirmed in comparing the results of evaluation made by qualified nurs-es and the patients themselves. This applied to both the overall results and those relating to the 4 above mentioned partial areas (22). IBDQ has proven adequate with respect to also relatively stable outpatients (23).
Also, IBDQ has been used in studies that evaluated efficacy and tolerance of drugs, such as 5-ASA (24), cyclosporine (25), oral budesonide (26) or methotrexate (27). It may also be useful in testing efficacies of new forms of medication: e.g., budesonide released in the ileum showed a significant change in the IBDQ scores as early as after 2 weeks of administration, both in doses of 9 mg and 15 mg budesonide (28).
The original authors of IBDQ have not at-tempted to consider the results obtained us-ing it as absolute, even if the above mentioned works have confirmed that the questionnaire is suitable for wide-spread use. The differences observed may be due to the age structure of the patient groups, coincident occurrence of other diseases, various frequencies of active and in-active diseases, differences in the approach to health care, differences in socio-economic sta-tus, etc. (29). A better awareness of the disease, i.e. a higher degree of patient s education in the same environment had however no effect on the level of the perceived quality of life (30).
Frequently, also the questionnaire monitor-ing the disease activity index (CDAI) is used in parallel with IBDQ. Values of up to 150 points are typical of remission, 150 points suggest ac-tive disease, and levels above 450 points are typical of extremely severe disease (11).
A high correlation between CDAI and IBDQ has been illustrated by surveys which reported IBDQ and CDAI values of 169 and 133 points,

32
respectively, for stable patients with Crohn s disease (21), with values of 131 and 293points, respectively for active ileocolic Crohn s disease (24).
Differences between results obtained by IBDQ and/or its modified version may also be evaluated using the so-called delta score. The differences observed in this score were most pronounced in patients during recurrence of the disease (0.9), being 0.3 during relapse. These dif-ferences were even smaller than expected. On the other hand, disease activity correlated with quality of life (31).
The results of a survey focusing on the qual-ity of life after surgery confirmed the need of ag-gressive therapy in selected patients with Crohn s disease: after resection, the health related qual-ity of life almost achieved the level of that in the general population, and remained there through-out the period of monitoring of 6 years (32).
conclusionsOur study confirmed the usefulness of the trans-lated version of IBDQ in the conditions of the public health system of the Slovak Republic. The questionnaire thus may be used as a proven com-ponent of projects or studies focusing on non-specific inflammatory bowel diseases.
A significant effect on the health related qual-ity of life of patients with Crohn s disease could be demonstrated with respect to disease activity, repeated surgical interventions and duration of the disease for more than 6 years. It is difficult to interprete the relationship between faith and quality of life – it would require a separate study. The other parameters studied could not be dem-onstrated to impact upon the health related quality of life, and this may point to a good diag-nostic, monitoring and therapeutical approach to patients with Crohn s disease.
Faith
Non-believers Believers (174,4)
191.1“Mild” believers “Moderate” believers “Strong” believers
182.9 163.4 169.5
Involvement site
Right side Left side Mixed Pancolitis
174.2 174.8 173.8 174.6
Drug treatment
Causal monotherapy Combination causal Combination causal and adjuvant th.
Adjuvant only or no therapy
170,0 167.0 176.6 187.3
Tab. 1: Basic characteristics of patient´s group

33
Age
up to 30 yrs. between 31 and 60 yrs. 61 and more yrs.
181.8 175.1 166.4
Marital status
Married Divorced Single
176.2 147.0 179.4
Duration of disease
Up to 3 yrs. Between 3 and 6 yrs. More than 6 yrs.
181.2 182.6 160.9
Course of disease
Mild Moderate Severe
181.0 176.8 167.8
Surgery
Without surgery With surgery One surgery
179.8 165.6 178.2
Socio - economic status
Poor Middle Rich
168.6 179.6 168.8
Disability
None Temporary inability to work Disability
176.4 176.1 153.4
Future expectations
Rather negative Negative and positive Rather positive
159.3 167.3 182.2
Extraintestinal symptoms
Present Absent
167.5 178.8
Histologic evidence
Positive Negative/non-C17specific
171.7 182.3
CDAI
Up to 150 151 or more
179.4 152.1
Tab. 2: The value of IBDQ in relationship to defined parametres

34
SPITZER1. WO. State of science 1986: quality of life and functional status as target variables for research. J Chronic Dis 1987;40:465-471.TORRANCE2. GW. Measurement of health state utilities for economic appraisal. A review. J Health Econ 1986;5:1-30.YACAVONE3. RF, Locke GR 3rd, Provenzale DT, Eisen GM. Quality of life measurement in gastroen-terology: what is available? Am J Gastroenterol 2001;96:285-297.MEYERS S, WALFISH JS, SACHAR DB, GREENSTEIN AJ, HILL AG, JANOWI4. tz HD.Quality of life after surgery for Crohn´s disease: a psychological survey. Gastroenterology 1980;78:1-6.GUYATT G, MITCHELL A, IRVINE EJ, SINGER J, WILLIAMS N, GOODACRE R, TOMKINS,5. C. A new measure of health status for clinical trials in inflammatory bowel disease. Gastroenterology 1989;96:804-810.DEBOER AGEM, WIJKER W, BARTELSMAN JWF, DEHAES H6. CJM. Inflammatory bowel disease questionnaire: cross-cultural adptation and further validitation. Eur J Gastroenterol Hepatol 1995;7:1043-1050.ROSE M, FLIEGE H, HILDEBRANDT M, KORBER J, ARCK P, DIGNASS A, KLAPP 7. B. Validation of the new German translation version of the „Short Inflammatory Bowel Disease QuestionnaireO (SIBDQ). Z Gastroenterol 2000;38:277-286.HAN SW, MCCOLL E, STEEN N, BARTON JR, WELFARE8. MR. The inflammatory bowel disease ques-tionnaire: a valid and reliable measure in ulcerative colitis patients in th North East of England. Scand J Gastroenterol 1998;33:961-966.Pallis AG, Vlachonikolis IG, Mouzas IA. Quality of life of Greek patients with inflammatory bowel 9. disease. Validation of the Greek translation of the inflammatory bowel disease questionnaire. Digestion 2001;63:240-246.KIM WH, CHO YS, YOO HM, PARK IS, PARK EC10. , Lim JG. Quality of life in Korean patients inflam-matory Behcet´s disease. Int J Colorectal Dis 1999;14:52- 57.BEST WR, BECKTEL JM, SINGLETON JW, KERN F11. . Development of a Crohn´s disease activity index. Gastroenterology 1979;70:439-444.TOOSON JD, VARILEK GW12. . Inflammatory diseases of the colon. Inflamm Dis 1998;98:46-74.LATOUR P, BELAICHE J, LUIS F, FONTAINE F, DEFLANDRE J, LOLY J, OGER A, DEFRANCE P, DI VAL-13. ENTIN A, DELFORGE M, DAENEN G, LEBAS M, MOHR E, WAIN E, GILLARD C, THys C. Incidence on inflammatory bowel disease in the province of Liege (Belgium). La Societe de Gastroenterologie Liegeoise. Acta Gastroenterol Belg 1996;59:3-6.GOWER-ROUSSEAU C, SALOMEZ JL, DUPAS JL, MARTI R, NUTTENS MC, VOTTE A, LEMAHIEU 14. M, LEMAIRE B, COLOMBEL JF, CORTOT A. Incidence of inflammatory bowel disease in northern France (1988-1990). Gut 1994;35:1433-1438.HAUG K, SCHRUMF E, HALVORSEN JF, FLUGE JF, HAMRE G, HAMRE T, SKJOLLINGSTAD R15. . Epide-miology of Crohn´s disease in western Norway. Study group on Inflammatory bowel disease in Western Norway. Scand J Gastroenterol 1989;24:1271-1275.EKBOM A, HELMICK C, ZACK M, ADAMI H16. O. The epidemiology of inflammatory bowel disease: a large, population-based study in Sweden. Gastroenterology 1991;100:350-358.COTTONE M, MARTORANA G, DI MITRI R, CAMMA C, CAPRILLI R.17. Epidemiology of inflammatory bowel disease in Italy. Ital J Gastroenterol Hepatol 1999;31:503-7.
Literature

35
TRAGNONE A, CORRAO G, MIGLIO F, CAPRILLI R, LANFRANCHI GA. 18. Incidence of inflammatory bowel disease in Italy: a nationwide population-based study. Gruppo Italiano per lo Studio del Colon e del Reto (GISC). Int J Epidemiol 1997;26:904-906.BIELIK J, HLISTA M, ČERNOK S, ŠORF19. , M. Clinical and drug profile of Crohn´s disease. Ceska Slov Gastroenterol Hepatol 2002;56:158-163.WARE JF, SHERBOURNE CD20. . The MOS 36-item short-form health survey (SF-36). I.Conceptual framework and item selection. Med Care 1992;30:473-483.IRVINE EJ, FEAGAN B, ROCHON J, ARCHAMBAULT A, FEDORAK RN, GROLL A, KINNEAR D, SAIBIL F, 21. MCDONALD JW. Quality of life: a valid and reliable measure of therapeutic efficacy in the treat-ment on an inflammatory bowel disease. Gastroenterology 1994;106:287-296.IRVINE E22. J. Quality of life- measurement in inflammatory bowel disease. Scand J Gastroenterol Suppl 1993;199:36-39.LOVE JR, IRVINE EJ, FEDORAK R23. N. Quality of life in inflammatory bowel disease. J Clin Gastroen-terol 1992;14:15-19.MARTIN F, SUTHERLAND F, BECK24. IT et al: Oral 5-ASA versus prednisone in short term treatment of Crohn´s disease: a multicentre controlled trial. Can J Gastroenterol 1990;4:452-7. FEAGAN B, MCDONALD J WD, ROCHON, LAUPACIS AJ, FEDORAK RN, KINNEAR D25. et al. Chronic low dose cyclosporine in the treatment of Crohn´s disease. N Engl J Med 1994;330:1846-1851.GREENBERG GR, FEAGAN BG, MARTIN F ET AL.26. Oral budesonide as maintenance treatment for Crohn´s disease: a placebo-controlled, dose ranging study. Gastroenterology 1994;110:45-51.FEAGAN B, ROCHON J, FEDORAK RN, IRVINE EJ, WILD G, SUTHERLAND L E27. t al. Methotrexate for the treatment of Crohn´s disease. N Engl J Med 1995;332:292-297.IRVINE EJ, GREENBERG GR, FEAGAN BG, MARTIN F, SUTHERLAND LR, THOMSON AB, NILSSON 28. LG, PERSSON T. Quality of life rapidly improves with budesonde therapy for active Crohn´s dis-ease. Canadian Inflammatory bowel disease group. Inflamm Bowel Dis 2000;6:181-187.IRVINE29. EJ. Quality of life in inflammator bowel dissease: biases and other factors affecting scores. Scand J Gastroenterol Suppl 1995;208:136-140.VERMA S, TSAI HH, GIAFFER M30. H.: Does better disease-related education improve quality of life? A survey of IBD patients. Dig Dis Sci 2001;46:865-869.GUASSORA AD, KRUUSE C, THOMSEN OO, BINDER V31. . Quality of life study in a regional group of patients with Crohn´s disease. A structured interview study. Scand J Gastroenterol 2000;35:1068-1074.THIRLBY RC, SOBRINO MA, RANDALL JB.32. The long-term benefit of surgery on health related quality of life in patients with inflammatory bowel disease. Arch Surg 2001;136:521-527

36
nikoleta PoliaKoVá
involvement oF nurses in promoting health child population
Nurses may be significantly involved in prevention and health promotion of the
pediatric population. Thanks to the position of nurses can apply their personal impact on specific population groups, are competent to give advice on health, have the opportunity to cooperate with the various institutions that affect thinking and behavior in humans (Set of documents ..., 2003). The role of nurses work-
ing in policlinic for children and adolescents are aimed at enhancing and strengthening the health of children and youth, leading parents to good child care and early identification of risk factors. Sister knowledge of risk factors, early identification of individuals at risk and preven-tive use of available means and methods may try to positively influence the development of the baby’s health immediately after its birth.
The author in this paper presents the results of research aimed at measuring the involvement of nurses working in clinic for child and adolescent health promotion. Involvement of nurses in pre-ventive care was expressed as a percentage of time of working hours spent on counseling, the implementation of family visiting services, the level of communication with parents, cooperation with institutions and participation in projects. The research was aimed at finding a link between en-gagement of nurses and their age, length of experience and educational attainment. The research sample consisted of 95 nurses working in general outpatient children and adolescents. Research method was semi-structured questionnaire. The research results showed that the involvement of nurses is highest in counseling. At least the nurses involved in the cooperation with institutions and participation in projects. Involve the nurses on prevention and health promotion significantly increased with increasing education of nurses, but has not been proven significant negative correla-tion between exposure to age nor length of nurses’ professional experience in a clinic for children and adolescents.
counseling, communication, cooperation, age of nurses, the length of professional practice
Key words
Abstract

37
goalsIdentify level of involvement of nurses work- J
ing in clinics for children and adolescents in the field of counseling aimed at child care and prevention. Identify the relationship between the in- J
volvement of nurses and their age, the length of professional experience and high-est educational attainment.
methodology Data collection to meet the research objec-tives, we used semi-structured questionnaire for nurses working in policlinics for children and adolescents. Questionnaire, we surveyed such a measure such as nursing and strategies involved in prevention. We handed out 120 question-naires, the return was 79%. Data were collected from June 2009 to December 2009.
The sample of nurses consisted of 95 nurses working in policlinics for children and adoles-cents. Nurses younger than 50 years was 59 (62,1%), nurses over 50 years was 36 (37,9%). The average length of practice nurses was 12,43 years. Schools of nursing as the highest level of education had 84 nurses (88.4%). Specialization of them were 40 (42,1%) nurses. University de-gree I. or II. level was observed in 11 (11,6%) nurses. Given the use of the questionnaire method and its evaluation, we have worked with diverse types of data. In order to have notice of the maximum value of the acquired data, we se-lected the use of nonparametric tests. For com-parisons between two independent variables was used nonparametric consecutive Mann -Whitney test and the variables with binomial data based on the assumption: the higher rep-resentation of the phenomenon of higher value, the greater the average within the study period will be in group of. For the evaluation of more than two variables between the subsample we used Kruskal-Wallis nonparametric analysis as an alternative to one-way analysis of variance (ANOVA) for comparing independent files.
For the statistically significant test result was considered level of significance p less than 0,05
(p <0,05) and less. Above this value, although perhaps establish the presence of differences, but undersized statistical significance.
resultsInvolvement of nurses in prevention and health promotion in our study reflect the following in-formation:
advice, J
visiting in families, J
communication with parents, J
cooperation with various institutions such J
as crèche, kindergarten and primary school, parent center, cooperation on various projects aimed at prevention.
The average time spent counseling was 14,33% eight-hour working time, which represented an average of 1,14 hours (68 minutes). The maximum upper limit of the time dedicated to counseling was 35%, representing 2,8 hours (168 minutes). Frequently nurses give advice 10% of working time, which is the equivalent of 0,8 hours (48 minutes). The advice to most nurses, 80 (84,2%) focused on the issue of breastfeeding. The issue of hygiene, skin care and repackaging educate mothers 77 (81,1%) nurses, the introduction of additional food to the diet educate 58 of nurs-es (61,1%). The replacement milk preparations provide advice to 49 nurses (51,6%). Specific is-sues in prevention of allergy has been paid to 38 nurses (40,0%). The research results showed that the interest of parents for advice in the last three years has increased, confirmed up to 60 nurses (63,2%). Only 14 nurses (14,7%) indicat-ed that parents’ interest remains unchanged, and 21 nurses (22,1%) were unable to assess. Interested in information grows mainly on the issue of voluntary vaccination, which indicated 90% of parents. Other areas on which parents show interested, are the probiotics, hardening and strengthening the immune system. One visit to the home after the birth of a child en-gaged in 40 nurses (42,1%). Visits at home only if necessary carried out 37 nurses (38,9%) and 18 nurses (19%) visits in the home has not been made. Communication with parents rated as av-erage was 55 (57,9%) nurses, good quality com-

38
munication was perceived 26 (27,4%) nurses as weak and inadequate it assessed 14 (14,7%) nurses. Cooperation with institutions reported only 36 (37,1%) nurses. With no institutions co-operated to 59 (62,1%) nurses. The project in 24 nurses, i.e. 25,3%. Projects in which nurses have participated, were aimed at vaccinating children anthropometric measurements, cholesterol and blood glucose monitoring in adolescents. Of the nurses who work with the institutions (n 36), up 83,3% of them worked with primary and nurs-ery schools, 41,7% worked with parent centers and 13,9% worked with the crèche.
Involvement of nurses in promoting health child population were evaluated in relation to the age of nurses, the length of professional ex-perience and educational attainment.
Activities sisters differed significantly with regard to their age only in cooperation with parent centers (MC), younger cooperated sig-nificantly higher rate (p = 0,034) compared with older ones. Older sisters had a somewhat poor-er cooperation with other institutions- creches, kindergartens and primary school (p = 0,114). Other differences were not statistically signifi-cant. Differences in the level of communication and implementation of visits to the homes of children between nurses in relation to age have not been confirmed (tab.1).
Been confirmed nor a significant relationship between involvement and length of practice nurses (tab. 2).
In relation to the level of educational achieve-ment is confirmed differences in counseling, collaboration with institutions and participation in projects. Devote most of their time advising nurses with a university degree, up 17,73% of working time. Nurses specializing give advice 16, 68% of working time and nurses with nurs-ery school 11,36% of working time. The results also show that most visiting of nurse are carried out with the highest educational attainment (p = 0,03). We found that cooperation with institu-tions statistically significantly increased with in-creasing education nurses (p = 0,002). The most striking was the cooperation with the parent centers (p <0,001) and the kindergarten and pri-mary school (p = 0,02). Nurses with the highest education were statistically very significantly in-volved in the projects, compared with the other two categories (p <0,001), which are essentially the same level and almost do not participate in the projects. A marginally significant and varied differences in communication (Tab.3).
discussionAn important aspect that is helpful in maintain-ing and promoting health awareness and the ability to work with information. Nurses seek more than just engage in information provision.
Parameter age of nurses less than 50 years age of nurses over 50 years p
n x n x
Advise 59 14,322 36,000 14,361 0,835
Visit 59 1,712 36,000 1,861 0,295
Communication 59 1,797 36,000 2,000 0,160
Cooperation with
Institutions 59 1,559 36,000 1,722 1,114
Parent centers 59 1,780 36,000 1,944 0,034
Creche 59 1,949 36,000 1,944 0,921
Primary schools 59 1,644 36,000 1,750 0,284
Tab. 1: Activities of nurses due to their age
Legend: n-number of individuals, x-average, p, statistical significance test results (Mann-Whitney)

39
Tab. 2: Activities of nurses with regard to length of professional experience
Tab. 3: Activities of nurses with regard to education
Legend: n-number of individuals, x-average, p, statistical significance test results (Kruskal-Wallis)
Legend: n-number of individuals, x-average, p, statistical significance test results (Kruskal-Wallis)
Parameter Less than 10 years 11-20 years 21-30 years More than 30 yearsp
n x n x n x n x
Advise 17 15,06 18 13,28 33 14,67 27 14,19 0,9
Visit 17 1,53 18 1,83 33 1,82 27 1,82 0,52
Communica-tion
17 2 18 1,67 33 1,91 27 1,89 0,45
Cooperation with
Institutions 17 1,59 18 1,44 33 1,7 27 1,67 0,32
Parent centers
17 1,88 18 1,67 33 1,85 27 1,93 0,13
Creche 17 2 18 1,89 33 1,97 27 1,93 0,44
Primary schools
17 1,59 18 1,67 33 1,73 27 1,7 0,78
Projects 17 1,77 18 1,72 33 1,76 27 1,74 0,99
Parameter Nursing school Specialisation Universityp
n x n x n x
Advise 44 11,36 40 16,68 11 17,73 <0,001
Visist 44 1,93 40 1,73 11 1,27 0,03
Communi-cation
44 2,05 40 1,73 11 1,73 0,06
Cooperation with
Institutions 44 1,75 40 1,60 11 1,18 0,002
Parent centers
44 1,93 40 1,88 11 1,36 <0,001
Creches 44 1,93 40 2,00 11 1,91 0,57
Primary schools
44 1,80 40 1,65 11 1,36 0,02
Projects 44 1,84 40 1,80 11 1,18 <0,001

40
However, it is important to provide informa-tion so that compliance advice to parents was the best. The basic prerequisite for effective cooperation with parents is good communica-tion and quality. Level of communication and cooperation with parents assessed the majority of nurses, 55 (57,9%) than average. Communica-tion and collaboration with families as weak and inadequate evaluated 14 nurses (14,7%). These nurses said they do not perceive their parents and respected as an adviser, but with all the problems are turning to the doctor. The prob-lem must be sought in a lack of communication skills of sisters in our society and still continuing medical dominance. The issue of effectiveness of education and counseling deal with a multi-tude of scientific studies. An example would be learning Carol Bobb (2009), which compared the health status of 2 groups of patients suffering from bronchial asthma.
The first group of experiment participants received information leaflets aimed at lifestyle modification in asthma, the second group was controlled and educated systematically taking into account individual needs. After 4 months had significant improvement in respiratory func-tion in the second group. It has been shown to provide succinct and concise information is not enough. In terms of achieving desired changes in behavior, a comprehensive and system-atic approach. Protecting people from disease development is possible without their coop-eration. It is necessary to use all possible and available options counseling and education. De Blay et al. (2003) based on the results of their research, which aimed to assess the compliance of patients to the advice of experts proposing a new paramedical specialty: medical advisor for the home environment. Ideal opportunity for advice on home visiting service is an obligation at home after childbirth. The first visit the fam-ily after childbirth always held only 40 nurses (42,1% ).
The importance of visiting services in fam-ily studies confirm the results of Bracken et al. (2009), drawing attention to the fact that home visits by nurses in helping to identify early risk
factors associated with inadequate hygiene requirements, improper storage or storage of time-expired medicines and medicinal practices and inappropriate behavior of parents. Visiting sister in the family and adequate communica-tion is essential to follow-up of a confidential and friendly relations and good team to work together (Vincent, 2007; Vojtíšková, 2006).
The set of documents for the World Health Organization nurses and midwives (2003) states that nurses working in the field of community-based services can provide a wide range of services to the population of psychosocial inter-ventions, networking and social support to pre-natal care and nursing programs. Participation of nurses in the field of public health is limited by a number of barriers (financial, legal, prob-lems of lifelong professional development). The contribution of nursing to society is recognized, but the overall picture of nursing is still very narrow (Rebová, Boledovičová, 2009). Perhaps that is why nurses cooperation with institutions and their participation in projects was not sig-nificant. Cooperation with institutions reported only 37,1% of nurses and the projects were in-volved 25,3% of nurses.
We investigated the involvement of nurses in relation to their age, length of professional prac-tice and highest educational attainment. Age of nurses had an impact only on cooperation with institutions, when younger sister in a significantly higher level of cooperation with the parent cent-ers compared to older. Length of practice nurses had no impact on their engagement. The similar results also came Rybárová et al. To explore the participation of nurses working in clinic settings for prevention programs. For the survey sam-ple, 181 nurses found that nurses involvement in programs and projects is not dependent on age or length of professional experience. We found that the most important factor that directly re-lates to the involvement of nurses in promoting children’s health is education. Quality system of lifelong education of nurses is essential for in-creasing their involvement in preventive care. Educated nurses create a good condition to pro-vide quality community care.

41
conclusion Support the role of nursing in prevention is fo-cused on the application of scientifically proven preventive measures in community care. Nurs-es working in community care in the context of preventive care should:
assess and record risk factors for disease J
soon after birth, parents of children at risk systematically, de- J
liberately and comprehensively educate on how to reduce the risk of no good nutrition, hygiene and environmental adaptation, comply with the obligation of visiting servic- J
es in the family, the first visit made after the arrival of mothers with a child from hospi-tal to assess the physical, psychological and social environment of the child and recom-mend appropriate care, implement the visiting service to families, J
especially in the case of an increased risk of harm, or in children from disadvantaged backgrounds, in the event of symptoms of disease to in- J
form the need for timely doctor visits, engage in programs and projects to promote J
breastfeeding, in cooperation with the par-ent centers to keep advice on breastfeed-ing, engage in programs and projects aimed at J
environmental protection, engage in programs and projects with the J
aim of education to adopt healthy lifestyles of children,
increase collaboration with school facili- J
ties, to engage in health promoting schools project, improve educational activities on nutrition, J
hygiene and environmental factors in par-ents and children from disadvantaged back-grounds (also work with community social workers), to increase educational activities and coun- J
seling aimed to promote child health through media, increase publications focusing on the advice J
in magazines available for mothers, engage in public functions, J
increase and maintain the required profes- J
sional level through lifelong learning, increase and maintain the communication, J
education, interpersonal and counseling skills.
The issue of prevention and health promotion is a challenge for nursing. Nurses are the group of health workers to create and maintain links between individuals, families, communities and other elements of the health system, working independently, but also in cooperation with other entities for prevention and support, im-prove, maintain and restore health. Their work involves public health, health promotion, dis-ease prevention, the first contact with health care and disease management throughout the lifespan (ICN, 2008).
BOBB, C. Allergy advice beneficial in asthma. In: Practice nurse. 2009, Vol.38, Issue 7, p6-6, 1. 1/4p.BRACKEN, M et al. The importance of nurse-led home visits in the assessment of children 2. with problematic asthma. In: Archives of Diseasein Childhood. 2009, Vol 94, Issue 10, p7/7, 1p.DE BLAY, F., FOURGAUT, G., VERVLOET, D. et al. Medical indoor enviroment counselor (MIEC): 3. role in compliance with advice on mite allergen avoidance and on mite allergen exposure. In: Allergy. 2003, 58, pp. 27-33.
Literature

42
DOBIÁŠOVÁ, V., ČERVEŇANOVÁ, E., BUČKOVÁ, E.: Význam vzdelávania zdravotníckych pracovník-4. ov pre podporu zdravia. In. : Zborník Ošetrovateľstvo a zdravie III. a Pohyb a zdravie IV., vedecká konferencia, Trenčín, 2. apríl 2009, ISBN 978-80-8075-384-9, EAN 9788080753849,Medzinárodná rada sestier (ICN). Sestry vo vedení primárnej zdravotnej starostlivosti. Medz-5. inárodný deň sestier. 2008. Geneva: ICN, 2008. 33s. REBOVÁ, M., BOLEDOVIČOVÁ, M. Postavenie sestier na Slovensku. In: Ošetrovateľstvo 21. 6. storočia v procese zmien III.: zborník z medznárodného sympózia. Nitra, 2009. s.761-772.RYBÁROVÁ, Ľ., ŽULTÁKOVÁ, S., MAGUROVÁ, D. Hodnotenie účasti sestier a pôrodných asisten-7. tiek na preventívnych programoch. [online]. [online]. [cit.2010-01-06]. Dostupné na internete: http://old.unipo.sk/files/docs/fz_veda/svk/dokument_158_31.pdfSúbor dokumentov svetovej zdravotníckej organizácie pre sestry a pôrodné asistentky. 1.vyd. 8. Bratislava: Slovenská komora sestier a pôrodných asistentiek, 2003.202 s. VINCENTOVÁ, D. Preventivní prohlídky v pediatrii, role dětské sestry v primární péči v ČR. In: 9. Pediatrie pro praxi. 2007, roč. VIII., č. 2, s. 110-111VOJTÍŠKOVÁ, J. 2006. Kompetence všeobecní sestry v ordinaci praktického lékaře. In: Medicina 10. pro praxi. 2006, č.2, s.94-96
jana SlobodníKoVá
ultrasound guided biopsy and cytology during diFFerential diagnosis and therapy oF postoperative changes aFter conserving treatment oF breast cancer
The aim of our retrospective study was evaluation of interventional ultrasound methods – fine needle aspiration cytology and biopsy in the differential diagnostics of changes after conservative surgical treatment for early breast carcinoma.
The analysis of ultrasound, cytologic and bioptic findings in 2 312 patients after conservative therapy of breast cancer performed between January 1996 and November 2010 is reported. The major find-ings were: seromas, postoperative scars, haematomas, fat necrosis, skin thickening, inflammatory changes, granulomas and local tumor recurrence. In our experience, the interventional ultrasound guided methods are reliable methods for the follow up of early and late postoperative changes.
Abstract

43
breast, carcinoma, conserving treatment, biopsy, ultrasound, recidivation
Key words
Cancer occurs as a result of DNA miss-re-pairing or mutations, but in a most manner
is caused by epigenetically effects, which can modify expression of target genes. In the Slovak Republic, breast cancer is the most frequent tu-mor disease in women. There are known epige-netical risk factors: dose-specific alcohol effect, oral contraceptives, racial effect and age-speci-fication. They must be regarded together with mammographic density and genetic predisposi-tion.
Ultrasound imaging is an important tool in screening and diagnostics of breast abnormali-ties as well as in control during fine needle as-piration biopsy of the area with the suspected neoplasma.
aim The aim of the retrospective study was to asses the diagnostic value of sonography for detec-tion and characterization of changes after breast conserving therapy and radiation. Extension, echogenicity, configuration of lession in ultra-sound examination and follow-up examinations were the basis for correct diagnosis.
material and methodsBetween January 1996 and November 2011 we examined 2311 patients after conservative sur-gical therapy for early breast carcinoma. 720 patients of them have postoperative changes. We performed mammography, additive ultra-sound examination and invasive procedures after ultrasound control for correct differential diagnosis.
Range of age was found in the interval from 23 to 82 years. Most of the examined patients were within the range of 40th – 50th year of life.
The examinations were performed with ul-trasound analyser Sonoline Versa Pro, Sonoline, SG 50 and with mammography equipment Nova 3000 and Mammomat, produced by Siemens.
All biopsy were collected under biopsy con-trol with the free hand method, with the use of the needle 16, 18 and 20 G.
results and discussionThe analysis of the findings of the 720 patients showed a lot of varieties – postoperative chang-es, scares, granulomas, seromas, haematomas, fatt-necrosis, inflammatory changes after radio-therapy, fibrosis and tumor recurrence (Table 1).
The results of ultrasound guided interven-tional procedures; examinations of the solid breast masses for differential diagnosis are in Table 2. Cytologic examinations for treatment of seroma and haematoma were regular.

44
Changes Number %
Atypical scares 45 6.3
Keloid 39 5.2
Fatt necrosis 18 2.5
Granuloma 48 6.7
Seroma 102 14.2
Haematoma 51 7.1
Inflammatory changes 36 5.0
Fibrosis 69 9.6
RAT changes 282 39.2
Total 720 100.0
Type of changes Number of FNAC Results ( 1/ 2 ) %
Atypical scares 24 24/24 100.0
Keloid 30 27/30 90.0
Fatt necrosis 12 12/12 100.0
Granuloma 48 42/48 87.5
Tumor reccurence 30 30/30 100.0
Fibrosis 36 30/36 83.3
Type of changes Number of biopsy (aspirations)
Th and Dg effects %
Seroma 75 / 102 60 / 75 80.0
Heamatoma 30 / 51 24 / 30 80.0
Inflamatory changes 24 / 36 24 / 24 100.0
Tab. 1: Types of postoperative changes
Tab. 2: Differential diagnosis of solid masses
Tab. 3: Treatment of liquid collections, results of diagnostical and therapeutical effects
Legend: 1- number of coincidencie cytology, 2 - total number of aspiration cytology (biopsy)

45
Fig. 1: Sonography of the postoperative scars. Typical scar with acoustic shadowing starting at the skin level and interrupting all tissue layers
Legend: Patient – 47 years old, right breast, st.p. QE, Histology: Invasive ductal carcinoma, T1,N0,M0, G2
Fig. 2: Typical sonographic visualisation of hematoseromas under scar after quadrantectomyLegend: Patient - 39 years old women, left breast, Histology: Invasive ductal carcinoma, T1,N0.M0, G1

46
Fig. 3: Sonographic manifestations of atypical scar – hypoechoic, irregulary outlined scar
Legend: Patient: 58 years old women, right breast, Hi: Invasive lobular carcinoma, T2, N0,M0, G2. Cytology (FNAB): reparative changes, Histology (core biopsy): keloid
Fig. 4: Sonography of the granuloma. A round hypoechogenic lesion
Legend: Patient – 42 years old women, left breast, QE, EA. Histology: Lobular breast carcinoma, T1,N1, M0, G2. Cytology (FNAB): reparative changes. Histology (core cut biopsy): granuloma

47
Fig. 5: Sonographic manifestations of large seromas. Aspiration of seromas with visualization correct needle positioning before and during aspiration (biopsy) Volume: 68 ml
Legend: Patient: 59 years old women, left breast, histology: Adenocarcinoma, T1, N0, M0, G2. Cytology of aspiration (FNAB): seroma
Fig. 6: Typical hypoechoic breast lesion in area under scar after lumpectomy. Inhomogeneous structure, with accoustic shadowing
Legend: Patient: 67 years old women, histology: Invasive ductal carcinoma of the left breast T2,N1,M0. Cytology: (FNAB): local tumor recidive.
Histology (definitive, reoperation): tumor reccurence of invasive ductal carcinoma.

48
discussionUltrasound technique can be used in monitor-ing of disease response to surgical therapy, chemotherapy and radiotherapy and is neces-sary for differential diagnosis of the postopera-tive changes of breast tissues structure after conserving surgery. For planning and manage-ment of control and fellow-up after oncology therapy are clinical, imaging (mammography, ultrasound, ultrasound guided procedures, magnetic resonance) and pathology correlation fundamental to collaborative multidisciplinary diagnosis. Breast ultrasound has an important role in the detection and fellow-up of postop-erative changes. This imaging technique has an excellent sensitivity and specificity, when per-formed by experienced practitioners within a “triple“ assessment context. Reliable applica-tion of sonographic criteria of evaluation of le-
sions must by combined with comprehensive and practitioner knowledge of breast anatomy, breast pathology.
conclusionsOur experience showed that the interventional ultrasound together with cytological and histo-logical examinations is the reliable method for differential diagnosis and fellow-up postopera-tive time period and during later phases.
The aspiration ultrasound guided biopsy with needle has its importance in the therapy of larges seromas and haemagtomas, the core cut biopsy for the determination differential di-agnosis of solid postoperative changes.
Fig. 7: Sonographic image of the typical changes after radiotherapy (postiradiation inflammatory changes skin and tissue under skin of the breast in acute phasis)

49
BOSCH A.M, KESSELS AG et al. Preoperative estimation of the pathological breast tumor size 1. by physical examination, mammography and ultrasound . a prospective study on 105 invasive tumours. Europen Jurnal of Radiology, 2003, 48 (3): 285 - 292.CARDER PJ, GARVICAN J, HAIGH I et al. Needle core biopsy can reliably distinguish between 2. benign and malignant papillary lesions of the breast. Histopathology, 2005, 46 (3) : 320 – 327.DIXON, A.M. Breast ultrasound, how, why and when. 2008, Churchill Livingstone, 282p.3. HEYWANG – KOBRUNNER S, DERSHAV DD, SHEER I. Diagnostic breast imaging. 2nd. Ed., 2002, 4. Stuttgart, Deutschland.MADJAR H. Practical breast ultrasound. 2000, Stuttgart, Deutschland.5. STAVROS AT. Breast ultrasound. 2004, Philadelphia, Lippincott, Wilkinson § Williams.6. TOT T, TABAR L, DEAN PB. Practical breast pathology. 2002, New York, Thieme.7. ZONDERLAND HM, COERKAMP EG te al. Diagnosis of breast cancer. Contribution of US as an 8. adjunct to mammography . Radiology, 1999, 213 : 413-422.
Literature
Gabriela roZVadSKÝ GuGoVá
coping strategies in conFlict situations (anXiety and avoidance)
The paper presents the outcomes of research with the ECR-R, in the attachment, briefly referred to the administration in the selected sample. Part of the article is partial output of descriptive sta-tistics and frequency analysis of one of the scales. The main ideas are on the conflict and coping strategies of avoidance and anxiety.
Abstract
coping strategies, The Experiences in Close Relationships-Revised (ECR-R) Questionnaire, anxiety, avoidance
Key words

50
coping strategiesConflict situations are for each individual rou-tine. Theory defines what may be construed as a conflict, it may be a meeting of two conflict-ing or competing trends, views and intentions, it is an entity for a number of options, the two incompatible tendencies, conflict as disorien-tation, abnormal behavior of the organism, a situation in which person must make a decision. Sources of conflict are the external environ-ment - requirements, constraints, errors in the upbringing, temperament, personality traits, at-titudes and moral qualities, and ultimately man himself - the shortcomings in physical and men-tal characteristics, current mental status, mood, fatigue, illness, distorted image of themselves . Individual reactions when confronted with con-flict in general tend to either punitive outward-ly, the outer barrier, fury, rage. Or it is punitive inside, blame, remorse. create reactions. One frustration of the defense mechanisms that we use in its defense are certainty, rituals, coping strategies.
They can be characterized as a coping strat-egy. Coping responses may vary, for example, a man apparently exactly the opposite message as he calls (defense reaction), sometimes to the layout method of coping with situations. More often, people use trans-situational style. It's about developing a certain way and it is used regardless of the type of situation. Such coping strategies can include anxiety and avoidance. Both factors are of course an important part of defense mechanisms that protect the individu-al. We believe that if the bird avoidance model familiar to him as satisfactory, it will reproduce well as coping strategies. Avoidance and anxiety are factors encountered in the attachment. For these reasons we chose for our research ques-tionnaire ECR-R. We wondered how respond-ents use anxiety and avoidance in relation to the close person.
One of the most commonly used question-naires of attachment in adults is already men-tioned questionnaire The Experiences in Close Relationships-Revised (ECR-R) Questionnaire authors Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). The revised version contains the same as the original 18 items, which saturate both anxiety and avoidance factors. Combining the two areas incurred subsequent four basic types of attachment adults: secure type, anxious type, avoidant type, disoriented type (Biescad, M. and Hasto, J., 2010). The following lines contain a short questionnaire administration and sub outputs from the statistical processing.
research sample and admin-istration oF the revised Ques-tionnaire (ecr-r)In the research we have to determine rates of anxiety and avoidance questionnaire used for the typology of attachment (attachment) in adulthood, as I live close relationships - revised questionnaire (ECR-R) The Experiences in Close Relationships-Revised (ECR-R) Questionnaire authors Brennan, K . A., Clark, C. L., & Shaver, P. R. (1998). For the purposes of research, we modified the order of items, 18 items is a range of anxiety and 18 items is a range of avoidance. Administration took place in the period Septem-ber to December 2010. To illustrate a sample of the questionnaire and order items, which fed the modified version of both scales.
In the survey there was total of 920 respond-ents, of whom 428 men and 492 women rang-ing in age from 18 to 55 years, with secondary school graduates, Czech and Slovak national-ity. Administration of the test was conducted during the months of September to December 2010 in groups from 50 to 100 respondents. For administration paper sheet questionnaire was
1. I fear that the loss of love partner for support. 1 2 3 4 5 6 7
2. I feel uncomfortable when revealing their national partner for support. 1 2 3 4 5 6 7
3. My desire for a very close relationship sometimes discourage people. 1 2 3 4 5 6 7
Tab.1: Sample of questionnaire ECR-R, I totally agree is 7 points, I completely disagree is1 point

51
used. Respondents filled in data on pre-printed sheet of A4 paper with questions. The time limit was not set, respondents were able to adapt well to a group of 100 people and had no prob-lem with time. Time-administration group was disproportionately less demanding without the presence of a psychologist. Who was responsi-ble for explaining and answering any questions of respondents.
In the first part of the administration, respond-ents were given instructions on what type of questionnaire goes and for what purpose, in the second part the paper sheets were provided to each participant. In the next section, as the ad-ministrator verified that all respondents have completed the basic data in anamnestic part a short briefing of how the respondents should score followed.. Characteristics of survey sam-ple is shown in the following graphs.
scale items
anxiety 1, 3, 4, 5, 7, 8, 9, 11, 13, 15*, 17*, 19, 22, 23, 24, 27, 30, 31
avoidance 2, 6*, 10*, 12, 14*, 16*, 18*, 20*, 21*, 25*, 26, 28, 29, 32*, 33*, 34, 35*, 36*
Tab.2: Items in the questionnaire, which saturate both scales anxiety and avoidance
Reverse items: 9, 11, 20, 22, 26, 27, 28, 29, 30, 31, 33, 34, 35, 36 *reversed polarity items 1→7, 2→6, 3→5, 4→4, 5→3, 6→2, 7→1
Graph 1: Gender of respondents, research 2011
Graph 2: Age of respondents, research 2011

52
Graph 3: Status of respondents, research 2011
partial outputs From researchBelow we present a partial outputs from the statistical compilation of research, the tables
give the range of anxiety in the descriptive sta-tistics and frequency analysis.
N Range Minimum Maxi-mum
Sum Mean Std. De-viation
Variance
V1 920 6 1 7 3302 3,59 1,949 3,801
V3 920 6 1 7 2754 2,99 1,759 3,095
V4 920 6 1 7 2470 2,68 1,825 3,330
V5 920 6 1 7 2944 3,20 1,896 3,594
V7 920 6 1 7 4630 5,03 2,061 4,247
V8 920 6 1 7 1808 1,97 1,513 2,288
V9 920 6 1 7 2949 3,21 2,002 4,009
V11 920 6 1 7 3158 3,43 1,982 3,930
V13 920 6 1 7 2698 2,93 1,866 3,482
V19 920 6 1 7 2469 2,68 1,832 3,357
V22 920 6 1 7 2195 2,39 1,709 2,921
V23 920 6 1 7 3960 4,30 2,253 5,076
V24 920 6 1 7 3097 3,37 1,935 3,745
V27 920 6 1 7 2871 3,12 1,979 3,917
V30 920 6 1 7 2223 2,42 1,656 2,744
V31 920 6 1 7 2452 2,67 1,734 3,006
Valid N (listwise)
920
Tab. 3: Descriptive Statistics Anxiety, research 2011

53
I fear that the loss of love partner for support.
Frequency Percent Valid Percent CumulPercent
Valid 1 158 17,2 17,2 17,2
2 183 19,9 19,9 37,1
3 131 14,2 14,2 51,3
4 144 15,7 15,7 67,0
5 111 12,1 12,1 79,0
6 97 10,5 10,5 89,6
7 96 10,4 10,4 100,0
Total 920 100,0 100,0
I feel uncomfortable when revealing their national partner for support.
Frequency Percent Valid Percent CumulPercent
Valid 1 238 25,9 25,9 25,9
2 196 21,3 21,3 47,2
3 150 16,3 16,3 63,5
4 151 16,4 16,4 79,9
5 80 8,7 8,7 88,6
6 65 7,1 7,1 95,7
7 40 4,3 4,3 100,0
Total 920 100,0 100,0
My desire for a very close relationship sometimes discourage people.
Frequency Percent Valid Percent CumulPercent
Valid 1 326 35,4 35,4 35,4
2 227 24,7 24,7 60,1
3 96 10,4 10,4 70,5
4 100 10,9 10,9 81,4
5 75 8,2 8,2 89,6
6 45 4,9 4,9 94,5
7 51 5,5 5,5 100,0
Total 920 100,0 100,0
Tab. 4: Frequencies Statistics Anxiety, item No. 1 in the questionnaire
Tab. 5: Frequencies Statistics Anxiety, item No. 2 in the questionnaire
Tab. 6: Frequencies Statistics Anxiety, item No. 3 in the questionnaire

54
conclusionThe frequency analysis of item no. 1 shows that up to 96 respondents are afraid of losing love partner, while 158 individuals are not worried at all. The frequency analysis of item no. 2 shows that 40 respondents think that their desire for closeness discourages people and vice versa 238 respondents do not think so. The frequency
analysis of item no. 3 showed that 51 individuals are often plagued by partner who does not love him and vice versa 326 respondents were not afraid of the facts. For those outcomes we can say that from 4% to 10% of respondents in the sample examined anxiety. Other interpretations will be able to present after statistical research processing.
BRENNAN, K. A., CLARK, C. L., & SHAVER, P. R..: Self-report measurement of adult attachment: 1. An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). 1998, New York: Guilford Press.BIEŠČAD, M. a HAŠTO, J. :Ako prežívam blízke vzťahy-revidovaný dotazník (ECR-R) The experi-2. ences in Close Relationship-Revised (ECR-R) Questionnaire. In: Fraley, R.C., Waller, N.G., Bren-nan, K.A. (2000) An item-response theory analysis of self report measures of adult attachment. Journal of Personality and Social Psychology, 78(2), 350-356BIEŠČAD, M. a HAŠTO, J.: Diagnostikovanie typov vzťahovej väzby (attachmnet) v dospelosti s 3. použitím nástrojov dostupných v našich podmienkach. Psychiatrie 2010,14(2): 68-74
Literature