Embed Size (px)
DESCRIPTION
How can We Capitalize on Connections between Theory and Practice? Perspectives from the Study of Behavior Change. Alex Rothman Department of Psychology University of Minnesota Center for Health, Intervention, and Prevention University of Connecticut November 2010. - PowerPoint PPT Presentation
Citation preview

How can We Capitalize on Connections between Theory and Practice?
Perspectives from the Study of Behavior Change
Alex RothmanDepartment of PsychologyUniversity of Minnesota
Center for Health, Intervention, and PreventionUniversity of Connecticut
November 2010

Does it Matter How We Think about the Interplay Between Theory and Practice?
•Why Construals/Metaphors Might Matter?
•Guide how investigators think about and conduct their work
•Guide the composition of research teams
•Guide how/where/to whom findings are communicated
•Guide how resources are allocated
•Guide where resources are allocated (e.g., the design and implementation of systems that support the efforts of investigators)
•All have implications for progress in theory and practice

Conceptualizing the Interplay Between Theory and Practice
Social/Personality Psychology
(Basic/Theory)
Health(Applied/Practice)

Classic View of the Link between Theory and Practice
Social/Personality Psychology
(Basic/Theory)
Health(Applied/Practice)

“…Many psychologists working today in an applied area are keenly aware of the need for close cooperation between theoretical and applied psychology. This can be accomplished in psychology, as it has been accomplished in physics, if the theorist does not look toward applied problems with highbrow aversion or with a fear of social problems, and if the applied psychologist realizes that there is nothing so practical as a good theory.”
--Kurt Lewin (1943-44), “Problems of research in social psychology”

Classic View of the Link between Theory and Practice
Social/Personality Psychology
(Basic/Theory)
Health(Applied/Practice)Weak/Passive
Links

Re-conceptualizing the Link between Theory and Practice
Basic/Theory Applied/Practice
Understanding(Social/Personality
Psychology)
Use(Health)
Understanding and Use(Social/Personality &
Health)
Adapted from Stokes (1997), Pasteur’s Quadrant

“…if the theorist does not look toward applied problems with highbrow aversion or with a fear of social problems, and if the applied psychologist realizes that there is nothing so practical as a good theory.”
--Kurt Lewin (1943-44), “Problems of research in social psychology”
•The pursuit of understanding and use provides the opportunity to transform a theory into a good theory (Rothman, 2004)
(For further discussion, see Suls & Rothman, 2004; Weinstein & Rothman, 2005, Michie , Rothman , & Sheeran, 2008; Rothman, 2009)

Intervention Behavior
ActionTheory
ConceptualTheory
What Could a “Good Theory” Do?
PredictorMediator

Intervention Behavior
Moderator(action)
What Could a “Good Theory” Do?
Mediator
For Whom (people)? For What (behavior)?
Moderator(conceptual)

Intervention Behavior
What Could a “Good Theory” Do?
Mediator
Timing: When does it matter?Specificity: What matters when?
Behavior
Mediator
Initiation
Maintenance

Pursuing Understanding and Use in Research at the Interface Between Social/Personality Psychology and Health
1. Initiation and Maintenance of Behavior Change (Rothman, 2000; Rothman et al., 2004, 2010)
•Specify the psychological processes that regulate the initiation and maintenance of behavior
•Design and test theory-based intervention strategies to promote healthy behavior
2. Framing Health Messages (Rothman & Salovey, 1997; Rothman et al., 2008; Rothman & Updegraff, in press)
•Specify the processes that mediate and moderate the influence of gain- and loss-framed messages
•Design and test theory-based communication strategies to promote healthy behavior

Model of Behavioral Initiation and Maintenance(Rothman, 2000; Rothman, Baldwin, & Hertel, 2004;
Rothman, Hertel, Baldwin, & Bartels, 2008)
Behavioral Initiation• Guided by expectations about
outcomes and process
• Optimistic expectations predict interest and initial success
• Motivated by desire to approach favorable goal (i.e., to be thin)
• Progress is marked by a change in discrepancy between current state and a goal state
Behavioral Maintenance• Guided by satisfaction with
outcomes and process• Satisfaction predicts long-term
success• Satisfaction based on comparison
of experiences to expectations• Motivated by a desire to avoid
unfavorable goal (i.e., not be a smoker)
• Progress is marked by a sustained discrepancy between current state and a prior state

Intervention InitialBehavior
Expectations/Confidence
SustainedBehavior
Satisfaction
Model of Behavioral Initiation and Maintenance(Baldwin et al., 2006, Health Psychology; Finch et al., 2005, Health Psychology; Hertel et al., 2008, Health Psychology)
(Tested in a parallel set of community-based Interventions designed to promote either smoking cessation or weight loss)

Challenge Smoking Cessation Project:Expectation-Based Intervention
• 8 week group-based quit program
• Quit date between 4th and 5th session
• 529 Participants were randomly assigned to:
(a) Optimistic treatment program– Focus on the benefits of quitting; Emphasize maintaining
a positive view of cessation outcomes and process
(b) Balanced treatment program– Focus on both benefits and costs of quitting; Emphasize
maintaining a balanced view of cessation outcomes and process
(Hertel et al., 2008, Health Psychology; see also Finch et al., 2005)

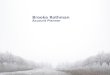
Effect of Intervention Condition on Smokers’ Quit Status at End of Active Treatment (Session 8)
53.7%
32.0%39.7% 41.3%
0%10%20%30%40%50%60%
Prior Quit > 3Months
Prior Quit < 3Months
Optimistic ConditionBalanced Condition
[Condition x Prior Abstinence Interaction: p < .05]
Per
cent
Sm
oke
Fre
e fo
r la
st 7
day
s

Effect of Intervention Condition on Smokers’ Expectations and Confidence
Longest Prior Quit Longest Prior Quit > 3 months < 3 months
Optimistic Balanced Optimistic Balanced condition condition condition condition
Beliefs assessed at Session 4 on 9 point scale ranging from –4 to +4 (expectations) and from 0 to 8 (self-efficacy)
[Condition x Prior Abstinence Interaction: p’s < .05]
Expectationsabout outcomes
4.80(.14)
2.25(.07)
2.19(.08)
2.39(.08)
Confidence aboutability to quit
5.21(.14)
4.75(.12)
2.42(.08)
4.93(.14)

Do Beliefs About Cessation Mediate the Interaction Effect on Smoking Status at Session 8?
Intervention Intervention Condition X Condition X
Prior Quit Prior Quit LengthLength
Self-Efficacy Self-Efficacy (session 4)(session 4)
Smoke Free at Smoke Free at Session 8Session 8(p > .10)(p > .10)
=.77=.77
[Direct effect: [Direct effect: =.87, =.87, pp < .05 ] < .05 ][Sobel test: z = 1.90, p < .05][Sobel test: z = 1.90, p < .05]
Expectations Expectations (session 4)(session 4)
=.65=.65(p<.05)(p<.05)
=.21=.21(p<.01)(p<.01)
=.38=.38(p<.05)(p<.05)
=.17=.17(p<.01)(p<.01)
ActionTheory
ConceptualTheory

Effect of Intervention Condition on Smokers’ Quit Status after 6 Months and 18 Months
34.7%
14.0%
24.4%
28.3%
0%
10%
20%
30%
40%
50%
60%
Prior Quit > 3 Months Prior Quit < 3 Months
Optimistic Condition Balanced Condition
31.0%
11.0%
25.0% 22.0%
0%
10%
20%
30%
40%
50%
60%
Prior Quit > 3 Months Prior Quit < 3 Months
Optimistic Condition Balanced Condition
Per
cent
Sm
oke
Fre
e fo
r la
st 7
day
s
[Condition x Prior Abstinence Interaction: p’s < .05]

Specifying the Process:Did the Intervention Have a Direct or Indirect Effect
on Smoking Status at 6 Months?
Intervention Intervention Condition X Condition X
Prior Quit Prior Quit LengthLength
Smoke Free at Smoke Free at Session 8Session 8
Smoke Free at Smoke Free at 6 Months6 Months(p > .20)(p > .20)
=.72=.72
[Direct effect: [Direct effect: =1.05, =1.05, pp < .05] < .05][Sobel test: z = 2.04, p < .05][Sobel test: z = 2.04, p < .05]
=.87=.87(p<.05)(p<.05)
=2.53=2.53(p<.01)(p<.01)

Specifying the Process:Does Satisfaction with Behavior Change Underlie
Sustained Behavior Change?
Smoke Free at Smoke Free at Session 8Session 8
Satisfaction Satisfaction with quit at with quit at Session 8Session 8
Smoke Free at Smoke Free at 6 Months6 Months(p < .01)(p < .01)
=1.53=1.53
[Direct effect: [Direct effect: =2.53, =2.53, pp < .01] < .01][Sobel test: z = 2.36, p < .05][Sobel test: z = 2.36, p < .05]
=4.02=4.02(p<.01)(p<.01)
=.23=.23(p<.05)(p<.05)
(See also Baldwin et al., 2006)

Implications and Lingering Questions: I
• Integrating models of prediction and models of change: Action theory and conceptual theory(cf. Jeffery, 2004; Rothman, 2004)
• What are the determinants of people’s satisfaction?(Baldwin et al., 2009, Psychology & Health; in press, Annals of Behavioral Medicine)
• How can we design methods to enhance the satisfaction people derive from changes in their behavior?

InitialBehavior
BehavioralOutcomes/Experience
What Could a “Good Theory” Do?:
SubsequentBehavior
Satisfaction
Moderators of Output:Biological Factors
Moderators of Input:Dispositional/Goal Factors
What mediates the Mediator?
What moderates the Mediator?
Targets forIntervention

Do Initiation and Maintenance benefit from different self-regulatory strategies?
•Higgins (1998) proposed two styles of self-regulation:–Promotion-focus: Concern with accomplishments, hopes, aspirations; focus on eager approach-based strategies and positive outcomes.
–Prevention-focus: Concern with safety, responsibility, obligations; focus on vigilant avoidance-based strategies and negative outcomes.

InitialBehavior
Promotion Focus:Concern with accomplishments, hopes, aspirations; focus on eager approach-based strategies and positive outcomes
SustainedBehavior
Prevention Focus:Concern with safety, responsibility, obligations; focus on vigilant avoidance-based strategies and negative outcomes
•RFQ (regulatory focus questionnaire; Higgins et al., 2001) was completed at baseline in both the smoking cessation and weight loss interventions (Fuglestad et al., 2008)

Challenge Study: Weight Loss
(Fuglestad et al. (2008) Health Psychology)
H1: Participants who score higher on promotion-focus will have greatersuccess losing weight
Effect of Promotion Focus on Weight
190192194196198200202204206208
Month
Wei
ght
(lb
)
low promotion
high promotion

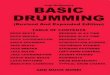
Challenge Study: Weight Loss
•Hypothesis 2: Participants who score higher on prevention-focus will have greater success maintaining weight that was lost
How do you operationalize maintenance?5% weight loss maintained for at least 1 monthDiscrepancy between weight and acceptable weight loss goal (assessed at base line)
•Small Discrepancy: Focus on maintaining weight loss•Large Discrepancy: Focus on continuing to lose weight

Challenge Study: Weight Loss
(Fuglestad et al. (2008) Health Psychology)
Effect of Prevention Focus on Weight by Discrepancy between Actual and Acceptable Weight Goal
184
186
188
190
192
194
196
198
mo1mo3
mo5mo7
mo9mo11
mo13mo15
Month After 5% Decrease in Weight
Wei
ght
(lb
)
small discrepancy low prevention
small discrepancy high prevention
large discrepancy low prevention
large discrepancy high prevention

Challenge Study: Weight Loss
(Fuglestad et al. (2008) Health Psychology)
Effect of Prevention Focus on Weight for People Close to their Acceptable Weight Goals
184
186
188
190
192
194
196
198
mo1mo4
mo7mo10
mo13
Month After 5% Decrease in Weight
Wei
ght
(lb
)
small discrepancy low prevention
small discrepancy high prevention

Challenge Study: Weight Loss
(Fuglestad et al. (2008) Health Psychology)
Effect of Promotion Focus on Weight by Discrepancy between Actual and Acceptable Weight Goal
184
186
188
190
192
194
196
mo1mo3
mo5mo7
mo9mo11
mo13mo15
Month After 5% Decrease in Weight
Wei
ght
(lb
)
small discrepancy low promotion
small discrepancy high promotion
large discrepancy low promotion
large discrepancy high promotion

Challenge Study: Weight Loss
(Fuglestad et al. (2008) Health Psychology)
Effect of Promotion Focus on Weight for People Far from their Acceptable Weight Goals
184
186
188
190
192
194
196
mo1mo3
mo5mo7
mo9mo11
mo13mo15
Month After 5% Decrease in Weight
Wei
ght
(lb
)
large discrepancy low promotion
large discrepancy high promotion

Challenge Study: Smoking Cessation
Looking more closely at how promotion focus may help:Does a promotion-focus help people respond to a slip?
Behavioral Response to Slip by Promotion Focus
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
Month After 1st Slip
Pro
babi
lity
Sti
ll S
mok
ing
low promotion
high promotion

Challenge Study: Smoking CessationLooking more closely at how promotion focus may help:Does a promotion-focus help people respond to a slip?
Behavioral Response to Slip by Self-Efficacy and Promotion Focus
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
mo1mo3
mo5mo7
mo9mo11
mo13
Month After 1st Slip
Pro
babi
lity
Sti
ll S
mok
ing
low efficacy low promotion
low efficacy high promotion
high efficacy low promotion
high efficacy high promotion

Challenge Study: Smoking CessationLooking more closely at how promotion focus may help:Does a promotion-focus help people respond to a slip?
Behavioral Response to Slip by Self-Efficacy and Promotion Focus
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
mo1mo3
mo5mo7
mo9mo11
mo13
Month After 1st Slip
Pro
babi
lity
Sti
ll S
mok
ing
low efficacy high promotion
high efficacy high promotion

Challenge Study: Smoking Cessation
Avoiding Slips by Prevention Focus for People who have Quit for 2 Months
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
mo1mo3
mo5mo7
mo9mo11
mo13
Month After 2 Months of Being Quit
Pro
bab
ility
Sti
ll Q
uit
low prevention
high prevention

Challenge Study: Smoking Cessation
Avoiding Slips by Self-Efficacy and Prevention Focus for People who have Quit for 2 Months
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
mo1mo3
mo5mo7
mo9mo11
mo13
Month After 2 Months of Being Quit
Pro
bab
ility
Sti
ll Q
uit
low efficacy low prevention
low efficacy high prevention
high efficacy low prevention
high efficacy high prevention

Challenge Study: Smoking Cessation
Avoiding Slips by Self-Efficacy and Prevention Focus for People who have Quit for 2 Months
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
mo1mo3
mo5mo7
mo9mo11
mo13
Month After 2 Months of Being Quit
Pro
bab
ility
Sti
ll Q
uit
high efficacy low prevention
high efficacy high prevention

Implications and Lingering Questions: II
• Potential implications for practice• Provide initiation/maintenance strategies that match people’s
chronic focus
• Use RFQ scores to identify “vulnerable” actors and provide additional support
• (A few) Lingering questions:• What does the RFQ measure?
• How do we integrate models of self-regulation with models of behavior change?

Pursuing Understanding and Use in Research at the Interface Between Social/Personality Psychology and Health?
1. Initiation and Maintenance of Behavior Change (Rothman, 2000; Rothman et al., 2004, 2010)
•Specify the psychological processes that regulate the initiation and maintenance of behavior
•Design and test theory-based intervention strategies to promote healthy behavior
2. Framing Health Messages (Rothman & Salovey, 1997; Rothman et al., 2008; Rothman & Updegraff, in press)
•Specify the processes that regulate the influence of gain- and loss-framed messages
•Design and test theory-based communication strategies to promote healthy behavior

Predicting the Impact of Gain and Loss Framed Messages: Two Perspectives
• Perspective #1: The impact of gain- and loss-framed messages depends on the match between the frame and the risk implications of the behavior promoted (e.g., Rothman & Salovey, 1997; Rothman et al., 2008; Bartels et al., 2010)
• Function of the behavior (e.g., detection/prevention)
• Construal of the behavior/health issue (e.g., risk)
• Perspective #2: The impact of gain- and loss-framed messages depends on the match between the frame and the motivational orientation of the recipient (e.g., Mann et al., 2004; Updegraff et al., 2007)
• BIS/BAS (Carver & White, 1994)

Rothman et al. (1999) Mann et al. (2004)

Message Framing Intervention to Promote Mammography:Testing Competing Moderators
• 355 women (40 and older, M=51) recruited at an inner city hospital (49% African American); all due for a mammogram
• Measured:
(a) How mammography is construed (i.e., illness detecting vs. health affirming)
(b) Perceived susceptibility for developing breast cancer (Champion, 1999)
(c) Motivational orientation (BIS/BAS)
• Viewed 10 minute gain- or loss-framed video about mammography• 3 month follow-up interview (mammography utilization)
(Funded by NCI Grant R03-CA128468; Updegraff, PI)

Main Effect of Frame on Mammography UtilizationP
erce
nt S
cree
ned
at 3
Mon
ths
(Gallagher, Updegraff, Rothman, & Sims (in press), Health Psychology)

Perceived Susceptibility of Developing Breast Cancer Moderated Effect of Message Frame on Screening Behavior
(Gallagher, Updegraff, Rothman, & Sims (in press), Health Psychology)

Construal of Mammography Moderates Framing Effect: Women with Family History of Breast Cancer
(N=63)P
erce
nt S
cree
ned
at 3
mon
ths

Implications and Lingering Questions: III
• Implications for Theory and Practice (understanding and use): • Provides an initial progress toward integrating current theoretical
models (Rothman & Updegraff, in press)
• Better specification of the factors that moderate responses to gain- and loss-framed appeals
• Lingering questions: • To what extent does the pattern of findings obtained generalize to
other behavioral domains?
• Are there specific situations when the moderating effect of dispositional factors such as motivational orientation will be obtained?
• Are framed appeals effective because they persuade people to act or because they nudge people to act?

What can be done to promote the pursuit of understanding and use?
• Take our theories seriously• We need to mindful of what our theories do and do not say
• We need to pursue opportunities to challenge our theories and discern what they can and cannot do.
• Need an environment that supports these efforts:• NCI Theories Project (
http://cancercontrol.cancer.gov/brp/theories_project/)
• Work by Susan Michie and colleagues
• Advanced Training Institute on Health Behavior Theory (2012), (http://cancercontrol.cancer.gov/workshop/ )

Promoting the Pursuit of Understanding and Use:
Linking Social/Personality Psychology and Health
• Social Personality & Health Network (www.sphnetwork.org)
•Social Personality and Health Pre-conference prior to 2011 SPSP meeting

Contact InformationAlex RothmanDepartment of PsychologyUniversity of MinnesotaPhone: 612-625-2573Email: [email protected]