Embed Size (px)
DESCRIPTION
pathology
Citation preview

1
ALCOHOLIC LIVER DISEASE
Dr Kavita Karmacharya

2
INTRODUCTION
•Alcohol consumption is high in most of the countries
• In the US, > 10% of people abuse or are dependent on alcohol
•The male:female ratio is about 2:1.

3
Definition
•Disorders that occur in alcohol abusers, often in sequence, include
▫Fatty liver ( > 90%)▫Alcoholic hepatitis (10 to 35%)▫Cirrhosis (10 to 20%)

4

5
Fatty liver
•Occurs after acute alcohol ingestion, is generally reversible with abstinence

6
Alcoholic hepatitis•Acute form of alcohol-induced
liver injury
•Occurs with the consumption of a large quantity of alcohol over a prolonged period of time
•Encompasses a spectrum of severity ranging from asymptomatic derangement of biochemistries to fulminant liver failure and death

7
Cirrhosis
•Replacement of the normal hepatic parenchyma with extensive thick bands of fibrous tissue and regenerative nodules
•Results in the clinical manifestations of portal hypertension and liver failure

8
RISK FACTORSThe main causative factors in alcoholic liver disease :
1. Quantity and duration of alcohol use
2. Sex
3. Genetic and metabolic traits
4. Nutritional status

9
Quantity of alcohol: •Among susceptible people, a linear correlation
generally exists between the amount and duration of alcohol use and the development of liver disease.
•Risk increases markedly for men who drink▫ > 40 g/day
•For cirrhosis to develop, consumption must usually be ▫> 80 g/day for > 10 yr▫If consumption exceeds 230 g/day for 20 yr, risk of
cirrhosis is about 50%.

10
Sex:
•Women are more susceptible to alcoholic liver disease
•Women require only 20 to 40 g of alcohol to be at risk—½ of that for men
•Because they have less alcohol dehydrogenase in their gastric mucosa; thus, first-pass oxidation of alcohol is decreased

11
Genetic factors:
•Alcoholic liver disease often runs in families
•Suggesting genetic factors
•eg, deficiency of cytoplasmic enzymes that eliminate alcohol

12
Nutritional status:
•Undernutrition, particularly protein-energy malnutrition
•Diet high in unsaturated fat
•Obesity

13
PATHOPHYSIOLOGYAlcohol (ethanol) is readily absorbed from the stomach, but most is absorbed from the small intestine.
Alcohol dehydrogenase (ADH) Acetaldehyde
Acetaldehyde dehydrogenase Acetate

14

15
1.Chronic alcohol consumption enhances acetate formation
2.These oxidative reactions generate hydrogen, which converts nicotinamide-adenine dinucleotide (NAD) to its reduced form (NADH), increasing the redox potential (NADH/NAD) in the liver
3.The increased redox potential inhibits fatty acid oxidation and gluconeogenesis, promoting fat accumulation in the liver

16

17
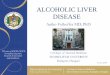
PATHOLOGY •Fatty liver (steatosis)
▫ Initial and most common consequence
▫Macrovesicular fat accumulates as large droplets of triglyceride and displaces the hepatocyte nucleus
▫Usually follows moderate intake of alcohol
▫Rarely causes any symptoms –Does not cause significant liver damage
▫Can be reversed if alcohol consumption is stopped for about 4-6 weeks

Gross
•Large, soft, yellow & greasy
•Fibrous tissue around terminal veins
•Completely reversible
Microscopic
•Microvesicular steatosis
•Macrovesicular steatosis
•Initially centrilobular

Fatty Liver

Microvesicular and macrovesicular Steatosis

21
• Alcoholic hepatitis (steatohepatitis)
•Combination of fatty liver, diffuse liver inflammation, and liver necrosis (often focal)—all in various degrees of severity

22
•The damaged hepatocytes Swollen with a granular cytoplasm
(ballooning degeneration) Contain fibrillar protein in the cytoplasm –
cytokeratin and intermediate filaments(Mallory hyaline bodies)
Severely damaged hepatocytes become necrotic Cholestasis and hemosiderin in hepatocytes Increased Kupffer cells Neutrophilic reaction around degenerating cells Sinusoidal and perivenular fibrosis

23


Mallory Hyaline bodies

26
• Alcoholic cirrhosis
• Advanced liver disease
• Characterized by extensive fibrosis that disrupts the normal liver architecture
• The feeble compensatory attempt at hepatic regeneration produces relatively small nodules (micronodular cirrhosis) - As a result, the liver usually shrinks
• In time, even with abstinence, fibrosis forms broad bands, separating liver tissue into large nodules (macronodular cirrhosis)

Alcoholic cirrhosis

28

29

30
SIGNS AND SYMPTOMS •Symptoms are unique to the severity of the disease•The most common symptoms include
• Pain in the abdomen • Loss of appetite
• A very dry mouth which makes a person feel very thirsty and has to takes water regularly
• Nausea• Jaundice• Sudden weight loss• Tiredness and fatigue• Pedal oedema and ascitis

31
Symptoms usually become apparent in patients during their 30s or 40s
Severe problems appear about a decade later.
Fatty liver asymptomatic.In 1/3 of patients, the liver is enlarged and smooth, but it is not
usually tender
Alcoholic hepatitis ranges from mild and reversible to life threateningUndernourished Fatigue, fever, jaundice, right upper quadrant pain, tender
hepatomegaly

32
•About 40% deteriorate soon after hospitalization
•Consequences ranging▫Mild
eg, increasing jaundice▫Severe
eg, ascites, portal-systemic encephalopathy, variceal bleeding, liver failure with hypoglycemia, coagulopathy

Spider Nevi

Esophageal Varices

Caput medussae

36
DIAGNOSIS•Confirmed history of alcohol use
Chronic consumption of excess alcohol, particularly > 80 g/day
History should be confirmed by family members
• Increase in Gamma Glutamyl Transferase Ethanol induces production of this enzyme more
•Macrocytosis MCV > 100 fL reflects the direct effect of alcohol on bone
marrow Because of Folate deficiency – in undernourished alcoholics

37
•Prolongation of PT▫Coagulation factors I, II, V, VII, VIII, IX, X, XI, XII,
and XIII are synthesized in the liver normally▫When circulating levels of factors I, V, VII, IX, and
X are sufficiently reduced, the prothrombin time (PT) becomes prolonged
▫PT prolongation is related to the severity of liver disease and decreased synthetic activity in the liver
•Decrease in serum albumin▫Because of deficient synthesis

38
•Liver biopsy ▫Confirms liver disease▫Helps identify excessive alcohol use as the likely cause▫Establishes the stage of liver injury
•CT Scan ▫Fatty liver ▫Show evidence of splenomegaly▫Portal hypertension▫Ascites

Cause of Death
•Hepatic coma
•Massive GI bleed
•Intercurrent infection
•Hepatorenal syndrome following alcoholic
hepatitis
•Hepatocellular carcinoma

40
TREATMENT•Abstinence is essential.•Agents to suppress inflammation(corticosteroids).•Nutritional improvement(supplimental amino acids).•Promoters of hepatic regeneration(insulin, glucagon).•Modifiers of metabolism (propylthiouracil).•Fibrosis inhibitors(colchicine).•Anabolic steroids

41
Thank You