Embed Size (px)
Citation preview

September-October 2014 | Volume 39 | Number 5
Mandatory influenza
immunization?
DIGEST
North/South Doctors’ Golf Tournament raises over $37,000
Physicians tee off in support of Alberta’s next generation of physicians
Physicians and nurse practitioners
Working collaboratively for better patient care
Alberta Doctors'
Are you what you eat? The AMA’s Emerging Leaders in Health Promotion
grant recipients say "yes"
Patients First®
Two health professional views

Direct IME:
Is a preferred vendor for many national carriers;
Pays in a timely manner for completed services;
Promotes you and your specialty, educating our
large customer base; and
Manages and assumes the IME services
overhead and expenses for you.
Direct IME is a leading provider of Independent
Medical Examination services in Canada.
Use Direct IME Transcription Service
If you don’t have transcription services, use
ours at not charge. Direct IME uses a
state-of-the-art digital phone in dictation from
Digital Voice Incorporated which is available
24/7. Instructions are provided with every case.
You can use your own phone to call the
dedicated line and dictate as you normally
would. Once you hang up, the dictation is
immediately available to the Direct IME‘s
qualified medical transcription team to
transcribe the dictated report. It’s quick, easy
and free.
To learn more about opportunities with
Direct IME Contact:
Sal Ismail
Email: [email protected]
Phone: 1-403-707-6330
Diversify Your Practice
Direct IME can schedule appointments at your
convenience at dozens of locations and service
centers. We can schedule the service that you
prefer and are qualified to perform such as:
Functional Ability Examinations;
Independent Dental Examinations;
Independent Medical Examinations;
Medical Status Examinations; or
Paper Reviews.
Would you like to diversify your practice?
Does evidence-based medicine interest you?
Would you like to provide IME services?
Join Our Medical Panel
By joining the Direct IME medical panel
physicians and allied health practitioners can
diversify their medical practice without additional
investment or expense.
©2014 Direct IME | 520-63100-505-0007
SOCaicpa.org/socFormerly SAS 70 Reports
AIC
PA Se
rvice Organization Control Reports
S E R V I C E O R G A N I Z AT I O N S
AMA MISSION STATEMENT
The AMA stands as an advocate for its physician members, providing leadership and support for their role in the provision of quality health care.
6 Mandatory influenza immunization? Two health professional views
12 Physicians and nurse practitioners Working collaboratively for better patient care
17 North/South Doctors’ Golf Tournament raises over $37,000 Physicians tee off in support of Alberta’s next generation of physicians
18 Are you what you eat? The AMA’s Emerging Leaders in Health Promotion grant recipients say “yes”
26 AMA Readership Survey 2014 We’re still going strong!
Patients First® is a registered trademark of the Alberta Medical Association.
Alberta Doctors’ Digest is published six times annually by the Alberta Medical Association for its members.
Editor: Dennis W. Jirsch, MD, PhD
Co-Editor: Alexander H.G. Paterson, MB ChB, MD, FRCP, FACP
Editor-in-Chief: Marvin Polis
President: Richard G.R. Johnston, MD, MBA, FRCPC
President-Elect: Carl W. Nohr, MDCM, PhD, FRCSC, FACS
Immediate Past President: Allan S. Garbutt, PhD, MD, CCFP
Alberta Medical Association 12230 106 Ave NW Edmonton AB T5N 3Z1 T 780.482.2626 TF 1.800.272.9680 F 780.482.5445 [email protected] www.albertadoctors.org
November-December issue deadline: October 15
The opinions expressed in Alberta Doctors’ Digest are those of the authors and do not necessarily reflect the opinions or positions of the Alberta Medical Association or its Board of Directors. The association reserves the right to edit all letters to the editor.
The Alberta Medical Association assumes no responsibility or liability for damages arising from any error or omission or from the use of any information or advice contained in Alberta Doctors’ Digest. Advertisements included in Alberta Doctors’ Digest are not necessarily endorsed by the Alberta Medical Association.
© 2014 by the Alberta Medical Association
Design by Backstreet Communications
CONTENTS
FEATURES
DEPARTMENTS 4 From the Editor
10 Health Law Update
14 Mind Your Own Business
16 Insurance Insights
21 Dr. Gadget
23 PFSP Perspectives
29 Residents' Page
3 1 In a Different Vein
34 Letters
34 Classified Advertisements
SEPTEMBER - OCTOBER 2014
3
MORE WAYS TO GET ALBERTA DOCTORS’ DIGESTWe’re using QR codes to enhance your experience. Scanning this code will take you to the Alberta Doctors' Digest page on the AMA website including pdf and ebook versions. There are also QR codes embedded in a few articles in this magazine issue. Scan the codes using your smartphone or tablet device to go to the alternate content. If you don’t have a QR code reader app on your phone or tablet, download one for free from www.scanlife.com.

AMA - ALBERTA DOCTORS’ DIGEST
Our restless search for new ideas and new ways of
doing things is a defining feature of our species. In our pre-history we domesticated plants and animals, subdued fire,
developed language and so on. It is likely our creativity played some role in our displacement of our Neanderthal cousins, who died out millennia ago, while we persisted.
Our creativity hasn’t always helped us health-wise. Trephining skulls, blood-letting and leeches seemed novel, and even auspicious at one time, but were generally harmful and didn’t work. They were supplanted by therapies that were reproducible and based on science. We’ve been left with the public health achievements of better hygiene, clean water and immunization ¬ along with the technical achievements of sophisticated diagnosis, powerful pharmaceuticals, organ transplantation and the promise of genomic medicine.
where dialysis machine inventor, Dr. Willem J. Kolff, had turned his attention to building an artificial heart. Bright, bright people all, I remember, but my take-home message was that these folk and their staff “worked like dogs,” as the saying goes. What is it they say about creativity after all? A smidgeon of inspiration perhaps, but a ton of perspiration.
Eureka moments are few and far between and most creative achievement is based on a step-wise accumulation of small victories. The prototype for discussing creativity in science and in medicine has to be James Watson and Francis Crick’s discovery of the double helical structure of DNA and this is a case in point. Dr. Oswald T. Avery discovered that DNA is the basis for heredity in 1944; Erwin Chargaff discovered the equivalence of guanine and cytosine units, and that of adenine and thymidine units in the early 50s. Linus Pauling described the helical structure of proteins in 1951, and the stage was set for Watson and Crick to outline the double helix a year or so later.
Of course, there’s often real resistance to our creativity, especially as it interrupts the status quo. Thirty years ago Robin Warren saw small helical bacteria in inflamed antral gastric mucosa. Subsequent work with Dr. Barry J. Marshall confirmed the relationship of inflammation with bacteria and changed forever our understanding and treatment of peptic ulcer disease. An enormous corpus of knowledge about gastric parietal cells and their relationship to disease ¬ remember the learned discussions of how much stomach to remove, which little bits of vagus should persist ¬ was rendered redundant and wrong despite the exhortations of surgeons who had grown up in an earlier paradigm.
Now, there is big C creativity, small c creativity and everything in between. If we’re not all capable of E = MC2 types of eurekas, I’m inclined to believe that we’re all happier if we can effect changes that improve matters for our patients and ourselves. Administrators are wont to say that innovation is key to the practice of medicine. I suppose these folk are well intentioned, but they appear disingenuous, since the practice milieu has become more constrained and controlled than ever before. The fixed notion that drives administrators has
FROM THE EDITOR4
Dennis W. Jirsch, MD, PhD | EDITOR
Trephining skulls, blood-letting and leeches seemed novel, and even auspicious at one time, but were generally harmful and didn’t work. They were supplanted by therapies that were reproducible and based on science.
Our unmined creativity
>
No one knows how to spark creativity. As a young researcher I was lucky enough to tour some renowned American research centers. I visited Dr. C. Walton Lillehei’s digs in Minneapolis, then those of vascular pioneer Dr. Frank J. Veith at the Montefiore Medical Center in New York City. After this I went on to see renal transplant pioneer Dr. Joseph A. Murray’s shop in Boston and lung xenografter Dr. James D. Hardy in Jackson, Mississippi before my final stop at Salt Lake City,

SEPTEMBER - OCTOBER 2014
5become a tired fiction: waste is everywhere, cost is everything, control the only salvation. We’ve become a corporate state, relying on care through algorithms that promise standardization and cost control.
The great paradox, of course, is that health care reform is likely endangering our future. The complexity of health care, and in particular the nuances of need and tangled social situations, make new approaches essential. Front-line health care workers (and I include an array of persons here), have unique opportunities to provide insights into patient circumstances and obstacles to care. As stated in PLoS some years ago,1 “Unless exasperated clinicians are able to believe that they can impact some aspect of the way medicine is practiced, nothing will change.”
> We even had “program advisory” committees, though they were never actually charged with real resources or real dollars. To be sure, problems loomed. Trust issues. What to do if a program ran out of money? Equally vexing ¬ what to do if a program actually saved money ¬ who got the reward moolah? As I’ve said, the time and effort spent identifying program personnel were lost, since we never went down that road, but retreated to impatient command-and-control structures that have left us in present circumstances.
People working in the trenches of patient care will not only have an idea about how to do things efficiently, for sure, but they will also know how to do things better.
I’m in favor of small experiments in matters of administration and governance, rather than the fully dressed, large order eruptions we’ve become accustomed to.
Experience at the “coal-face” determines the more intimate understanding of persons actually involved in care. I’m reminded of an afternoon I spent listening to author Frederick Forsyth and his advice for would-be authors when he was drafting a book about stealing a nuclear submarine. How to steal a nuclear sub? Forsyth’s secret: talk to the men who guard the sub; they may not want to steal it but they will surely have an idea about how to go about it.
Forsyth’s insight has to do with the nature of knowledge on the front-lines of an activity and has parallels everywhere. People working in the trenches of patient care will not only have an idea about how to do things efficiently, for sure, but they will also know how to do things better. For real improvement in health care we must find ways to incorporate the experiences of providers and patients alike.
In our search for bureaucratic fixes to health care, we’ve been through radical change in the last two decades, devolving authority at first to multiple regions, and then in a spasm of reversal, we’ve embraced total centralization. Some years ago, midst the hurly-burly that has brought us to this pass, we seemed to be edging toward “program management,” or decentralized governance in which some mix of clinicians would be charged with running clinical activities with minimal outside interference.
It might have worked, given a modicum of patience. But I have to admit perhaps it might not. Accordingly, I’m in favor of small experiments in matters of administration and governance, rather than the fully dressed, large order eruptions we’ve become accustomed to. As Google’s Larry Page has observed,2 “the clash of old rules and rapidly evolving technology leads us to believe that innovative systems of governance could serve humanity better than modern governments do today.” Maybe, as Page goes on to say ¬ just maybe ¬ we should have some safe places where we can try out new things, figure out their effects on society and people without having full deployment in the larger world.
This fires the imagination of the residual researcher in me. Maybe we should try something different. Something less impulsive, less risky and with more promise.
It sounds like hard work to me. It sounds creative.
But hey, we’re not Neanderthals.
Or are we?
References
1. http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.0010034.
2. http://www.change.org/petitions/support-google-ceo-larry-page-s-call-to-improve-governance-with-experimental-zones.

AMA - ALBERTA DOCTORS’ DIGEST
The question of whether health care professionals should be required to be immunized against influenza is a contentious one. In this issue, we present two
different views.
After considerable review and careful reflection, we support a mandatory influenza immunization program for health care workers.
There are very few absolutes in medicine, and influenza immunization is no exception.
Whenever a topic in health care seems complex or when views seem polarized, it can be helpful to focus first on those items we agree upon with reasonable certainty. Consider these three facts:
1. Our shared primary goal, and our responsibility as leaders in health, is to ensure safe patient care. “First do no harm.” In Alberta, we are committed to Patients First®.
2. Influenza virus is common and it causes serious disease. During Alberta’s 2013-14 season, influenza led to 1,133 hospitalizations, 189 intensive care unit admissions and 28 recognized deaths.1 More deaths are attributed to influenza each year in Canada than any other communicable (and vaccine-preventable) disease.2
3. Vaccines protect people from communicable diseases in two ways. They directly protect most vaccinated individuals. There is further indirect protection through “herd immunity” when most of the population is immunized. This is critically important to those at highest risk of serious disease who may not respond directly to vaccination.
If only half a population is immunized (such as the estimated ~ 54% of Alberta health care workers last season1,3,4), then the full prevention potential is not being realized. This is a problem, and it introduces risks and inequities for patients we serve, and for us as motivated care providers, many of whom line-up to obtain our vaccine voluntarily each year.
>
6 COVER FEATURE
Mandatory influenza immunization? Two health professional viewsPart 1: Mandatory immunization ¬ let’s give it a shot
Published evidence and collective experience in North America over the past 30 years demonstrate clearly that education, voluntary campaigns and signing declination forms are not sufficiently effective.
Robyn A. Harrison, MD, FRCPC | COMMUNICABLE DISEASE CONSULTANT, WORKPLACE HEALTH AND SAFETY, ALBERTA HEALTH SERVICES, COVENANT HEALTH
A. Mark Joffe, MD, FRCPC | SENIOR MEDICAL DIRECTOR, INFECTION PREVENTION AND CONTROL, ALBERTA HEALTH SERVICES
With these considerations, an ethical framework5 may further facilitate the decisions at hand.
Why is obtaining annual influenza immunization a good thing and, in fact, the right thing to do?
Influenza immunizations are safe, and they work. Health care workers are at heightened risk for influenza6, and vaccination prevents influenza infections and disease among health care workers.7,8
The vaccine is not perfect. Overall, it is 60% effective2,7 in young healthy individuals with some variation in efficacy year-to-year, resulting from mismatch between circulating strain and vaccine composition. Currently, it is the best prevention we have though and it remains the cornerstone of our interventions for influenza.2
Vaccinating health care workers protects patients. Four randomized controlled trials demonstrate that vaccinating health care workers reduces mortality in long-term care residents.9,10,11,12
In acute care settings, many outbreaks have been reported, some linked to influenza shedding from health care workers.13 When patients acquire influenza in health care settings, the infection can be severe.1,14,15,16

SEPTEMBER - OCTOBER 2014
7> How should the decision to be vaccinated for influenza be made?
Voluntary choice to obtain immunization seems ideal, balancing desire for autonomy with a utilitarian view of the greater good. However, published evidence and collective experience in North America over the past 30 years demonstrate clearly that education, voluntary campaigns and signing declination forms are not sufficiently effective.17,18
As such, values of autonomy stand juxtaposed against the ethics of care, and the duty to care. Freedom to choose, and informed consent are part of our medical culture, but so too is evidenced-based medicine and learning from the experience of others. It is time to look at other models.
We cannot afford to lose public trust on this issue. Many view obtaining immunizations, including influenza immunization, as simple a requirement as scrubbing before surgery.
In a publicly funded health care system, our patients should not have to worry about whether their risk of hospital-acquired influenza is higher at one hospital vs another, or under the care of one physician vs another and so on.
Finally, while our immediate concern is patient safety in our care facilities, an additional longer term benefit of a mandatory immunization campaign for health care workers is the clear message it sends to the public about the legitimacy and overall safety of vaccines in general. Failed voluntary programs do not inspire the public to prioritize immunization. We must do better than that.
So it is after careful reflection that we stand along-side our Canadian Association of Medical Microbiology and Infectious Disease, the Infectious Disease Society of America and an increasing number of other physician organizations and provinces, in supporting mandatory influenza immunization for health care workers.
It is a reasonable compromise, after three decades of failed voluntary programs, and with our focus and goal of patient and worker safety clearly in sight. Getting vaccinated is the right thing to do, and it is time for every health care provider to make it work. In our own view and in the view of the public, it is simply not acceptable to make patients ill. Let us take this step together as physicians, role models and leaders in health.
References available upon request.
Is a mandatory immunization influenza policy a reasonable compromise?
With patient safety our primary focus, it becomes easier to contemplate a “mandatory” approach. Like most things we decide in medicine though, careful analysis of potential risks and benefits remains important.
The benefits are clear. The vaccine works, albeit imperfectly and immunizing health care workers helps to protect patients.
Influenza vaccination is safe and serious adverse events are rare. Concerns about Guillain-Barré Syndrome (GBS) have long been raised, but research has clarified the risk following influenza vaccination to be approximately one per million. The risk of acquiring GBS is now known to be significantly higher from influenza infection than from immunization.19
Some may argue that by removing choice and autonomy we could cause harm. While this may be true, immunization for influenza as condition of employment has been explored and tested in multiple legal and ethical arenas.20,21,22,23 In addition, one only has to read the public response to British Columbia, Saskatchewan or Ontario’s proposed immunization policies to see that the public expects health care workers to be immunized.
We cannot afford to lose public trust on this issue. Many view obtaining immunizations, including influenza immunization, as simple a requirement as scrubbing before surgery. Perhaps there should not be choice involved.

AMA - ALBERTA DOCTORS’ DIGEST
8
Influenza immunization Part 2: Masked workers and veiled politics
Kevin M. Hay, MD
It’s a no-brainer ¬ if you dance to the piper’s tune from British Columbia (BC) and Saskatchewan. They claim that health care workers put patients in so much
danger that we must force them to take the influenza vaccination. Last year BC mandated the flu shot for health care workers, Saskatchewan recently followed suit and there are calls for similar action in Alberta.
Naturally this is based on the premise that everyone is fully protected and safe once the health care worker gets a flu shot.
NOT!
Reality is a bit more complex.
So what is the “modest” benefit from the influenza vaccine? ~30% protection on average. This is far from the Holy Grail of public health.
The big worry for public health officials is the vulnerable patient at risk from influenza, especially within health care facilities. But some of the saddest cases are healthy people in the community who become profoundly ill, or die, from influenza.
For the record:
• The vaccine provides some modest prevention. (The antiviral Oseltamivir is better prevention but not recommended for widespread use.1 Then there are avoidance measures: hand washing, barriers such as masks, etc.)
• The vaccine is presented as the "best" prevention ¬ only true because it is the one generally available prevention.
• I get the flu shot every year unless advised otherwise by the public health nurse (which has happened). And no, I do NOT want to be forced to wear a mask for months on end if told not to take the shot.
• Most everyone should take the shot voluntarily (herd immunity).
• Influenza mutates regularly, which is why we need jabs annually to maintain protection. That’s a hard sell to the skeptics.
• A free society should allow an occasional dingbat to refuse the shot. Those who are prepared to stay and treat patients should have some ability to decide their own fate.
• It is our job to keep up the education and expectation that most rational people will immunize themselves.
So what is the “modest” benefit from the influenza vaccine? ~30% protection on average.
This is far from the Holy Grail of public health.
Each year, scientists choose three strains for the vaccine before that season’s winning mutation is identified. Amazingly, they are correct about half the time. In Canada, vaccine was well-matched in only seven of the last 14 years.2,3
This also means that on average, every other year the shot is practically useless in preventing influenza. According to the Communicable Disease Center, when the prevalent strain in the community matches one in the vaccine (i.e., H1N1), there is about 60% protection from influenza.4 So, over ~two years on average there is ~30% protection per annum (~70% not protected). In 2013, Alberta Health Services had about 117,000 employees.5 If we estimate ~100,000 employees have direct patient contact and are vaccinated with a correct strain, then ~40,000 are still vulnerable to influenza. In a non-matching year all 100,000 are vulnerable.
Alberta Health claims that ~50% of health care workers were immunized last winter.6 I found a clear majority at each of the four meetings where I asked physicians as to how many had taken the shot. Indeed, at the Spring >
COVER FEATURE

SEPTEMBER - OCTOBER 2014
9
A free society should allow an occasional dingbat to refuse the shot. Those who are prepared to stay and treat patients should have some ability to decide their own fate.
2014 AMA Representative Forum, conservatively 80% of doctors indicated that they had taken the shot.
The harsh alternative for BC workers who do not take the influenza vaccine is that they are compelled to wear a mask all the time they are in patient-care areas for the winter months, even though they are healthy.7 That’s a nasty four-month long quarantine. Sounds more like a punishment than a fair public health restriction when, on average, 70% of immunized health care workers are still vulnerable to influenza.
Anyone who thinks it is easy to wear a mask should try a surgical mask or an N95 mask for a few hours. We are not talking about the flimsy ones tourists sometimes wear in public places. Proper masks worn properly are unpleasant for extended periods and interfere with personal interactions.
The shot/mask requirement was stringently enforced in BC. Non-compliant staff were threatened and a few stalwarts fired. These were healthy, non-immunized staff members who refused to accept the mask punishment and then were denied a livelihood.
Influenza circulates through the community during an outbreak and sources to patients include neighboring patients with influenza, visitors, relatives and hospital staff ¬ immunized and not.
So perhaps the politicos should:
• Mandate vaccination for everyone in Alberta.
• Properly isolate the sick ¬ enforced in the community and health care facilities.
• Make everyone in facilities wear a mask full-time for the winter months (including patients, visitors, relatives and staff).
• Allow visitors into health care facilities only if they have proven vaccination.
The limited effectiveness of the vaccine with the very disabling (but thankfully rare) risk of Guillain-Barré
Syndrome gives vaccine naysayers some reason to oppose the shot. One-in-a-million risk is rare ¬ unless you are the one. Some workers in BC/Saskatchewan with relative contraindications to vaccination are now more likely to take the shot simply to avoid the punishment of full-time masking putting their personal health at risk. There is no government insurance for BC physicians who get vaccination side effects. So for example, what resident has insurance to cover such a serious disability?
Focussing on health care workers is a tiny portion of the overall risk here. But we are easy targets. To really deal with the risks to the vulnerable we need vigorous wide-reaching measures. How many can get the flu at a hockey game? About 17,000 in Edmonton and 19,000 in Calgary. And those sorts of numbers spread infection like wildfire.8,9 If we are true believers, why is there no requirement to have a current immunization card to get into Rexall Place and the Scotiabank Saddledome? Closing that big barn door would help, although might annoy 36,128 voters.
References available upon request.
Post Surgical NeedsCompression Garments
Drain Containment Camisoles
Lymphedema SupportSleevesGloves
Donning AidsMedical Compression Stockings
Mastectomy Needs Breast Forms
SwimwearSports Solutions
Sports Injury RecoveryCompression Garments
Braces (ankle, knee, etc.)Hernia Supports
Air Casts
Our team members are certified to provide consultations and professional fittings for your patients.
9309 Macleod Trail SW, Calgary403-299-4488
4938 Richmond Road SW, Calgary 403-252-2266
Products and exceptional service for better health and healing.
>

AMA - ALBERTA DOCTORS’ DIGEST
In August of this year, one of the hot topics for discussion at
the Canadian Medical Association’s (CMA’s) Annual Meeting in Ottawa was the prescribing of medical marijuana by
Canadian doctors. This, in part, was a response to the federal government’s restructuring of Canada’s medical marijuana system in the early part of 2014.
Prior to the restructuring, patients would seek authorization directly from Health Canada to either produce their own marijuana or obtain it directly from suppliers. The changes now essentially make the physician the gatekeeper ¬ patients need to obtain a prescription from their physician which, in turn is then submitted to one of an increasing number of federally licensed growers. This has caused significant discomfort for many physicians who simply are not satisfied that the science supports the use of this drug. Even if it did, do the supposed benefits of marijuana use outweigh the known risks?
Dr. Louis Hugo Francescutti, then the outgoing president of the CMA, stated it this way: “It’s just bad medicine to be asked to authorize a product when we don’t know how it works, we don’t know when it works, for whom it works. Where are the studies? We try to base what we do on evidence.”
Another concern expressed by Dr. Francescutti is that doctors will face enormous pressure from patients who insist that marijuana helps them, and a regime that he says “calls on doctors to ‘blindfoldedly’ prescribe a medication.” He fears that patients frustrated by physicians’ refusal to prescribe will turn to emergency departments.
Finally, Dr. Francescutti raised an interesting collateral issue ¬ that of the safety of smoking itself. Even assuming the use of marijuana was clinically proven to be beneficial, he wishes there were ways to administer it other than as a drug to smoke. “If we could deliver it through a cookie or a milkshake or a pill or a liquid, and we know that it works, well we would welcome it with open arms because it’s another tool we can use.
At the same conference, Health Minister Rona Ambrose refuted Dr. Francescutti’s concerns, saying, “Health Canada does not endorse the use of marijuana, nor is it an approved drug in this country, nor has it gone through any of the clinical trials that other pharmaceutical products that are approved in this country have gone through.”
10 HEALTH LAW UPDATE
I get high with a little help from my… doctor?
>
Jonathan P. Rossall, QC, LLM | PARTNER, MCLENNAN ROSS LLP
It’s just bad medicine to be asked to authorize a product when we don’t know how it works, we don’t know when it works, for whom it works. Where are the studies? We try to base what we do on evidence.
In the meantime, medical marijuana suppliers are becoming increasingly aggressive. A simple Google search of “medical marijuana” reveals numerous websites dedicated to advocating the use of this drug. Much of this advocacy is focused directly on physicians.
One example: “For the sake of our patients we strongly encourage you to be open to learning first-hand the medical benefits of marijuana. If you sign the Marijuana

SEPTEMBER - OCTOBER 2014
11
Medical Access Regulations forms, thus allowing your patients to try medical marijuana as an alternative, you are helping them into the only legal program that allows them to be exempt from the criminal code of Canada for their prescribed amount. This exemption is valid for one year. Many doctors fear Health Canada and opt to only sign forms for compassion clubs, however this does not exempt your patient from possession charges and they may be harassed or arrested.”
This is not the first time that a pharmaceutical manufacturer has put pressure on physicians to utilize its product. However, it is arguably the first time that the manufacturer of an otherwise illegal and largely untested product has done so. Adding to the theatre of the absurd, Ross Rebagliati is the founder of Ross’ Gold, a “budding” BC company seeking to license a brand system distribution process for medical marijuana in Ontario. Readers may remember Mr. Rebagliati as the Canadian Olympic champion snowboarder who was notoriously stripped of his gold medal in Nagano, Japan in 1998 (only to have it returned when it came out that tetrahydrocannabinol [THC], the active ingredient in marijuana, was not a banned substance).
And, just when you thought that all the interest groups were accounted for, in steps organized crime who sees the growing and sale of medical marijuana as a “growth” industry. According to RCMP, many criminal organizations are using licensed medical marijuana grow operations as a front for the more lucrative growth and sale for non-medical purposes.
All of this raises very interesting and complex legal and ethical issues, all against a political backdrop where the leader of the federal Liberal party is advocating the de-criminalization of marijuana. This should remind us to pause and reflect on the fact that, like it or not, possession and trafficking in marijuana is still a criminal offence in Canada. As Dr. Francescutti points out, doctors are being put in the very uncomfortable position of being asked to prescribe an otherwise illegal drug, largely untested, for a variety of ailments with only the benefit of anecdotal evidence to support the use.
> Doctors are being put in the very uncomfortable position of being asked to prescribe an otherwise illegal drug, largely untested, for a variety of ailments with only the benefit of anecdotal evidence to support the use.
CANADA’S HEALTHCARE LANDLORD
LOOKING TO SET UP YOUR PRACTICE? WE’RE JUST WHAT THE DOCTOR ORDERED.
NORTHwEST HEALTHCARE pROpERTiESOur in-house property management and leasing teams can accommodate all your office or clinic space requirements.
We Provide:•Competitiveleaserates•turn-keyConstruCtionavailability•attraCtivebuildingamenities
For leasing inquiries Please call:Lindsay Hills, Leasing Manager, Calgary 403-282-9839 ext.3301Shelly Fedorak, Leasing Manager, Edmonton 780-293-9348
www.nwhp.ca
•Calgary•toronto•montreal•Halifax
#70, 585 St. Albert Trail, St. Albert, AB
Competitive lease rates.
Walking distance of Sturgeon Community Hospital, Dynacare Kasper Labs, and Medical Imaging Consultants.Generous TI and Free Rent o�ered.
Medical or Laboratory Space
2,319 sq. ft.
FOR LEASE
CALL ANYTIME FOR A VIEWINGAND MORE INFORMATION
Corner unit with great exposure and two entrances
St. Albert rated the best city to live in Canada in 2014 (Money Sense Magazine)
Nama Properties [email protected](877) 977-NAMA (6262)
SIERRAS OF INGLEWOOD

AMA - ALBERTA DOCTORS’ DIGEST
12 FEATURE
Physicians and nurse practitioners Working collaboratively for better patient care
Health care delivery is evolving rapidly in Canada and this is linked to factors such as new models of care, technological innovations, new regulations
or requirements, expanding scopes of practice of non-physicians and evolving patient expectations.
An important change for physicians is the expanded role of nurse practitioners (NPs) in many Canadian jurisdictions, including Alberta. NPs in the province are regulated independent health professionals licensed by the College & Association of Registered Nurses of Alberta (CARNA). NPs can work autonomously and they also work with other health care providers.
For physicians, the role of NPs reinforces the importance of understanding and respecting scopes of practice, and how to best reduce medico-legal risk when patient care is provided by multiple health care professionals. While inter-professional care requires effective coordination and communication, when this is achieved, patient care is generally enhanced.
Nurse practitioners in Alberta
In Alberta, NPs work in various settings such as community health centers, clinics, urgent care centers, public health units, long-term care facilities, and hospital in-patient and outpatient units. NPs are also part of inter-professional teams in primary care networks and family care clinics.
As regulated independent health professionals, NPs can work independently within their legislated scope of practice and the limits of their training and experience. NPs working outside of their scope of practice can only do so with a medical directive and appropriate supervision. The Health Professions Act (HPA) and the Registered Nurses Profession Regulation outline the legal authority for NP’s scope of practice.1 Moreover CARNA's Scope of Practice
for Registered Nurses outlines the scope of practice for registered nurses.2
Currently, NPs in Alberta perform a range of clinical duties, such as ordering diagnostic tests, prescribing medication, managing chronic disease, monitoring client outcomes, providing continuing care, consulting and referring patients to physicians, and other health care providers.
An important change for physicians is the expanded role of nurse practitioners (NPs) in many Canadian jurisdictions, including Alberta.
Collaboration and communication between physicians and nurse practitioners
Physicians and NPs should collaborate and cooperate to deliver effective and efficient patient care. It is important to delineate the roles and accountabilities of physicians and NPs within the health care team. Physicians should be aware of any guidelines in their hospital, clinic or regulatory authority concerning collaborative care. Some hospitals and clinics have policies and procedural frameworks that are specific to the physician-nurse collaborative relationship. It is also important to determine early on who is the most responsible practitioner.
A physician’s and NP’s scope of practice may sometimes overlap, such as when both professionals may carry out a specific intervention (e.g., ordering a diagnostic test or assessing a change in the patient’s condition). A common understanding on the part of all team members about roles and accountabilities will help to coordinate care, enhance patient safety and reduce medico-legal risk. >

SEPTEMBER - OCTOBER 2014
13Clear, timely, and respectful communication between physicians and NPs is vital. When collaborating in the care of a patient, the physician and the NP must also explain their functions and responsibilities to the patient and should inform the patient to whom he or she should address any questions or concerns. The goal of inter-professional care is to improve outcomes for patients.
Physicians should always document all relevant clinical activities and discussions in the patient’s health record.
5. Review the patient’s health record and conduct a clinical assessment of the patient.
6. Document the consultation in the patient’s health record.
Risks and accountability for patient care
Each health care professional, including the NP, is accountable for his/her decisions and actions. The courts have determined physicians working in collaborative practice are not required to check the work of other independent health care professionals, such as NPs, who are providing care within their scope of practice.
All health care professionals should have adequate liability protection. The Canadian Medical Protective Association (CMPA) and the Canadian Nurses Protective Society have published a joint statement on liability protection for doctors and nurses in collaborative practice. An updated version can be found on the CMPA website.
Physicians with questions about inter-professional care and working with NPs may contact the CMPA. More information on inter-professional care, the most responsible practitioner and improving communication is available on the CMPA website at cmpa-acpm.ca.
References
1. College & Association of Registered Nurses of Alberta, “Scope of Practice.” Retrieved on May 8 2014 from: http://www.nurses.ab.ca/Carna/index.aspx?WebStructureID=3074
2. Ibid.
>
Each health care professional, including the NP, is accountable for his/her decisions and actions.
SHORT AND TWEET!
Get the latest AMA news in 140 letters or lessTwitter is a great way for you to get the latest AMA: • News, events and announcements.• President’s Letter and other publications.• Important information from other medical associations.
How can you find us?• Already have a Twitter account? Follow us at
twitter.com/albertadoctors.
Scan to go directly to the AMA's Twitter account, or visit us at twitter.com/albertadoctors.
• Don’t have a Twitter account? Signing up for Twitter is fast, easy and free. Just go to twitter.com. You can open an account in under a minute.
Check in regularly at twitter.com/albertadoctors or see the most recent tweets on the AMA website, e.g., the Twitter box on www.albertadoctors.org/media-publications.
We tweet new items almost every day. Join us!
Providing consultations to nurse practitioners
When asked to consult, physicians should consider the following activities:
1. Review policies related to inter-professional care to become familiar with the scope of practice of NPs.
2. Establish a mutually agreed-upon process for consultation with NPs.
3. Identify the reason for, and the level of urgency of, the consultation.
4. Understand the level of consultation requested (e.g., an opinion, recommendation, concurrent intervention or immediate transfer of care).

AMA - ALBERTA DOCTORS’ DIGEST
It is likely that you’re working with several generations in your
work environment. It’s not uncommon for four, or possibly five, generations to be working side-by-side. This presents some challenges but also great opportunities for leveraging diverse skills and strengths.
Each generation is shaped through their shared experiences and values which in turn influence how they interact and are motivated in the workplace. Understanding the strengths and motivators of each generation is important to achieving cohesiveness and effective working relationships.
Practice Management Staff
to work alone to get the needed result. Generation Yers respond well to workplace structure, challenges and coaching. Similar to Baby Boomers, they work well in team situations.
Work/life balance has a different meaning to each generation. It’s no surprise: Veterans and Baby Boomers believe hard work leads to success and expect to adapt personal life to the needs of the organization. Generation Xers enjoy challenging work but want balance in their lives. While Generation Yers, are committed to their careers but expect the flexibility of time and technology.
Communication
Proving effective feedback to different generations varies by generation. Veterans tend to operate on the premise that “no news is good news” and expect feedback only when a goal is met. Baby Boomers expect corporate accomplishments to be recognized through promotions, a hierarchy of titles and yearly pay raises. Generation Xers and Generation Yers both seek immediate and continual feedback to assure they are on target with organizational goals. Generation Yers have been raised with high expectations and abundant praise; they appreciate immediate rewards and feedback.
Finding the right method or approach to communicating with the various generations can be challenging. The Veterans are used to formality ¬ a memo, personal conversation or a phone call. Baby Boomers also respond best to personal contact but have adapted to voice mail and email. Generation Xers expect direct, immediate response that email and instant messaging bring, while Generation Yers and millennials have been communicating via technology all their lives. They are most comfortable with cell phones, texting and utilizing social networking.
Relationships
The explosion of social media has heralded the arrival of the virtual relationship and Generation Yers are leading the charge. Generation X/Baby Boomers are more likely to a value fewer, more personal relationships over an extended network of affinity-based connections.
Embracing a multi-generational workforce: Here’s how to do it
MIND YOUR OWN BUSINESS14
>
Understanding the strengths and motivators of each generation is important to achieving cohesiveness and effective working relationships.
Five generational categories are generally recognized:
• Veterans (born 1930-45)
• Baby Boomers (born 1946-64)
• Generation Xers (born 1965-76)
• Generation Yers (born 1977-90)
• Millennials (born since 1991)
Work style
Each generation tends to have a preferred work style. Veterans prefer detailed directions and guidance. Baby Boomers work best in teams, value meetings and ask for direction when needed. Generation Xers, many of whom grew up as “latchkey” kids, are independent, resilient and adaptable. They work best when they are empowered

SEPTEMBER - OCTOBER 2014
15Expectations on how to manage conflict also vary by generations. Veterans grew up respecting authority and utilizing the corporate chain of command to resolve conflict. Baby Boomers tend to value team consensus. Generation Xers prefer to resolve problems immediately and directly, while Generation Yers proactively utilize the conflict management skills taught during school years.
Managing the generations
The conventional employer relationship is not necessarily a thing of the past, but it is no longer the standard ¬ or won’t be for long. We need to recognize this as not just an adjustment in leadership, but a cultural shift in the workplace. While the roles of employee and manager will continue to morph, the dynamic will always be there.
> • “Do as I say, not as I do” won’t work ¬ the new generation is bright, they watch and learn. If they desire reasons for why we do things, tell them.
• Tap into their skills and social influence ¬ this generation grew up with advanced technology and instant access to information. They want to make a difference and they follow trustworthy leaders.
Here are some suggestions if you are part of Generation Y/Millennial generations:
• Be patient ¬ it takes time to earn trust and to impress people with your abilities. Being patient will pay off in long-term confidence in you.
• Limit texting to your personal life ¬ although texting is your norm, the abbreviated style of texting to communicate is typically not well received in most businesses and may be viewed as ambivalence. Full sentences please ¬ LOL.
• Pursue mentors and advocates ¬ there is enormous value in having experienced guides to help you navigate your career. Many leaders are willing to be a mentor, but you must win their advocacy first by showing your commitment to the relationship.
• Embracing the generations can be effective and powerful in your organization. When creating a new project or solving a problem, develop teams that draw from a cross-section of skills and ages to maximize the strengths of each generation.
• Finally, keep in mind, no matter what generation you are working with, everyone likes to feel engaged and valued. Clear and good communication can go a long way, no matter how old or young one is.
Here’s to finding our way forward together!
No matter what generation you are working with, everyone likes to feel engaged and valued.
Here are some suggestions if you are part of the Veteran/Baby Boomers/Generation X generations:
• Start listening; stop assuming. Engage younger employees and listen to what they have to say.
• Start viewing Generation Y as a strategic business investment ¬ invest resources and time in engaging, training, developing and retaining our future leaders. They will someday run our organizations!
Are you looking to lease or purchase a new or pre-owned vehicle?
– Top price paid for your trade. – No shopping dealership to dealership.– Delivery available to your hometown.
– No hassles.– Factory incentive programs.– All makes offered.
“Let my 40 years of Auto Experience and Fleet Connections work for you. I will save you time and provide a no pressure quote on any vehicle.”
David Baker spouse of Dr. Karen Bailey knows first hand that a physician’s time is valuable. He has helped many physicians
in Alberta obtain their vehicle of choice without any hassle.
Call: 1.888.311.3832 or 403.262.2222Email: [email protected]: www.internationalmotorcars.caMANY REFERENCES AVAILABLE

AMA - ALBERTA DOCTORS’ DIGEST
In this edition of Insurance Insights, I would like to briefly
let you know how to securely access and make changes to your home or auto insurance coverage 24/7. How easy can it
be? Here’s what you can do with MyInsurance from TD Insurance:
• Log-in and review your coverage.
• View your billing details.
• Change your address.
• Modify home coverage (perhaps you just put new shingles on).
• Add a driver (new driver in your home).
• Add or substitute a vehicle (new car).
• Download a temporary pink card (can’t find your existing one?).
• Obtain a quote for auto, home, all-terrain vehicle or motorcycle.
• Ask questions.
Visit myinsurancecpo.td.com. All you need is your TD Insurance Meloche Monnex policy number.
INSURANCE INSIGHTS16
Don Warden | SENIOR MANAGER, AFFINITY MARKET GROUP, TD INSURANCE MELOCHE MONNEX
You’re in control and we’re good with that: Making changes to your home or auto policy
MEDICAL SPACEFOR LEASE
For more information, please contact:
(780) 420 - 1177
www.cwedm.com
IMMEDIATE POSSESSION
EXCELLENCE PROFESSIONAL CENTRE5603 - 199 Street, Edmonton, Alberta

SEPTEMBER - OCTOBER 2014
FEATURE 17
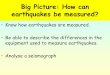
Physicians, medical students, residents and community leaders from across the
province hit the links July 28 at the Red Deer Golf and Country Club for the 87th Annual North/South Doctors’ Golf Tournament.
The tournament, co-hosted by the College of Physicians & Surgeons of Alberta (CPSA), Alberta Medical Association and Canadian Medical Foundation raised funds for Alberta medical student bursaries and physician health programs.
Golfers enjoyed 18 holes of golf, buffet breakfast, BBQ lunch, a silent auction and many draw prizes.
Congratulations to the skilled golfers and draw prize winners and thank you to everyone who participated. We hope to see you out on the course again next year!
North/South Doctors’ Golf Tournament raises over $37,000 Physicians tee off in support of Alberta’s next generation of physicians
Presenting sponsor
Birdie sponsors
Par sponsors
A special thank you to all of our sponsors for their generous support, including:
Getting ready to hit the links. ( provided by CPSA) Dr. J. Guy Gokiert is happy with the great day. ( provided by CPSA)
Warming up. ( provided by CPSA)

AMA - ALBERTA DOCTORS’ DIGEST
18 FEATURE
Cooking with Ravi'oli
In the warmth of the kitchen in a women’s shelter in northern Alberta, Ravi Seyed Mahmoud, third-year medical student in the University of Alberta’s
Integrated Community Clerkship program, imparted valuable, healthy food preparation skills and in the process, set the stage for the formation of friendships.
Its primary purpose was educating and encouraging women and mothers to cook healthy meals for themselves and their families. Secondary was using the activity of cooking together as the basis for forming friendships and positive relationships. Ravi Syed Mahmoud’s Cooking with Ravi’oli project perfectly fit the requirements of the Alberta Medical Association’s (AMA’s) Emerging Leaders in Health Promotion grants program:
• Promote development of the physician’s role as advocate for healthy populations.
• Provide experience in health promotion as integral to medical practice.
• Facilitate growth of leadership and advocacy skills in a mentored environment.
“I wanted to plant the seed of an idea that cooking inexpensive, fresh meals was an attainable goal,” explains Ravi. “Diet is a major determinant of health for a mother and her children. I wanted to show that quality cooking is not difficult or inaccessible and that cooking fresh meals is a better option than buying processed, instant foods. Fast, easy, affordable and delicious ¬ that was my mantra for this project.”
“And my more subtle, second purpose,” Ravi continues, “was to have the cooking, cleaning and eating that would result from this project help promote and foster positive relationships among the participants and the staff.”
With these goals in mind and the encouragement of project mentor Dr. Harvey P. Woytiuk, Ravi began in January by meeting with the director of the Columbus
Are you what you eat? The AMA’s Emerging Leaders in Health Promotion grant recipients say “yes”
House of Hope (CHH) in St. Paul, Alberta to discuss his Cooking with Ravi’oli project. The CHH is a center of refuge and rescue for women in crisis and/or situations of abuse, with or without children. It provides short-term accommodation (average stay is 11 days), referrals and a 24-hour crisis line. The average guest age is 25-40; most guests have two or three children. Columbus House of Hope has a large kitchen and dining room, as well as educational and recreational facilities.
I’m more mindful of the role social determinants of health play in a person’s eating habits; realities such as not having a car, fridge or freezer, running water or the ability to read…
>
The director, plus all staff and guests were supportive of Ravi’s plan to attend the CHH every second Monday evening, to work with CHH guests for about two hours, guiding them in the preparation of deliciously simple (and simply delicious!), healthy and economical meals, to be served to the rest of the CHH guests, staff, children ¬ and Ravi.
“I conducted eight sessions with different house guests, informally coaching them in techniques for preparing a variety of healthy, family-friendly entrees based on a selection of culturally diverse recipes, including fajita chicken, butter chicken, taco salad, baked salmon, shepherd’s pie, chicken stir-fry, breaded fish fillet and beef kabob.
Responsible for all planning, logistics and leading/directing the cooking sessions, Ravi called extensively on his background of “apprentice” cooking with his parents during his teen years.

SEPTEMBER - OCTOBER 2014
19“Every night, I was responsible for helping with the cooking and although I didn’t appreciate the extra work at the time, I now have over a decade of cooking experience that I applied to this project. I also continue to apply it to my own life, cooking one or two full, three-course meals, daily.”
On his Cooking with Ravi’oli days, Ravi would phone the CHH and find out how many women, children and staff would be there at meal time. He would then purchase groceries, take them to the house and with his (normally) two participants, discuss the day’s entrée, including the cost of the groceries and directions on how to prepare the dish. While Ravi guided the participants through the various steps of the meal preparation process, participants were encouraged to carry out as many of the tasks as possible, with Ravi stepping in to assist with cooking, clean-up or other tasks, only when required. Staff always ate with participants, as a gesture of goodwill and unity.
After the participants had set the table and served the meal to house staff, other guests, children and Ravi, clean-up fell to the guests, particularly those who hadn’t been involved in the cooking.
Upon project wrap-up in mid-May, Ravi reflected positively on the experience.
“It was very rewarding, the food was consistently good, the participants enjoyed themselves and learned from the process and the CHH staff was pleased with the results,” Ravi commented. “And although I didn’t solve the problem of poor nutrition in St. Paul, I like to think that I prompted a handful of women to seek less expensive, healthier options when it comes to eating and nourishing themselves and their families.”
Good food CAN come in a box!
This good news is true, particularly when the box is full of fresh fruits, vegetables and dairy products, complete with recipes. Even better, it comes with a how-to workshop led by Peace Regional Good Food Box program leader Charley Switzer, a third-year medical student completing her Integrated Community Clerkship at the University of Alberta.
What originally began as a plan to provide 15 low-income families in Peace River with a subsidized box of produce (the “Good Food Box”) for five months, grew to reach over 60 families (150 individuals) in the area. As she focused on exposing low-income families in Peace River to the affordability and healthful living benefits of purchasing and eating fresh produce, Charley also addressed preparation, cleaning and storage of the produce with her monthly, themed workshops, recipes and tip sheets.
“We found that by providing the necessary tools ¬ in this case, the produce, recipes, tips, instructions and guidance ¬ we were able to achieve our desired results: the adoption by many area families of new, healthy habits,” says Charley. “And an added bonus of the program was introducing new foods to many of the participants, such
>
>
“Cooking with Ravi’oli creator Ravi Seyed Mahmoud, third year medical student, U of A’s ICC program. ( provided by Ravi Seyed Mahmoud)
Caution: Do not view this photo of one of Ravi’s many, delicious dishes on an empty stomach! Yum! ( provided by Ravi Seyed Mahmoud)

AMA - ALBERTA DOCTORS’ DIGEST
20 “The experience with produce purchase and preparation really varied,” notes Charley. “Some cut pineapple for the first time, they learned how to read food labels and discovered new uses for expired dairy products.”
In keeping with a requirement of the ICC program to partner with a community organization, Charley worked closely with the Sagitawa Friendship Centre in Peace River ¬ Tracy Zwiefel, executive director and Karen Watson, secretary ¬ to deliver the Good Food Box program. Staff from the centre picked up the groceries from local grocer, Freson Brothers, and brought them back to the centre, where program participants and their families gathered for the workshop and to assemble their boxes. Many of the participant families were already connected with the Sagitawa Friendship Centre, through the centre’s I-Cook class and youth Food Fight class. The centrally located Sagitawa Friendship Centre also advertised the program and collected box orders and payments prior to each workshop and box delivery.
Dr. Dave L. Willox was Charley’s project mentor. As a Peace River native, Dr. Dave was an invaluable resource and aide for Charley, as he identified community networks for advertising, had a keen understanding and appreciation of the community’s needs and assisted with culturally relevant tips and recipes.
Working with and leading a good team left a lasting impression on Charley, who describes herself as being “much better as a leader in trusting the work done by my teammates. I relied upon them to help implement this project and in the process, learned that delegating tasks and trusting your team is key.”
Charley views her Good Food Box program as a win-win, with its significant value to the community balanced by its immeasurable value to her, as she observed the relevance and benefits of tailoring health projects to the community’s needs, rather than to her own (or someone else’s) agenda.
“I’m more mindful of the role social determinants of health play in a person’s eating habits; realities such as not having a car, fridge or freezer, running water or the ability to read ¬ all these things make it far more challenging to make and follow through on healthy choices,” she comments. “As a result, I find myself taking the time to examine each person’s situation before I offer advice, to try to ensure it’s relevant to them.”
Based on the program’s positive reception and success, the Sagitawa Friendship Centre plans to continue the Good Food Box program this fall, using community-based fundraising to sponsor the program for approximately nine months.
In addition to “helping me see how my role as a future physician can affect change at the community level,” the program’s success also reminded Charley of “the utility of small, grassroots projects and the larger ripples they may have. I’m more encouraged to envision change now; to be a do-er rather than a talker.”
>
By providing the necessary tools – in this case, the produce, recipes, tips, instructions and guidance – we were able to achieve our desired results: the adoption by many area families of new, healthy habits.
“Good Food Box” creator Charley Switzer, third year medical student, U of A’s ICC program, with two friends from the Peace River SPCA. ( provided by Charley Switzer)
Overflowing with goodness, Charley’s Good Food Box helps start healthy habits for a Peace River family. ( provided by Charley Switzer)
20
as cantaloupe, flavored yogurt, butternut squash, fresh pineapple, broccoli and sweet potatoes.”
Containing $30 worth of produce at a participant cost of $15, Charley aligned the contents of the Good Food Boxes with in-season produce, sale produce and her selected recipes. The purpose of requiring participants to contribute half the cost of the boxes was so they would “have some ownership” in their boxes, Charley explains. The workshops were a vital component of the program, as simple tip sheets and hands-on instruction and participation helped bridge the variety in the participant’s educational backgrounds.

SEPTEMBER - OCTOBER 2014
Technological advances have been key in
the development of civilization and progress throughout man’s existence. Ancient Egyptians, for example,
became adept in working with iron and went on to invent several types of simple machines including chariots, which brought about the conquest of surrounding nations. Other advances in astronomy, navigation, ship building, architecture, mathematics and medicine contributed to a dynasty lasting over 1,000 years, with remnants still considered some of the “Wonders of the World” today. Surrounding nations, in order to compete, developed their own technological advances, building on those of Egypt and others.
Technology has never advanced as rapidly, or in as many fields, as we are experiencing in modern times. Specifically, some of the more recent technological advances in modern medicine are:
• 3D printing technology of organs, including, more recently, living cells.1 This technology has also helped surgeons to improve surgical techniques.2
• The ability to diagnose malaria using a smartphone.3
• Digital pills that transmit a signal when exposed to the acidic fluids of the stomach, which is then transmitted to the care provider to monitor patient compliance.4
• A “wearable, bi-hormonal, automated, bionic pancreas” which, in early trials, seems superior to insulin pump therapy.5
• The production of a smart contact lens that will not only treat farsightedness, but also monitor blood glucose levels.6
There are numerous other advances including iPhone attachments to auscultate and visualize cardiac murmurs or to diagnose ophthalmic disease in third-world countries and many more. Some of these innovations will go on to be game changers, others will make their
inventors rich and famous, while others will simply be considered good ideas that were ahead of their time.
As technology advances rapidly, our physician-patient relationship remains our anchor
DR. GADGET 21
Wesley D. Jackson, MD, CCFP, FCFP
Technology has never advanced as rapidly, or in as many fields, as we are experiencing in modern times.
>
I would like to make three observations regarding technological advances:
1. In July 1969, using less computing power than a modern USB stick, NASA was able to put a man on the moon. Today’s tablets are much more powerful, but it seems that Angry Birds Space (and other well-written apps) can be somewhat distracting. In order to make advances in modern times, more focus on our goals is required than ever before.
2. Ancient Egypt, despite being in possession of superior technology, succumbed to the common tendency to look inward for advances. As such, it did not collaborate with surrounding countries, choosing instead to dominate rather than cooperate. This eventually led to the fall of arguably one of the greatest dynasties that has ever existed. This pattern has repeated itself throughout known history.
3. Hippocrates, a Greek physician who lived about 400 years BC, is referred to as the “Father of Western Medicine.” His teaching and theories revolutionized medicine in ancient Greece and laid the groundwork for many of our current practices. He was able to use the technological advances of his time and apply and adapt them using his own theories. He is credited with penning the Hippocratic Oath, which, while briefly mentioning some of the technologies of the time, focuses squarely and appropriately on the importance of professionalism and the physician-patient relationship, making it still very valid today.

AMA - ALBERTA DOCTORS’ DIGEST
22
Modern medical technology will continue to grow at an exponential rate, making it almost impossible for the average physician to stay abreast. In the future, physicians will need to incorporate at least some of this new technology into their practices. In order to do so successfully, physicians will need to be very focused
> Some of these innovations will go on to be game changers, others will make their inventors rich and famous, while others will simply be considered good ideas that were ahead of their time.
Family Physician Locum Opportunity
The Leduc Beaumont Devon Primary Care Network (LBD PCN) is a joint ven-ture between participating local family
physicians and Alberta Health Services. Our mandate is to sustain and enhance the quality, coordination and integration of health care services in Leduc and area and to improve the quality of life for the community of patients and physicians.
The LBD PCN is looking for long term locums to help support our group of 50 family physicians. Locums would be asked to sign a contract (negotiable but ideally 3-12 months), and to be available to provide locum coverage preferentially to our LBD PCN physicians. We are seek-ing physicians wanting to practice full-scope family medicine, including inpatient care, ER, and long term care with the added support of our multi-disciplinary team. We provide favourable compensation with an additional $500 per week available to help defray overhead costs. CME benefits of $2500 per year would be provided to locums working for our group more than 42 weeks per year. Start dates are flexible. Get involved with primary care reform, in communities offering the challenge and diversity of rural care, but right in your back yard. Please forward a letter of interest and resume to:
Len Frank, Executive Director#301, 4710-50 Street Leduc, AB T9E 6W2Phone: 780-980-8800 Fax: 780-986-6634 Email: [email protected]
Only candidates selected for an interview will be contacted.
“Please call me to
experience the dedicated,
knowledgeable, and
caring service that I provide
to all my clients.”
Ann DawrantAnn Dawrant
Websitewww.anndawrant.com
• Consistentlyintop5%ofEdmontonrealtors
• PrestigiousRE/MAXPlatinumClub
• 28yearsasasuccessfulresidentialrealtorinwestandsouthwestEdmonton
• BornandraisedinBuenosAiresandhaslivedinEdmontonsince1967
• BilingualinEnglishandSpanish
RE/MAXRealEstateCentre780-438-7000 - office780-940-6485 - cell
on appropriate goals, be willing to collaborate openly and freely, and, most of all, remember that “in every house where I come I will enter only for the good of my patients, keeping myself far from all intentional ill-doing...” (Hippocratic Oath).
References
1. http://pubs.acs.org/doi/abs/10.1021/la501430x.
2. http://www.cnet.com/news/3d-printing-helps-surgeons-save-5-year-olds-life/.
3. http://ychacks.challengepost.com/submissions/ 25781-athelas.
4. http://www.proteus.com/technology/digital-health-feedback-system.
5. http://www.nejm.org/doi/full/10.1056/NEJMoa1314474.
6. http://www.novartis.com/newsroom/media-releases/en/2014/1824836.shtml.

SEPTEMBER - OCTOBER 2014
We can thank Homer for giving us two
common metaphors for life: the battle and the journey. That’s Homer, the Greek writer of The Iliad and The Odyssey not Homer Simpson, his
namesake and contemporary antihero. Our news media prefer stories of war and conflict, and some days a life in medicine can seem like a series of battles. The battle or the journey ¬ what’s your preference?
Speaking of journeys, physician friends of mine are just back from a combo trip/conference in Istanbul, Turkey. A friend phoned me recently while attending a medical meeting in New York. Last evening I said, “Have a good trip,” to a colleague and his spouse driving to Nelson British Columbia (BC) for a mid-summer weekend with friends. My wife and I will be leaving town and country next week for some extended “overseas” travel.
Not too long ago I spoke to a group of surgeons about travel experiences in our lives, especially those travel opportunities that recur over the span of a career in medicine. Many physicians and their families are members of a fortunate minority of tourists who have time, motivation and income to leave homes and offices, and set off for just about anywhere on planet earth.
While acknowledging our freedom to travel, it’s good to ask ourselves a few questions before we pass through security en route to the departure lounge. What kind of journeys appeal to you in your life situation and career stage? There are the obvious questions about continuing medical education (CME) destinations: Will it be the Canadian sub-specialty meeting in Toronto, or an update on ebola (and a Spurs game) in San Antonio, or a “live and learn” family ski weekend at the scientific assembly in Whistler, BC?
Necessary journeys
Writer and restless traveler Bruce Chatwin quotes Blaise Pascal: “The sole cause of man’s unhappiness is that he doesn’t know how to rest quietly in his room.” I recently submitted an abstract for a presentation at the September 2014 International Conference on Physician
Health in London, United Kingdom.1 I proposed leading a discussion about the healthiness or not of traveling long distances to attend international physician health conferences. Even though my proposal was rejected, I still think it’s worth doing a rudimentary cost/benefit analysis of some of our travel plans.
Is your life a battle or journey?23PFSP PERSPECTIVES
>
Many physicians and their families are members of a fortunate minority of tourists who have time, motivation and income to leave homes and offices, and set off for just about anywhere on planet earth.
Vincent M. Hanlon, MD | ASSESSMENT PHYSICIAN, PFSP
A surgeon told me she’s seriously considering a “stay-cation” the next time the conference travel bug bites. The exhaustion from a week of disrupted sleep for her and her young daughter while recovering from eight time zones of jet lag was too great a price to pay to attend a specialty meeting with her family. A few years ago, Granta The Magazine of New Writing published a collection of essays and stories called Necessary Journeys. These are journeys that we feel a need to make. Leaving aside basic questions of where and when to go, what do we consider necessary journeys in our lives?
To what extent do our various perambulations (for pleasure, professional development or other reasons) contribute to our health, happiness or fulfillment? Do they restore energy, provide meaning, or give direction to our lives? Here I’m borrowing questions that recur in the work and writing of Dr. Rachel Remen.2 Maybe leaving home is a quest for healing when surprised by illness, or a chance to check out an exotic time-share “opportunity” in Fort Lauderdale, Florida ¬ always “at no cost to you.” It could be a brief getaway from the stress of practice, or part of a deliberate and lifelong search for self-knowledge. Can travel be a peripatetic form of health promotion?

AMA - ALBERTA DOCTORS’ DIGEST
24 > Why go anywhere?
“Why go anywhere?” is a question to help clarify our motives for traveling. The pursuit of CME/continuing professional development and the resulting education credits is just one of many good reasons to get out of town.
Then again, you may be looking for something less educational and more exotic: to cruise the fiords of Norway with your new spouse, to take a photo of your daughter shaking the hand of Mickey Mouse in Orlando, or to take a hike with your retired brother on the pilgrimage road to Santiago de Compostela. Sometimes it’s hard to articulate exactly why we want to go somewhere and why now? A generation ago Paul Simon sang, “For reasons I cannot explain, there’s some part of me wants to see Graceland.”
Let’s hear it for vicarious travel
Some years our vacations are few and far between. Eventually, a day will come when we’ll no longer be capable of driving, flying or hiking hither and yon. During these times, we can still avail ourselves of the joy and consolation of vicarious travel. You can visit many places these days by tapping on a screen or turning a page. I enjoy stirring up the travel memories in my morning cup of Costa Rican Tarrazu coffee or a spoonful of lemon gelato. A lot of geography is contained in the aroma of a freshly opened bottle of Malbec.
What kind of journeys appeal to you in your life situation and career stage?
How was your trip?
And how do our travel plans change from early to mid to late career? Does the accumulated experience of 20 or 30 years practicing radiation oncology or sports medicine modify the travel itinerary? How do our reasons for going or not going somewhere evolve over time? Do concerns arise over the size of our ecological travel footprint or perceived threats to personal security? And how about our response to that perennial question from curious or disinterested colleagues when we reappear at work: “How was your trip?” Think of your many replies over the years to that query as rehearsals for your “final answer” before you shuffle off this mortal coil.
As we age, we acquire a few grains of wisdom which help us understand the inevitable diminishment of energy, endurance, resilience, mobility and brain power along the way. The aging process affects our travel plans. The road looks different through progressive bifocals.
Leaf Van Boven and Laurence Ashworth tell us that anticipating a vacation makes you feel better than retrospection about a trip you’ve completed.3 Just thinking about going somewhere can have the effect of raising our spirits.
Most of us, however, return to our emotional baseline pretty quickly after returning home. Jeroen Nawijn, Miquelle A. Marchand, Ruut Veenhoven and Ad J. Vingerhoets, PhD, report that over time, “Generally, there were no differences between vacationers’ and non-vacationers’ post-trip happiness. Only vacationers on a ‘very relaxed’ holiday trip benefit in terms of post-trip happiness.”4 My exhausted surgery colleague could add anecdotal support to this conclusion.
One final question
So is it the destination or the souvenirs, or the journey itself? Good questions, but not the final one. The final question comes from that solicitous friend who asks, “Have you edited your photos?” Better to do it on the go, because you know you won’t have time when you get home and resume the battle.
References
1. https://www.waset.org/conference/2014/09/london/ICPH.
2. http://www.rachelremen.com.
3. Looking forward, looking back: Anticipation is more evocative than retrospection. Van Boven L; Ashworth L. Journal of Experimental Psychology: General, Vol 136(2), May 2007, 289-300. doi: 10.1037/0096-3445.136.2.289.
4. Vacationers Happier, but Most not Happier After a Holiday. Nawijn J, Marchand M A, Veenhoven, R, Vingerhoets, A J. Applied Research Quality Life (2010) 5:35-47. doi: 10.1007/s11482-009-9091-9.
Outside the Roman arena in Nimes, France. ( provided by Dr. Vincent M. Hanlon)
PHYSICIAN AND FAMILY SUPPORT PROGRAM

SEPTEMBER - OCTOBER 2014
albihomes.com astoriahomes.ca calbridgehomes.com
5 MINUTES FROM YOUR FIRST PATIENT, 5 MINUTES FROM THE 1ST TEE BOX. Located just minutes from the South Health Campus, Artesia puts you in the heart of everything that matters to you, including luxurious living. Artesia at Heritage Pointe features vista views, water features, elegant architecture and amenities that make your free time even more fulfi lling. Artesia was just awarded New Community of the Year adding even more great reasons to explore life in Artesia. Choose a high-end Villa from the low $800’s that o� ers a true “lock-and-leave” lifestyle or build your dream home from the mid $900’s on
homesites ranging from 65 to 90 feet wide. Visit our show homes today. For more information visit LIVEATARTESIA.COM
SHOWHOME HOURS: MONDAY TO THURSDAY: 2PM—8PM WEEKENDS & HOLIDAYS: 12PM—5PM FRIDAY: CLOSED
BECAUSE WHEN IT COMES TO GOOD LIVING ARTESIA IS THE PERFECT
PRESCRIPTION
docket 14073 client Heritage Pointe title Good Living publication Doctor’s Digestsize 8.5” x 11” (trim – full page) + .25” bleed colour 4 Colour – CMYK date June 12, 2014 foundrycommunications.ca

AMA - ALBERTA DOCTORS’ DIGEST
2626 FEATURE
AMA Readership Survey 2014 We’re still going strong!
An Alberta Medical Association (AMA) member readership survey earlier this summer revealed that the AMA continues to provide quality, effective
communication to its members, both in the value and relevance of information or topics covered and in the presentation format.
The recent survey let the AMA know that, by and large (with a preference for short and concise!), AMA members are reading AMA publications (President’s Letter, Billing Corner, MD Scope, Alberta Doctors’ Digest, Section News, AMA Membership Guide and Primary Care News) and are generally satisfied with the AMA’s communication channels. This survey provided us with good information regarding our members’ communication preferences, particularly the growing desire for making communications and membership services available online and ensuring that information is timely, relevant and brief, with links providing an option for the reader to delve deeper, if desired. We look forward to rising to these communication challenges as we strive to inform and engage AMA members.
The most recent in a series of readership surveys that the AMA has undertaken (either as a member tracker survey or as a full communication channel survey) over the past 10 years, this summer’s survey was distributed to 11,800 members between May 29 and June 13 and netted 924 responses, for a response rate of 8%. The data is valid 19 times out of 20 within a margin of error of +/- 3.1%.
The last full communication channel survey, similar to this one, was conducted in 2012 and yielded very similar results with the same, overall conclusion: generally, the association is maintaining excellent communication vehicles, with publications that the members find useful and applicable to the conduct of their careers and practices. Membership was well represented in the survey, with the respondent data sporting equal representation between specialists and family physicians.
In general, family physicians find the AMA’s publications somewhat more useful than the specialists do and their topic preferences haven’t changed significantly over the last two years.
>
I am interested in AMA communications about the following topics: (top five)
Questions Mean Category percentages
Benefits (negotiated) e.g., Retention Benefit, Parental Leave, Continuing Medical Education (CME), Medical Liability Reimbursment (MLR)
4.57
Physician fees, fee equity, Physician Compensation Committee 4.52
Alberta Health Services activities that affect physicians 4.43
Alberta Health/government activities that affect physicians 4.39
Billing Tips 4.25
0 20 40 60 80 100
93.0%
0 20 40 60 80 100
91.0%
0 20 40 60 80 100
91.3%
0 20 40 60 80 100
89.8%
0 20 40 60 80 100
81.5%

SEPTEMBER - OCTOBER 2014
27
>
to the President’s Letter and online AMA Membership Guide
The AMA’s internal publication with the highest readership is the President’s Letter, followed by MD Scope, Alberta Doctors’ Digest, Section News and Optimized Prescribing with Seniors. The publication with the lowest readership is the AMA Membership Guide. Thus, there’s no surprise with another readership preference revealed by the survey: 87% of respondents agreed with the AMA moving the @ Your Service Membership Guide to a digital format this year. When asked if the AMA Membership Guide should be sent to members either in its current paper format with the paper membership form or by an email link to the AMA website, 18% said in its current paper format and 42% preferred an email link. The preference for obtaining information online is supported by the fact that when members need information about their AMA benefits and services, 75% of respondents refer to the AMA website.
With respect to other AMA publications, Primary Care News is read by 35% of respondents and Billing Corner is read by 75% of respondents; 77% find it useful ¬ an increase of 7.5% since the 2012 readership survey.
I rely on information, about issues that affect physicians, from the following sources: (select all that apply)
Response Frequency Percent 0 100
AMA 864 95.4%
College of Physicians & Surgeons of Alberta 776 85.7%
Alberta Health 186 20.5%
Alberta Health Services 426 47.0%
Media 525 57.9%
Word-of-mouth 458 50.6%
Vital Signs 133 14.7%
Other 36 4.0%
Readership useful (%)
0 20 40 60 80 100
3
3
4
6
20
32
31
41
77
65
65
53
Billing Corner
AMA Membership Guide
MD Scope
Section News
AMA: The “go-to” for physician information
In a strong show of support for AMA communications, 95% of survey physician respondents rely on the AMA as an information source, with the second highest ranking of preferred information sources going to the College of Physicians & Surgeons of Alberta, at 86%.
20 40 60 80
90% of respondents said the AMA keeps them informed about important issues that affect them in their professional practice and 81% said the AMA keeps them informed about important issues that affect them personally as physicians. Eighty-two to 87% of respondents agreed that AMA communications provides timely information about issues affecting physicians; they use clear language to explain complex issues; and they help physicians feel connected to the association. The fact that the 2014 survey results regarding AMA communications were all within 1-2% of the 2012 survey results for the same subject area demonstrates a high level of consistency in communications service delivery.
Areas for improvement … you said …
AMA written communications could be improved by being:
• Summaries with links, key points, headlines
• Shorter, more concise; more interesting, relevant, timely content; issues-specific
• Email, not in paper form
• Brief, provide links
• Precise and shorter, bullet points
• Response/feedback options, links; discussion forums
• Videos, blogs? Drowning in electronic print news
>

AMA - ALBERTA DOCTORS’ DIGEST
28
LOOK MA, NO LOGIN! Want to comment on the President’s Letter or other pages on our website, but don’t want to log into the site? You can!
We’ve produced a new way for you to tell us what you think or to participate in group discussions. We’ll be including this feature with President’s Letters and on other web pages in the coming months.
Give it a try! For example, next time we send you a President’s Letter, click on the link at the top of the email. Scroll down to the bottom of the web page and post your comment. It’s just that easy.
Take a look at our commenting policy for some common-sense advice on keeping the conversation productive. And, of course, you’ll still be able to contact the president directly by email.
> Topics of interest to survey respondents:
• Student opportunities and information
• Billing information/tips
• Political climate
• Social issues (e.g., end of life)
• Compensation/pension/benefits
• Alternative Relationship Plan ¬ issues
• Information related to retired physicians
• Electronic medical records
• Inter-provincial news/collaboration
• Foreign workers
• Wellness programs
PHYSICIAN(S) REQUIRED FT/PT
MILLWOODS EDMONTON
Also locums required
Phone: Clinic Manager (780) 953-6733 Dr. Paul Arnold (780) 970-2070
ALL-WELLPRIMARY CARE CENTRES

SEPTEMBER - OCTOBER 2014
A speaker at a recent conference I attended, brought
to light a question that, up until that point I had contemplated periodically, but never explored in detail: do our clinical skills decrease the further we get from the rigors of residency training and medical school?
As a family physician in training, I’m often burdened by the notion that my breadth of knowledge will either decrease or become obsolete in certain areas of medicine the longer I practice medicine. This feeling of uncertainty comes from acknowledging that once I’ve completed residency I will no longer be routinely exposed to the variety of patient panels from numerous specialties and centers that occurs during training.
So, without possessing the mythical photographic memory, I wonder: What hope do I have of retaining all of that knowledge? What is the risk of what I colloquially phrase “brain leak,” and more importantly, what might be done to stop it?
for the best patient care.1 This is a significant concern, and as noted in the article, is paradoxical to what we as trainees believe when we contemplate challenging our preceptor’s differential diagnoses or case management plans. A related editorial by Dr. Steven Weinberger identified this as a “wake up call” to the profession.2 But, almost 10 years later, is the profession hitting the snooze button?
Rightfully so, this research brought with it a level of concern from patients, the general public and politicians. It has led physicians, in conjunction with the national licensing and accreditations boards, professional associations and colleges to seek a means of maintaining their autonomy. Thus, the duality between recertification and Maintenance of Certification (MOC) occurred ¬ and for now, MOC is the victor.
Help, help! My brain is leaking
RESIDENTS' PAGE
Dr. Rithesh Ram | FAMILY MEDICINE RESIDENT PHYSICIAN
29
The longer a physician is in practice, the harder it is to remain current in terms of the latest research and treatment plans available for the best patient care.
Choudry et al provided the most methodologically rigorous (albeit, highly criticized) evidence of this phenomenon. The conclusion of their study suggests that the longer a physician is in practice, the harder it is to remain current in terms of the latest research and treatment plans available
Is the profession hitting the snooze button?
MOC, the champion of continuous professional development, is facilitated through MAINPORT or MAINPRO here in Canada. As stated on its website: “the MOC framework is intending to promote a competency-based approach to lifelong learning that is not just focused on knowledge (the traditional domain of the medical expert) but on multiple skills, competencies and abilities.”
Excellent! One would imagine that with this program in place, all of my concerns would be alleviated. At the very least, this tool provides ongoing stability around a structured learning environment that I have come to depend on during many years of medical training.
Perfect.
Yet, even with this learning mechanism in place, I am left wondering why I still have that uneasy feeling that >
Dr. Rithesh Ram (left) with family and friend

AMA - ALBERTA DOCTORS’ DIGEST
30 10 years from now I won’t be able to spot diagnose Blau Syndrome or remember that plica syndrome should be in my differential for knee pain.
As a professional student ¬ after all I’ve spent more than half my life as a student already ¬ I’m not sure I want to continue with the formal forms of education I’ve experienced. My desire is to have access to professional development tools through various mediums, in varying presentation formats, with multiple points of view.
I am becoming convinced that my brain won’t be too leaky, that as I continue in the practice of medicine I will provide quality care to my patients.
Not to worry. MAINPORT and MAINPRO both have different sections or categories to account for my inclination to have access to multimedia, thereby allowing me to take charge of my continuing development through personal selection of what conferences, meetings, workshops, etc. I would like to attend to supplement my day-to-day life as a physician (assuming all are accredited, of course).
Ok. I’m starting to relax.
But if this kind of program, or an iteration thereof, has been around for a number of years, then what was all the fuss about length of time in practice leading to less capable physicians? Although Choudry et al acknowledged a number of different limitations to their study, it remains the only systematic review on this topic and the upper level of the evidence-based medicine pyramid. Is there any other research out there?
I believe a qualitative study by Elstad et al alleviates some of my concerns.3 They found that over time physicians gain complex social, behavioral and intuitive wisdom leading to increased patient adherence and satisfaction in comparison to their less experienced or freshly graduated colleagues. They believe that the guideline-based process and outcome measure analysis usually done to assess care biases the results towards inflating the more favorable outcomes of a less experienced physician to that of someone who has been in practice for many years. Generally speaking, the less experienced physician is characterized as someone who is less likely to “make a connection” with problem patients in comparison to the more experienced physician.
Between the MOC and my eventual growth of social, behavioral and intuitive wisdom, I am becoming convinced
that my brain won’t be too leaky and that as I continue in the practice of medicine I will provide quality care to my patients. This thought process was my convoluted way of realizing that as a physician I am an adult learner, always seeking out knowledge that will allow me to provide optimal care to my patients regardless of how far along I am in my practice. Recognizing that learning styles are as diverse as practicing physicians, I am relieved that tools available for continued learning are accessible in a wide range of formats. Thankfully, there are ways to stop the leak!
Now if only getting my kids to sleep early on a school night was that easy.
References
1. Choudhry NK, Fletcher RH, Soumerai SB. Systematic review: the relationship between clinical experience and quality of health care. Ann Intern Med. 2005;142(4):260-73.
2. Weinberger SE, Duffy FD, Cassel CK. Practice makes perfect … or does it? Ann Intern Med. 2005;142(4):302-3.
3. Elstad EA, Lutfey KE, Marceau LD, Campbell SM, von dem Knesebeck O, McKinlay JB. What do physicians gain (and lose) with experience? Qualitative results from a cross-national study of diabetes. Soc Sci Med. 2010;70(11):1728-36.
calgarycoop.com/pharmacy
By appointment only. Patients should sign up in advance as space is limited. All individuals must live, work or go to school in Alberta, must be nine years of age or older and must show
Alberta Health Care card to be eligible for flu shots.
All Co-op pharmacies are hosting in-store complimentary
flu shot immunizations.
For clinic dates and to book appointments, patients
can call or visit any Co-op Pharmacy.
Flu Shot Clinics
Your patients can avoid the seasonal flu and the seasonal line-up!
>

SEPTEMBER - OCTOBER 2014
>
The art of “evergreening” is something we all
practice at times ¬ you know, the game of keeping a good thing going as long as you can: keeping the free muffins at rounds,
using government aircraft when commercial flights are available, keeping the disability payments going when you should be back at work, routinely taking the monthly “sickness day.”
Sometimes too much of a good thing brings on infantile feelings of entitlement. That good deal is ours and we want to keep it going ¬ to evergreen it.
Alexander H.G. Paterson, MB ChB, MD, FRCP, FACP | CO-EDITOR
although (for the record) I saw Justin Trudeau on a recent flight from Ottawa to Toronto sitting right at the back of economy with the advantage that he glad-handed his way right to the back of the aircraft. But what I’m really saying here is that to rouse an apathetic public, it seems that “monstering” is part of the process.
This summer the most outrageous ¬ and seemingly far less interesting as a news item to people, than the Sky Palace and private government jets ¬ was the release of the Fraser Institute’s report1 showing that in 2013 the average Canadian family earned $77,381 while paying $32,369 in taxes (41.8% of income) compared to 36.1% for food, shelter and clothing. By comparison, in 1961 ¬ a time of big pay-out for war costs ¬ the average family earned $5,000 and spent much more of its income on food, shelter and clothing (56.5%) while $1,675 went to taxes (33.5%).
Where is all this new tax money going? Well, with the last six months of Not Your Grandfather’s Party (NYGFP) revelations, you know one little sink hole. But there are much bigger ones that rarely make it to Twitter.
One huge tax-draining wheeze flourishes in the world of pharmaceuticals: the lark of evergreening. These drug costs are covered by provincial governments so there are no faces attached, no one person to scapegoat. This drain does not back-up in flood season. It’s gigantic with a great gurgle of sodden cash sliding into the pockets of Zurich, Basel and New Jersey Big Pharma Gnomes and their legal, financial and miscellaneous free-loading buddies ¬ not the inventors.
I glow with pleasure when a researcher pockets a couple of hundred million for an innovative discovery, but that’s not where the moola is going. United States of America (USA) patents are meant to run for 20 years. But it’s the art of evergreening that feeds higher prices for longer than the already generous patent laws intended ¬ and most of this extra cash goes to blokes whose only job is to think up new ways to keep the cash flowing. This will not be easily changed since well-paid lawyers and big companies have a money hose that keeps on hosing. Throw in a few lawmakers who are in the pockets of Big Pharma and you have a revenue river that leaves cash
The art of evergreening is costing taxpayers big moolah
IN A DIFFERENT VEIN
Ask anyone about drug patent evergreening and their eyes glaze over. Ask them about the Red Queen’s Sky Palace and eyes bulge with resentment. But, which loses you more money?
We direct anger at the politicians while the pickpockets sneak off with our wallet. Ask anyone about drug patent evergreening and their eyes glaze over. Ask them about the Red Queen’s Sky Palace and eyes bulge with resentment. But, which loses you more money? Progressive Conservative government perks? Or drug patent evergreening? Hello! It’s the latter by a big chunk of dough. In the last few years I’ve been consulted by generic companies trying to challenge the evergreening of drug patents. There’s been too much of a good thing there, and worse, the big money’s going to the wrong people.
Poking fun at politicians is one thing but “monstering” a la Murdoch News Corporation is quite another. Why shouldn’t the premier of Alberta fly business class ¬
31

AMA - ALBERTA DOCTORS’ DIGEST
32 cows in the ditch. And the lobbying power of small, incentivized groups outweighs that of a larger, poorly organized majority.
Let me expand.
Five years ago in New York, I consulted for a generic company who were challenging (along the muddy legal lines of “anticipated inherency”) a patent extension after 20 years of a commonly used bisphosphonate in patients with bone metastases and/or osteoporosis. Its marketing had been clever ¬ the Big Pharma company not only differentiating it from other similar drugs by a different chemical name but by using the word “potent” in all its literature. Now “potent” (as all should know) does not mean “clinically more effective,” it means a smaller amount of stuff required to achieve a similar effect. But American oncologists love IV infusions that can be given over a short time and have a financial incentive to use them and so it sold like Tim Hortons Double-Doubles.
gracious, she was. And the questioning started. I got on well with Marcia. We rapped about the history of bisphosphonates from Herbie Fleisch, grandfather of these agents, through their clinical development and their individual characteristics. We broke for coffee, then lunch, everything being recorded. It was a nice lunch ¬ tasty quiches, fresh vegetable salads and cold cuts. I had two helpings of ice cream and fruit salad and a couple of chocolate chip cookies and we returned to the interrogation room. We commenced the afternoon session going over dosages and infusion times. Marcia was friendly, even chatty. Three o’clock came around and I mulled over tickets to a Broadway show that evening, perhaps after a dinner at the Trump Tower. I was relaxed in the spotlight and stifled a yawn.
It was then she passed over the table a glossy pamphlet ¬ it looked like a newsletter and was a report of some medical meeting in the south of France from about seven years before ¬ the kind of rag no one in their right senses reads.
“Would you look at the second page, dah-cter? Is that your name as second author in an interview titled New Bisphosphonates ¬ the Future. Would you please read the third paragraph from the end, dah-cter?”
It was one of those “And what do you think professor?” interviews gussied up to look like an article, featuring an interview with me and an old friend from London (no doubt after we’d had a few cocktails). He was blathering (with no follow-up objection from me) that the drug we were here discussing might be a unique agent, convenient to use and might inhibit bone metastases better than other earlier agents.
I’d never seen the article and my old friend must have assumed it was so minor a publication that he wouldn’t bother me with it. He swears he can’t remember it either.
Drug costs are covered by provincial governments so there are no faces attached, no one person to scapegoat.
The generic company’s argument was that the drug was hardly a new discovery with a unique mode of action and would have been “anticipated inherently” as the lawyers term it. It was just another amino-bisphosphonate with a CH2-imidazole ring tagged on and had similar efficacy as any other bisphosphonate. The differences between the claimed “invention” and the “prior art” were such that the claimed invention would have been obvious to a person having ordinary skill in the art. Everything revolved around the vague concept of “obviousness.”
Now I was a devotee of the television show The Sopranos (about the New York Italian mob) and there were big bucks at stake here, so I first checked whether an innocent from the boonies of Canada would end with his feet in concrete at the bottom of the Hudson River. The attorney assured me this was unlikely, but it would depend on how things went by late afternoon on the day of the “examination for discovery.”
We met at 9 a.m. in a law office off Times Square. I felt good. At 9:15 a.m. my attorney and I were invited into a large flood-lit room ¬ video cameras and sound equipment strewn around ¬ and around the table were eight Big Pharma attorneys and their assistants with their expert witness, whom I recognized as a University of Columbia oncologist.
An attractive, efficient female attorney, black hair (like Marcia Clark, the O.J. Simpson prosecutor) ran through my qualifications and experience. Polite, friendly and
Big Pharma no longer innovates; it’s now more lucrative to market and litigate than to innovate. And the taxpayer is the rube forking out.
“I’ve never seen this before,” I said.
“But your name is on it, dah-cter.”
“I don’t recall this. Anyway, nobody reads these things.”
“But that is your name on it isn’t it, sir?”
The flood-lit room seemed to warm up. Tiny beads of sweat oozed from the face and armpits. The credibility of this expert witness began to circle the toilet bowl
>
>

SEPTEMBER - OCTOBER 2014
33> like support for the NYGFP. The patent challenge was unsuccessful. I still can’t find that glossy pamphlet.
The French have a neat phrase ¬ “l’esprit d’escalier” ¬ the apt witticism coming too late, the perfect retort that’s too late because you’re at the stairwell bottom on the way out. Dammit. I should have said:
“That was years ago, madam. I don’t think that at all now. Next question.”
Evergreening games in Canada come under the Patented Medicines (Notice of Compliance) Regulations of the Patent Act. Patents run for 20 years but the length of market exclusivity here is shorter because of legal challenges, research needs and regulatory hurdles (and are often less than 10 years) though tasty profits are made. Patents in the USA run for 20 years from the earliest claimed patent date ¬ but that’s just the beginning. Evergreening allows patents to be extended by concocting an infringement challenge and/or by bringing in some minor development: a new delivery system; a minor change of formulation for a new composition patent; a different software programme; even a trade name change or manufacturer name change or a change in packaging. The complexities of patent rights are meat and drink for the lawyers.
Generic companies are no Robin Hoods but the price to taxpayers does come down.
As Marcia Angell, former editor-in-chief of the New England Journal of Medicine wrote:
“Nothing drug companies do is as profitable as stretching out monopoly rights on their blockbusters. Extending that privileged time by a variety of stratagems is the most innovative activity of Big Pharma. For blockbuster drugs, it is certainly the most lucrative.”2
Tying a case up in the courts allows for patent extensions of one to two years. Even an extra six months of a blockbuster drug has a huge effect on the bottom line. It might be better if companies were rewarded an exclusive patent and license for exploring older drugs for new indications as suggested by this recent letter to The Times of London:
“Sir, There is a real barrier to licensing old drugs for new purposes, even when they are effective, so some beneficial, even life-saving, treatments with minimal costs are not available.
“A private member’s bill introduced by Jonathan Evans, MP, today is an opportunity to address this anomaly. We fully support the bill and hope it will lead to a change in access to treatments. These include breast cancer treatments that could prevent some people at high risk of the condition from developing it and prevent some people with primary breast cancer from developing secondary breast cancer and ultimately dying from the disease.”3
Twenty-year patents should be awarded for discovery of a new agent with a unique mode of action improving efficacy or decreasing toxicity and perhaps shorter patents for accumulating the evidence for a completely new indication for an off-patent drug and not for some legal wheeze or change in packaging.
References
1. Lammam C and Palacios M: The Fraser Institute: Taxes Versus the Necessities of Life: The Canadian Consumer Tax Index, 2014, published August 12 2014.
2. The Truth about Drug Companies pp 173-74.
3. Coleman, Copson, Cuzick et al: Letter to The Times of London, July 2 2014.
Generic companies are no Robin Hoods but the price to taxpayers does come down.
The idea of patents was to encourage innovation, but the idea of evergreening is to provide a nice source of income for companies and a livelihood for their lawyers. Big Pharma no longer innovates; it’s now more lucrative to market and litigate than to innovate. And the taxpayer is the rube forking out. There have been many calls to curtail these practices in Canada and the USA, all of which have for some reason come to nothing. No one has been monstered. There’s no monster to point your finger at.
Fun and games have been seen with paroxetine, omeprazole, citalopram, norfloxin and the multitude of cholesterol inhibitors and many others, with litigation lasting three to four years or more allowing continued exclusivity.
AMA - ALBERTA DOCTORS’ DIGEST
can offer you flexibility with regard to hours and location. We provide nursing support and electronic medical records. We’ll move your practice or help you build a practice. Walk-in shifts are also an option. All inquiries will be kept strictly confidential.
Contact: Margaret Gillies TF 1.866.624.8222, ext. 133 [email protected]
CALGARY AB
Braeside on 24th Medical Clinic is recruiting three full-time family physicians and must be eligible to be
imaging. This would be primarily at an established outpatient clinic in Calgary with an excellent reputation for subspecialty level breast work. Fellowship training preferred.
Contact: Dr. Robert Davies Medical Director T 403.828.3849 [email protected]
CALGARY AB
MCI The Doctor’s Office™ has family practice options available in Calgary. With more than 27 years of experience managing primary care clinics and eight locations, we
PHYSICIAN WANTED
CALGARY AB
Dr. Neville Reddy is recruiting family physicians and specialists for his two medical clinics, Innovations Health Clinic SE and Innovations Health Clinic SW. Competitive expenses offered.
Contact: [email protected]
CALGARY AB
Canada Diagnostic Centres is seeking a consulting radiologist for a rewarding career focused on women’s
CLASSIFIED ADVERTISEMENTS
34
>
CMPA clarifies
I would like to clarify some information that can be found in an article written by Dr. Alexander Paterson in the July-August issue of Alberta Doctors’ Digest. The article, “Going to pot in the clinic” mentions that if a physician is worried about drug interactions, they can ask the patient to sign a waiver on a Canadian Medical Protective Association (CMPA) release form.
Under the federal government’s new rules for medical marijuana, patients seeking medical marijuana must now consult with a prescribed health care practitioner (i.e., a physician or a qualified nurse practitioner) and obtain a signed “medical document.” Patients can then obtain marijuana from a licensed commercial producer.
Well done
I just had the pleasure of reading Dr. Alexander Paterson’s article “Going to pot in the clinic” in the July-August issue of Alberta Doctors’ Digest.
Fabulous! How refreshing to read (from an authentic medical perspective) an overview of many people’s “bud.” This article is edgy, funny and factual and avoids all the sanitized and politically neutered dialogue that I am so tired of hearing.
Notwithstanding the opinion disclaimer, I think the Alberta Medical Association is being progressive weighing in on this important conversation and brings some clarity (clearing the smoke if you will) for the uninformed and undecided.
Thank you.
Henri Ferguson Canmore AB
The CMPA no longer suggests physicians ask patients to sign a waiver and this document has been removed from our website.
Here is the link to the CMPA’s current article on medical marijuana on our website. It overviews the regulations and college policies.
https://oplfrpd5.cmpa-acpm.ca/en/legal-and-regulatory-proceedings/-/asset_publisher/a9unChEc2NP9/content/medical-marijuana-new-regulations-new-college-guidance-for-canadian-doctors
Many thanks.
Tracy Murphy Senior Policy Analyst Canadian Medical Protective Association
LETTERS

SEPTEMBER - OCTOBER 2014
35
As a part of our expanding services, IHC is looking for an obstetrician/gynecologist specialist to manage patients referred within our large family physician network for women’s health concerns. In addition, the successful candidate will have opportunities to help develop leading programs for health promotion and preventative strategies for IHC’s women’s health division.
An attractive compensation package is available and includes extended health/dental benefits plus even more compelling rewards.
All candidates must be immediately eligible for licensure or already licensed with the CPSA and provide proof of malpractice insurance from the Canadian Medical Protective Association. Compensation is fee-for-service and/or salary.
All inquiries will be kept strictly confidential and only qualified candidates will be contacted.
Contact: Submit your CV to: Joanne Oliver [email protected]
EDMONTON AB
Calwood Medical Clinic centrally located in Edmonton, Alberta is looking for part- and full-time general practitioners and family physicians. Must be licensed with the College of Physicians & Surgeons of Alberta or eligible for licensing. Our clinic has private furnished offices and examination rooms with great medical staff ready to support your practice. We offer flexible hours. Overhead is negotiable. The clinic is associated with Edmonton North Primary Care Network.
Contact: Dr. S. Mausolf T 780.452.4590 C 587.920.2774
EDMONTON AB
Urban Medical Clinic in vibrant southeast Edmonton is a new state of-the-art medical clinic that is rapidly expanding. The clinic uses TELUS PS Suite electronic medical records. Our team currently includes two family physicians and we are part of Edmonton Southside Primary Care Network with full-time nurse and dietician. We have 8,000 patients registered. The clinic is growing and we are recruiting part- and full-time physicians. Competitive overhead for long term commitments. We have eight examination rooms, one procedure room and one specially designed wheelchair room.
Contact: Dr. Oshean Naidoo [email protected] or Dr. Dhanakodi Rengan [email protected] T 780.757.9545
EDMONTON AB
Imagine Health Centres (IHC) in Edmonton has an immediate opening for an obstetrician/gynecologist licensed or eligible to be licensed with the College of Physicians & Surgeons of Alberta (CPSA).
Imagine Health Centres are dynamic multidisciplinary clinics with a large array of services including family physicians, specialists and many other allied health professionals. Imagine Health Centres is dedicated to promoting the health of patients utilizing the most up-to-date preventative and screening strategies.
licensed by the College of Physicians & Surgeons of Alberta.
Fee-for-service billing, attractive overhead split and Accuro electronic medical records. Office hours are Monday to Friday, 9 a.m. to 5 p.m.
Contact: 11466 Braeside Dr SW T 587.296.3363 [email protected]
CALGARY AND EDMONTON AB
Imagine Health Centres in Calgary and Edmonton have an immediate opening for a psychiatrist certified or eligible for certification with the College of Physicians & Surgeons of Alberta (CPSA).
Imagine Health Centres are dynamic multidisciplinary clinics with a large array of services including family physicians, specialists and many other allied health professionals such as pharmacists, physiotherapists, psychologists and more. Imagine Health Centres is dedicated to promoting the health of patients utilizing the most up to date preventative and screening strategies.
The successful candidate will work closely with our multidisciplinary team to optimize management of our patients with mental health issues. Collaborate with our large network of family physicians and their referrals to maximize outcomes for your patients. Opportunities for group therapy and corporate health are available. There are also opportunities to help develop leading programs for mental health at all levels of primary care within our multiple sites located throughout Calgary and Edmonton.
An attractive compensation package will be offered to the successful candidate.
All candidates must be immediately eligible for licensure or already licensed with the CPSA and provide proof of malpractice insurance from the Canadian Medical Protective Association. Compensation is fee-for-service.
All inquiries will be kept strictly confidential and only qualified candidates will be contacted.
Contact: Submit your CV to: Joanne Oliver [email protected] >
>

AMA - ALBERTA DOCTORS’ DIGEST
36 EDMONTON AB
North Town Medical Centre is looking for part- and full-time family physicians and specialists to join our team. North Town Medical Centre is a multidisciplinary clinic with three family physicians, two specialists and two chiropractors. The clinic is in a strip mall with plenty of free parking, close to medical imaging, pharmacy and laboratory. Modern well-equipped facility with highly trained staff allow for no administrative burdens, electronic medical records, no hospital on-call, plenty of examination rooms, offices for physicians and competitive fee split. Flexible schedule can accommodate physicians who are looking to pick up extra shifts or a new physician wanting to open their practice to new patients.
If interested in knowing more regarding this great opportunity, please contact us.
Contact: Dr. Hassen Taha T 780.905.0027 or Dr. Ataher Mohamed T 780.298.2986 [email protected]
EDMONTON AB
Beverly Medical Clinic is a new state-of-the-art medical clinic that is rapidly expanding. Our team currently includes three family physicians, two internists and a pediatrician.
The clinic is growing and needs more dedicated family physicians as one of the physicians is planning on slowing down. Competitive overhead for long term commitments; 75/25% split.
We have 10 examination rooms, one treatment room and one specially designed pediatric room.
Contact: Dr. A. Elfourtia or Dr. Z. Ramadan Beverly Medical Clinic 4243 118 Ave Edmonton AB T5W 1A5 T 780.756.7700 C 780.224.7972
EDMONTON AB
Ellerslie Medical Centre in southwest Edmonton is seeking part- and full-time physicians. The busy clinic is in a prestigious and fast-growing community which has a high public demand for family physicians. The
physician income will be based on fee-for-service with an average annual income of over $300,000. The physician must be licensed or eligible to apply for licensure by the College of Physicians & Surgeons of Alberta (CPSA). For the eligible physicians, their qualifications and experience must comply with the CPSA licensure requirements and guideline.
Contact: Walid 11140 Ellerslie Rd SW Edmonton AB T6W 1A2 T 780.884.4124 [email protected]
EDMONTON AB
Evansdale Medical Clinic, 8214 144 Avenue in Edmonton is looking for a part- and full-time family physician to be part of our community to support and help with patients continuing health care needs. We are looking for a doctor on a permanent basis. We are a growing busy clinic in north Edmonton with friendly, supportive and outgoing staff. Income per year depending on fee per service would be approximately $300,000. Our clinics offer pleasing working conditions with well-equipped modern facility and electronic medical records in each room.
Contact: Dr. A. Aradi T 780.478.0975 F 780.478.0976 Evansdale Medical Clinic 8214 144 Ave Edmonton AB T5E 2H4 Send résumé to: [email protected]
EDMONTON AB
Two positions are immediately available at the West End Medical Clinic, unit M7, 9509 156 Street. Full-time family physician/general practitioner positions are available. The physician who will join us at this busy clinic will provide family practice care to a large population of patients in west Edmonton.
The physician income will be based on fee-for-service with an average annual income of over $300,000 and overhead fees are negotiable.
The physician must be licensed or eligible to apply for licensure by the College of Physicians & Surgeons of Alberta (CPSA). For the eligible physicians, their qualifications and
experience must comply with CPSA licensure requirements and guidelines.
Contact: Dr. Gaas T 780.756.3300 C 780.893.5181 [email protected]
EDMONTON AB
True Balance Medical Spa is seeking a motivated physician to serve as a location medical director as we grow our business. As a leader in the industry, we are a well-established, premier medical spa with three locations in the Edmonton area. True Balance combines the beauty you love and the health you feel.
The medical director position will be a part- to full-time, permanent position that will require some travel between three locations in the Edmonton area. The capital region of Alberta has so much to offer with close proximity to year-round outdoor recreational opportunities. We offer top notch training and support in facial injectables and a variety of the latest laser treatments including laser hair removal, spider vein removal and sun damage correction. We feature state-of-the-art equipment in a modern, upscale facility and have a significant marketing budget. Overseeing staff is required and we pride ourself on our positive work environment and commitment to team work.
Generous salary and benefit package based on experience.
Contact: Submit a detailed résumé to: [email protected]
EDMONTON AB
Imagine Health Centres in Edmonton has an opening for a medical director and is building a new kind of health care, one that is ready to help create a healthier future for women.
Our ability to excel depends on the integrity, knowledge, imagination, skill, diversity and teamwork of people like you. To this end, we strive to create an environment of mutual respect, encouragement and teamwork. As part of our team, you’ll have the opportunity to collaborate with talented and dedicated colleagues while developing and expanding your career.
>
>

SEPTEMBER - OCTOBER 2014
37The medical director develops and fosters on-going professional relationships with health care practitioners to help achieve positive health outcomes for our patients.
The medical director is responsible for the clinical elements of the entire system including professional duties as well as supervising physicians, and provide general supervision and guidance to practitioners in clinical disciplines.
Essential functions include working closely with the clinic management team; assist in the development of the clinical and managerial skills of the site medical staff; assume responsibility for clinical program operations in accordance with facility policy; impact directly on patient care through the development of appropriate clinical guidelines, polices, and procedures as well as discussion of individual case management and as needed individual patient evaluation through physical assessment and chart reviews; supervise the quality improvement coordinator in the development, implementation, training and monitoring of the continuous quality improvement (CQI) program; maintain ultimate responsibility for the CQI program; must be able to apply principles of critical thinking to a variety of practical and emergent situations and accurately follow standardized procedures that may call for deviations; knowledge of medical esthetics an asset; evaluate the medical potential of inline and pipeline products in the Canadian market; advance patient interests while demonstrating an understanding of key business drivers; generate innovative ideas for clinical programs and support for new product approvals; develop and implement an advisory board and medical educational plan; provide medical input into commercial activities, including strategic business plans; monitoring product safety; maintain subject matter expertise through medical and scientific literature and conferences; provide leadership and oversight for professional medical education, communications, and product safety related activities; collaborate with internal and external colleagues to develop and conduct clinical trial
and other scientific strategies to the highest ethical principles and in compliance with applicable legal and regulatory standards; review medical and clinical information provided to health care professionals by marketing, and provide support for internal and external scientific and medical training; and share departmental management functions including budget, forecasting and management, meetings and training.
Position requirements are licensed practitioner with a special interest in women’s health, proven successful leadership in medical affairs, including development of medical strategic plans, business acumen, pharmacovigilance, and medical education. FRCP or CCT in Obstetrics/gynecology or CCFP or MRCGP; minimum of five years’ experience; knowledge and understanding of health care needs, attitudes and experience in advocacy development; excellent analytical, verbal and presentation skills are essential; ability to work effectively with others in a matrix environment and ability to manage multiple projects and product responsibilities.
Our employees are the key to our company’s success. We demonstrate our commitment to our employees by offering a competitive and valuable rewards program. Our benefits are designed to support the wide range of goals, needs and lifestyles of our employees, and many of the people that matter the most in their lives.
We offer a very attractive base salary plus incentive bonuses as well as the opportunity to practice and bill fee-for-service. Qualified applicants are encouraged to apply.
Contact: Joanne Oliver Physician Recruitment [email protected]
EDMONTON AB
The College of Physicians & Surgeons of Alberta is looking for experienced physicians in good standing to serve on complaints review committees or hearing tribunals. Deadline to apply is October 31.
Contact: [email protected]
EDMONTON AND FORT MCMURRAY AB
MD Group, Lessard Medical Clinic, West Oliver Medical Centre and Manning Clinic each have 10 examination rooms and Alafia Clinic with four examination rooms are looking for six full-time family physicians. A neurologist, psychiatrist, internist and pediatrician are required at all four clinics.
Two positions are available at the West Oliver Medical Centre in a great downtown area, 101-10538 124 Street and one position at the Lessard Medical Clinic in the west end, 6633 177 Street, Edmonton. Two positions at Manning Clinic in northwest Edmonton, 220 Manning Crossing and one position at Alafia Clinic, 613-8600 Franklin Avenue in Fort McMurray.
The physician must be licensed or eligible to apply for licensure by the College of Physicians & Surgeons of Alberta (CPSA). For the eligible physicians, their qualifications and experience must comply with the CPSA licensure requirements and guidelines.
The physician income will be based on fee-for-service with an average annual income of $300,000 to $450,000 with competitive overhead for long term commitments; 70/30% split. Essential medical support and specialists are employed within the company and are managed by an excellent team of professional physicians and supportive staff. We use Healthquest electronic medical records (paper free) and member of a primary care network.
Full-time chronic disease management nurse to care for chronic disease patients at Lessard, billing support and attached pharmacy are available at the Lessard and West Oliver locations.
Work with a nice and dedicated staff, nurse available for doctor’s assistance and referrals. Also provide on-site dietician and mental health/psychology services. Clinic hours are Monday to Friday 8:30 a.m. to 8:30 p.m., Saturday and Sunday 10:30 a.m. to 5 p.m.
Contact: Management Office T 780.757.7999 or T 780.756.3090 F 780.757.7991 [email protected] >
>

AMA - ALBERTA DOCTORS’ DIGEST
38 SHERWOOD PARK AB
Well-established clinic with five family physicians recently expanded and has opportunities for one to two part- or full-time physicians. Flexible hours and competitive fee split. We are in a professional building with laboratory and X-ray on site. We have current electronic medical records, primary care network nurse support and excellent support staff.
Contact: Dr. Lorraine Hosford T 780.464.9661 [email protected]
PHYSICIAN AND/OR LOCUM WANTED
CALGARY AND EDMONTON AB
You require balance … you demand the best. Join the fastest growing medical group in Alberta to practice medicine the way it was meant to be.
Imagine Health Centres (IHC) is currently looking for family physicians and specialists to come and join our dynamic team in part-time, full-time and locum positions available in Calgary or Edmonton. Physicians will enjoy extremely efficient workflows allowing for very attractive remuneration, no hospital on-call, paperless electronic medical records, friendly staff and industry-leading fee splits.
Imagine Health Centres are multidisciplinary family medicine clinics with a focus on health prevention and wellness. Come and be a part of our team which includes physicians, physiotherapists, massage therapists, psychologists, nutritionists and pharmacists.
Imagine Health Centres prides itself in providing the very best support for family physicians and their families in and out of the clinic. Health benefit plans and full financial/tax/accounting advisory services are available to all IHC physicians. There is also an optional and limited time opportunity to participate in ownership of our innovative clinics.
We currently have three Edmonton clinics with a fourth coming to Windermere (southwest Edmonton) in early 2015. The current clinics are near South Edmonton Common, Old Strathcona and West Edmonton.
We currently have one clinic in southeast Calgary with a second clinic opening downtown in September.
If you are interested in learning more about our exceptional clinics, please contact us. All inquiries will be kept strictly confidential.
Contact: Joanne Oliver T 780.907.3777 [email protected]
EDMONTON AB
Summerside Medical Clinic and Edge Centre Walk-in Clinic require part-time and full-time physicians. Locums are welcome. The clinics are in the vibrant, rapidly growing communities of Summerside and Mill Woods. Examination rooms are fully equipped with electronic medical records, printers in all examination rooms and separate procedure room.
Contact: Dr. Nirmala Brar T 780.249.2727 [email protected]
RED DEER AB
Associate Medical Group was established in 1946 and is one the largest full-spectrum family medicine clinics in Red Deer. Associate Medical Group offers a diverse practice and is currently seeking part- and full-time physicians, as well as locums, interested in seeing patients in a busy walk-in environment and/or an office practice. Hospital in-patient care and an obstetrical practice are also available. The walk-in clinic and downtown office are in high-traffic retail locations which generate large income potential with generous financial splits. A pharmacy is located at both locations and the laboratory and hospital are located within minutes.
We have an excellent and knowledgeable support team, supportive colleague base, competitive 70/30 split and fully integrated electronic medical records. All staffing and administration support is provided. The clinic is connected to the Red Deer Primary Care Network and has several health care professionals collaboratively working with family physicians.
Contact Dr. Hopfner [email protected]
PRACTICE WANTED
CALGARY AB
I am a family doctor looking to take over any medical clinic from which the owner is relocating or retiring. I would also consider buying a medical building.
If you are a family physician or specialist looking for part- or full-time work please contact me.
Contact: Dr. D. Das T 403.585.6840 [email protected]
PRACTICE FOR SALE
CALGARY AB
Well-established group family medicine practice for sale in northwest Calgary. Part of the Calgary Foothills Primary Care Network co-located with physiotherapy, rehabilitation, dentist, optometrist and pharmacies. Turn-key solution, furnished, all equipment and new computer hardware included. Large patient base and sufficient Physician Office Support Program funding remaining to assume. Ten examination rooms, five physician practice, leased premises, clinic manager with experienced staff including registered nurse and licensed practical nurse.
Contact: Dr. Virani [email protected]
COURSES
CME CRUISES WITH SEA COURSES CRUISES • Accredited for family physicians
and specialists • Unbiased and pharma-free • Canada’s first choice in CMEatSEA®
since 1995• Companion cruises FREE
CARIBBEAN NEW YEAR’S December 28-January 4, 2015 Focus: Endocrinology, psychology and dermatology Ship: Allure of the Seas
AUSTRALIA AND SOUTH PACIFIC January 16-30, 2015 Focus: Rheumatology, gastroenterology and infectious diseases Ship: Oosterdam
>
>

SEPTEMBER - OCTOBER 2014
39
TO PLACE OR RENEW, CONTACT:
Daphne C. Andrychuk
Communications Assistant, Public Affairs
Alberta Medical Association
T 780.482.2626, ext. 275 TF 1.800.272.9680, ext. 275
F 780.482.5445
daphne.andrychuk@ albertadoctors.org
DISPLAY OR CLASSIFIED ADS
ANTARCTIC AND SOUTH AMERICA February 3-24, 2015 Focus: Explorations in medicine Ship: Seabourn Quest
EASTERN CARIBBEAN March 14-22, 2015 Focus: Primary care update Ship: Independence of the Seas
TAHITI AND TUAMOTUS March 18-28, 2015 Focus: Geriatrics, physician health Ship: Paul Gauguin
HAWAIIAN ISLANDS April 20-May 1, 2015 Focus: Improved patient care Ship: Celebrity Solstice
DALMATIAN COAST May 28-June 9, 2015 Focus: Cardiology and dermatology Ship: Celebrity Constellation
EXOTIC ASIA June 15-24, 2015 Focus: Women’s health and endocrinology Ship: Quantum of the Seas
ALASKA GLACIERS July 12-19, 2015 Focus: Leadership for physicians Ship: Celebrity Infinity
August 2-9, 2015 Focus: Cardiology and respirology Ship: Celebrity Infinity
BRITISH ISLES July 15-27, 2015 Focus: Endocrinology, gastroenterology and infectious diseases Ship: Celebrity Silhouette
MEDITERRANEAN September 19-October 2, 2015 Focus: Challenges in medicine Ship: Celebrity Equinox
ST. LAWRENCE September 19-27, 2015 Focus: Third annual McGill CME cruise Ship: Crystal Symphony
FIJI TO TAHITI November 10-21, 2015 Focus: Endocrinology and diabetes Ship: Paul Gauguin
SOUTH AFRICA November 24-December 9, 2015 Focus: Adventures in medicine Ship: Regent Seven Seas Mariner
For current promotions and pricing, contact: Sea Courses Cruises TF 1.888.647.7327 [email protected] www.seacourses.com
WORKSHOP
PROFESSIONAL BOUNDARIES IN THE PHYSICIAN-PATIENT RELATIONSHIP MATRIX HOTEL EDMONTON AB NOVEMBER 14-15
Interactive workshop on understanding and adhering to boundaries in medical practice. Presented by the College of Physicians & Surgeons of Alberta.
Keynote speaker: Dr. Glen Gabbard. Cost: $630 including tax.
Register or for more information: T 780.423.4764, ext. 4938 or 4943
SERVICES
DOCUDAVIT MEDICAL SOLUTIONS
Retiring, moving or closing your family or general practice, physician’s estate? DOCUdavit Medical Solutions provides free storage for your paper or electronic patient records with no hidden costs. We also provide great rates for closing specialists.
Contact: Sid Soil DOCUdavit Solutions TF 1.888.781.9083, ext. 105 [email protected]
DR. RxSONIC
I am your colleague and also a musician. I have been to many physicians’ conferences, workshops and get-togethers and felt that they could be more interesting with the live music. This is what I am trying to accomplish with my Dr. RxSonic project. I will be happy to play at your event whether it is a conference or workshop, seminar or friendly get-together to make it more entertaining and memorable. You will be able to listen to original music and check out unusual instruments.
> Contact: [email protected] www.DrRxSonic.com
PRIVATUS CONSULTING LTD.
Privacy Impact Assessments (PIA), does your clinic require a PIA to be completed? We specialize in PIAs for the following: VCUR 2008 or 2006 electronic medical records (EMR) solutions, Netcare access, primary care networks, diagnostic imaging clinics and amendments for existing PIAs. Competitive pricing and efficient turn-around.
Contact: Privatus Consulting Ltd. T 780.716.8100 [email protected] www.privatusconsulting.ca
RUTWIND BRAR PROFESSIONAL ACCOUNTANTS
With an established medical PC clientele, we are able to efficiently and effectively meet all of your financial needs. Our services include PC incorporations, tax planning specifically designed for physicians, their families and their PCs, as well as full accounting services.
Contact: Rutwind Brar Professional Accountants T 780.483.5490 F 780.483.5492 [email protected] www.rbpa.ca

When’s the last timeyou got excited about insurance? Some people would rather watch paint dry than talk about life insurance. But at MD, insurance is a conversation that can get pretty colourful. That’s because our clients are using creative insurance strategies to reduce tax, build wealth, create tax-smart legacies and more. MD ExO™ is a collaboration among financial advisors and specialists who engineer financial strategies exclusively for physicians. So if you could use some colour, talk to an MD Advisor about insurance-driven tax strategies. You’ll be glad you did.
The MD ExO service provides financial products and guidance to eligible clients, delivered through the MD Group of Companies (MD Physician Services Inc., MD Management Limited, MD Private Trust Company, MD Life Insurance Company and MD Insurance Agency Limited). MD Physician Services is owned by the Canadian Medical Association. Incorporation guidance limited to asset allocation and integrating corporate entities into financial plans and wealth strategies. Professional legal, tax and accounting advice regarding incorporation should be obtained in respect to an individual’s specific circumstances. All life-licensed MD advisors and specialists have life licenses with MD Insurance Agency Limited.
Let’s talk about insurance.Call 1 877 877-3707 or learn more at md.cma.ca/savetax
ACQ-14-01323 MDExO Insurance Ad_8.5x11_AlbertaDocs.indd 1 2014-08-18 1:41 PM