Embed Size (px)
Citation preview

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 1/7
Exacerbation of the ochronosis of alkaptonuria due to
renal insufficiency and improvement after renal transplantation
Wendy J. Introne,a Chanika Phornphutkul,a Isa Bernardini,a Kevin McLaughlin,b
Diana Fitzpatrick,a and William A. Gahla,*
a Section on Human Biochemical Genetics, Heritable Disorders Branch, National Institute of Child Health and Human Development,
National Institutes of Health, and the National Human Genome Research Institute, Building 10, Room 10C103 10 Center Drive,
MSC 1851, Bethesda, MD 20892-1851, USAb Faculty of Medicine, University of Calgary, Calgary, Alberta, Canada
Received 1 May 2002; received in revised form 28 June 2002; accepted 1 July 2002
Abstract
In alkaptonuria, homogentisate 1,2-dioxygenase deficiency causes tissue accumulation of homogentisic acid (HGA), followed by
signs and symptoms of ochronosis. These include massive urinary excretion of HGA, arthritis and joint destruction, pigmentation of
cartilage and connective tissue, and cardiac valve deterioration. We describe a 46-year-old man with alkaptonuria and diabetic renal
failure whose plasma HGA concentration was twice that of any other alkaptonuria patient, and whose ochronosis progressed much
more rapidly than that of his two alkaptonuric siblings. After renal transplantation, the plasma HGA normalized, and the daily
urinary excretion of HGA decreased by 2–3 g. This case illustrates the critical role of renal tubular secretion in eliminating HGA
from the body, and suggests that renal transplantation in a uremic patient not only restores HGA excretion, but may also provide
homogentisate 1,2-dioxygenase activity for the metabolism of HGA.
2002 Elsevier Science (USA). All rights reserved.
Keywords: Alkaptonuria; Homogentisic acid; Renal tubular secretion; Kidney transplantation; Ochronosis
1. Introduction
Alkaptonuria is a rare metabolic disorder due to defi-
ciency of homogentisate 1,2-dioxygenase (HGO), an en-
zyme in the tyrosine degradation pathway [1,2]. The
homogentisatedioxygenase gene, HGO, hasrecentlybeen
isolated [3], its organization reported [4], and several dif-
ferent mutations defined [3,5–7]. As a consequence of HGO deficiency, homogentisic acid (HGA) accumulates.
This compound is readily oxidized to benzoquinones,
which polymerize and constitute the ochronotic pigment
which binds to connective tissue [1]. This process destroys
joints, spinal disks, and bones. Often, the first sign of al-
kaptonuria is dark urine, which acquires its color due to
oxidation of HGA upon standing or exposure to alkaline
substances. Other manifestations include ochronotic
pigmentation of the sclerae, ear helices, and fingers, early
onset of arthritis affecting the spine first andlater the large
joints, kidney and prostate stones, and valvular heart
disease [1,8]. Definitive diagnosisis based uponthe finding
of gram quantities of HGA in a 24-h urine collection; the
HGA can be detected by gas chromoatography-mass
spectrometric analysis for organic acids, or by a specificassay [9]. Treatment of alkaptonuria is symptomatic [1],
although the use of 2-(2-nitro-4-trifluoromethylbenzoyl)-
1,3-cyclohexanedione (nitisinone), an approved therapy
for tyrosinemia type I [10], to block HGA formation has
recently been proposed [11].
Normally, the kidney clears the offending homogen-
tisic acid so effectively that alkaptonuria patients excrete
gram quantities of HGA each day. This high level of
HGA removal is achieved by active renal tubular se-
cretion of HGA; patients with large filtered loads of
HGA have fractional excretions which are several
hundredfold normal. The salutary effects of tubular
Molecular Genetics and Metabolism 77 (2002) 136–142
www.academicpress.com
*Corresponding author. Present address: MGB, NHGRI, NIH, 10
Center Drive, MSC 1851, Building 10, Room 10C103, Bethesda, MD
20892-1851, USA. Fax: 301-402-2740.
E-mail address: [email protected] (W.A. Gahl).
1096-7192/02/$ - see front matter 2002 Elsevier Science (USA). All rights reserved.
PI I : S 1 0 9 6 - 7 1 9 2 ( 0 2 ) 0 0 1 2 1 - X

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 2/7
secretion on the symptoms of AKU become especially
apparent when severe renal disease occurs. We now
report the impact of kidney failure on the severity of
ochronosis in a single member of a sibship including
three adults with alkaptonuria.
2. Patients and methods
2.1. Case histories
Two brothers and their sister, all having alkaptonu-
ria, were admitted to the NIH Clinical Center under a
protocol approved by the National Institute of Child
Health and Human Development institutional review
board. Each gave informed consent to participate in a
study of the clinical, biochemical, and molecular aspects
of alkaptonuria. Patient numbers correspond to a mas-
ter list of enrolled individuals.Patient #11 was a 48-year-old woman with intermit-
tent hip pain for 10 years, right shoulder pain for 2.5
years following a motor vehicle accident, recent onset of
knee pain, and bouts of migrating bone pain. She also
complained of back stiffness, but without pain, and had
an intermittent black discharge from her breasts. She
was diagnosed with alkaptonuria based upon ear pig-
mentation and the previous diagnosis of her brother,
patient #12.
Patient #12, a 46-year-old male, noted episodes of
numbness in his left leg at 34 years of age. Spine ra-
diographs revealed five calcified discs, and a discectomy
was performed at the age of 35. The patient also un-
derwent steroid injections into his ears to relieve in-flammation and tenderness in both helices. A biopsy of
his inflamed right ear at age 43 revealed ochronotic
material, making the diagnosis of alkaptonuria. At age
45, the patient underwent a right total knee replacement.
At the time of surgery, the right fibula was healing from
a spontaneous fracture. Upon admission to the NIH
Clinical Center, the patient suffered from back pain,
most severe in the lumbosacral region and associated
with severe degenerative changes throughout the spine.
Ambulation was limited to approximately one-half a
block. He also complained of shoulder, elbow, and leftknee pain, and range of motion was decreased in his
shoulders, elbows and knees. The patient had a 23-yearhistory of insulin-dependent diabetes, and the resultant
nephropathy had worsened significantly since his knee
replacement.
A third sibling, patient #13, was a 41-year-old man
with a history of dark urine. He had been otherwise
asymptomatic until the age of 37 when he sustained an
injury to his back. The pain and limited mobility
worsened despite physical therapy. One and one half
years after the injury, this man underwent a discectomy.
Like his brother, he suffered from inflammation andtenderness of the ears. A biopsy of the left helix at age 38
showed black cartilage. He never required a joint re-
placement. When seen at the NIH, the patient com-
plained of severe back pain, as well as pain in the
shoulders, knees, and hips.
2.2. Mutation analysis
Genomic DNA was obtained from whole blood using
standard extraction procedures [12]. The coding region of
the HGO gene, comprising exons 1–14, was amplified
using primers shown in Table 1. PCR amplification of
genomic DNA was performed using 1 lL of DNA, 1
PCR buffer (GIBCO-BRL), 0.75 mM MgCl2,100 lMdNTPs, 0.1 lM of each primer, and 1.0U Taq
DNA polymerase in a total volume of 25 lL. An initial
denaturation step of 96 C for 4 min was followed by 35
PCR cycles, each with a denaturation step of 94 C for
Table 1
PCR amplification primers for exons of the HGO gene
Exon Primers Fragment
size (bp)
Annealing
temperature
Forward Backward
1 gcctctggaaacacttaggaac ctgataccctgaagttctcag 355 60
2 gaggttacagtgtagacccac gaccatctggcaacccgatatg 479 62
3 catatcgggttgccagatggtc gaacatacctctagtcagctc 638 62
4 gagccattctgtgtatcactc catagcagcatgagaatggac 223 58
5 caaacatgtgtgtgcacgtgc cttggcattcaggctgcaaatg 359 64
6 gaaatgtgcctcatgaacctc gtgcatatgacttcacaag 285 60
7 gactctaagttccacaagggc ctagacctcagtctctggattg 338 64
8 aatgcagccttaagcctttcc ctcgttgtccagacatgacag 278 58
9 tatctctggacccaatgagag ctgggaagacacttggtctag 517 60
10 taccagactggaaatgcagtg aacactcgccttggcaatcag 354 62
11 cagctgcagcttatgaacc ctgtaaatgtcaggggtctac 413 60
12 gtccttctcacaacatgtggg gtgcagcaggatcctgaattc 546 62
13 ctgattcctgtcagagagtgg ctgctgggttggatactatac 780 60
14 cccataccttctgttgacatc tcttgcaagactgacctgac 512 60
W.J. Introne et al. / Molecular Genetics and Metabolism 77 (2002) 136–142 137

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 3/7
30 s, a 1 min annealing step at the temperatures listed in
Table 1, and an extension step at 72 C for 1 min. Am-
plification cycles were followed by an elongation step at
72 C for 10 min, with storage at 4 C. Automated se-
quencing was performed using a CEQ Dye Terminator
Cycle sequencing Kit, according to manufacturer’s pro-
tocol (Beckman–Coulter).
2.3. Homogentisic acid determinations
Homogentisic acid in urine and deproteinized plasma
was assayed using the colorimetric method of Lustberg
et al. [9]. The HGA was first oxidized to benzoquinone
acetic acid and then reacted with diethylene-triamine to
form an adduct, which exhibited an absorption maxi-
mum at 385 nm and a very high extinction coefficient.
The assay was reliable for samples containing >2.5 lg/
mL or >15 lM.
3. Results
3.1. Molecular diagnostics
All 14 exons of the HGO gene of patient #12 were
sequenced and two heterozygous mutations were iden-
tified. One is a known G to A substitution at the IVS1-1
position creating a splice site abnormality [6]. The sec-
ond mutation is a G to A substitution at nucleotide 648,
changing a glycine to an arginine at codon 161. Based
on functional analysis studies performed by Rodriguez
et al. [13], this mutation is predicted to provide 1% of
wild-type activity.
3.2. Renal function
Creatinine clearances were calculated in duplicate for
all three siblings, as well as for unaffected individuals,
and adjusted for body surface area. The renal function
of patient #12 was approximately 31 mL/min/1.73 m2, or30% of that of his affected brother and sister (Table 2).
The value for patient #12 was consistent with the
technetium-99 m DTPA measurement of glomerular
filtration rate performed one year prior to the NIHadmission, i.e., 28.4 mL/min/1.73 m2.
3.3. Homogentisic acid (HGA) levels
Homogentisic acid was measured in plasma and urine
for all three siblings and for normal and AKU controls.
While patients #11 and #13 displayed plasma and urine
HGA values typical of AKU patients, the plasma HGA
values for patient #12 were 4–7 times higher (Table 2).The urine HGA of patient #12, 200 times that of normal
controls, was well within the range for his siblings andother alkaptonuria patients.
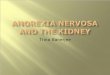
3.4. Ochronosis
In the three years prior to admission to the NIH,
patient #12 had noticed a significant increase in the
degree of ochronotic pigmentation of his skin, particu-
larly his face. On physical examination, he manifested
significant darkening of his neck, face, and sclerae,
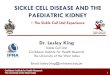
particularly compared with his two affected siblings(Fig. 1). Additional evidence of enhanced ochronosis
appeared over his spine, along the lateral aspects of his
index fingers, and in his disfigured ear helix (Fig. 2).
3.5. Radiographic findings
The radiographic findings of patient #12 were signifi-
cantly advanced compared to those of his siblings and of
other alkaptonuria patients his age. Patient #12 had
pronounced degenerative changes in the cervical spine,
while the cervical spine of hisolder sister, patient #11, was
relatively spared, with good intervertebral disc height and
no evidence of calcification (Fig. 3A). In addition, patient
#12 had nearly complete loss of the discs in the thoracicand lumbar spine, with obvious calcification at nearly
every level of thethoracic and lumbarregion andcomplete
loss of lumbar lordosis (Fig. 3B). In contrast, the thoracic
and lumbar regions of the spine of patient #11 showed
milder loss of intervertebral disc height and disc calcifi-
cation, with the lumbar region more severely affected than
the thoracic area (Fig. 3B).
Patient #11 had mild narrowing of the knee joints, but
no other bone or joint abnormalities in the upper or lower
extremities. Radiographs of the upper extremities of pa-
tient #13 revealed no significant bone or joint abnor-malities. Views of the lower extremities demonstrated
Table 2
Baseline renal function and HGA values
Parameter Patients Other Alkaptonuriaa
#11 #12 #13
Cr Cl (mL/min/1.73 m2) 83, 71 33, 29 104, 133 79 22
Plasma HGA (lg/mL) 3.8, 9.1 14.4, 27.8 5.0, 5.0 6.6 2.6
Urine HGA (g/day) 2.7, 3.1 6.3, 6.4 10.8, 9.1 4.9 2.2
a N ¼ 58, mean SD. Normal creatinine clearance values for adults are 90–125mL/min. Normal plasma HGA values are below the level of
detection. Plasma and urine values of HGA in alkaptonuria patients are 2–3 orders of magnitude greater than normal.
138 W.J. Introne et al. / Molecular Genetics and Metabolism 77 (2002) 136–142

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 4/7
Fig. 1. Faces and sclerae of patients #11, #12, and #13. Note enhanced pigmentation in patient #12 compared with his older sister

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 5/7
mild degenerative changes in the hip joints. In contrast,
patient #12 had narrowing of both hips and elbow joints
and the left knee joint. Calcifications were also noted in
both hips adjacent to the greater trochanter and ischium
and in the shoulders adjacent to the greater tuberosity(data not shown).
3.6. Effects of renal transplantation
Patient #12 received a renal allograft from an unaf-
fected sister proven on molecular grounds not to carry
either of her brother’s HGO mutations. Three to six
months after renal transplantation, his plasma and urine
HGA values had fallen to approximately half their pre-
transplant levels (Table 3).
4. Discussion
The signs and symptoms of alkaptonuria, including
cartilage pigmentation, arthritis, and cardiac valve dete-
rioration, reflect generalized damage to connective tissue.
This occurs due to binding of HGA and/or its oxidation
products, benzoquinone acetic acid and its polymers,
to cartilage, bones, and joints. Ochronotic pigment ac-
cumulation and damage may exhibit a predilection forthese tissues, either because they turn over slowly and
accumulate benzoquinones over time, or because their
abundant collagen content avidly binds HGA and ben-
zoquinones.Although alkaptonuria manifests clinically in joints
and peripheral tissues, the bulk of tyrosine catabolism,
and HGA production, occurs in the liver, with a minor
contribution from the kidneys [1]. The kidney eliminates
nearly all the HGA produced in the body, with the
blood serving as a conduit for transport from the liver to
the kidney. Consequently, the flux through the tyrosine
catabolic pathway can be estimated by the total daily
urinary HGA in alkaptonuria patients lacking HGO
activity, i.e., 4–8 g [1]. Glomerular filtration alone can-
not rid the alkaptonuric body of this huge HGA load.
Even if the plasma HGA level rose as high as 10 lg/mL,
Fig. 2. Ochronotic tissues in patient #12. Darkened cartilage is visible under the skin covering the spine (A), in the helix of the disfigured right ear (B),
and in the webbing between the first and second digits (C).
140 W.J. Introne et al. / Molecular Genetics and Metabolism 77 (2002) 136–142

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 6/7

8/10/2019 alakpt kidney.pdf
http://slidepdf.com/reader/full/alakpt-kidneypdf 7/7
a glomerular filtration rate of 100 mL/min would yield a
filtered load of only 1 mg/min or 1.44 g per day. This is
less than the measured excretion in most patients. In
actuality, renal tubular secretion enhances HGA re-
moval, such that HGA clearances approximate 400–
500 mL/min, close to the rate of renal blood flow [1].
This enormous clearance rate maintained plasma HGA
levels in the range of 7 lg/mL in our alkaptonuria pa-
tients (Table 2).
In view of the critical role of the kidney in HGA re-
moval, it is reasonable to expect that the renal failure of
patient #12 was responsible for his increased plasma
HGA concentrations and worsening ochronosis. There-
fore, it was not surprising that this patient’s plasma HGA
decreased after his filtration and secretion functions were
restored by a renal allograft procedure (Table 3).
It was surprising, however, that normalization of renal
filtrationandsecretionwas accompanied by a reductioninurinary HGA. We propose that this occurred because the
donor kidney provided HGO activity, reducing the
amount of HGA that accumulated. Based upon the spe-
cific activity of HGO in human kidney, i.e., 2.7–5.4 lmol
of HGA metabolized per hour per 0.1 g of wet weight [14],a normal 120-gram kidney should be able to metabolize
13–26 g of HGA per day. The actual amount metabolized
would depend upon how much of the plasma HGA could
be delivered to the intracellular location of the enzyme.
Nevertheless, it appears plausible that the transplanted
HGO enzymatic activity may have been responsible for
the absolute reduction (by 2–3 g) in the patient’s daily
HGA excretion (Table 3), in spite of the relative increase
(i.e.,as a percentage of thefilteredload) in HGA secretion.
This case illustrates the critical role the kidneys play in
eliminating HGA from the bodies of alkaptonuria pa-
tients. We suggest that renal transplantation may havedual salutary effects upon patients in kidney failure, i.e.,
increased fractional excretion of HGA, resulting in lower
plasma HGA concentrations, and increased metabolism
of HGA, resulting in lower total body production of
HGA. Further evidence and additional cases are required
to substantiate this hypothesis. The course of patient #12
alsoemphasizes the crucial importance of preserving renal
function in alkaptonuria patients. Only a single case of
ochronotic nephrosis has been reported [15], but ob-
struction from renal stones, which occurs frequently in
alkaptonuria[1], should be avoided to prevent consequent
renal impairment.
References
[1] B.N. La Du, Alkaptonuria, in: C.R. Scriver, A. Beaudet,W. Sly,D. Valle (Eds.), The Metabolic and Molecular Bases of Inherited
Disease, vol. 2, eigth ed., McGraw-Hill, New York, 2001, pp.
2109–2123.
[2] B.N. La Du, V.G. Zannoni, L. Laster, J.E. Seegmiller, The nature
of the defect in tyrosine metabolism in alkaptonuria, J. Biol Chem
230 (1958) 251–260.
[3] J.M. Fernandez-Canon, B. Granadino, D. Beltran-Valero de
Bernabe, M. Renedo, E. Fernandez-Ruiz, M.A. Penalva, S.
Rodriguez de Cordoba, The molecular basis of alkaptonuria, Nat.
Genet. 14 (1996) 19–24.
[4] B. Granadino, D. Beltran-Valero de Bernabe, J.M. Fernandez-
Canon, M.A. Penalva, S. Rodriguez de Cordoba, The human
homogentisate 1,2-dioxygenase (HGO) gene, Genomics 43 (1997)
115–122.
[5] D. Beltran-Valero de Bernabe, B. Granadino, I. Chiarelli, B.
Porfirio, E. Mayatepek, R. Aquaron, M.M. Moore, J.J.M. Festen,
R. Sanmarti, M.A. Penalva, S. Rodriguez de Cordoba, Mutation
and polymorphism analysis of the human homogentisate 1,2-
dioxygenase gene in alkaptonuria patients, Am. J. Hum. Genet. 62
(1998) 776–784.
[6] D. Beltran-Valero de Bernabe, F.J. Jimenez, R. Aquaron, S.
Rodriguez de Cordoba, Analysis of alkaptonuria (AKU) muta-
tions and polymorphisms reveals that the CCC sequence motif is a
mutational hot spot in the homogentisate 1,2 dioxygenase gene
(HGO), Am. J. Hum. Genet. 64 (1999) 1316–1322.
[7] A. Zatkova, D. Beltran-Valero de Bernabe, H. Polakova, M.
Zvarik, E. Ferakova, V. Bosak, V. Ferak, L. Kadasi, S. Rodriguez
de Cordoba, High frequency of alkaptonuria in Slovakia:
Evidence for the appearance of multiple mutations in HGOinvolving different mutational hot spots, Am. J. Hum. Genet. 67
(2000) 1333–1339.
[8] W.M. O’Brien, B.N. La Du, J.J. Bunim, Biochemical, pathologic,
and clinical aspects of alkaptonuria, ochronosis and ochronotic
arthropathy, Am. J. Med. 34 (1963) 813–838.
[9] T.J. Lustberg, J.D. Schulman, J.E. Seegmiller, The preparation
and identification of various adducts of oxidized homogentisic
acid and the development of a new sensitive colorimetric assay for
homogentisic acid, Clin. Chim. Acta 35 (1971) 325–333.
[10] S. Lindstedt, E. Holme, E.A. Lock, O. Hjalmarson, B. Strand-
vik, Treatment of hereditary tyrosinaemia type I by inhibition of
4-hydroxyphenylpyruvate dioxygenase, Lancet 340 (1992) 813–
817.
[11] Y. Anikster, W.L. Nyhan, W.A. Gahl, NTBC and alkaptonuria,
Am. J. Hum. Genet. 63 (1998) 920–921.[12] J. Sambrook, E.F. Fritsch, T. Maniatis, Molecular Cloning: A
Laboratory Manual, second ed., Cold Spring Harbor Laboratory,
Cold Spring Harbor, NY, 1989.
[13] J.M. Rodriguez, D.E. Timm, G.P. Titus, D. Beltran-Valero de
Bernabe, O. Criado, H.A. Mueller, S. Rodriguez de Cordoba,
M.A. Penalva, Structural and functional analysis of mutations in
alkaptonuria, Hum. Mol. Genet. 9 (2000) 2341–2350.
[14] V.G. Zannoni, J.E. Seegmiller, B.N. La Du, Nature of the defect
in alkaptonuria, Nature 193 (1962) 952–953.
[15] J.A. Cooper, T.J. Moran, Studies on ochronosis. I. Report of case
with death from ochronotic nephrosis, Arch. Pathol. 64 (1957) 46–
53.
Table 3
Effects of renal transplantation on HGA values of patient #12
Pre-transplant Time after transplant
3 months 6 months
Cr Cl (mL/min/1.73 m2) 31 71 55
Plasma HGA (lg/mL) 21.1 7.3 13.3
Urine HGA (g/day) 6.4 2.7 4.0
142 W.J. Introne et al. / Molecular Genetics and Metabolism 77 (2002) 136–142