Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 8 , N O . 1 2 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 6 . 0 5 3
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
AL (Light-Chain) Cardiac Amyloidosis
A Review of Diagnosis and TherapyRodney H. Falk, MD,a Kevin M. Alexander, MD,a Ronglih Liao, PHD,a Sharmila Dorbala, MD, MPHa,b
JACC JOURNAL CME
This article has been selected as the month’s JACC Journal CME activity,
available online at http://www.acc.org/jacc-journals-cme by selecting the
CME tab on the top navigation bar.
Accreditation and Designation Statement
The American College of Cardiology Foundation (ACCF) is accredited by
the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
The ACCF designates this Journal-based CME activity for a maximum
of 1 AMA PRA Category 1 Credit(s). Physicians should only claim credit
commensurate with the extent of their participation in the activity.
Method of Participation and Receipt of CME Certificate
To obtain credit for JACC CME, you must:
1. Be an ACC member or JACC subscriber.
2. Carefully read the CME-designated article available online and in this
issue of the journal.
3. Answer the post-test questions. At least 2 out of the 3 questions
provided must be answered correctly to obtain CME credit.
4. Complete a brief evaluation.
5. Claim your CME credit and receive your certificate electronically by
following the instructions given at the conclusion of the activity.
CME Objective for This Article: On completion of this activity the learner
should be able to: 1) recognize the clinical and non invasive features that
From the aBrigham and Women’s Hospital Cardiac Amyloidosis Program, H
Section of Cardiology, Brigham and Women’s Hospital, Boston, Massachus
Nuclear Medicine and Molecular Imaging, Harvard Medical School, Boston,
the Demarest Lloyd Jr. Foundation, The Friends of Burt Glazov Cardiac Amy
Foundation. Dr. Falk receives funds for consulting from Ionis Pharmaceu
support from GlaxoSmithKline. All other authors have reported that they h
paper to disclose.
Manuscript received June 9, 2016; accepted June 14, 2016.
suggest a diagnosis of light-chain (AL) cardiac amyloidosis; 2) promptly
initiate and complete a diagnostic workup for cardiac amyloidosis,
including a timely referral to a hematologist if AL amyloidosis is sus-
pected; and 3) prescribe appropriate heart failure therapy for cardiac
amyloidosis, avoiding drugs that are poorly tolerated in AL amyloidosis
and providing appropriate diuretic therapy adjustments in a patient un-
dergoing chemotherapy.
CME Editor Disclosure: JACC CME Editor Ragavendra R. Baliga, MD,
FACC, has reported that he has no financial relationships or interests to
disclose.
Author Disclosures: This study was supported in part by the Demarest
Lloyd Jr. Foundation, The Friends of Burt Glazov Cardiac Amyloidosis
Fund, and the Harold Grinspoon Charitable Foundation. Dr. Falk receives
funds for consulting from Ionis Pharmaceuticals and Alnylam Pharma-
ceuticals; and research support from GlaxoSmithKline. All other authors
have reported that they have no relationships relevant to the contents of
this paper to disclose.
Medium of Participation: Print (article only); online (article and quiz).
CME Term of Approval
Issue Date: September 20, 2016
Expiration Date: September 19, 2017
arvard Medical School and Department of Medicine,
etts; and the bDepartment of Radiology, Division of
Massachusetts. This study was supported in part by
loidosis Fund, and the Harold Grinspoon Charitable
ticals and Alnylam Pharmaceuticals; and research
ave no relationships relevant to the contents of this

Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1324
AL (Light-Chain) Cardiac Amyloidosis
A Review of Diagnosis and Therapy
Rodney H. Falk, MD,a Kevin M. Alexander, MD,a Ronglih Liao, PHD,a Sharmila Dorbala, MD, MPHa,b
ABSTRACT
The amyloidoses are a group of protein-folding disorders in which$1 organ is infiltrated by proteinaceous deposits known
as amyloid. The deposits are derived from 1 of several amyloidogenic precursor proteins, and the prognosis of the disease is
determined both by the organ(s) involved and the type of amyloid. Amyloid involvement of the heart (cardiac amyloidosis)
carries the worst prognosis of any involved organ, and light-chain (AL) amyloidosis is the most serious form of the disease.
The last decade has seen considerable progress in understanding the amyloidoses. In this review, current and novel
approaches to the diagnosis and treatment of cardiac amyloidosis are discussed, with particular reference to AL
amyloidosis in the heart. (J Am Coll Cardiol 2016;68:1323–41) © 2016 by the American College of Cardiology Foundation.
C ardiac amyloidosis is a condition in whichthe extracellular space of the heart isexpanded by an amorphous, fibrillar pro-
teinaceous material known as amyloid (Figure 1).The nonbranching fibrils of amyloid are composednot only of fragments of the precursor protein, butalso contain proteoglycans and serum amyloid P(SAP). They are generally extremely resistant todegradation, although evidence suggests that amy-loid does slowly resorb from the body once fibrillo-genesis has been halted (1,2). Amyloid can beformed from a large number of different precursorproteins (Table 1), but the most common forms thatproduce amyloid that affects the heart areimmunoglobulin-derived light chains and transthyre-tin (TTR; previously called prealbumin). Rarely, sec-ondary amyloid may cause cardiac involvement, butthis is an uncommon manifestation of a type of amy-loid rarely seen in Western countries. TTR is a trans-port protein of thyroid hormone and retinol(vitamin A); hence, the name, transthyretin.TTR-derived amyloid may be formed from wild-type(normal) TTR or from a mutant form, of which >80amyloidogenic mutations have been described. Pre-cise definition of the precursor protein causing amy-loid deposition is essential because the differentforms of amyloidosis have differing clinical coursesand completely different therapies. TTR amyloidosis(ATTR) has recently been reviewed in detail in theJournal (3), and therefore, this review concentrateson light-chain (AL) amyloidosis as it affects the heart,addressing TTR amyloidosis predominantly when itdiffers from AL amyloidosis.
It is important to recognize that cardiac amyloidosisis part of a systemic disease, and is not an isolated
condition. In AL amyloidosis, renal, neural, and/ordermatologic involvement often coexists with heartinvolvement. Less commonly, symptomatic hepaticand gastrointestinal infiltration may occur. Patientswith familial amyloidosis (mutant TTR amyloidosis[ATTRm]) often have a phenotype that is deter-mined to a large degree by the specific mutation,with neuropathy-predominant, cardiac-predominant,and mixed phenotypes tending to run in families,although exceptions do exist. Wild-type TTRamyloidosis (ATTRwt), in which the precursor proteinis structurally normal TTR, almost invariably presentsas a clinically isolated cardiomyopathy. However, thecondition was formerly named senile systemicamyloidosis because of the subclinical involvement ofother organs noted at autopsy (most commonly, thelungs and gastrointestinal tract) and a high prevalenceof carpal tunnel syndrome due to amyloid infiltration.
Until recently, cardiac amyloidosis was viewed as arare condition, often only diagnosed at autopsy, andwas considered untreatable when diagnosed duringlife. Enormous advances have been made over the lastdecade, both in diagnosis and treatment of cardiacamyloidosis, along with a recognition that the condi-tion is more common than previously believed. Thisreview gives a detailed overview of cardiac amyloid-osis with an emphasis on AL amyloidosis, describes adiagnostic approach to the various types, and dis-cusses novel and experimental treatments.
AL amyloidosis is a hematologic disorder of plasmacells closely related to, but generally distinct from,multiple myeloma. It is caused by the proliferation ofan abnormal clone of plasma cells that overproducelambda, or less commonly, kappa light chains. Inmultiple myeloma, most of the cellular components

AB BR E V I A T I O N S
AND ACRONYM S
AL amyloidosis = light-chain
amyloidosis
ATTR amyloidosis =
transthyretin amyloidosis
ATTRm amyloidosis = mutant
transthyretin amyloidosis
ATTRwt = wild-type
transthyretin amyloidosis
CMR = cardiac magnetic
resonance
CPHPC = (R)-1-[6-[(R)-2-
carboxy-pyrrolidin-1-yl]-6-
oxo-hexanoyl]pyrrolidine-2-
carboxylic acid
DPD = 2,3-dicarboxypropane-1,
1-diphosphonate
ECG = electrocardiography
LGE = late gadolinium
enhancement
LV = left ventricular
MGUS = monoclonal protein of
unknown significance
NT-proBNP = N-terminal pro–
B-type natriuretic peptide
SAP = serum amyloid
P component
TcPYP = technetium
pyrophosphate
TTR = transthyretin
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1325
of the bone marrow may consist of plasma cells, andin overt disease, this results in bone lesions, anemia,hypercalcemia, and/or renal dysfunction (4). Incontrast to myeloma, most patients with ALamyloidosis have #20% of plasma cells in themarrow, and the manifestations of the disease aredue to the formation of amyloid from the abnormalcirculating free light chains (5). Approximately 5% to10% of patients with AL amyloidosis will have evi-dence of overt multiple myeloma, and a similar pro-portion of multiple myeloma patients will have ALamyloidosis. It is estimated that AL amyloidosis isapproximately one-tenth as common as multiplemyeloma, with an estimated annual age-adjustedincidence in the United States of 10.5 cases permillion person-years (6).
AL amyloidosis is a multiorgan disease, although 1organ system usually predominates. It mostcommonly affects the kidney, resulting in nephroticsyndrome, with clinical cardiac involvement beingthe second most common presenting manifestation.Other organ systems that may be involved include theperipheral and autonomic nervous system, thevasculature, the liver and gastrointestinal tract, andthe soft tissues. Cerebral involvement does not occurin AL amyloidosis. Previous reviews of amyloidosishave often stressed that cardiac involvement in ALamyloidosis almost always occurs in the setting ofanother significant organ involvement, and that iso-lated cardiac disease is present in <5% of cases. In ourexperience, this is probably not true. Although the
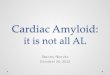
FIGURE 1 Endomyocardial Biopsy
Staining with hematoxylin and eosin (left) and sulfated Alcian blue (rig
compressing the cardiomyocytes. This leads to myocardial dysfunction,
damage. The inset on the left shows an electron microscope image of an
the right shows amyloid surrounding a small vessel. This can result in a
coronary angiography. (see text for more details). Courtesy of Robert P
exact prevalence of clinically isolated ALcardiac amyloidosis is unknown, it is likelythat is has been underestimated in the past,due to the rapid progression to death in un-diagnosed patients. The increasingly sophis-ticated diagnostic tools currently used inheart failure appear to be leading to earlierdiagnosis, thereby possibly lessening misseddiagnoses.
The importance of early diagnosis of ALcardiac amyloidosis cannot be stressedstrongly enough. Untreated, the median sur-vival from onset of heart failure is approxi-mately 6 months (6), but modern therapiescan put the disease into a prolonged remis-sion and extend life by many years (7). Thereis a slight male predominance of AL cardiacamyloidosis, and the disease generally pre-sents from the fifth to seventh decade,although it may occur at all ages from thefourth decade onward.
CLINICAL ASPECTS. All types of cardiacamyloidosis share a common pathologicalaspect, namely, the extracellular depositionof amyloid in the heart. The different formsof amyloid are generally indistinguishable bylight microscopy, and by the time heart fail-ure is present, extensive amyloid is easilyvisible (Figure 1). The amyloid deposits
expand the extracellular space and stiffen the heartht). Note that the amyloid deposits are extensive and extracellular,
due to both stiffening of the extracellular space and direct myocyte
amyloid deposit, demonstrating the nonbranching fibrils. The inset on
ngina with normal-appearing epicardial coronary arteries seen on
adera, MD, Brigham and Women’s Hospital, Boston, Massachusetts.

TABLE 1 Overview of the Common Forms of Amyloidosis That May Affect the Heart
AmyloidNomenclature Precursor Protein Age Range, yrs Sex Clinical Clues Laboratory Abnormalities
AL Light chains 50þ Either Multiorgan involvement.Periorbital bruising or
macroglossia are almostpathognomonic of AL insetting of typical MRI orechocardiogram.
Severe hypotension with ACEinhibitors.
Elevated serum free lambda orkappa, with abnormal ratio.Monoclonal spike in serumand/or urine. Suppressedimmunoglobulins.
Proteinuria.
ATTRwt Wild-type (normal)transthyretin
65þ Marked malepredominance,>15:1
History of carpal tunnel syndrome5-10 yrs earlier, with noother organ involvement.
No specific abnormalities.(Normal free light chainvalues, no proteinuria)
ATTRm Mutant transthyretin 40þ (mutationdependent). InV122I, thecommon African-American variant,usual age ofclinical onset is60-65 yrs.
Either, slight malepredominance.
African-American/Caribbean origin(for V122I TTR variant).
No specific abnormalities onroutine testing.
Genetic testing reveals mutationin TTR molecule
AA (Secondary) Serum amyloid A(an acute phase protein)
May occur in 20s–30supward withsevereinflammatorydisease.
Either Underlying chronic inflammatorydisease.
Hepatomegaly, splenomegaly.Usually no cardiac involvement,
but in rare cases may be severe
High ESR/CRP. Proteinuria.
ACE ¼ angiotensin-converting enzyme; CMR ¼ cardiac magnetic resonance; CRP ¼ C-reactive protein; ECG ¼ electrocardiogram; ESR ¼ erythrocyte sedimentation rate; LBBB ¼ left bundle branch block;TTR ¼ transthyretin.
Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1326
without producing compensatory dilation, which re-sults in a restrictive pathophysiology involving bothventricles (Figure 2). Atrial amyloid infiltration isalmost always present and frequently causes atrialcontractile dysfunction. Amyloid deposition also
FIGURE 2 Autopsy Specimen of the Heart From a Patient Who Died
(Left) Biatrial dilation with thickened atrial septum and extensive thicke
due to amyloid infiltration. (Right) Close-up view of the atrium, showing t
leads to atrial dysfunction, and the irregular endocardial deposits can for
of atrial thrombi in amyloid cardiomyopathy. Courtesy of Robert Padera
occurs on valves and perivascularly. Although theprecise type cannot be distinguished from the patternof amyloid deposition, it appears that there aredifferent deposition patterns in TTR and AL amyloid-osis, with a predominance of diffuse peri-cellular,
of Cardiac Amyloidosis
ning of the left ventricle (and, to a lesser degree, the right ventricle),
he waxy, irregular surface due to amyloid deposition. Atrial infiltration
m a nidus for thrombus formation, accounting for the high prevalence
, MD, Brigham and Women’s Hospital, Boston, Massachusetts.

FIGURE 3 Postulated Mechanisms Leading to Progressive Heart Failure in
AL Amyloidosis
Amyloid fibersAmyloid precursorprotein and/oroligomers
Structural damage Proteotoxicity
Increased cardiac andvascular stiffnessImpaired contractionand relaxationDisturbed electricalconductance
Stress kinase activationLysosomal dysfunctionDefective autophagyROSCellular dysfunction/impaired calciumhomeostasisDefectedmitochondrialfunctionCell death
Infiltration of the myocardium causes physical cellular damage and restrictive patho-
physiology, whereas circulating cardiotoxic light chains produce cellular damage through
various pathways (see text for details). In other forms of cardiac amyloid, such as TTR, the
sole (or overwhelmingly predominant) mechanism of cardiac dysfunction is the infiltrative
component. ROS ¼ reactive oxygen species; other abbreviations as in Figure 1.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1327
endocardial, and arterial and/or arteriolar depositsin AL amyloidosis and nodular deposits in ATTR (8).
The pathophysiology of cardiac AL amyloidosisdiffers from that of ATTR amyloidosis. Specifically,although both diseases are associated with extracel-lular fibril deposition within the myocardium, whichleads to passive myocardial restriction and dysfunc-tion, clinical observations have suggested that theseverity of heart failure in AL amyloidosis is moresevere than in TTR amyloidosis, despite higher leftventricular (LV) mass in the latter (9). This observa-tion, coupled with the discordance between clinicalimprovement and lack of change in standard echo-cardiographic parameters after successful hema-tologic treatment, led to the suggestion that ALamyloidosis might have both toxic and infiltrativecomponents (10).
Shortly after this observation was made, amyloi-dogenic light-chain toxicity was demonstrated in anisolated, perfused heart model—a case of “bedside tobench” research (11). Not all light chains are car-diotoxic, and LV dysfunction is not seen in multiplemyeloma without amyloidosis, nor in AL amyloidosiswithout myocardial infiltration, which suggests thatamyloid infiltration of the heart is required beforelight-chain cardiotoxicity can be clinically manifest.Unpublished observations by one of the authors(R.H.F.) has also suggested that, although most ALamyloidosis patients with evidence of cardiacamyloidosis have heart failure, there is a small groupwho develop marked amyloid infiltration with mini-mal heart failure, similar to many ATTR amyloidosispatients. It is postulated that the amyloidogenic lightchain in these patients does not have cardiotoxicproperties.
CELLULAR ABNORMALITIES. The past decade hasseen considerable activity in elucidating the mecha-nism of the rapidly progressive nature of ALamyloidosis of the heart. Following the observationthat amyloidogenic light chains produce cardiacdysfunction in the isolated heart (12), it was demon-strated that physiological levels of amyloidogeniclight chains caused an increase in cellular reactiveoxygen species and up-regulation of heme oxygenasein rat cardiomyocytes, with associated impairment incontractility and relaxation (12). This toxic effect wasblocked by antioxidants. In a series of experiments,a cascade effect of toxic light chains from patientswith amyloidosis was demonstrated at a subcellularlevel. The initial response was lysosomal dysfunc-tion, which led to impaired autophagy and culmi-nated in elevated reactive oxygen species, cellulardysfunction, impaired calcium homeostasis, and
eventually, cell death (13). It was postulated thatimpaired autophagy, the failure to clear breakdownproducts in cells, led to this cascade, and sirolimus, apotent enhancer of both autophagosome formationand clearance, prevented the cardiomyocyte toxicityinduced by amyloidogenic light chains (13). Sirolimusis in clinical use to prevent post-transplantationrejection, but clinical studies of its use in amyloidcardiomyopathy have not yet been performed.
There have been several other investigations intopotential mechanisms by which AL amyloidosis ofthe heart causes such significant clinical dysfunc-tion. Amyloidogenic light chains were found to havea significant effect on vascular reactivity, both inhuman adipose tissue and coronary arterioles (14).Light chain–induced apoptosis and necrotic injurywere attributable to oxidative stress, and bothimpaired arteriolar reactivity and cellular damagewere largely abolished using a potent antioxidant.This vascular dysfunction, seen in vitro in humanarterioles, has a parallel in AL amyloidosis patients,in whom early endothelial dysfunction has been

FIGURE 4 Two Noncardiac Clinical Clues to the Presence of AL Amyloidosis
(Left) Small periorbital spontaneous bruise in a man with cardiomyopathy due to AL amyloidosis. He had had recurrent spontaneous bruising of
the eyes for >1 year and dyspnea for 6 months before the diagnosis was recognized. The combination of spontaneous periorbital bruising
and heart failure is virtually pathognomonic of AL amyloidosis cardiomyopathy. (Right) Macroglossia in a 65-year-old woman with AL
amyloidosis of the heart and soft tissues. Note the prominent tooth indentations on the tongue. She had seen 2 ear, nose, and throat specialists
because of her large tongue. Despite the fact that the differential diagnosis is small, neither was aware of the association with amyloidosis, and
both failed to recognize the cause. This is unfortunate, because early diagnosis would have allowed her to tolerate treatment better.
Abbreviation as in Figure 1.
Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1328
described, and in whom microvascular coronary ar-tery dysfunction is common and often severe (15).On the basis of these basic science observations, amodel of cardiac dysfunction in AL amyloidosis canbe illustrated (Figure 3), in which AL cardiacamyloidosis can be viewed as a toxic infiltrativecardiomyopathy, rather than merely an infiltrativecardiac disease.
Although much emphasis has been placed ontoxicity in AL amyloidosis, recent data suggest acardiotoxic effect of the amyloid fibrils themselves.Fibrils synthesized from light chains originallyderived from a patient with renal amyloidosis werefound to bind tightly to the surface of human car-diomyocytes and produced a disturbance of cellularmetabolic activity, but not cell death (16). There arefew animal models of AL amyloidosis, and nonemimic human cardiac amyloidosis of any variety.Nevertheless, the transgenic mouse model may behelpful for evaluating therapies, and both a TTRtransgenic mouse and an AL mouse have beendeveloped that express human mutant TTR andhuman light chains, respectively. Ward et al. (17)developed a transgenic AL mouse model that ex-presses amyloidogenic lambda-6 light chain variabledomains in the gastrointestinal tract. Using thismodel, they demonstrated that doxycycline, fed tothe mice in the drinking water, resulted in a sig-nificant reduction in amyloid deposition, with a
suggestion, on electron microscopy, that it might notonly prevent fibrillogenesis, but could induce fibrildisruption (17). A similar effect of doxycycline wasseen in a TTR amyloid model (18), and clinical trials ofthis drug are in progress (19).CLINICAL MANIFESTATIONS. Probably the mostcommon early manifestation of cardiac amyloidosisof any type is dyspnea on exertion, which progressesrelatively rapidly, and is often followed by periph-eral edema and ascites. Peripheral edema in ALamyloidosis may also be due to hypoalbuminemiaassociated with amyloid-related nephrotic syn-drome; proteinuria should always be assessed. Dys-pnea is due to LV diastolic dysfunction. However,the atria, although they do dilate, are also abnor-mally stiff, and likely contribute to dyspnea onexertion. Prominent V waves may be seen in thepulmonary capillary wedge tracings in the absence ofsignificant mitral regurgitation. Atrial arrhythmiamay be the initial manifestation of the disease; sur-prisingly, this is relatively uncommon as a present-ing feature, particularly in AL amyloidosis. Atrialinfiltration with amyloid deposits results in atrialdysfunction, and thrombus formation may occur,even in this setting of sinus rhythm. Thromboem-bolism may thus be an early manifestation of thedisease, and unless the clinician is aware of thephenomenon of left atrial systolic dysfunction,the source of neurological or systemic embolism may

FIGURE 5 Example of Typical Electrocardiograms in AL Amyloidosis
Electrocardiogram showing very low limb lead voltage with indeterminate axis and poor precordial R-wave progression in AL amyloid cardiomyopathy.
Coronary angiography was normal, and the echocardiogram showed a thick left ventricle and no pericardial effusion. This voltage/left ventricular mass
mismatch strongly suggests cardiac amyloidosis. Abbreviation as in Figure 1.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1329
not be recognized. In advanced disease, exertionalsyncope, which is most likely due to a low and fixedcardiac output, can occur, and this has a particularlypoor prognosis (20). Jaw claudication, leg claudica-tion, and angina may all occur due to small vesselamyloid deposition (21).
Physical examination of the patient with heartfailure due to cardiac amyloidosis is little differentfrom that in a patient with other forms of heart fail-ure. However, there are subtle clues that should raisethe possibility of this diagnosis. In AL amyloidosis,signs of the noncardiac disease are commonly pre-sent. Approximately 10% of patients have macro-glossia, which may vary from obvious tongueenlargement to subtle tooth indentation of thetongue (Figure 4). Periorbital bruising in the setting ofheart failure is almost pathognomonic of ALamyloidosis. Because it may be subtle, the eyelidsshould be inspected for small bruises (Figure 4).Jugular venous pressure frequently reveals an inspi-ratory rise (Kussmaul sign), a sign that is shared withpatients with constrictive pericarditis. Unlike severeheart failure caused by most other etiologies, a thirdheart sound is uncommon in cardiac amyloidosis, asis a fourth heart sound. Valvular dysfunction due to
amyloidosis is rarely severe, although on occasion,tricuspid regurgitation can be severe. Hepatomegalyusually reflects congestion, but an enlarged liver mayalso be due to amyloid infiltration in patients with ALamyloidosis. When hepatic infiltration occurs, theliver is hard and nonpulsatile, and quite distinct fromthe congested liver of heart failure. Nephrotic syn-drome is a common manifestation of AL amyloidosis,and a clinical clue to the presence of hypo-albuminemia in a patient with anasarca is extensiveedema in the absence of an elevated jugular venouspressure. The blood pressure in suspected cardiacamyloidosis is frequently low, due to a combinationof reduced cardiac output and low peripheral tone. Itshould always be measured both supine and stand-ing, because autonomic nervous system dysfunctionmay manifest as significant postural hypotension.Peripheral neuropathy is also a feature of both ALamyloidosis and familial TTR amyloidosis. It is sym-metric, predominantly sensory, and may be missed ifthe neurological examination is performed casually.However, if questioned, patients will often describemanifestations of early sensory neuropathy in thelower limbs, such as numbness in the feet or asensation of “walking on rolled up socks.” Numbness

FIGURE 6 Typical Echocardiogram in AL Amyloidosis
(Top left and right) End-systolic and end-diastolic frames, respectively, demonstrating normal ejection fraction. Note moderately thick left
ventricular walls with biatrial enlargement. The atrial size changes minimally throughout the cardiac cycle, representing failure of atrial
function, despite sinus rhythm. (Bottom) Septal tissue Doppler recording in the same patient, showing reduction in both systolic and diastolic
longitudinal velocities, despite normal ejection fraction, typical of amyloid cardiomyopathy.
Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1330
and pain in the hands may be due to carpal tunnelsyndrome, and a history of surgery for carpal tunnelsyndrome may precede the onset of heart failure by7 or 8 years.
DIAGNOSTIC TESTS
The electrocardiogram (ECG) in AL amyloidosis withcardiac involvement frequently shows low voltage,often with an unusual axis, particularly an extremeright axis (22) (Figure 5). When present, low voltage isseen in the limb leads, although voltage may benormal, or occasionally, high, in the precordial leads.Despite low-voltage QRS complexes, the P-wave isusually of normal voltage, but frequently abnormal inmorphology, and is often markedly prolonged, rep-resenting slowed atrial conduction due to amyloidinfiltration. Low-voltage ECG often precedes heartfailure, and may be present before an increase in LVwall thickness is apparent on an echocardiogram.This is an early marker of the disease. Low-voltageQRS complexes are far less common in ATTR than inAL amyloidosis, despite a greater amyloid burden inthe heart (23).
The echocardiogram typically shows concentric LVthickening, often with right ventricular thickening(Figure 6). The LV wall may be more echogenic than intrue LV hypertrophy, and due to the extensive amy-loid deposits, LV wall thickness frequently equals orexceeds 15 mm. A wall thickness >18 mm can be seenin AL amyloidosis, but is more common in ATTR. It isunusual for hypertensive heart disease to have LVwalls >15 mm, unless hypertension is severe, long-standing, and persistent; the discrepancy betweenincreased LV mass on the echocardiogram and lowvoltage on the ECG should increase suspicion of car-diac amyloidosis (23,24). Valves are mildly thickened,but there is rarely significant valvular regurgitation orstenosis. If a pacemaker is present, tricuspid regur-gitation may be more severe, both clinically andvolumetrically, than is usually seen with a pacemakerlead. This is partly because the amyloid-infiltratedtricuspid valve may not adequately mold around thepacemaker wire, and partly because even a volumet-rically small amount of regurgitation entering a stiffatrium can further significantly elevate the pressure.Left atrial contractile dysfunction may be suspectedby the absence of a transmitral A-wave and tissue

FIGURE 7 Typical Impairment of Atrial Function in Cardiac Amyloidosis Despite Sinus Rhythm, Measured by Strain Imaging
(Top left) Absence of atrial expansion during ventricular systole (loss of reservoir function) and absence of atrial contraction during late
ventricular diastole (loss of contractile function). The atrium is acting as a conduit only. (Top right) Normal atrial function in a normal patient.
(Bottom left) A transmitral Doppler pattern corresponding to the atrial strain images. Note the diminutive A-wave, despite normal E-wave
deceleration time, indicating atrial contractile dysfunction.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1331
Doppler a0 in a patient with sinus rhythm (Figure 7).Although it may be difficult to determine whether adiminutive transmitral A-wave is a function of trueatrial dysfunction or of restrictive LV pathophysi-ology, it is likely that there is at least a component ofatrial dysfunction, because cardiac amyloidosis is a4-chamber disease. Atrial strain imaging often revealsnot only a pattern of impaired atrial shortening dur-ing the period of atrial systole, but also shows a fail-ure of the atrium to expand during filling, therebyacting merely as a conduit throughout thecardiac cycle (Figure 7). Coupled with a low strokevolume and irregular atrial endocardial surfacebecause of amyloid deposits, the atrium becomes asource of thrombus formation, even when in sinusrhythm.
Doppler and tissue Doppler imaging show diastolicdysfunction in virtually all patients with cardiac
amyloidosis. It is often severe, with a restrictivepattern characterized by a short deceleration time onthe transmitral pulsed Doppler and low tissueDoppler velocities in the LV wall. E/e0 frequentlyexceeds 15, which indicates elevated LV fillingpressure. Speckle strain imaging of the LV shows anunusual pattern, which strongly suggests cardiacamyloidosis (25) (Figure 8). The apical longitudinalstrain is near-normal, with marked impairment at thebase, usually with the midventricle falling betweenthese extremes. This appearance may be present earlyin the disease, and longitudinal contractile dysfunc-tion may be severe, even when the LV ejection frac-tion is within the normal range. The stiff ventriclealso causes a prolonged period of diastasis duringmeasurement of longitudinal contraction, starting inmid-to-late systole and persisting into mid-diastole.This contrasts with the normal contractile pattern,

FIGURE 8 Typical Pattern of Color-Coded Speckle Tracking Strain Imaging in a Patient With AL Amyloidosis and a Normal LV Ejection Fraction
(Left panel) Segmental color coding in the apical 4-chamber view, with apex showing darker red, indicating more negative strain compared with pink, lesser
strain at base. (Middle panel) Individual segmental strain for the same view. (Right panel) A bull’s-eye plot derived from the 3 apical views, showing sparing
of apical strain (center of plot) with impaired mid and basal strain. LV ¼ left ventricular; other abbreviation as in Figure 1.
Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1332
in which the longitudinal ventricular relaxation be-gins shortly after maximal ventricular shortening.
Pericardial effusion is common, but is rarely large.Cardiac tamponade is rare, and if it occurs, it may bedifficult to diagnose, because it is often superimposedon heart failure with an already elevated jugularvenous pressure. In addition, the high right ventric-ular and right atrial diastolic pressures, and increasedstiffness of the chamber walls can prevent the typicalechocardiographic features of right atrial and rightventricular diastolic collapse. Thus, tamponade be-comes a diagnosis of clinical suspicion, and mayonly be confirmed if the effusion is tapped undercareful hemodynamic monitoring of cardiac fillingpressure.
Occasionally, patients with cardiac amyloidosisshow an atypical pattern of infiltration, characterizedby asymmetric septal thickening, sometimes with anLV outflow tract gradient (26). The typical abnor-mality of preserved apical longitudinal strain maystill be seen in these patients, and the cardiac mag-netic resonance (CMR) appearance usually suggestsamyloidosis, and not hypertrophic cardiomyopathy.Cardiac amyloidosis with normal wall thickness hasbeen described (27). Most of these patients have onlymild cardiac amyloidosis and may have an increasedLV thickness compared with their healthy state, butit will still be within the normal echocardiographic
range. Rarely, patients have severe heart failure witha minimal increase in wall thickness; this may be dueto extensive replacement of the myocardium byamyloid, with a reduction in cellular volume. Suchpatients usually have low voltage and a markedlyabnormal CMR. A particularly difficult patient is onewith moderate, unrelated aortic stenosis and cardiacamyloidosis, usually ATTRwt. Impaired longitudinalfunction and decreased LV cavity size can lower car-diac output, which results in apparent low-flow, low-gradient aortic stenosis. Severe LV thickening, evenfor aortic stenosis patients, may be a clue to thecoexistence of these diseases, and nuclear imagingwith pyrophosphate (PYP) or 2,3-dicarboxypropane-1,1-diphosphonate (DPD; see the following) can helpdetermine the presence of cardiac amyloidosis (28).
CMR imaging has emerged as a useful diagnosticand prognostic tool in several forms of cardiacamyloidosis. In addition to biventricular thickeningand biatrial enlargement, which can be recognizedeasily by echocardiography, there are 2 main CMRfeatures that suggest the diagnosis of cardiacamyloidosis (Figure 9): 1) difficulty in nulling themyocardium following gadolinium injection; and 2) anoncoronary, usually subendocardial, pattern ofdelayed gadolinium enhancement, both within theventricular myocardium and in the atrium (29). Gad-olinium uptake in the atrium is rarely seen in other

FIGURE 9 Use of MR for Diagnosis of Cardiac Amyloidosis and Estimate of Myocardial Amyloid Burden
TI = 100 ms TI = 180 ms TI = 260 ms TI = 920 ms TI = 1455 ms
Bull’s Eye Plot for ECVANT.
POST.
0.700.650.600.550.500.450.400.350.300.25
1
2
3
4
5
67
8
9
10
11
12 1314
1516
17
18
(Top panel) Images from a modified Look-Locker acquisition in a patient with TTR cardiac amyloidosis, shown here in the order of increasing
times after the magnetization inversion (TI). The images were acquired approximately 25 min after injection of 0.2 mmol/kg of gadolinium
contrast, and the T1 in myocardium averaged 490 and 597 ms in the blood pool. The myocardial signal nulls characteristically early compared
with the blood pool signal. (Bottom left panel) A bull’s-eye plot of extracellular volume (ECV) fraction in the same patient, calculated from
pre- and post-contrast relaxation rate measurements for each of 6 myocardial segments in basal, mid, and apical slice locations, respectively.
(Bottom right panel) Images of late gadolinium enhancement (LGE) in a 2-chamber view for the same patient. Although ECV values in this
patient approach the range measured for ECV in myocardial infarcts, the LGE image shows more muted enhancement than is seen for
myocardial infarctions, which reflects the diffuse and global effect of cardiac amyloidosis in comparison to LGE in myocardial infarctions. LGE
may therefore underestimate the severity of disease, whereas ECV provides an objective measure of extracellular space expansion. Other
abbreviations as in Figure 1. Courtesy of Michael Jerosch-Herold, PhD, Brigham and Women’s Hospital, Boston, Massachusetts.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1333
cardiac diseases, is associated with atrial contractiledysfunction, and is a strong clue to the presence ofcardiac amyloidosis (30). CMR has demonstratedincreased extracellular volume in the hearts of pa-tients with biopsy-proven amyloidosis, even in theabsence of late gadolinium enhancement (LGE),which suggests that absence of LGE does not rule out(usually early) cardiac amyloidosis (31). Although LGEis not 100% specific for the presence of amyloidosis,it does have prognostic significance. Among 241 pa-tients with amyloidosis and 9 asymptomatic carriers,there was a continuum of LGE in the myocardium,from none, through subendocardial, to transmural(32). Extracellular volume (representing amyloidburden) was measured by T1 mapping. TransmuralLGE was determined to represent advanced cardiacamyloidosis and predicted death over a mean 2-yearfollow-up, with a hazard ratio of 4.1. Importantly,these investigators pointed out that the evaluation ofLGE was technically far more accurate when phase-sensitive inversion recovery was used to determine
the null point of the myocardium compared withmagnitude-only inversion recovery, and they recom-mended that this technique be universally used in theevaluation of cardiac amyloidosis. T1 mapping alonehas also been evaluated as a prognostic indicator incardiac amyloidosis. In a study by the same group(and probably using some of the same patients), meanextracellular volume in patients with amyloidosis was44% compared with 25% in healthy volunteers (31).Extracellular volume >45% carried a hazard ratio fordeath of 3.84 and a pre-contrast T1 of >1,044 ms had ahazard ratio of 5.39 for mortality. The prognosticsignificance of these CMR values remained, evenwhen more traditional negative prognostic factors(e.g., elevated N-terminal pro–B-type natriureticpeptide [NT-proBNP] and grade of diastolic dysfunc-tion) were evaluated in multivariate analysis.
An attempt was made to determine whether or notCMR could differentiate AL and TTR amyloidosis (33).In a group of 97 patients, which consisted of 46 pa-tients with AL amyloidosis and 51 patients with ATTR,

FIGURE 10 Multimodality Imaging for Determining Presence and Type of
Cardiac Amyloidosis
(Top left) A planar whole body image of a patient with TTR amyloidosis, showing marked
uptake of 99mtechnetium pyrophosphate (Tc99mPYP) in the heart. Top right, in comparison,
the patient with AL amyloidosis (top right) shows no cardiac isotope uptake, despite a
severe amyloid cardiomyopathy. (Bottom color panel) Single-photon emission computed
tomography Tc99mPYP imaging in TTR (left) and AL amyloidosis (right) confirming intense
uptake in TTR and none in AL amyloidosis. Other abbreviations as in Figure 1.
Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1334
LV mass was much higher in the ATTR group (228 g)compared with the AL group (167 g). LGE was moreextensive in the ATTR group, with 90% demon-strating transmural LGE, compared with 37% of ALpatients. Intriguingly, despite these findings, survivalwas significantly better in cardiac ATTR patients.Although it was concluded that the transmural
pattern of LGE helped to distinguish ATTR from ALamyloidosis, the overlap was considerable, and thistechnique should not be used to determine what typeof cardiac amyloidosis is being imaged.
Evaluation of extracellular volume as a percentageof total LV volume has provided an interesting insightinto the response of the myocardium to amyloiddeposition. It has long been recognized that ALamyloidosis involving the heart has a worse prognosisthan ATTR, despite a smaller increase in LV mass (9).Fontana et al. (34) compared 92 patients with ALamyloidosis with 242 patients with ATTRm and 66patients with ATTRwt using CMR. As anticipated, LVmass was much higher in the ATTR group, but thisgroup also had an 18% increase in the intracellularspace compared with both AL amyloidosis patientsand normal control subjects (34). These data suggestthat there is a true hypertrophic response of themyocardium to infiltration with amyloid derived fromTTR fibrils, which is not seen with AL amyloidosis.Intriguingly, and contrary to expectation, the intra-cellular volume in AL amyloidosis (a marker of car-diomyocyte volume) did not differ from controlsubjects, which implied that the low voltage seenwith AL amyloidosis cannot represent loss of car-diomyocytes, but must be attributed to some othermechanism (e.g., myocyte dysfunction).
In the 1980s, there was interest in using99mtechnetium pyrophosphate (99mTcPYP) as amarker for cardiac amyloidosis, because it was foundthat this isotope was taken up in the heart of somepatients with cardiac amyloid infiltration (35). How-ever, this fell into disuse after the sensitivity of thetest was deemed to be low (36). Within the last fewyears, it has become apparent that 99mTcPYP and DPDare avidly taken up by hearts infiltrated by TTR am-yloid, whereas patients with AL amyloidosis have no,or minimal, myocardial uptake (37) (Figure 10).Particularly when single-photon emission computedtomography analysis is used, a diffuse and intensemyocardial uptake (equal to or greater than rib up-take) is extremely sensitive and highly specific forTTR cardiac amyloidosis, to the degree that a stronglypositive DPD or PYP scan in a patient with echocar-diographic or CMR imaging suggests an infiltrativecardiomyopathy. The absence of a plasma celldyscrasia has been deemed acceptable as specificenough for the diagnosis of TTR amyloidosis to avoida cardiac biopsy (38). Although 99mTcPYP scanning forAL amyloidosis of the heart is of no value in isolation(because it is usually negative), the finding of a highlysuggestive echocardiogram or typical CMR appear-ance of amyloidosis with a strongly positive 99mTcPYPor DPD scan points away from AL amyloidosis and

J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1335
strongly suggests ATTR. This may be of additionalhelp in the >20% of patients with ATTR who have anunrelated monoclonal gammopathy of unknown sig-nificance (MGUS), because the presence of MGUS insuch patients may lead clinicians to incorrectly as-sume that they are dealing with AL amyloidosis (39).
As noted previously, circulating free light chainsappear to have an effect on vascular reactivity,impairing vasodilation. Patients with AL amyloidosishave, on occasion, typical angina, but normalepicardial coronary arteries on coronary angiography;this suggests small vessel dysfunction. Using positronemission tomography scanning in conjunction withvasodilator stress, severe impairment in coronaryartery flow was demonstrated in a group of patientswith AL amyloidosis (15). In some patients, treatmentof the amyloidosis resulted in an improvement incoronary flow, concomitant with the decrease and/orresolution of angina, which suggests that circulatingfree light chains might play a major role in angina inthis subgroup of patients. In centers that are able toaccurately perform this technique, it is useful indetermining the presence or absence of impairedsmall cardiac vessel function.
LABORATORY TESTING
Standard laboratory tests in the amyloidoses aregenerally unrevealing; however, there may be certainabnormalities that give a clue to the diagnosis. Ifnephrotic syndrome is present, hypoalbuminemiawill be seen, and hypercholesterolemia may be pro-found. Any sudden elevation of serum cholesterol ina patient should prompt a search for hypothyroidismor proteinuria; if the latter is found, and heart failureis present, the likelihood of a systemic disease is high.Amyloidosis with heart failure is high on that list.NT-proBNP is elevated in any cause of heart failure,but it may be disproportionally high in cardiacamyloidosis due to the cellular release caused bydirect myocyte compression, in addition to high car-diac filling pressure.
Troponin levels are frequently chronically elevatedat a low level, and failure to recognize the absence ofthe typical rise and fall of troponin occurring withacute myocardial damage may lead to a misdiagnosisof myocardial infarction. Amyloid deposits in ALamyloidosis are due to the misfolding of a part of adysfunctional immunoglobulin, and this is reflectedin plasma protein levels. In AL amyloidosis, severalimmunoglobulin subclasses are often suppressed.Unlike multiple myeloma, in which there is usually alarge amount of circulating paraprotein that causesan abnormal band on serum or urine protein
electrophoresis, these tests are normal in as many asone- half of patients with AL amyloidosis, because theparaprotein level is often low. Immunofixation ofthe serum and urine is a much more sensitive testand usually demonstrates a monoclonal band. Thus,immunofixation and serum-free light chains shouldalways be measured when amyloidosis is suspected.An abnormal free light chain kappa/lambda ratio isfound in >90% of patients with untreated ALamyloidosis. A normal ratio makes the diagnosis lesslikely, but it does not rule it out and certainly doesnot exclude other forms of non-AL amyloidosis, inwhich the precursor protein is unrelated to a plasmacell dyscrasia. All patients with suspected ALamyloidosis should have an initial bone marrow bi-opsy to determine the percentage of plasma cells andto rule out both concomitant multiple myelomaand less common hematologic conditions that maycause amyloid deposition (e.g., Waldenström macro-globulinemia and lymphomas). Biomarkers values ofNT-proBNP, troponin T, and free light chains wereshown to be useful in determining prognosis amongnewly diagnosed patients with AL amyloidosis,and the Mayo Clinic developed a staging systemincorporating all 3 of these biomarkers (40). However,this system is based upon survival after treatmentwith older therapeutic regimens and may not berelevant for patients treated with bortezomib-containing combination therapies, because survivalappears to be longer than in patients treated witholder therapies (41).
TISSUE BIOPSY
Although the combination of a plasma cell dyscrasiawith an abnormal free light chain ratio and a typicalechocardiographic appearance, with or without CMRimaging, is highly suggestive of AL cardiac amyloid-osis, almost 1 in 4 patients with ATTR have associatedMGUS (39), some of whom have an abnormal freelight chain ratio (42). Thus, the sine qua non ofdefinitive diagnosis in patients with evidence of amonoclonal gammopathy who are suspected of hav-ing cardiac AL amyloidosis remains a tissue biopsyshowing amyloid deposits, whether of abdominal fat,another involved organ, or the heart. At our institu-tion, we tend to favor endomyocardial biopsy becauseit allows for cardiac hemodynamic measurement atthe same time of the biopsy, which can be helpful inmanagement. However, cardiac biopsy has a smallrate of serious complications and should only beperformed in centers that do this procedure regularly.Abdominal fat pad biopsy by needle aspirationhas approximately a 70% to 80% sensitivity for

CENTRAL ILLUSTRATION Diagnosing and Typing Cardiac Amyloidosis in a Patient With Unexplained Heart Failure
Echocardiogram or MRI suggestive of cardiac amyloidosis
Clinical and laboratory evaluation including:
Is plasma-cell dyscrasia present?*
Myocardial uptake of 99mTcPYP/DPD assessment Bone marrow biopsy +/- cardiac or non-cardiac biopsy
Cardiacamyloidosisis unlikely.
IMPORTANTLY, proceed with
endomyocardial biopsy if clinical
suspicion of amyloidosisis still high.
ATTRwt(non-hereditary
form causedby wild-type
TTR)
ATTRm(hereditary
form causedby a genetic mutation of
TTR)
Light -chain(AL)
amyloidosis
None or traceImmunohistochemistry
strongly positive forlight chains and negative
for transthyretin in amyloid deposits
Immunohistochemistry shows ambiguous results
Mass spectrometry
in amyloid deposits
Is there a transthyretin protein (TTR) mutation
present?
Strongly positive
N
N
Y
Y
Falk, R.H. et al. J Am Coll Cardiol. 2016;68(12):1323–41.
*The finding of evidence of a plasma cell dyscrasia does not necessarily confirm light-chain (AL) amyloidosis because monoclonal gammopathy of unknown significance
(MGUS) might coexist with transthyretin (TTR) amyloidosis. Thus, if the clinical picture suggests TTR amyloidosis (e.g., isolated cardiac amyloidosis in an elderly man
with a history of carpal tunnel syndrome and no proteinuria or neuropathy), further workup is required to exclude transthyretin amyloidosis (ATTR). A classical
appearance on imaging for amyloidosis, with a strong 99mtechnetium pyrophosphate (Tc99mPYP) (or 2,3-dicarboxypropane-1, 1-diphosphonate [DPD] in Europe) cardiac
uptake, and no evidence of a plasma cell dyscrasia appears to be diagnostic of TTR amyloidosis, without the need for a biopsy (42). ATTRm ¼ mutant transthyretin
amyloidosis; ATTRwt ¼wild-type transthyretin amyloidosis; MRI ¼magnetic resonance imaging; NT-proBNP¼ N-terminal pro–B-type natriuretic peptide; SPEP ¼ serum
protein electrophoresis.
Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1336
identifying amyloid deposition, but these figurescome from centers skilled in appropriate staining ofthe small amount of tissue often obtained by thistechnique. Both false negatives and false positives(from overstaining) may occur in less experiencedcenters (43–45).
Appropriate staining of the biopsy to determineboth the presence and the type of amyloidosis is
critical. Congo red will stain the amyloid pink, withapple-green birefringence when viewed with polar-ized microscopy, but several centers, including ourown, prefer sulfated Alcian Blue as an amyloid stainin cardiac biopsies (46,47). Standard immunohisto-chemistry and immunofluorescence, even in the mostexperienced hands, may give misleading results, andif the clinical picture is not consistent with the biopsy

J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1337
chemistry, further investigation should be per-formed. Currently, the gold standard is proteomicevaluation of amyloid deposits by mass spectrometry.This technique determines the precise components ofthe amyloid deposits, which allows for a highly sen-sitive and specific result. It is limited to a few centers,but specimens can be sent there for evaluation, evenif already fixed in a paraffin block. Using this tech-nique, it has become apparent that immunochemicalstaining of tissue amyloid deposits is often an inac-curate technique (48,49). A flowchart in the CentralIllustration shows an approach to diagnosing cardiacamyloidosis.THERAPY. Therapy of AL cardiac amyloidosis is2-fold: 1) optimal treatment of heart failure, and2) chemotherapy aimed at abolishing the amyloido-genic plasma cell dyscrasia. Diuretic agents arethe mainstay of heart failure therapy becauseangiotensin-converting enzyme inhibitors andangiotensin-receptor blockers are poorly tolerateddue to hypotension. We tend to favor a combinationof a loop diuretic agent, usually torsemide, withspironolactone. Beta-blockers may also aggravatehypotension and are usually avoided (they maybe used cautiously in selected patients with atrialfibrillation and a rapid ventricular response).Although severe diastolic dysfunction is often pre-sent, there is no role for calcium-channel blockers,and these drugs often significantly worsen congestiveheart failure. Digoxin appears to offer no benefit inheart failure due to amyloid cardiomyopathy, anddigoxin toxicity with “therapeutic digoxin levels”may occur because of altered binding properties (50).
Amyloid infiltration of the atrium results in atrialarrhythmias in some patients, and there appears to bea higher incidence of atrial tachycardia and flutter inrelation to the incidence of atrial fibrillationcompared with many other heart diseases. Despitethe poorly functioning atrium in amyloidosis, theonset of atrial arrhythmias is often associated withworsening of congestive heart failure, possiblybecause of an irregular or excessively fast rhythm.Attempts at catheter ablation of these arrhythmiasmay be difficult due to the multifocal nature, and therecurrence rate is high (51). If antiarrhythmic agentsare used, those with a negative inotropic or chrono-tropic effect should be avoided. We have found thatamiodarone is generally quite effective and well-tolerated, and we have also used dofetilide rela-tively frequently with good long-term maintenance ofsinus rhythm. Anticoagulation, either with warfarinor with the oral nonvitamin K antagonist anticoagu-lants can usually be safely administered to patientswith AL amyloidosis and should be given for any
atrial arrhythmia. Furthermore, even if the patient isin sinus rhythm, anticoagulation should be used if theechocardiogram shows features of left atrial me-chanical dysfunction, because thrombus formationand thromboembolism may occur in these patients.
Nonsustained ventricular arrhythmias are uncom-mon in AL amyloidosis, and sudden death, if it oc-curs, is most commonly due to sudden profoundbradycardia or pulseless electrical activity (52). Itusually occurs in patients with severe amyloid car-diomyopathy. There is no proven benefit of eitherprophylactic pacing or prophylactic implantabledefibrillator use in these patients, and although smallseries report occasional successful defibrillation,there is little evidence that long-term survival isaffected (53,54). Postural hypotension in ALamyloidosis may be due to over-diuresis, but is mostcommonly related to some degree of autonomicneuropathy. It may be exposed by diuresis and can betreated, on occasion, with midodrine. Midodrine-induced supine hypertension, a complication ofcertain autonomic neuropathies, is not seen ALamyloidosis, and thus high doses of the drug can beused. An occasional patient may complain of exer-tional lightheadedness and yet have normalsupine and standing blood pressures. This can bedue to a fixed cardiac output, but it may also bedue to autonomic neuropathy-associated exertionalhypotension. This may be revealed by careful tread-mill testing and often responds to pre-exercisemidodrine.
Chemotherapy that targets the underlying plasmacell dyscrasia has changed considerably in the pastdecade, with markedly improved response rates andprolonged survival. It is of critical importance toinvolve cardiologists with experience in the diseaseduring the chemotherapy treatment, and they shouldbe willing to see patients at frequent intervalsthroughout chemotherapy to adjust concomitantmedications. It is beyond the scope of this paper toaddress details of specific chemotherapeutic regi-mens, but the interested reader is directed to anexcellent recent review of this topic (55). Initialattempts at treating AL amyloidosis with oralmelphalan and prednisone showed a modest survivalbenefit among patients without cardiac involvement,but showed no benefit in AL cardiac amyloidosis (56).High-dose melphalan chemotherapy with autologousstem cell transplantation had a significant positiveimpact on the percentage of patients who achieved acomplete hematologic remission, and this wasaccompanied by an improvement in survivalcompared with those who did not achieve remission.However, this is an aggressive therapy, and patients

Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1338
with severe cardiac involvement have a hightreatment-related mortality, even among carefullyselected subjects. It is now less commonly usedas an initial therapy (57). With the institution ofproteosome-inhibiting agents, specifically bortezo-mib, the prognosis of patients with light chain cardiacamyloidosis has considerably improved. Bortezomibis relatively well-tolerated, even in the presence ofamyloid cardiomyopathy, and is usually combinedwith dexamethasone and frequently with low-dosecyclophosphamide (58,59). For example, in patientswithout cardiac involvement, 40 mg of dexametha-sone is usually administered weekly, but this dosemay often worsen heart failure in cardiac amyloid-osis. In such patients, it is prudent to start with 10 mgweekly, increasing every week or 2 to the maximumtolerated dose, while adjusting diuretic agentsaccordingly. Concern has been raised about bortezo-mib cardiotoxicity (60), but this appears to be rare(61), and the drug is generally well-tolerated inpatients with cardiac amyloidosis. When lenalido-mide, an immunomodulatory agent, is used in ther-apy, a paradoxical elevation in B-type natriureticpeptide or NT-proBNP may be seen, despite evidenceof hematologic improvement; the mechanism for thisis unknown (62,63). High-dose chemotherapy withautologous stem cell transplantation is generallyreserved for suitable cardiac amyloidosis patients inwhom oral regimens have failed, and may produce acomplete hematologic response. Cardiology input isimportant because stem cell collection is often asso-ciated with fluid retention and hypotension, andatrial arrhythmias may occur following chemo-therapy. Generally, hypotension is well-tolerated,and the temptation to treat with intravenous fluidsshould be avoided in the asymptomatic patient.
CARDIAC TRANSPLANTATION
Cardiac transplantation in AL amyloidosis has beenperformed, but the outcome depends upon extremelycareful selection of patients. A commitment to pursuechemotherapy following transplantation for patientswith active hematologic disease is essential, becausesystemic disease will otherwise progress, and amy-loid infiltration of the transplanted heart can occur.Most patients who have undergone successfulchemotherapy for AL amyloid (defined as normaliza-tion of their free light chain ratio) have a clinicalimprovement in heart failure, and rarely need post-chemotherapy cardiac transplantation. The patientsin whom cardiac transplantation should be consid-ered are those with severe cardiac amyloidosis that islimited to the heart, and in whom systemic
chemotherapy is deemed to be too toxic to be toler-ated because of their heart disease. These patientshave high mortality, and in 1 single-center series,11 of 31 patients died while awaiting cardiac trans-plantation. Successful orthotopic heart trans-plantation occurred in 18 patients, with 1 post-operative death. Fourteen patients subsequentlyunderwent high-dose chemotherapy with autologousstem cell transplantation, with 3 subsequent deaths.Although the investigators reported no difference insurvival between these patients and age-matchedcontrol subjects in the Scientific Registry of Trans-plant Recipients database, the numbers were verysmall and the death rate on the waiting list was veryhigh, making precise comparisons difficult.
Data from the Mayo Clinic shed light on theimportance of obtaining a complete hematologicresponse to high-dose chemotherapy and autologousstem cell transplantation after heart transplantation,as well as on the rarity of the need and/or patientsuitability for cardiac transplantation. Among >3,000patients with AL amyloidosis seen over a 20-yearperiod, 23 patients underwent heart transplantation.Median survival for those able to complete autolo-gous stem cell transplantation was 6.3 years, and inthe subgroup of 7 patients who achieved a completeremission, median survival was 10.8 years. Becauseone of the main reasons for heart transplantation inthe time period studied was severity of disease pre-cluding high-dose chemotherapy with autologousstem cell transplantation (at that time the mosteffective therapy for the plasma cell dyscrasia), it ispossible that some of these patients might havebeen treatable today with a bortezomib-containingregimen. This might argue for early heart trans-plantation evaluation in suitable, severely ill patientswith AL cardiac amyloidosis, while also initiatingchemotherapy and reassessing patients accepted on await list for ongoing transplantation need. Thisapproach has been adopted by some centers (M.Semigran, personal communication, March 2016).
Patients with a small LV cavity, such as is seen inamyloidosis, are not deemed good candidates for aLV assist device, and right ventricular function is alsooften severely impaired in amyloidosis. In a report ofoutcomes of LV assist device implantation at theMayo Clinic for patients with restrictive cardiomy-opathy, 10 of 28 patients had amyloid cardiomyopa-thy, 2 of whom died before hospital discharge. Only 1patient had AL amyloidosis, but this patient achievedhematologic remission before device implantation.One-year overall survival was 64% after LV assistdevice implantation, with no difference betweenamyloidosis and non-amyloidosis patients, but with

J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1339
poor survival if the LV end-diastolic dimensionwas <46 mm.
In addition to chemotherapy to abolish the amy-loidogenic light chains, several novel adjunctivetherapies have been proposed or are in clinical trials.In vitro evidence suggests that doxycycline mayprevent the formation of fibrils from light chains anddisrupt fibrils that have already formed, and there isan ongoing trial of doxycycline in conjunction withstandard chemotherapy.
Antibody therapy has been developed to specif-ically target misfolded light chain aggregates. Aradiolabeled antibody specifically localized withhuman AL amyloid extracts was implanted in mice,and treatment with this antibody expedited regres-sion of AL kappa amyloidomas in these animals(64). Preliminary data from a phase 1/2 study in 27patients with AL amyloidosis treated with thisantibody showed a decrease in NT-proBNPfollowing antibody therapy in some AL amyloid-osis patients with cardiac involvement, but it isunclear whether this represented ongoing cardiacimprovement related to previous chemotherapyor an effect of the drug. A phase 3 randomizedmulticenter study is currently ongoing, withpatients randomized to chemotherapy alone orchemotherapy plus antibody.
All amyloid deposits contain an SAP component, anormal, nonfibrillar plasma glycoprotein that isbelieved to render amyloid fibrils resistant todegradation. In an attempt to rid fibrils of SAP, asmall molecule was developed, (R)-1-[6-[(R)-2-carboxy-pyrrolidin-1-yl]-6-oxo-hexanoyl]pyrrolidine-2-carboxylic acid (CPHPC), but initial experiments inhumans revealed that the amount of circulating SAPwas too great, and although this drug depletedcirculating SAP (65), it had little effect on amyloid
deposits. This led to the concept of a 2-prongedapproach: depletion of circulating SAP with CPHPC,followed by the administration of a fully humanizedimmunoglobulin-1 anti-SAP monoclonal antibody totarget the SAP on the amyloid fibrils, in the hope thatnormal phagocytic processes would resorb the SAP-depleted fibrils. Using this approach, 16 patientswith amyloidosis, including 8 with AL amyloidosis,were studied. There was a significant reduction inamyloid burden noted in most patients over a 6-weekperiod (66). Of note, none of the 16 patients had car-diac amyloidosis by trial design, but a trial of thispromising therapy in patients with AL and ATTRcardiac amyloid is planned to start before the endof 2016.
SUMMARY
The past decade has seen major advances in diagnosisand therapy of all forms of amyloidosis, particularlyin AL amyloidosis. Modern diagnostic techniques,such as CMR and advanced echocardiography, in-crease the likelihood of diagnosing the disease, butthere is still no substitute for physician awareness ofthis condition, without which delayed diagnosis isinevitable. Early diagnosis is critical for the bestoutcome of therapy, and it is hoped that this reviewhas given the reader insight into the importance ofearly diagnosis and of precise amyloid typing, alongwith a recognition that a previously hopeless diseasehas now rapidly become a treatable and possiblycurable condition.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Rodney H. Falk, Division of Cardiology Brigham andWomen’s Hospital, 75 Francis Street, Boston, Massa-chusetts 02115. E-mail: [email protected].
RE F E RENCE S
1. Brahmanandam V, McGraw S, Mirza O, et al.Regression of cardiac amyloidosis after stem celltransplantation assessed by cardiovascular magneticresonance imaging. Circulation 2014;129:2326–8.
2. Hawkins PN. Serum amyloid P componentscintigraphy for diagnosis and monitoringamyloidosis. Curr Opin Nephrol Hypertens 2002;11:649–55.
3. Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis,prognosis, and therapy of transthyretin amyloid-osis. J Am Coll Cardiol 2015;66:2451–66.
4. Palumbo A, Anderson K. Multiple myeloma.N Engl J Med 2011;364:1046–60.
5. Hasserjian RP, Goodman HJ, Lachmann HJ,et al. Bone marrow findings correlate with clinical
outcome in systemic AL amyloidosis patients.Histopathology 2007;50:567–73.
6. Kyle RA, Linos A, Beard CM, et al. Incidence andnatural history of primary systemic amyloidosis inOlmsted County, Minnesota, 1950 through 1989.Blood 1992;79:1817–22.
7. Comenzo RL. Out, out–making amyloid’s candlebriefer. N Engl J Med 2015;373:1167–9.
8. Larsen BT, Mereuta OM, Dasari S, et al. Corre-lation of histomorphological pattern of cardiacamyloid deposition with amyloid type: a histo-logical and proteomic analysis of 108 cases. His-topathology 2016;68:648–56.
9. Dubrey SW, Cha K, Skinner M, et al. Familialand primary (AL) cardiac amyloidosis:
echocardiographically similar diseases withdistinctly different clinical outcomes. Heart 1997;78:74–82.
10. Dubrey S, Mendes L, Skinner M, et al. Reso-lution of heart failure in patients with ALamyloidosis. Ann Intern Med 1996;125:481–4.
11. Liao R, Jain M, Teller P, et al. Infusion of lightchains from patients with cardiac amyloidosiscauses diastolic dysfunction in isolated mousehearts. Circulation 2001;104:1594–7.
12. Brenner DA, Jain M, Pimentel DR, et al. Humanamyloidogenic light chains directly impair car-diomyocyte function through an increase incellular oxidant stress. Circ Res 2004;94:1008–10.

Falk et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
AL Amyloidosis and the Heart S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1
1340
13. Mishra S, Guan J, Plovie E, et al. Human amy-loidogenic light chain proteins result in cardiacdysfunction, cell death, and early mortality inzebrafish. Am J Physiol Heart Circ Physiol 2013;305:H95–103.
14. Migrino RQ, Truran S, Gutterman DD, et al.Human microvascular dysfunction and apoptoticinjury induced by AL amyloidosis light chain pro-teins. Am J Physiol Heart Circ Physiol 2011;301:H2305–12.
15. Dorbala S, Vangala D, Bruyere J Jr., et al.Coronary microvascular dysfunction is related toabnormalities in myocardial structure and functionin cardiac amyloidosis. J Am Coll Cardiol HF 2014;2:358–67.
16. McWilliams-Koeppen HP, Foster JS,Hackenbrack N, et al. Light chain amyloid fibrilscause metabolic dysfunction in human car-diomyocytes. PLoS One 2015;10:e0137716.
17. Ward JE, Ren R, Toraldo G, et al. Doxycyclinereduces fibril formation in a transgenic mousemodel of AL amyloidosis. Blood 2011;118:6610–7.
18. Cardoso I, Martins D, Ribeiro T, et al. Synergyof combined doxycycline/TUDCA treatment inlowering transthyretin deposition and associatedbiomarkers: studies in FAP mouse models. J TranslMed 2010;8:74.
19. Obici L, Cortese A, Lozza A, et al. Doxycyclineplus tauroursodeoxycholic acid for transthyretinamyloidosis: a phase II study. Amyloid 2012;19Suppl 1:34–6.
20. Chamarthi B, Dubrey SW, Cha K, et al. Featuresand prognosis of exertional syncope in light-chainassociated AL cardiac amyloidosis. Am J Cardiol1997;80:1242–5.
21. Ing EB, Woolf IZ, Younge BR, et al. Systemicamyloidosis with temporal artery involvementmimicking temporal arteritis. Ophthalmic SurgLasers 1997;28:328–31.
22. Mussinelli R, Salinaro F, Alogna A, et al.Diagnostic and prognostic value of low QRS volt-ages in cardiac AL amyloidosis. Ann NoninvasiveElectrocardiol 2013;18:271–80.
23. Rapezzi C, Merlini G, Quarta CC, et al. Systemiccardiac amyloidoses: disease profiles and clinicalcourses of the 3 main types. Circulation 2009;120:1203–12.
24. Carroll JD, Gaasch WH, McAdam KP. Amyloidcardiomyopathy: characterization by a distinctivevoltage/mass relation. Am J Cardiol 1982;49:9–13.
25. Phelan D, Collier P, Thavendiranathan P, et al.Relative apical sparing of longitudinal strain usingtwo-dimensional speckle-tracking echocardiogra-phy is both sensitive and specific for the diagnosisof cardiac amyloidosis. Heart 2012;98:1442–8.
26. Philippakis AA, Falk RH. Cardiac amyloidosismimicking hypertrophic cardiomyopathy withobstruction: treatment with disopyramide. Circu-lation 2012;125:1821–4.
27. Lee GY, Kim K, Choi JO, et al. Cardiacamyloidosis without increased left ventricular wallthickness. Mayo Clin Proc 2014;89:781–9.
28. Longhi S, Lorenzini M, Gagliardi C, et al.Coexistence of degenerative aortic stenosis andwild-type transthyretin-related cardiac amyloid-osis. J Am Coll Cardiol Img 2016;9:325–7.
29. Fontana M, Chung R, Hawkins PN, et al. Car-diovascular magnetic resonance for amyloidosis.Heart Fail Rev 2015;20:133–44.
30. Kwong RY, Heydari B, Abbasi S, et al. Char-acterization of cardiac amyloidosis by atrial lategadolinium enhancement using contrast-enhancedcardiac magnetic resonance imaging and correla-tion with left atrial conduit and contractile func-tion. Am J Cardiol 2015;116:622–9.
31. Banypersad SM, Fontana M, Maestrini V, et al.T1 mapping and survival in systemic light-chainamyloidosis. Eur Heart J 2015;36:244–51.
32. Fontana M, Pica S, Reant P, et al. Prognosticvalue of late gadolinium enhancement cardiovas-cular magnetic resonance in cardiac amyloidosis.Circulation 2015;132:1570–9.
33. Dungu JN, Valencia O, Pinney JH, et al. CMR-based differentiation of AL and ATTR cardiacamyloidosis. J Am Coll Cardiol Img 2014;7:133–42.
34. Fontana M, Banypersad SM, Treibel TA, et al.Differential myocyte responses in patients withcardiac transthyretin amyloidosis and light-chainamyloidosis: a cardiac MR imaging study. Radi-ology 2015;277:388–97.
35. Falk RH, Lee VW, Rubinow A, et al. Sensitivityof technetium-99m-pyrophosphate scintigraphyin diagnosing cardiac amyloidosis. Am J Cardiol1983;51:826–30.
36. Gertz MA, Brown ML, Hauser MF, et al. Utilityof technetium Tc 99m pyrophosphate bone scan-ning in cardiac amyloidosis. Arch Intern Med 1987;147:1039–44.
37. Rapezzi C, Quarta CC, Guidalotti PL, et al.Usefulness and limitations of 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintig-raphy in the aetiological diagnosis of amyloidoticcardiomyopathy. Eur J Nucl MedMol Imaging 2011;38:470–8.
38. Gillmore JD, Maurer MS, Falk RH, et al.Non-biopsy diagnosis of cardiac transthyretinamyloidosis. Circulation 2016;133:2404–12.
39. Pinney JH, Whelan CJ, Petrie A, et al. Senilesystemic amyloidosis: clinical features at presen-tation and outcome. J Am Heart Assoc 2013;2:e000098.
40. Kumar S, Dispenzieri A, Lacy MQ, et al.Revised prognostic staging system for light chainamyloidosis incorporating cardiac biomarkers andserum free light chain measurements. J Clin Oncol2012;30:989–95.
41. Sperry BW, Ikram A, Hachamovitch R, et al.Efficacy of chemotherapy for light-chainamyloidosis in patients presenting with symp-tomatic heart failure. J Am Coll Cardiol 2016;67:2941–8.
42. Maleszewski JJ, Murray DL, Dispenzieri A,et al. Relationship between monoclonal gamm-opathy and cardiac amyloid type. CardiovascPathol 2013;22:189–94.
43. Vrana JA, Theis JD, Dasari S, et al. Clinicaldiagnosis and typing of systemic amyloidosis insubcutaneous fat aspirates by mass spectrometry-based proteomics. Haematologica 2014;99:1239–47.
44. Gertz MA, Li CY, Shirahama T, et al. Utility ofsubcutaneous fat aspiration for the diagnosis of
systemic amyloidosis (immunoglobulin lightchain). Arch Intern Med 1988;148:929–33.
45. Libbey CA, Skinner M, Cohen AS. Use ofabdominal fat tissue aspirate in the diagnosis ofsystemic amyloidosis. Arch Intern Med 1983;143:1549–52.
46. Maleszewski JJ. Cardiac amyloidosis: pathol-ogy, nomenclature, and typing. Cardiovasc Pathol2015;24:343–50.
47. Pomerance A, Slavin G, McWatt J. Experiencewith the sodium sulphate-Alcian Blue stain foramyloid in cardiac pathology. J Clin Pathol 1976;29:22–6.
48. Sethi S, Vrana JA, Theis JD, et al. Lasermicrodissection and mass spectrometry-basedproteomics aids the diagnosis and typing of renalamyloidosis. Kidney Int 2012;82:226–34.
49. Theis JD, Dasari S, Vrana JA, et al. Shotgun-proteomics-based clinical testing for diagnosis andclassification of amyloidosis. J Mass Spectrom2013;48:1067–77.
50. Rubinow A, Skinner M, Cohen AS. Digoxinsensitivity in amyloid cardiomyopathy. Circulation1981;63:1285–8.
51. Barbhaiya CR, Kumar S, Baldinger SH, et al.Electrophysiologic assessment of conduction ab-normalities and atrial arrhythmias associated withamyloid cardiomyopathy. Heart Rhythm 2016;13:383–90.
52. Sayed RH, Rogers D, Khan F, et al. A study ofimplanted cardiac rhythm recorders in advancedcardiac AL amyloidosis. Eur Heart J 2015;36:1098–105.
53. Kristen AV, Dengler TJ, Hegenbart U, et al.Prophylactic implantation of cardioverter-defibrillator in patients with severe cardiacamyloidosis and high risk for sudden cardiacdeath. Heart Rhythm 2008;5:235–40.
54. Varr BC, Zarafshar S, Coakley T, et al.Implantable cardioverter-defibrillator placementin patients with cardiac amyloidosis. Heart Rhythm2014;11:158–62.
55. Kastritis E, Dimopoulos MA. Recent advancesin the management of AL amyloidosis. Br JHaematol 2016;172:170–86.
56. Skinner M, Anderson J, Simms R, et al. Treat-ment of 100 patients with primary amyloidosis: arandomized trial of melphalan, prednisone, andcolchicine versus colchicine only. Am J Med 1996;100:290–8.
57. Merlini G, Palladini G. Amyloidosis: is a curepossible? Ann Oncol 2008;19 Suppl 4:iv63–6.
58. Jimenez-Zepeda VH, Duggan P, Neri P, et al.Bortezomib-containing regimens for the treatmentof newly diagnosed and relapsed amyloid lightchain amyloidosis: a single-center experience. ClinLymphoma Myeloma Leuk 2016;16:e79–84.
59. Palladini G, Sachchithanantham S, Milani P,et al. A European collaborative study of cyclo-phosphamide, bortezomib, and dexamethasone inupfront treatment of systemic AL amyloidosis.Blood 2015;126:612–5.
60. Enrico O, Gabriele B, Nadia C, et al. Unex-pected cardiotoxicity in haematological

J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Falk et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 3 2 3 – 4 1 AL Amyloidosis and the Heart
1341
bortezomib treated patients. Br J Haematol 2007;138:396–7.
61. Xiao Y, Yin J, Wei J, et al. Incidence andrisk of cardiotoxicity associated with bortezo-mib in the treatment of cancer: a systematicreview and meta-analysis. PLoS One 2014;9:e87671.
62. Dispenzieri A, Dingli D, Kumar SK, et al.Discordance between serum cardiac biomarker andimmunoglobulin-free light-chain response inpatients with immunoglobulin light-chain amy-loidosis treated with immune modulatory drugs.Am J Hematol 2010;85:757–9.
63. Tapan U, Seldin DC, Finn KT, et al. Increases inB-type natriuretic peptide (BNP) during treatmentwith lenalidomide in AL amyloidosis. Blood 2010;116:5071–2.
64. Wall JS, Kennel SJ, Williams A, et al. AL am-yloid imaging and therapy with a monoclonalantibody to a cryptic epitope on amyloid fibrils.PLoS One 2012;7:e52686.
65. Gillmore JD, Tennent GA, Hutchinson WL,et al. Sustained pharmacological depletion ofserum amyloid P component in patients with sys-temic amyloidosis. Br J Haematol 2010;148:760–7.
66. Richards DB, Cookson LM, Berges AC, et al.Therapeutic clearance of amyloid by antibodies toserum amyloid P component. N Engl J Med 2015;373:1106–14.
KEY WORDS cardiomyopathy, multiplemyeloma, TTR amyloidosis
Go to http://www.acc.org/jacc-journals-cme to take the CMEquiz for this article.