Embed Size (px)
Citation preview
Exercise EchocardiographyExercise EchocardiographyCardiac Issues 2011Cardiac Issues 2011
Douglass A Morrison, MD, PhDDouglass A Morrison, MD, PhD
Exercise EchocardiographyExercise EchocardiographyTopicsTopics
• Indications
• Assessing Prognosis with exercise echo
• Limitations
• Appropriateness
Indications for Indications for Exercise EchocardiographyExercise Echocardiography
• Reserve of Ventricular Function
• Detection of coronary artery disease/ myocardial ischemia
• Risk assessment/ prognosis
• Viability/ suitability for revascularization
• Timing of intervention in valvular heart disease
• Adequacy of therapy
Limitations of Exercise EchocardiographyLimitations of Exercise Echocardiography
• Inability to exercise: orthopedic, neurological, pulmonary or psychological
• Inability to image: acoustic windows; hyperinflation, obesity
• Delay in getting into position for imaging, after completing exercise
• Inability to lie on side and/or breath-hold (briefly)
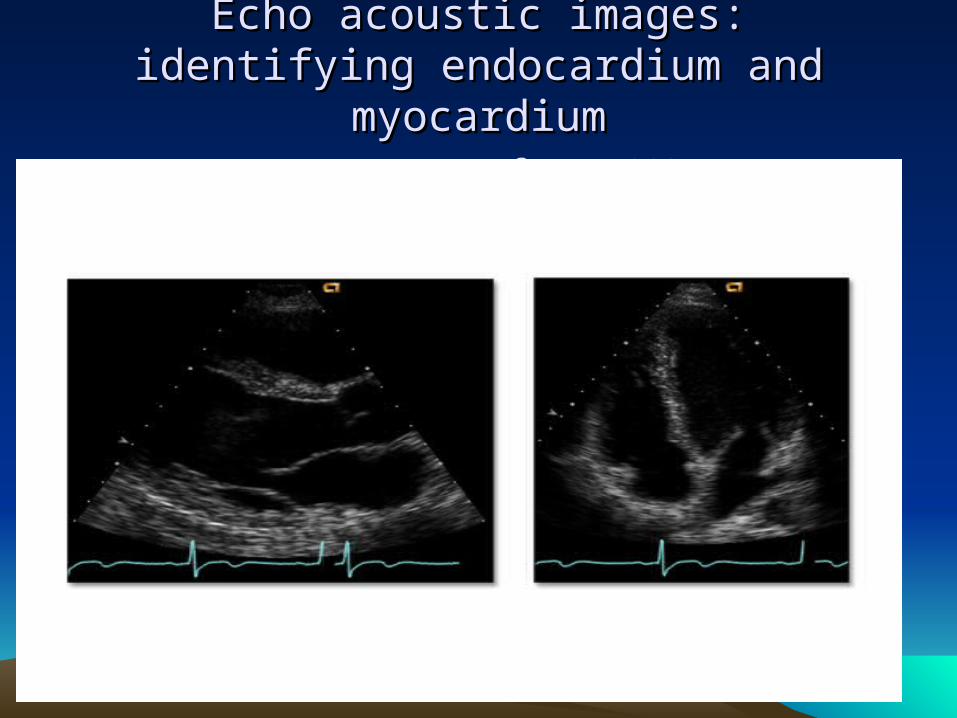
Echo acoustic images:Echo acoustic images:identifying endocardium and myocardiumidentifying endocardium and myocardium
from ACCSAP7from ACCSAP7

Echo contrast to aid in identifying endocardiumEcho contrast to aid in identifying endocardiumACCSAP7ACCSAP7

Sensitivity and SpecificitySensitivity and Specificity
• Disease Present Disease Absent
• Positive test true positive (TP) false positive (FP) PPV• Negative test false negative (FN) true negative (TN) NPV
• Sensitivity = TP/ (TP +FN) Specificity = TN/ (TN +FP)

Sensitivity and Specificity (continued)Sensitivity and Specificity (continued)
• SpPin: for a specific test (few false positives); positive test, rules in
• SnNout: for a sensitive test (few false negatives); negative test, rules out
• Wall motion (echocardiography) is more specific than symptoms or ECG
• Sensitivity is greatly influenced by adequacy of exercise, in terms of both exercise duration/ level, and double product (peak systolic blood pressure x peak exercise heart rate).
• Positive predictive value (PPV) = TP/ (TP = FP)• Negative predictive value (NPV) = TN/ (TN + FN)

Bayesian principleBayesian principleConditional ProbabilityConditional Probability
• All good clinicians use all the diagnostic information they have; test results should be taken ‘in-context’.
• Accuracy of any test depends not only on the test’s sensitivity/ specificity, but also the pre-test probability of disease.– Consider the clinical usefulness of screening
for lung cancer in kindergarten children.

Limitations of Exercise Electrocardiography Limitations of Exercise Electrocardiography (ECG)(ECG)

Detection of Myocardial IschemiaDetection of Myocardial Ischemia
from ACCSAP7from ACCSAP7

Exercise vs. Pharmacological EchoExercise vs. Pharmacological Echoas reported in JACC (2003;42:954-970) and cited by ACCSAP7as reported in JACC (2003;42:954-970) and cited by ACCSAP7

Exercise myocardial perfusion imaging (nuclear) vs. Exercise myocardial perfusion imaging (nuclear) vs. echocardiographyechocardiography
as reported in Eur Heart J(2003;24;789-800) and cited by as reported in Eur Heart J(2003;24;789-800) and cited by ACCSAP7ACCSAP7
““Party Line”Party Line”
• Nuclear stress testing is more sensitive for detecting myocardial ischemia. Echo has more false negatives.
• Exercise echo is more specific for myocardial ischemia than nuclear. Nuclear has more false positives.
Guideline and Appropriateness Concepts regarding Guideline and Appropriateness Concepts regarding work-up of suspected coronary artery disease (CAD)work-up of suspected coronary artery disease (CAD)
• Careful history is most important.
• Further work-up should be guided by clinical likelihood of CAD.
• Exercise ECG is preferred, if patient can exercise and resting-ECG is normal.
• Value of stress testing, to infer CAD, is highest among intermediate probability patients.

Guideline and Appropriateness Concepts regarding Guideline and Appropriateness Concepts regarding work-up of suspected coronary artery disease (CAD) (2)work-up of suspected coronary artery disease (CAD) (2)
• Stress imaging should NOT be used as initial evaluation of low probability patients, because of high likelihood of false positives leading to unnecessary work-up.
• Coronary angiography is recommended for high-risk (of events) patients, regardless of symptom severity.
• However, among patients with known CAD looking for silent ischemia, among asymptomatic patients is eschewed.

Pre-test likelihood of coronary artery disease Pre-test likelihood of coronary artery disease (CAD) (NEJM 1979;300:1350-1358(CAD) (NEJM 1979;300:1350-1358

Assessment of myocardial viabilityAssessment of myocardial viability

Stages of Bruce protocolStages of Bruce protocolfrom ACCSAP7from ACCSAP7

Prognosis/ Risk AssessmentPrognosis/ Risk Assessmentfrom ACCSAP7from ACCSAP7
Prognosis: Duke score of exercise ECGPrognosis: Duke score of exercise ECG
• Duration of exercise on Bruce protocol
• - 5X (ST depression in mm)
• - 4x (angina index; 1 point for any chest pain; 2 points if angina was limiting symptom).
• Low risk >+5 annual mortality 0.25%
• Intermediate -10 to +4 annual mortality 1.25%
• High risk <-10 annual mortality 5.0%
Predicting multi-vessel CAD, from Stress Test Predicting multi-vessel CAD, from Stress Test ResultsResults
• Early positive= Stage I of Bruce or ‘low-level’
• Markedly positive ECG: ST >2 mm depression or ST-elevation
• Prolonged: ST depression >8 minutes into recovery
• Fall in systolic blood pressure, with exercise; especially if accompanied by signs or symptoms

Prognosis: Exercise Duration + 2 mm ST Prognosis: Exercise Duration + 2 mm ST depressiondepression
from JACC (2000;36:2140-2145) as cited in ACCSAP7from JACC (2000;36:2140-2145) as cited in ACCSAP7
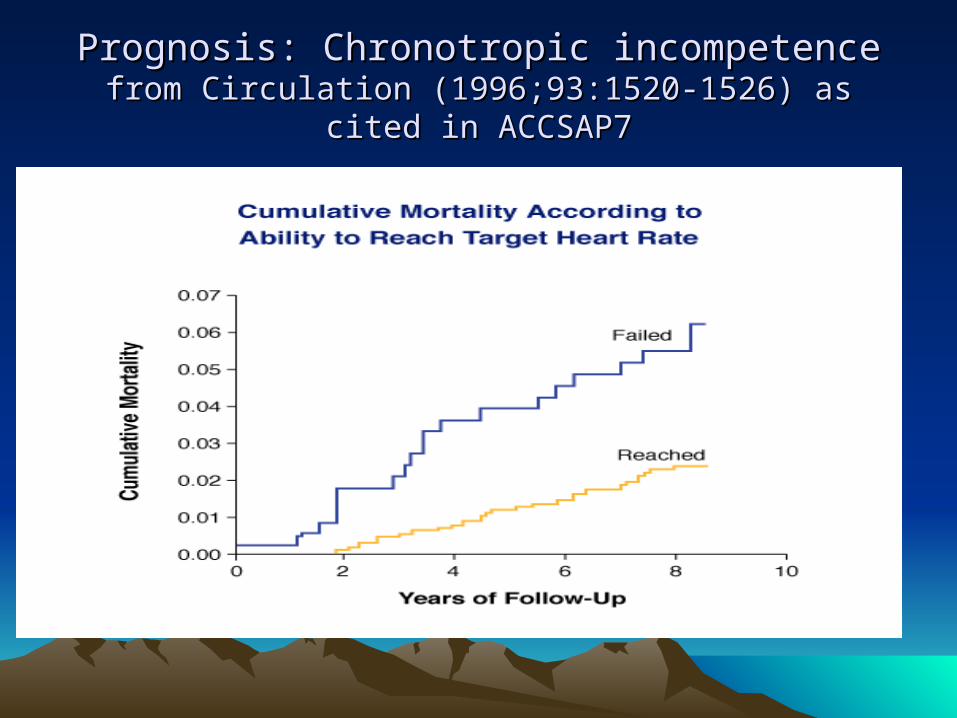
Prognosis: Chronotropic incompetencePrognosis: Chronotropic incompetencefrom Circulation (1996;93:1520-1526) as cited in ACCSAP7from Circulation (1996;93:1520-1526) as cited in ACCSAP7

Prognosis: Exercise ST-elevationPrognosis: Exercise ST-elevationas shown in ACCSAP7as shown in ACCSAP7
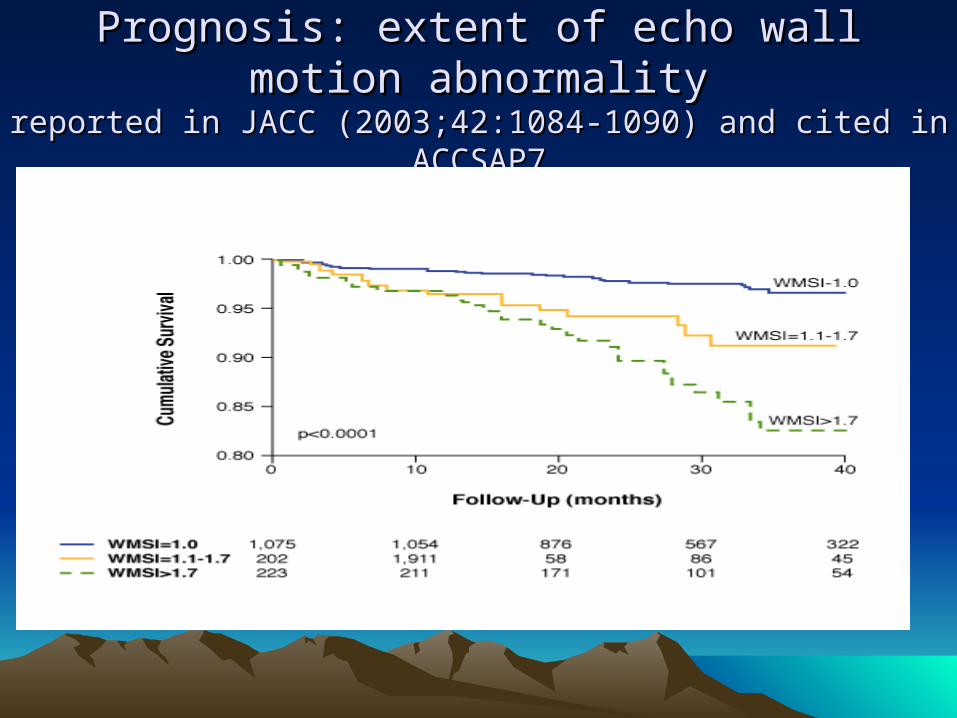
Prognosis: extent of echo wall motion abnormalityPrognosis: extent of echo wall motion abnormalityreported in JACC (2003;42:1084-1090) and cited in ACCSAP7reported in JACC (2003;42:1084-1090) and cited in ACCSAP7

YHC Exercise Echo ReportYHC Exercise Echo Report
• Duration• Limiting symptom• Heart rate response• BP response• ST-segments• Disclaimers: weight• Rest wall motion• Exercise wall motion
• Prognosis and RX efficacy• What limits this pt.?• Chronotropic reserve• Inotropic reserve• ECG-ischemia• Technical limitations • Prior infarction• Reversible ischemia

Exercise Echocardiography: AppropriatenessExercise Echocardiography: AppropriatenessJACC 2008;51:1127-1147.JACC 2008;51:1127-1147.
• Indication categories– Detection of CAD/Risk Assessment: symptomatic– Detection of CAD/Risk Assessment: asymptomatic– Detection of CAD/Risk Assessment: co morbidities– Risk assessment with prior test results– Risk assessment: Pre-operative for non-cardiac surgery– Risk assessment: after acute coronary syndrome (ACS)– Risk assessment: after revascularization (PCI or CABG)– Assessment of viability/ Ischemia– Hemodynamic assessment

Summary of Exercise EchoSummary of Exercise Echo
• Why did you order this test?
• How will you use the results, of this test, to better manage your patient?
• Have you taken into account the limitations of these test data?