-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
1/9
Acute kidney injury and chronic kidney disease:an integrated
clinical syndromeLakhmir S. Chawla1,2 and Paul L. Kimmel2,3
1Department of Anesthesiology and Critical Care Medicine, George
Washington University Medical Center, Washington,
District of Columbia, USA; 2Division of Renal Diseases and
Hypertension, Department of Medicine, George Washington
University
Medical Center, Washington, District of Columbia, USA and
3National Institute of Diabetes, Digestive, and Kidney
Disorders,
National Institutes of Health, Bethesda, Maryland, USA
The previous conventional wisdom that survivors of acute
kidney injury (AKI) tend to do well and fully recover renal
function appears to be flawed. AKI can cause end-stage renal
disease (ESRD) directly, and increase the risk of developing
incident chronic kidney disease (CKD) and worsening ofunderlying
CKD. In addition, severity, duration, and
frequency of AKI appear to be important predictors of poor
patient outcomes. CKD is an important risk factor for the
development and ascertainment of AKI. Experimental data
support the clinical observations and the bidirectional
nature
of the relationships between AKI and CKD. Reductions in
renal mass and nephron number, vascular insufficiency, cell
cycle disruption, and maladaptive repair mechanisms appear
to be important modulators of progression in patients with
and without coexistent CKD. Distinction between AKI and
CKD may be artificial. Consideration should be given to the
integrated clinical syndrome of diminished GFR, with acuteand
chronic stages, where spectrum of disease state and
outcome is determined by host factors, including the balance
of adaptive and maladaptive repair mechanisms over time.
Physicians must provide long-term follow-up to patients with
first episodes of AKI, even if they presented with normal
renal
function.
Kidney International (2012) 82, 516524;
doi:10.1038/ki.2012.208;
published online 6 June 2012
KEYWORDS: acute kidney injury; acute on chronic; acute renal
failure;
chronic kidney disease; progression; risk factor
Acute kidney injury (AKI) is responsible for approximately2
million deaths annually worldwide.13 AKI is increasinglycommon in
critically ill patients, and those patients with themost severe
form of AKI, requiring renal replacement
therapy, have a mortality rate of 5080%.3 Over the past 10years,
there has been substantial progress in the field of AKI.In
particular, work on consensus definitions, epidemiologicand
database studies, AKI biomarkers, and the appropriatedosing of
renal replacement therapy has continued at a briskpace. The classic
teaching regarding patients who survive anepisode of AKI, in
particular acute tubular necrosis (ATN),was that those patients
achieved full or nearly full recovery.4
This notion was based on studies that followed survivors ofAKI
after hospital discharge.4,5 The most recent comprehen-sive study
of AKI survivors followed 187 patients with ATNfor 10 years.5 The
authors concluded that for those who
survived renal function is adequate in most patients.
5
However, the notion that most patients with AKI return
topre-morbid renal function is contradicted by a series of smallbut
careful clinical studies conducted over 50 years ago.6,7
Good clinical recovery, which is sustained, is the rule
wasreported by Lowe6 in his study of 14 selected patients
whosurvived an episode of oliguria or anuria associated withATN.
Three patients (of the eight who had the assessment) inthis series,
however, had creatinine clearance ofo80 ml/min.Lowe attributed any
renal dysfunction to scarring or vasculardamage. Finkenstaedt and
Merrill7 reported inulin clearancesofo70 ml/min in 6 of the 16
patients with no evidence ofrenal disease before occurrence of
acute renal failure (ARF)
1376 months after the episode. They concluded that thefindings
demonstrated that an episode of ARF resulted inmore chronic renal
damage than would be expectedand that subnormal renal function late
in the follow-upperiod occurred in the majority of cases studied.
Theyattributed chronic dysfunction to rupture of basementmembranes
with abnormal epithelial regeneration, resultingin nephron
loss.
Up to 2007, however, when the epidemiology of AKIsurvivorship
was assessed, there was a lack of large longitudinalstudies to
assess the effects of AKI on long-term renal function.8
More recently, from 2008 through 2012, multiple
observational
m i n i r e v i e w http://www.kidney-international.org
& 2012 International Society of Nephrology
Received 20 October 2011; revised 13 January 2012; accepted
21
February 2012; published online 6 June 2012
Correspondence: Lakhmir S. Chawla, Department of Anesthesiology
and
Critical Care Medicine, George Washington University Medical
Center, 900
23rd Street, NW, RILF, G-105, Washington, District of Columbia,
20037, USA.
E-mail: [email protected]
516 Kidney International(2012) 82 , 516524
http://dx.doi.org/10.1038/ki.2012.208http://www.kidney-international.org/mailto:[email protected]:[email protected]://www.kidney-international.org/http://dx.doi.org/10.1038/ki.2012.208
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
2/9
studies assessing unique cohorts of patients, often using
largeadministrative databases, demonstrated that patients who
survivean episode of AKI have a significant risk for progression
toadvanced-stage chronic kidney disease (CKD).914
We review data suggesting that AKI is a cause of CKD andthat
prevalent CKD is a cause of incident AKI, and focus onthe
interrelationships between these two entities. We reviewthe
potential mechanistic factors underlying links betweenAKI and CKD,
and offer clinical considerations based onthese observations.
AKI AS A RISKFACTOR FOR INCIDENT CKD
Ishani et al .10 assessed a random sample of
Medicarebeneficiaries and found that patients diagnosed with
anepisode of AKI were more likely to develop end-stage renaldisease
(ESRD) compared with patients without a history ofeither AKI or
CKD. In their analysis, the risk of developingESRD was eightfold
higher in those with AKI compared withpatients without a history of
AKI or CKD. As this study used
ICD-9 diagnostic codes, it is difficult to determine
theproportion of patients who suffered AKI and then
progresseddirectly to ESRD compared with patients who
sufferedAKI,recovered renal function, and then progressed to
ESRD.10
Lo et al.,1 1 by using a Kaiser Permanente database inNorthern
California, retrospectively studied inpatient admis-sions. Patients
with an episode of AKI treated with dialysis werecompared with
patients without an episode of AKI. Patientswith a history of ESRD
or a preadmission estimated glomerularfiltration rate (eGFR) o45
ml/min per 1.73m2 were excluded.In this study, the investigators
found that an episode ofdialysis-requiring AKI was associated with
a 28-fold increased
risk of developing advanced CKD, and a 2-fold increase
inmortality. As patients who developed ESRD within 30 daysof
discharge were excluded from the long-term follow-up ofadvanced
CKD, these data are consistent with a severe formof AKI followed by
renal recovery and then progression toadvanced-stage CKD.11 It
should be noted that some patientsassessed had pre-existing
CKD.
Wald et al.13 conducted a population-based cohort studyin
Ontario, Canada of AKI patients who required in-hospitaldialysis
and survived free of dialysis for at least 30 days afterdischarge.
These patients were matched with patients withoutAKI or dialysis
therapy during their index hospitalization.Patients with AKI
requiring dialysis were over three times
more likely to develop ESRD compared with
control-matchedpatients.
We and colleagues at the Veterans Affairs Medical Centerin
Washington, DC assessed a United States Department ofVeterans
Affairs database to ascertain long-term renal functionin over
79,000 hospitalized patients with and without AKI.12
A particular focus was on the long-term outcome in patientswith
a diagnosis of ATN. Patients hospitalized for acutemyocardial
infarction or pneumonia without AKI were desig-nated as controls.
The remaining 5404 hospitalized patientswho comprised the AKI group
had diagnostic codes indicat-ing ARF or ATN. Patients with
pre-existing CKD were
excluded. Over the 5-year follow-up period, renal
functiondeteriorated over time in all groups, but with
significantlygreater severity in those who had ATN and ARF
comparedwith controls. Patients with AKI, especially those with
ATN,with pre-existing normal renal function were more likelythan
controls to enter stage 4 or 5 CKD. We found thatpatients who had
an episode of AKI were at high risk for thedevelopment of stage 4
CKD andhad reduced survival timecompared with control
patients.12
Our studies in AKI survivors identified advanced age,
thepresence of diabetes mellitus, and decreased baseline eGFRasrisk
factors for the progression to advanced-stage CKD.12,15 Inaddition
to these risk factors, along with our colleagues, werecently showed
that low serum albumin concentration (SAlb)is a strong predictor of
poor long-term renal outcome.9 Thevalue of the SAlb as a predictor
of CKD progression is notsurprising, because this parameter has
been associated withpoor outcomes in both the general population
and in a varietyof diseases including ESRD, surgical illness, and
acute stroke.1618
Low SAlb levels can be a result of nutrition-related
factorsand/or high levels of inflammation.19,20 As several
recentstudies have shown that markers of inflammation predictAKI,
it is likely that the relationship between SAlb level andCKD
progression is based on a complex set of factors,including those
related to diet, nutrition, and catabolism, aswell as increased
inflammation.15,21
Collectively, these studies underscore the strong associa-tion
between AKI and the future development of CKD.
SEVERITY, DURATION, AND FREQUENCY OF AKI AND CKD
PROGRESSION
More recently, severity of AKI has been linked to CKDprogression
in survivors of AKI. Ishaniet al.22 assessed patientswho underwent
cardiac surgery, and found that the magnitudeof serum creatinine
concentration during the postoperativehospital course was directly
linked to progression. This effectwas seen in patients with AKI
with previously normal renalfunction (de novoAKI), as well as in
patients with an episodeof AKI superimposed on CKD (acute on
chronic renalfailure).22 The magnitude of increase in serum
creatinine aftercardiac surgery was associated in a graded manner
withincreased risk of CKD progression and mortality.
This same trend has been demonstrated in patients whohad
percutaneous coronary revascularization. James et al.23
showed that patients undergoing percutaneous
coronaryrevascularization who had AKI were at risk for future
develop-ment of ESRD. Patients with AKIN stage I AKI were over
4times more likely to develop ESRD, whereas patients with AKINstage
II/III were over 11 times more likely to develop ESRD. 23
We have similarly shown that the severity of AKI is linkedto CKD
progression.9 We assessed a cohort of 11,589 patientswith a
spectrum of AKI from RIFLE stage R through F.9
Severity of AKI, assessed by peak serum creatinine,
wasassociated with progression to advanced CKD (Figure 1).
Inparticular, patients who required dialysis were at muchhigher
risk for progression to CKD than patients with less
Kidney International(2012) 82 , 516524 517
LS Chawla and PL Kimmel: Acute kidney injury and chronic kidney
disease m i n i r e v i e w
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
3/9
severe AKI.9 Although it is seemingly intuitive that the
severity of AKI would be associated with progression
toadvancedCKD, these three studies are the first to show
thislink.9,22,23 These findings suggest that when the severity
ofAKI reaches a certain threshold the course of AKI is
altered,initiating a chronic, progressive disease.
In addition to severity, the duration of AKI has beenlinked to
mortality but not to CKD progression. Coca et al.24
assessed a large cohort of patients with diabetes
mellitusundergoing cardiac surgery in the Veterans
Administrationsystem. Both severity and duration of AKI were linked
tolong-term mortality. However, the duration of AKI was notlinked
to CKDprogression.24 Consistent with these findings,
Brownet al.
25
assessed a separate cohort of US Veterans aftercardiac surgery
and confirmed that the duration of AKI waslinked to worse long-term
survival.
Not surprisingly, patients who sustain multiple episodes ofAKI
as compared with a single episode of AKIhave higherlikelihoods of
CKD progression. Thakar et al.26 have shown,in a cohort of US
Veterans with diabetes, that those whoexperienced two or more
episodes of AKI were much morelikely to progress to stage 4 CKD
than patients whoexperienced only one episode of AKI (Figure
2).26
These data are consistent with the hypothesis that for
somepatients a single episode of AKI has biologic
ramificationsbeyond the acute event, engendering an ongoing state
that
predisposes to the development of further injury,
manifesteddifferentially in time as worsened AKI (short-term) or
thedevelopment or worsening of CKD over longer periods(Figure 3).
Some patients can fully recover from their initialAKI, but subsets
of AKI survivors appear to go on toexperience vicious cycles of
intertwined AKI and CKD.26 It islikely that the severity of renal
injury along with other clinical,treatment, and host risk factors
mediate such processes.
AKI AS ANACCELERANT OF CKD
Hsu et al.27 showed that the incident growth of the
ESRDpopulation exceeded the prevalent CKD population. The
authors hypothesized that physician-related decisionsto start
chronic dialysis earlier might account for thisdiscrepancy. We
believe that the more likely explanation isthe marked effect of AKI
on the development and progres-sion of CKD.
CKD has consistently been shownto be a significant riskfactor
for the development of AKI.28,29 Probable explanationsinclude the
hemodynamic instability and failure of auto-
regulation30 in CKD patients, the ease of detection of
smallchanges in GFR when renal function is impaired, and
apredispositionto further injury in patients with diminishedrenal
function.31,32 These consist of at least susceptibility
tonephrotoxic agents, and the effects of ongoing humoral andrenal
pathologic mechanisms in the setting of CKD.Unfortunately, this
risk appears to be bidirectional. Ishaniet al.10 showed that
patients with CKD who experienced anepisode of AKI were 41 times
more likely to develop ESRDthan patients without kidney disease,
whereas patients withCKD and no episodes of AKI had an 8.4-fold
higher riskcompared with patients without kidney disease. The risk
of
a b
80
90
100
70
50
60
40
30
MeaneGFR
Tertile 1: meaneGFR>79.2
Tertile 2: meaneGFR 61-79.2
Tertile 3: meaneGFR
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
4/9
developing ESRD was enhanced almost fourfold by
thesuperimposition of AKI in CKD patients. AKI enhanced therisk
almost 10-fold compared with patients without eitherCKD or AKI, and
astonishingly was associated with greaterrisk of developing ESRD
than those identifiedwith CKD in
the Medicare population. Similarly, Hsu et al.
33
showed thatpatients with an eGFR o45ml/min per 1.73m2
whoexperienced an episode of dialysis-requiring AKI were atvery
high risk for impaired recovery of renal function. In
apopulation-based cohort in Scotland, Ali et al.1 showed thatonly
64% of patients with an episode of acute on chronicrenal failure
had full recovery of kidney function.1
In these studies, CKD was defined by an eGFR of460 ml/min per
1.73 m2. In addition to low baseline eGFR,patients with CKD as
assessed by proteinuria are at increasedrisk for AKI. Jameset al.29
showed in a cohort of over 920,000patients that the level of
proteinuria and diminished baselineeGFR were independent risk
factors for developing AKI.29
The risk of progression to CKD in patients who developAKI is not
limited to adults but affects children as well. 34,35
Large pediatric cohort studies suggest that certain subsets
ofchildren (such as bone marrow transplant patients) are athigh
risk for CKD progression. In contrast to adults, childrentend to be
less burdened with chronic disease. Thus, theevidence that AKI in
children puts those patients at risk forCKD suggests processes
subsequent to AKI that are integralto the acute episode, as opposed
to simply changes that occurin an acute on chronic disease
paradigm.
Hui-Stickle et al.36 assessed pediatric intensive care
unitpatients upon discharge from a tertiary care center. In
all,
34% had either reduced kidney function or were dialysisdependent
upon discharge.36 The most compelling dataregarding AKI and the
risk of CKD in children came from along-term follow-up of
participants in the aforementionedstudy conducted by Askenazi et
al.37 They followed up acohort of children for 3 to 5 years after
an episode of AKI.Mortality was 79.9%, with the majority of the
deathsoccurring within 2 years of the AKI episode. In all, 17 of29
patients followed up in an outpatient clinic demonstratedevidence
of CKD, manifested by hyperfiltration, reducedkidney function,
hypertension, or microalbuminuria.37
Although this represents a small sample, it is consistent
withanimal and adult human studies showing that subsets ofpatients
who develop AKI are at high risk for developingCKD and experiencing
progression.
These data suggest that for some patients AKI and CKDlikely
coexist in an intimate but vicious cycle. This concept issupported
by the fact that CKD was thought to progress in alinear manner,38
but this is not always the case. Shah and
Levey39 showed that as many as one-third of patients
deviatedfrom their reciprocal creatinine slope. The African
AmericanStudy of Kidney Disease and Hypertension study has
delinea-ted several different courses in patients with CKD
(personalcommunication, Tom Greene). Some of these courses
areconsistent with the notion of intermittent episodes of
AKIcomplicating CKD, with varying levels of repair occurring.An
episode of AKI that results in a decrement in GFR willnecessarily
affect the trajectory of GFR change; the course willultimately be
determined by whether the injury is reversible(volume-related
changes in GFR and filtration fraction) andby the balance between
effective and maladaptive repair
mechanisms (Figure 4). The exact mechanism(s) by whichAKI
accelerates/initiates CKD in humans are unknown.Preclinical data,
however, suggest that a variety of mechanismsmay be operative.
MECHANISMS UNDERLYING PROGRESSION OF AKI TO CKD
An important concept for understanding the course of CKD isthat
the progression to ESRD occurs via processes that maybe independent
of the original pathology of CKD.32,40 Suchconceptswere originally
proposed for a variety of glomerulardiseases,40 after follow-up
studies in patients with post-streptococcal glomerulonephritis
delineated long-term sequelae41
linked to current definitions of CKD, including decrements
in GFR and the persistence of proteinuria, as well as
thedevelopment of hypertension. Data from animal modelssuggest that
kidneys after episodes of injury may be sus-ceptible to progression
to CKD, which is similarly indepen-dent of the initial cause of
AKI. Key constructs regarding CKDprogression are based on findings
from the remnant kidneymodel in which nephron loss leads to
glomerular hypertrophyin the remaining nephrons.42 Hypothesized
mechanismsunderlying CKD progression include effects of systemic
andintrarenal hypertension and hyperfiltration, tubular
hyper-trophy, and hypertension resulting in arteriosclerosis,
tubu-lointerstitial fibrosis, and glomerulosclerosis,4345 as well
as
100%
0
GFR
Time
AKI Repair Chronic
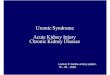
Figure 3 | Theoretical range of outcomes after acute
kidneyinjury (AKI). The range of possible long-term outcomes after
anepisode of AKI comprises the entire spectrum of the
glomerularfiltration rate (GFR). The final GFR is determined by the
level ofGFR at the time of injury, the severity and duration of the
injury,and responses across several phases over time. It is
envisionedthat repair and chronic phases have different and
variable timeframes, and different magnitudes of responses.
Responses duringrepair and chronic phases are determined by the
balance ofprocesses that result in amelioration and worsening of
GFR.
Kidney International(2012) 82 , 516524 519
LS Chawla and PL Kimmel: Acute kidney injury and chronic kidney
disease m i n i r e v i e w
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
5/9
the effects of derangements of the endocrine response and
abnormalities in circulating mediators associated with
decre-ments in renal function. The latter may affect cell structure
andfunction, as well as physiologic responses. In the case of
normalkidneys after an episode of injury, multiple injury pathways
andmaladaptive processes have been identified, which maycontribute
to determining the course of renal function afteran initial
insult.
Nephron loss and glomerular hypertrophy
The pathophysiology of loss of nephron mass followed
byglomerular hypertrophy has been well described in animalmodels.43
After an episode of AKI, it is possible that signi-ficant permanent
loss of nephron mass results in a clinical
state comparable to that of the remnant kidney model.
Aftersubtotal nephrectomy, single-nephron GFR increases
viahyperfiltration and glomerular hypertrophy. Cellular
prolif-eration ensues, ultimately resulting in tubulointerstitial
fibrosisand progressive nephron loss.32 These processes are
exacer-bated by high-salt and high-protein diets.46,47
Increasedtubular workload predisposes nephron segments to
fibrosisand senescence, which can be mitigated by protein and
calorierestriction.47,48
The lessons from animal studies have been successfullytranslated
into patient-care paradigms. As an example, acornerstone of CKD
therapy is mitigation of glomerular
hypertrophy and hyperfiltration via hypertension control and
reninangiotensinaldosterone system blockade.
Interstitial inflammation and fibrosis
In human CKD and in the remnant kidney model,tubulointerstitial
fibrosis predominates over glomerulo-sclerosis.32 As a consequence,
human CKD often progresseswithout the need for continued glomerular
injury.45,4951
Further support of a pro-fibrotic effect in the setting
ofreduced renal mass is provided by experiments that show thatthe
kidneys of animals exposed to ischemiareperfusion (IR)injury are
more predisposed to developing fibrosis if nephronloss (e.g.,
unilateral nephrectomy) occurs before injury.52,53
In addition, inflammation after AKI can lead to interstitial
immune cell infiltration followed by interstitial
fibrosis.Inflammation has been shown tobe an important feature
ofischemic and septic AKI.15,5456 Animal models of ATNconsistently
show an interstitial neutrophil infiltrate duringthe acute phase of
ATN, often followed by monocyticlymphocytic infiltration in later
stages.32,55,57,58 Monocytescan exacerbate injury and promote
fibrosis.59 The effects oftubulointerstitial fibrosis are critical,
as tubulointerstitialfibrosis injury scores predict the decline of
renal functionbetter than glomerular injury scores.60,61 Reduced
renalmass impairs recovery of experimental AKI and maypredispose to
the development of fibrosis.32 In most models
Peri-tubularblood vessels
Interstitium
c
Normal repairand regeneration
a b ATN
Endothelialinjury
Cellsand casts
Cell cycle arrestEpigenetic changes
Zones ofhypoxia
d Maladaptiveresponse
Interstitialfibrosis
Depletedblood supply
Neutrophils andmonocytes
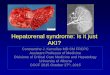
Figure 4 | Tubule cross-section. (a) Cross section of normal
renal tubule with intact epithelial cells, renal interstitium, and
peri-tubularblood vessels. (b) Cross section of renal tubule with
acute tubular necrosis (ATN) with epithelial cell necrosis,
intra-tubular cast formation,endothelial injury of peri-tubular
blood vessels, and migration of monocytes and macrophages into
renal interstitium. (c) Cross section ofrenal tubule after normal
repair and regeneration showing restoration of normal renal
architecture. (d) Cross section of renal tubule aftersevere episode
of AKI, resulting in maladaptive repair. Epithelial cells have
evidence of cell cycle arrest and epigenetic changes that favor
afibrosis phenotype. Renal interstitium shows evidence of fibrosis.
Post-injury vascular supply is less dense than baseline. The
combinationof decreased blood supply and fibrosis leads to zones of
hypoxia wherein the combination of decreased vascular supply and
fibrosis caninitiate a vicious cycle leading to ongoing
fibrosis.
520 Kidney International(2012) 82 , 516524
m i n i r e v i e w LS Chawla and PL Kimmel: Acute kidney injury
and chronic kidney disease
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
6/9
of experimental AKI, renal tubular regeneration occurs,
butdepending on the severity of the initial damage the recoveryis
often incomplete. Areas that do not complete full recoverymay
develop into focal areas of fibrosis.32,55,62
Both human and animal models link severity andfrequency of AKI
with worsening of long-term renalfunction.9,22,63 Multiple episodes
of IR-induced AKI havebeen shown to cause CKD and
tubulointerstitial fibrosis inanimal models. Thus, it is
conceivable that subclinicalepisodes of AKI could both cause and
worsen CKD.32 Thesedata are consistent with the previously cited
human datashowing the effect of multiple episodes of AKI to
enhanceCKD progression.26
Endothelial injury and vascular rarefaction
Experimental models of AKI demonstrate endothelialinvolvement
and vascular injury. Tubular repair after injurytends to be robust,
but the vascular restorative capacity afterAKI is more blunted.64
Various different injury models (e.g.,
IR, folate, nitric oxide synthase inhibition, and
ureteralobstruction) all demonstrate diminished vascular
densityafter injury.6568 The loss of vascular density varies
between30 and 50%.69 The loss of vascular reserve may be oneof the
key components of the development of fibrosisafter injury. Injured
tissue that has insufficient vascularsupply becomes hypoxic,
potentially setting into motion aself-propagating injury cascade.
Rarefaction of capillariesinitiates activation of hypoxia-inducible
pathways that canpromote inflammation and downstream fibrosis.32
Thus,capillary rarefaction in fibrotic foci can be both a cause
andan effect of tissue hypoxia, in turn leading to activation
of
hypoxic signaling, inflammation, and activation of
factorsenhancing fibrosis.In experimental models, treatment with
angiogenic factors
such as vascular endothelial growth factor-121
amelioratesvascular dropout and endothelial damage.54 However,
thesecompounds are only useful in the immediate post-injuryperiod,
and do not improve vascular dropout after AKI whenadministered43
weeks after the insult.32
Cell cycle and maladaptive repair
Normal repair processes involve a host of growth factors
andproliferative and other signaling cascades, which must
bedeployed, and function in coordinated, integrated temporal,
and spatial manners. These mechanisms are critical
forappropriate repair and regeneration.70 Cell cycle
abnormalitiesaffect the outcome of AKI. Preclinical studies
demonstratethat p21, a cyclin-dependent kinase, is a critical
check-point effector for induction of the cell cycle.71 In
preclinicalmodels of AKI, p21 antagonism worsens AKI, whereas
p21induction improves outcomes in AKI models.72,73 Cell
cycledysfunction can have effects at the point of injury and
furtherdownstream during repair. Pathways that affect the cell
cyclecan also activate fibroblasts and inflammation. Selected
anti-inflammatory therapies have been shown to decrease theseverity
of AKI during its acute phase.32,74 Recently, studies
involving the cell cycle of reparative cells have shed light
onsuch processes.72,73
When AKI is severe, the corresponding tubular injury
andinterstitial inflammation are associated with proliferation
oftubular epithelial cells. Yanget al.63 showed that when
kidneydamage was accompanied by fibrosis there were largenumbers of
proximal tubule epithelial cells arrested in theG2/M phase of the
cell cycle. In contradistinction to prolif-erating epithelial
cells, the arrested cells produced greaterlevels of transforming
growth factor-b1 and connective tissuegrowth factor. These findings
suggest that in response toinjury a maladaptive repair process may
ensue, causingfibrosis instead of repair of tubular epithelia. Cell
cycle arrestcauses tubular epithelial cells to convert to a
phenotype thatpromotes the growth and activation of fibroblasts.
Interest-ingly, in this same study, moderate IR injury did
notproduce this maladaptive process. Only severe injury with IRor
aristolochic acid activated pro-fibrotic processes. Cell arrestwas
mitigated by agents, such as p53 inhibitors, that affect the
cell cycle, and was exacerbated by agents that prolong cellcycle
arrest.63
Animal studies support the notion that fibrosis is ongoingafter
AKI. Bechtelet al.69 investigated mechanisms of fibrosisthat were
temporally remote from the initiation of kidneyinjury. They showed
that fibrosis continues owing to a failureof fibroblasts to return
to their resting state. Epigeneticfactors including
hypermethylation ofRASAL1gene loci wereinvolved. Both studies by
Yang et al.63 and Bechtel et al.69
implicate the pathologic role of transforming growth
factor-b
in promoting fibrosis.63,69
When tubular epithelial cells arrest in the G2/M phase of
the cell cycle, they produce transforming growth factor-b1.If
transforming growth factor-b1 secretion and activationis sustained,
epigenetic changes in fibroblasts may ensue,which can transform
them into tumor-like myofibroblaststhat proliferate in a growth
factorindependent manner.74
Altogether, cell cycle arrest and epigenetic changes representat
least two maladaptive repair mechanisms that appear tohave major
roles in determining the post-AKI fibroticphenotype. As cell cycle
arrest and epigenetic changes appearto be sequentialin nature, they
may form pathways amenableto interruption.63,73,75,76
Identification of patients and risk factors for CKD
progression
To help clinicians identify AKI survivors at increased risk
forCKD development and progression, along with our collea-gues, we
developed three multivariable models. The mostaccessible (and
therefore clinically useful) model is based onsentinel clinical
events (i.e., RIFLE stage, need for dialysis,baseline eGFR, and
sAlb).9 This model performed well,explaining 11% of the variance in
the development of CKD(area under ROC curve 0.77). We validated
this equation ina separate large cohort of hospitalized Veterans
(Po0.001,c-statisticX0.81). As these end points are accessible
andclinically relevant, clinicians could potentially use
suchequations to risk stratify AKI survivors at highest risk
for
Kidney International(2012) 82 , 516524 521
LS Chawla and PL Kimmel: Acute kidney injury and chronic kidney
disease m i n i r e v i e w
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
7/9
progression toCKD for therapeutic reasons or for inclusionin
clinical trials.9
In addition to clinical models, novel AKI biomarkers showpromise
in improvingrisk assessment of patients with severeAKI. Srisawat et
al.77 have shown that plasma neutrophilgelatinaseassociated
lipocalin improves the discrimination ofclinical models to predict
renal recovery. Future studiesshould incorporate plasma and urine
biomarkers in riskassessment strategies to determine the best
approach toidentify patients at risk for CKD progression.
Summary
The paradigm of AKI has markedly shifted over the past 5years.
The previous conventional wisdom that survivors ofAKI tend to do
well and fully recover renal function, perhapsbased on indistinct
recollections of early, limited studies,appears to be flawed.6,7
AKI can cause ESRD directly,8,10,78
and appears to increase the risk for incident CKD and
worsenunderlying CKD.12,22 In addition, severity and frequency
of
AKI appear to be important predictors of poorer out-comes.9,26
Experimental data support the clinical observa-tions.
Mechanistically, renal mass, vascular insufficiency, cell
cycledisruption, and maladaptive repair appear to be
importantmodulators of outcome, and these pathophysiologic
processesare likely operative in mediating the poor outcomes
observedin the clinical epidemiologic studies reviewed above.
The public health impact of the long-term outcomes ofAKI is
significant. The population incidence of AKI isapproximately 2100
per million population.1 Given thepopulation of the developed world
(USA, Canada, WesternEurope, and Australia) of approximately 1
billion, there
will be over 2 million cases of AKI this year, with an
expected1.5 million AKI survivors. Of these patients,
approxi-mately 1520% will progress to advanced-stage CKD within24
months, resulting in approximately 300,000 cases ofadvanced CKD per
year. Given the increasing incidence ofAKI in the aging
population,8,79,80 the projected incidence isexpected to increase.
The National Institute of Diabetes,Digestive and Kidney Disease
supports the Assessment, SerialEvaluation, and Subsequent Sequelae
of Acute Kidney Injury(ASSESS AKI) study, which evaluates the
long-term outcomeof hospitalized patients, with and without CKD,
whoexperience an episode of AKI, to determine the naturalhistory of
AKI and delineate risk factors for progression and
development of complications, including
cardiovasculardisease.81
We propose a new model integrating acute and CKD. Theseparation
of ARF and CKD into two distinct syndromes astaught in medical
school is not in the best interest of anintegrated approach to the
long-term care of patients withkidney disease. Rather, we propose
consideration of the stateof diminution in GFR as a clinical
entity, which hasdifferential initiation and expression in time and
along thespectrum of magnitude of GFR (Figure 3). Phases of
diseaseinclude initiation, repair, and long-term outcomes (Figure
3and/or4). Differences in timing and severity of injury and the
balance of adaptive and maladaptive repair determineclinically
apparent outcomes. The range of change inresponse to differential
injury and the balance of adaptiveand maladaptive repair in
patients with different initial levelsof renal function comprise
the entire spectrum of GFR(Figure 3). Interventions to preserve
function and enhancerepair are presumably appropriate at several
stages of thedisease. Commonalities and differences in
mechanismsmediating the different courses of long-term outcome
mustbe delineated and translated into clinical trials and
practiceover the next decade.
The giants, such as Lowe and Merrill, on whose shoulderswe
stand, were correct, even if their early findings were
lost,misinterpreted, or incorrectly recalled. AKI and CKDcomprise
an intertwined clinical entity, a disease ofdiminished renal mass
resulting in diminished GFR.
Recommendations and future directions
We recommend that hospital survivors of AKI who experience
severe AKI (AKIN stage III) be followed up by a
nephrologistafter discharge. Currently, this does not occur. At 30
days afterdischarge from the hospital with an episode of AKI, 74.5%
ofpatients were seen by a primary physician compared with11.9% and
29.5%, respectively, who were seen by a nephrologistor a
cardiologist.82 Surprisingly, only about one-third of AKIpatients
requiring dialysis (AKIN stage III) are seen by anephrologist
within 30 days of discharge. This increases to48.6% within 1 year
ofdischarge, which is likely a result of arising serum
creatinine.82 Overall, a very small fraction of AKIpatients are
currently followed up by nephrologists afterhospital discharge.82
To put this into context, an assessment
of the nephrology follow-up of AKI survivors as compared withthe
cardiology follow-up of myocardial infarction survivorsreveals a
stark difference (11.9% vs. 76%, respectively).31,82 Atthe very
least, we should continue to see our patients.Monitoring patients
for blood pressure control, the use ofdrugs that interfere with the
reninangiotensin system, andavoidance of nephrotoxins may prove
critical as public healthmeasures, which may oppose current secular
trends.
DISCLOSURE
All the authors declared no competing interests.
ACKNOWLEDGMENTS
We thank Paul Eggers and Richard Amdur for reviewing
themanuscript.
DISCLAIMERThe views expressed in this article do not necessarily
represent theviews of the Department of Health and Human Services,
the NationalInstitutes of Health, the National Institute of
Diabetes, Digestive andKidney Diseases, or the United States
Government.
REFERENCES1. Ali T, Khan I, Simpson Wet al. Incidence and
outcomes in acute kidney
injury: a comprehensive population-based study.J Am Soc
Nephrol2007;18: 12921298.
2. Murugan R, Kellum JA. Acute kidney injury: whats the
prognosis?Nat RevNephrol2011; 7 : 209217.
522 Kidney International(2012) 82 , 516524
m i n i r e v i e w LS Chawla and PL Kimmel: Acute kidney injury
and chronic kidney disease
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
8/9
3. Uchino S, Kellum JA, Bellomo Ret al. Acute renal failure in
critically illpatients: a multinational, multicenter study. JAMA
2005; 294: 813818.
4. Kjellstrand CM, Ebben J, Davin T. Time of death, recovery of
renalfunction, development of chronic renal failure and need for
chronichemodialysis in patients with acute tubular necrosis.Trans
Am Soc ArtifIntern Organs 1981; 27: 4550.
5. Liano F, Felipe C, Tenorio MT et al. Long-term outcome of
acute tubularnecrosis: a contribution to its natural history.Kidney
Int2007;71: 679686.
6. Lowe KG. The late prognosis in acute tubular necrosis; an
interim follow-
up report on 14 patients. Lancet1952: 10861088.7. Finkenstaedt
JT, Merrill JP. Renal function after recovery from acute
renalfailure.N Engl J Med1956; 254: 10231026.
8. Xue JL, Daniels F, Star RAet al. Mortality and advancing to
end-stagerenal disease in patients with hospital and non-hospital
acquired renalfailure.J Am Soc Nephrol2007; 15: SA-PO965.
9. Chawla LS, Amdur RL, Amodeo Set al.The severity of acute
kidney injurypredicts progression to chronic kidney disease.Kidney
Int2011; 79:13611369.
10. Ishani A, Xue JL, Himmelfarb Jet al.Acute kidney injury
increases risk ofESRD among elderly. J Am Soc Nephrol2009; 20:
223228.
11. Lo LJ, Go AS, Chertow GM et al. Dialysis-requiring acute
renal failureincreases the risk of progressive chronic kidney
disease.Kidney Int2009;76: 893899.
12. Amdur RL, Chawla LS, Amodeo Set al.Outcomes following
diagnosis ofacute renal failure in U.S. veterans: focus on acute
tubular necrosis.KidneyInt2009; 76: 10891097.
13. Wald R, Quinn RR, Luo Jet al.Chronic dialysis and death
among survivorsof acute kidney injury requiring dialysis.JAMA2009;
302: 11791185.14. Garg AX, Suri RS, Barrowman N et al. Long-term
renal prognosis of
diarrhea-associated hemolytic uremic syndrome: a systematic
review,meta-analysis, and meta-regression. JAMA2003;290:
13601370.
15. Chawla LS, Seneff MG, Nelson DRet al.Elevated plasma
concentrations ofIL-6 and elevated APACHE II score predict acute
kidney injury in patientswith severe sepsis. Clin J Am Soc
Nephrol2007; 2: 2230.
16. Engelman DT, Adams DH, Byrne JGetal. Impact of body mass
index andalbumin on morbidity and mortality after cardiac surgery.
J ThoracCardiovasc Surg1999; 118: 866873.
17. Gariballa SE, Parker SG, Taub N et al. Influence of
nutritional status onclinical outcome after acute stroke.Am J Clin
Nutr1998; 68: 275281.
18. Owen Jr WF, Lew NL, Liu Yet al. The urea reduction ratio and
serumalbumin concentration as predictors of mortality in patients
undergoinghemodialysis. N Engl J Med1993;329: 10011006.
19. Friedman AN, Fadem SZ. Reassessment of albumin as a
nutritional marker
in kidney disease. J Am Soc Nephrol2010; 21: 223230.20. Don BR,
Kaysen G. Serum albumin: relationship to inflammation andnutrition.
Semin Dial2004; 17: 432437.
21. Liu KD, Glidden DV, Eisner MDet al.Predictive and
pathogenetic value ofplasma biomarkers for acute kidney injury in
patients with acute lunginjury. Crit Care Med2007; 35:
27552761.
22. Ishani A, Nelson D, Clothier B et al. The magnitude of acute
serumcreatinine increase after cardiac surgery and the risk of
chronic kidneydisease, progression of kidney disease, and death.
Arch Intern Med2011;171: 226233.
23. James MT, Ghali WA, Knudtson MLet al. Associations between
acutekidney injury and cardiovascular and renal outcomes after
coronaryangiography. Circulation 2011; 123: 409416.
24. Coca SG, King Jr JT, Rosenthal RAet al. The duration of
postoperativeacute kidney injury is an additional parameter
predicting long-termsurvival in diabetic veterans.Kidney Int2010;
78: 926933.
25. Brown JR, Kramer RS, Coca SGet al. Duration of acute kidney
injury
impacts long-term survival after cardiac surgery.Ann Thorac Surg
2010;90: 11421148.26. Thakar CV, Christianson A, Himmelfarb J et
al. Acute kidney injury
episodes and chronic kidney disease risk in diabetes
mellitus.Clin J AmSoc Nephrol2011; 6: 25672572.
27. Hsu CY, Vittinghoff E, Lin Fet al.The incidence of end-stage
renal diseaseis increasing faster than the prevalence of chronic
renal insufficiency.AnnIntern Med2004; 141: 95101.
28. Thakar CV, Arrigain S, Worley Set al.A clinical score to
predict acute renalfailure after cardiac surgery.J Am Soc
Nephrol2005; 16: 162168.
29. James MT, Hemmelgarn BR, Wiebe Net al. Glomerular filtration
rate,proteinuria, and the incidence and consequences of acute
kidney injury:a cohort study. Lancet2010; 376: 20962103.
30. Bidani AK, Griffin KA, Williamson Get al. Protective
importance of themyogenic response in the renal
circulation.Hypertension 2009; 54:393398.
31. Daugherty SL, Ho PM, Spertus JAet al.Association of early
follow-up afteracute myocardial infarction with higher rates of
medication use.ArchIntern Med2008; 168: 485491 discussion 492.
32. Venkatachalam MA, Griffin KA, Lan Ret al. Acute kidney
injury: aspringboard for progression in chronic kidney disease.Am J
Physiol RenalPhysiol2010; 298: F1078F1094.
33. Hsu CY, Chertow GM, McCulloch CEet al.Nonrecovery of kidney
functionand death after acute on chronic renal failure.Clin J Am
Soc Nephrol2009;4: 891898.
34. Goldstein SL, Devarajan P. Acute kidney injury in childhood:
should we beworried about progression to CKD?Pediatr Nephrol2011;
26: 509522.
35. Goldstein SL, Devarajan P. Progression from acute kidney
injury tochronic kidney disease: a pediatric perspective. Adv
Chronic Kidney Dis2008; 15: 278283.
36. Hui-Stickle S, Brewer ED, Goldstein SL. Pediatric ARF
epidemiologyat a tertiary care center from 1999 to 2001. Am J
Kidney Dis 2005; 45:96101.
37. Askenazi DJ, Feig DI, Graham NMet al. 35 Year longitudinal
follow-upof pediatric patients after acute renal failure.Kidney
Int2006; 69:184189.
38. Mitch WE, Walser M, Buffington GAet al.A simple method of
estimatingprogression of chronic renal failure.Lancet1976; 2:
13261328.
39. Shah BV, Levey AS. Spontaneous changes in the rate of
decline inreciprocal serum creatinine: errors in predicting the
progression of renaldisease from extrapolation of the slope. J Am
Soc Nephrol1992; 2 :11861191.
40. Neugarten J, Feiner HD, Schacht RGet al. Aggravation of
experimentalglomerulonephritis by superimposed clip hypertension.
Kidney Int1982;22: 257263.
41. Baldwin DS. Poststreptococcal glomerulonephritis. A
progressive disease?Am J Med1977; 62: 111.
42. Ingelfinger JR. Disparities in renal endowment: causes and
consequences.Adv Chronic Kidney Dis 2008; 15: 107114.
43. Hostetter TH. Progression of renal disease and renal
hypertrophy. AnnuRev Physiol1995; 57: 263278.
44. Hostetter TH, Olson JL, Rennke HGet al. Hyperfiltration in
remnantnephrons: a potentially adverse response to renal
ablation.Jam SocNephrol2001; 12: 13151325.
45. Baldwin DS, Neugarten J. Hypertension and renal diseases.Am
J KidneyDis 1987; 10: 186191.
46. Shapiro JI, Elkins N, Reiss OKet al.Energy metabolism
following reductionof renal mass. Kidney Int Suppl1994; 45:
S100S105.
47. Nath KA, Croatt AJ, Hostetter TH. Oxygen consumption and
oxidant stress
in surviving nephrons.Am J Physiol1990; 258: F1354F1362.48. Tapp
DC, Wortham WG, Addison JFet al. Food restriction retardsbody
growth and prevents end-stage renal pathology in remnantkidneys of
rats regardless of protein intake.Lab Invest1989; 60:184195.
49. Risdon RA, Sloper JC, De Wardener HE. Relationship between
renalfunction and histological changes found in renal-biopsy
specimensfrom patients with persistent glomerular nephritis.
Lancet1968; 2 :363366.
50. Schainuck LI, Striker GE, Cutler REet al.
Structural-functionalcorrelations in renal disease. II. The
correlations.Hum Pathol1970; 1 :631641.
51. Striker GE, Schainuck LI, Cutler REet al.
Structural-functional correlationsin renal disease. I. A method for
assaying and classifying histopathologicchanges in renal disease.
Hum Pathol1970; 1 : 615630.
52. Azuma H, Nadeau K, Takada Met al. Cellular and molecular
predictors ofchronic renal dysfunction after initial
ischemia/reperfusion injury of a
single kidney. Transplantation 1997; 64: 190197.53. Azuma H,
Nadeau K, Takada Met al. Initial ischemia/reperfusion
injuryinfluences late functional and structural changes in the
kidney.TransplantProc 1997; 29: 15281529.
54. Liu KD, Glidden DV, Eisner MDet al.Predictive and
pathogenetic value ofplasma biomarkers for acute kidney injury in
patients with acute lunginjury*. Crit Care Med2007;
35:27552761.
55. Devarajan P. Update on mechanisms of ischemic acute kidney
injury.J Am Soc Nephrol2006; 17: 15031520.
56. Leelahavanichkul A, Huang Y, Hu Xet al.Chronic kidney
disease worsenssepsis and sepsis-induced acute kidney injury by
releasing high mobilitygroup box protein-1. Kidney Int2011; 80:
11981211.
57. Bonventre JV, Weinberg JM. Recent advances in the
pathophysiology ofischemic acute renal failure.J Am Soc
Nephrol2003; 14: 21992210.
58. Jang HR, Rabb H. The innate immune response in ischemic
acute kidneyinjury. Clin Immunol2009; 130: 4150.
Kidney International(2012) 82 , 516524 523
LS Chawla and PL Kimmel: Acute kidney injury and chronic kidney
disease m i n i r e v i e w
-
7/25/2019 AKI n CKD an Integrated Clinical Syndrome
9/9
59. Castano AP, Lin SL, Surowy T et al. Serum amyloid P inhibits
fibrosisthrough Fc gamma R-dependent monocyte-macrophage
regulationin vivo. Sci Transl Med2009; 1: 5ra13.
60. Nath KA. Tubulointerstitial changes as a major determinant
in theprogression of renal damage.Am J Kidney Dis 1992; 20:
117.
61. Bohle A, von Gise H, Mackensen-Haen Set al. The obliteration
of thepostglomerular capillaries and its influence upon the
function of bothglomeruli and tubuli. Functional interpretation of
morphologic findings.Klinische Wochenschrift1981; 59: 10431051.
62. Finn WF. Enhanced recovery from postischemic acute renal
failure.Micropuncture studies in the rat.Circ Res 1980; 46:
440448.63. Yang L, Besschetnova TY, Brooks CRet al.Epithelial cell
cycle arrest in G2/
M mediates kidney fibrosis after injury. Nat Med2010;16: 535543
531pfollowing 143.
64. Basile DP, Friedrich JL, Spahic Jet al. Impaired endothelial
proliferationand mesenchymal transition contribute to vascular
rarefactionfollowing acute kidney injury. Am J Physiol Renal
Physiol2011; 300:F721F733.
65. Basile DP, Donohoe D, Roethe Ket al. Renal ischemic injury
results inpermanent damage to peritubular capillaries and
influences long-termfunction. Am J Physiol Renal Physiol2001; 281:
F887F899.
66. Yuan HT, Li XZ, Pitera JEet al.Peritubular capillary loss
after mouse acutenephrotoxicity correlates with down-regulation of
vascular endothelialgrowth factor-A and hypoxia-inducible factor-1
alpha. Am J Pathol2003;163: 22892301.
67. O0Riordan E, Mendelev N, Patschan S et al. Chronic NOS
inhibition
actuates endothelial-mesenchymal transformation.Am J Physiol
HeartCirc Physiol2007; 292: H285H294.
68. Horbelt M, Lee SY, Mang HEet al. Acute and chronic
microvascularalterations in a mouse model of ischemic acute kidney
injury. Am J PhysiolRenal Physiol2007; 293: F688F695.
69. Bechtel W, McGoohan S, Zeisberg EMet al. Methylation
determinesfibroblast activation and fibrogenesis in the kidney.Nat
Med2010; 16:544550.
70. Bonventre JV. Dedifferentiation and proliferation of
surviving epithelialcells in acute renal failure.J Am Soc
Nephrol2003; 14Suppl 1: S55S61.
71. Price PM, Safirstein RL, Megyesi J. The cell cycle and acute
kidney injury.Kidney Int2009; 76: 604613.
72. Hodeify R, Tarcsafalvi A, Megyesi Jet al.Cdk2-dependent
phosphorylationof p21 regulates the role of Cdk2 in cisplatin
cytotoxicity. Am J PhysiolRenal Physiol2011; 300: F1171F1179.
73. Megyesi J, Price PM, Tamayo Eet al. The lack of a functional
p21(WAF1/CIP1) gene ameliorates progression to chronic renal
failure.Proc Natl
Acad Sci USA1999; 96: 1083010835.74. Wynn TA. Fibrosis under
arrest.Nat Med2010;16: 523525.75. Bechtel W, McGoohan S, Zeisberg
EMet al.Methylation determines fibroblast
activation and fibrogenesis in the kidney. Nat Med2010; 16:
544550.76. Megyesi J, Udvarhelyi N, Safirstein RLet al. The
p53-independent
activation of transcription of p21 WAF1/CIP1/SDI1 after acute
renalfailure. Am J Physiol1996; 271: F1211F1216.
77. Srisawat N, Murugan R, Lee Met al. Plasma neutrophil
gelatinase-associated lipocalin predicts recovery from acute kidney
injury followingcommunity-acquired pneumonia. Kidney Int2011; 80:
545552.
78. Lassnigg A, Schmidlin D, Mouhieddine Met al. Minimal
changesof serum creatinine predict prognosis in patients after
cardiothoracicsurgery: a prospective cohort study.J Am Soc
Nephrol2004; 15:15971605.
79. Chertow GM, Burdick E, Honour Met al. Acute kidney injury,
mortality,length of stay, and costs in hospitalized patients. J Am
Soc Nephrol2005;16: 33653370.
80. Anderson S, Eldadah B, Halter JBet al.Acute kidney injury in
older adults.J Am Soc Nephrol2011; 22: 2838.
81. Go AS, Parikh CR, Ikizler TA et al. The assessment, serial
evaluation, andsubsequent sequelae of acute kidney injury
(ASSESS-AKI) study: designand methods.BMC Nephrol2010; 11: 22.
82. USRDS Annual Report 2007 Department of Health and Human
Services,NIDDK, United States Renal Data System (USRDS) (NIH
publication no07-3176)2007; 1: 240241.
524 Kidney International(2012) 82 , 516524
m i n i r e v i e w LS Chawla and PL Kimmel: Acute kidney injury
and chronic kidney disease

















![Research Paper Klotho alleviates indoxyl sulfate-induced ......Chronic kidney disease (CKD) and acute kidney injury (AKI) have a high global prevalence and economic burden [1]. CKD](https://img.pdfslide.us/doc/110x75/607b01e843e06476762fc28a/research-paper-klotho-alleviates-indoxyl-sulfate-induced-chronic-kidney.jpg)