-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
1/8
AIRWAY MANAGEMENT DURINGCARDIOPULMONARY RESUSCITATIONIN
FILIPINOS: A NEW PERSPECTIVE
Ma. Minerva Patawaran-Calimag. M.D.*Julieta Canlas-Paiarillo,
M.D. *
Endotracheal intubation may be a life saving procedure. In fact
it remains the method of choice in maintaining an airway in
advanced cardiac life support . Indeed, the cuffed tracheal tube
has proven i tsel f to be aninvaluable tool during cardiopulmonary
resuscitation.In the hands of the inexperienced, however, it can be
aharbinger of disaster. The choice of the correct size andtype of
tube is only one aspect in the management ofthe compromised airway.
The length of the airway isas lmportant in so far as ignorance of
this fact can leadto inadvertent endobronchial intubation with
consequenthypoxemia. This study therefore aims to establish
standards for determining tracheal tube length in Filipinoadults
with the use of several anthroprometric data. Afterstudying
ninety-eight randomly selected Filipino adults,the following
conclusions were reached: I) The average'optimal orotracheal tube
length were 22.13 ern,.SD1.02 cm for males and 21.17 em, SD1.74 ern
forfemales; 2) There are significant statistical
correlationsbetween optimal orotracheal tube length and the
considered factors, namely height, cricoid to xiphoid tipdistance
and length of the third finger; 3) The maximumsafe length of
orotracheal tube in adult Filipinos can bepredicted as follows:
Orotracheal tube - cricoid toxiphoid distance minus 2 ern, or three
times the lengthof the third fmger minus I em. Nasotracheal tube
cricoid to xiphoid tip distance, or three times thelength of the
third fmger plus I ern.In the last quarter of the century, advances
in thebasic understanding, techniques, teaching and practiceof
cardiopulmonary resuscitation have resulted insaving countless
lives. Initial measures to establishartificial ventilation and
circulation are the same, whether performed by physicians or lay
rescuers, andwhether performed in a hospital or in any other
locations.In most instances, respiration stops before circulation.
Since any other measures will be ineffective inthe absence of
pulmonary ventilation, respirationshould always be checked.
first.Because of the difficulties, delays and cornplications in the
proper placement of an endotracheal tube,its use during
cardiopulmonary resuscitation is restric-ted mainly to medical
personnel or professional healthpersonnel who are highly trained in
the said procedure."Santo Tomas University Hospital. Section of
Anesthesia,Division of SurgeryJMMSI Vol. XXII No.4-6
April-8eptember, 1986
Even among the experienced, misconceptions stillabound as to the
choice of the proper type, size andlength of the endotracheal tube
to use in a given patient.Ignorance of important anatomical
considerationscan lead to immediate or delayed complications.
TheNational Conference on Cardiopulmonary Resuscitation ani!
Cardiac Care (1979)1 in affirming the recommendations set forth by
its Steering Committee in
19742 has stated that 8.0-8.5 mm LD. endotrachealtubes be used
for women and 8.5-9.0 mm LD. tubes formen. Since then, several
foreign authors have shownevidence that the above recommendations
are too largein many cases even for Caucastans.' Standards of
sub-glottic and tracheal diameters have been set by one ofthe
authors in two previous s t u d i e s . 4 ~ The choice ofthe
correct size and type of endotracheal tube, however, is only one
aspect in the management of thecompromised airway. The length of
the airway from theteeth or nose through the mouth, pharynx and
finallyinto the trachea has likewise been discussed in foreignl
iterature but no mention of it has yet been publishedin the local
literature.In an attempt therefore to set standards of endotracheal
tube length among Filipinos, this s tudy wasundertaken aimed at
estimating the distances from
the base of the nose, or from the upper anterior incisorteeth to
just above the carina.The data on Filipino subglottio- and tracheal
diameters and their anatomic correlates previously reported4,s will
also be reproduced here to point outpossible dimensional
interrelationships of the upper
airway. Aside from pure anthropometry, such inform-ation has
potential applications to studies in pulrnonary resuscitative
physiology and anesthesiology. Ifcertain critical dimensions and
their interrelationshipsare known, and further if they can be used
as a basisof prediction, many problems in the areas mentionedcan be
more precisely defined for study. Of course,there is a certain
general interest in the knowledge ofmeasurements of the human body
for its own sake.MATERIALS ANDMETHODS'The data for this study were
obtained from ninetyeight randomly selected adult patients
scheduled foroperation under general anesthesia via the
orotrachealor nasotracheal route at the Santo Tomas University
109
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
2/8
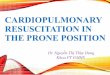
FIG. I. Number of subjects by gender and age group.
TABLE I. Summary of th e data for Filipino subjects (N '"
981.
so
MEAN AGE - 35.7 vrs.,SO 14.6 VI'S.\ ,\\\
___ males_femalet
D 1 subject
40 00Age (years I
t,o \I 'o \I \
20
4
2
B
'0
"0 B
RESULTSFigure I depicts the number of subjects by genderand age
group. The age range was 15 to 78 years with anoverall mean age of
35.7 years, SD14.6 years. A summary of the data and measurements
obtained on 98Filipino adults are presented OnTable l.The mean
optimal orotracheal tube length were 22.13ems, SD1.02 ems for the
male subjects, and 21.17 ems,SD1.74 ems for the female
subjects.
males and females separately. Regression lines werederived using
the least squares method.P:7To determine what effect advanced age
might have onthe observed differences between the distance from
thesuperior border of the cricoid cartilage to the ti p of
thexiphoid process and the orocarinal distance, data forsubjects
aged 50 and below Were compared with thosefrom 51 years old and
over. Student's "T" test was used.For all statistical analysis a p
value less than 0.0 I was
considered significant.
Number Numt.r., ..Subj""rs Me.., S,D, Subjeo:u "I n S.D.
AgIt tv.. rtl " 36.69 1!d Clnllage10 Xiphoid TipObllnee (em) "
24.15 0.99 ee 22-1ll I 1,32Length 01the 7.73 0.45iddle Finger lem)
ea es 7 .40 0.42OptlmelOrotrach.lTw e Llngth (eml .. 22.13 1.02 eo
21.11 1,74OpdmllNlIOtrach...1Tube Length (em) , 26.80 0.11 , 25.32
0.30
Hospital , Clinical Division, from February to March,1985.The
study included fifty-two males and forty-sixfemales.All
measurements were made with the patient lyingsupine on the
operating table with the head in theneutral position. Before in
tubation, the followingparameters were determined: height, cricoid
to xiphoiddistance and length of the third finger. Measurementswere
made to the nearest 0.5 em.Cricoid to xiphoid distance was measured
along thebody surface from the superior border of the
cricoidcartilage to the tip of the xiphoid process, using
ameasuring tape.
Third finger length was measured on the palmarsurface of the
hand from the metacarpophalangeal jointcrease to the finger
tip.Prior to intuba tion , the endotracheal tube and itscuff were
checked for defects. The tube is then lubricated with lidocaine
jelly. Patients were preoxygenatedand general anesthesia induced
with thiopental sodium,3-5 mgs/kg BW intravenously. After loss of
eyelid reflex, 1-2 mgs/kg BW of succinylcholine is administeredto
facilitate intubat ion. Intubat ion was then carriedou t with the
appropr ia te size of tracheal tube.' Deliberate endobronchial
intubation was done after whichthe tube was gradually withdrawn unt
il breath soundsare equal in all areas of the lungfields. The cuff
is theninflated to minimal occlusive (i.e. that cuff volumewhich is
needed to produce an airtight seal betweentrachea and cuff).
The level of the tube was verified further by performing the
following maneuvers: I) constant pressure isapplied to the pilot
balloon of the inflated cuff by theindex finger and the thumb of
one hand, while the otherhand palpates the trachea between the
cricothyroidcartilage and the suprasternal notch, where a
distinctincrease in pressure could be felt over the inflated
cuff;2) injecting one milliliter of sterile saline into the
pilotballoon and the balloon compressed and released gentlybetween
the fingers and auscultating for the presenceof crepitus over the
suprasternal notch at the approximate level of the cuff.These
maneuvers indicate that the cuff of the endotracheal tube is
located below the vocal cords and severalcentimeters above the
carina. Added documentation isacquired in those patients requiring
chest x-ray postoperatively, showing the exact position of the tip
of theendotracheal tube with the head in neutral posit ion. .Being
satisfied with the position of the tube an oralairway is inserted
and the tube fixed into position bymeans of adhesive tape. The
depth of tube insertion isdetermined by the centimeter markings on
the tube atthe level of the upper incisors, or in edentulous
patientsat the external surface of the upper gums. The lengthof the
tube is then compared with the various anthropometric measurements
obtained, i.e, height, thirdfinger length and cricoid cartilage to
xiphoid tilldistance.Statistical analysis were done using the
Pearsonproduct moment correlation coefficient matrices. Arnatix was
computed for the entire popula tion and for110 JMMSI Vol. XXII No.
4-5 April-September. 1986
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
3/8
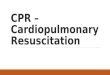
FIG. 3. Correlations and regressions of orotraeheal tube
lengthwith cricoid cartilage to xiphoid tip distance.
Figure 3 illustrates the opt imal tube length versuscricoid to
xiphoid process distance for each of the subjects. The regression
line for the entire population(N=84) was expressed by the equat ion
Y = O.969X-1.42. The equations Y =O.706X +4.80 and Y=O.994X- 1.84
represented the regression lines for male andfemale subjects,
respectively.
2642
REGRESSIONS
Cricoid - Xiphoid O!ltllnce
-- all melesand ferrel" IN 84)males IN -44)- ~ - females IN .
40)
20
o male.o females
18
28
18
24~} 22
..l 20!
Correlative and Predictive Factors of Optimal Endotracheal Tube
Length.
Age. Age had a very low correlation with optimaltube length.
When data from subjects aged 50 and belowwere compared with data
from those aged 50 and overusing the Student's 'T' test, the p
value obtained was notsignificant (p value> 0.50).Sex. There was
a highly significant level of correlation between sex and optimal
orotracheal tube length.Female subjects were shorter and required
shortercodertracheal tubes than theirmalecounterparts.Height. The
mean height for males was 160 .70 ems,SO5.87 ems (63.27 inches,
SO2.3 inches), and forfemales, 155.62 ems, S06.54 ems (61.27
inches,SO2.57 inches) . A significant correlation was foundwhen the
optimal tube length was compared with theheight. When broken down
by sex however, the correlation was better for males than for
females.Third "Inger Length The length of the middle
fingercorrelated wei! with optimal tube length. The orotracheallube
length was usually less than three times the lengthof the middle
finger in centimeters.The mean differencewas 0.5 em in malesand 0.9
em in females.
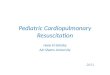
Figure 2 plots the optimal tube length versus thirdfinger length
for each of the subjects. The regressionline for the ent ire
populat ion (N=84) was expressed bythe equat ion Y = 1.75X + 8.2.
Regression lines wereplotted separately for male subjects (Y =
1.58X + 9.67)and female subjects (Y = 1.65X + 8.7).FIG. 2.
Correlations and regressions of crorrecheat tube lengthwith length
of the middle finger.
26
24
22
20
maleso females
REGRESSIONS-- all malesand femllleilN - 84).... - - males IN
-44)-.- females (N . 40)
The correlation coefficients and the levels of significance
between optimal endotracheal tube length and thevarious
anthropometric measurements considered arelisted in Tables II and
III.Because of the scarcity of patients subjected to naso-tracheal
intubation during the study period, no significant s ta tist ical
analysis can be done. Inspect ion of thedata obtained, however,
revealed that on the average,nasotracheal tube length approximate
the cricoid car-tilage to xiphoid tip distance.
TABLE II . Correlations of considered factors with
oPtImalorotracheal tube length in 84 Filipino adults.
Cricoid Cartilage to Xiphoid Tip Distance. The meandistance from
the superior border of the cricoid cartilageto the x iphoid process
for the male subjects was 24.15ems. SD 0.99 ems, and for the female
subjects, 22.98ems, SO1.32 ems.The orotracheal tube length was
usually less than thedistance from the cricoid cartilage to the tip
of theXiphoid process. The mean differences was 2.5 ems inmales and
2.0 ems. in females.JMMSI Vol . XXII No. 4-5
AprilSeptember.1986
Middlo Finger Length fern)
'8
6.5 7.0 7.5 8.0 8.5
Orotrachealtub81ength
Age O . ~Height 0.300
Length of Middle Finger 0.860"
Cricoid Cartilage toXiphoid TIp Distance 0.974Up value ( 0.001,
highly 5.lgntficant"p value ( 0.01, significant
111
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
4/8
TABLE III. Correlations of ~ o n s i d e r e d factors with
optimalorotracheal tube length in Fi lipino male (N = 44 ) and
femaleIN =40 ) subjects.
OrotrachealMALES tube length
Height 0.783-Length of Middle Finger 0.863'Crjcoid Cartilage
toXiphoid Tip Distance 0.779'
OrotracheatFEMALES tube length
Height 0.580'Length of Middle Finger 0.575'Cricoid Cartilage
toXiphoid Tip Distance 0.987-
"p value ( 0.001, highly significant
DISCUSSIONOpening the airway and restoring breathing are
thefirst steps in artificial ventilation during cardiopulmonary
resuscitation. Oxygenation of the lungs by simpleairway adjuncts
should precede attempts at trachealintubation." Adequate lung
inflations interposed between external chest compressions require
high pharyngeal pressures. This factor promotes gastric
distentionwhich elevates the diaphragm and interferes with adequate
lung inflation. Gastric distention likewise promotes regurgitation
with the potential hazard of aspiration of gastric contents into
the lungs. Therefore, assoon as is practical, the trachea should be
intubated.This isolates the airway, diminishes the chances
ofaspiration and ensures the entry of a high concentrationof oxygen
to the lungs. With a cuffed endotracheallube. it is easier to
provide adequate ventilation duringcardiopulmonary resuscitation
than with mouth-tomouth, mouth-to-mask, or bag-valve-mask
technique,The indications for endotracheal intubation includethe
following: I) inability of the rescuer to ventilate theunconscious
patient with conventional methods, 2)inability of the patient to
protect his own airway(coma,areflexia), or 3) the need for
prolonged artificial ventilation.'Indeed, the cuffed endotracheal
tube has proven itself to be an invaluable tool during
cardiopulmonary reo
suscitation. In the hands of the inexperienced and the
uninitiated, however, it can be a harbinger of disaster evenas soon
as the choice of a specific type and size of endotracheal tube
ismade.Many authors have reported on the complications
ofendotracheal i n t u b a t i o n . ~ 1 O , 1 I 1 2 , 1 3 , 1 4
Too large a tubecan result in pressure necrosis most especially in
thesubglottic region. The cricoid cartilage surroundingcompletely
the subglottic region forestalls any externalexpansion of the
swollen surfaces which can only expandinternally, giving rise to a
dangerous airway obstruction.The cuff On the endotracheal tube
poses yet anotherproblem. The high pressure, low volume cuffs
havebeen
112
unequivocally implicated as the cause of pressure neerosis in
the trachea. During prolonged intubation, however, a discrepancy
between tracheal size and endotracheal cuff size may result in
increased trachealdamage even with the use of low pressure, high
volumecuffs. Damage can Occur due to overinflation causingexcessive
lateral tracheal wall pressure herniation of theredundant cuff over
the end of the tubed Or actualcollapse of the endotracheal tube
lumen with consequent airway obstruction. Underinflation of too
largea CUff, on the other hand, can displace the tip of thetube
towards one side of the trachea especially in noncircular tracheas
wherein they cause noncircumferentialerosions. At times, floppy
cuffs may be thrown intodouble folds, thus allowing aspiration by
the channelingof liquids through the folds. This is especially true
ofcuffs with thickness of more than 0.1 rum.18Aside from the
problems associated with the externaldiameter of the tube and the
cuff; another dreadedcomplication that can arise following
intubation is theinadvertent insertion of the tube down to the
levelof the carina or eveninto a mainstem bronchus. Often,an
"airway" and ventilation. are established underemergency conditions
by an efficient well-informedteam which disperses when the
emergency is over. Whilethis team may be familiar with the
complications.ofintubation - ventilation, those charged with
subsequentcare of the patient are commonly less so. Or with
ventilation apparently well controlled, attention may bediverted to
other acute problems of the patient's care.When respiratory
distress recurs some hours later, therole of the airway itself in
producing the symptomsmay not be recognized. Endobronchial
intubation oftencauses amoreorlesscompletetermination of
ventilationin the opposite lung which is thus converted into agreat
shunt unit. The shunting of venous blood throughthe poorly
ventilated or nonventilated lung results insevere hypoxemia. When
imposed on a serious cardiopulmonary dysfunction, time is of the
essence and anydelays may lead to rapid deterioration and death.
Accidental right mainstem bronchus intubation has beenimplicated as
a cause of respiratory distress in about1025% of intubated
patients. Complications notedwere left-sided atelectasis,19
,20,21,22 right-sidedtensionpneumothorax, or right upper lobe
atelectasis.23The tube may go down into a bronchus as a resultof
the weight of the attachments or from frequentsuctioning if the
tube is not firmly anchored. Also,change in the position during the
emergency periodcan cause the tube to move up or down in the
trachea.It has been demonstrated that after an accurateintubation
of a patient in the supine position, a changeto the Trendelenburg
tilt will result into an upwardshift of the carina with impairment
of left lung ventilation. 24 Conrardy et a125 has shown that even
flexionof the head may cause the tip of the tracheal tube tomove an
average of 1.9 em. towards the carina, whileextension of the head
may cause it to move 1.9 em.away from tlie carina, i.e., regardless
of the route ofintubation (oral vs. nasal).Conversely, failure to
place the tracheal tube severalcentimeters beyond the vocal cords
may result ninadvertent extubation, vocal cord paralysis,
laryngo-
JMMSI Vol. XXII No.4-6 April-September, 1986
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
5/8
spasm and aspiration pneumonia. 9 , 24 , 2 5Determining proper
tube location has been the subject of many thesis in the past.
Among the recorn
mended maneuvers include I) placement of the endotracheal tube-
under direct vision I to 2 ern. below thevocal cords.?" 2)
confirmation by auscultation forequality uf breath sounds in all
areas of the lungfields,273) technique of deliberate endobronchial
intubationwith gradual withdrawal of the tube to 1 to 2 em. beyound
the point at which breath sounds are bilaterallycqual,27 4) rapid
inflation and deflation of the cuffwith palpation for a change in
pressure on the tracheajust above the suprasternal notch,'S ,'9 ,30
5) applyinga constant pressure to the pilot balloon of the
inflatedcu ff by the index finger and the thumb while the tracheais
palpated,'S 6) injecting one I ml of sterile saline intothe
partially inflated pilot balloon and listening forcrepitus at the
level of the cuff in the trachea while thepilot balloon is being c
0 " i ~ r e s s e d between the fingers,307) chest roentgenogram, ,
) j 8) using an eletromagnetic sensing device,32 9) detecting for
chanfes in endtidal CO, by continuous mass spectrometry. 3 Some
ofthese methods, however, are either complicated, inconvenient,
expensive, invasive and impratical. In essencetherefore, it appears
beneficial to utilize a combinationof common sense with simple
methods to verify properpositioning of an endotracheal tube. The
only ult imateguarantee of proper tube placement is the chest
roentgenogram and whenever doubt exists, it should berequested. The
maximum safe insertion of a tube inadults should not exceed beyond
T, leveL"
In this world where nature creates nothing to a standard size.
man since the earliest time has used his own
body as the basis for measurements. From hereon, theconcept of
anatomic correlates and anthropometricmeasurements have evolved and
the orocarinal andnasocarinal distances in man is no except ion.
Severalauthors have noted the "correct" length of orotrachealand
nasotracheal tubes to use in infants and children,34 ,35
,36.37,38,39,40,41 and in adults.42 ,4 3As early as 1907, Jackson
has reported the straightline distance from the upper anterior
teeth to thecarina measured along a bronchoscope to be 27 em.in men
and 23 em. in women. Hewer reported thepathway of inspired gas from
the anterior teeth to thecarina to be 26 em. in length. Gillespie,
in 1948, suggested that the length of an endotracheal tube
beselected by placing the tube alongside the patient'sneck whereby
its tip should not extend beyoml theangle of Louis, the anatomical
landmark for the bifurcation of the trachea/"Schellinger, in 1964,
determined airway length to thebifurcation of the trachea on
patients for autopsy.He has noted a positive correlation between
the distancefrom the superior border of the cricoid cartilage to
the
tip of the xiphoid process with the orocarinal distance.Whereas
the diameter of the criooid and the tracheacan be redicted accurate
ly in fresh cadaver specimens3,', the same cannot be said of
tracheal length.The trachea appears to . be longer in life than at
postmortem, mainly because of the elastic recoil of the diaphragm
making interpretation of these data difficult.Fearon and Whalen's
study 3S with living subjects (1965)demonstrated the unreliabili ty
of data obtained incadavers.
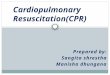
FIG. 4. An algorithm for airway management In the acutely
injured patient.
i -ICAlCOTHYFlOlDOTOMylIi
r,,!i,I....,,-,....
I'\e NASOTRACH'"- INTU8ATION
:::7::' -6- BAO MASK CWvIQl /\ l E N ~ r L A T I O N --.
.pl....a/T \Ia.::-:. -61 -L -_ "" : ' : ' : " : " ' . J - ,, ,.. -
- - - =.::.. _19_
SUPPLEMENTALOXYGEN
Trwchal tr- .ct lonorHYlfW anteriorInjury
X"-Vttudl.. Qlal nlm c.rvk:IlqoIne
- ....o'll'\IuryIo I.e.... 01 conad ........o
V.nllinianoO"Y....1ono Aff-.r _ _ I or
Imrni...nl
I TRACHEOSTOMY IJMMSI Vol. XXII No. 4-6 April-September, 1986
113
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
6/8
FIG. 5, Factors to consider In airway management of the acutely
injured F il ipino patient.
o Cricoid to Jdphofddi$unaJncm..
taller then 160 em(5'3'" - - - '. 0 mm 1.0.
BuIld onheight end "
Ieller Ihlln 145 em 14'9", 6.5 mm I.D.shorter then 145 em 14'9'"
--- B.Omm I.D.
shorter then 160 em 15'3'" 6.5 mm 1.0.
Bned on Lllnglh of the Third Finger
USEAPPROPRIATE SIZEOFENOOTAACHEALTUBE
Mo'a
oLength of thi rd f inger Inem 1.0. of tutMl ln mm
ORAL ROUTEo Crl
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
7/8
limited since the chest is often blocked by other resuscitators
applying external chest compressions.In a previous study by one of
the authors,' it wasfound that the third finger length has a high
correlationwith the cricoid ring size, thus making it an
invaluablereference in the choice of the proper size of
endotracheal tube to use among Filipino adults. In an emergency,
the length of the third finger in centimeterscorresponds well to
the correc t tube size ( in ternal diameter) in millimeters, that a
tube may be selected onthat basis. For example, if the third finger
length is6.7 crn., then a 7 mm. internal diameter endotrachealtube
should be used. In the present study, an attemptwas made to
correlate this anthropometric measure-men t with the optimal
orotracheal tube length. Theresults indicate that when one
centimeter is subtractedfrom the product of three times the length
of the thirdflnger, the value obtained corresponds well to theopt
imal orot racheal tube depth calculated for eachpatient.CONCLUSIONS
AND RECOMMENDAnONSOn the basis of the foregoing data; we can
thereforeconclude that a significant statistical correlation
wasobtained between optimal orotracheal tube length andthe
considered anthropometric measurements namely,height, cricoid to
xiphoid distance and the length of
the third finger, thus making them good predictorsof airway
length in Filipino adults. The maximum safelength for endotracheal
tubes in Filipino adults are asfollows:
Orotracheal tube:a) Cricoid to xiphoid distance (em) - 2 em.b)
(Third finger length in em x 3) - I em.
Nasotracheal tube:a) Cricoid to xiphoid distance in em.b) (Third
finger length in em x 3) + 1 em.Cognizant therefore of the
standards set forth in thisstudy and those of two previous studies
among Filipinos4,s a more rational approach to airway manage-ment
during cardiopulmonary resuscitation canbe done.
SUMMARYA method for the predetermination of the maximumsafe
length of orotracheal and nasotracheal tubes in Filipino adults is
presented.Correlations of such factors, i.e. age., sex, height.
cri-coid to xiphoid distance and third finger length withopt imal
orotracheal or nasotracheal tube length
werecomputed,andconclusionswere derived accordingly.A review of the
literature on the complications asso-
ciated with inadvertent endobronchial intubationwere presented
and the importance of predeterminationof the tube length in
prolonged intubation is crnphasized.REFERENCESI. AHA/NAS-NRC:
Standards and Guidelines forCardiopulmonary Resuscitation (CPR) and
Erner-
JMMSI Vol. XXII No. 4-5 AprilSeptember, 1986
gency Cardiac Care (ECe). JAMA 244 (5): 453-508,\980.
2. AHA/NAS-NRC: Standards for CardiopulmonaryResuscitation (CPR)
and Emergency Cardiac Care(ECe). JAMA 227 (Supp!) 833-868,
1974.
3. Koufman, JA, Fortson, JK, and Strong, MS: Predictive Factors
of Cricoid Ring Size in Adults in Relat ion to Acquired Subglottic
Stenosis. OtolaryngolHead Neck Surg. 91: 177-182,1983.
4. Patawaran-Calimag, MMV: Normative Data on Cricoid Ring Size
Among Adult Filipinos in Relationto Acquired Subglottic Stenosis.
Unpublished Thesispresented at the 19th Annual Convention of
thePhilippine Society of Anesthesiologists, December,1984.5.
Patawaran-Calimag,MMV:FilipinoTracheal Ci;cum
ferenceas an Index of Correct Cuff Size: A Studyon
Volume-Pressure Relationships in InflatableCuffs. Unpublished
Thesis presented at the 20thAnnual Convention of the Philippine
Society ofAnesthesiologists, December 1965.6. Rohlf', FJ and Sokal,
RR: Statistical Tables:W. H.Freeman and Co., San Francisco, 1969.7.
Sokal, RR, and Rohlf, FJ: Biometry: The Principlesand Practice of
Statistics in Biological Research.W.H. Freeman and Co., San
Francisco, 1969.8. Don Michael, TA: Comparison of the
EsophagealObturator 'Airway and Endotracheal lntubation
inPrehospital Ventilation during CPR. Chest 87 (6):
814-818,1985.9. Blanc, V. F. and Tremblay, NAG: The
Complications of Tracheal Intubation: A New Classificationwith a
Review of the Literature. Anes Analg 53:
202-214,1974.10. Bryce, D.P., Briant, TOR and Pearson, FG:
laryngeal and Tracheal Complications of Intubation.Ann 0101 Rhinol
Laryngol 77: 442-461,1968.I I . McGovern, FH, FitzHugh, GS, and
Edgemon, U:
The Hazards of Endotracheal Intubation. Ann 010180:
556-564,1971.
12. Peppard, SB and Dickens, JH: Laryngeal InjuryFollowing Short
Term Intubation. Ann Otol RhinolLaryngol92: 327-330,1983.13.
Stauffer , JB, Olson, DE and Petty , TL: Complications and
Consequences of Endotracheal Intubationand Tracheostomy. AmJMed70:
65-76,1981.14. Vogelhut, MM, Downs, JB: Prolonged
EndotrachealIntubation. Chest 76: 110-111, 1979.
15. Ching, NP, Ayres. SM, Paegle. RP, Linden. JM,115
-
7/27/2019 Airway Management During Cardiopulmonary Resuscitation
in Filipinos a New Perspective - Page 109
8/8
Nealon, TF: The Contribution of Cuff Volume andPressure in
Tracheostomy Tube Damage. J. ThoracCardiovasc Surg 62(3): 402-410,
1971.16. Dobrin, P, Canfield, T: Cuffed Endotracheal Tubes:Mucosal
Pressures and Tracheal Wall Blood How.
AmJ Surg 1333: 552568, 1977.17. Knowlson, GTG, Bassett, HFM: The
PressuresExerted on the Trachea by Endotracheal
InflatableCuffs.Dr.J Anesthesia 42:834-837,1970.18. Pavlin, EG,
vanNimwegan, D., Hornbein, TF: Failure of a High compliance, Low
Pressure Cuff toPrevent Aspiration. Anesthesiology 42(2):
216219,1975.19. Tisi, GM, Twigg, HL and Moser, KM: Collapse ofLeft
Lung Induced by Artificial Airway. Lancet. i :791, Apr 1968.
20. Hamilton, W. and Steven, W.: Malpositioning ofEndotracheal
Catheters.JAMA 198:1113, 1966.21. Alberti, J., Hanafa, W., Wilson,
G., et al: Unsuspected Pulmonary collapse during
NeuroradiologicProcedures Radiology 89:316320, 1967.22. Keane, WM,
Rowe, LD, Dennesy, JC and Atkins,JP: Complications of Intubation.
Ann Otol RhinalLaryngol91 :584.587,1982.23. Seta, K., Goto, H.,
Hacker, DC, Arakawa: RightUpper Lobe Atelectasis after- I n a ~ v e
r t e n t RightMain Bronchial Intubation. Anes Analg
62:851-854,1983.24. Heinonen, J., Tammisto, T., and Takki, S.:
Effect
of the Trendelenburg Tilt and Other Procedures onthe Position of
Endotracheal Tubes. Lancet 1:850,1969.25. Conrardy, P., Goodman,
L., Laing, F., Singer, M.:Alteration of Endotracheal Tube Position
- Flexionand Extension of the Neck Crit Care Med 4:8.12,1976.26.
Ripoll, I., Lindholm, CL, Carroll, R., and Grenwik,
A.: Spontaneous Dislocation of EndotrachealTubes. Anesthesiol49
:5052, 1978.27: Bendixen, HH, Egbert, LD, Hedley, et al.:
"TheAirway" Respiratory Care. St. Louis, C.V. Mosby,1965, pp
111121.28. Downes, JJ , Raphaely, R.C.: Pediatric IntensiveCare
AnesthesioI43:238250, 1975.29. Trincr. L : A Simple Maneuver to
Verify Proper
Positioning of An Endotracheal Tube.
Anesthesiol57(6):5489,1982.
30. Wallace, CT Cooke, JE: A New Method for Positioning
Endotracheal Tubes. Anesthesiol 44(3):272, 1976.31. Kopman, EA: A
Simple Method for Verifying
Endotracheal Tube Placement. Anes Analg 56(1):123-4,1977.32.
Cullen, OJ, Newbomer, RS ct al: A New Methodfor Positioning
Endotracheal Tubes. Anesthesiol43:596-599, 1975.33. Riley,
RH,Marcy, JH: Unsuspected EndobronchialIntubat ion - Detect ion by
Continuous MassSpectrometryAnesthesio163:203-4, 1985.34. Coldiron,
JS: Estimation of Nasotracheal TubeLength in Neonates. Pediatrics
41-823, 1968.35. Fearon, B., Whalen, JS: Tracheal Dimensions in
theLiving Infant Ann OtoI76:964, 1967.36. Kuhn, LR, Poznanskin, AK:
Endotracheal TubePosition in the Infant.JPediatrics 78:991,1971.37.
Leigh, DMand Belton,K.: PediatricAnesthesiology;ed 2 New York,
MacMillanCo" 1960, p. 208.38. Loew, A. and Thibeault, DW: A New and
SafeMethod to Control the Depth o f EndotrachealIntubation in
Neonates. Pediatrics 54:506, 1964.39. Mattila, MAK, Heikel, PE, et
al: Estimation o f aSuitable Nasotracheal Tube Length for
Infantsand Children. Acta Anaesthesiol Scand 15:239,1971.40.
Mcintyre, JWR: Endotracheal Tubes for Children.Anesthesia 12:94,
1957.41. Tochen, ML: Orotracheal In tubat ion in the New-
born Infant : A Method for Determining Depth o fTube Insertion.J
Pediattics 95:1050-1,1979.42. Saba, AK: The Estimation of the
Correct Length
o f Oral Endotracheal Tubes in Adults.
Anesthesia;32:919-920,1977.43. Schellinger, RH: The Length o f the
Airway to theBifurcation o f the Trachea. Anesthesiol
25:169,1964.44. Jackson-Rees: A Technique o f Pulmonary Yentilation
with a Nasotracheal Tube. Dr J Anesthesia
38:9016,1966.
116 JMMSI Vol. XXII No.4-6 April-September, 1986