-
8/7/2019 Airway Evaluation
1/26
CLINICAL REVIEW
Airway evaluation in obstructive sleep apnea
Boris A. Stuck*, Joachim T. Maurer
Department of Otorhinolaryngology, Head and Neck Surgery, Sleep
Disorders Center,
University Hospital Mannheim, 68135 Mannheim, Germany
KEYWORDSObstructive sleepapnea;Mueller maneuver;Sleep
endoscopy;Critical closingpressure;Upper airway;Imaging
Summary As the interest in sleep-disordered breathing has
increased, variousattempts have been made to assess upper airway
anatomy in patients with this rela-tively frequent disorder. The
aim is not only to reveal potential differences in upperairway
anatomy to better understand origin and pathophysiology of the
disease butalso to improve patient management and treatment
success. The present review isbased on a systematic literature
search with regard to upper airway evaluation insleep-disordered
breathing; the articles were selected and discussed in light ofour
clinical experiences. Based on clinical assessment including
endoscopy duringwakefulness, the value of the Mueller Maneuver,
static radiologic imaging tech-niques (X-ray cephalometry, computed
tomography (CT) scanning and magneticresonance imaging (MRI)),
dynamic scanning protocols (e.g. ultrafast CT or cine
MRI), upper airway endoscopy during sleep and sedated sleep,
pressure measure-ments and the assessment of the critical closing
pressure are discussed. Each tech-nique itself and its history in
the field of sleep medicine are briefly reviewed andproblems of
standardization and interpretation are discussed when
appropriate.Insights into the pathophysiology of the disease gained
with the help of the inves-tigational techniques are presented and
the impact of the techniques on patientmanagement is reported.
Although all these additional techniques for upper airwayassessment
have substantially improved our understanding of
sleep-disorderedbreathing, their significance in daily practice is
limited. In contrast to the wide-spread use of the Mueller maneuver
and sedated endoscopy, convincing data sup-porting their use in
terms of treatment outcome are lacking. So far, there is onlyvery
limited evidence that selected techniques improve treatment outcome
forselected indications. In general, there is not enough evidence
that these techniques
are superior to the routine clinical assessment. 2007 Elsevier
Ltd. All rights reserved.
Abbreviations: CT, computed tomography; MR, Magnetic resonance;
MRI, magnetic resonance imaging; PAS, posterior airwayspace; SNA,
angle from the sella to the nasion to the subspinal point; SNB,
angle from the sella to the nasion to the supramentalpoint; SDB,
sleep-disordered breathing; AHI, apneaehypopnea index; OSA,
obstructive sleep apnea.
* Corresponding author. Tel.: 49 621 383 3965; fax: 49 621 383
3827.E-mail address: [email protected](B.A.
Stuck).
1087-0792/$ - see front matter 2007 Elsevier Ltd. All rights
reserved.doi:10.1016/j.smrv.2007.08.009
Sleep Medicine Reviews (2008) 12, 411e436
www.elsevier.com/locate/smrv
mailto:[email protected]://www.elsevier.com/locate/smrvhttp://www.elsevier.com/locate/smrvmailto:[email protected]
-
8/7/2019 Airway Evaluation
2/26
Methods of airway evaluation
As the interest in sleep-disordered breathing (SDB)has
increased, various attempts have been made toassess upper airway
anatomy in patients with thisrelatively frequent disorder. From the
very begin-ning, researchers and clinicians used a multitude of
different techniques not only to reveal potentialdifferences in
upper airway anatomy to betterunderstand the origin and the
pathophysiology ofthe disease but also to improve patient
manage-ment and treatment success. While the value ofthorough
clinical assessment remains indubitable,the value of the Mueller
maneuver has been ques-tioned from the beginning. Static
radiologicimaging techniques such as X-ray cephalometry,computed
tomography (CT) scanning and magneticresonance imaging (MRI) have
been used mostly todetect differences in airway anatomy.
Dynamicscanning protocols (ultrafast CT or cine MRI e.g.)and
multiple pressure recordings have been used togain insights into
the mechanism and level ofairway obstruction. Upper airway
endoscopy hasbeen inaugurated during sleep and sedated sleep
todirectly visualize airway obstruction, and theassessment of
critical closing pressures has beenused to quantify upper airway
collapsibility.
The present review is based on a systematicliterature search in
the National Library of Medi-cine, textbooks, major journals in the
field ofsleep medicine and otorhinolaryngolgy, and addi-tional
personal sources of the authors. The articles
were selected and discussed in the light of ourclinical
experience.
The sections in this article are structured ina comparable
fashion. The technique itself and itshistory in the field of sleep
medicine are brieflyreviewed and problems of standardization
andinterpretation are discussed when appropriate.Potential
structural or functional differences inthe upper airway between
patients with SDB andhealthy controls are discussed and the
insights intothe pathophysiology of the disease gained with thehelp
of the investigational technique are pre-sented. Furthermore, the
impact of the techniqueon patient management is reported; finally,
theauthors summarize the overall potential and clin-ical usefulness
of the technique.
Clinical examination and clinical scores
A clinical examination including an endoscopy ofthe upper airway
during wakefulness still consti-tutes the basis of every airway
evaluation insnorers and obstructive sleep apnea (OSA)
patients. Given the early failures in the surgicaltreatment of
these patients, anatomic and staticfindings were the first
parameters to be evaluatedin order to improve treatment success.
The impactof enlarged palatine tonsils became evident in
thesurgical experiences with children. If performedsimultaneously,
tonsillectomy was described by
most authors as a positive predictive factor fora successful
UPPP,1e7 demonstrating a strongcorrelation between tonsil size and
success rate.8
This was also supported by studies investigatingsimple
tonsillectomy in OSA patients.9,10 All theother anatomic parameters
such as the size of theuvula, the existence of longitudinal
pharyngealfolds and so forth did not show any relationship tothe
success rate of UPPP if evaluated separately.11
In contrast to the significant influence of enlargedtonsils in
palatal obstruction, equivalent clinicalfinding for tongue base
obstructions could not bedetected. Woodson and Wooten12 only found
hints
that the oropharynx was normal in cases withretrolingual
obstruction.
Aware of this dilemma, Friedman et al.13e15
developed a clinical 4 degree staging systemincorporating the
tonsil size, the position of thesoft palate, the tongue size and
the body massindex (BMI). They reported a success rate of 80%after
a solitary UPPP with tonsillectomy in patientswith large tonsils,
visible posterior pharyngeal walland a BMI below 40 kg/m2 (defined
as stage 1).(According to our own experience these patientsare
rarely found among the group of typical OSA
patients.) If the tonsils were small or missing, thetongue was
rather large and the BMI was above40 kg/m2 (defined as stage 3),
Friedman et al.14
achieved a success rate of only 8%; it was improvedby a
simultaneous radiofrequency treatment of thetongue base in addition
to UPPP. Furthermore,their anatomical staging system predicted
thesuccess rate much better than OSA severitydid.16,17 Performing
UPPP with genioglossaladvancement on a series of 44 patients with
severeOSA, a study from Taiwan was not able todemonstrate a
similarly strong predictive value.But the results of this study are
problematicbecause almost every patient belonged to thesame
anatomical stage.18 One may argue that thestaging system merely
reflects the clinical exami-nation of an experienced sleep
physician; never-theless, such a system may be particularly
helpfulfor less experienced observers.
Whether there are further predictive anatomicparameters for
other surgical strategies has notbeen evaluated to date (except
those including theMueller maneuver which will be discussed
below).The subjectivity of the assessment and the
412 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
3/26
variability of the nomenclature of the clinicalfindings are a
significant limitation in this context.However, it has been shown
that this variabilitycan be reduced by using pictograms.19
The Mueller maneuver
Snoring as well as apneas can be simulated by mostpeople and a
direct effect of the Mueller maneuvermay be seen during
wakefulness. Thus, snoringsimulation and the effects of the Mueller
maneuverhave been used in upper airway evaluation beforesurgical
intervention in patients to predict surgicaloutcome and to improve
patient selection.20e22 Inaddition, the Mueller maneuver has been
per-formed to assess and predict postoperativechanges of the upper
airway,23e26 although thevalue of this relatively simple
examination hasbeen questioned repeatedly in the past.27
Techniques of the maneuver
In order to be able to compare results betweendifferent
investigators and patients as well asbefore and after an
intervention, the maneuvershould be performed and documented in a
stan-dardized fashion. Regarding the simulation ofsnoring, Herzog
et al.28 made a first attempt tostandardize snoring simulations
during wakeful-ness. They asked the patients to snore with
theirmouth open or during forced inspiration and used
a standardized documentation system which leadto a low
interrater variability. For the Muellermaneuver itself, the awake
patient is sitting orlying and inspiring maximally with nose and
mouthclosed while the pharynx is examined via a
flexibleendoscope.5,29e32 The endoscope is placed at thelevel of
the supraglottis, the uvula tip and thenasopharynx.
Due to its simplicity the classification accordingto Sher et
al.33 has been widely used. In thisclassification, 4 degrees of
airway obstruction atthe different levels are defined, ranging
fromminimal to complete occlusion. Furthermore, anyvisible
obstruction linked to the epiglottis isdescribed. Catalfumo et
al.34 described anepiglottic collapse that they found during
Muellermaneuver in 11.5% of UPPP failures. Fujita35 clas-sified
airway obstruction as isolated palatal (type1), isolated
retrolingual (type 2) or combined (type3) according to their
predominance. Terriset al.s36 study group integrated the collapse
ofthe lateral pharyngeal walls. He compared his ownresults of
airway evaluation using the Muellermaneuver with the results
obtained by one of his
residents. They found the same degree of collapsein one-third of
the patients. Allowing for thedifference of 1 according to the
classification ofSher as described above, both investigators
agreedupon the classification in 80% of their patients.However,
they found a difference of 3 in somecases. There was no systematic
error between
resident and specialist. Only Jager et al.
37
founda significant correlation of more than 0.8 betweenthe
degree of obstruction obtained by Muellermaneuver and MRI.
Recently, the problem of inter-investigatorvariability could be
eliminated by the quantita-tive, computer-assisted analysis of
digitizedendoscopic recordings of the maneuver.38e42 Horiet al.43
proposed a variation of the Muellermaneuver (sustained forced
transnasal inspirationwith the mouth closed) calling it the
Bernouillieffect producing maneuver. The significance ofthis
variation needs further evaluation.
Nevertheless, taking all the available data intoaccount, the
reliability of the Mueller maneuverremains highly questionable and
the evaluation ofthe maneuver seems highly subjective and hard
toreproduce.
Predicting airway obstruction during sleep
There is some evidence that the sites of obstruc-tion detected
with the Mueller maneuver do notreliably reflect the sites of
obstruction during
sleep. This could be demonstrated through acomparison with
videoendoscopy,12,44,45 multi-channel pressure recordings46 and
dynamic MRIduring sleep.47 Furthermore, several different sitesof
obstruction during sleep were documented thatcould not be
recognized with the Mueller maneuverduring wakefulness.46 Table 1
shows the differentsites of airway obstruction detected with
thedifferent methods of airway evaluation accordingto selected
examples from the literature.
The impact of body position on the significanceof the Mueller
maneuver also remains unclear.30,42
Some of our own (non-snoring) laboratory staff isable to produce
varying mechanisms and levels ofobstruction when performing the
Muellermaneuver. This active component of the Muellermaneuver is
confirmed by investigations concern-ing the critical closing
pressure which rangesbetween 10 and 17 mbar in healthy adultsduring
sleep.48 During the Mueller maneuver,healthy subjects may produce
extreme negativepressures of 80 mbar without any signs ofpharyngeal
collapse.42 This clearly demonstratesthe significant differences in
upper airway
Airway evaluation in obstructive sleep apnea 413
-
8/7/2019 Airway Evaluation
4/26
Table 1 Distribution of the sites of obstruction detected by
different methods of airway evaluation (selected literature
Method Author Diagnosis n Palatal Retrolingual Co
Mueller maneuver Petri et al.5 OSAS 30 8 0 22
Sher et al.33
OSAS 171 101 56 14Skatvedt46 SBAS 20 4 0 4
Sum (mean value %) 221 113 (51%) 56 (25%) 40
Endoscopy during sleep Launois et al.165 OSAS 18 11 2 5Woodson
and Wooten206 OSAS 11 5 6 n.d
Sum (Mean value %) 29 16 (55%) 8 (28%) 5 (
Endoscopy under sedation Croft and Pringle169 SBAS 56 25 n. d.
31Pringle and Croft177 SBAS 70 33 9 28Camilleri et al.184 SBAS 25
17 0 8Hessel and de Vries178 SBAS 340 111 8 22Steinhart et al.183
SBAS 306 139 23 13Den Herder et al.182 SBAS 127 65 15 47Quinn et
al.174 Snoring 50 35 4 5Marais173 Snoring 168 101 52 13El Badawey
et al.179 Snoring 46 8 2 36Abdullah et al.181 Snoring 30 12 0
18Abdullah et al.181 OSAS 89 12 4 71
Sum (mean value %) 1307 558 (43%) 117 (9%) 61
Pressure recordings during sleep Hudgel200 OSAS 9 4 5 0Chaban et
al.187 OSAS 10 5 5 0Metes et al.207 SBAS 51 30 7 n.dTvinnereim and
Miljeteig203 OSAS 12 6 2 n.dSkatvedt46 SBAS 20 2 5 10
Katsantonis et al.201 OSAS 20 5 4 9Woodson and Wooten206 OSAS 11
8 3 n.d
Sum (Mean value %) 133 60 (47%) 31 (23%) 19
SBASpatients with primary snoring or OSAS; OSASonly patients
with OSAS; palatalnasopharynx, tonsils, soft palate and/or lateral
pharynhypopharynx; epiglottisexclusively epiglottis; no
resulteither the method was not tolerated or the result was not
utilizable; n.d.not
-
8/7/2019 Airway Evaluation
5/26
collapsibility during wakefulness and sleep. All thedata given
do not support the idea that the resultsobtained by the Mueller
maneuver may be trans-ferred to natural sleep.
Predicting surgical success
It has to be questioned to what extent the Muellermaneuver can
predict surgical outcome. Variousresearch groups were not able to
better predictthe success rates obtained with UPPP when usingthe
Mueller maneuver.5,30,31,49 This was also truefor non-apneic
snorers.50 Recently, airway changesafter UPPP were first quantified
using the quanti-tative, computer-assisted analysis of
digitizedendoscopic recordings. Hsu et al.23 could demon-strate a
correlation between the postoperativeincrease of the retropalatal
area in the supineposition during the Mueller maneuver and
thedecrease of the AHI. Nevertheless, they did not
present data demonstrating that the surgicaloutcome of UPPP
could be predicted according totheir preoperative findings.23
Aboussouan et al.29 and Sher et al.51 consideredan additional
retrolingual collapse during theMueller maneuver as an exclusion
criterion fora UPPP because their success rate was only 5% inthese
cases. There is only one Chinese studyshowing a comparable success
rate for UPPP forpreoperative airway evaluation with the
Muellermaneuver and sleep endoscopy.52 Surgery of theepiglottis was
always considered and done sepa-
rately if it was seen during the Mueller maneuver.Catalfumo et
al.34 could reduce the apnea indexsignificantly in their
UPPP-failure patients withlaryngeal obstruction during the Mueller
maneuverby partial resection of the epiglottis.
Only Riley et al.21 report on the impact of usingselection
criteria based on the Mueller maneuverfor the combination of
different surgical proce-dures. In phase 1 of their protocol, an
isolated UPPwas only performed if the Mueller maneuver as wellas
cephalometry revealed an isolated retropalatalcollapse.21 In cases
of an isolated retrolingualcollapse in both examinations they
performed
a hyoid suspension and a genioglossal advance-ment. If there was
a combined collapse, all surgicalsteps were done simultaneously.
According to theirselection criteria, the authors found an
isolatedpalatal collapse in 10, an isolated retrolingualcollapse in
6 and a combined collapse in 223 (93%)of their patients. The
success rate of this protocolaveraged out at 61% which is higher
than Sheret al.51 found in their meta-analysis of isolatedUPPP
using Mueller maneuver, somnofluoroscopy orcephalometry (52%) or no
specific method (45%) for
airway evaluation. Rileys group did not providedata concerning
success rates without usingspecific selection criteria. Even though
theyincluded mainly patients with moderate to severeOSA, the
clinical relevance of the selection dis-cussed may be questioned as
patients with an iso-lated collapse of either palate or tongue base
seem
to be rare. This is stressed further by Vicenteet al.53 who
found a combined collapse in all 122OSA patients who rejected
CPAP.
Significance of the Mueller maneuver
The Mueller maneuver is a safe and simple exami-nation that does
not exert relevant strain on thepatient. The reliability of the
Mueller maneuver isinsufficient, but may be improved with the
imple-mentation of computer-aided evaluation tools.Nevertheless,
the results of the Mueller maneuver
cannot be transferred to natural sleep. A hypo-pharyngeal
collapse indicates the exclusion ofpatients from UPPP, thus
indirectly improving itssurgical success rate. Finally, the Mueller
maneuverdoes not facilitate patient selection for the
varyingsurgical interventions used in OSA patients.
X-ray cephalometry
Over the years, lateral X-ray cephalometry hasbecome one of the
standard diagnostic tools inpatients with SDB, especially with
regard to theevaluation of the skeletal craniofacial morphology.Not
specifically developed for the field of SDB,imaging techniques and
standards for data analysishave been incorporated from the field of
maxillo-facial surgery, where it has already been used
fordecades.
Being a standard tool for maxillofacial surgeonsand orthopedic
surgeons, one focus of X-ray ceph-alometry in SDB has always been
the assessment ofdentofacial characteristics before or after the
useof mandibular advancement devices or max-illomandibular
advancement surgery. The assess-
ment of potential differences in maxillofacial andupper airway
soft tissue anatomy has becomeanother focus for lateral X-ray
cephalometry.
Providing insights into the pathophysiologyof SDB
Comparing OSA patients with healthy controlsExtensive literature
is available comparing upperairway anatomy and dentofacial
structures usingX-ray cephalometry between OSA patients and
Airway evaluation in obstructive sleep apnea 415
-
8/7/2019 Airway Evaluation
6/26
healthy controls, both for obese and non-obesepatients as well
as for different ethnicities.
In a recent controlled study from Riha et al.,54
cephalometric characteristics of OSA patientswere compared with
those of their siblings. Theanalysis revealed a significantly
longer distancefrom the hyoid bone to the mandibular plane in
the
siblings affected by SDB (in addition, in dentatebrothers they
also found a shorter mandibularcorpus in OSA patients). While the
study designwas somewhat innovative by minimizing intra-individual
differences with the help of siblings, theresults confirmed those
of previous studies,particularly with regard to the significance
ofhyoid bone position.
Differences in craniofacial anatomy betweenOSA patients and
controls have been demonstratedby numerous other authors. The
concrete resultsare often difficult to compare, as the authors
oftennot only use different landmarks and parameters
but also sometimes rather complex calculatedindices and ratios
to describe the differences theyfound, therefore, the following
results can only bea selection of the data available.
Reporteddifferences were a longer soft palate,55,56 reducedminimum
palatal airway widths,55 increasedthickness of the soft
palate,56e59 differences ina calculated craniofacial score (the
sums of quar-tile points for distance from sella to nasion andfrom
hyoid bone to mandible),60 increasedpharyngeal length,56 a
retroposition of themandible59,61 or the maxilla,62,63
micrognathia,64
an increased mid-facial height,62
and differencesin hyoid bone position.56,57,61e66 Ingman et
al.67
reported no differences in naso- and hypophar-yngeal soft
tissues but a significant narrowing onthe velopharyngeal level.
Yu et al.61 demonstrated that the differenceswere more
pronounced in non-obese patients,concluding that craniofacial
changes play a domi-nant role in this subgroup. Ito et al.68 also
concludedthat the reported differences were morepronounced in the
non-obese group. Tangugsornet al.69 reported more pronounced
aberrations ofthe cervico-craniofacial skeletal in
non-obesepatients, while obese patients had more abnor-malities in
the upper airway soft tissue morphology,head posture and the
position of the hyoid bone.The predominant skeletal abnormalities
in non-obese patients compared to the predominant softtissue
aberrations in obese patients were alsoreported by Sakakibara et
al.70 in 1999 and byFerguson et al.71 in 1995.
Specific studies were performed with patientsfrom Asia, taking
the differences in maxillofacialappearance of this ethnic group
into account. Hsu
et al.72 used a modified technique of calibratedcephalometric
analysis by using a calibratedcatheter that was inserted into the
upper airwayto increase the accuracy of their measurements in106
south-east Asians. They could demonstratethat patients with OSA had
a longer lower-faciallength, a narrower skull base, a shorter
and
receding mandible, smaller posterior airwayspaces, a longer and
thicker soft palate, a longertongue length anddagaindmore
inferiorly dis-placed hyoid. According to Li et al.,73 the
morepronounced differences in craniofacial morphologyin Asians may
contribute to the fact that Asian OSApatients are often non-obese.
Cakirer et al.74
demonstrated that brachycephaly is associatedwith an increased
apneaehypopnea index (AHI) inwhites but not in African-Americans.
The reporteddifferences in craniofacial morphology betweendifferent
ethnic groups complicate the interpre-tation and the comparison of
cephalometric
studies.In addition to the use of a calibrated catheter as
described above, other modifications of cephalo-metric analysis
were used, such as cephalometryat the end-expiratory phase and
during the Muellermaneuver,25 but have not (yet) become a
routineprocedure.
Correlation to disease severityVarious authors have attempted to
correlate theirfindings in X-ray cephalometry with the severity
ofthe underlying SDB.
In a recent investigation, Hou et al.75
reportedthat the aberrations in craniofacial morphologythey
found in OSA patients (basically confirmingthe characteristics
mentioned above) were morepronounced in patients with severe OSA in
theirgroup of Chinese patients. Especially mandibularbody length,
craniofacial extension and sellaehyoid distance were predictive
variables for theAHI. Yucel et al.76 demonstrated that
differencesin hyoid bone position and a soft palate thicknesswere
more frequent in the subgroup of patientswith severe OSA. Other
authors, such as Bates andMcDonald,77 Kubota et al.,78 Naganuma et
al.32 andYoung et al.79 have confirmed the observation thatselected
anatomic variables were more prevalentin or predictive for severe
OSA, Young and McDo-nald79 again underlining the effects of hyoid
boneposition. Dempsey et al.80 demonstrated that innon-obese
patients and in patients with narrowupper airway dimensions, four
cephalometricdimensions were the dominant predictors of
AHI,accounting for 50% of the variance. Rose et al.81
question the diagnostic relevance of X-ray cepha-lometry for
OSA, as they found no direct
416 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
7/26
correlation between skeletal cephalometric find-ings and OSA
severity; nevertheless, they alsoreported a correlation with hyoid
bone position.
X-ray cephalometry and oral appliances
One of the dominant indications for performing X-
ray cephalometry has been the treatment with oralappliances.
Especially with regard to the evaluationof potential predictive
parameters for treatmentsuccess and dental side effects, X-ray
cephalom-etry has been the standard diagnostic tool.
As early as 1995, Mayer and Meier-Ewert,82 twoof the fathers of
the treatment with oral appli-ances in Europe, have looked for
cephalometricpredictors of treatment success. In a group of 30OSA
patients they reported that specific cephalo-metric variables were
indeed predictive for thetherapeutic effect, such as a narrow
oropharynx(posterior airway space (PAS) equal to or less than
3.4 mm), a narrow angle from the sella to thenasion to the
supramental point (SNB), a widerangle from the sella to the nasion
to the subspinalpoint (SNA) and a short uvula. Other authors
haveconfirmed the existence of predictive cephalo-metric
parameters, especially in relation to hyoidbone position and
oropharyngeal airway dimen-sion.83e87 A smaller airway on the
oropharyngeallevel is associated with good treatment
success.Nevertheless, the problems related to differentnomenclature
and selection of airway parametersdescribed above remain. Only
Battagel et al.88
reported no identifiable cephalometric features topredict
favorable response to the treatment.Although posttherapeutic follow
up is not part
of this review article, it should be mentioned thatX-ray
cephalometry has regularly been used toassess long term dental and
occlusal side effects oforal appliances.89e98
Evaluating the effects of therapeuticintervention
Predicting the results of UPPPX-ray cephalometry has also been
evaluated withregard to potential predictive parameters
forpostoperative results of UPPP alone or in combi-nation with
other approaches.
Liu et al.18 investigated UPPP in conjunctionwith genioglossus
advancement in a case series of44 patients and concluded that the
only predictiveparameter was the AHI. Boot et al.99 also could
notfind any cephalometric parameter predictingsuccess of UPPP. In
their retrospective study of 43patients with OSA, Woodson and
Conley100 alsocould not find a skeletal measurement predicting
the outcome of UPPP in the entire study group.Nevertheless, in
the subtype of patients withoutretrognathia, selected parameters
were predictiveof response.100 In addition to the AHI, the
absenceof retrognathia was another predictive parameterin a study
of Millman et al.101 in 2000. Doghramjiet al.30 also concluded that
a preoperative ceph-
alometry cannot be reliably used to predict orenhance surgical
success. Overall, the predictivevalue of X-ray cephalometry for
UPPP remains atleast questionable.
X-ray cephalometry and maxillofacial surgeryLateral X-ray
cephalometry is a standard tool in thepreoperative evaluation of
the craniofacial skel-etal anatomy before maxillomandibular
advance-ment surgery. It can be regarded as a mandatoryprocedure
and its value is not questioned.102
X-ray cephalometry in patient management
X-ray cephalometry has provided substantialinsights into the
pathophysiology of OSA, demon-strating significant craniofacial
characteristicsassociated with this disease. Although the
resultsare not easy to compare, specific
cephalometriccharacteristics have been repeatedly mentioned asa
risk factor for OSA, such as e.g., a thick and longsoft palate, a
retroposition of the maxilla ormandible and especially the more
inferiorly posi-tioned hyoid bone. Although there are
parametersthat correlate with the severity of the disease,
thenecessity of an assessment of the nature andseverity of the
disorder by nocturnal sleep testingremains. There are cephalometric
parameters thatare correlated with favorable results of
mandibularadvancement by oral appliances. Nevertheless, asno
cephalometric parameter exists that wouldreliably rule out
treatment success and as thetreatment is not invasive, at least the
authorswould routinely offer oral appliances for OSApatients as
long as the clinical examination (suffi-cient protrusion,
satisfactory dental status, limitedobesity) supports their use.
This may explain why X-
ray cephalometry has not become a routineprocedure in the
diagnostic work-up of OSA as longas maxillomandibular surgery is
not planned.
CT scanning
Compared to lateral X-ray cephalometry, CTscanning significantly
improves soft tissue contrastand allows precise measurements of
cross-sectional areas at different levels as well as
three-dimensional reconstruction and volumetric
Airway evaluation in obstructive sleep apnea 417
-
8/7/2019 Airway Evaluation
8/26
assessment. Fast scanning times and relativelyquiet scanning
conditions even allow a dynamicassessment of the airway during a
respiratory cycleas well as measurements during natural
sleep.Nevertheless, ionized radiation remains problem-atic and the
vast majority of the authors used CTdata merely for a structural
assessment during
wakefulness.
Techniques and standards
Despite its widespread use in airway assessment inpatients with
SDB, no standardized scanningprotocol exists for this indication
and the nomen-clature of the soft tissue structures is not
uniform.Each study group seems to apply its own scanningprotocol
and its own definition of the differentstructures described.
A first step was a two-dimensional assessment ofthe upper airway
of healthy controls and patients
with OSA, comparing two-dimensional structuressuch as soft
palate and tongue dimensions as well ascross-sectional areas.
Furthermore, 3D techniqueswere used to assess volumes of soft
tissue struc-tures and airway spaces.103e108 As early as
1987ultrafast or dynamic CTwas inaugurated in this fieldto evaluate
dynamic changes of the upper airwaydimensions during respiratory
cycles109,110 and wasfurther used in the following years.76,111e114
Whilethe vast majority used CT imaging during wakeful-ness, several
authors also used scanning protocolsunderhypnotic relaxation,115
sleep,110 sleep during
apneas110
and also used direct comparisonsbetween wakefulness and
sleep.109
Providing insights into the pathophysiologyof SDB
Comparing OSA patients with healthy controlsThe majority of
published data points to potentialdifferences in upper airway
structures anddimension between OSA patients and healthycontrols or
snorers. The various studies obtainedcomparable results. In
general, the upper airway isdescribed as smaller in apneic patients
compared
to controls,113 especially with regard to the ret-ropalatal
region.103 Cross-sectional areas werefound to be significantly
narrower in affectedpatients.116e118 Inversely, retropalatal tissue
wasdescribed as being greater in OSA patientscompared to
controls119 and larger tongue and softpalate dimensions and volumes
were found.59,120
Schwab et al.113 have pointed out the differencesin upper airway
configuration with an anterioreposterior configuration (in contrast
to the hori-zontal configuration in healthy subjects with the
major axis in the lateral direction)da result that isin line
with data obtained from MRI.
Correlation to disease severityDifferent authors have described
anatomic condi-tions that reflect the severity of the disease
andhave correlated their measurements with poly-somnographic data.
Lowe et al.59 reported that inhis group of 80 patients with OSA, a
high apneaindex was associated with large tongue and softpalate
volumes. In a study with three-dimensionalCT scan, a significant
correlation of the retro-palatal space and its lateral diameter
with therespiratory disturbance index was documented ina large
group of 194 patients with SDB.104 Voset al.108 used a combination
of the smallest cross-sectional area, the upper airway resistance
andthe BMI to predict the severity of OSA. In theirdynamic CT study
Yucel et al.76 described a nar-rower cross-sectional area and a
thicker soft
palate in severely affected patients compared topatients with
only mild-to-moderate OSA.
Mechanisms and sites of airway obstructionAvrahami et al.115
compared the cross-sectionalareas of 23 adult patients with severe
OSA in theawake state and during hypnotic relaxation.According to
the presented results, airways weresmaller during relaxation than
during wakefulness.With the help of dynamic and ultrafast CT,
furtherinsights into airway obstruction were gained. Inaddition to
the fact that the naso- and oropha-
ryngeal airways were smaller in OSA patientscompared to
weight-matched controls, Galvinet al.111 could show an increased
collapsibility inaffected patients compared to healthy
controls.During a respiratory cycle in 25 awake patientswith OSA,
substantial changes in cross-sectionalareas were seen in patients
with SDB, the velo-pharyngeal segment being the narrowest and
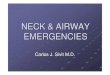
mostcollapsible region.114 These results were essen-tially
confirmed later, showing that patients withsevere OSA have
significantly narrower cross-sectional areas at the velopharyngeal
level76 (seeFigure 1).
Evaluating the effects of therapeuticintervention
Effects of therapeutic intervention have beenassessed with the
help of CT, mostly with regard tothe treatment with oral appliances
and surgicalintervention. Gale et al.121 investigated the
airwayenlargement achieved with an oral appliance in 32OSA
patients. Although the results were obtainedin awake patients in
the supine position, a
418 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
9/26
statistically significant increase in the minimal
pharyngeal cross-sectional area was described.The results were
confirmed in a more sophisticatedstudy 5 years later with cine
CT.112 Whilea decrease in the diameters at the retropalatal
andretroglossal level was seen during apnea, thesecross-sectional
areas were significantly enlargedwith the help of the appliance.
Sam et al.demonstrated that a non-adjustable oral appliancecan
increase overall airway volume.122
With regard to surgical treatment effects, it hasbeen
demonstrated that the upper airwayincreases after mandibular
distraction osteo-genesis in children106 and after
maxillomandibularadvancement in adults.123 Even more data
isavailable for the effects of UPPP and its modifi-cations. Shepard
and Thawley124 demonstratedthat UPPP more than doubled the upper
airwaycross-sectional area in his 23 patients with OSA andhe
describes specific appearances that were morelikely to lead to
surgical success. Langin et al.125
also concluded that a postoperative oropharyngealenlargement
seen in pharyngeal CT measures isassociated with a good outcome in
UPPP whileRyan et al.107 demonstrated that patients withsmaller
upper airways respond well to UPPP.
Finally, Li et al. demonstrated that an extendeduvulopalatal
flap led to a significant increase inretropalatal space in their 15
patients with OSA.105
CT scanning in patient management
A significant number of the above mentioned andcited authors
have concluded that CT scanningdoes play or will play a major role
in themanagement of patients with SDB. To givea selection, it has
been stated that CT can play
a role in evaluation of OSAS and indications for
surgery,126
that the outcome of UPPP may bepredicted,120 or the surgical
treatment will bemodified with the help of CT scanning.110
Incontrast to these statements, CT scanning has notbecome part of
the routine assessment of patientswith SDB, especially not with
regard to surgicaltreatment selection. Beneficial effects on
treat-ment selection and thereby treatment outcomehave been
postulated repeatedly but could not bedemonstrated to date.
MR imaging
Compared to lateral X-ray cephalometry or CTscanning MRI offers
various advantages, such asexcellent soft tissue contrast,
three-dimensionalassessments of tissue structures and lack
ofionized radiation. The advantages with regard tothe lack of
ionized radiation have made MRimaging the imaging technique of
choice in theassessment of children with SDB.
Techniques and standards
Concerning their scientific or clinical use in thecontext of
SDB, routine imaging techniques wereinitially applied following
various protocols used ineveryday clinical practice. For patients
sufferingfrom SDBdboth children and adultsdit wasattempted to
determine anatomical preconditionsand peculiarities for SDB. In
this research, compar-isons with healthy controls have been
utilized,measuringtwo-dimensionaldistances and diametersof the
upper airway or its related structures.127e131
In addition to simple two-dimensional assessment,
Figure 1 Upper airway narrowing during tidal breathing as
assessed with CT scanning: (A) cross-sectional image ofa patient at
the level of uvula in tidal breathing and (B) the significant
narrowing at the same level in forced expirationis seen. The region
of interest (white line) was used to assess total cross-sectional
areas in each image (reproducedwith permission from Yucel et
al.76).
Airway evaluation in obstructive sleep apnea 419
-
8/7/2019 Airway Evaluation
10/26
researchers began to evaluate volumes of either softtissue
structures such as the tongue, the adenoids,the soft palate or the
pharyngeal walls132e134 orthe remaining compromised or
non-compromisedairway spaces.132,135 To obtain
three-dimensionaldata, volumes were either calculated based
oncross-sectional areas and slice thickness133,136 or
established by various computerized models.
134,137
Ultimately, ultrafast or dynamic imaging was used tovisualize
dynamic motion of the upper airway toassess upper airway collapse
or differences in upperairway motion between patients with SDB
andhealthy controls.127,134,138e144 Subjects were eithermeasured
during wakefulness39,137 or during wake-fulness and
sleep127,142,145; children were routinelyscanned under
sedation.138,139,141,146 Sleep inadults was either
pharmacologically induced143 orspontaneous.47,140
Only a small number of authors have attemptedto establish
distinct protocols for MRI of the upper
airway in SDB136,137,147; the results of themeasurements were
either validated witha phantom137 or tested for variability in
repeatedmeasures over time and with different investiga-tors.136
Validation and standardization of thisimaging paradigm seems
essential; nevertheless,in contrast to, e.g., lateral X-ray
cephalometry,hardly any consensual standards exist for
thisindication.
Providing insights into the pathophysiologyof SDB
OSA in childrenEspecially in children, extensive research has
beendone with regard to the pathophysiology of pedi-atric OSA.
Fricke et al.129 compared children withor without persistent OSA
after tonsillectomy andadenoidectomy and demonstrated that
enlargedlingual tonsils were present in those children
withpersistent disease; this was especially true forchildren with
Down syndrome. Arens et al.132
found significant differences in upper airwaystructures between
children with and childrenwithout OSA. An airway restriction was
detected inthe vicinity of both the adenoids and the
tonsils(especially where adenoids and tonsils overlap)and an
enlarged soft palate was found in theaffected group. Nevertheless,
the airway restric-tion is not limited to these areas but seems
tooccur throughout the initial two thirds of the
upperairway.132,135 These results were confirmed byFregosi et
al.,128 additionally demonstratinga close dependency between the
frequency ofrespiratory events and the size of the tonsils andthe
soft palate. Furthermore, the upper airway
narrowing was more pronounced in those childrenwith a high
number of respiratory events comparedto the less affected group.
Differences inmandibular dimensions between patients with
andwithout OSA, however, could not be detected, atleast not in
children without apparent craniofacialabnormalities.148
With regard to dynamic airway evaluation, morepronounced
fluctuations in airway area during tidalbreathing138 and
significant differences in airwaymotion (static patent or dynamic
patent vs.intermittent collapsed or static collapsed)141
weredemonstrated in children with OSA compared tocontrols. Shott
and Donnelly149 investigated chil-dren with Down syndrome with
persistent airwayobstruction after tonsillectomy and adenoidec-tomy
and could confirm multiple sites of airwayobstruction in this
severely affected group of OSApatients. As the source of
obstruction, recurrentadenoid tissue, glossoptosis, soft palate
collapse,
hypopharyngeal collapse and enlarged lingualtonsils were
described.149
OSA in adultsIn adults, potential differences in upper
airwayanatomy and structure have been described withstatic and
dynamic imaging. As early as 1989,authors pointed out the
significance of pharyngealfat deposits in patients with OSA.150 In
theircomparative trial, Horner et al.150 concluded thatin patients
with OSA more fat is present in theareas surrounding the
collapsible segment of the
pharynx. In more recent publications, morespecific sites of fat
deposition have been described(especially anterolateral to the
upperairway) evenin non-obese patients with OSA.151 While
otherauthors described alterations of the lingualmusculature in
OSA,152 in the study of Do et al.133
there was only a weak trend for larger tongues inpatients with
SDB (tongue size was independentfrom AHI and showed a better
correlation with BMIand neck circumference). In contrast, Schwabet
al. could demonstrate an increased risk of OSAin patients with
increased tongue volume; Iida-Kondo et al.153 described a
significantly highertongue volume in relation to the oral cavity
volumein patients with OSA compared to controls. Otheranatomical
conditions associated with SDB were anelliptic horizontal
cross-sectional area of thepharynx with the long axis oriented in
the sagittalplane131 and large volumes of the lateral pharyn-geal
walls and total soft tissue surrounding theupper airway.134 In a
recent publication of Okuboet al.,154 the anatomic appearance of
themandible and soft tissue structures of the upperairway in
Japanese patients with OSA was
420 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
11/26
compared to controls. While the authors did notfind any
significant differences in tongue volume,soft palates or pharyngeal
walls, they pointed outspecific anatomic factors of the mandible in
OSApatients, such as a wider mandibular divergence
and a smaller mandibular internal length.154
With regard to dynamic imaging, two mainaspects have been the
focal point of interest: first,to learn more about the dynamics of
upper airwayobstruction and second, to detect the level
ofobstruction with regard to potential surgical ornon-surgical
therapeutic interventions.
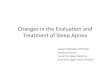
Numerous authors have demonstrated that themechanism and level
of airway obstruction can bevisualized by MRI,39,127,142,143 even
under naturalsleep.47 Figure 2 demonstrates an example ofupper
airway obstruction during natural sleep.
The fact that patients with OSA presentmultiple sites of
pharyngeal abnormality wasdemonstrated by Suto et al.143 as early
as 1993;nevertheless, the authors pointed out that thelevels of
airway obstruction during wakefulnessdid not match those levels
found during sleep.Jager et al. used fluoroscopic MRI in patients
withOSA and healthy controls and demonstrated thatthe entire length
of airway obstruction can bevisualized on MR images.37 Furthermore,
theyrevealed significant differences between the twogroups in terms
of degree of obstruction. In 2001,
Ikeda et al.142 compared patients with OSA andhealthy controls
during wakefulness and sponta-neous sleep. While no pharyngeal
airway nar-rowing was seen in the healthy patients,a significant
narrowing was seen in the OSA
patients already during wakefulness, but evenmore so during
sleep. Ciscar et al.127 essentiallyconfirmed these findings;
moreover, they coulddemonstrate that apnoeic patients have a
morecircular occlusion, underlining the relevance ofthe lateral
pharyngeal walls in the pathogenesisof airway obstruction.
Several authors have speculated that detectingthe site of airway
obstruction with the help ofdynamic MRI may be useful in the
determination oftherapeutic, especially surgical,
interven-tion.142,144,145 Nevertheless, data demonstratingthat the
detection of the sites of airway obstruc-tion with this method is
indeed beneficial in patientselection for surgery are lacking. This
is especiallytrue with regard to a potential improvement insurgical
outcome.
Evaluating the effects of therapeuticintervention
Finally, MRI has been used to assess the effects orside effects
of various therapeutic interventions,including surgical and
non-surgical strategies.
Figure 2 Complete pharyngeal collapse as detected with dynamic
MRI during natural sleep. Dynamic single sliceimages of a
45-year-old man during an apnea period. The first images show the
complete naso-, oro- and hypo-pharyngeal obstruction, the arrows
mark collapse of the different pharyngeal regions (reproduced with
permissionfrom Schoenberg et al.47).
Airway evaluation in obstructive sleep apnea 421
-
8/7/2019 Airway Evaluation
12/26
With regard to conservative treatment, Sanneret al.155 evaluated
the effects of mandibularadvancement devices in 13 patients with
OSA withultrafast MRI and demonstrated that the use of sucha device
can prevent pharyngeal obstruction ina subgroup of patients, at
least during wakefulness.They concluded that ultrafast MRI together
with
the Mueller maneuver while wearing the devicemay be predictive
of the success of a treatmentwith a mandibular advancement device
in OSA.Although Gao et al.156 also reported potentialanatomic
criteria as assessed with MRI forsuccessful treatment with
mandibular advance-ment devices, MRI has not become a
routineprocedure in the management of patients desig-nated for a
treatment with a mandibular advance-ment device.
With regard to surgical treatment, MRI hasbeen used to assess
potential effects of surgeryon upper airway anatomy. In
radiofrequency
surgery, imaging has been used to visualizeimmediate
postoperative effects on the softtissue of the soft palate157 and
the tonguebase.158 Especially the latter study had
practicalconsequences insofar as the extent of the lesionscreated
by radiofrequency surgery were corre-lated with energy application
and concreterecommendations for the use of this technique atthe
tongue base could be made. A standardizedprotocol has furthermore
been used to studyanatomic changes at the upper airway
afterradiofrequency surgery of the tongue base159 and
after hyoid suspension.160
In both studies, nochange in upper airway anatomy could be
detec-ted during wakefulness, indicating that theseinterventions
work more via functional changes inupper airway collapsibility than
via an enlarge-ment of the upper airway.
Latest developments have led to a computa-tional model of the
human upper airway based onsignal averaging of MRI.161 Based on
this model andwith the help of the finite element method,various
surgical interventions have been simulatedand the effects of these
simulated interventions onupper airway mechanics and collapsibility
havebeen assessed, offering new possibilities in thedevelopment and
improvement of surgical andnon-surgical treatment.
MRI in patient management
Static and dynamic MRI has substantially improvedour
understanding of the pathophysiology of SDB.With the help of this
method, significant differ-ences in upper airway anatomy and
structure have
been detected between patients with SDB andhealthy subjects, and
relevant insights have beengained in terms of the mechanisms and
levels ofairway obstruction. Nonetheless, MRI has notbecome a
standard procedure neither in thediagnostic work-up for patients
with SDB nor in themanagement of the disease in terms of surgical
or
non-surgical treatment.A number of issues remain unresolved:
MRIduring sleep (especially spontaneous sleep) ispossible but not
easy to perform and measure-ments during wakefulness or induced
sleep are,to a certain extent, artificial or may simply notreflect
clinical conditions. Furthermore, theresults of MRI, even when
performed duringsleep, can only provide information concerninga
short period of time and are limited to thesupine position. For
routine clinical application,the limited availability and the
associatedcosts are additional limiting factors. Although
MRI has substantially improved our understandingof SDB, it has
not yet become a part of routineclinical evaluation of patients
with thiscondition.
Videoendoscopy during spontaneoussleep
As early as 1978 the first report about video-endoscopic
recording of the pharynx and larynxduring sleep was published.
Borowiecki et al.162
described a palatopharyngeal collapse at the endof expiration
and directly before inspiration inpatients with OSA. They described
differentdegrees of airway obstruction, often associatedwith a
medialization of the lateral pharyngealwalls. Snoring sounds during
arousals wereattributed to the soft palate and the
lateralpharyngeal walls. As there was no treatmentother than
tracheotomy available at this time forthose patients, patient
selection was not anissue.
Today videoendoscopy during spontaneous sleepis performed in
order to improve patient selectionfor the different treatments
available and mayalso be performed in combination with
overnightsleep recordings.163e168 Because videoendoscopyduring
spontaneous sleep allows the assessment ofthe upper airway during
different sleep stages andlacks the side effects of sedating drugs,
thismethod may be considered superior to video-endoscopy under
sedation. However, sleep video-endoscopy is scarcely performed as
it usuallyrequires nightly measurements and puts additionalstrain
on both patient and doctor.
422 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
13/26
Videoendoscopy under sedation
Impact of videoendoscopy under sedation onsleep, breathing and
snoring
Videoendoscopy under sedation also makes itpossible to visualize
the site and mechanism of
snoring and pharyngeal obstruction in patientswith SDB.
Therefore, it is mandatory that snoringand airway obstruction can
be provoked inaffected patients and that neither the
endoscopeitself nor the drugs used for sedation disturb orinfluence
breathing patterns, snoring or airwayobstruction during sedation.
At first video-endoscopy during sedated sleep was described
inchildren and 1 year later in adults using mid-azolam.169,170
Sadaoka et al.171 could demonstratethat during a 3-h videoendoscopy
under sedationwith midazolam only the longest apnea and the
portion of REM sleep showed statistically signifi-cant
differences compared to natural sleep inpatients with suspected
sleep-related breathingdisorders. On the other hand, Jones et
al.172 foundsignificantly different snoring sounds when
acous-tically analyzing a few snores generated duringsedation
endoscopy and comparing them to snoresobtained during natural
sleep. These results mayindicate that the generation of apneas and
snoringsounds follow different mechanisms and that vid-eoendoscopy
during sedation is only partiallyequivalent to videoendoscopy
during spontaneoussleep. Furthermore, it has to be mentioned
that
videoendoscopy during sedation is usually per-formed for 10e15
min due to practical consider-ations, and not for 3 h as described
by Sadaokaet al.171
Not in all patients endoscopy under sedatedsleep succeeds in
inducing existing breathingdisorders, namely snoring and
obstructiveapnoeas, and on the other hand, snoring may beprovoked
even in healthy patients. According tothe current literature,
snoring and airwayobstructions can be observed and induced in
79e95% of all manually sedated patients.169,173e175 In
a cohort study using propofol, Marais
173
detectedsnoring sounds in 45% of 126 healthy,
non-snoringcontrols. He described the sound as being lessintense
but displaying the same pattern as found insnorers. When titrating
propofol with target-controlled infusion, all 53 snorers did snore
reli-ably at a plasma level of 8 mg/ml whereas nota single control
person did at the same plasmalevel, amounting to a sensitivity and
specificity of100%.176 Therefore, target-controlled infusion
withpropofol seems superior to manual titration.
Description of findings
The patterns of snoring and airway obstructionthat can be
observed during videoendoscopy undersedation are multiform. Pringle
and Croft177 werethe first to standardize the findings according
totheir data obtained in a large series of patients.
Currently, different classifications coexist and,ultimately,
none of them are feasible. Theydistinguish either between an
isolated or a multi-segmental obstruction,178 or they are
modifica-tions of the classification according to Pringle andCroft
comprising the epiglottis.173,179 The classifi-cation according to
Catalfumo describing theposition of the epiglottis during the
Muellermaneuver was transferred to sleep video-endoscopy by Golz et
al.180 in 2000. All theremaining authors do not classify their
findings butenumerate the various mechanisms and anatom-ical sites
of snoring and obstruction.174,181 The
obstructive patterns are described as beingcircular,
antero-posterior and latero-lateral at thelevel of the soft palate,
the tonsils, the tonguebase and the epiglottis. An involvement of
thelatter is found in less than 1% to up to 40%.173e175,180,181
Abdullah et al.181 mentioned a combi-nation of as many as five
different concomitantsites of obstruction in primary snorers and
even sixin sleep apnea patients. An isolated site of obstruc-tion
was found in only 15% of the OSA patients.
Impact on clinical decision making
Even if a sleep-like status can be achieved, ifsnoring sounds
and obstructions can be initiatedreliably and documented in detail
during video-endoscopy under sedation, the additional time
andeffort are only justified under the condition thatthe success
rate of surgery for OSA and primarysnoring can be improved with the
help of thismethod. In other words, the question is
whethervideoendoscopy under sedation has a substantialimpact on
clinical decision making and treatmentselection.
Hessel and de Vries178 have established a flow-chart for the
therapeutic proceedings, but limit itto the enumeration of all the
various operationsavailable at the site of major obstruction. In
clin-ical routine a large tongueddefined by a modifiedMallampati
score of 3 or 4dis usually considereda negative predictive
parameter for a successfulUPPP. However, den Herder et al.182 could
notdemonstrate a correlation between video-endoscopy under sedation
(retrolingual obstruc-tion) and Mallampati index (tongue size),
Airway evaluation in obstructive sleep apnea 423
-
8/7/2019 Airway Evaluation
14/26
questioning treatment selection based on Mal-lampati index only.
Nevertheless, the combinedscore has not yet been compared with
video-endoscopy under sedation.
Pringle and Croft177 compared their results ofthe Mueller
maneuver to those obtained by vid-eoendoscopy under sedation in a
group of 50
patients. Based on the Mueller maneuver, 25patients would have
been selected for UPPP.However, 11 (44%) of those patients showeda
substantial hypopharyngeal collapse undersedation, which would have
meant excluding themfrom UPPP. On the other hand, eight of 25
(32%)patients who were excluded from UPPP due to theMueller
maneuver had isolated palatal vibrationsor obstructions under
sedation, making themsuitable for UPPP. In this regard Steinhart et
al.183
examined 324 patients with suspected OSA ina waking state with
Mueller maneuver as well asunder sedation with propofol. They found
a signif-
icant increase in airway collapse during sedatedendoscopy at the
palate (64.3 vs. 80%) and tonguebase (32.3 vs. 59.7%) compared to
clinical exami-nation during wakefulness. Among the pool ofpatients
who did not have a relevant obstructionduring Mueller maneuver
(n78), isolatedobstructions were found at the palate in
one-third,at the tongue base in 14% and at both levels in 50%during
sedated endoscopy. In a study of Camilleriet al.,184 four of 27
patients scheduled for UPPPwere excluded after videoendoscopy under
seda-tion due to tongue base collapse.
Impact on the success rate
Surprisingly enough, no prospective data is avail-able to date
comparing success rates of surgicalintervention with and without
the use of video-endoscopy under sedation. This is
particularlyconfusing as there have been numerous advocatesof
sedated endoscopy presenting data and videoson countless patients
with SDB, but they have notyet been able to demonstrate its
usefulness withregard to surgical outcome. In the study ofCamilleri
et al.184 mentioned above, no superioritywas seen with regard to
success rates compared tohistoric controls, despite using sedated
endoscopy.Yet an improved success rate was found in thosepatients
who did not even show the slightestinvolvement of structures other
than the palate.Hessel and de Vries185 retrospectively reviewed
48snorers and 88 sleep apnea patients after UPPP. Inthose patients
where the soft palate was leastinvolved in airway collapse during
preoperativesedated videoendoscopy, the outcome was supe-rior
compared to the others. In another
retrospective analysis of 55 sleep apnea patientsafter UPPP, the
same investigators did not findsignificantly different success
rates for differentsites of obstruction as revealed by
videoendoscopyunder sedation.3
Videoendoscopy under sedation and the role
of the epiglottis
According to our own experience videoendoscopyunder sedation or
in sleep is particularly helpful indetecting or excluding a
possible glottic or supra-glottic obstruction, most often described
asa posterior movement of the epiglottis duringinspiration.34 In 27
adult patients with epiglotticcollapse during sleep videoendoscopy,
Golzet al.180 found a reduction of the AHI from 45 to 14after
partial epiglottectomy. The publication doesnot reveal whether the
same result could havebeen achieved by basic
clinicaleendoscopicexamination or Mueller maneuver.
Videoendoscopyunder sedation or during sleep may be
particularlyhelpful in cases of laryngeal collapse and failuresof
standard therapy.
Significance of videoendoscopy duringsedation
Videoendoscopy under sedation is able to initiatesnoring and
upper airway obstruction duringa short period of induced sleep,
mostly restricted
to the supine position. The severity of the under-lying disorder
appears comparable to naturalsleep, although snoring sounds seem
different andthe short examination time is a significant
limita-tion. The classification of findings can be reducedto
isolated obstruction at the palate, the tonguebase or the
epiglottis or to combinations of these.There are subtle hints that
videoendoscopy undersedation may change the indication for a
limitednumber of surgical interventions. Nevertheless,there is not
enough evidence to date that thisprocedure improves the outcome of
snoring andsleep apnea surgery.
Multi-channel pressure measurements
Changes in inspiratory pressure in the upper airwayduring
obstructive events can be measured withcatheters. To assess airway
obstruction, differentmeasuring points meaning different
pressuretransducers can be used from the nasopharynxthrough the
oro- and hypopharynx down to theesophagus. Initially, pressure
transducers were
424 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
15/26
used mainly to investigate the mechanisms ofairway obstruction
in general; nowadays researchis focused on the diagnostic
potentials comparedto standard polysomnography and on the
assess-ment of obstruction levels and its impact on theoutcome of
sleep apnea surgery.
To provide useful results, catheters must be
tolerated during sleep without a significant alter-ation of
sleep or breathing. Furthermore, theposition of the measuring
points needs to be stableduring the entire investigation, as there
is no visualcontrol after the initial positioning. Finally,
theimpact on sleep apnea surgery must be assessed asdiscussed
above.
Tolerability of the pressure catheters
Initially, pressure recordings in the field of SDBwere performed
with balloon and open cathe-ters.186 Chaban et al.187 used
stationary balloon
catheters for the esophagus (10 cm long) and thenasopharynx but
added a catheter with a built-inpressure transducer (micro-tip
catheter) to beslowly pulled through the entire upper airway.
Herecorded pressure changes during single apneas ateach different
site. Esophageal balloon cathetersirritated the patients
significantly, leading to anincrease of alpha waves and thus
objectivelydestroying the microstructure of sleep.188
Thereliability of the results of micro-tip catheters wasshown
during wakefulness and sleep for theesophagus by Panizza and
Finucane189 and for the
pharynx by Tvinnereim et al.190
Chervin andAldrich191 and Skatvedt et al.192 presented
well-designed studies demonstrating that catheterswith no more than
2 mm diameter did not alter thesleep structure of patients
suspected of SDB andthe results obtained with or without catheters
inplace did not differ significantly. In a study ofOeverland et
al.193 with 799 patients 3% rejectedthe placement of the catheter
and 1% refusedfurther measurement during the night, while
96%tolerated the procedure. From our experienceswith numerous
available catheters, the two cath-eters developed by Skatvedt and
Tvinnereim are
associated with the least discomfort for thepatients due to the
small diameter and softmaterial.
Reliability of measuring points
Multi-channel pressure catheters require a reliablepositioning
of the measuring points in order toattribute the site of
obstruction to the anatomi-cally defined segment of the airway.
Verse et al.194
demonstrated with the help of lateral X-ray
cephalometry that the distance from the nostril tothe vertebral
bodies, the epiglottic tip and thehyoid bone varies significantly
between individ-uals. Therefore, most investigators choose
theoropharyngeal sensor as a reference to be placedunder visual
control at the free edge of the softpalate. Skatvedt195 reported
that the sensor was
found exactly where it had been placed theevening before after
one night of measurement.Taking this into account, the level of
obstruction isusually described as an upper or lowerobstruction,
meaning an obstruction at the level ofthe soft palate or the level
of the tongue base. (Anisolated collapse at the level of the
epiglottiscannot be assessed with this method.)
Assessment of obstructive events withmulti-channel pressure
recordings
Pressure catheters also can be used to measure
nasal and pharyngeal airflow. This implies thatthey are suitable
to assess increased respiratoryeffort as well as the AHI.
Tvinnereim et al.196
demonstrated that the absolute number ofobstructive and mixed
apneas during sleep can beassessed with these catheters with
minimal devi-ation from the results obtained by poly-somnography.
The overall sensitivity, specificityand the negative predictive
value for the detectionof the different types of apneas and
hypopneasreached 85e100%.197 In a blinded investigation,Reda et
al.198 found a correlation of 0.97 between
the AHI assessed by pressure sensors and thermis-tors used for
polysomnography. When addingactimetry to the pressure measurements
todistinguish between sleep and wakefulness thecorrelation can be
improved even further, as theAHI is based on total sleep time in
polysomno-graphic recordings.199 The data available indicatesthat
multi-channel pressure recordings are suit-able to assess the
severity of SDB.
Assessing the sites of airway obstruction
Hudgel et al.186 were the first to describe thetypical pattern
of obstructions at different locali-zations with the help of one
measuring pointplaced at different levels of the upper airway.They
already pointed out that it was difficult toidentify a combined
collapse at different levels ofhypo- and oropharynx.200 Katsantonis
et al.201
postulated that a short segment obstruction dis-played a high
pressure gradient between twoneighboring sensors. In contrast a
long segmentobstruction would show pressure gradientsextending over
two or more sensors.202
Airway evaluation in obstructive sleep apnea 425
-
8/7/2019 Airway Evaluation
16/26
Skatvedt195 used a catheter with six sensors,placing the third
at the free edge of the softpalate. He found a collapse extending
over morethan one segment in 13 of 20 patients with SDB. Inone case
the segments were not even neighboringand in seven of 20 patients
the site of obstructionchanged during the night. In another study
he
found a combined collapse of the upper and loweroropharynx in
half of his patients.46 Tvinnereimand Miljeteig203 published their
data using a 5-sensor catheter, placing the second sensor at
thefree edge of the soft palate. They describedpressure
oscillations of high frequency beingsuperimposed on the pressure
swings of normaland obstructed breathing and suspected that
thosemight be soft tissue vibrations due to snoring. Inaddition,
Tvinnereim et al.202 calculated a distri-bution of the obstructive
events assessed duringa 3-h recording. Over 90% of the apneas
originatedfrom the middle oropharynx while the remaining
events originated more caudally.
Reliability of the determination of the siteof obstruction
Investigations concerning night-to-night variabilityof the
distribution of the obstructive sites showedthat the predominant
site of obstruction can bereproduced during the second night in 72%
of thecases.Resultswere best reproduced in patients withan apnea
index above 5 or with more than 75%
palatal events.204
Rollheim et al.205
compared thepatterns of obstruction as obtained in the
hospitalwith a recording at home. Although the mean
AHIwassignificantly higherin thehospital than at home,the
occurrence of palatal obstructions did not differbetween both
recordings. In patients who had lessthan 40% or more than 60%
palatal obstructions inthe first recording, this relationship was
reproducedin 90% of the cases during the second recording.
Skatvedt found that in 15 of 20 cases the site ofobstruction
assessed by Mueller maneuver differedfrom the site obtained by
multi-channel pressurerecordings. In 12 cases the Mueller
maneuvermissed a site of obstruction that was clearlydetectable by
manometry.46 Multi-channel pres-sure recordings and videoendoscopy
during sleepdid not produce identical results either. Woodsonand
Wooten12 examined 22 patients with severesleep apnea and described
significant differencesbetween both methods. In another
investigation 11UPPP failures with persistent severe sleep apneahad
a tongue base obstruction in 67% of the casesas assessed by
videoendoscopy versus 17% asassessed by manometry.206
Impact on the success rate of surgery for SDB
Metes et al.207 were the first to publish dataconcerning the
impact of pharyngeal pressuremeasurements on the success rate of
surgery.They used a catheter with one measuring pointonly which was
pulled through the pharynx and
placed at several sites along the upper airway inorder to record
several obstructive events at eachsite. The obstruction they found
in this way per-sisted in eight of 12 patients after UPPP.
Thesuccess rate of UPPP did not differ betweenpatients with
predominant palatal or tongue baseobstruction. The evaluation of
only a limitednumber of obstructive events as well as theselection
of severe sleep apnea patients mayhave limited the results.
Skatvedt et al.208
selected 16 patients with different degrees of SDBand
predominant palatal obstruction detected bymulti-channel pressure
transducers for laser-
assisted uvulopalatoplasty and reporteda decrease in the AHI
from 18.6 to 6.4. While therate of upper obstructions dropped from
90% to8.8% of all apneas, the number of upper hypo-pneas was
reduced only minimally. Osnes et al.209
compared the efficacy of UPPP in patients withpredominantly
transpalatal and subpalatalobstructions. After UPPP, transpalatal
apneas andhypopneas were reduced by 81% whereas sub-palatal events
only dropped by 42%. The successrate in patients with transpalatal
obstruction wassignificantly higher than in those with
subpalatal
obstruction. Supporting the usefulness of pressurecatheters, Ng
et al.210 described a significantlybetter response of mandibular
advancementsplints in OSA patients with a predominantlysubpalatal
collapse compared to those witha palatal collapse.
Multi-channel pressure recordings seem to besuperior to
single-channel pull-through techniquesin predicting surgical
success of soft palatesurgery.
Significance of multi-channel pressure
recordings
Pressure catheters with a small diameter of notmore than 2 mm
are well tolerated and have onlyminimal impact on sleep quality and
airwayobstructions. The pressure curves allow a reliabledetection
of respiratory events. Positioning of themeasuring points by means
of pharyngeal inspec-tion seems to be sufficiently accurate for
theevaluation of the palatal airway segment. Upperand lower
obstructions can be detected. In
426 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
17/26
principle, combined obstructions are more difficultto recognize
and are therefore rarely mentioned.There is no data supporting that
obstructions atthe hypopharynx and the epiglottis can
bediscriminated reliably. The distribution of theobstructions can
be determined for the entirerecording period. The data available
supports the
idea that the success rate of soft palate surgerycan be improved
when using multi-channel pres-sure recordings for patient
selection.
Critical closing pressure
The severity of SDB is usually described by the AHI,representing
the number of upper airwayobstructions during sleep. Nevertheless,
it has tobe kept in mind that the AHI simply describes thefrequency
of upper airway obstructions, not theseverity of the pharyngeal
collapse itself.
Furthermore, measuring the severity of upperairway collapse is
believed to be important whenestimating the forces needed to
overcome theseobstructions or to maintain upper airway
stability.Schwartz et al.211 and Smith et al.212 firstdescribed the
airway collapsibility, coining theterm Starling resistor. The model
posits thatthe nasal and tracheal airway remain constantlyopen as
they consist of rigid tubes, whereas thepharynx behaves as a
collapsible segment wherethe airway obstructions occur. Airflow and
airway
pressure are assessed using a nasal CPAP devicewith integrated
pneumotachograph and pressuresensor. The CPAP device must be able
to producepositive as well as negative pressure levels ifneeded. A
pressure-flow diagram can be drawn atdifferent levels of airway
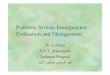
pressure and a regres-sion line can be calculated. Smith defined
the
critical closing pressure (Pcrit) as being the upperairway
pressure when the regression line iscrossing the zero line,
indicating that airflowcompletely stops (see Figure 3). Gleadhill
et al.,213
Gold and Schwartz48 and Gold et al.214 demon-strated that
patients with obstructive apneas havea Pcrit clearly above zero; in
patients withobstructive hypopneas it is slightly negative, inUpper
Airway Resistance Syndrome Pcrit rangesbetween 2 and 6 mbar, in
simple snorers iteven drops further to 3 to 12 mbar, whereas
innormal controls Pcrit it is on average below8 mbar. Therefore,
any successful therapy
should result in shifting Pcrit to values more nega-tive than 8
mbar. By measuring Pcrit it wasbelieved that patients surgical
success may bepredicted as patients with Pcrit levels close
tonormal might be better candidates for surgicalinterventions than
those with a positive Pcritbecause only minimal improvements of
Pcrit arenecessary to eliminate SDB. On the other handthese
favorable patients will mainly present withhypopneas and
respiratory arousals during poly-somnography but not with
apneas.
500
450
400
350
300
250
200
150
100
50
0-2 -1 0 1 2 3 4 5 6 7 8
PN (cm H2O)
VImax(ml/s)
Supine
Side
Figure 3 Representative pressureeflow relationships in the
lateral recumbent and supine positions for one subjectin non-REM
sleep. Maximal inspiratory airflow (VI max) vs nasal mask pressure
(PN) is illustrated for lateral recumbent(open circles) and supine
(closed circles) positions with corresponding regression lines and
confidence interval.Critical closing pressure is represented by the
PN at which airflow becomes zero in each body position
(reproducedwith permission from Boudewyn et al.215).
Airway evaluation in obstructive sleep apnea 427
-
8/7/2019 Airway Evaluation
18/26
The initial method was later simplified andabbreviated.
Boudewyns et al.215 could demon-strate that Pcrit was 2 mbar lower
in the lateralposition compared to the supine position (seeFigure
3). Furthermore, sleep stages did not haveany impact on Pcrit.
Gender differences were found in OSA patients,
with men having a more positive Pcrit than women,independent of
BMI216 whereas healthy men andwomen had the same Pcrit.
217
Impact of treatment on Pcrit
Schwartz et al.218 could show that substantialweight loss
resulted in an improvement of Pcritfrom 3.1 to 2.4 mbar and a
concomitant reduc-tion of the AHI. In another study6 they
investigatedthe effect of UPPP on Pcrit in 13 patients. Theyfound a
significant decrease for the entire group.
Even though a complete normalization of Pcrit from0.8 to 7.3
mbar could be demonstrated in thesubgroup of responders (in
contrast, an insignifi-cant change from 1.1 to 0.6 mbar in the
subgroupof non-responders occurred) they could not findany
preoperative predictor of response. An iden-tical operation had
individually varying effects onPcrit. Due to the difficult and
extensive measure-ment of Pcrit Huang et al.
219 developed a compu-tational model using finite elements in
order tosimulate the effect of upper airway surgery inOSA.219 They
could show that stiffening the
tongue base or the palate or resecting parts of thelatter
results in an improvement of Pcrit. Howeverthere are no clinical
studies validating theseresults.
In summary, the assessment of the criticalclosing pressure is an
important tool in theinvestigation of upper airway patency. It is
thegold standard for the measurement of the overallcollapsibility
of the pharynx and is especiallyuseful in research projects. Up to
now, there is nodata concerning the benefit of a
preoperativeassessment of Pcrit for a better prediction ofsuccess
of upper airway surgery. Together withthe relatively complex
assessment of Pcrit thismay explain why Pcrit measurements have
notbecome a routine procedure in clinical testingso far.
Summary
The various techniques of airway evaluation pre-sented in this
review have significantly increased
our insight into the pathophysiology of SDB.Nevertheless,
potential benefits with regard topatient management or the
superiority oversimple clinical assessment remains
underdiscussion.
The role of routine clinical and endoscopicevaluation of the
upper airway is unquestioned
especially in terms of patient management andtreatment
selection. Although the subjectivity ofthe assessment and the
variability of the nomen-clature of the clinical findings are a
significantlimitation, clinical assessment is inevitable
espe-cially before surgical intervention or treatmentwith
mandibular advancement devices. Over thelast years, different
staging systems have beeninaugurated that may especially be helpful
for lessexperienced physicians and for standardizationpurposes.
Nevertheless, whether the use of thesestaging systems is superior
to simple clinicalassessment of experienced observers remains
to
be seen.Since snoring as well as apneas can be simulated
by most people and direct effects of the Muellermaneuver may be
seen on upper airway behaviorduring wakefulness, this technique has
been usedin upper airway evaluation before surgical inter-vention
to predict surgical outcome and toimprove patient selection.
Nevertheless, the reli-ability of the Mueller maneuver remains
highlyquestionable and the evaluation of the maneuverseems highly
subjective and hard to reproduce.Furthermore, the data available do
not support the
idea that the results obtained by the Muellermaneuver may be
transferred to natural sleep. Anisolated hypopharyngeal collapse
(although rare)during the Mueller maneuver indicates
clinicalfailure with UPPP. Nevertheless, the Muellermaneuver does
not facilitate patient selection forthe varying surgical
interventions used in OSApatients.
X-ray cephalometry has demonstrated signifi-cant craniofacial
characteristics associated withSDB. Specific cephalometric
characteristics havebeen repeatedly mentioned as a risk factor
forOSA; especially the more inferiorly positionedhyoid bone. There
are parameters that correlatewith the severity of the disease and
with favorableresults of mandibular advancement by oral
appli-ances, but no cephalometric parameters exist thatwould
reliably rule out treatment success with oralappliances. Therefore,
X-ray cephalometry has notbecome a routine procedure in the
diagnosticwork-up of OSA as long as maxillomandibularsurgery is not
planned.
Both scanning techniques (CT and MRI) haverepeatedly
demonstrated three-dimensional upper
428 B.A. Stuck, J.T. Maurer
-
8/7/2019 Airway Evaluation
19/26
airway narrowing in children and adults with SDB.Dynamic
investigations have been used to visualizeand localize upper airway
obstruction and havesubstantially improved our
three-dimensionalunderstanding of the pathophysiology of
thedisease. Beneficial effects on treatment andpatient selection
(particularly for surgical inter-
vention) have repeatedly been postulated but havenot been
demonstrated to date. Furthermore, theresults of these scanning
techniques, even whenperformed during sleep, can only provide
infor-mation concerning a short period of time andare limited to
the supine position. For routineclinical application, the limited
availability, theassociated costs and the associated ionized
radia-tion at least for CT scanning are additional
limitingfactors.
Videoendoscopy during spontaneous sleep
allows the assessment of the upper airway duringdifferent sleep
stages and lacks the side effects of
sedating drugs. However, sleep videoendoscopy isscarcely
performed as it usually requires nightlymeasurements and puts
additional strain on bothpatient and doctor. Videoendoscopy under
seda-tion is able to initiate snoring and upper airwayobstruction
during a short period of induced sleep,mostly restricted to the
supine position. Theseverity of the underlying disorder
appearscomparable to natural sleep, although snoringsounds seem
different and the short examinationtime is a significant
limitation. There are subtlehints that videoendoscopy under
sedation may
change the indication for a limited number ofsurgical
interventions. Nevertheless, there is notenough evidence to date
that this procedureimproves the outcome of snoring and
OSAsurgery.
Pressure recordings with catheters are rela-tively well
tolerated and have only minimal impacton sleep quality and airway
obstructions. Thepressure curves allow a reliable detection
ofrespiratory events and upper as well as lowerobstructions can be
detected. There is no datasupporting that obstructions at the
hypopharynxand the epiglottis can be discriminated reliably.The
distribution of the obstructions can be deter-mined for the entire
recording period. The dataavailable support the idea that the
success rate ofsoft palate surgery can be improved when
usingmulti-channel pressure recordings for patientselection.
The assessment of the critical closing pressureis the only tool
to directly measure upper airwaycollapsibility. Up to now, there is
no data con-cerning the benefit of a preoperative assessmentof
critical closing pressure for a better prediction
of success of upper airway surgery. Togetherwith its relatively
complex assessment this mayexplain why these measurements have
notbecome a routine procedure in clinical testing sofar.
Although all these additional techniques forupper airway
assessment exceeding simple clinical
assessment have substantially improved ourunderstanding of SDB,
their significance in dailypractice is limited. In contrast to the
widespreaduse of the Mueller maneuver and sedated endos-copy,
convincing data supporting their use in termsof treatment outcome
is lacking. So far, there isonly very limited evidence that
selected tech-niques improve treatment outcome for
selectedindications. In general, there is not enoughevidence that
these techniques are superior to theroutine clinical
assessment.
Practice points
The significance of the different techniquesfor the evaluation
of the upper airway insleep-disordered breathing are presented
withregard to the clinical management:
Clinical examination including rigidendoscopy is essential,
staging systems
may be useful in the hands of less experi-enced observers.
The Mueller maneuver may be performedbefore considering UPPP, as
an isolatedhypopharyngeal collapse indicates clinicalfailure, but
the overall value is limited.
There is no convincing indication forroutine X-ray cephalometry
as long asmaxillomandibular surgery is not planned.
There is no indication for routine evalua-tion with radiologic
scanning techniquessuch as CT or MRI.
Videoendoscopy under sedation or duringsleep may be particularly
helpful in casesof laryngeal collapse and failures of stan-dard
therapy.
Pressure recordings may help improvingsuccess rates of palatal
surgery, butobstructions at the hypopharynx and theepiglottis
cannot be discriminated reliably.
Apart from scientific approaches, there isno data supporting the
routine assessmentof the critical closing pressure.
Airway evaluation in obstructive sleep apnea 429
-
8/7/2019 Airway Evaluation
20/26
Acknowledgment
We want to thank Mr. J. Wich-Schwarz, Ph.D., forhis editorial
assistance.
References*1. Anand VK, Ferguson PW, Schoen LS. Obstructive
sleep
apnea: a comparison of continuous positive airway pres-sure and
surgical treatment. Otolaryngol Head Neck Surg1991;105:382e90.
2. Boot H, van Wegen R, Poublon RM, et al. Long-termresults of
uvulopalatopharyngoplasty for obstructivesleep apnea syndrome.
Laryngoscope 2000;110:469e75.
3. Hessel NS, Vries N. Increase of the apnoeaehypopnoeaindex
after uvulopalatopharyngoplasty: analysis offailure. Clin
Otolaryngol Allied Sci 2004;29:682e5.
4. McGuirt Jr WF, Johnson JT, Sanders MH. Previous
tonsil-lectomy as prognostic indicator for success of
uvulopala-topharyngoplasty. Laryngoscope 1995;105:1253e5.
5. Petri N, Suadicani P, Wildschiodtz G, et al. Predictivevalue
of Muller maneuver, cephalometry and clinicalfeatures for the
outcome of uvulopalatopharyngoplasty.Evaluation of predictive
factors using discriminant anal-ysis in 30 sleep apnea patients.
Acta Otolaryngol 1994;114:565e71.
6. Schwartz AR, Schubert N, Rothman W, et al. Effect
ofuvulopalatopharyngoplasty on upper airway collapsibilityin
obstructive sleep apnea. Am Rev Respir Dis 1992;145:527e32.
7. Stevenson EW, Turner GT, Sutton FD, et al.
Prognosticsignificance of age and tonsillectomy in
uvulopalato-pharyngoplasty. Laryngoscope 1990;100:820e3.
8. Fukuda N, Abe T, Katagiri M, et al. Effects of
uvulopala-topharyngoplasty on patients with obstructive
sleepapneadthe severity of preoperative tonsillar hyper-trophy.
Nihon Kokyuki Gakkai Zasshi 1998;36:34e40.
9. Nakata S, Noda A, Yanagi E, et al. Tonsil size and bodymass
index are important factors for efficacy of simple
tonsillectomy in obstructive sleep apnoea syndrome.
ClinOtolaryngol 2006;31:41e5.
10. Verse T, Kroker BA, Pirsig W, et al. Tonsillectomy asa
treatment of obstructive sleep apnea in adults withtonsillar
hypertrophy. Laryngoscope 2000;110:1556e9.
11. Hormann K, Verse T, editors. Surgery for sleep
disorderedbreathing. Berlin, Gottingen, Heidelberg: Springer;
2005.
12. Woodson BT, Wooten MR. Comparison of upper-airwayevaluations
during wakefulness and sleep. Laryngoscope1994;104:821e8.
13. Friedman M, Ibrahim H, Bass L. Clinical staging for
sleep-disordered breathing. Otolaryngol Head Neck Surg
2002;127:13e21.
14. Friedman M, Ibrahim H, Joseph NJ. Staging of
obstructivesleep apnea /hypopnea syndrome: a guide to
appropriate
treatment. Laryngoscope 2004;114:454e9.15. Friedman M, Tanyeri
H, La Rosa M, et al. Clinical
predictors of obstructive sleep apnea.
Laryngoscope1999;109:1901e7.
16. Friedman M, Vidyasagar R, Bliznikas D, et al. Doesseverity
of obstructive sleep apnea /hypopnea syndromepredict
uvulopalatopharyngoplasty outcome? Laryngo-scope
2005;115:2109e13.
17. Li HY, Wang PC, Lee LA, et al. Prediction of
uvulopala-topharyngoplasty outcome: anatomy-based stagingsystem
versus severity-based staging system. Sleep 2006;29:1537e41.
18. Liu SA, Li HY, Tsai WC, et al. Associated factors to
predictoutcomes of uvulopharyngopalatoplasty plus
genioglossaladvancement for obstructive sleep apnea.
Laryngoscope
2005;115:2046e50.19. Fischer Y, Panis A, Rettinger G.
Interindividuelle Varia-
bilitat klinischer Befunde bei Patienten mit primaremSchnarchen
und obstruktiver Schlafapnoe. HNO-Informa-tionen 2004;29:174.
20. Naya M, Vicente E, Llorente E, et al. [Predictive value
ofthe Muller maneuver in obstructive sleep apneasyndrome]. Acta
Otorrinolaringol Esp 2000;51:40e5.
21. Riley RW, Powell NB, Guilleminault C. Obstructive sleepapnea
syndrome: a review of 306 consecutively treatedsurgical patients.
Otolaryngol Head Neck Surg 1993;108:117e25.
22. Schafer J, Pirsig W, Lenders H, et al. Was bringt
dienasopharyngeale Video-Fiberendoskopie fur die Diag-nostik von
Schnarchern und Patienten mit obstruktiver
Apnoe. Laryngorhinootologie 1989;68:521e8.23. Hsu PP, Tan AK,
Tan BY, et al. Uvulopalatopharyngoplasty
outcome assessment with quantitative
computer-assistedvideoendoscopic airway analysis. Acta Otolaryngol
2007;127:65e70.
24. Li KK, Guilleminault C, Riley RW, Powell NB.
Obstructivesleep apnea and maxillomandibular advancement:
anassessment of airway changes using radiographic
andnasopharyngoscopic examinations. J Oral Maxillofac
Surg2002;60:526e30.
25. Liao YF, Huang CS, Chuang ML. The utility of cephalom-etry
with the Muller maneuver in evaluating the upperairway and its
surrounding structures in Chinese patients
Research agenda
The following main questions remain withregard to the clinical
use of upper airwayevaluation in sleep-disordered breathing:
Various techniques (especially video-endoscopy and pressure
measurements)provide information with regard to themechanism and
level of airway obstruc-tiondbut do they really cha