Embed Size (px)
Citation preview

Air pollution and its impact on health:
Comparing findings in China with findings in Europe and the USA
Kristin Aunan, CICERO
CCICED, October 29, 2007, Beijing

2
0 100 200 300 400 500 600 700 800
Beijing
Guangzhou
Taiyuan
Lanzhou
Shanghai
Tokyo
New York
Los Angeles
Rio de Janeiro
Mexico City
Delhi
NO2
SO2
TSP
mg/m 3
16 of the 20 most polluted cities in the world are Chinese
What are the health benefits of abating air pollution?

3
Deaths from diseases associated with air pollution exposure are frequent in China (2002)
Annual deaths per 100,000 people. Source: WHO, 2004

4
Why should there be differences between d-r coefficients across countries?
• Differences in composition of air pollution
• Demographic factors, e.g. age distribution
• Health status and socio-economic conditions
• Access to health services

5
.. differences may (misleadingly) be due to
• Confounding factors (e.g. exposure to indoor air pollution)
• Conversion factors between different PM fractions (e.g. TSP to PM10)
• Classification of disease (ICD 9, ICD 10)

6
Dose-response for acute all-cause mortality (time-series studies): Very good agreement across regions
End-point
(air pollutant)
China (meta-analysis)
Aunan & Pan, 2004
Europe (APHEA II)
Reanalysis
USA
(NMMAPS)
Reanalysis
USA
Harvard 6 cities
Reanalysis
All-cause
deaths (PM10)
0.03
(HEI, 2004: 0.04-0.05)0.04-0.06 0.02-0.03 0.07
All-cause
deaths (SO2)
0.04
(HEI, 2004: 0.04-0.05)0.03-0.06 No evidence Not included
(Eastern Europe:
0.01-0.04
Western Europe:
0.03-0.06)
Percent change in health outcome per 1 mg/m3

7
Dose-response for other end-points (time-series and cross-sectional studies): Less agreement
End-point (air
pollutant)
China (meta-analysis)
Aunan & Pan, 2004Europe (APHEA II)
Europe (Kunzli
metaanalysis)USA
Hosp. admissions (CVD)
P100.07 0.04-0.05 0.13 0.10 NMMAPS (US-EPA, 2003)
Hosp. admissions (CVD)
SO20.19 0.07
Hosp.admissions (resp.)
PM10
0.12
(HEI, 2004: 0.07-0.16)0.09 0.13 0.10-0.40
NMMAPS (US-EPA, 2003)
Hosp.admissions (resp.)
SO20.15 0.05
Chronic Resp. illness
Adults PM100.31
Chronic Resp. illness
Children PM100.44
Chronic bronchitis Adults
PM100.48 0.91-1.27
Portnay Mullahy, 1990;
Schwartz, 1993; Abbey et al.,
1993
Chronic bronchitis
Children PM100.34 2.5
Ware et al., 1996; Dockery et al.,
1989
Infant mortality 0.39
Meta-analysis (Eastern Europe,
USA, S.Korea, Mexico) (Aunan
and Pan, 2004)

8
Generally: Large variations across studies for most end-points

9
How to deal with long-term effects on mortality in China?
• Shortterm time-series studies do not capture the long-term cumulative effects of pollution exposure
• No long-term cohort studies in China (or similar countries)
• Cohort studies from USA (Pope et al., 1995, 2002) yield implausibly high risks in China
• World Bank 2007: Use Pope et al. (low pollution areas) and cross-sectional Chinese studies (high pollution areas -Shenyang and Benxi) and adjust a logarithmic function

10
A compromise solution(gives around 400,000 premature deaths in urban China in 2003)
11
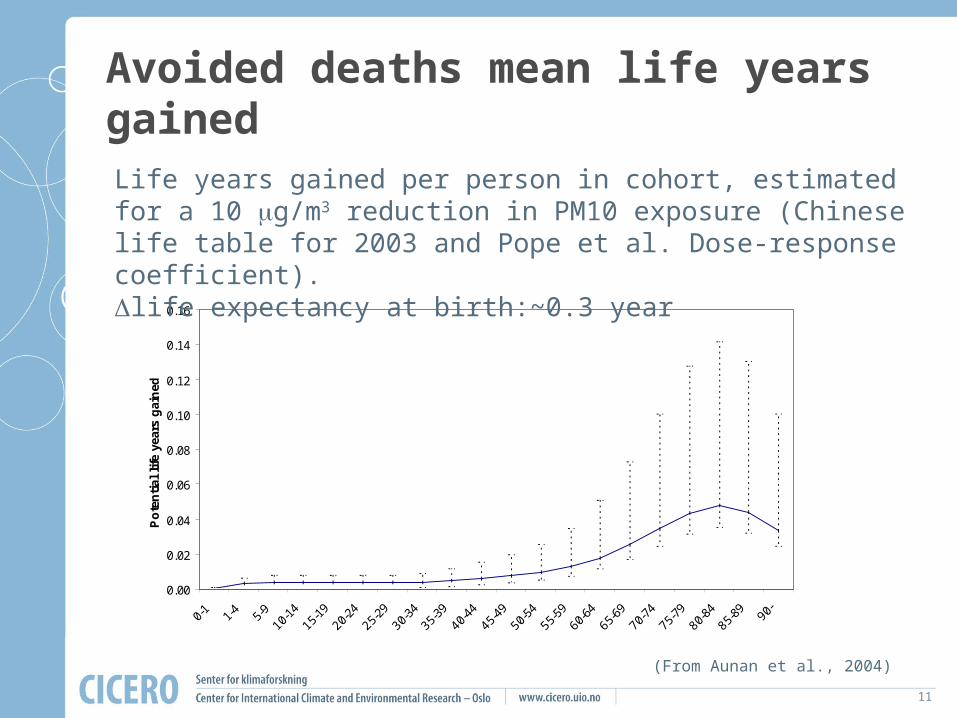
Avoided deaths mean life years gained
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0.16
Po
ten
tial
lif
e ye
ars
gai
ned
Years of age
Life years gained per person in cohort, estimated for a 10 mg/m3 reduction in PM10 exposure (Chinese life table for 2003 and Pope et al. Dose-response coefficient). life expectancy at birth:~0.3 year
(From Aunan et al., 2004)
12
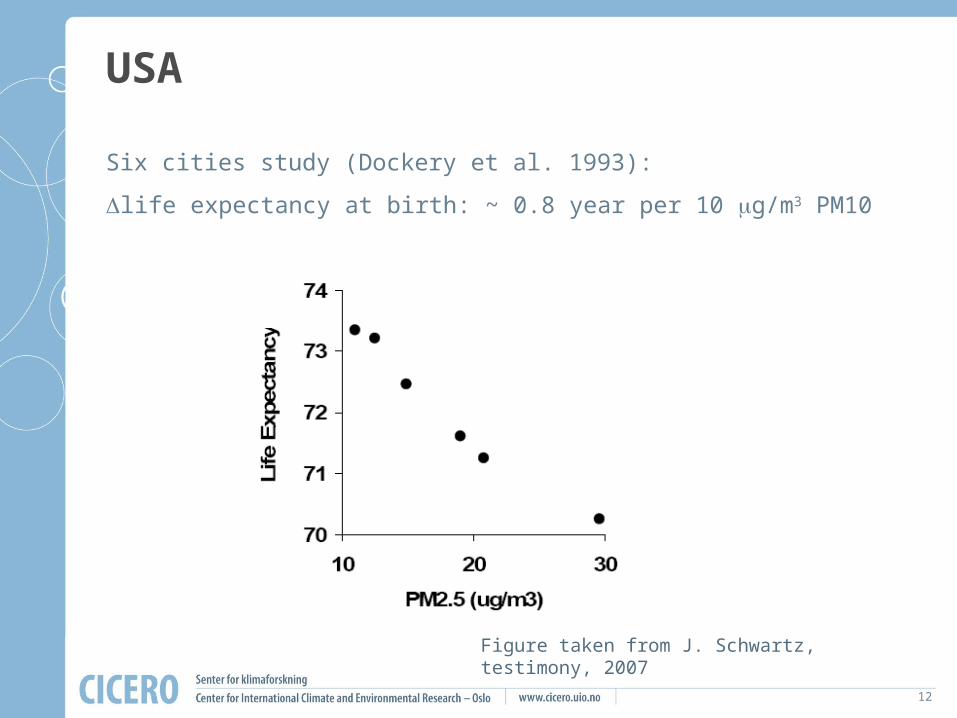
USA
Six cities study (Dockery et al. 1993):
life expectancy at birth: ~ 0.8 year per 10 mg/m3 PM10
Figure taken from J. Schwartz, testimony, 2007

13
COPD: An important health endpoint for which knowledge is scarce
Global Health Statistics, Murray and Lopez, 1996
Incidence rate 1990 345 Per 100,000
Prevalence rate 1990 2499 Per 100,000
Average duration 7.8 years
Ministry of Health, 2004
1/2 year prevalence (huan bin lu) 750 Per 100,000
Estimated average duration 12.8 (?)years
What is the incidence rate and prevalence rate in China? Regional differences?
14
Conclusions• Acute effect om premature mortality:
– High degree of certainty and coherence across regions (d-r and baseline rates)
– But no studies on infant mortality
• Better to transfer d-r for chronic mortality effects than to omit – Long-term cohort studies in China needed!
• Chronic respiratory diseases (e.g. COPD):– Large uncertainties remain (d-r and baseline
rates)
• Data on present frequencies of health outcomes and exposure levels are insufficient, especially in rural areas