Embed Size (px)
Citation preview
Aging: Change and AdaptationAging and Mental Health
Andrea S. Schreiner PhD
The University of Vermont
February 15,2005

PSYCHOLOGY OF AGING
Cognition—attention, memory, problem-solving
Self & Personality---this includes moods and emotions—who you are---what you value---temperament, character
Social Relationships —how you relate to others, social support groups, networks
Mental Health-- focuses on differentiating normal changes that occur with aging as opposed to pathological changes in each of the above areas.

Review of Changes to the Brain and Nervous System with aging
I. The Central Nervous System
Brain
Spinal cord

Nervous System
• II. The Peripheral Nervous System
Nerves –afferent & efferent
• III. Synapses & Neurotransmitters
norepinephrine, serotonin,
dopamine, and the enzyme
acetylcholine

Normal Structural Changes To the Brain and Nervous System Related to Aging
Anatomical Changes:
• Increase in the size of the ventricals and
a widening of sulci resulting in some
cortical atrophy and an increase in
cerebral spinal fluid
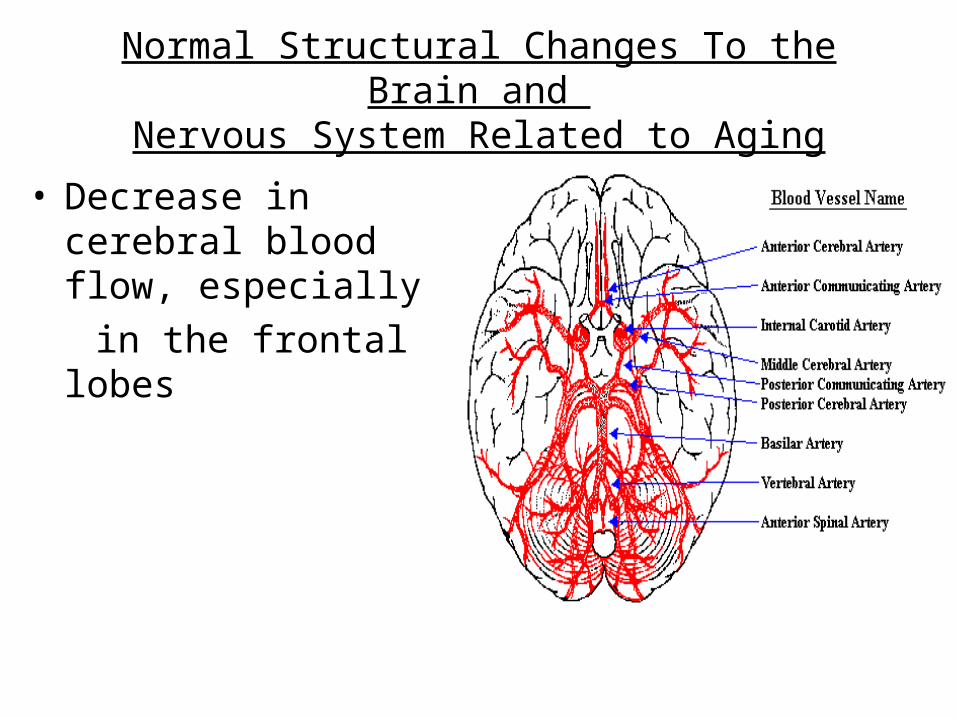
Normal Structural Changes To the Brain and Nervous System Related to Aging
• Decrease in cerebral blood flow, especially
in the frontal lobes

Normal Structural Changes To the Brain and Nervous System Related to Aging
• Decrease in number of synaptic connections between neurons
HOWEVER, functional changes such as cognitive performance among older adults have not demonstrated similar consistent changes.
***High Degree of Plasticity***

IN GENERAL,
• older adults experience a general loss of neurons, slowed conduction of nerve impulses, and loss of peripheral nerve function that makes maintenance of homeostasis, recovery from stress and adaptation to heat and cold and exercise less quick and less complete
.
1. Thermoregulation Increased risk for hypothermia and hyperthermia. Reasons for this include changes in thyroid functioning, loss of body fat, malnutrition, decreased activity, certain drugs (tranquilizers, pain killers and so on).
Hypothermia--- 35°C or lower person appears confused---all body systems slow down, heart rate, respiration, muscle response
Hyperthermia --- 40°C or higher Dizziness, weakness, nausea and vomiting, diarrhea and headache-- As the temperature rises, the classic symptoms of psychosis, delirium, loss of consciousness, and hot, dry skin appear. The cardiac output decreases and circulatory failure and death occur
FIVE Functional Changes and Health Risks That Occur with Normal Aging

2. Motor function—
• Reaction time slows down---the time between a stimulus and the person’s response--response is slower but it is more accurate---
an example of Selective Optimization with Compensation
• We should follow the**Rule of 5-second-wait**
• Reflexes also slow down and there may be a slight tremor of the limbs with aging

3. Memory/Cognition- "Universal-Decrementalist Perspective" is false
TYPES OF MEMORY• "Working Memory“---declines in the ability to store and process--- but could be related to testing time.• "Epidsodic Memory" ---declines in ability to remember past events. • “Semantic Memory“—may have improvements and there are cohort
effects• Crystallized intelligence –increases• Procedural Memory---few declines in ability to remember how to
perform motor
Again, Selective Optimization with Compensation
Cognitive Training leads to lasting improvements

Differential Diagnosis
• Physiological conditions such as brain tumors, or metabolic, endocrine , or electrolyte disturbances, as well as dietary insufficiencies, certain medications, and alcoholism can effect the memory. Therefore, extensive testing is necessary to determine the nature of any memory deficit.

4. Sleep---the older we get the longer it takes us to fall asleep and the less deeply we sleep. Older persons Have more awakenings and less REM sleep.
• Medications such as beta blockers, alcohol, and caffeine can inhibit sleep, having to wake often to urinate alsoreduces sleep. Establishing a regular cycle of sleep and waking is important as you age.


• 5. Proprioception
• Balance becomes less stable with aging, especially if the person has visual loss. The sensation of dizziness increases with aging.
• There are 4 types of dizziness and persons with sensory loss are most at risk for this.
Syncope—is a condition in which consciousness is briefly lost. It can relate to orthostatic hypotension.
To prevent problems, older persons with orthostatic hypertension should get up from seated positions slowly and be careful.

Most Common Cognitive Problems Related to Aging
3 main types of Age-Related Cognitive 3 main types of Age-Related Cognitive disorders—disorders—
(REMEMBER the brain is VERY sensitive to changes(REMEMBER the brain is VERY sensitive to changes in metabolism or oxygen supply)in metabolism or oxygen supply)

1. Delirium1. Delirium—— Acute condition (which means it occurs suddenly in Acute condition (which means it occurs suddenly in response to a change and is self-limiting---i.e. NOT permanent) response to a change and is self-limiting---i.e. NOT permanent) in which the person experiences severe confusion and possibly in which the person experiences severe confusion and possibly hallucinations as well as poor judgement, loss of reality, and hallucinations as well as poor judgement, loss of reality, and restlessness or drowsiness. Delirium can be a reaction to restlessness or drowsiness. Delirium can be a reaction to medications such as anesthesia. It is a very common medications such as anesthesia. It is a very common occurence in older adults after surgeryoccurence in older adults after surgery
(occurs in 25% of older adults who have been hospitalized). It (occurs in 25% of older adults who have been hospitalized). It may also be caused by fluid-electrolyte imbalance or acid-base may also be caused by fluid-electrolyte imbalance or acid-base imbalance, fever or even infection. There are many possible imbalance, fever or even infection. There are many possible causes. causes.
Interventions for this include making sure the person has their Interventions for this include making sure the person has their eye glasses or hearing aid, explaining to them what is eye glasses or hearing aid, explaining to them what is happening, and explaining to the family that this is a happening, and explaining to the family that this is a temporary condition. Hospital staff may confuse this with temporary condition. Hospital staff may confuse this with dementia if the patient has no case history.dementia if the patient has no case history.
• 2. Dementia --- There are eleven types of dementia but Alzheimer’s,
Cerebral Vascular Accident (CVA or Stroke) are the most common. These are chronic conditions related to actual tissue (cell) damage of the brain. The symptoms are related to the area of damage but the main characteristic is memory loss. However, in CVA dementia there may be other losses including functional
losses such as problems with speech and paralysis.
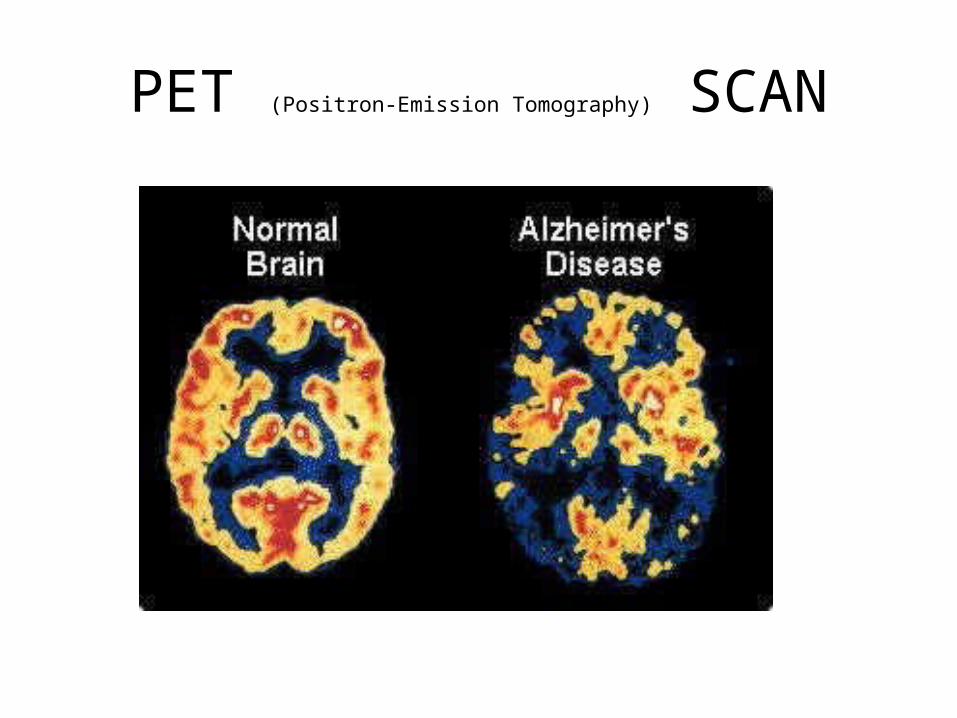
PET (Positron-Emission Tomography) SCAN

3. Depression ---relatively uncommon in older adults --should never be considered a normal part of aging.
There is a distinct type of depression in late life which may be reactive—such as after NH admission.
In general, depressive symptoms may increase overall but to a lesser degree of severity. Late onset depression often has a cognitive component, some memory impairment, which may be related to decreased blood flows or TIAs.
Stroke is related to increased depressive symptoms
Depressive symptoms are very similar to dementia so the person is often labeled “demented”. Again, the correct diagnosis for these cognitive problems will involve ruling out the possibility of physiological problems that could affect cognition.
Prevalence of Depression and Medical Diagnosis
• 17.1%--Lifetime prevalence
• 1-15%---Prevalence among older adults
• Diagnostic and Statistical Manual of Mental Disorders (4th edition, revised)

Diagnostic Criteria
• During a 2 week period or more:• Four or more of the following including either depressed
mood (most of the day) or loss of interest/pleasure:
• wt loss or gain, insomnia or hypersomnia, fatigue, feelings of worthlessness, diminished ability to think or concentrate recurrent thoughts of death
• Concept of Late Life Depression—less severe symptoms but includes presence of cognitive impairment

Differential Assessment
• 1. identifying presenting symptoms
• 2. obtaining a history
• 3. mental status testing
• 4. psychological and neuropsych testing
• 5. coordination with medical evaluation
• 6. when dementia is present, identifying
the probable cause

“Rule-Out” Medical tests
• Brain Scan—CT, MRI• CBC Complete Blood Count• BMP Basic Metabolic Profile—kidney fx,
liver fx, glucose• Thyroid fx test• Chest x-ray• Tests for syphilis or HIV• Urinalysis

Assessment Scales
• Geriatric Depression Scale—mood, affect
• Cornell Scale for Depression in Dementia—mood, eating, sleeping, thought processes, motor function
• Cognitive Testing

Neuropsych Testing
• WAIS III Test--Performance Tests like block design or digit span---to test attention, concentration, working memory
• Verbal tests—vocabulary, comprehension, and memory fx like recall & recognition (naming)
• Wechsler Memory Scale (WMS-III)—tests attention/concentration, general memory, verbal memory, visual memory, delayed recall.
Cohort effects, SES, influence outcomes

BIOCHEMISTRY OF DEPRESSION
“Therefore both emotion and cognition potentially have a biologic substrate—the transmission of information from one nerve cell to the another”
Neurotransmitters and neurohormones:Serotonin (5-HT), Norepinephrine, Dopamine, thyroid hormones as well as the Hypothalamic-Pituitary-Adrenal Axis (HPA).
Serotonin system and the HPA --both respond to chronic stress by changing secretion of various neurotransmitters and hormones in the hippocampus and hypothalamus---i.e.limbic system which is involved in sleep, appetite, pleasure and mood control.


Stress
• Stress secretion of glucocorticoids & cortisol from adrenal cortex these bind to receptors in the hypothalamus where they inhibit corticotrophin releasing hormone and pituitary adrenocorticotropin secretion.
• The hippocampus has an abundance of glucocorticoid receptors which control negative feedback

IN DEPRESSION---this system changes from stress--- cortisol secretion increases and is not controlled by normal feedback Findings in autopsy of suicide victims show changes in the HPA system (referred to as over-activity) . Point, circulating glucocorticoid levels provide important hormonal control of affect.
Biochemistry of Depression

Treatments for Depression• Pharmacologic Therapy --Antidepressant Medications—
• Tricyclics—
• MonoAmineOxidase Inbitors
• SSRIS— Prozac (1987), Zoloft, Lexapro, Celexa, Paxil
• It may be difficult to treat chronic depression in the older adults due to the presence of other health problems.
• Antidepressant medications often have many side effects such as drowsiness, dizziness, blurred vision, dry mouth, urinary retention, constipation, weight gain, hypotension and others.
• ECT---Electric Convulsive Therapy
• Psychotherapy---learned helplessness
• Behavioral and cognitive approaches have better outcomes with older adults—
• Late onset depression may be more reactive than melancholic

I have little control over the things that happen to me.
What happens to me in the future depends mostly on me." (reverse scored)
There is really no way I can solve some of the problems I have.
There is little I can do to change many of the important things in my life.
I can do just about anything I set my mind to." (reverse scored)
I often feel helpless in dealing with the problems in life."
Scoring scale: strongly agree (4) , agree (3), disagree (2), strongly disagree (1)
Mastery items from Pearlin, L.I. & Schooler, C., (1978). The structure of coping.
Journal of Health and Social Behavior. 19, 2-21.
Self-Mastery or Control

Emotional Changes with Aging
• Mood or Affect:
• Positive mood is stable ---or may increase
• Duration of negative mood decreases
• Emotional Regulation or Control increases with aging

Adult Personality Development
• Personality is one aspect of the SELF: stable over age
• Erik Erikson’s Developmental Tasks or Crises:
Generativity versus Stagnation
• Integrity versus Despair—importance of life reflection or reminiscence
Older persons not more prone to depression and anxiety but LESS

Life Events
• Older Adults have to cope with major life events including:
• Family—changing relationships
• Love & Marriage—widowhood
• Health—chronic illness• Finances• Work---retirement

Personality Inventory Factors (NEO-PI-R) Costa et al 1986
• Neuroticism--
• Extraversion--
• Openness to experience--
• Agreeableness—increases with age
• Conscientiousness—increases with age
Disengagement Theory
• Cumming & Henry, 1960
“Normal aging is a mutual withdrawal or disengagement between the ageing person and other in the social system to which he belongs..”
The focus is really on SUCESSFUL AGING---the idea that we can do this better and more positively “maximizing the positive, minimizing the impact of age-related losses on QOL.”
Adaptive functioning in the face of declining resources Baltes & Baltes (1990)
Selective Optimization with Compensation Model
Select what’s important to you to maintain—for your sense of QOLCompensate for losses so you can continue to have what’s important---focus on attaining the goal in alternate ways.

““There’s much to There’s much to forgive in what I forgive in what I have written—have written—the rawness, the the rawness, the self-consciousness, self-consciousness, the vanity, the folly. the vanity, the folly. I’m older now, but I’m older now, but am I wiser--or merely am I wiser--or merely not so young?” not so young?” Miss M Miss M in Walter de La Mare’sin Walter de La Mare’sMemoirs of MidgetMemoirs of Midget

• ElderCare Online is a beacon for people caring for aging loved ones. ….we are committed to providing an online community where supportive peers and professionals help you improve quality of life for yourself and your elder.
• The Caregiver's Beacon –Bi-monthly newsletter
• http://www.caregiving-solutions.com/index.html