Embed Size (px)
Citation preview

1
Fostick, L. Ben-Artzi, E., Babkoff, H. (2013). Aging and Speech Perception among the Elderly:
Beyond Hearing Threshold and Cognitive Ability. Journal of Basic & Clinical Physiology &
Pharmacology, 24(3), 175-83
***This is a self-archiving copy and does not fully replicate the published version***
Aging and Speech Perception: Beyond Hearing Threshold and Cognitive
Ability
Leah Fostick,1* Elisheva Ben-Artzi,2 Harvey Babkoff3
1Department of Communication Disorders, Ariel University, Israel
2Kinneret Academic College, Tzemach, Israel
3Ashkelon Academic College, Ashkelon, Israel
Running Head: Aging and Speech Perception
*Corresponding author:
Leah Fostick
Department of Communication Disorders
Ariel University, Ariel 40700
Israel
Tel. 972-3-9765776
Email. [email protected]

2
Abstract
Background. Older adults manifest difficulties in speech perception, especially when speech
is accompanied by noise or when speech is rapid. Several explanations have been suggested
to account for age-related changes in speech perception, such as changes in hearing sensitivity
or a more general decline in cognitive functioning. The purpose of the present study was to
directly examine the relative contribution of hearing sensitivity and perceptual and cognitive
factors in the understanding of age-related differences in speech perception under difficult
conditions.
Method. Eighty nine healthy participants, with normal hearing thresholds, age 21 to 82 years,
were tested for speech perception under four conditions: quiet, speech noise, white noise, and
time-compressed speech at 60% compression rate. Since all participants had age-normal
hearing, absolute thresholds were tested for click trains, 1kHz 15msec duration pure tone,
1kHz 50msec duration pure tone, and 1.8kHz 15msec duration pure tone, which are relatively
short and discriminative for hearing ability. Cognitive ability was examined using WAIS-III
matrices and digit span.
Results. When words were presented against a quiet background or against white noise speech
perception was not significantly affected by aging, although in the latter case, increased
thresholds predicted poorer speech perception. However, when words were presented against
a background of speech noise or when speech was time-compressed at a 60% rate, age
significantly predicted a decline in speech perception, even after controlling for hearing
thresholds and cognitive functioning.
Conclusions. Hearing threshold for short sounds is the major factor predicting speech
perception in background noise, across age, due to changes in hearing sensitivity or in

3
temporal resolution. For adult and aging population with preserved cognitive ability,
cognitive functioning does not predict decline in speech perception.
Key Words: Aging, Speech Perception, Cognitive ability, Hearing thresholds

4
Introduction
Many older individuals, even if they do not suffer from extensive hearing loss, report
difficulties in understanding speech especially under less favorable conditions, such as when
speech is accompanied by noise or when speech is rapid. Some surveys [e.g., 1] have reported
that over 30% of elderly individuals find it difficult to understand conversations in everyday
listening situations. A number of studies have reported that older individuals were poorer than
younger adults in word recognition, when speech was accompanied by several types of noise,
e.g., white noise, speech noise, and speech babble [2-4], or when speech was compressed
[e.g., 5,6].
Because of the well-documented age-related general decline in a variety of
physiological, behavioral and cognitive functions, there are potentially several possible
sources for the reported difficulties in speech perception. Among the well-documented age-
related auditory changes is that of hearing sensitivity. As individuals age there is a
progressive decrease in hearing sensitivity to pure tones, especially in the high frequency
range. Presbycusis affects one of every three individuals under the age of 60. By age 80,
nearly one half of all individuals suffer from presbycusis [7].
The hearing-sensitivity theory argues that presbycusis and other age-related changes in
hearing are the main causes for the difficulties in speech perception reported by older
individuals [6,8-12]. However, a number of studies have shown this explanation to be
insufficient. Elderly individuals tended to have more difficulties in speech perception than
was predicted by the hearing sensitivity theory even when their absolute hearing thresholds
were matched to that of younger individuals [13-15].
The apparent presence of difficulties by the elderly in comprehending speech even
when their thresholds are equated to younger individuals has led to an alternative explanation

5
of the age-related decline in speech perception that posits age-related changes in cognitive
processes may also be an important factor in accounting for difficulties in speech perception
[e.g., 16-18]. A number of studies have reported that difficulties in speech perception in
young populations suffering from hearing difficulties can, in part, be attributed to cognitive
factors [19,20]. Humes [21] reported that cognitive factors were the second major factor after
hearing thresholds that accounted for the variance in speech perception scores in a population
of elderly individuals outfitted with hearing aids.
Several researchers have suggested that poorer speech perception by older adults
could be explained by a reduction in processing speed or "cognitive slowing" [5,6,22,23].
Other researchers have focused on difficulties in executive functioning associated with aging
(including memory) and have suggested that a deficit in at least one of the executive control
components (working memory, attention, and goal maintenance) could contribute to a
reduction of the overall cognitive functioning in aging, and consequently lead to difficulties in
successfully performing complex tasks, including speech perception [24-30].
If changes in hearing sensitivity and decline in certain cognitive functions are
exclusively responsible for the reported decline in speech perception under difficult
conditions by the elderly, then this would mean that were these variables to be controlled, age
as an independent variable, would not predict any decline in speech perception. However, if
age predicts difficulties in speech perception even when hearing sensitivity and cognitive
functioning are controlled, this would imply that some additional variables associated with
age are also involved in the age-related difficulties in comprehending speech.
Very few of the earlier studies have systematically examined the contributions of
changes in hearing sensitivity, cognitive functioning or auditory temporal resolution and
aging as separate predictor variables of speech perception performance in individuals, whose
hearing thresholds are within the norms for their age groups and who do not require hearing

6
aid corrections. As a first attempt to clarify the contributions of the putative variables noted
above as predictors of the age-associated decline in speech perception, we examined the
separate contributions of hearing thresholds, cognitive function and aging on speech
perception. Therefore, the major purpose of the present study was to test the hypothesis that
speech perception declines as a function of age even after controlling for hearing thresholds
and cognitive functioning. Since all the participants in the study had normal hearing relative
to their age, we did not use the classical audiometric thresholds in this study, but hearing
thresholds for shorter sounds (such as click trains, 15 and 50 msec pure tones) in order to have
a discriminative measure with higher resolution of hearing sensitivity. We tested speech
perception in a healthy sample of adults, ranging in age from 21-82, who were screened to
exclude any individuals with hearing loss beyond the norm for his or her age group, or who
evinced any cognitive deterioration.

7
Method
Participants
Eighty nine participants were included in the study, 46 (52%) females and 43 (48%)
males, aged 21 to 82 (30 participants age 21-40, 30 participants aged 41-60, and 29
participants aged 61-82). Participants' age and sex were distributed equally. No correlation
was found between age and years of education (r = -.108, p > .05). All participants were
screened for normal hearing thresholds meeting the criteria of Lebo and Reddell [31], and had
interaural threshold differences less than 10 dB. All participants were native Hebrew
speakers, had more than 12 years of education, and reported being healthy and independent in
their functioning, with no history of diseases related to the central nervous system.
Participants whose age was over 60 years also performed the Mini Mental State Examination
(MMSE) [32]. All scores were 29-30 reflecting a high level of mental ability.
Tasks and stimuli
Absolute threshold was measured for short duration stimuli in an attempt to create a
distinctive measure with higher resolution of hearing sensitivity in age-normal hearing
population. In order to measure than participants' cognitive ability, participants performed two
cognitive tasks that measures short-term working memory, and non-verbal general
intelligence (i.e., matrices and digit span). Speech perception was tested four conditions that
were designed to reflect different speech perception environments
Absolute threshold.Absolute thresholds were measured for click train, 1kHz pure tone
15msec duration, 1kHz pure tone 50msec duration, and 1.8kHz pure tone 15msec duration
using a 2-forced-choice adaptive paradigm with a two-down-one-up methodology [33]. Three
blocks of stimuli were presented to each subject. The first block of stimuli was considered
practice. Thresholds were computed from the averaged thresholds of the last two blocks.

8
Thresholds were calculated as the mean of the last eight out of 10 reversals in the two-down-
one-up paradigm.
Cognitive ability. Cognitive ability was measured using the Wechsler Adult
Intelligence Test (WAIS-III) [34].
Speech perception. Speech perception was tested using four tasks: speech perception
in quiet, speech noise, white noise, and time-compressed speech at 60% compression rates. In
the quiet condition, words were presented with no background noise. In the speech noise
condition, words were accompanied by background broadband noise composed of steady-
state frequencies within the range of 0.5-2kHz (band-passed noise), while in the white noise
condition words were accompanied by wide band white noise. The words in these conditions
were presented at a rate of 120 wpm. Speech- and white noise were recorded using the
Diagnostic Audiometer DA64 and were presented at a signal to noise ratio = 0dB. In the 60%
time-compressed speech condition, words were compressed to be 60% of their original length,
and were presented with no background noise at a rate of about 200 wpm with the same three
seconds of silent interval between them. The compression was carried out using the WSOLA
(Waveform Similarity Overlap and Add) algorithm [35]. This algorithm produces high quality
time-scale modification of speech signals with no changes to other characteristics of the
auditory stimuli, such as pitch. For all of the speech conditions, the silent gap between words
was 2.5 seconds.
The words used in the speech perception tasks were taken from the HAB (Hebrew
AB) test, which is the Hebrew version [36] of the AB words test [37]. The tasks were
composed of 12 lists of ten one syllable Consonant-Vowel-Consonant meaningful words. The
lists were phonemically balanced such that each list contains all of the consonants, and the
vowels appear twice. The speech noise and white noise conditions were composed of four

9
lists each. The speech in quiet and the speech presented at 60% compression rate were
composed of two lists each.
Apparatus
Speech perception tasks were presented using digital compact disk player with
SONY's Digital Reference MDR-CD770 earphones. Screening for hearing sensitivity was
done using Danplex DA64 or Maico Hearing Instruments Ltd MA32 audiometers.
Procedure
The experiment was carried out in two sessions of two and a half hours each. The
various tasks were performed in random order and were split between the sessions, except for
the absolute threshold test which was always performed during the first test session. The first
session included the screening procedure, during which participants were informed of the
nature of the testing procedure and signed an informed consent. Participants then filled out a
personal questionnaire, underwent audiometer testing and the performed the MMSE. All
participants were paid an amount in NIS equivalent to $50 for participating in the study.
Results
Age and hearing sensitivity
Hearing sensitivity, as measured by the absolute threshold task, for the click train, and
the 15-msec duration 1 kHz and 1.8 kHz tones declined significantly with age (Table 1).
However, the threshold of the 50- msec duration 1 kHz tone did not change significantly with
age. Based on these results, hearing sensitivity for the click trains, 1kHz, 15-msec duration,

10
and the 1.8 kHz 15-msec duration tones were statistically controlled for in the subsequent
analyses that tested the relationships between age and speech perception.
Age and cognitive ability
Cognitive ability, as measured by the digit span test and matrices was not found to
correlate significantly with age (Pearson's r = -0.12, p>.05; Pearson's r = -0.08, p > .05, for
digit span and matrices, respectively). These results indicate that for the population sample in
this study, there was no significant age-related decline in these cognitive abilities.
Age and speech perception
Speech perception accuracy (percent correct) is plotted as a function of age in Figure 1
for each of the speech conditions separately: 1) speech in quiet; 2) speech with white noise
background; 3) speech with speech noise background; and 4) time-compressed speech. Note
that the Pearson correlation between age and speech perception is not significant when speech
is presented either in quiet (r = -.07, p > .05) or with white noise background (r = -.14, p
>.05), but is significant when speech is presented with speech noise background (r = .51; p <
.0001), and when speech is time-compressed (r = .23, p = .03).
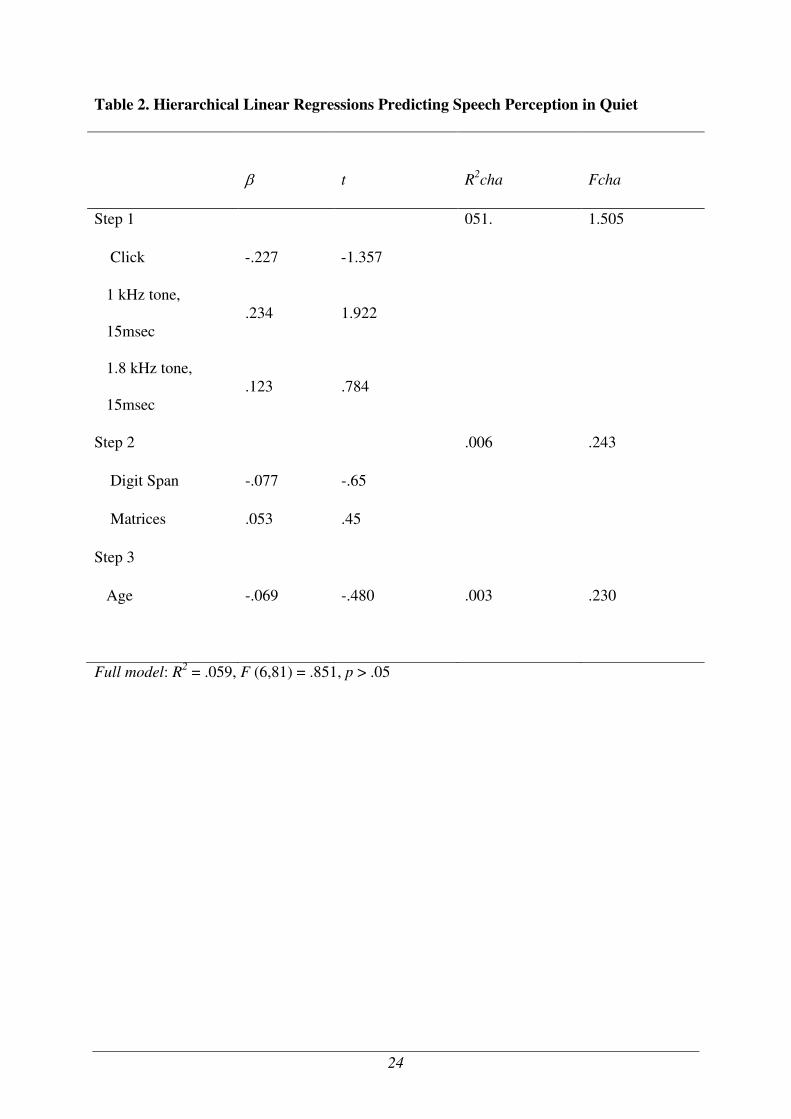
In order to test whether age predicts speech perception after controlling for hearing
sensitivity and cognitive ability, a series of four hierarchical linear regressions were applied to
predict speech perception in quiet, in white noise, in speech noise, and time-compressed
speech at 60% compression rate. In each regression analysis, three variables of hearing
sensitivity, namely the absolute threshold for the click train, and the 15-msec duration 1 kHz
and 1.8 kHz tones, were entered in Step 1, digit span and matrices scores were entered in Step
2, and age was entered in Step 3. Tables 2-5 present the results of these regression analyses.
As can be seen in Tables 2-5, age did not predict speech perception in quiet and in white noise

11
beyond hearing sensitivity and cognitive ability. However, age significantly predicted the
decline in speech perception and explained a large part of the variance when words were
presented in speech noise, and made a moderate contribution in predicting the decline in
perceiving time-compressed speech at a 60% compression rate These results indicate that
speech perception significantly declines with age even after controlling for hearing sensitivity
and cognitive ability when speech was time-compressed and when speech was presented with
a speech noise background
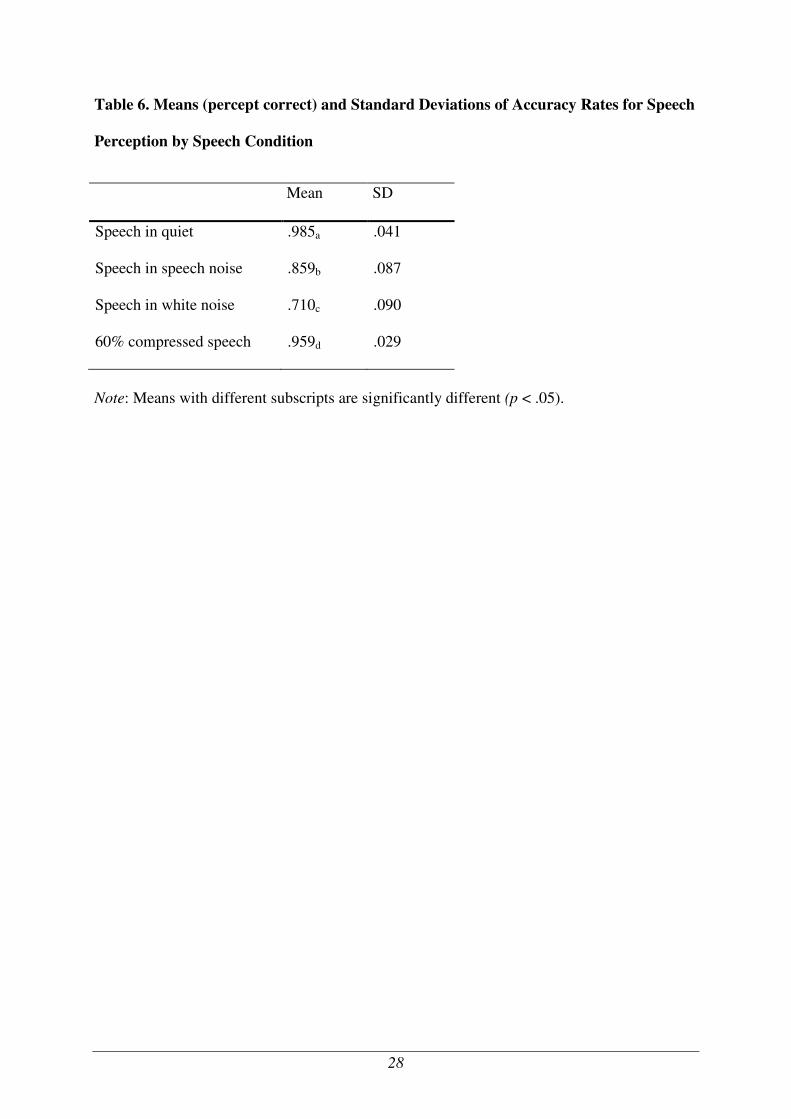
Next, we tested the possibility that perhaps age was a significant predictor of the
decline in speech perception only for conditions that are generally more difficult. Table 6
presents accuracy levels of speech perception for the four speech conditions. A repeated-
measures ANOVA conducted on accuracy levels by speech condition (speech in quiet,
speech in white noise, speech in speech noise, speech at 60% compression rate) revealed a
significant effect of speech condition on accuracy, F (3, 86) = 271. 03, p < .001. Bonferroni's
post-hoc analyses indicated that all four speech conditions significantly differed in difficulty.
Speech perception was the most difficult when words were presented in a white noise
background and was the easiest one when words were presented in quiet. Therefore, task
difficulty cannot be the explanation for the age-related decline in speech perception when
speech is time-compressed or when speech is presented against a background noise.

12
Discussion
The major findings of the present study relate to the decline in speech perception
associated with aging. A number of recent studies have shown that older adults are poorer
than younger adults in word recognition, when speech was accompanied by several types of
noise, e.g., white noise, speech noise, and speech babble [2-4], or when speech was time-
compressed [5,6]. In the present study, we examined changes in speech perception in a
population of healthy individuals, aged 21-82, screened for: 1) hearing thresholds within the
normal range for their age; 2) intact cognitive functioning, as measured by the Mini Mental
State Examination [32]; and 3) with no differences in level of education.
We found that both speech perception in speech noise and speech perception in white
noise conditions were associated with hearing sensitivity. The common feature for these
conditions is that words were presented against background noise. The results suggest that
when noise accompanies speech, hearing sensitivity plays a role in the perception, as
compared to when speech is not accompanied with noise, even when it is rapid (such as in
time compressed speech). In contrast to the condition of speech presented against white noise
background, when words were presented against a background of speech noise, speech
perception was also significantly predicted by aging after controlling for hearing thresholds
and cognitive functioning (as measured by performance on the digit span and matrices tasks).
Similarly, when speech was time-compressed at a 60% rate, age significantly predicted a
decline in speech perception, after controlling for hearing thresholds and cognitive
functioning. Both speech perception in speech noise and in time-compression represent
difficult conditions for speech perception which might explain the association with age.
Along this line, we would have expected such an association also with the speech perception
in white noise which was not observed in the current study. A small variability in this

13
measure, due to floor effect, might explain the lack of relationship between age and speech
perception in white noise.
A number of factors have led researchers to suggest that age-related difficulties in
speech perception reflect more general age-related changes in basic perceptual and cognitive
functions. First of all, speech perception and production are very likely dependent upon the
normal functioning of a number of sensory and perceptual as well as cognitive mechanisms
[e.g., 19]. Perceiving spoken language is cognitively and perceptually complex. The listener
must perform a perceptual analysis of the speech sounds, identify each word, resolve the
syntactic structure of what is being heard, and integrate the newly arriving information with a
memory trace of what has already been heard [38,39]. All this must be accomplished at
speech rates which, even in ordinary conversation, average between 150 and 250 words per
minute [40-41]. Second, there is a growing literature that documents an age-related general
decline in a variety of physiological, behavioral and cognitive functions, including those very
closely related to speech perception, e.g., speed of cognitive processing [24,26,42].
Consequently, two of the more popular candidates as possible sources for the age-related
difficulties in speech perception have been: 1) changes in hearing sensitivity; and 2) decline in
cognitive functioning.
A number of researchers have suggested that presbycusis and other age related
changes in hearing sensitivity are the main causes for the difficulties in speech perception in
older individuals [6,8-12,43]. This approach implies that one should be able to predict decline
in speech perception by changes in hearing sensitivity, unrelated to their ages. In fact, the
extent of hearing loss has been shown to be a significant predictor variable for speech
recognition performance in individuals with hearing impairment, even when they wear their
hearing aids. For example, Humes [21] tested 171 new and experienced hearing aid wearers
(aged 60-87) and reported that the decline in speech recognition was predicted both by the

14
extent of hearing loss and by cognitive function. Furthermore, Humes reported that the
“…(hearing loss) factor alone accounted for 53.2% of the variance in speech recognition
factor scores and was the single largest contributing factor among predictor variables". When
Humes analyzed a sub-group of his participants with “milder amounts of hearing loss”, the
amount of variance accounted for by the hearing loss factor was 14.8%. Nevertheless, this
was also approximately half of the variance accounted for by all of the factors (33.9%) for
that sub-group of listeners.
Humes’ findings that hearing thresholds were less of a factor in predicting speech
perception in the participants who were less impaired lead to the suggestion that speech
recognition for older individuals with very mild hearing loss, may either not be significantly
predicted by hearing thresholds, or if significantly predicted, the variance accounted for may
be much less than for individuals with hearing loss levels that require correction by hearing
aids [21]. Our findings are consistent with this conclusion. We examined speech perception in
individuals whose thresholds were within the normal range for their age, and who were not
hearing aid wearers. In order to measure hearing sensitivity in higher resolution and to enable
variance in hearing sensitivity in spite having all the participants screened for age-normal
hearing thresholds, we used hearing sensitivity for short sounds. We found that when words
were presented against a background of white noise or speech noise, speech perception was
significantly predicted by hearing thresholds. The amount of variance accounted for, however,
was 10.1% when speech was presented in white noise and 19.5% when speech was presented
in speech noise (see Table 3 and 4, step 1 results). These findings, thus, tend to support the
conclusion that although hearing thresholds may be a major factor in accounting for the
explained variance in speech perception scores, this factor accounts for less of the variance in
participants whose thresholds are within the normal range for their age, as compared to the
more impaired participants in the study reported by Humes [21].

15
Although changes in hearing thresholds account for a large amount of the variance of
speech perception under certain difficult conditions, other variables have also been
implicated. A number of researchers have suggested that reduced hearing sensitivity was not a
sufficient explanation for the decline in speech perception in older individuals [13-15]. For
example, elderly individuals tended to have more difficulty in speech perception than younger
participants even when their absolute hearing thresholds were matched to that of the younger
participants [13-15]. Also, as noted above, Humes [21] reported that the second factor
accounting for the variance in the performance of speech perception tasks by hearing aid
wearers was non-verbal IQ and age. Some researchers have viewed these findings as further
evidence for one of the more popular recent theories in aging research, that posits that as
individuals age, there is a generalized slowing of brain/cognitive functioning.
The putative slowing of cognitive processing is reflected in an almost linear decline in
problem solving, reasoning, memory and language from early adulthood to senescence
[22,44-47]. Age-related deficits in working memory, executive functioning, the ability to
maintain a goal, or processing speed have been suggested as the causes responsible for the
difficulties in speech perception in the elderly [5,22,28,29,48]. Age-related changes in one or
more of the executive control components (working memory, attention, or goal maintenance)
could contribute to a reduction of the overall cognitive functioning in the elderly, and
consequently lead to difficulties in successfully performing complex tasks, including speech
perception [e.g., 27,30].
In the present study, we attempted to assess the effect of age on speech perception
while controlling for the possible decline of cognitive function by two procedures: 1) pre-
selection screening; and 2) by direct testing and inclusion of scores on cognitive tests in the
data analyses. First, the candidates for the study who were over 60 years of age were pre-
screened with the Mini Mental State Examination (MMSE) [32]. Only individuals with scores

16
of 29-30, reflecting a high level of mental ability, were included in the subject sample.
Second, all participants were tested on the WAIS-III matrices and digit span tests. The results
indicated that, for the population sampled in this study, there was no significant age-related
decline in these cognitive abilities. These test scores were also entered in all of the regression
analyses of speech perception. The results of the regression analyses indicated that
performance on the WAIS-III matrices and digit span tests did not add significantly to the
explained variance and, therefore, did not predict performance on any of the speech
perception tasks. In contrast, age as a variable, independent of hearing thresholds and scores
on the digit span and matrices tasks, did significantly add to the explained variance (7.6%)
when words were presented against background speech noise and when speech was time-
compressed (5%). Apparently, when words are presented against background speech noise or
when speech is compressed, a significant decline in speech perception with age can be found
even when working memory and reasoning are intact and unchanged over the life span.
These suggest that there are other factors associated with aging, other than changes in
hearing thresholds and in cognitive functioning, may be involved in the age-related decline in
speech perception when speech is presented in speech noise and when speech is time-
compressed. Perceiving speech when words were presented against a speech noise
background and when speech was time-compressed were not the two most difficult of the
experimental conditions. In fact, when comparing the accuracy of speech perception between
all four conditions, speech against a white noise background was clearly the most difficult
condition. However, although it was the most difficult of the tasks, the amount of explained
variance accounted for by increases in hearing thresholds was less (10.1%) than when speech
was presented against a speech noise background (19.5%) (Tables 3-5). Yet under the white
noise background condition, age, as an independent variable was not significant in predicting
a decline in speech perception.

17
In summary, we found that under the conditions of the present study, change in
hearing thresholds for short duration sounds was the major factor in predicting a decline in
speech perception, when words are presented against a white noise or speech noise
background, even when all individuals were within the normal range for their age groups. In
an aging population, screened for intact cognitive functioning and whose level of cognitive
performance was equivalent to the younger participants, cognitive functioning was not
predictive of a decline in speech perception. Under two of the conditions in the present
experiment, i.e., when words were presented against a speech noise background and when
speech was time-compressed at 60% rate, age, as an independent variable, significantly
predicted a decline in speech perception even when hearing sensitivity and cognitive
functioning were controlled.
The authors have no conflict of interests.

18
References
1. Committee on Hearing, Bioacoustics and Biomechanics (CHABA). Speech.
Understanding and Aging. J Acoust Soc Am 1988;83:859-820.
2. Snell KB, Frisina DR. Relationships among age-related differences in gap detection
and word recognition. J Acoust Soc Am 2000;107(3):1615-1626.
3. Snell KB, Mapes FM, Hickman ED, Frisina DR. Word recognition in competing
babble and the effects of age, temporal processing, and absolute sensitivity. J Acoust Soc Am
2002;112(2):720-727.
4. Agus TR, Akeroyd MA, Gatehouse S, et al. Informational masking in young and
elderly listeners for speech masked by simultaneous speech and noise. J Acoust Soc Am
2009; 126: 1926–1940.
5. Wingfield A. Cognitive factors in auditory performance: context, speed of
processing, and constraints of memory. J Am Acad Audiol 1996;7(3):175-182.
6. Humes LE, Dubno JR, Gordon-Salant S, Lister JJ, Cacace AT, Cruickshanks KJ,
Gates GA, Wilson RH, Wingfield A. Central presbycusis: a review and evaluation of the
evidence. J Am Acad Audiol 2012;23(8):635-66
7. Cienkowski KM. Auditory aging. The Journal of Self Help for Hard of Hearing
People 2003;24:12-15.
8. Dubno JR, Lee, FS, Matthews LJ, Mills JH. Age-related and gender-related changes
in monaural speech recognition. J Speech Lang Hear Res 1997;40: 444-452.
9. Halling DC, Humes LE. Factors affecting the recognition of reverberant speech by
elderly listeners. J Speech Lang Hear Res 2000;43(2):414-31.
10. Humes LE, Watson BU, Christensen LA, Cokely CG, Halling DC, Lee L. Factors
associated with individual differences in clinical measures of speech recognition among the
elderly. J Speech Lang Hear Res 1994; 37(2):465-74.

19
11. Schneider BA, Daneman M, Pichora-Fuller MK. Listening in aging adults: from
discourse comprehension to psychoacoustics. Can J Exp Psychol 2002;56(3):139-152.
12. Wingfield A, Lindfield KC, Goodglass H. Effects of age and hearing sensitivity on
the use of prosodic information in spoken word recognition. J Speech Lang Hear Res
2000;43(4):915-925
13. Drager KD, Reichle JE. Effects of discourse context on the intelligibility of
synthesized speech for young adult and older adult listeners: applications for AAC. J Speech
Lang Hear Res 2001;44(5):1052-1057.
14. Gordon-Salant S, Fitzgibbons PJ. Temporal factors and speech recognition
performance in young and elderly listeners. J Speech Lang Hear Res 1993;36(6):1276-1285.
15. He NJ, Dubno JR, Mills JH. Frequency and intensity discrimination measured in a
maximum-likelihood procedure from young and aged normal-hearing subjects. J Acoust Soc
Am 1998;103(1):553-65.
16. Grossman M, Cooke A, Devita C, Alsop D, Detre J, Chen W, Gee J. Age-related
changes in working memory during sentence comprehension: an fMRI study. Neuroimage
2003;15(2):302-317.
17. Schneider BA, Daneman M, Murphy DR. Speech comprehension difficulties in
older adults: cognitive slowing or age-related changes in hearing? Psychol Aging
2005;20:261-271.
18. Frtusova JB, Winneke AH, Phillips NA. ERP evidence that auditory-visual speech
facilitates working memory in younger and older adults. Psychol Aging. 2013;28(2):481-94.
19. Pisoni DB, Cleary M. Measures of working memory span and verbal rehearsal
speed in deaf children after cochlear implantation. Ear Research 2003;24(1):106s-1290s.

20
20. Pisoni DB, Geers AE. Working memory in deaf children with cochlear implants:
correlations between digit span and measures of spoken language processing. Ann Otol
Rhinol Laryngol 2000;185:92-93.
21. Humes LE. Factors underlying the speech-recognition performance of elderly
hearing-aid wearers. J Acoust Soc Am 2002;112:1112-1132.
22. Salthouse TA. The processing-speed theory of adult age differences in cognition.
Psychol Rev 1996;103(3):403-28.
23. Benichov J, Cox LC, Tun PA, Wingfield A. Word recognition within a linguistic
context: effects of age, hearing acuity, verbal ability, and cognitive function. Ear Hear
2012;33(2):250-6.
24. Bunce D, Macready A. Processing speed, executive function, and age differences in
remembering and knowing. Q J Exp Psychol A 2005;58(1):155-168.
25. Clark CR, Veltmeyer MD, Hamilton RJ, Simms E, Paul R, Hermens D, Gordon E.
Spontaneous alpha peak frequency predicts working memory performance across the age
span. Int J Psychophysiol 2004;53:1–9.
26. Duverne S, Lemaire P. Age-related differences in arithmetic problem-verification
strategies. J Gerontol B Psychol Sci Soc Sci 2004;59(3):135-142.
27. Eenshuistra RM, Ridderinkhof KR, van der Molen MW. Age-related changes in
antisaccade task performance: inhibitory control or working-memory engagement? Brain
Cogn 2004;56(2):177-188.
28. Hogan MJ. The cerebellum in thought and action: a fronto-cerebellar aging
hypothesis. New Ideas Psychol 2004;22:97–125.
29. Pichora-Fuller MK. Processing speed and timing in aging adults: psychoacoustics,
speech perception, and comprehension. Int J Audiol 2003;42Sup1:S59-S68.

21
30. Shimamura AP. Memory and the prefrontal cortex. Ann N Y Acad Sci
1995;769:151-159.
31. Lebo CP, Reddell RC. The presbycusis component in occupational hearing loss.
Laryngoscope 1972;82(8):1399-1409.
32. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: A practical method for
grading the state of patients for the clinician. J Psych Res 1975;12:189-198.
33. Grimault N, Micheyl C, Carlyon RP, Collet L. Evidence for two pitch encoding
mechanisms using a selective auditory training paradigm. Percept Psychophys 2002;64:189-
197.
34. Wechsler D. Weschsler Adult Intelligence Scale-III, San Antonio, TX: The
Psychological Corporation, 1997.
35. Verhelst W. Overlap-add methods for time-scaling of speech. Speech Comm 2000;
30:207–221.
36. Segal O, Kishon-Rabin L, Hildesheimer M. The effect of linguistic context on
speech perception of hearing impaired using hearing aid and cochlear implant. Dash (Dibur
VeShmia) 1999;21:85-99.
37. Boothroyd A. Auditory perception of speech contrasts by subjects with
sensorineural hearing loss. J Speech Lang Hear Res 1984;27(1):134-44.
38. Cohen G. Speech comprehension in the elderly: The effects of cognitive changes. Br
J Audiol 1987;21:221-226.
39. Benichov J, Cox LC, Tun PA, Wingfield A. Word recognition within a linguistic
context: effects of age, hearing acuity, verbal ability, and cognitive function. Ear Hear
2012;33(2):250-6.
40. Goldman-Eisler F. Psycholinguistics: Experiments in Spontaneous Speech, NY:
Academic press, 1968.

22
41. Huggins AWF. Distortion of the temporal pattern of speech: Interruption and
alternation. J Acoust Soc Am 1964;36:1055-1064.
42. McCabe J, Hartman M. Examining the locus of age effects on complex span tasks.
Psychol Aging 2003;18(3):562-572.
43. Humes LE. Speech understanding in the elderly. J Am Acad Audiol 1996;7(3):161-
167.
44. Lindenberger U, Baltes PB. Sensory functioning and intelligence in old age: a
strong connection. Psychol Aging 1994;9:39-355.
45. Park D, Lautenschlager G, Hedden T, Davidson NS, Smith AD, Smith PK. Models
of visuospatial and verbal memory across the adult life span. Psychol Aging 2002;17:299-
320.
46. Salthause TA, Rogan JD, Krill KA. Division of attention: age differences on a
visually presented memory task. Mem Cognit 1984; 12(6):612-630.
47. Singh-Manoux A, Kivimaki M, Glymour M, Elbaz A, Berr C, Ebmeier KP, Ferrie
JE, Dugravot A. Timing of onset of cognitive decline: results from Whitehall II prospective
cohort study. BMJ;2012:344
48. Schneider BA, Daneman M, Murphy DR, See SK. Listening to discourse in
distracting settings: the effects of aging. Psychol Aging 2000;15(1):110-125.

23
Table 1. Pearson Correlations between Age and Hearing Sensitivity
r
Click train 0.65***
1 kHz pure tone, 15msec duration 0.28**
1 kHz pure tone, 50msec duration -0.02
1.8 kHz pure tone, 15msec duration 0.55***
**p<.01; ***p<.001;
α = .01 after Bonferroni's correction for multiple comparisons was applied
24
Table 2. Hierarchical Linear Regressions Predicting Speech Perception in Quiet
β t R2cha Fcha
Step 1 051. 1.505
Click 227.- 1.357-
1 kHz tone,
15msec 234. 1.922
1.8 kHz tone,
15msec 123. 784.
Step 2 006. .243
Digit Span -.077 -.65
Matrices .053 .45
Step 3
Age -.069 -.480 .003 .230
Full model: R2 = .059, F (6,81) = .851, p > .05

25
Table 3. Hierarchical Linear Regressions Predicting Speech Perception in White Noise
β t R2cha Fcha
Step 1 .101 3.135*
Click -.121 -.756
1 kHz tone,
15msec -.280 -.236*
1.8 kHz tone,
15msec .082 .538
Step 2 .026 1.198
Digit Span .030 .271
Matrices .154 1.346
Step 3
Age .001 .139
-.052 -.373
* p < .05
Full model: R2 = .128, F (6,81) = 1.976, p > .05

26
Table 4. Hierarchical Linear Regressions Predicting Speech Perception in Speech Noise
β t R2cha Fcha
Step 1 .195 6.792***
Click -.402 -2.647**
1 kHz tone,
15msec -.049 -.437
1.8 kHz tone,
15msec -.018 -.127
Step 2 .010 .506
Digit Span .105 .983
Matrices -.058 -.533
Step 3
Age .076 8.570**
-.367 2.928**
* p < .05, ** p < .01, *** p < .001
Full model: R2 = .281, F (6,81) = 5.279, p < .001

27
Table 5. Hierarchical Linear Regressions Predicting Speech Perception for Speech
Compressed at 60% Compression Rate
β t R2cha Fcha
Step 1 .067 2.02
Click .179 1.093
1 kHz tone,
15msec -.292 -2.418*
1.8 kHz tone,
15msec -.054 -.351
Step 2 .011 .510
Digit Span -.017 -.148
Matrices -.105 -.892
Step 3 .050 4.62*
Age -.297 -2.148*
* p < .05
Full model: R2 = .128, F (6,87) = 1.99, p > .05
28
Table 6. Means (percept correct) and Standard Deviations of Accuracy Rates for Speech
Perception by Speech Condition
Note: Means with different subscripts are significantly different (p < .05).
Mean SD
Speech in quiet .985a .041
Speech in speech noise .859b .087
Speech in white noise .710c .090
60% compressed speech .959d .029

29
A.
B.
C.
D.
Figure 1. Speech perception accuracy (percent correct) by age for four conditions used in the
study: A. Speech perception in quiet; B. Speech perception in speech noise; C. Speech
perception in white noise; D. Time-compressed speech perception in 60% compression rate

30




















![[756] HEARING IN CERTAIN ORTHOPTERA · Hearing in certain orthoptera 759 Fig. 1 shows graphs relating the threshold intensity in decibels to frequency of a pure tone stimulus for](https://img.pdfslide.us/doc/110x75/5e86810f7ace8239892ef11c/756-hearing-in-certain-orthoptera-hearing-in-certain-orthoptera-759-fig-1-shows.jpg)







