Embed Size (px)
Citation preview

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
26 Journal of Dental Sciences and Research
Case Report
Aggressive Juvenile Ossifying Fibroma of the Anterior
Mandible
Dr.Ravikumar.R1, Dr.Raghavendra.K2, Dr.Santhosh Kumar3
1Senior Lecturer, 2Reader Department of Oral Surgery, 3Senior Lecturer Departmant
of Periodontics, Sri Siddhartha Dental College, Tumkur, Karnataka.
Abstract:
Juvenile ossifying fibroma (JOF) is an uncommon fibro-osseous lesion
containing different amounts of calcified tissue scattered in a cellular
fibroblastic stroma. bones. It is highly aggressive and has a strong tendency
to recur. It has been recognized as a separate histopathological entity
among the fibro-osseous group of lesions. The clinical behavior of Juvenile
ossifying fibroma is variable and difficult to predict. This article reports a
case of Aggressive JOF of the anterior mandible in a 10 year old girl.
Key words: ossifying fibroma; fibro-osseous lesion; juvenile ossifying
fibroma; psammomatoid; trabecular; active fibrous dysphasia.
Journal of Dental Sciences & Research 2:1: Pages 26-34
Introduction:
The fibro osseous lesions of
the jaws represent a diverse group
of entities that are characterized by
replacement of normal bone by a
fibrous connective tissue matrix,
with in which varying amounts of
osteoid, immature and mature bone
and in some instances, cementum-
like material are deposited1. Fibro
osseous lesions of the jaws include
developmental (hamartomatous)
lesions, reactive or dysplastic
processes and neoplasms.
One such rare or atypical fibro
osseous lesion is Juvenile ossifying
Fibroma (JOF). The term JOF
describes two distinct
histopathological variants:
Psammomatoid and Trabecular
varieties2 .Psammomatoid JOF is an
extra-gnathic lesion occurring

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
27 Journal of Dental Sciences and Research
predominantly in the sinonasal and
orbital bones. Trabecular JOF is a
gnathic lesion affecting the jaws with
a predilection for maxilla2, 3, 4. Cases
affecting the mandible have been
reported; the ramus- molar area
being the most common site3. This
presentation highlights the third
documentation of a JOF occurring in
the mandibular anterior region; thus
making it a rare entity.
Case report:
A 10-year-old girl presented to the
department of oral and maxillofacial
surgery with a rapidly enlarging
mass of 20days duration over the
mandibular anterior region[Figure-
1]. On physical examination, an
ovoid, firm, intra oral swelling,
measuring about 3x3 cm; in relation
to 31, 32, 41 and 42, slightly
extending into the floor of the mouth
with minimal tenderness on
palpation and no significant regional
lymphadenopathy.There was Lateral
displacement with gradeII mobility
of permanent mandibular incisors
and deciduous mandibular
canines[Figure-2a,b].
Panoramic and intra-oral periapical
radiographs revealed a radiolucent
mass in the symphyseal region
displacing 31, 32, 41 and 42
laterally and perforating both the
cortical plates of the mandible
[Figure-3a, b].
CT scan revealed an expansile
osteolytic mass, encompassing
symphysis of the mandible causing
splaying of the incisors; with an
intact lower mandibular border. Few
bony spicules were seen with in the
lesion [Figure-4 a,b].
Routine blood examination and
biochemical investigations were with
in the normal limits. An incisional
biopsy was performed, fixed in 10%
formalin and sent for
histopathological examination.
Correlating the age, duration, clinical
behavior, radiological pattern and
microscopic appearance [Figure-
5a,b,c],the lesion was diagnosised
as “Aggressive JOF(Trabecular
variant).” Under general
anaesthesia, an enbloc resection was
carried out through a trans-oral
approach followed by chemical

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
28 Journal of Dental Sciences and Research
cauterization using carbolic
acid[Figure-6 a,b,c]. The
postoperative recovery was un
eventful without a significant
problem[Figure-6c]. The patient was
reviewed regularly and on a follow
up of one year, showed no signs of
recurrence[Figure-8&9].
Discussion:
The most characteristic feature of
JOF, as the name suggests, is its
higher incidence in children and
young adults.5,6 However, it can also
occur in the older age-groups4.
Johnson et al 5 have reported JOFs
occurring at any age between 3
months and 72 years. Among the
many classification systems for this
lesion, the classification by Slootweg
et al 7 is noteworthy. They have
classified JOF into two distinct
groups, the JOF-WHO type and JOF-
PO (psammoma-like ossicles) type,
based primarily on the difference in
the age of occurrence: the mean age
of occurrence of JOF-WHO is 11.8
years and that of JOF-PO is 22.6
years. 2The most recent classification
is by El-Mofty [4] who identified two
categories, trabecular JOF (TrJOF)
and psammomatoid JOF (PsJOF),
based on histologic criteria.
However, the two categories also
have a distinct predilection for
specific age-groups: the average age
of occurrence of TrJOF is 8½-12
years, whereas that of PsJOF is 16-
33 years.4
Although JOF can occur anywhere in
the skeleton, its highest incidence is
in the facial bones, most commonly
the maxilla.3,4,5,8 One clinical feature
that helps differentiate TrJOF from
PsJOF is the site of involvement,
with PsJOF occurring mainly in the
paranasal sinuses and TrJOF
occurring mainly in the maxilla.4
Mandibular and extracranial
involvement is rare.5
Gender predilection has been a
matter of controversy, with some
authors claiming no predilection for
either sex, whereas Johnson et al .
found a higher incidence in females
3,5 and El-Mofty reported a male
predilection.4

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
29 Journal of Dental Sciences and Research
The histogenesis of this lesion is
poorly understood.Johnson et
al.believe that mandibular
lesions arise from the myxoid dental
papilla of the developing tooth.
Virtanen et al. consider JOF as a
neoplasm that develops from the
undifferentiated cells of the
periodontal ligament.4
JOF usually manifests as an
asymptomatic bony-hard swelling,
the duration and extent of which
may vary depending on the site and
aggressiveness of the lesion;
however, it does not demonstrate
the chronic, long-standing evolution
of some of the other fibro-osseous
lesions. It can expand the involved
bones, causing facial asymmetry.
Depending on the site, symptoms
such as pain, paresthesia,
malocclusion, sinusitis, proptosis,
etc., can also occur due to the
swelling.8,9
In general, JOF has a more
aggressive growth pattern than the
adult variant of ossifying
fibromas.They are usually
asymptomatic, exhibit rapid growth
of the involved site and the first
presentation will be a clinically
obvious swelling.
All these features were seen in our
case.
Radiographically the internal
structure can be radiolucent, mixed,
or radiopaque, depending on the
degree of calcification.3,4 Root
displacement is common and
resorption, though rare, can
occur.4,8,9 The lesion can cause
expansion as well as perforation.4
The radiographic features of JOF can
resemble that of other lesions, such
as fibrous dysplasia and cemento-
ossifying fibroma. 2,4JOF is not
capsulated but is separated from
surrounding bone by a radiopaque
border, 3,8and this finding can help in
differentiating it from fibrous
dysplasia.3,10 A 'ground-glass'
appearance on radiographs has been
reported.4 It usually has a concentric
or centrifugal growth pattern, which
can lead to an erroneous clinical
diagnosis of cemento-ossifying
fibroma.8,10 JOF has also been
reported to be associated with other

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
30 Journal of Dental Sciences and Research
bony lesions such as aneurysmal
bone cyst.4 Aggressive lesions with
marked destruction of adjacent
structures may radiographically
mimic osteogenic sarcoma. 8,9
The microscopic features of the
lesion are distinctive and include a
cell-rich fibrous stroma containing
bands of cellular osteoid without
osteoblastic lining, osteoid strands,
and trabeculae of woven bone.4,7,10
PsJOF is slightly more cellular than
TrJOF. Due to the resemblance of
the psammoma-like ossicles seen in
PsJOF to the cementicles in
cemento-ossifying fibroma, it has
been argued that PsJOF is a type of
cemento-ossifying fibroma.
2,4However, the marked cellularity of
JOF is in sharp contrast to the
usually stroma-rich appearance of
the latter group of lesions.
The aggressive nature of this entity,
along with the reported high rates of
recurrence (30-58%), 4,8 suggests
that JOF should be treated like a
locally aggressive neoplasm, very
much like an ameloblastoma.
Surgical resection, rather than
conservative curettage, is therefore
the preferred line of treatment.6,8 In
the present case we followed
modified Troulis et al’s staged
protocol for the treatment of the jaw
tumours in children.
Conclusion:
Although JOF is an uncommon
clinical entity, its aggressive local
behaviour and high recurrence rate
calls for an early diagnosis, prompt
treatment and
especially, long term follow up of the
patient.The rapid growth rate often
exhibited by these lesions can be
quite alarming and cause the
clinician to suspect the presence of a
malignancy.
FIGURE-1: A 10-year-old girl presented
with a rapidly enlarging mass of 20 days
duration over the mandibular anterior
region.

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
31 Journal of Dental Sciences and Research
Figure 2a:
Figure 2b:
FIGURE-2a, b: Local examination reveals an
ovoid, firm, intra oral swelling, measuring
about 3x3 cm; in relation to 31,32, 41 and
42, slightly extending into the floor of the
mouth and causing lateral displacement of
the above mentioned teeth.
Figure 3a:
Figure 3b:
FIGURE-3a, b: OPG and IOPA radiographs
revealed a radiolucent mass in the
symphyseal region displacing 31, 32, 41
and 42 laterally and perforating both the
cortical plates of the mandible.
Figure-4a:
Figure-4b: FIGURE-4a, b: CT revealed a
well-defined radiolucent expansile mass
encompassing symphysis of the mandible
causing splaying of the incisors; with an
intact lower mandibular border. Few bony
spicules were seen with in the lesion.
Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
32 Journal of Dental Sciences and Research
Figure-5a
Figure-5b:
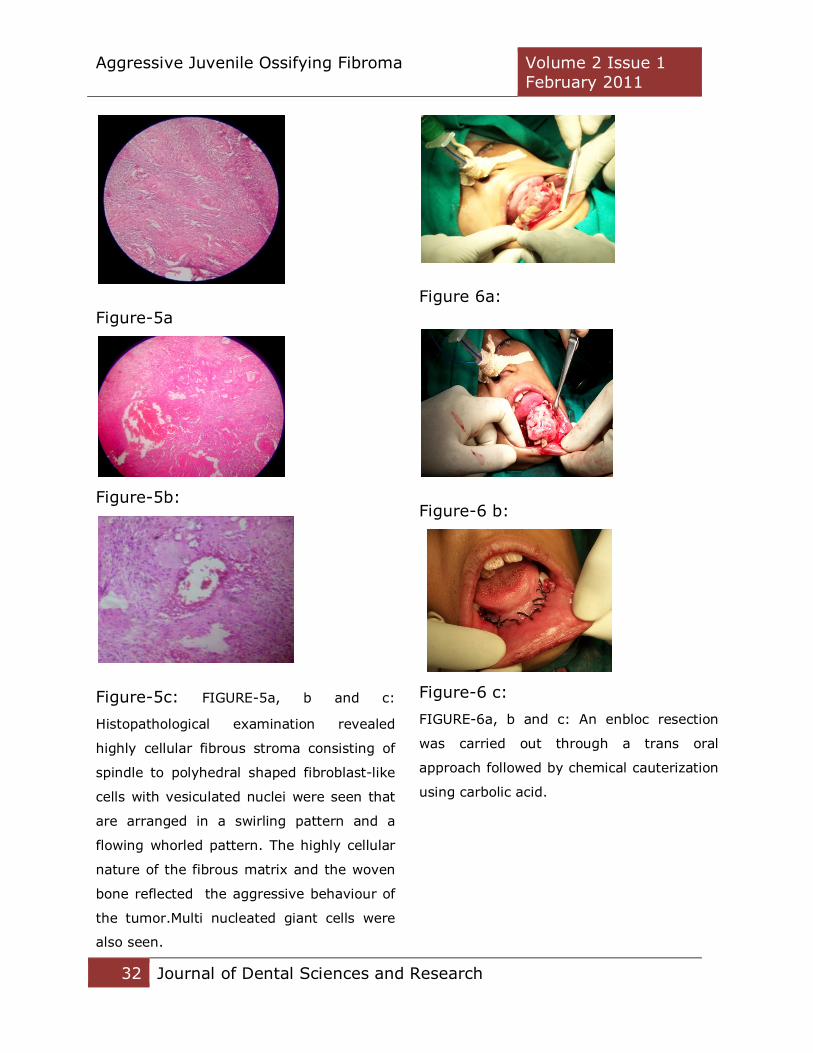
Figure-5c: FIGURE-5a, b and c:
Histopathological examination revealed
highly cellular fibrous stroma consisting of
spindle to polyhedral shaped fibroblast-like
cells with vesiculated nuclei were seen that
are arranged in a swirling pattern and a
flowing whorled pattern. The highly cellular
nature of the fibrous matrix and the woven
bone reflected the aggressive behaviour of
the tumor.Multi nucleated giant cells were
also seen.
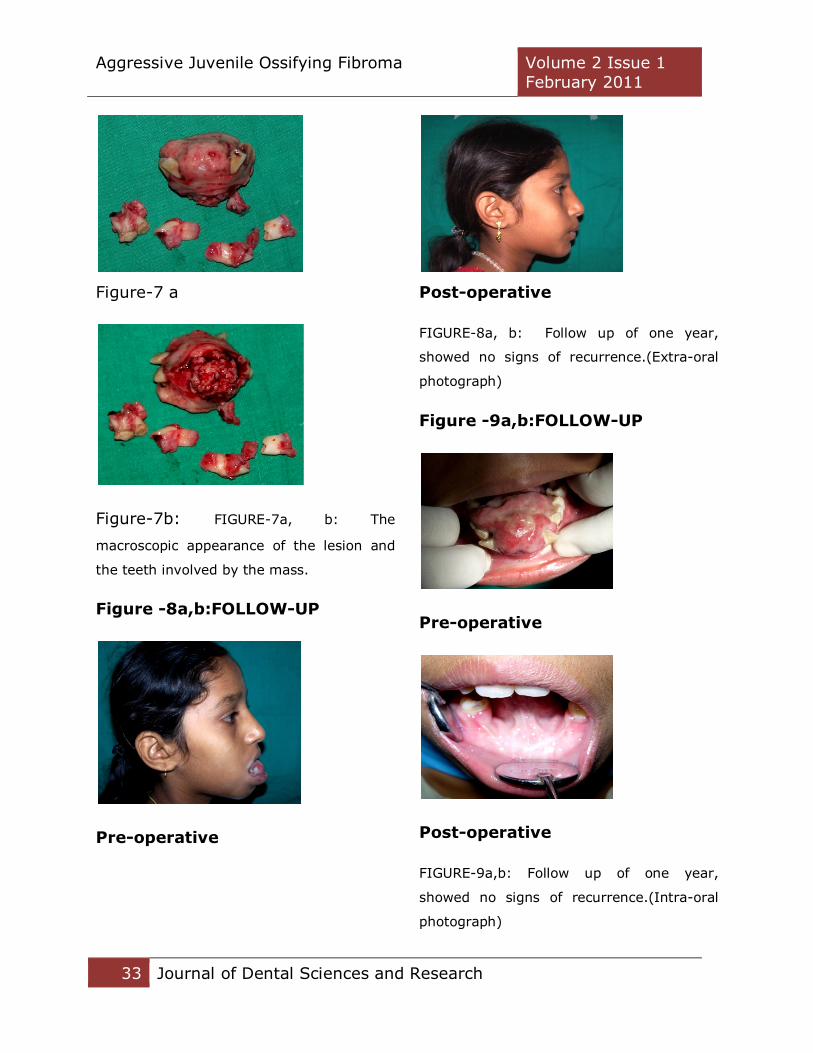
Figure 6a:
Figure-6 b:
Figure-6 c:
FIGURE-6a, b and c: An enbloc resection
was carried out through a trans oral
approach followed by chemical cauterization
using carbolic acid.
Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
33 Journal of Dental Sciences and Research
Figure-7 a
Figure-7b: FIGURE-7a, b: The
macroscopic appearance of the lesion and
the teeth involved by the mass.
Figure -8a,b:FOLLOW-UP
Pre-operative
Post-operative
FIGURE-8a, b: Follow up of one year,
showed no signs of recurrence.(Extra-oral
photograph)
Figure -9a,b:FOLLOW-UP
Pre-operative
Post-operative
FIGURE-9a,b: Follow up of one year,
showed no signs of recurrence.(Intra-oral
photograph)

Aggressive Juvenile Ossifying Fibroma
Volume 2 Issue 1
February 2011
34 Journal of Dental Sciences and Research
References
1.Rinaggio J, Land M, Cleveland DB.
Juvenile ossifying fibroma of the
mandible. J Pediatr Surg
2003;38:648-50.
2. Philipsen HP, Reichert PA.
Ossifying fibroma, odontogenic
tumors and allied lesions. London:
Quintessence Publishing Co, Ltd;
2004.
3. Saiz-Pardo-Pinos AJ, Olmedo-
Gaya MV, Prados-Sαnchez E,
Vallecillo-Capilla M. Juvenile
ossifying fibroma: A case study. Med
Oral Patol Oral Cir Bucal
2004;9:454-8.
4. El-Mofty S. Psammomatoid and
trabecular juvenile ossifying fibroma
of the craniofacial skeleton: Two
distinct clinicopathologic entities.
Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2002;93:296-304.
5. Johnson LC, Yousefi M, Vinh TN,
Heffner DK, Hyams VJ, Hartman KS.
Juvenile active ossifying fibroma: Its
nature, dynamics and origin. Acta
Otolaryngol Suppl 1991;488:1-40.
6. Zama M, Gallo S, Santecchia L,
Bertozzi E, De Stefano C. Juvenile
active ossifying fibroma with
massive involvement of the
mandible. Plast Reconstr Surg
2004;113:970-4.
7. Slootweg PJ, Panders AK,
Koopmans R, Nikkels PG. Juvenile
ossifying fibroma: An analysis of 33
cases with emphasis on
histopathological aspects. J Oral
Pathol Med 1994;23:385-8.
8. Noffke CE. Juvenile ossifying
fibroma of the mandible: An 8 year
radiological follow-up.
Dentomaxillofac Radiol
1998;27:363-6.
9. Offiah C, Hall E. The rapidly
enlarging chin mass. Br J Radiol
2005;78:175-6.
10. Williams HK, Mangham C,
Speight PM. Juvenile ossifying
fibroma: An analysis of eight cases
and a comparison with other fibro-
osseous lesions. J Oral Pathol Med
2000;29:13-8.





























