Embed Size (px)
Citation preview

Agenda Item: 2.4
REPORT TO THE TRUST BOARD MEETING IN PUBLIC 26 SEPTEMBER 2013
Title
Infection Control Annual Report 2012-13
Lead Director
Director of Nursing & Quality, Lynne Wigens
Author(s)
Head of Infection Control, Grant Crawshaw
Purpose
For Information
Previously considered by
Hospital Infection Control Committee 25 September 2013
Executive Summary
Achievement of HCAI reduction targets in Clostridium difficile
Missed MRSA bacteraemia target (2 cases against a target of 1)
Overview of infection prevention actions within the hospital to meet the challenges and approve objectives for Infection Control for 2013/14
Related Trust Objectives Sub-objectives
To provide safe, reliable, personal & responsive care
Processes for improving and measuring infection control
Risk and Assurance
Assurance on infection prevention actions
Related Board Assurance Framework Entries
N/A
Financial Implications
Penalties for non achievement of infection prevention targets
Legal Implications/Regulatory Requirements
Health and Social Care Act 2008
Code of Practice for health and social care on the prevention and control of infections and related guidance
CQC Outcome 8 - Cleanliness and Infection Control
Action Required by the Board The Trust Board is asked to receive the report

1
Infection Prevention and Control
Annual Report
April 2012 - March 2013

2
Contents
Executive summary ........................................................................................................................... 3
1 Compliance Criterion One ........................................................................................... 4 1.1 Risk assessment ............................................................................................................. 4 1.2 Director of Infection Prevention and Control .................................................................. 4 1.3 Assurance Framework .................................................................................................... 5 1.4 Infection Prevention and Control Programme ................................................................ 5 1.5 Infection Prevention and Control Infrastructure .............................................................. 5 1.6 Movement of Patients ..................................................................................................... 5
2 Compliance Criterion Two ....................................................................................................... 6 2.1 Policies on the Environment ........................................................................................... 6 2.2 Cleaning Services ........................................................................................................... 6 2.3 Decontamination ............................................................................................................. 7 2.4 Linen, Laundry and Dress .............................................................................................. 8
3 Compliance Criterion Three .................................................................................................... 8
4 Compliance Criterion Four ...................................................................................................... 9
5 Compliance Criterion Five ....................................................................................................... 9
6 Compliance Criterion Six ......................................................................................................... 9
7 Compliance Criterion Seven ................................................................................................. 10
8 Compliance Criterion Eight ................................................................................................... 11 8.1 Laboratory Support ....................................................................................................... 11
9 Compliance Criterion Nine .................................................................................................... 12 9.1 Policies ......................................................................................................................... 12 9.2 Policy Audit ................................................................................................................... 12 9.3 Hand Hygiene Audit ...................................................................................................... 12 9.4 High Impact Interventions Audits .................................................................................. 12 9.5 Antibiotic Stop/Review Date and Indication Policy Audit .............................................. 13
10 Compliance Criterion Ten ...................................................................................................... 14 10.1 Occupational Health Services ...................................................................................... 14 10.2 Induction, Training Programmes and On-going Education .......................................... 15
11 Education Strategy .................................................................................................................. 15
12 Performance against National Targets .............................................................................. 16 12.1 National Surveillance .................................................................................................... 16 12.2 MRSA Bacteraemias .................................................................................................... 16 12.3 MRSA screening ........................................................................................................... 18 12.4 MSSA Bacteraemias..................................................................................................... 19 12.5 Clostridium difficile ........................................................................................................ 19 12.6 Surgical Site Infection Surveillance .............................................................................. 20 12.7 Glycopeptide-Resistant Enterococci Bacteraemias (GRE) .......................................... 20
13 Outbreaks and Untoward Incidents .................................................................................... 20 13.1 Norovirus ...................................................................................................................... 20
14 Finance ....................................................................................................................................... 21 14.1Budget Allocation and Financial Investment ..................................................................... 21
15 Key objectives for 2013/14 Annual plan............................................................................. 21
Appendix A - Infection Prevention and Control Team Accountability Framework......... 23
Appendix B - Infection Control Annual Audit Work Plan delivered 12/13 ......................... 24
Appendix C - Abbreviations used in this document ............................................................... 25

3
Executive summary
The Annual Report of the Director of Infection Prevention and Control provides information on the progress of all the Infection Control activities throughout the year 2012-13. The report seeks to demonstrate a Hospital-wide commitment to the prevention and control of Healthcare Associated Infections (HCAIs).
The Hospital has on the whole performed well against the key Infection Prevention and Control (IPC) targets from the Department of Health (DH), attaining the reduction targets in Clostridium difficile (C difficile) cases (27) but unfortunately missing the target of one MRSA bacteraemia by having two cases.
The target for cases of C difficile was fewer than 27 cases. The hospital reported 27 so we were precisely on target. All cases were thoroughly investigated and in the few cases which were deemed avoidable actions have been taken.
The challenges linked to the management of patients with a diagnosis of suspected infection in hospital continues and the actions taken in response to these are outlined within this report.

4
Compliance with The Health and Social Care Act 2008: Code of Practice for health and adult social care on the prevention and control of infections and related guidance.
1 Compliance Criterion One
Systems to manage and monitor the prevention and control of infection. These systems use risk assessments and consider how susceptible service users are and any risks that their environment and other users may pose to them.
The Trust Board recognises its responsibilities for overseeing infection control arrangements across the hospital guided by Compliance Criterion One. This includes the Infection Prevention and Control Policy which outlines individual and the Trust‟s collective responsibility for keeping to a minimum the risks of infection and the general means by which it will prevent and control such risks. The Infection Prevention and Control Policy was reviewed in June 2012 and is published on the Ipswich Hospital website.
1.1 Risk assessment
Infection prevention and control (IPC) is included in all Executive objectives and individual Directors are identified as responsible for the implementation of specific areas of the IPC strategy.
The Trust Board receives monthly Infection Control (IC) performance reports, quarterly updating on compliance with the Health Act and an annual report.
Compliance with the Health Act and any action plans pertaining to infection prevention and control are monitored through the Hospital Infection Control Committee (HICC), Risk Management Committee and the Trust Board.
All operational areas have submitted regular performance reports to the HICC.
IPC performance is discussed at meetings with the DIPC and CEO and monitored through the operational area Risk and Governance meetings.
IPC has its own risk register maintained by the Head of Infection Control and considered at both HICC and the Risk Management Committee. It is reviewed at a minimum on a quarterly basis to ensure it remains relevant.
1.2 Director of Infection Prevention and Control
The Director of Nursing (DoN) is the Director of Infection Prevention and Control, and this has been in the remit of the role since April 2007.
The DoN‟s job description and objectives reflect the responsibilities set out in Winning Ways: working together to reduce Healthcare Associated Infections in England (DH 2003).
The DoN meets formally with the CEO on a monthly basis and as a member of the Trust Board reports on infection prevention and control at each meeting, including taking questions at the public board meetings.
The DIPC directly manages the Head of Infection Control and this includes at least monthly one to one meetings.
This is the sixth annual report presented by the DIPC to the Trust Board. It is also published on the Ipswich Hospital website and made available to the public.

5
1.3 Assurance Framework
The Hospital has an Infection Prevention and Control Strategy. This sets out the clear objective for the Hospital of ensuring that patients‟ safety in respect of IPC is delivered. This strategy is currently under review for 13/14.
IPC is contained within the Integrated Performance report as a standing agenda item for the Trust Board and is included in the public board meetings. A more detailed report which includes performance against targets, audit results, incidents and outbreaks and updates any on-going action plans is reported monthly at HICC.
All operational clinical areas submit a monthly highlight report to the HICC which details essential elements for IPC such as compliance with staff training, hand hygiene, antibiotic prescribing and cleanliness of environment and equipment.
IPC performance within operational clinical areas is discussed and is monitored through the operational clinical area Risk and Governance meetings.
Root cause analysis is undertaken on all cases of Clostridium difficile and MRSA and MSSA bacteraemias that are hospital apportioned. Any case not hospital apportioned is investigated to identify any links to the hospital.
The assurance process includes both internal and external measures. Internally the accountability is exercised via HICC ensuring that there is internal scrutiny of compliance with national standards, local policies and clinical practice. External assurance is obtained through the Care Quality Commission (CQC) registration and unannounced visits, assessment by the National Health Service Litigation Authority (NHSLA) against their standards for infection control and the Patient Environment Action Teams (PEAT).
1.4 Infection Prevention and Control Programme
The infection prevention and control programme is published annually and areas of the audit programme are monitored through the monthly performance report.
The annual programme for 2012-2013 is attached at Appendix C and includes details of audit and policy revision.
1.5 Infection Prevention and Control Infrastructure
The Infection Prevention and Control Team structure is attached at Appendix B.
The budget for Infection Control is held by the Head of Infection Control.
There are two Consultant Microbiologists.
The DoN is the Director of Infection Prevention and Control.
The Medical Director has the role of Infection Control Doctor.
1.6 Movement of Patients
The movement of patients is one of the most significant aspects of infection control management particularly in an outbreak situation. A great deal of time is spent daily ensuring patient safety when relocating patients. The team also advises regarding prioritisation of patients for isolation/single rooms.
There are daily meetings (Monday to Friday) between the ICT and the Hospital Co-ordinators to ensure that all patients requiring isolation are appropriately placed

6
and to prioritise through risk assessment the best use of those resources available. The compliance with the isolation policy is monitored through monthly audit and reported in the Infection Prevention and Control monthly report. The Head of Infection Control is available for advice out of hours and at weekends via the Hospital Coordinator, and there is an on-call arrangement for microbiology medical advice.
The Patient Placement Policy is monitored by the Hospital Co-ordinators to minimise the number of non-clinical moves.
2 Compliance Criterion Two
Provide and maintain a clean and appropriate environment which facilitates the prevention and control of HCAI.
The Director of Infection Prevention and Control is the decontamination lead for the Hospital.
The Director of Finance and Performance is the designated lead for environmental cleaning. As high standards of cleaning are vital to the control of infection, this post is supported by the DIPC, the ICT and the Matrons and Ward Sisters/Charge Nurses in assuring any shortfalls are identified and rectified.
The Hotel Services contract was awarded to ISS in October 2010; the specification for the contract was based on The National Specifications for Cleanliness in the NHS: a framework for setting and measuring performance outcomes. (National Patient Safety Agency. The National Specifications for Cleanliness in the NHS: A framework for setting and measuring performance outcomes, 1st April 2007). The contract review group meets regularly and includes the Head of Infection Control and designated Matrons.
2.1 Policies on the Environment
The Food Hygiene and Pest Control Policies were implemented in November 2010, and updated as required.
Other policies are in line with the requirements of the revised Health and Social Care Act 2008.
The Management of the Estate is laid out in the Estates Strategy (published 2012/13) available on the Ipswich Hospital website.
2.2 Cleaning Services
All inpatient areas are compliant with the recommended cleaning and audit frequencies as set out in The National Specifications for Cleanliness in the NHS: a framework for setting and measuring performance outcomes (April 2007).
Compliance with the above is reported to the HICC by each clinical operational area.
Equipment decontamination is audited monthly in all clinical areas. The target of 95% was agreed by the Hospital Infection Control Committee. The percentage average score for the month of February was 95%. This is the lowest reported score for this year to date (since April 2012). Identified failures are reported and

7
rectified within a set timescale as per NPSA National Specification for Cleanliness in the NHS 2007.
There are Cleaning Action Teams (CAT teams) in place that provide additional input such as decontamination of isolation rooms and provide cleaning services around the clock.
Monitoring is the responsibility of the IHT Contracts Manager whose duties include monitoring the compliance with the cleaning standards as set out in the National Specifications for Cleaning (2007).
2.3 Decontamination
The Director of Infection Prevention and Control is the Trust‟s decontamination lead.
Responsibility for decontamination is identified in the Decontamination and Disinfection Policy. This Policy will be reviewed in 2013.
All reusable surgical instruments (excluding only flexible endoscopes) are reprocessed through the hospital‟s centralised sterilisation unit.
In 2012/13 the Ipswich Hospital Trust Board achieved the recommendation for a separate HSDU for this hospital through refurbishment of the existing unit. Both the CQC and the Department of Health were kept informed of the progress of this work, which has now completed.
Flexible endoscopes are decontaminated locally at the point of use. The areas undertaking this have been audited against the National Endoscopy Programme‟s Decontamination Standards for Flexible Endoscopes.
The facility for the centralised decontamination of endoscopes used in South Theatres and the Urology Investigation Suite (UIS) continues to operate and provide a robust audit trail for the decontamination of these instruments.
The age of the Automatic Endoscope Reprocessors, the need for JAG (Joint Advisory Group on GI Endoscopy) on-going accreditation and the problems associated with the use of Chlorine Dioxide for endoscope disinfection has prompted discussions around developing a revised/new decontamination facility.
90%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Apr'12 May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage
compliance
Target

8
The provision of a centralised mattress decontamination service for dynamic mattresses continues to provide pressure relieving mattresses ready for patient use to the ward staff.
A steam cleaning system for equipment (thermal clean) was developed by the ICT in collaboration with the ISS Contracts Manager and ISS to further reduce the risk of residual contamination. This is used by the previously mentioned CAT team.
2.4 Linen, Laundry and Dress
In order to facilitate good standards of hand hygiene the Hospital follows the “bare below the elbows” guidance and this is endorsed in the Uniform Policy and Dress Code. The policy also identifies key measures required for the appropriate decontamination of uniforms and clothing worn by staff having patient contact.
Compliance with the Uniform Policy and Dress Code has been monitored monthly and included in the Quality Management System reports.
3 Compliance Criterion Three
Provide suitable accurate information on HCAI to the service users and their visitors.
The Infection Prevention and Control Policies are made available to the public on the hospital‟s website as they are reviewed and updated. This includes both the Infection Prevention and Control Strategy and Policy.
Infection control advice is available at all times including out of hours to IHT Staff.
The monthly performance reports are made available to the public on the hospital‟s website.
Leaflets giving information and advice about specific infections are available as well as information about “being a good visitor” that contains general information about hand hygiene and not visiting relatives and friends if unwell.
Voluntary Services staff were also involved in „meet and greet‟ infection control training where they are able to provide information to visitors and gave practical demonstrations on hand hygiene to visitors using the ultra violet light box.
Alcohol hand gel is available at the entrance to all departments and visitors and patients are encouraged to use it by both posters and reception staff as appropriate.
In areas such as lavatories there are signs informing patients and their visitors of what to do if they are dissatisfied with the cleanliness. These are also available in general clinical areas.
In the case of an outbreak, signs are used to inform visitors of the problem and patients‟ relatives are kept informed by telephone if visiting is suspended.
Each ward area has information displaying individual ward or department performance in hand hygiene and environmental cleanliness.
All information developed for patients or their visitors is agreed through patient/ user group review before publication by Design & Print Services.

9
4 Compliance Criterion Four
Provide suitable accurate information on infections to any person concerned with providing further support or nursing/medical care in a timely fashion.
Information on infections specific to an individual patient is included in the patient‟s discharge summary and there is a specific area on the electronic discharge system. In addition the GPs of all patients identified as having Clostridium difficile are sent a letter at the time of the identification of the infection.
Patients who may have been exposed to infections such as in a confirmed outbreak of Norovirus are not discharged to any other institutions until the end of the outbreak.
Patients with a significant infection will be seen by a member of the ICT and will be given information as well as the opportunity to ask questions, in a small number of instances this information will be imparted by senior nursing/medical staff on behalf of the ICT.
5 Compliance Criterion Five
Ensure that patients who have or develop an infection are identified promptly and receive the appropriate treatment and care to reduce the risk of passing on the infection to other people.
All patients identified with MRSA are “flagged” on their electronic patient records so that they are easily identified to all staff on subsequent admissions to facilitate their appropriate care.
Microbiology results are available to staff with access to the hospital‟s intranet and an appropriate password. In addition, results can also be sourced through the electronic system used to request the tests.
Policies regarding the management of patients with specific infections are available on the intranet to all staff to ensure that patients are managed appropriately to reduce the risk of transmission to other patients and/or staff.
The placement of all patients identified as having, or of being suspected as having, an infection is reviewed daily by one of the Infection Control Nurses (ICNs).
All clinical operational areas have Clinical Champions, Clinical Leads and Matrons who all have specific responsibilities within these roles for infection prevention and control practice.
The most important system of early identification is the surveillance system which collects data from a variety of databases to provide the Infection Control Team with the current status of patients with infection in the hospital. The current system (ICNET) is in the process of review and determining the needs for 13/14 onwards.
6 Compliance Criterion Six
Ensure that all staff and those employed to provide care in all settings are fully involved in the process of preventing and controlling infection.
All permanent and bank staff are required to attend an induction session which includes a session on Infection Prevention and Control based on the Standard Principles for Preventing Healthcare Associated Infections in Hospital Policy.

10
Specific induction sessions are provided for locum medical staff.
Infection Prevention and Control is part of the annual mandatory training required by all permanent and bank hospital staff and monitored through the mandatory training matrix. Specific in-house e-learning has been developed as an alternative to attending a face to face session.
All policies and guidelines are published on the Intranet to which all staff and permanent contractors have access.
The monthly and annual Infection Prevention and Control reports are published on the intranet and publicly on the Hospital‟s internet site.
Any external contractors undertaking temporary work (eg building or refurbishment) in the hospital are required to produce method statements and are supervised by the Estate and Facilities staff in line with the Managing Contractors Policy.
7 Compliance Criterion Seven
Provide or secure adequate isolation facilities.
The Management of Patients in Isolation Policy has been published. This outlines the care of all patients requiring isolation.
Compliance with the appropriate placement of patients is undertaken monthly. The following graph shows the isolation of patients in 2013. MRSA colonised is the largest single patient group requiring isolation and is an increasing challenge to the limited single room accommodation.
Compliance with the isolation policy for in-patients is audited for a five day period every month. The target was agreed at 100% by the Hospital Infection Control Committee. The following graph shows the total number of patient days that required isolation during the study period (120) and the number of days when appropriate isolation was not in place (27). Compliance was 77.50%.
Patients who cannot be isolated through lack of resources are formally risk assessed to ensure that the priority for the single room is given to the patient with
01020
30405060
708090
100
110120130
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2012 / 2013
Days Iso lated
Days not iso lated

11
greatest need. One of the ICNs reviews all patients requiring isolation daily in conjunction with the Hospital Co-ordinator.
The ICT is available to provide guidance on single room prioritisation, particularly in the acute admission areas (Brantham, Capel etc) where patient flow may be affected as a consequence of inappropriate use of the sideroom.
Elective and emergency patients are segregated as far as practicable within the Hospital with clear segregation of those patients who are to undergo elective surgical procedures both in general and orthopaedic surgery. During periods of high capacity the elective wards were used to accommodate emergency admissions.
The ICT are involved in capacity meetings at times of high capacity in the hospital to optimise the use of isolation facilities within the hospital.
The hospital has access to negative pressure rooms within Critical Care.
8 Compliance Criterion Eight
Secure adequate access to laboratory support.
8.1 Laboratory Support
Infection Prevention and Control activity remains high from a microbiology laboratory view. The following graph illustrates one area of this in the increasing number of MRSA screens being processed by the laboratory. Guidance is in the process of being revised regarding MRSA screening and once this is finalised will be adopted by IHT.
The laboratory works to standard operational procedures in line with best practice.
The laboratory has extended the availability of C difficile testing to seven days per week. This has reduced the time required for results to less than 24 hours in most
12
cases. This would also include the two stage testing of C difficile to identify the organism in the first stage and the toxin in the second.
The laboratory has also supported the ICT in research, training, trials and in particular specimen processing for everything from water safety issues to environmental sampling.
9 Compliance Criterion Nine
Have and adhere to appropriate policies, designed for the individual’s care and provider organisations, that will help to prevent and control infections.
9.1 Policies
5 Existing policies continue to be reviewed and updated systematically. 6 One new policy was developed and ratified this year: the Management of patients
with Mycobacterium tuberculosis.
9.2 Policy Audit
Assurance that the Infection Prevention and Control policies are being applied is sought through audit and is reported monthly in the Infection Prevention and Control performance report and as part of the QMS for each clinical operational area.
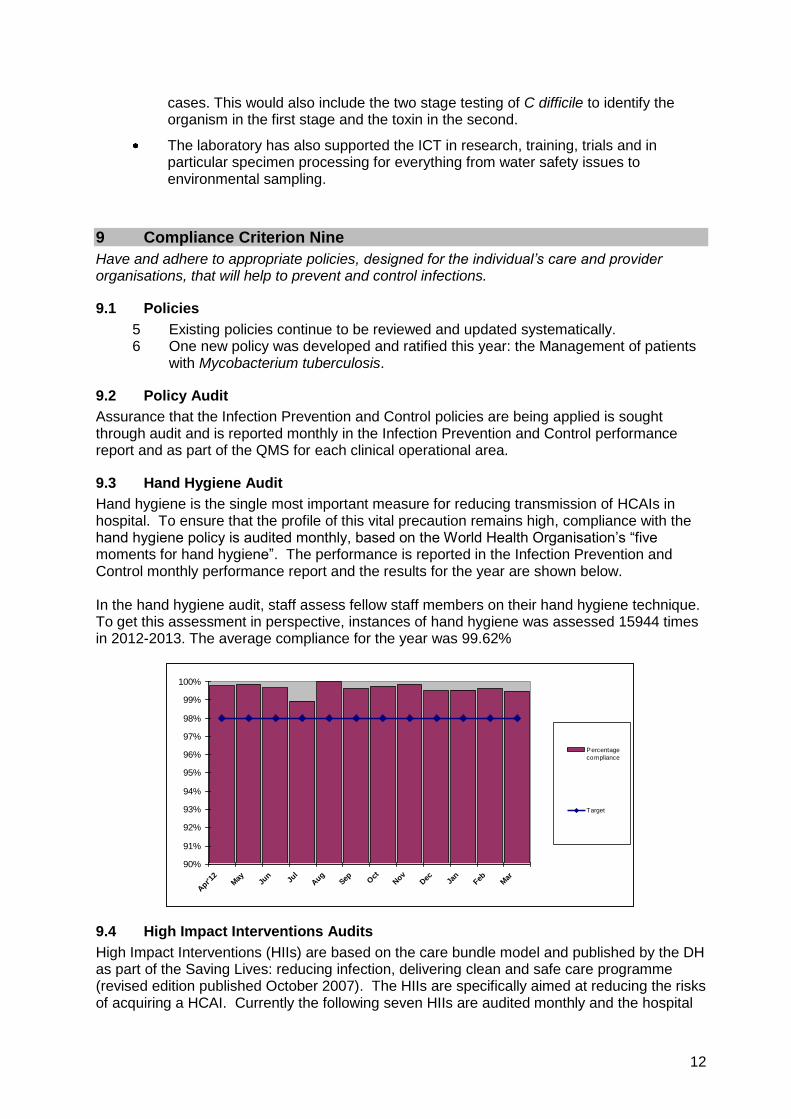
9.3 Hand Hygiene Audit
Hand hygiene is the single most important measure for reducing transmission of HCAIs in hospital. To ensure that the profile of this vital precaution remains high, compliance with the hand hygiene policy is audited monthly, based on the World Health Organisation‟s “five moments for hand hygiene”. The performance is reported in the Infection Prevention and Control monthly performance report and the results for the year are shown below. In the hand hygiene audit, staff assess fellow staff members on their hand hygiene technique. To get this assessment in perspective, instances of hand hygiene was assessed 15944 times in 2012-2013. The average compliance for the year was 99.62%
9.4 High Impact Interventions Audits
High Impact Interventions (HIIs) are based on the care bundle model and published by the DH as part of the Saving Lives: reducing infection, delivering clean and safe care programme (revised edition published October 2007). The HIIs are specifically aimed at reducing the risks of acquiring a HCAI. Currently the following seven HIIs are audited monthly and the hospital
90%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Apr'1
2M
ayJu
nJu
l
Aug
Sep Oct
Nov
Dec Ja
nFeb M
ar
Percentage
compliance
Target

13
wide results are included in the Infection Prevention and Control monthly reports with the individual clinical operational areas.
a. HII1 a&b - Insertion and on-going care of central venous devices. b. HII2 a&b - Insertion and on-going care of peripheral intravenous devices. c. HII3 a&b - Insertion and on-going care of renal dialysis catheters d. HII4 a&b - Preoperative and perioperative actions to prevent surgical site
infection e. HII5 a&b - Regular observations and on-going care for ventilated patients f. HII6 a&b - Insertion and on-going care of urinary catheters g. HII7 - Reducing the risk from Clostridium difficile
HII7 audit is carried out on each patient confirmed as having C difficile associated disease and every element of the care bundle has been carried out on each case attributed to the hospital for the whole of 2012-2013.
The high level of compliance with the HIIs is reflected in the performance against national targets. For example, the audits associated with the care of intravenous devices (HII one and two) illustrates the high standard of care provided to patients with these invasive devices. This is likely to be one of the factors in reducing not only MRSA bacteraemias but also those of Meticillin sensitive Staphylococcus aureus (MSSA).
HIIs are presented to HICC by a representative of each operational clinical area with explanation and actions if an area has not achieved the target. Some of the lower scores are reflective of the low denominator, where fewer patients have undergone the procedure (CVC Insertion) Sub optimal trends of are identified and actioned by the ICT as well as the Matron.
9.5 Antibiotic Stop/Review Date and Indication Policy Audit
Antibiotics are, without doubt, life saving drugs. However they are not without unwanted side effects and to reduce the risk of these, whilst maximising their therapeutic potential, antibiotics
14
need to be prescribed with care. The Antibiotic Review Group revise the antibiotic guidelines on a yearly basis.
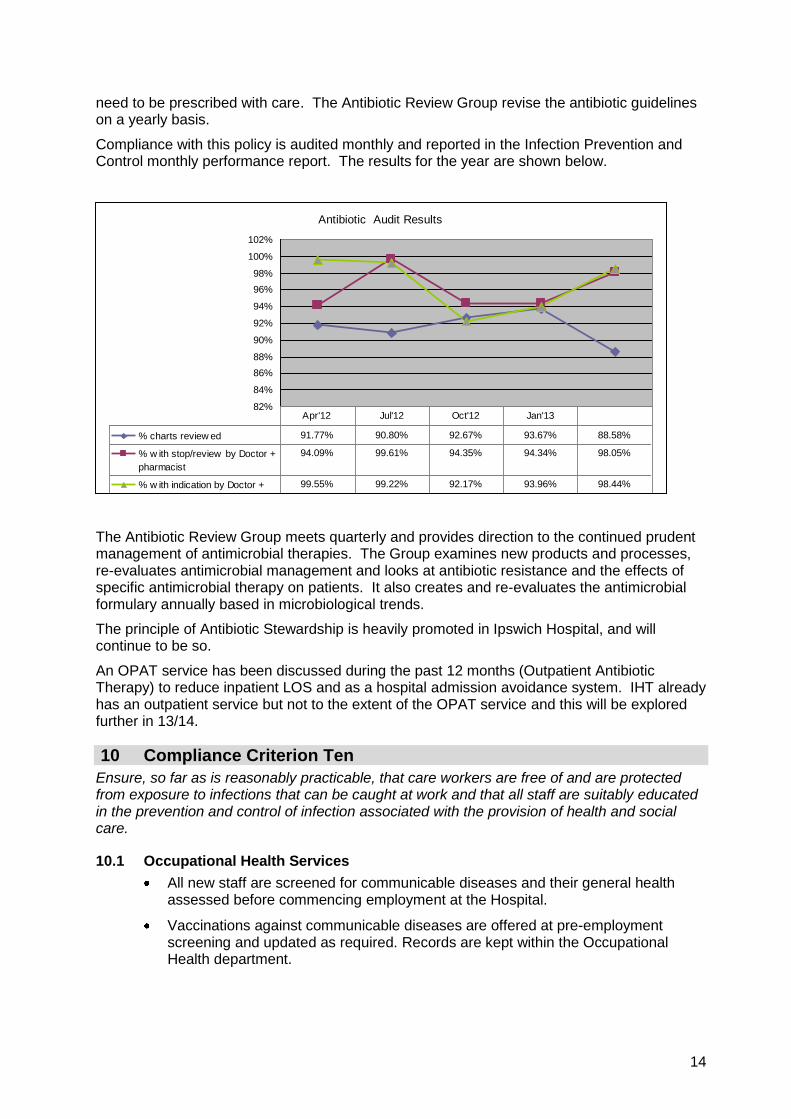
Compliance with this policy is audited monthly and reported in the Infection Prevention and Control monthly performance report. The results for the year are shown below.
The Antibiotic Review Group meets quarterly and provides direction to the continued prudent management of antimicrobial therapies. The Group examines new products and processes, re-evaluates antimicrobial management and looks at antibiotic resistance and the effects of specific antimicrobial therapy on patients. It also creates and re-evaluates the antimicrobial formulary annually based in microbiological trends.
The principle of Antibiotic Stewardship is heavily promoted in Ipswich Hospital, and will continue to be so.
An OPAT service has been discussed during the past 12 months (Outpatient Antibiotic Therapy) to reduce inpatient LOS and as a hospital admission avoidance system. IHT already has an outpatient service but not to the extent of the OPAT service and this will be explored further in 13/14.
10 Compliance Criterion Ten
Ensure, so far as is reasonably practicable, that care workers are free of and are protected from exposure to infections that can be caught at work and that all staff are suitably educated in the prevention and control of infection associated with the provision of health and social care.
10.1 Occupational Health Services
All new staff are screened for communicable diseases and their general health assessed before commencing employment at the Hospital.
Vaccinations against communicable diseases are offered at pre-employment screening and updated as required. Records are kept within the Occupational Health department.
Antibiotic Audit Results
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
102%
% charts review ed 91.77% 90.80% 92.67% 93.67% 88.58%
% w ith stop/review by Doctor +
pharmacist
94.09% 99.61% 94.35% 94.34% 98.05%
% w ith indication by Doctor +
Pharmacist
99.55% 99.22% 92.17% 93.96% 98.44%
Apr'12 Jul'12 Oct'12 Jan'13

15
Emergency treatment for exposure to blood and body fluids is provided in line with the Management of Blood and Body Fluid Exposure Incidents in Healthcare Staff Policy.
Staff who are to undertake exposure prone procedures are screened for blood borne viruses in line with DH guidelines.
At the start of 2013 IHT had two patients admitted with measles. In response to this rare condition the staff in all areas were recommended MMR vaccine if there was no record of immunity. Staff in higher risk areas (ED, Maternity etc) were targeted for vaccination. The ICT ran educational sessions on all admission wards to enable early identification of a case of measles and for staff to understand the severity of the condition. The ICT produced a number of algorithms and factsheets to provide information to staff working in emergency services with specific information and guidance on the condition.
The ICT worked with Suffolk Occupational Health to encourage the influenza vaccine immunisation for all appropriate staff in the hospital with the main focus on emergency services.
The ICT have rolled out a sharp safe system to protect IHT employees and conform to European safety legislation and Health and Safety recommendations. Sharp safe products are now available on all clinical areas and will replace the current hypodermic needles.
In response to a issue in 2012 where a patient drank alcohol hand rub from a variety of dispensers in the hospital, the ICT arranged and managed a complete change of dispenser in all areas to lockable secure dispensers.
10.2 Induction, Training Programmes and On-going Education
Infection Prevention and Control training is mandatory for all hospital staff. Compliance with this is monitored through the mandatory training matrix by the education department.
The hospital‟s local e-learning package is available to all staff.
The ICT also provide bespoke training which is increasingly popular in some specialist units as it provides training specifically related to the speciality.
The education system is regularly reviewed to examine ways to optimise its effect. New training systems are frequently presented to staff at all levels.
11 Education Strategy
Training needs analysis has identified that all staff employed at the Ipswich Hospital are required to undertake education in Infection Prevention and Control at the beginning of their employment (usually as part of their induction to the Hospital) and have annual updates during their employment. These sessions are similar in content concentrating on those issues essential to reducing healthcare associated infections in hospital. Within these boundaries the content of the sessions is tailored to the group receiving it. The following table shows the hospital wide compliance with Infection Prevention and Control education for 2012-13.
Staff Groups Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total % staff trained
Add Prof Scientific and
Technical 13 4 2 4 6 8 11 6 7 10 8 5 84 56.00%

16
Staff Groups Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total % staff trained
Additional Clinical
Services 47 50 40 28 29 63 48 69 61 45 67 73 620 83.00%
Administrative and Clerical
25 16 16 37 11 51 40 60 50 72 105 63 546 63.93%
Allied Health Professionals
4 3 4 5 11 6 4 12 9 52 34 31 175 62.95%
Estates and Ancillary
6 1 5 46 1 4 1 0 0 0 64 62.75%
Healthcare Scientists
2 1 8 3 2 8 1 4 1 24 1 55 46.22%
Medical and Dental
8 4 33 17 94 34 31 10 21 30 64 50 396 94.74%
Nursing & Midwifery
Registered 120 91 102 62 44 97 89 139 108 99 122 155 1228 96.77%
Total 225 169 205 157 200 307 232 301 261 309 424 378 3168 80.47%
There is always a balance between the time required for training and service needs, ie releasing staff from their duties on the ward to allow training. This is particularly the case at times of high capacity in the hospital. To this end the ICT produced a questionnaire to evaluate current understanding in infection control. The questionnaire can be completed at a convenient time for the staff member, and is based on two premises - the basic understanding that is required in mandatory training, and the fact that all staff undertaking the „competency assessment‟ have already received that training. To supplement the above, bespoke training is encouraged for all departments and has a good uptake in specialist areas (Nuclear Medicine, Radiology etc) where specific information related to the service is required. Staff groups where the uptake of training has been suboptimum are being encouraged in 13/14 to increase their staff compliance with mandatory training requirements. Medical training continues to be lecture based, but a number of different presentation styles have been trialled to examine the optimum way of delivering the important messages. The most successful to date has been the development of case study related/decision making educational packages which have been developed by the ICT and will be produced as distance learning later in 2013.
12 Performance against National Targets
12.1 National Surveillance
Since April 2001 all Acute Trusts are required to report all cases of MRSA Bacteraemia to the Health Protection Agency (HPA). This mandatory enhanced surveillance has since been extended to include Clostridium difficile, Orthopaedic Surgical Site Infection (SSI) and Glycopeptide Resistant Enterococci (GRE).
12.2 MRSA Bacteraemias
The Hospital continues to participate in the mandatory MRSA Bacteraemia surveillance. A Root Cause Analysis (RCA) is undertaken for all MRSA either within the hospital or within the CCG as appropriate. An action plan is formulated after the RCA, fed back to the Clinical Team and actions monitored through HICC and Business Unit Governance Groups. All RCAs are reported to Trust Management Team.

17
There were two cases of MRSA bacteraemia apportioned to the hospital in 2012-13. One case was considered unavoidable when investigated by the multi-disciplinary team through root cause analysis, the other was considered avoidable due to the lack of screening on admission.
18
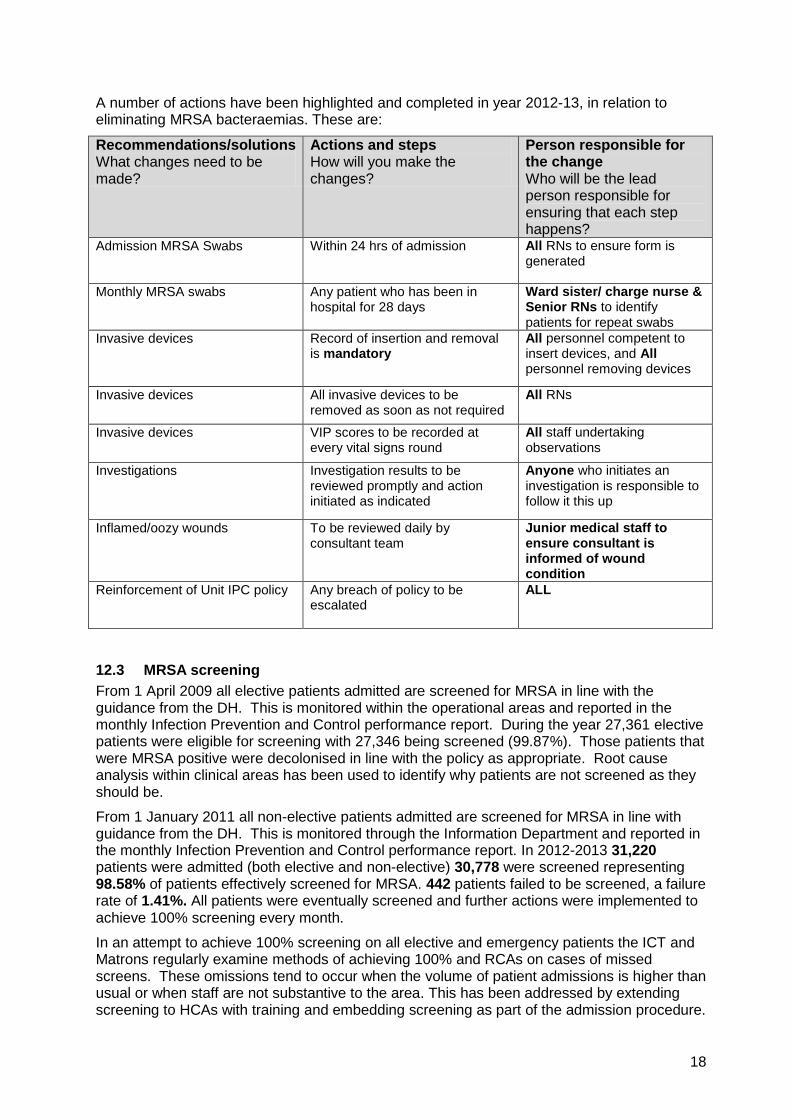
A number of actions have been highlighted and completed in year 2012-13, in relation to eliminating MRSA bacteraemias. These are:
Recommendations/solutions What changes need to be made?
Actions and steps How will you make the changes?
Person responsible for the change Who will be the lead person responsible for ensuring that each step happens?
Admission MRSA Swabs
Within 24 hrs of admission All RNs to ensure form is generated
Monthly MRSA swabs Any patient who has been in hospital for 28 days
Ward sister/ charge nurse & Senior RNs to identify patients for repeat swabs
Invasive devices Record of insertion and removal is mandatory
All personnel competent to insert devices, and All personnel removing devices
Invasive devices All invasive devices to be removed as soon as not required
All RNs
Invasive devices VIP scores to be recorded at every vital signs round
All staff undertaking observations
Investigations Investigation results to be reviewed promptly and action initiated as indicated
Anyone who initiates an investigation is responsible to follow it this up
Inflamed/oozy wounds To be reviewed daily by consultant team
Junior medical staff to ensure consultant is informed of wound condition
Reinforcement of Unit IPC policy Any breach of policy to be escalated
ALL
12.3 MRSA screening
From 1 April 2009 all elective patients admitted are screened for MRSA in line with the guidance from the DH. This is monitored within the operational areas and reported in the monthly Infection Prevention and Control performance report. During the year 27,361 elective patients were eligible for screening with 27,346 being screened (99.87%). Those patients that were MRSA positive were decolonised in line with the policy as appropriate. Root cause analysis within clinical areas has been used to identify why patients are not screened as they should be.
From 1 January 2011 all non-elective patients admitted are screened for MRSA in line with guidance from the DH. This is monitored through the Information Department and reported in the monthly Infection Prevention and Control performance report. In 2012-2013 31,220 patients were admitted (both elective and non-elective) 30,778 were screened representing 98.58% of patients effectively screened for MRSA. 442 patients failed to be screened, a failure rate of 1.41%. All patients were eventually screened and further actions were implemented to achieve 100% screening every month.
In an attempt to achieve 100% screening on all elective and emergency patients the ICT and Matrons regularly examine methods of achieving 100% and RCAs on cases of missed screens. These omissions tend to occur when the volume of patient admissions is higher than usual or when staff are not substantive to the area. This has been addressed by extending screening to HCAs with training and embedding screening as part of the admission procedure.

19
Patients identified as being colonised with MRSA are decolonised in line with the policy as appropriate. RCA within clinical areas is carried out to identify why patients have not been screened. In the case of patients who are identified as being colonised after their discharge, letters are sent to them and to their GPs identifying the results.
12.4 MSSA Bacteraemias
The Department of Health has not yet set reduction targets for MSSA bacteraemias, but for the year 2012/13, the Ipswich Hospital NHS Trust reported 11 cases identified post 48 hours of admission and root cause analysis was carried out for each case.
12.5 Clostridium difficile
Reporting of all cases of C difficile identified in the laboratory is mandatory for all hospitals in England. Targets for reducing the number of cases have been identified centrally by the DH and more challenging levels set locally by the Strategic Health Authority. For 2012-13 the target was for the Hospital to have no more than 27 cases in patients over the age of two years and who had been in hospital for more than two days when their sample was taken.
The following graph shows that the hospital achieved the target at year end.
All Trusts are provided with a target for C difficile. The target is based on a percent reduction of the previous year‟s target. As time has gone on the number of hospital acquired cases of C difficile have diminished dramatically, the severity of the disease has reduced and the majority of cases, after investigation, have been shown to be unavoidable (mainly due to the justifiable treatment of common infections with antibiotics). The target for C difficile for Ipswich Hospital in 2013-14 set by the DH and monitored by the CCG is no more than 21 cases. The achievement of this reduction requires a continuing focus on:
Prudent antibiotic use
Early recognition of the symptoms of C.difficile
Appropriate use of the Bowel evaluation tool and the SMART protocol
Appropriate isolation of all patients with diarrhoea
Hand washing
Effective decontamination of equipment and the environment.
5
10
15
20
25
30
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2012 / 2013
Cumulat ive actual
cases at IHNHST
Cumulat ive
trajectory

20
12.6 Surgical Site Infection Surveillance
The national surveillance scheme for surgical site infection (NINSS) was introduced in 1996. The surveillance scheme is currently co-ordinated by the Healthcare-associated Infection and Antimicrobial Resistance Department (HCAI & AMR) of the Communicable Disease Surveillance Centre (CDSC) at the Health Protection Agency (HPA). Participation in surveillance was optional for Trusts until 2004. Currently it is mandatory for Trusts undertaking Orthopaedic surgery to participate in surveillance for a minimum of three consecutive months a year. The Ipswich Hospital undertakes continuous surveillance of all elective orthopaedic surgery. Individual reports are provided for hospital Trusts. Regional, national and international reports are compiled using anonymised data. In addition the hospital participates in some of the voluntary surveillance modules.
Infection rates are provided by the HPE but are significantly retrospective (often over six months after reconciliation. Current infection rates are 0 infection for orthopaedic surgery (hips and knees) and 7 large bowel surgery cases as inpatients and 2 cases readmitted with infection. This is comparable with national SSI figures.
12.7 Glycopeptide-Resistant Enterococci Bacteraemias (GRE)
Enterococci are mainly acquired from the food chain and are a normal gut commensal organism. However, patients who are hospitalised for another reason and treated with glycopeptides may experience a GRE infection as a result, and outbreaks of cross-infection may then occur. GRE outbreaks are controlled by strict hand washing regimes, environmental cleaning and control of glycopeptide usage. However, in high risk patients, glycopeptide therapy for other infections is often unavoidable. The main groups at risk of GRE infection are haematology, renal and intensive care patients. The Hospital recorded no cases of GRE bacteraemias during 2012/13.
13 Outbreaks and Untoward Incidents
An outbreak is defined by the Health Protection Agency as:
“an incident in which two or more people, thought to have a common exposure, experience a similar illness or proven infection”
In an inpatient situation there may be patients who fit this criteria and are exhibiting similar symptoms but for different reasons. Diarrhoea is the most common sign of an outbreak but a common symptom in hospital not necessarily due to an infectious cause. Early action to prevent transmission and then careful investigation of an apparent outbreak may identify a different cause to common symptoms, the approach of the Hospital is to be cautious in the event of doubt and review the situation frequently.
13.1 Norovirus
During 2012-2013 there were two outbreaks identified as likely to be due to Norovirus. One of these outbreaks resulted in total ward closure and a SIRI was performed as a consequence.
The ICT examine all infected patients daily to identify early cases of infectious disease that have the potential of causing outbreaks. All suspected cases with symptoms are seen by a member of the infection control team and a member of the ICT is available at weekends to provide early control management advice to staff in the wards and in the bed management office. The management of these two outbreaks was viewed by the CCG as in line with best practice.

21
14 Finance
14.1 Budget Allocation and Financial Investment
The Head of Infection Control is responsible for the budget. Excess costs associated with outbreaks are funded centrally by the Hospital.
The team structure was reviewed during 2012/13 and following consultation there was a reduction of one band 7 WTE to the team. The current team structure can be seen in appendix A.
15 Key objectives for 2013/14 Annual plan
15.1 HCAI target delivery
The ICT will continue to work to further reduce HCAIs (target for Clostridium difficile 13/14 21, MRSA bacteraemia 13/14 0). There are other „emerging organisms‟ being monitored by infection control teams locally and nationally. The ICT are ensuring that IHT is well prepared for these infections as well as maintaining MRSA Bacteraemia and Clostridium difficile.
There have been discussions about „new‟ targets and two which have not yet been determined but may be given targets in the future are Escherichia.coli bacteraemia, and Meticillin sensitive Staphylococcus aureus bacteraemia.
15.2 Increase uptake of mandatory training for bank and staff groups
To ensure mandatory training levels are achieved for all staff groups requires a) the time to access the training and b) presented in a way which makes it personally applicable to staff in their work setting.
With this in mind the new education process will increase the amount of access to a wider variety of teaching approaches/presentation styles.
15.3 Increasing isolation facilities/contingency planning during the winter period
Norovirus and gastrointestinal illness as well as the frequent admission of communicable respiratory transmitted viruses in the winter have been a perennial problem for most hospitals in the country.
The ICT will in 13/14 examine methods of extending our current facility to allow for the more effective use of siderooms as isolation beds. Optimisation of our current facility will be assisted by the development of clear admission criteria linked to infection risk which will be developed by the ICT for approval at HICC.
15.4 A more effective data collection system and analysis for SSIs
The current system is based on information completed on the wards which is sent to the ICT. It is collected over three months and then sent to the HPE for analysis. Analysis normally takes around three months and when this is available is linked to surgical procedures and anonymised (no patient identifiable data). Following additional training the ICT intends to analyse data in-house to give more timely feedback to individual surgeons as appropriate.
15.5 Improved surveillance
Surveillance of infectious disease, trend analysis and early warning systems are essential in infection control. The current surveillance system is use is limited and a new system will need to be implemented in 13/14. Surveillance systems now available enable more detailed

22
analysis of inpatient results as well as provide information on antibiotic resistance patterns and trend data for intelligent outbreak control.
The Head of Infection Control has contacted microbiology & ICT colleagues in Essex and Suffolk and will work to try and establish an „east of England‟ surveillance system where patients can be traced and risk analysed as they are transferred to different hospitals and discharged into the community.

23
2 Consultant Medical Microbiologists
Director of Infection Prevention & Control
(DIPC)
Head of Infection Control (1 wte)
Senior Infection Control Nurse
(0.85 wte)
Infection Control Nurse (1 wte)
Audit & Surveillance Officer (1 wte)
Chief Executive
Named Infection
Prevention Doctor
Appendix A - Infection Prevention and Control Team Accountability Framework

Appendix B - Infection Control Annual Audit Work Plan delivered 12/13
Audits Quality Indicator Frequency Definition Suggested trend
MRSA bacteraemia cases Monthly Number of MRSA bacteraemia taken after two days after admission.
Reducing in line with trajectory set by SHA (no more than one cases for 2012-‟13).
MSSA bacteraemia cases Monthly Number of MSSA bacteraemia taken two days after admission.
Maintain reduction in S aureus bacteraemias achieved over last two years.
C difficile cases Monthly Number of cases of C difficile taken after 72 hours after admission.
Reducing in line with trajectory set by SHA (no more than 27 cases for 2012-‟13).
C difficile on death certificates
Monthly Cases where C difficile is recorded as primary cause of death.
Reducing, aim for zero avoidable cases.
High impact interventions (HIIs)
Monthly Care bundle audit of all seven HIIs In line with targets set by HICC
Isolation Policy compliance (appropriate placement)
Monthly The proportion of patients who require isolation being appropriately isolated.
In line with target set by HICC
Isolation Policy compliance (appropriate care)
Monthly Compliance with the care identified in the isolation policy.
Aim for 100% or formal risk assessment if varying from policy.
Transfer to C difficile isolation ward
Monthly Compliance with two hour transfer once C difficile confirmed.
Aim for 100% of compliance with operational guidance
Transfer from C difficile isolation ward
Monthly Compliance with transfer off the ward once diarrhoea has settled.
Aim for 100% of compliance with operational guidance
Antibiotic Stop/Review Date and Indication Policy Audit
Monthly Compliance with the Policy In line with target set by HICC
Environmental decontamination audit
Monthly Audit of cleanliness and tidiness in wards and departments
In line with target set by HICC
Hand hygiene Monthly Audit of compliance with Hand Hygiene Policy (WHO five moments for hand hygiene)
In line with target set by HICC
Safe use and disposal of sharps
Annually In line with Standard Principles for preventing HCAIs in Hospital Policy.
Mattress audit Monthly Annually report the number of mattresses inspected and condemned
Monthly review of mattresses in store and condemnation of those no longer suitable for use. Audit also undertaken throughout deep clean programme
Catheter associated urinary tract infection
All patients in study areas
High Impact Actions. Prospective surveillance. Maintain reduction
Use of Bristol Stool Chart At each RCA Bristol Stool chart should be used to monitor all patients with diarrhoea
Ensure appropriate recording and monitoring of bowel action

Appendix C - Abbreviations used in this document
AER Automated endoscope reprocessor
BU Business Unit
C difficile Clostridium difficile
CAT Cleaning action team
CDSC Communicable Disease Surveillance Centre
CEO Chief Executive Officer
CQC Care Quality Commission
DH Department of Health
DIPC Director of Infection Prevention and Control
DON Director of Nursing
GRE Glycopeptide Resistant Enterococci
HCAI Healthcare Associated Infection
HCAI & AMR Healthcare Associated Infection and Antimicrobial Resistance Department
HCHS Hospital and Community Health Services
HICC Hospital Infection Control Committee
HII High Impact Intervention
HPA Health Protection Agency
HSDU Hospital Sterilising and Disinfecting Unit
IC Infection Control
ICN Infection Control Nurse
ICT Infection Control Team
IPC Infection Prevention and Control
JAG Joint Advisory Group on gastro-intestinal endoscopy
MRSA Meticillin resistant Staphylococcus aureus
MSSA Meticillin sensitive Staphylococcus aureus
NHS National Health Service
NHSLA National Health Service Litigation Authority
NINSS Nosocomial Infection National Surveillance Scheme
PCT Primary Care Trust
PEAT Patient Environment Action Team
PGD Patient Group Directive
PSSRU Personal Social Services Research Unit
QMS Quality Management System
RCA Root Cause Analysis
SHA Strategic Health Authority
SLA Service Level Agreement
SSI Surgical Site Infection
TMT Trust Management Team
UIS Urology Investigation Suite





























