Embed Size (px)
Citation preview

Agenda
Bay of Plenty Hospital Advisory Committee
Venue: CEO Building, Cnr Cameron Road & 20th Avenue, Tauranga Date and Time: Wednesday 26th February 2014 at 2:00pm
Health Targets Shorter stays in emergency departments;
Improved access to elective surgery; Shorter waits for cancer treatment/radiotherapy;
Increased immunisation; Better help for smokers to quit; and
More heart and diabetes checks
Ministers Expectations Better Public Services: Results for New Zealanders
National Health Targets Care Closer to Home
Shorter Waiting Times Health of Older People
Regional and Clinical Integration Living within our means
Board Priorities Health Targets
Maori Health/Reducing Health Disparities Health of Older People
Primary Health Wellness/Chronic Conditions
Child and Youth
Healthy, Thriving Communities

Item No. Item Page
1
Apologies
2 Interests Register
3 Minutes of Meeting
3
4
Matters Arising
4.1 Matters Arising
4.2 Committee Members Matters Arising - NIL
6
5
Reports requiring Decision
5.1 Chief Operating Officer’s Highlights Report – Provider Arm 5.2 Chief Operating Officer’s Performance Report – Provider Arm
5.3 GM Property Services Monthly Report
5.4 Reducing Perioperative Harm
7
19
29
36
6
Reports for Noting 6.1 Work Plan
6.2 Outpatient Appointment Attendance by Dr George Gray, Public Health
Physician
42
43
7
Presentations 7.1 Hand Hygiene – the Way Forward by Bella Mark, Gwenda Ruegg and Jill
Van Der Wouden, Surgical Ward Whakatane
7.2 Reducing Harm from Falls by Anamaria Watene, CNM 2a Kaupapa & Maurice Chamberlain, Nurse Leader (Falls clinical lead)
64
76
8
General Business
9
Resolution to Exclude the Public
10
Next Meeting – Wednesday 26th March 2014

Minutes
Bay of Plenty Hospitals Advisory Committee
Venue: CEO Building, Tauranga Hospital Date and time: 23 October 2013 at 2pm
Committee: Mark Arundel (Chair), David Stewart, Sally Webb, Marion Guy, Jacob Te
Kurapa, Punohu McCausland (Runanga Rep) – arrived 1:25pm. Attendees: Phil Cammish (CEO), Helen Mason (Acting COO), Letham White (GM
Corporate Services), John Kyngdon (Chief Medical Advisor), Karina Thomson (Executive Assistant), Julie Robinson (Director of Nursing & Midwifery)
Item No. Item Action Who
1
Apologies There were no apologies received.
2
Interests Register The Board was asked if there were any conflicts in relation to items on the agenda.
3
Minutes and Chair report Back Resolved that the minutes of the meeting held 28th August 2013 be confirmed as a true and correct record.
Moved: D Stewart
Seconded: J Te Kurapa
4
Matters Arising As per report circulated with agenda. H Mason circulated a report regarding the 6 hour target.
3

Page 2 of 3
Item No. Item Action Who
5
Reports Requiring Decision 5.1 Chief Operating Officer Report
The Committee discussed the report as circulated with the agenda. The committee raised concerns
around the centralisation of HRIS and the impact of central rostering impacting on patient care and staff.
Resolved that the committee receive the report.
Moved: S Webb
Seconded: M Guy
Ask HBL when the ICC for HRIS is coming out. Check Ministers availability to visit the stroke unit and some of the releasing time to care wards.
GMCS
CEO
5.2 Revised BOPHAC Report
The Committee discussed the report as circulated with the agenda. The committee like the new format of
the report. Executive summary to be at the start
of the report showing highlights and particular attention to anything of concern to then be more detailed in a separate paper.
Resolved that the committee agree the new format for the report.
Moved: S Webb
Seconded: M Guy
5.3 GM Property Services Monthly Report
The Committee discussed the report as circulated with the agenda. Resolved that the Committee receive the report.
Moved: M Guy
Seconded: D Stewart
4

Page 3 of 3
Item No. Item Action Who
6
Reports for Noting 6.1 Work Plan
The Committee noted the information.
7
Presentation There were no presentations.
8
General Business
9
Next Meeting – Wednesday 26th February 2014.
There being no further business the meeting closed at 2:50pm. The minutes will be confirmed as a true and correct record at the next meeting.
5

Bay of Plenty Hospitals Advisory Committee
Matters Arising (open) – 26 February 2014
Meeting Date Item Action required Who Action Taken
23 Oct 13 5.1 Ask HBL when the ICC for HRIS is coming out. GMCS HBL have advised it is
unknown at this stage.
23 Oct 13
Check Ministers availability to visit the stroke unit and some of the releasing time to care wards.
CEO Completed.
6

CHIEF OPERATING OFFICER’S HIGHLIGHTS REPORT
PROVIDER ARM January 2014 SUBMITTED TO: BOPHAC
Submitted by: Helen Mason, Chief Operating Officer
RECOMMENDED RESOLUTION: Note the report.
7

HIGHLIGHTS SUMMARY CHIEF OPERATING OFFICER Implementation of CARE Values Good progress has been made across the Provider Arm on implementing the CARE values. An example is given below. The visual representation of CARE has been formatted for small “poster versions” of our values. These have been laminated and made available across the organisation to improve the visual reminders of CARE. In addition, a flyer describing the Board actions on CARE has been produced and made available. The values are proving helpful in a number of areas, as a productive way to frame difficult conversations. The flyer includes a page for individual staff members to record their personal CARE actions. Nursing To demonstrate nursing’s commitment to implementing the CARE values these are incorporated into the nursing job descriptions as they come up for renewal. The generic registered nurse JD was changed immediately following the release of the values. Senior nurse JDs are changed when a role is advertised. When the values were released the Nurse/Midwife recruiter reviewed the questions used at recruitment of new nurse and midwives to ensure there are questions asked which would require the applicant to demonstrate attributes related to the values. Nursing used a cascade approach to deliver the new values through each level. The Nurse/Midwife Leaders shared the values with their direct reports, in the main Clinical Nurse/Midwife Managers, who were then required to share this with their staff. Under the Releasing Time to Care programme one of the surgical wards also used CARE as their ward values. Acute Flow There has been a significant increase in the acute load over December. For example there has been an 8% increase in ED attendances compared to the same period last year. The week after New Year was also exceptionally busy. As Senior Manager on Call recently, I had an excellent opportunity to see more closely the daily pressures which our staff encounter in providing a responsive service, particularly for acute patients. There is excellent engagement from the Medical Leaders within the Medical Cluster on improving acute flow. There is an increasing level of awareness and commitment to a whole of system response to the acute patient journey. A number of new “small tests of change” are being trialled currently. In addition, a review of a number of existing action plans which impact on acute flow is currently underway. The intent is to be able to prioritise the many actions that have been identified, and to ensure that there is not unnecessary duplication across a number of plans. A number of the team are attending a Health Round Table meeting on the Hospital After Hours in February. This will provide additional support to improving acute flow.
MEDICAL DIRECTOR Dr John Kyngdon has made a decision to retire this year. Dr Hugh Lees, Medical Leader of Women, Child and Family Services, has agreed to step into the role for three months from the end of April, whilst a permanent appointment is made.
8

DIRECTOR OF NURSING Nursing Entry to Practice (NETP) BOPDHB has 33 NETP participants commencing 10 February. This is one less in the primary sector than last year leaving a primary sector placement available. The NETP coordinator is still actively trying to find to take up the remaining funded placement. There are a further 5 entry to practice placements in Mental Health. An Aged Residential Care facility in Eastern BOP was successful under the special ARC NETP funding scheme coordinated by Waikato DHB for the Midland region. This facility will receive $20,000 funding for the position less the DHB portion. A new initiative for Very Lost Cost Access (VLCA) NETP positions became available late 2013. Practices who met specified criteria were asked to apply for the $50,000 funding per NETP position. BOPDHB gained 5 funded positions, four at practices in western BOP and 1 in Eastern BOP. These positions are on top on the usual 34 funded NETP places in BOP.
SURGICAL, ANAESTHESIA & RADIOLOGY SERVICES Trauma Service: Inter-Agency Collaboration Following Trauma Report Alleviates Accident Blackspot Collaborative efforts between the Bay of Plenty District Health Board (BOPDHB), Police and NZ Transport Agency have seen a renowned accident blackspot record no serious crashes in 2013. A BOPDHB Trauma Service report into the region’s serious crashes of 2012 highlighted a hotspot at the intersection of State Highways 2 and 33, at Paengaroa. Of the five crashes at this site in 2012, four were head on collisions, resulting in multiple victims from each crash being hospitalised. Following the report’s publication in January 2013, and as part of the ongoing Tauranga Eastern Link construction, the intersection speed limit was reduced to 80kmph. This, allied to other minor safety improvements, has contributed to zero serious crashes being recorded at the intersection in 2013. Serious crashes were defined as those which resulted in a hospital stay of greater than 24 hours for the injured. Author of the report, BOPDHB Trauma Nurse Specialist Katrina O’Leary, said the result showed what organisational cooperation and information sharing could achieve. “The BOPDHB and the Police have a successful partnership in aiming to drive down trauma-related injuries,” she said. “An example of which is the lowered crash rate seen at the crash hotspot identified in last year’s report at the intersection at Rangiuru on SH2 and the turn off to Whakatane. “This has seen a drastic reduction in road traffic crashes thanks to the lowering of the speed limit to 80 kmph. There have been no hospital admissions with significant injury from road crashes from this site for 2013.” The SH2/SH33 intersection was a renowned crash spot, said the NZ Transport Agency’s Highways Manager Brett Gliddon, whose organisation is responsible for setting speed limits. As part of the Tauranga Eastern Link project a new roundabout is being constructed not far from the current intersection, which it is hoped will provide long-term safety benefits. It is scheduled to open in autumn 2014. “With two lanes of traffic in all directions and a proposed permanent speed limit of 80 kmph, the new Paengaroa roundabout adheres strongly to the Transport Agency’s commitment to reducing deaths and serious injuries on our roads,” said Mr Gliddon. The Trauma Service report investigated a total of 64 separate accidents during an 11 month period from 1 January 2012 to 30 November 2012. Medical lead for the BOPDHB Trauma Service, Barnaby Smith, said sharing information and close partnership with other government departments could make a difference because the same data could be viewed from different perspectives. “This identification of motor vehicle accident ‘hotspots’ shows the strong drive the BOPDHB has for primary prevention in the community. The BOPDHB has a commitment to audit and research and this research has made a difference for the local community.” The 2012 Trauma Service report was the first of its kind. The report into the Bay’s serious crashes and their causes for 2013 will be available in January 2014.
9

Tauranga MRT Roster Changes The department is working towards a move to the new MRT roster on the 10 March 2014. All newly recruited staff which includes MRT’s (Medical Radiation Technologist) and Nurses should be orientated to the service by this time. Major changes to the service offered by radiology will be:
• Introduction of a General MRT ED Night Shift - 24 hour on-site MRT service for general x-ray
• CT Evening Shift Monday to Fridays 5pm – 9pm – mixture of OP and IP scans to be completed
• CT Weekend Dayshift – CT MRT onsite between 8.00am – 4.30pm • General MRT on-call 24 hours during weekends • All MRTS move from a 7 hour day to a 7.5 hour day
Meetings will take place with relevent staff including ED and Wards to discuss how the CT evening sessions should operate. The Tauranga Radiology department will be striving to scan all in-patients where the referral is received by an agreed time (i.e. 3pm) on the same day. Endoscopy Support General Surgeons have undertaken additional colonoscopy sessions to support endoscopy including Saturday lists. Good progress is being made on reducing waiting lists. CT Scanners The business cases for replacement CT Scanners for Tauranga and Whakatane Hospitals in conjunction with Waikato DHB has been approved. Eastern Bay Energy Trust have confirmed that they will purchasing the Whakatane CT Scanner and provide an operating a lease arrangement for the use of the CT Scanner by BOPDHB. This includes a grant by Eastern Bay Energy Trust. Clinical Trial – Bard – Drug Eluting Ballons The Tauranga Radiology Department are involved in a trail of Bard – Drug Eluting Ballons for patients with vascular insufficency below the inguinal ligament (below the hip). The clinical school is involved with the trial ,in particular in following up patients post procedure. Tauranga, Christchurch, Wellington and Dunedin Hopsitals are all involved in this trial in NZ. For BOPDHB we are likely to do 15-20 patients a year. Risks and Mitigating Actions Orthopaedic Volumes Orthopaedic Acute numbers continue to be high impacting on elective operating time. This is increasingly impacting on the elective throughput for orthopaedic elective surgery. Plans are in progress to undertake additional operating sessions to address the increasing under delivery of electives. ENT SMO vacancy The locum Lakes based locum ENT SMO has advised that he may not be able to continue. An offer has been made to another ENT SMO for a 12 month position commencing in August. In the interim the service is seeking locum cover to provide some support. General Surgery January has seen a high volume of complex cancer cases impacting on the department’s workload. New Year Week
10

Across all services and departments the occupancy and activity was very high. Theatre were required to organise several additional acute lists (over and above the planned additional) to manage demand and this unplanned activity impacted across many services. Following a debrief, a summary of activity is being prepared.
MEDICINE Cardiology/Clinical Physiology Joelene Walker (Cardiac Physiologist) with the DHB for 15 years, has been awarded a Maori Scholarship for $5,000. This will enable her to complete the CRFS Course at Sturt University Australia (Certificate in Respiratory Function Scientist) in 2014. Once complete this will give the DHB a second qualified respiratory scientist, which will reduce patient waiting time and increase service support for complex respiratory studies. Negotiations are underway regarding providing Waikato an additional 100 Echo with an expanded access to include TOE and stress ECHOs. This is following the successful 100 ECHOs completed for Waikato at the end of last year. Oncology-Respiratory Lung Cancer Co-ordinator interviews have been completed with an appointment imminent. At present this role is being covered internally to maintain Fast Cancer Treatment (FCT) target input etc, the appointment will allow the development of the role and further the FCT co-ordination. The Decision to Treat target continues to be achieved at 100% for Radiotherapy and Chemotherapy. Gastroenterology The Gastroenterology team will be fully recruited from mid-February and continue with a focus on colonoscopy to meet ESPI compliance (see below) General Medicine Due to the stability of the workforce at Whakatane within acute medicine, discussions have been initiated to introduce clinics in Te Kaha, Kawerau and Opotiki ED A new SMO has commenced this month in Whakatane, filling a vacant slot and a new SMO has been appointed to Tauranga and will commence in April. Two RNs in ED Tauranga have completed their CNS (Clincal Nurse Specialist) post graduate papers and this will allow for greater flexibility in backfilling etc the existing CNS roles. Risks and Mitigating Actions 6hr Target The hospital 6 Hour Target remains the key focus for all acute services particularly given a year to year increase in ED attendances of greater than 8%. Clinical leadership is engaged in improving performance on this measure, with a focus on reviewing the Standard Operating Procedure, Hospital Out Of Hours Project and Breach resolution. Gastroenterology Colonoscopy remains a concern with both ESPI compliance and surveillance scope under-delivery. A mitigation plan has been put in place to rectify both ESPI by February and surveillance by the end of the year. MOH have approved the plan.
WOMAN CHILD & FAMILY
11
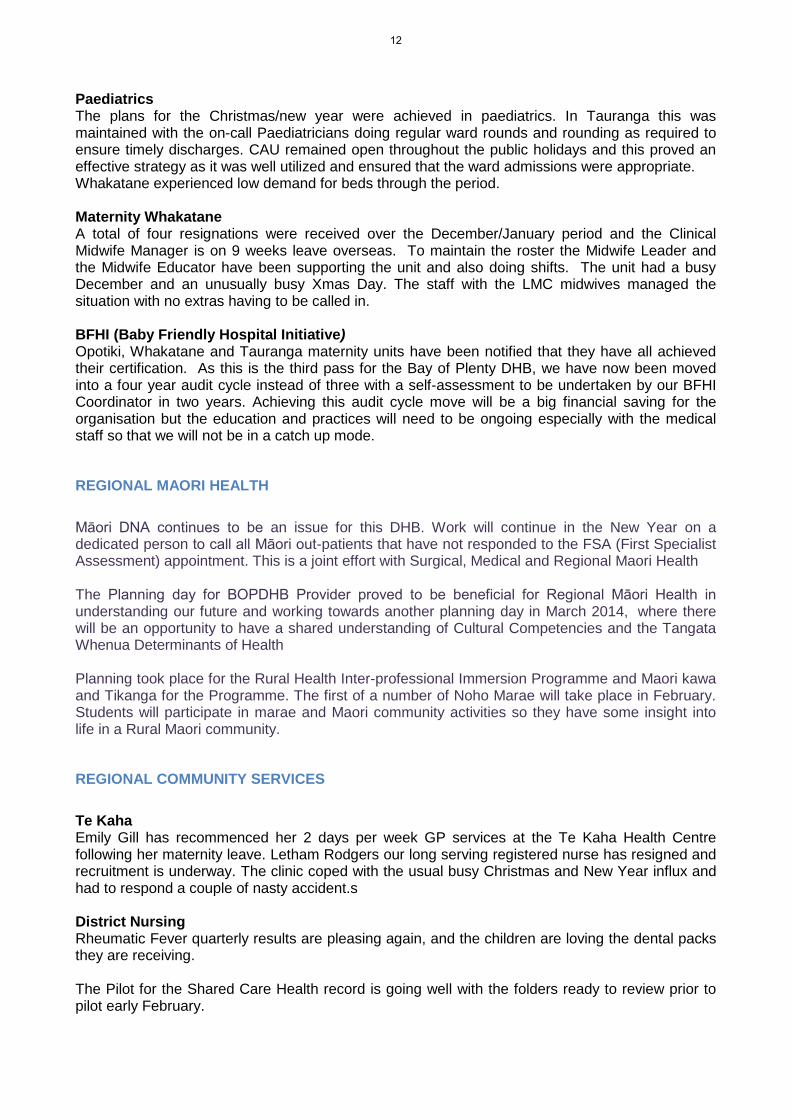
Paediatrics The plans for the Christmas/new year were achieved in paediatrics. In Tauranga this was maintained with the on-call Paediatricians doing regular ward rounds and rounding as required to ensure timely discharges. CAU remained open throughout the public holidays and this proved an effective strategy as it was well utilized and ensured that the ward admissions were appropriate. Whakatane experienced low demand for beds through the period. Maternity Whakatane A total of four resignations were received over the December/January period and the Clinical Midwife Manager is on 9 weeks leave overseas. To maintain the roster the Midwife Leader and the Midwife Educator have been supporting the unit and also doing shifts. The unit had a busy December and an unusually busy Xmas Day. The staff with the LMC midwives managed the situation with no extras having to be called in. BFHI (Baby Friendly Hospital Initiative) Opotiki, Whakatane and Tauranga maternity units have been notified that they have all achieved their certification. As this is the third pass for the Bay of Plenty DHB, we have now been moved into a four year audit cycle instead of three with a self-assessment to be undertaken by our BFHI Coordinator in two years. Achieving this audit cycle move will be a big financial saving for the organisation but the education and practices will need to be ongoing especially with the medical staff so that we will not be in a catch up mode.
REGIONAL MAORI HEALTH Māori DNA continues to be an issue for this DHB. Work will continue in the New Year on a dedicated person to call all Māori out-patients that have not responded to the FSA (First Specialist Assessment) appointment. This is a joint effort with Surgical, Medical and Regional Maori Health The Planning day for BOPDHB Provider proved to be beneficial for Regional Māori Health in understanding our future and working towards another planning day in March 2014, where there will be an opportunity to have a shared understanding of Cultural Competencies and the Tangata Whenua Determinants of Health Planning took place for the Rural Health Inter-professional Immersion Programme and Maori kawa and Tikanga for the Programme. The first of a number of Noho Marae will take place in February. Students will participate in marae and Maori community activities so they have some insight into life in a Rural Maori community.
REGIONAL COMMUNITY SERVICES Te Kaha Emily Gill has recommenced her 2 days per week GP services at the Te Kaha Health Centre following her maternity leave. Letham Rodgers our long serving registered nurse has resigned and recruitment is underway. The clinic coped with the usual busy Christmas and New Year influx and had to respond a couple of nasty accident.s District Nursing Rheumatic Fever quarterly results are pleasing again, and the children are loving the dental packs they are receiving. The Pilot for the Shared Care Health record is going well with the folders ready to review prior to pilot early February.
12

The GP referral form for DN services has been updated to enable GP’s using Medtec to refer electronically directly to District Nursing. Toi Te Ora Public Health Services An internal review of the Health Promoting Schools (HPS) programme has been completed and key findings have been discussed with the Education team. This is the first time a formal review has been undertaken and included a review of all programme resources, gathering feedback from the HPS advisors, schools and reviewing against Ministry priorities and the national delivery model. The review provides significant information to the service and will result in key recommendations for quality improvements for consideration by management team. Allied Health Allied health have participated in the Debrief for the Christmas New year plans and reviewing what improvements may assist in supporting the services throughout public holidays. The occupational therapy team in Tauranga worked very well together with decreased staff for the xmas /new year break, when the hospital was busy. There were issues with the fax machine so referrals were not able to be received in the usual manner. But with good team work and focus on discharges everyone requiring review /assessment was completed. Te Koru Whakatane Work has begun with Brent Gilbert De Rios, Regional Social Work Team Leader, to help to define what services are done where within the Social work team. Social Work has physically moved into Te Koru, the rehab unit. The current set up is still being reviewed and improved, however some staff have remarked that the Social Work presence in Te Koru has enabled a big improvement in multidisciplinary team work and is much valued.
A stocktake by Child Development Services and Equipment Officer this month have shown a much improved tracking and recall of equipment with minimal losses.
The top Clinical physiotherapy student for final year students at AUT was Alex Petrie, a student who was here last year and now has a parental leave contract with Te Koru. A great achievemen.t Risks and Mitigating Actions Toi Te Ora Public Health Services Measles Thirteen confirmed cases of measles have been notified to Toi Te Ora since the last week of December. This outbreak originated from people attending a dance competition in Sydney early in December. Unfortunately one of the competitors from the Philippines was infectious at the time of the competition even though he was only diagnosed with measles afterwards. From that single case at least 16 people in the North Island have become infected, along with numerous others in Australia. Two of our local cases were significantly ill and were hospitalised. All of the cases were unimmunised as were a number of their close contacts, who as a result were placed in quarantine to prevent further spread of the infection. In an unrelated incident a passenger arriving in Auckland on a plane from the Philippines via Singapore was found to have measles. As he would have been infectious at that time of travel all passengers and crew who were on the flight are being followed up. Toi Te Ora was advised by our Auckland colleagues that eight passengers from the flight gave Bay of Plenty or Lakes addresses on their passenger arrival cards. Each of these individuals is being contacted and offered the appropriate advice. This includes placing into quarantine anyone who may be susceptible to getting measles ie anyone younger than 45 years old and who has not had two doses of a measles containing vaccine.
13

Both of these outbreaks represent excellent reminders of the practical importance of vaccination against what is a very preventable but potentially serious infection. Tuberculosis (TB) TB (or what used be known as Consumption) is an infectious disease which has dramatically decreased in incidence over the past 100 years. However, it is unlikely to ever disappear altogether. Recent cases which have been notified to Toi Te Ora typify the difficulties associated with completely controlling the spread of this bacterial illness. One is a family member of an elderly person who was notified and died last year. This recent case is the third person who appears to have caught TB from last year’s case. An unrelated case of TB migrated to New Zealand a few years ago from a country which has an annual incidence of TB which is over 20 times that of New Zealand. Unfortunately, this person, who has had symptoms of TB for the past three months, works with a significant number of people many of whom now need to be tested, which Toi Te Ora is co-ordinating. Allied Health The Dietetics team are unable to responds to the high number of referrals received. A business case has been submitted for one additional FTE, to address the workload. The dietetics team is a key part of our MDT (multi-disciplinary team) approach. Occupational therapy Tauranga are organising for computers to be bracketed to the wall. With the extra FTE for the ortho rehab contract and other FTE increase overtime, they have run out of desk space (OTs spend at least 40% of their writing reports phoning etc). This move will clear the centre table for work space if required. They have also expanded into the extra space in Silver Birch house.
MENTAL HEALTH & ADDICTION SERVICES MENTAL HEALTH SERVICES FOR OLDER PEOPLE The In-Patient Unit renovations and new personal alarm system has been completed. This now allows for improved health and safety in regards to hygiene, privacy and we hope decreased aggression between residents with more floor space to separate the patients on the unit.
The decant to HIA (Health in Aging) whilst a stressful period due to the small space to contain our client group, allowed the staff to develop more activities and review the changes to the daily programme on return.
Midland Regional Dementia Behavioral Support and Advisory Service Coordinator • Having had substantial input into the design of the new build dementia unit at Bethlehem
Views, it was pleasing to see on a visit there that many of the design principles had been incorporated into the now opened unit..
• BOPDHB has been invited to be part of the National Steering Group regarding a Review of Information Resources for people diagnosed with dementia. It is hoped that the review and subsequent development of national resources will be completed within a year.
Bay Navigator Uncomplicated Dementia Care Pathway Nurse Educator Cheryl Collier has been granted a $2000 from the Mai i Nga Kuri a Wharei Ki Tihirau Scholarships Fund - Congratulations Cheryl – Cheryl will be using this scholarship to completed a post graduate diploma in Dementia Studies via University of Sterling. ADULT COMMUNITY MENTAL HEALTH & ADDICTION SERVICE Inter-service Co-operation
14

An excellent example of inter-service co-operation in the interests of patient-centred care occurred between the Child & Adolescent Mental Health Service (CAMHS) and the BOP Addiction Service. A young woman in the care of the CAMHS Addiction Team had been arrested and remained in the custody of the Police overnight. The next morning she was bailed to her home address, which was outside Tauranga (without easy access to emergency care if required) and into a home with others, which included a baby, with the conditions on her bail that she was not to consume alcohol or drugs. The CAMHS clinicians were concerned as to the safety of those bail conditions given her reports of her level of use of alcohol and substances, and also her reports of previous withdrawal risks. The BOP Addiction Service Detox Nurse was able to provide an urgent detox assessment prior to her returning to her home, to assess safety and risk issues pertaining to possible withdrawal from substances. The client was able to be bailed safely and appropriately for all concerned, following that assessment. BOP Addiction Service – Opioid Substitution Treatment Review The Bay of Plenty Addiction Service undertook a review of the Opioid Substitution Treatment (OST) aspect of their service this month. Opioid Substitution Treatment is the medical procedure of replacing an illegal opioid drug such as heroin, (or more commonly in New Zealand, morphine derivatives) with a longer acting but less euphoric opioid, usually methadone or suboxone that is taken under medical supervision. The review was designed to ensure that service provision is aligned with the National Guidelines, which directs best practice in opioid substitution treatment, and to ensure that there is a consistent approach within the service to the provision of opioid substitution treatment to clients. Group Work A series of groups is in the process of being developed and facilitated by Elsabe Van Wyk, Clinical Psychologist and Siobhan Wilson, Occupational Therapist for service users in the Eastern Bay. These will range from life skills, anxiety management and depression. Other team members have been approached to supply ideas for other groups that maybe considered depending on need. This we are hoping to begin in early February. Renovations Adult Community Mental Health and Addiction Service in Tauranga has had an exciting start to 2014 with the building renovations to Kowhai House. Work is now completed in the reception area where we have relocated the reception opposite the entrance to improve visibility for safety reasons and created room for both receptionists to attend to presenting clients which should improve efficiency. Relocation of the waiting room has created a safer space for clients as they can see the corridors and receptionists and call for assistance if needed. A new second clinic room is in progress which will enhance the work of the dietician with people with eating disorders and weight gain attributed to psychotropic medication. Our colleagues in Addictions will also have access and nurses at ACMH can have the space to work on metabolic monitoring. Teams are being informed of the plans and developments and whilst there were concerns about noise overall we have been pleased with the professionalism of the contractors and the minimal disruption to the work environment. ASSOCIATE DIRECTOR OF NURSING District Nurses DN have requested support in descalation techniques and understanding aggression. A 1.5 hour program has been developed for them. Students Student placements have increased from 11 to 12. A request for a further increase from Waiarieki was declined. The extra student will be placed in Consult Psych Liaison and the Crisis Team. The first cohort of students are expected at the end of February. New Graduates (NESP)
15

All 5 places have been filled A request to RMH for cultural supervision has been made as the Family/Whanau advisor is not available this year. Clinical Supervision A pilot foundation course for the region has been developed through collaboration with Lakes and Waikato DHB’s. BOPDHB MH Services has 2 graduates from the recent pilot. An E-Learning package will be going “live” in February. CHILD AND ADOLESCENT MENTAL HEALTH SERVICES Recruitment Both CAMHS and Voyagers are currently recruiting to vacancies. CAMHS have had a record number of applications for Key Worker positions being advertised. We are hopeful that the new recruits will be joining the team in March. KPI Project BOPCAMHS has developed a poster in the form of a snakes and ladders game as part of the national KPI benchmarking day. We have been recommended for the creative and fun way in which the team has been taking the KPI’s on. Access Rates Colin Hamlin from the MOH has invited BOPCAMHS to speak at the Leaders sector day with regards to our high access rates. BOPCAMHS has one of the highest access rates in the country. The MOH is especially interested in how BOPCAMHS manages this high access rate while also reaching our target around wait times. Facilities upgrades in MHSOP and Adult Community Mental Health and Addiction Services as outlined in the above reports is welcomed by the staff and patients alike.
SUPPORT SERVICES
SERVICE IMPROVEMENT UNIT Project Waka The Migration Readiness report has been received from an external reviewer with the recommendation for additional project support, which has been supported. The additional Project Manager will start on February 4th and provide support for the significant Training and Orientation component of the move to the new facility in May. The risk meeting for Service Leadership has occurred to review the “draft move macro plan for Project Waka”. Further evaluation of the work required for the lead-in period for the extensive training and orientation programme planned has also occurred. Areport will be sent to the COO and GM Property services prior to the next Steering group meeting. A Watch list of tasks needing to be completed prior to the Move week has been introduced to ensure close tracking of progress. CIRCA & OTHER PROJECTS UPDATE CCUG CCUG (Care Capacity User Group) has updated the Business Case to increase the visibility of the Hospital Status at a Glance screens. This will support improved buy in from across the hospital into initiatives to improve acute flow through the hospital. CIRCA (Quality Improvement Programme) The evaluation criteria have now been reviewed and updated for CIRCA 1 through to 4. Business Leaders have been asked to review their areas, marking of progress in line with these new criteria.
16

Volunteer Management The Programme Manager, Service Improvement is continuing to both respond to and process applications to volunteer from members of the public and secondly is leading the project on improving the system of Volunteer management. Activity over the past month on improving the system of volunteer management has focussed on advertising specific volunteer roles on the BOPDHB website. The response to this has been slightly higher than previous months. 10 applications were being processed in late December and early January. Microster Project This project will see the inclusion of all staff groups onto Microster, with Medical staff moving on to the system. The wider Microster Project group met on 13 January. The Project Initiation document was discussed, this included membership of the project committees, details of Microster processes and reasons for the project. Attendees were asked to give feedback on the PID. Another meeting is planned for early February. ERAS Orthopaedics This project (Enhanced recovery after surgery) is underway with the development of a project charter, driver diagrams, story board and project plan. Meetings are scheduled fortnightly with the project team and the first PDSA cycle is underway with discharge date confirmation with patients within 24 hours of admission. Anaesthetic, analgesic and surgical protocols are developed and in the consultation phase. Three team members are scheduled to attend a Master class in Auckland in February 2014. Releasing Time to Care - Productive Community A planning meeting was held with the Nurse leader for District Nursing and a implementation plan agreed for the remaining 3 modules to be completed by June 2014. GP Liaison & Bay Navigator DHB IT has completed its part of integration of the hospital electronic clinical record with BPAC (the provider of the eReferral system as well as other modules for general practice). BPAC should complete integration with Medtech, the most commonly used general practice patient management system by the end of January. This will enable general practice clinicians to go directly from their own practice records into the patient’s hospital records. This should lead to better communication, increased patient safety and time savings as practices will no longer need to phone and fax the hospital for information. This is a major step forward in the integration of care across hospital and community settings. We are currently looking at how this system compares to other initiatives around the country as we believe that our level of functionality will be better than most. This initiative supports activities in CIRCA One – improving communication between general practice and specialist services. New eReferral forms have been created on the BPAC eReferral system to improve the quality of information upon which specialists make grading decisions for elective referrals. In particular a form has been created for the sleep clinic which has previously struggled with a large number of referrals containing insufficient information. The new form should make the process quicker and safer for patients. In addition the suspected colorectal cancer referral form has been updated to include national guidance on direct access to endoscopy. A form is being developed at the moment to support the chest pain clinic as it is also challenged by demand exceeding capacity and difficulty in effectively triaging referrals based on the information being provided. There have been a number of complaints from GPs recently regarding discharge summaries not being completed, particularly when a patient has died. I have started investigating specific cases and identifying causes. Clinical Governance Committee has been looking at those services which
17

should be completing discharge summaries and we will then be providing services with reports on completion rates. I am holding training sessions with junior doctors on both sites providing education on communication with general practice. General Practice After-hours Service – the first meeting of the user group that will implement the new service took place on Thursday 30th January. There has been a high level of interest in participating. Future Care Planning meetings continue. The group is working its way through existing documentation that is produced by a number of organisations e.g. the Advanced Care Planning Cooperative, the HDC Health Passport, local nursing home advance directive and resuscitation status documentation, comparing it against a matrix to see which best meets BOP needs. Level 2 Advance Care Planning courses are being held locally later in the year and the Future Care Planning group will consider who should be targetted to attend these courses and what support can be given.
18

COO Report – 26 February 2014 Page 1 of 10
CHIEF OPERATING OFFICER’S PERFORMANCE REPORT PROVIDER ARM January 2014
SUBMITTED TO: Bay of Plenty Hospital Advisory Committee 26 February 2014
Submitted by: Helen Mason, Chief Operating Officer
RECOMMENDED RESOLUTION: That the Committee receive the report.
19
COO Report – 26 February 2014 Page 2 of 10
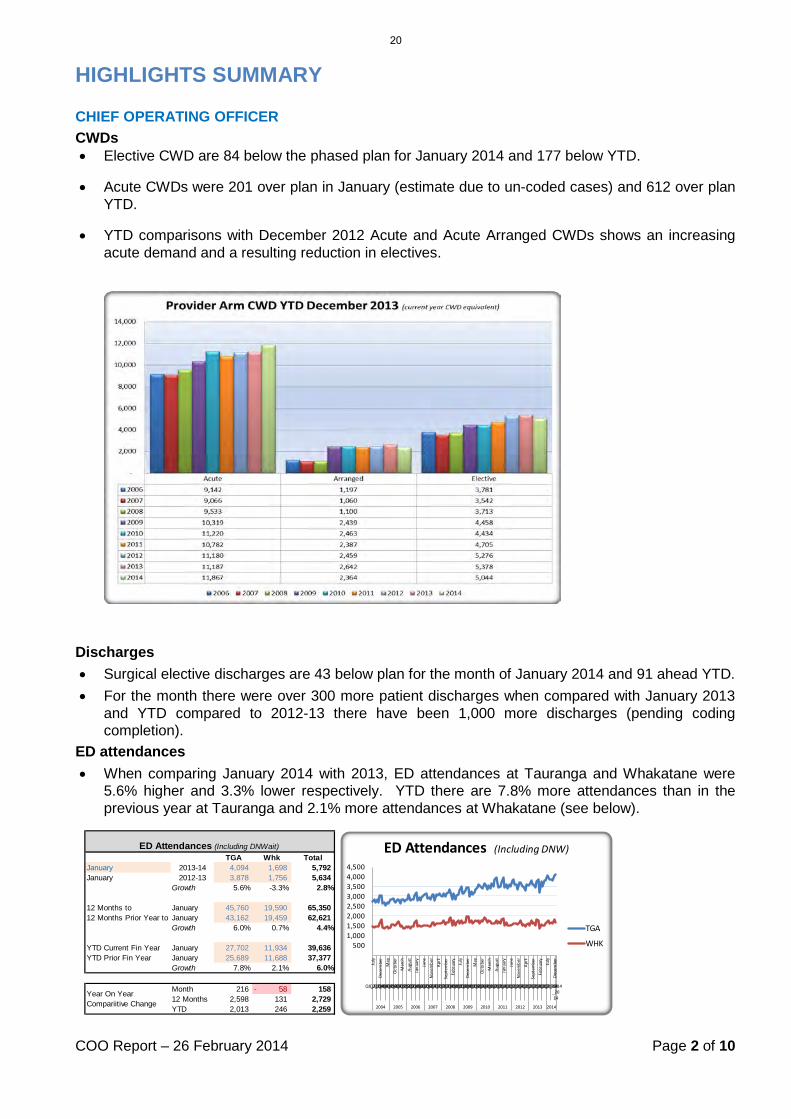
HIGHLIGHTS SUMMARY CHIEF OPERATING OFFICER CWDs • Elective CWD are 84 below the phased plan for January 2014 and 177 below YTD.
• Acute CWDs were 201 over plan in January (estimate due to un-coded cases) and 612 over plan YTD.
• YTD comparisons with December 2012 Acute and Acute Arranged CWDs shows an increasing acute demand and a resulting reduction in electives.
Discharges • Surgical elective discharges are 43 below plan for the month of January 2014 and 91 ahead YTD. • For the month there were over 300 more patient discharges when compared with January 2013
and YTD compared to 2012-13 there have been 1,000 more discharges (pending coding completion).
ED attendances • When comparing January 2014 with 2013, ED attendances at Tauranga and Whakatane were
5.6% higher and 3.3% lower respectively. YTD there are 7.8% more attendances than in the previous year at Tauranga and 2.1% more attendances at Whakatane (see below).
TGA Whk TotalJanuary 2013-14 4,094 1,698 5,792 January 2012-13 3,878 1,756 5,634
Growth 5.6% -3.3% 2.8%
12 Months to January 45,760 19,590 65,350 12 Months Prior Year to January 43,162 19,459 62,621
Growth 6.0% 0.7% 4.4%
YTD Current Fin Year January 27,702 11,934 39,636 YTD Prior Fin Year January 25,689 11,688 37,377
Growth 7.8% 2.1% 6.0%
Month 216 58- 158 12 Months 2,598 131 2,729 YTD 2,013 246 2,259
ED Attendances (Including DNWait)
Year On Year Compariitive Change
5001,0001,5002,0002,5003,0003,5004,0004,500
July
Dece
mbe
rM
ayOc
tobe
rM
arch
Augu
stJa
nuar
yJu
neNo
vem
ber
April
Sept
embe
rFe
brua
ryJu
lyDe
cem
ber
May
Octo
ber
Mar
chAu
gust
Janu
ary
June
Nove
mbe
rAp
rilSe
ptem
ber
Febr
uary
July
Dece
mbe
r
Q1_20 04Q2_20 04Q3_20 04Q4_20 04Q1_20 05Q2_20 05Q3_20 05Q4_20 05Q1_20 06Q2_20 06Q3_20 06Q4_20 06Q1_20 07Q2_20 07Q3_20 07Q4_20 07Q1_20 08Q2_20 08Q3_20 08Q4_20 08Q1_20 09Q2_20 09Q3_20 09Q4_20 09Q1_20 10Q2_20 10Q3_20 10Q4_20 10Q1_20 11Q2_20 11Q3_20 11Q4_20 11Q1_20 12Q2_20 12Q3_20 12Q4_20 12Q1_20 13Q2_20 13Q3_20 13Q4_20 13Q1_20 14Q2_20 14Q3_2014
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
ED Attendances (Including DNW)
TGA
WHK
20
COO Report – 26 February 2014 Page 3 of 10
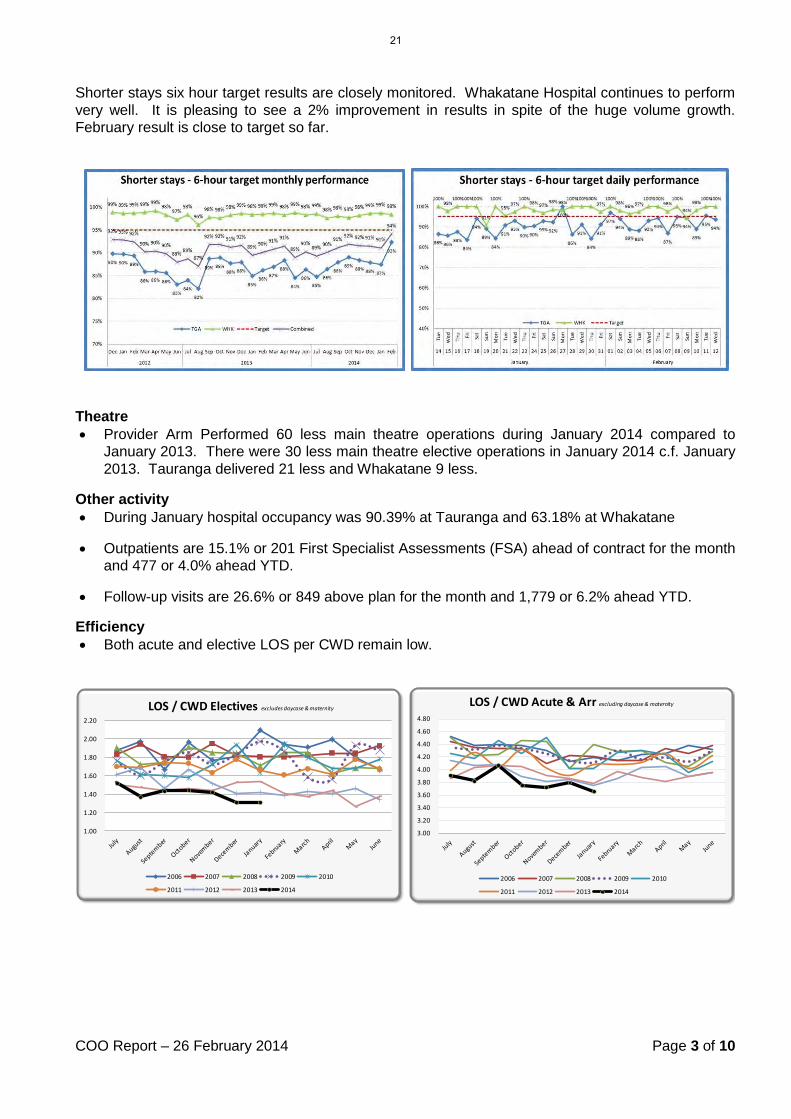
Shorter stays six hour target results are closely monitored. Whakatane Hospital continues to perform very well. It is pleasing to see a 2% improvement in results in spite of the huge volume growth. February result is close to target so far.
Theatre • Provider Arm Performed 60 less main theatre operations during January 2014 compared to
January 2013. There were 30 less main theatre elective operations in January 2014 c.f. January 2013. Tauranga delivered 21 less and Whakatane 9 less.
Other activity • During January hospital occupancy was 90.39% at Tauranga and 63.18% at Whakatane
• Outpatients are 15.1% or 201 First Specialist Assessments (FSA) ahead of contract for the month and 477 or 4.0% ahead YTD.
• Follow-up visits are 26.6% or 849 above plan for the month and 1,779 or 6.2% ahead YTD.
Efficiency • Both acute and elective LOS per CWD remain low.
1.00
1.20
1.40
1.60
1.80
2.00
2.20
LOS / CWD Electives excludes daycase & maternity
2006 2007 2008 2009 2010
2011 2012 2013 2014
3.00
3.20
3.40
3.60
3.80
4.00
4.20
4.40
4.60
4.80
LOS / CWD Acute & Arr excluding daycase & maternity
2006 2007 2008 2009 2010
2011 2012 2013 2014
21
COO Report – 26 February 2014 Page 4 of 10
55.00
QUALITY, SAFETY & EXPERIENCE OF CARE
PATIENT & QUALITY Jan-13 Jan-14 Target Var Actual Target Var ORGANISATIONAL HEALTH & MONTIORING Jan-13 Jan-14 Target Var Actual Target Var
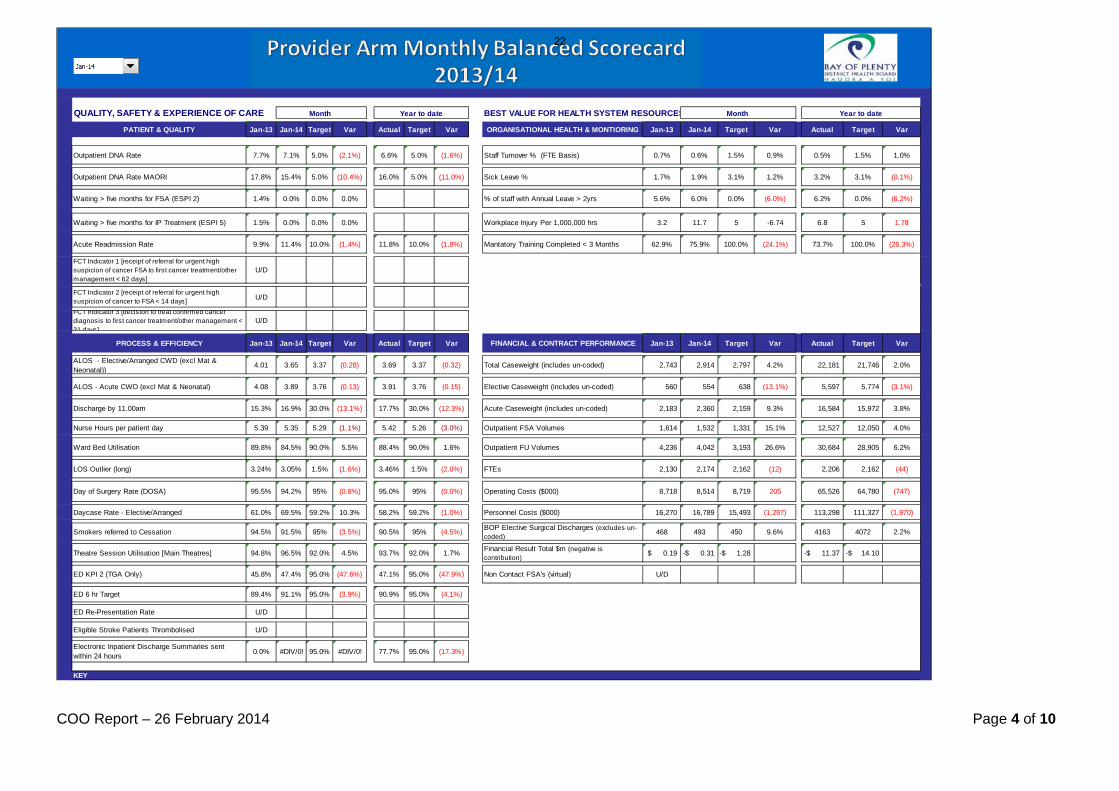
Outpatient DNA Rate 7.7% 7.1% 5.0% (2.1%) 6.6% 5.0% (1.6%) Staff Turnover % (FTE Basis) 0.7% 0.6% 1.5% 0.9% 0.5% 1.5% 1.0%
Outpatient DNA Rate MAORI 17.8% 15.4% 5.0% (10.4%) 16.0% 5.0% (11.0%) Sick Leave % 1.7% 1.9% 3.1% 1.2% 3.2% 3.1% (0.1%)
Waiting > five months for FSA (ESPI 2) 1.4% 0.0% 0.0% 0.0% % of staff with Annual Leave > 2yrs 5.6% 6.0% 0.0% (6.0%) 6.2% 0.0% (6.2%)
Waiting > five months for IP Treatment (ESPI 5) 1.5% 0.0% 0.0% 0.0% Workplace Injury Per 1,000,000 hrs 3.2 11.7 5 -6.74 6.8 5 1.78
Acute Readmission Rate 9.9% 11.4% 10.0% (1.4%) 11.8% 10.0% (1.8%) Mantatory Training Completed < 3 Months 62.9% 75.9% 100.0% (24.1%) 73.7% 100.0% (26.3%)
FCT Indicator 1 [receipt of referral for urgent high suspicion of cancer FSA to first cancer treatment/other management < 62 days]
U/D
FCT Indicator 2 [receipt of referral for urgent high suspicion of cancer to FSA < 14 days] U/D
FCT Indicator 3 [decision to treat confirmed cancer diagnosis to first cancer treatment/other management < 31 days]
U/D
PROCESS & EFFICIENCY Jan-13 Jan-14 Target Var Actual Target Var FINANCIAL & CONTRACT PERFORMANCE Jan-13 Jan-14 Target Var Actual Target Var
ALOS - Elective/Arranged CWD (excl Mat & Neonatal))
4.01 3.65 3.37 (0.28) 3.69 3.37 (0.32) Total Caseweight (includes un-coded) 2,743 2,914 2,797 4.2% 22,181 21,746 2.0%
ALOS - Acute CWD (excl Mat & Neonatal) 4.08 3.89 3.76 (0.13) 3.91 3.76 (0.15) Elective Caseweight (includes un-coded) 560 554 638 (13.1%) 5,597 5,774 (3.1%)
Discharge by 11.00am 15.3% 16.9% 30.0% (13.1%) 17.7% 30.0% (12.3%) Acute Caseweight (includes un-coded) 2,183 2,360 2,159 9.3% 16,584 15,972 3.8%
Nurse Hours per patient day 5.39 5.35 5.29 (1.1%) 5.42 5.26 (3.0%) Outpatient FSA Volumes 1,614 1,532 1,331 15.1% 12,527 12,050 4.0%
Ward Bed Utilisation 89.8% 84.5% 90.0% 5.5% 88.4% 90.0% 1.6% Outpatient FU Volumes 4,236 4,042 3,193 26.6% 30,684 28,905 6.2%
LOS Outlier (long) 3.24% 3.05% 1.5% (1.6%) 3.46% 1.5% (2.0%) FTEs 2,130 2,174 2,162 (12) 2,206 2,162 (44)
Day of Surgery Rate (DOSA) 95.5% 94.2% 95% (0.8%) 95.0% 95% (0.0%) Operating Costs ($000) 8,718 8,514 8,719 205 65,526 64,780 (747)
Daycase Rate - Elective/Arranged 61.0% 69.5% 59.2% 10.3% 58.2% 59.2% (1.0%) Personnel Costs ($000) 16,270 16,789 15,493 (1,297) 113,298 111,327 (1,970)
Smokers referred to Cessation 94.5% 91.5% 95% (3.5%) 90.5% 95% (4.5%) BOP Elective Surgical Discharges (excludes un-coded)
468 493 450 9.6% 4163 4072 2.2%
Theatre Session Utilisation [Main Theatres] 94.8% 96.5% 92.0% 4.5% 93.7% 92.0% 1.7% Financial Result Total $m (negative is contribution)
0.19$ 0.31-$ 1.28-$ 11.37-$ 14.10-$
ED KPI 2 (TGA Only) 45.8% 47.4% 95.0% (47.6%) 47.1% 95.0% (47.9%) Non Contact FSA's (virtual) U/D
ED 6 hr Target 89.4% 91.1% 95.0% (3.9%) 90.9% 95.0% (4.1%)
ED Re-Presentation Rate U/D
Eligible Stroke Patients Thrombolised U/D
Electronic Inpatient Discharge Summaries sent within 24 hours 0.0% #DIV/0! 95.0% #DIV/0! 77.7% 95.0% (17.3%)
KEY
Month Year to date Month Year to dateBEST VALUE FOR HEALTH SYSTEM RESOURCES
22
Jan-14
Key: Trend Arrows shows improvement, shows deterioration, shows no change, from previous month
Target Achieved (A), Target Not Achieved (NA)
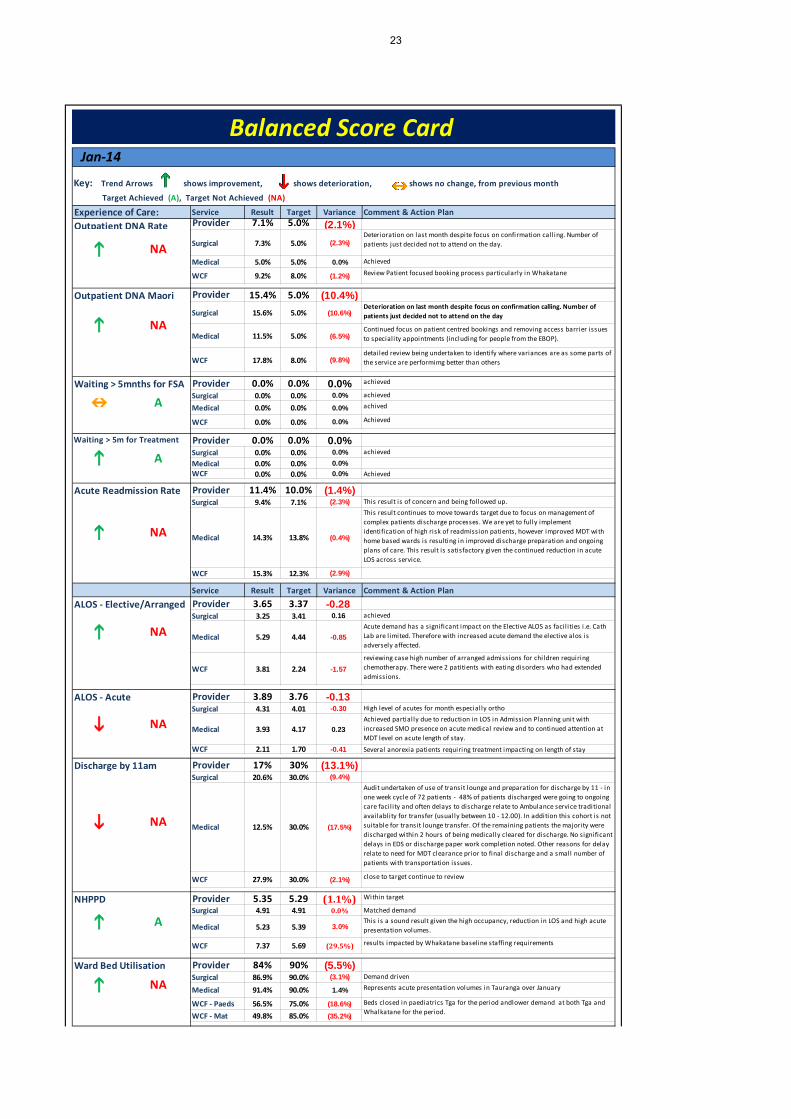
Experience of Care: Service Result Target Variance Comment & Action Plan
Outpatient DNA Rate Provider 7.1% 5.0% (2.1%)Surgical 7.3% 5.0% (2.3%)
Medical 5.0% 5.0% 0.0%
WCF 9.2% 8.0% (1.2%)
Outpatient DNA Maori Provider 15.4% 5.0% (10.4%)Surgical 15.6% 5.0% (10.6%)
Medical 11.5% 5.0% (6.5%)
WCF 17.8% 8.0% (9.8%)
Waiting > 5mnths for FSA Provider 0.0% 0.0% 0.0%Surgical 0.0% 0.0% 0.0%
Medical 0.0% 0.0% 0.0%
WCF 0.0% 0.0% 0.0%
Waiting > 5m for Treatment Provider 0.0% 0.0% 0.0%Surgical 0.0% 0.0% 0.0%Medical 0.0% 0.0% 0.0%WCF 0.0% 0.0% 0.0%
Acute Readmission Rate Provider 11.4% 10.0% (1.4%)Surgical 9.4% 7.1% (2.3%)
Medical 14.3% 13.8% (0.4%)
WCF 15.3% 12.3% (2.9%)
Service Result Target Variance Comment & Action Plan
ALOS - Elective/Arranged Provider 3.65 3.37 -0.28 Surgical 3.25 3.41 0.16
Medical 5.29 4.44 -0.85
WCF 3.81 2.24 -1.57
ALOS - Acute Provider 3.89 3.76 -0.13 Surgical 4.31 4.01 -0.30
Medical 3.93 4.17 0.23
WCF 2.11 1.70 -0.41
Discharge by 11am Provider 17% 30% (13.1%)Surgical 20.6% 30.0% (9.4%)
Medical 12.5% 30.0% (17.5%)
WCF 27.9% 30.0% (2.1%)
NHPPD Provider 5.35 5.29 (1.1%)Surgical 4.91 4.91 0.0%
Medical 5.23 5.39 3.0%
WCF 7.37 5.69 (29.5%)
Ward Bed Utilisation Provider 84% 90% (5.5%)Surgical 86.9% 90.0% (3.1%)
Medical 91.4% 90.0% 1.4%
WCF - Paeds 56.5% 75.0% (18.6%)WCF - Mat 49.8% 85.0% (35.2%)
High level of acutes for month especially ortho
Demand drivenRepresents acute presentation volumes in Tauranga over January
close to target continue to review
Within target
Matched demandThis is a sound result given the high occupancy, reduction in LOS and high acute presentation volumes.
results impacted by Whakatane baseline staffing requirements
reviewing case high number of arranged admissions for children requiring chemotherapy. There were 2 patitients with eating disorders who had extended admissions.
Deterioration on last month despite focus on confirmation calling. Number of patients just decided not to attend on the day
Continued focus on patient centred bookings and removing access barrier issues to speciality appointments (including for people from the EBOP).
detailed review being undertaken to identify where variances are as some parts of the service are performimg better than others
This result is of concern and being followed up.This result continues to move towards target due to focus on management of complex patients discharge processes. We are yet to fully implement identification of high risk of readmission patients, however improved MDT with home based wards is resulting in improved discharge preparation and ongoing plans of care. This result is satisfactory given the continued reduction in acute LOS across service.
achieved
Achieved
Deterioration on last month despite focus on confirmation call ing. Number of patients just decided not to attend on the day.
Achieved
Review Patient focused booking process particularly in Whakatane
Beds closed in paediatrics Tga for the period andlower demand at both Tga and Whalkatane for the period.
achieved
achievedachived
Achieved
Achieved partially due to reduction in LOS in Admission Planning unit with increased SMO presence on acute medical review and to continued attention at MDT level on acute length of stay.
Several anorexia patients requiring treatment impacting on length of stay
Audit undertaken of use of transit lounge and preparation for discharge by 11 - in one week cycle of 72 patients - 48% of patients discharged were going to ongoing care facil ity and often delays to discharge relate to Ambulance service traditional availablity for transfer (usually between 10 - 12.00). In addition this cohort is not suitable for transit lounge transfer. Of the remaining patients the majority were discharged within 2 hours of being medically cleared for discharge. No significant delays in EDS or discharge paper work completion noted. Other reasons for delay relate to need for MDT clearance prior to final discharge and a small number of patients with transportation issues.
achievedAcute demand has a significant impact on the Elective ALOS as facil ities i .e. Cath Lab are l imited. Therefore with increased acute demand the elective alos is adversely affected.
Balanced Score Card
NA
NA
A
A
NA
NA
NA
NA
A
NA
23

Service Result Target Variance Comment & Action Plan
Day of Surgery (DOSA) Provider 94.2% 95.0% (0.8%)Surgical 93.3% 95.0% (1.7%)WCF 100.0% 95.0% 5.0%
Day Surgery Rate Provider 69.5% 59.2% 10.3%Surgical 70.3% 59.8% 10.5%WCF 57.8% 66.1% (8.3%)
Theatre Session UtilisationProvider 96.5% 92.0% 4.5%Surgical Tga 96.7% 93.0% 3.7%Surgical Whk 95.8% 93.0% 2.8%WCF 117.2% 93.0% 24.2%
ED KPI 2 Provider 47.4% 95.0% (47.6%)Surgical 51.7% 95.0% (43.3%)
Medical 46.4% 95.0% (48.6%)
WCF 41.8% 95.0% (53.2%)
6 Hour Target Provider 91.1% 95.0% (3.9%)
NA
LOS Outlier Provider 3.1% 1.5% (1.6%)Surgical 3.4% 1.5% (1.9%)
Medical 4.0% 1.5% (2.5%)
WCF 1.4% 1.5% 0.1%
Smokers Referred to Cessation Provider 91.5% 95.0% (3.5%)
NA
System: Service Result Target Variance Comment & Action Plan
Sick Leave Provider 1.9% 3.1% 1.2%Surgical 2.0% 3.1% 1.1%Medical 1.8% 3.1% 1.3%WCF 2.5% 3.1% 0.6%Support Service 2.1% 3.1% 1.0%Maori Health 1.4% 3.1% 1.7%RCS 1.3% 3.1% 1.8%
Mental Health 2.3% 3.1% 0.8%
Mandatory Training completed Provider 75.9% 100.0% (24.1%)within 3m of start date Surgical 72.0% 100.0% (28.0%)
Medical 81.8% 100.0% (18.2%)
WCF 47.6% 100.0% (52.4%)
Support Service 100.0% 100.0% 0.0%
Maori Health 0.0% 100.0% (100.0%)
RCS 100.0% 100.0% 0.0%
Mental Health 70.6% 100.0% (29.4%)
Annual Leave balance >2yrs Provider 6.0% 0.0% (6.0%)Surgical 5.6% 0.0% (5.6%)
Medical 6.1% 0.0% (6.1%)
WCF 16.4% 0.0% (16.4%)
Support Service 6.6% 0.0% (6.6%)
Maori Health 14.5% 0.0% (14.5%)
RCS 2.8% 0.0% (2.8%)
Mental Health 2.5% 0.0% (2.5%)
High levels of staff on leave over the period but result sti l l impacted on a small number of parttimers accumulating leave
Improved from last monthLeave planning continues to manage down high leave balances. Significant factor SMO leave balances.
Despite leave being planned and taken some areas sti l l struggling to reduce given
Nursing is the main issues working with staff to bring down
No Issues
Team leaders to manage compliance achieved
achieved
Big improvement from last monthContinued improvement - JMO and SMO orientation remains an issue
main issue is RMO orientation
achievedachievedachieved
achieved
LOS outleirs are reviewed twice a week following the IOC meeting of the day with each patient discussed as to determine clinical appropriateness and highlight stranded patients. If te patienst are stranded they are discussed further for strategies to move the patient to discharge.
The January 2014 result of 91% is in l ine with last months result. Total volumes remain significantly up on last years activity, with health target qualifying attendances up 2.3% on the same month last year, and 7.1% for the YTD. Whakatane ED continues to deliver above target (99%), with Tauranga performance below target (87%).Out of hours activity continues to be identified as an area of high impact. Presently, there is a project to look at the hospital at night, which will appraise the availabil ity of all resources and their responsiveness to demand surge. Additionally, the project will look at the tasks required at night and how these may be spread more effectively across all the available resources. Surges in patient numbers and high acuity have been contributing factors with weekend demand also influencing the result. In response, a third medical registrar is now rostered on to the weekends to assist in managing demand. The monitoring and measurement of demand continues to improve, with ‘breach’ reporting in place to identify individual ‘breaches’ with the cause and effect for daily analysis. The model of medicine introduced in mid-July continues to be developed to increase the focus on the front door. In January the function and form of APU is to be reviewed and developed particularly with respect to the flow from ED to APU. The Heads of Departments are now meeting on a regular basis to support improvement on this measure. The Standard Operating Procedure (SOP) for Acute Demand is currently out for consultation with all departments. Tauranga Hospital remains focused on achieving the whole of system action plan outlined in previous Dashboard reports.
Achieved
achieved
It is important to note that data is for all patients not those that have failed the 6Hr target. Based on breach reports the number of patienst fail ing the 6Hr target with Medicine KPI 2 as a contributing factor has been reduced.
Good result for month
Achieved
Achieved
No change from last month
reviewing data recording as this result differs from daily breach reports
Relects case complexity
NA
NA
NA
A
A
NA
NA
A
24

Service YTD Result YTD Target Variance Comment & Action Plan
Elective CWD Provider 5,597 5,774 -177 Surgical 4,694 4,858 -164
Medical 442 469 -27
WCF 461 447 14
Elective Discharges Provider 4,163 4,072 91Surgical 3,637 3,555 82WCF 526 516 10
Acute / Arranged CWD Provider 16,584 15,972 612Surgical 5,322 5,172 150
Medical 8,019 7,392 627
WCF 3,243 3,408 -165
OP FSA Provider 12,527 12,050 477Surgical 6,927 6,520 407
Medical 3,587 3,687 -100
WCF 2,013 1,843 170
OP FU Provider 30,684 28,905 1,779Surgical 15,908 15,061 847
Medical 8,586 8,654 -68
WCF 6,190 5,189 1,001
Service Result Target Variance Comment & Action Plan
Operating Expenses Provider 8,514 8,719 205Surgical 2,833 3,056 224
Medical 1,956 1,943 -14
WCF 343 305 -39
Support Service 102 68 -34 Maori Health 10 13 3
RCS 889 864 -26
Mental Health 288 300 12
Personnel Costs Provider 16,789 15,493 -1297 Surgical 5,192 4,500 -692
Medical 4,237 3,981 -256
WCF 1,660 1,430 -231
Support Service 593 498 -95 Maori Health 407 293 -113
RCS 2,039 2,063 24
Mental Health 2,094 2,055 -39
FTE's Provider 2,174 2,162 -12 Surgical 592 562 -30
Medical 524 507 -17
WCF 170 157 -13
Support Service 148 136 -12
Maori Health 63 50 -13
RCS 334 384 50
Mental Health 285 297 11
Undercontracted in FU as a result of incorrect Gen Surg FSA:Fup ratioYTD variance reduced from -191 last month to -68. Greater volume of cl inic performed due to less annual leave, reduced acute medicine model impact and increased physician numbers across both sites
F/u ratios being monitored and trending down
Nursing FTE(5) as detailed above with LOS adjust of 3 FTE in conjunction with impact of unbudgetted safety watch. In addition number of unbudgetted FTE approved in year. SMO FTE remains positive however this is offset in operating costs of locums to cover vacancies.
SMO vacancy factor (1.00 FTE); Medical annual leave impact 3.50 FTE; LOS adjuster FTE (5.38); Midwifery vacancy Factor (3.00 FTE); HCA speciall ing in Paeds (3.68 FTE); Lieu Leave impact (2.09 FTE);
Medical Ward nursing( 0.77 fte under) Mental Health Nursing (0.33 fte under)
Mainly due to the large amount of Annual Leave taken in the month esp. services built around school terms e.g. PHN's & Dental services
Vacancies in a number of All ied Health areas and the impact of annual leave taken (and not replaced) offset sl ightly by DNS requirements due to patient demand and also budgeted vacancy factors
Nursing over budget by 34 FTE for month (5 FTE theatre activity) -ve 1 l ine of 17FTE Patient transport over by 2 FTE
Behind on Orth electives due to high acute volumes
ahead of target
LOS Adjuster -2.09 fte and $170.526 Nurse effeciencey adjuster 1.05 fte and $77.96
Nursing over budget by 34 FTE for month (5 FTE theatre activity) One l ine adjusters fri nursing equating to 5 FTE and impacting -$375K YTD, in addition IR adjuster equivalent to 8 FTE across all service groups equatingYTD to $428K. Medical Staffing vacancies offset against locum costs as detailed above
Staff 1 Line Adjuster & Vacancy Factor in Budget ($72k); High levels of speciall ing (HCA) in TGA Paeds ($14k); Annual Leave growth due to Lieu leave impact ($116k); Timing of Professional Fee payments ($9k)
Within budgetLocum costs remain the highest contributing factor with vacancies in first half of the year affect YTD. This is however reducing as vacancies are steadily fi l led including long standing vacancies at Whakatane which have now been recruited to with permanent staff. Oanotehr significant area has been gastroenterology (fully recruited) however due to colonoscopy requirements the gastroenetrologists remain off the acute medicone roster being backfil led with locums.
Mainly due to RMO / SMO locum cover esp. WHK O&G's offset by lower demands on clinical supplies due to fall ing patient numbers
Continue to mange within budget as often as canMainly due to OPINS contract budgeted at 50% of actual , Te Kaha SMO Locum , Audiology locums offset by timing of Support Net payments
The variance YTD has been reduced compared to last month. The variance remains significantly impacted by the Haematology FSA currently having to be done in Waikato. ahead of target
achieved
High acute demandAcute demand drives acute CWD and there has been a increase in acute demand
demand driven
As detailed above elective procedures are low volumes and are dependant on l imited resources (staffing and facil ities). Acute demand therefore has a significant impact on elective delivery.
Ahead of target
achieved
A
A
A
NA
A
A
NA
NA
25

FINANCIAL
Month Ended: FY Period 7 -JanuaryDivision: PROVIDER
Actual Budget Var Var % Actual Budget Var Var %($000's) REVENUE ($000's)
14,102 13,616 486 4% Government Revenue 24,008 23,342 666 3%2,594 2,390 204 9% Other Revenue 4,097 4,097 - 0%
173,499 174,197 698- 0% Funder Revenue 300,903 299,905 999 0%190,194 190,203 8- 0% Total Revenue 329,009 327,344 1,665 1%
EXPENDITURE113,298 111,327 1,970- -2% Staff Costs 196,720 192,787 3,933- -2%
12,917 10,723 2,194- -20% Outsourced Costs 21,912 18,472 3,440- -19%30,397 31,827 1,430 4% Clinical Costs 53,753 55,423 1,670 3%
9,570 9,535 35- 0% Infrastructure Costs 16,549 16,549 - 0%12,643 12,695 52 0% Recharges 21,762 21,762 - 0%
178,824 176,107 2,717- -2% Total Expenditure 310,696 304,993 5,703- -2%11,371 14,096 2,725- -19% Net Result 18,313 22,351 4,038- -18%
2206.40 2162.21 -44.19 -2% FTE 2,162.21 2,162.21 - 0%
BOPDHB Provider2013/2014
Year to Date Year End Estimate
-3,500
-3,000
-2,500
-2,000
-1,500
-1,000
-500
-
500
Mon
thly
resu
lt $0
00's
Monthly Net Result
Result Budget
6,000
7,000
8,000
9,000
10,000
11,000
12,000
Mon
thly
resu
lt $0
00's
Monthly Operating Costs
Result Budget
13,500
14,000
14,500
15,000
15,500
16,000
16,500
17,000
Mon
thly
resu
lt $0
00's
Monthly Staff Costs
Result Budget
26

FY Period 7 -January YTDTotal Variance: 974,593-$ 2,725,232-$
Revenue: 117,076$ 8,459-$
Salaries & Wages: 1,296,624-$ 1,970,210-$
-$252,357-$1,688,895
Outsourced: 172,431-$ 2,194,002-$
$392,720-$237,935
-$1,430,940-$336,262
Clinical Supplies: 268,337$ 1,430,326$
$154,501$48,456
$334,205$245,945
-$276,652$303,634$523,928
Infra-Structure: 92,568$ 34,926-$
Recharges: 16,293$ 51,851$
$44,912$22,414
Year End ForecastActual: 18,312,864$ 4,038,106-$
* Renal fluids and supplies* Road & Air Ambulance
* Instruments & equipment
* Blood products* Pharmaceutical drugs excluding Oncology
* Implants
* Ophthalmology outsourced service is under YTD plan but will be on track by year end
* Vehicle use
Variance to Budget:
* Publishing
Significant positive variance in implants and patient transfers. The clinical supplies group of expenses is $1m or 4% lower than the corresponding period last financial year. $102k positive variance YTD for Intragam
BOPDHB Provider
Though S&W variance was very high for the month of January this is partly related to the higher than seasonaly expected number of acute patients through the hospital and partly relating to low budget phasing for the month. A review of nursing workload for the month shows there was no further capacity to reduce staff and if anything staffing levels provided were just enough to match demand. YTD we have had 6.0% more ED attendances than same period in the prior year with Tauranga up by 7.8% and Whakatane up by 2.8%. YTD we have experienced approximately 4% more discharges than same period last year.
Financial Commentary - PROVIDER
Year to date elective CWD are 177 below plan and acute CWD are CWD are 612 ahead of plan. The value of unfunded acute CWD over delivery is $2.85m. Public Health funding is $351kk ahead of plan YTD and expected to be $471k above plan by year end.
Some good savings materialising in communications with new contract
Some overspend in doctors but offset by under recruitment in-house with some vacancies and SMO positions that are slower to recruit to.
* Doctors are over budget* Nursing is over budget YTD
* Oncology drugs
* Outsourced doctors is over budget YTD* Orthopaedic outsourced service is above YTD plan but is expected to be on target by year end
* Outsourced nursing is over budget mainly related to Opotiki
27

FTE RESOURCE MANAGEMENT
Very high acute workload made January a challenging month. CONTRACTS Acute demand above planned levels continues to be a factor as can be seen in the graphs below. Higher acute numbers particularly in Orthopaedics has a crowding out effect on electives. There is a plan in place to address elective under delivery.
FY Period 7 -JanuaryData
Account Report Group1FTE
ActualFTE
Budget
FTE Variance Actual to Budget
FTE Variance% Actual to Budget
FTE Actual YTD
FTE Budget
YTD
FTE Variance Actual to
Budget YTD
FTE Variance% Actual to
Budget YTD
MEDICAL PERSONNEL 2002 281.62 295.55 13.93 4.71% 286.54 295.55 9.01 3.05%NURSING PERSONNEL 2202 1,106.72 1,038.97 -67.75 -6.52% 1,091.71 1,038.97 -52.74 -5.08%ALLIED HEALTH PERSONNEL 2402 393.67 450.65 56.98 12.64% 433.95 450.65 16.70 3.71%SUPPORT PERSONNEL 2602 86.69 80.90 -5.79 -7.16% 84.53 80.90 -3.63 -4.49%MANAGEMENT ADMIN PERSONN 2802 305.17 296.14 -9.03 -3.05% 309.67 296.14 -13.53 -4.57%Grand Total 2,173.87 2,162.21 -11.66 -0.54% 2,206.40 2,162.21 -44.19 -2.04%
Month YTD
Printed: 14 February 2014
Note: Graphs monitor all Funder contracted CWD with BOPDHB Provider ArmElectives = All elective CWDAcute & Arranged = all acute and arranged CWD
0
500
1000
1500
2000
2500
3000
3500
4000
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Total CWD Delivery - 2013/14
Elective Acute Contract
0
500
1000
1500
2000
2500
3000
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Acute & Arranged CWD Delivery - 2013/14Acute Uncoded Est Acute Actual
Acute Contract
0
150
300
450
600
750
900
1050
1200
1350
Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun
Elective CWD Delivery - 2013/14
Elective Unocoded Est Elective Actual Elective Total Contract
Elective Base Target Adj Elect Target
28

Property Services General Manager Monthly Report December 2013 / January 2014
1. Red Flags
Nothing to report. Highlights Tauranga Campus Black Building Test Following 4 years of continuous improvement and substantial capital investment in the site electrical systems, on 22 January we switched the main power supply off to the key buildings (those buildings that are supported by genset power) and allowed the automated system to deliver genset power. The key objectives were:
Check the the automated system would work in event of a power failure. Establish the peak mid-day summer energy demand (created by the chiller plant). Check that on returning to mains supply all systems switched back without issues.
The following observations were made:
The system switched to genset power without and issues. The peak load power demand was great then the individual genset capacity. We needed 2 chillers to manage the building cooling demand load.
2. General
Tauranga Campus Site Designation A hearing date has been set down for 20 February, to force the objecting parties to withdraw their objections, or attend the hearing and defend their objections.
3. Project Waka
General The project remains on programme for completion on 4 April. There would appear for be some compression in the Fletchers commissioning programme, however, we have been assured that the quality of commissioning will not be impacted. Our project team will closely monitor the commissioning to minimise the commissioning risks. The DHB is planning it’s own building services performance validation during April. The objective being to test and test again critical items of plant and systems. Project Milestones Construction Commenced 1 January 2012 Planned Completion Date 20 February 2014 Revised Completion Date 4 April 2014 Planned Move Date (start of decanting) Mid-May 2014
29

GM Monthly Report - Dec 2013/Jan 2014 DocMan/Management
Budget FCC Contract: $41,791,319.00 The project remains on budget. Project Waka Decanting Planning for the May 2014 decant is ongoing. During December we arranged for a consultant to undertake a review of the “readiness of the change management and training and orientation work streams”. The consultant’s report identified a number of significant risks. We have engaged an extra change manager to commence on 4 February and take responsibility of the training and orientation work stream. With careful monitoring of the work streams we expect the risk can be managed to an acceptable level. Occupation Readiness Plan (ORP) We continue to add items to the ORP and monitor progress on the actions. Gateway 4 Review The gateway team will be on site 10 to 14 March. I have commenced the preparation of an evidence folder for the team and we are setting up an interview programme. Furniture Fixtures and Equipment Installation of the new steriliser and batch washer in early January was a major milestone for the project. The theatre pendants and lights are due to arrive in NZ in early February, and installation will commence on 17 February.
4. Other Major Projects Tauranga MSB 5 (MSB3 Replacement) Builders Work Planned Commencement Date January 2014 Planned Completion Date March 2014 - Percentage complete last month 40% - Percentage complete this month 70%
30

GM Monthly Report - Dec 2013/Jan 2014 DocMan/Management
Tauranga MSB 5 (MSB3 Replacement) Electrical Work Planning and ordering of materials and equipment is underway. Planned Commencement Date April 2014 Planned Completion Date August 2014 - Percentage complete last month 5% - Percentage complete this month 15%
Whakatane – New Water Tanks We have agreed with Fletchers than the project is more suited to the contractor with major steelwork experience. Page McCrae have been engaged to manage and deliver the construction of the water tanks and associated piping. Planned Commencement Date July 2013 Planned Completion Date August 2014 - Percentage complete last month 6% - Percentage complete this month 10% Tauranga - Kowhai House (Community Mental Health) Fire Compliance Works (Stage 2) Work commenced during the Xmas / New Year period and the new reception and waiting room area was completed with a minimum of disruption to the business unit. Work is currently underway to fit-out the ex-library area into publications and a union office area. The balance of the work will be progressively completed up to August. Planned Completion Date July 2013 Revised Planned Completion Date August 2014 - Percentage complete last month 10% - Percentage complete this month 40%
Tauranga MSHOP and SHSOP Improvement works This project is now complete and we have received positive feedback. Planned Completion Date February 2014 Percentage complete last month 10% - Percentage complete this month 100%
Tauranga – Clarke St Car Park Lift Upgrade This work is now complete. Planned Completion Date December 2013 Percentage complete last month 80% - Percentage complete this month 100%
Whakatane – Santon Demolition and Post Demolition Strategy On Friday 6 December a 2 hour drop in session was held and we received constructive feedback. A further meeting was held with the doctors in January to clarify their specific needs. A final concept will be tabled in February for final sign-off.
31

GM Monthly Report - Dec 2013/Jan 2014 DocMan/Management
Early indications are that during the demolition period we may be short of some office space as approximately 12 works spaces that are in the demolition safety zone. Planned Completion Date December 2014 - Percentage complete last month 50% - Percentage complete this month 75%
Whakatane – Relocation of Pathlab to a Stand-alone Facility Heads of Agreement has been executed by both parties Final design is due for sign-off by 30 January. Revised Planned Completion Date August 2014 - Percentage complete last month 8% - Percentage complete this month 15%
Tauranga ED UPS Upgrade The room has been upgraded and the new UPS installed Completion Date February 2014 - Percentage complete last month 20% - Percentage complete this month 75%
Tauranga Theatre UPS Upgrade No progress due the resources working on the ED UPS. Planned Completion Date January 2014 - Percentage complete last month 25% - Percentage complete this month 25%
Tauranga Intermediate – Fixed Dental Clinic Work will commence in late December, following receipt of the building consent. Planned Completion Date April 2014 - Percentage complete last month 8% - Percentage complete this month 15%
Tauranga Boiler House Seismic Upgrade AMC has approved the funding. Planned Completion Date August 2014 - Percentage complete last month 0% - Percentage complete this month 5% Tauranga Campus – Energy Management Programme The first stage of the programme has been completed and the opportunities for energy savings identified. The cost of stage one has been partly funded by ECCA. We now await the full report before being able to commit to the implementation of the actions to deliver the savings.
32
GM Monthly Report - Dec 2013/Jan 2014 DocMan/Management
Security Access System Upgrade A full upgrade of the security system will be undertaken. The upgrade includes conversion to a windows-based system and a reliable system configuration. Tauranga – Emergency Lighting Upgrade Following preparation of as-built plans, we will now re-write and upgrade the non-compliant BWOF system. The issues identified are all ex Project Leo. Planned Completion Date August 2014 - Percentage complete last month 5% - Percentage complete this month 10%
5. Third Party Projects Radiotherapy Development (KKC)
Work is proceeding without any direct impacts on the DHB. The underpinning of the Cancer Centre has commenced by KKC. Further work is planned for February. Planning of how space will be used by the Cancer Centre will be undertaken in February.
Northern Campus Development (NCD) No progress to report on NCD. 6. Risk, Compliance & OHS
Following the running of a further training coruse there has been an improvement in the deployment of on the job writing of JSA’s by the DHB staff. We will continue to monitor the use of JSA’s.
7. Facilities Management Update Following implementation of the facilities manager being the first point of call for after-hours call-outs, we continue to experience a reduction in call-outs. This Month December
Fire Alarms Activation (false) TGA - Site General 1 - Acute Mental Health 0 WHK - Site General - Ward 8 0 We have been charged $1500 for the event by the NZFS.
33

GM Monthly Report - Dec 2013/Jan 2014 DocMan/Management
Fire Alarms Activation (real) TGA - Site General - Acute Mental Health 0 WHK - Site General 0 - Ward 8 0 Reportable Events TGA WHK 2 Power interruption TGA 1 Power interruption WHK 0 Lost time injury TGA 0 Lost time injury WHK 0 After Hours Call-outs TGA this month 10 WHK this month 0 This Month January Fire Alarms Activation (false) TGA - Site General 0 - Acute Mental Health 0 WHK - Site General 0 - Ward 8 3 We have been charged $1500 for the event by the NZFS. We are working with Ward 8 to reduce the false call-outs. Fire Alarms Activation (real) TGA - Site General 0 - Acute Mental Health 0 WHK - Site General 0 - Ward 8 0 Reportable Events TGA WHK 0 Power interruption TGA 1 (planned Black Test) Power interruption WHK 0 Lost time injury TGA 0 Lost time injury WHK 0 After Hours Call-outs TGA this month 12 WHK this month 6
34
GM Monthly Report - Dec 2013/Jan 2014 DocMan/Management
8. Property Management Nothing to report.
9. National & Regional Facilities Management Initiative Regional Nothing to report. National Jeff Hodson will be chairing the monthly conference calls.
35

Reducing Perioperative Harm SUBMITTED TO: Bay of Plenty Hospital Advisory Committee 26 February 2014 Submitted by: Rosalind Jackson, Nurse Leader, Anaesthesia and Surgical Services Endorsed by: Helen Mason, Chief Operating Officer RECOMMENDED RESOLUTION: That BOPHAC review and accept this report. ATTACHMENTS: Surgical Safety Checklist BACKGROUND: Reducing perioperative harm will be the third programme for Health Quality and Safety Commission’s Open campaign, from April to mid-2014. The surgical safety checklist has been selected as the focus for this part of the programme representing an evidenced based tool to ensuring the correct surgical procedures are carried out on the correct patient. When implemented properly the checklist requires our theatre staff to stop and consider what they are doing and why. It involves checking the right people are present and that they all are in agreement about why they are operating.
The surgical safety checklist used at Tauranga and Whakatane theatres has been adapted from the World Health Organisation’s checklist, is consistent across the district and complies with the content recommendations from a recent national stocktake undertaken by the commission.
As part of our reporting requirements to the commission, Lorraine Wilson, Quality and Patient Safety Co-ordinator submitted a draft report to the Quality and Patient Safety Manager outlining BOPDHB’s results and response against quality safety marker for the audit period 2013 Q4, Oct-Dec 2013. For this document the following information has been sourced from this draft report and Lorraine’s contribution is acknowledged.
36

The HQSC asks DHBs to report on the following question: What proportion of operations in the
sample audit had all three parts of the surgical checklist used? Concepts related to use of the Safe Surgery Checklist (SSC) are well understood in our perioperative departments following investment in team building in previous years. Anecdotal evidence has suggested that at the time of the baseline audit (beginning of 2013), the SSC was often filled in as a box-ticking exercise and was not always used as a tool to guide structured conversation between surgical team members. Our DHB has continued to respond very positively to the challenge to improve compliance. Improvement activity for this quarter builds on activity initiated following the baseline and Q3 audits and is summarised following the results section of this report. DATA COLLECTION: This summary reports on data collected for the quarter October – December 2013. Perioperative Charge Nurse Managers (CNMs) were asked to confirm what data collection method they wanted to use. Both elected to do as they had done for the Q3; Whakatane elected to continue to use a retrospective audit of health records, whilst Tauranga wanted to continue with observational audits. The combined results are
Method
No. of observations/
health records
No. that were
compliant %
compliant
TAURANGA TGA observations 81 73 90% WHAKATANE Retrospective audit of health records 45 33 73% Combined Whakatane and Tauranga results (reported) 126 106 84%
Note. Base refers to our baseline result after the first round of submitting data to the commission
37

Our performance nationally for our baseline and 2013Q3 results are,
IMPROVEMENT ACTIVITY: Whilst the combined results appear disappointing it is important to consider these results in context. Currently there remain no opportunities to train auditors within a national standardised framework because this is not currently being offered by the commission. We continue to wait for national leadership to provide a uniform approach and guidance around data collections going forward. We also have not received any feedback related to our investment in undertaking the quarterly audits to date (however we expect this to change once the programme gets underway). Anecdotally, observational audit encourages correct use of the checklist because people are being observed. However considering available resources for audit we elected to give the CNM’s the choice of audit method. A consistent method of data collection will be implemented once the national direction is confirmed. Furthermore, the approach that midland DHB’s are taking to data collection will be explored via the Midland “Open” Quality Steering Group.
38

Therefore, we are mindful that submission of poor quality data that lacks structured context, poses a risk to the gains that can be realised from enhanced understanding about the importance of the SSC. Consequently we have put strategies in place to minimise these risks and build positive momentum until such time as the national programme finds its feet. The medical and nursing leads for surgical services continues to promote the correct use of the SSC as do senior staff members of the Perioperative User Group in Tauranga. The perioperative Nurse Educator (NE) at Tauranga continues to promote orientation and training information about the SSC that has been recently developed, and these materials have also been provided to all perioperative staff. It is also provided to all new staff as part of their orientation to the Tauranga perioperative department where it is now mandatory that this training is completed every 12 months. Where breaches in the use of the SSC occur the NE provides a one on one session to the staff member responsible. Resources developed in Tauranga have been shared with Whakatane. It will be some time before the quality of data collected (both from our DHB as well as across the country) can be relied upon; especially related to standardisation of audit methodology and feedback. However we are making the most of this requirement by using it to highlight and educate staff about the correct use of the SSC.
39

40

41

Updated 27 December 2013
Bay of Plenty Hospitals Advisory Committee Work Plan 2014
Month Activity Documentation Source
January • No meeting February • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
March • No Meeting April • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
May • No Meeting June • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
July • No Meeting August • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
Sept • No meeting Oct • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
Nov • No Meeting Dec • Monthly COO Report
• General Manager Property Services Report
• COO • GMPS
42

DNA Project Summary SUBMITTED TO: Bay of Plenty Hospital Advisory Committee (BOPHAC) 26th February 2014 Prepared by: Dr George Gray, Public Health Physician, Maori Health Planning and Funding Endorsed by: Janet McLean, General Manager, Maori Health Planning and Funding Submitted by: Janet McLean, General Manager, Maori Health Planning and Funding RECOMMENDED RESOLUTION: That BOPHAC note the attached summary information on hospital did-not-attend (DNA) rates. ATTACHMENTS: Summary presentation provided to Te Tumu Whakarae BACKGROUND: Dr Gray was engaged as a private contractor by the DHB Maori health general managers’ collective Te Tumu Whakarae (TTW) to provide a summary of DNA rates, issues, and solutions at their November meeting in Dunedin. This information was distributed to the executive leadership team of BOPDHB by Janet McLean. Dr Gray was asked to summarise this information for BOPHAC by Helen Mason. The aims of the brief project were to:
1. Summarise DNA trends in New Zealand for Maori and non-Maori; 2. Identify the common causes of DNA events; 3. Identify evidence-based solutions which have successfully reduced DNA rates.
The project was completed through quantitative analysis of three years of DNA data for all DHBs (except Auckland) supplied by the Ministry of Health. In parallel, a literature review was performed to identify the leading causes of DNA and evidence-based solutions which have successfully reduced DNA rates. Finally, the DHB with the lowest DNA rates was contacted in an effort to learn more about interventions used to help reduce ASH rates. ANALYSIS: Results (refer to the attached slides for specific journal references):
• DNA events are costly – there are direct and indirect costs for patients and providers. There are opportunity costs for providers where staff are not utilised appropriately;
43

• DNA rates in New Zealand are similar to those seen in other countries such as Australia,
the United Kingdom, and the United States; • DNA rates in New Zealand-based studies have produced results ranging between 5.5
and 27%; • DNA rates for Maori have ranged between 15.5% and 17.5% over the past three years; • Taranaki DHB has consistently achieved the lowest DNA rates for Maori, ranging
between 11.3-12.5% over the past three years. However, inter-DHB DNA comparisons are problematic due to differences in coding used around the country;
• DNA rates are typically 2.5 times those of non-Maori; • Multiple studies have demonstrated that a small proportion of causes account for the
majority of DNA events; • The causes of DNA provide opportunities for tailored interventions. These interventions
may be developed on the basis of published evidence of effectiveness, or through the development and pilot-testing of new interventions;
• Single solutions are unlikely to produce sustainable improvements in DNA rates. A multifactorial and sustained quality improvement methodology is required to generate sustainable and consistent improvements in DNA rates;
• Key intervention points can be identified by mapping the patient journey and identifying barriers to patient attendance. This can be performed through a mixed methods approach involving quantitative analysis and patient interviews. An appropriate intervention may then be developed relevant to patient and provider needs and resources;
• A small number of interventions have been closely evaluated and these are generally focussed on the patient reminder step e.g. patient reminder systems such as personal or automated reminder calls, and text messaging;
• Economic evaluation data on DNA interventions is sparse;
Recommendations Based on the findings of this project lower DNA rates in BOPDHB may be achieved through: 1. Resourcing time for appropriate personnel to work on this issue; 2. Working with the Ministry of Health to identify any national DNA strategies or projects that
BOPDHB could benefit from or become involved with; 3. Standardising DNA terms, definitions, and collection methodology within BOPDHB based on
guidance from the Ministry of Health; 4. Evaluating local DNA intervention needs; 5. Selecting, implementing, and evaluating DNA interventions within the framework of a CQI
system; 6. Sharing DNA data among DHBs in order to track performance and identify leading
organisations. DEFINITIONS USED: Term Definition DNA Did-Not-Attend (Outpatient appointment) TTW Te Tumu Whakarae
44

Outpa&ent)Appointment)A.endance)
Dr)George)Gray)
Public)Health)Physician)
Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
45

Importance)
1. Pa&ent)cost)2. Wai&ng)list)cost)
3. Financial)cost)
Importance)
1. Pa&ent)cost)2. Wai&ng)list)cost)
3. Financial)cost)
46

Seen)by)GP) Referred)to)specialist) Triage)
Appointment)made)
Appointment)info)sent)
Appointment)info)received)
Reminder)generated)
Pa&ent)travels)to)
appointment)
Seen)by)health)professional)
Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
47

Aims)
1. Iden&fy)causes)of)DNAs)2. Iden&fy)evidenceMbased)solu&ons)to)DNAs)
Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
48
Methods)
1. Literature)review)2. Local)data)collec&on)and)analysis)3. Develop)recommenda&ons)
Methods)
1. Literature)review)1. Iden&fy)rates)(interna&onal))2. Iden&fy)rates)(local))3. Iden&fy)reasons)for)DNA)4. Iden&fy)solu&ons)for)DNA)
49
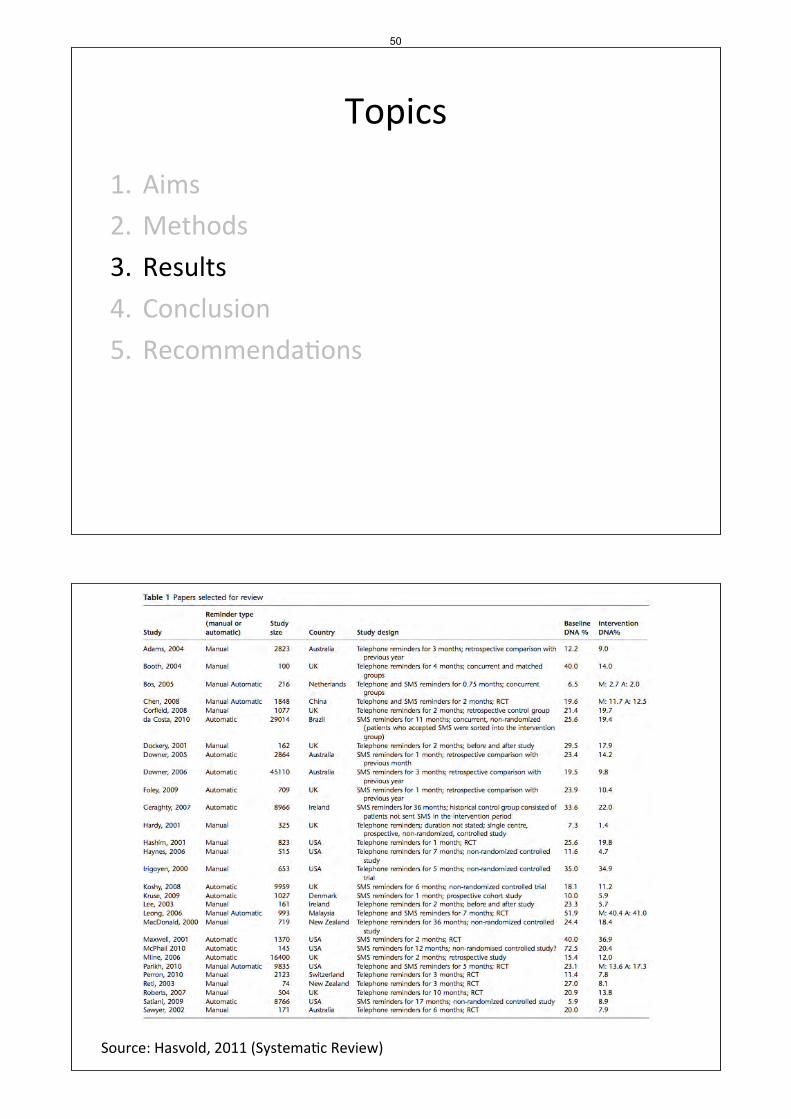
Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
Source:)Hasvold,)2011)(Systema&c)Review))
50

Interna&onal)DNA)Rates)
• Outpa&ent)DNA)rates)vary)by:)– Organisa&onal)factors)
• Clinical)• Administra&ve)
• Logis&cal)– Pa&ent)
• Demographics)
Local)Es&mates)
Year% Author% Es-mate%
1992) Dockerty) 21%)
2002) Coffin,)Emery,)Zwier) 24%)(Māori))
2002) Re&) 5.5M15%)
2003) Re&) 27%)
51

Reasons)for)DNA)
Collins,)2003)
Reasons)for)DNA)
Source:)Collins,)2003)
52
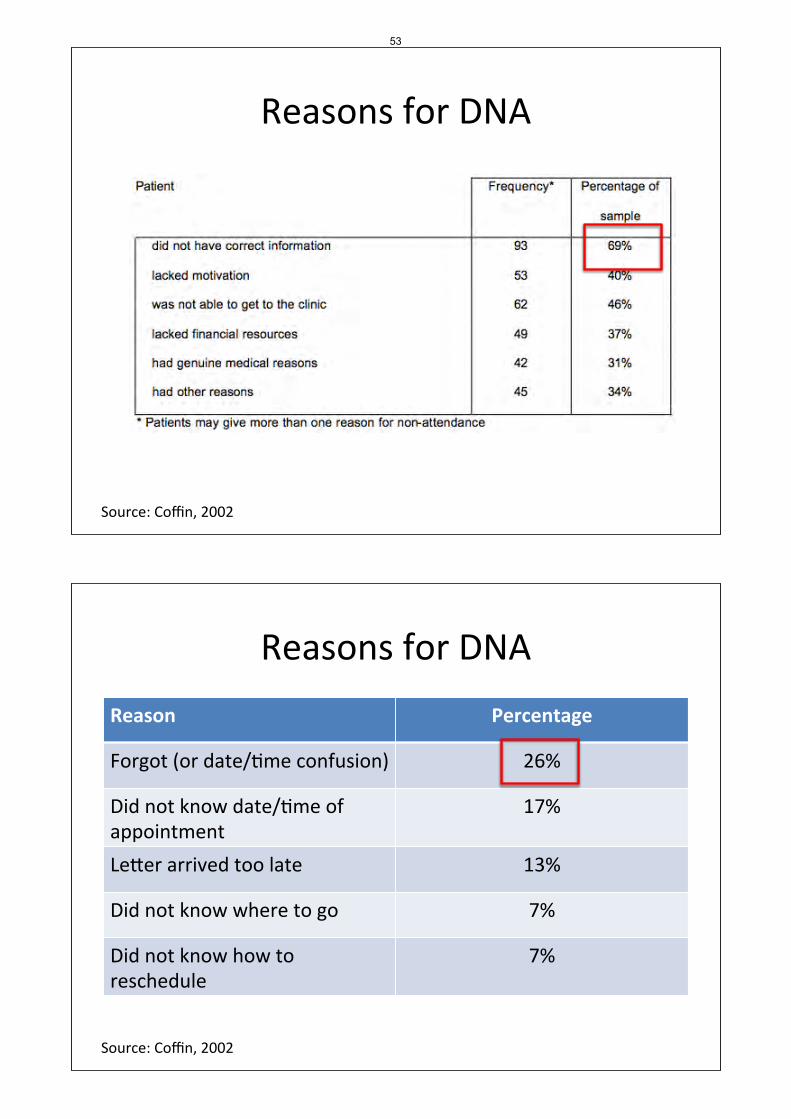
Reasons)for)DNA)
Source:)Coffin,)2002)
Reasons)for)DNA)
Reason% Percentage%
Forgot)(or)date/&me)confusion)) 26%)
Did)not)know)date/&me)of)appointment)
17%)
Le.er)arrived)too)late) 13%)
Did)not)know)where)to)go) 7%)
Did)not)know)how)to)reschedule)
7%)
Source:)Coffin,)2002)
53

Solu&ons)for)DNA)
1. Mul&ple)interven&on)points)
2. Tailored)towards)the)big)causes)of)DNA)
Seen)by)GP) Referred)to)specialist) Triage)
Appointment)made)
Appointment)info)sent)
Appointment)info)received)
Reminder)generated)
Pa&ent)travels)to)
appointment)
Seen)by)health)professional)
54

Interven&ons)
Year% Author% Interven-on% Effect%
2003) Re&) Phone)reminder) 27%)vs)5%)
2011) Hasvold) Manual)vs.)automated)(voice,)SMS))reminders)
Reminders:)10%)absolute)reduc&on:)Manual)39%)(rela&ve)reduc&on),)automated)29%)(rela&ve)reduc&on))
2012) Car) SMS)(Cochrane)review)) SMS)effec&ve)
2012) Guy) SMS)(metaManalysis)and)systema&c)review))
Summary)effect)from)RCTs)=)1.48)
Seen)by)GP) Referred)to)specialist) Triage)
Appointment)made)
Appointment)info)sent)
Appointment)info)received)
Reminder)generated)
30%)
Pa&ent)travels)to)
appointment)
Seen)by)health)professional)
Le.er)reminder)Automated)reminder)Manual)reminder)
55

Seen)by)GP) Referred)to)specialist) Triage)
Appointment)made)
Appointment)info)sent)
Appointment)info)received)
Reminder)generated)
30%)
Pa&ent)travels)to)
appointment)
Seen)by)health)professional)
Results)
1. Literature)review)
2. Local)data)collec&on)and)analysis)
56

Data)Collec&on)
• Assisted)by)Na&onal)Health)Board)• Determined)DNA)defini&on)
• Gathered)three)years)of)DNA)data)• Māori)as)priori&sed)ethnicity)
DNA)Trends)
2010/11) 2011/12) 2012/13) Change)
Māori) 15.4%) 15.4%) 14.9%) M0.5%)
NonMMāori) 6.2%) 6.1%) 5.7%) M0.5%)
Ra&o) 2.5) 2.5) 2.6)
57

DNA)and)Ethnicity) 2010/11 2011/12 2012/13
DHB of Service Maori Non-Maori Maori Non-Maori Maori Non-Maori
Northland DHB 17.1% 5.8% 17.9% 5.7% 16.9% 5.3%
Waitemata DHB 19.4% 9.2% 16.9% 8.6% 15.1% 8.3%
Counties Manukau DHB 14.5% 7.5% 13.1% 6.6% 13.6% 6.9%
Waikato DHB 15.8% 7.3% 16.5% 7.1% 16.6% 6.7%
Lakes DHB 16.7% 6.5% 17.7% 6.1% 14.1% 4.4%
Bay of Plenty DHB 16.6% 5.3% 17.4% 5.4% 16.9% 5.0%
Tairawhiti DHB 18.1% 6.6% 16.1% 5.5% 15.4% 5.0%
Taranaki DHB 12.5% 4.6% 12.4% 4.5% 11.3% 4.7%
Hawkes Bay DHB 14.6% 6.0% 14.4% 6.0% 13.8% 5.7%
MidCentral DHB 12.5% 4.9% 13.2% 5.6% 12.2% 4.9%
Whanganui DHB 19.9% 6.0% 17.9% 5.6% 19.8% 5.6%
Capital and Coast DHB 14.0% 7.0% 13.0% 5.8% 13.2% 5.8%
Hutt Valley DHB 19.4% 8.8% 20.0% 8.8% 19.9% 8.1%
Wairarapa DHB 10.7% 4.3% 18.8% 6.6% 18.6% 6.2%
Nelson Marlborough DHB 15.6% 5.4% 15.3% 5.3% 15.2% 5.1%
West Coast DHB 12.6% 7.2% 10.6% 6.8% 11.4% 6.3%
Canterbury DHB 15.8% 6.8% 14.6% 6.3% 13.8% 6.2%
South Canterbury DHB 11.9% 3.4% 10.8% 3.7% 10.8% 3.3%
Southern DHB 14.5% 5.9% 15.7% 6.2% 15.1% 5.6%
16.9%)15.1%)
13.6%)
16.6%)
14.1%)
16.9%)15.4%)
11.3%)
13.8%)12.2%)
19.8%)
13.2%)
19.9%)18.6%)
15.2%)
11.4%)
13.8%)
10.8%)
15.1%)
5.3%) 8.3%)
6.9%)
6.7%)
4.4%)
5.0%)
5.0%)
4.7%)
5.7%)
4.9%)
5.6%)
5.8%)
8.1%)
6.2%)
5.1%)
6.3%)
6.2%)
3.3%)
5.6%)
0.0%)
5.0%)
10.0%)
15.0%)
20.0%)
25.0%)
30.0%)
Percen
tage%of%O
utpa
-ent%App
ointmen
ts%th
at%Resulted%in%DNA%
Outpa-ent%Did?Not?A@end%Rates%for%Māori%and%Non?Māori%2011/12%
Māori) NonMMāori)
58
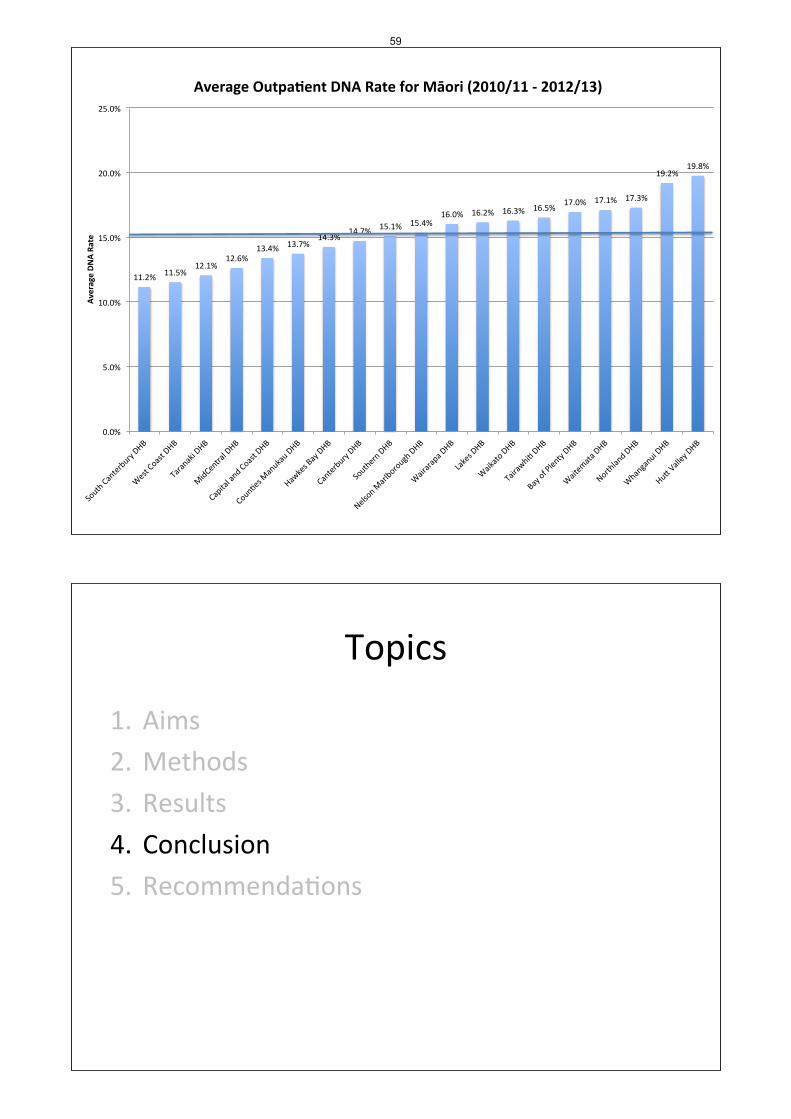
11.2%) 11.5%)12.1%)
12.6%)13.4%) 13.7%)
14.3%)14.7%) 15.1%) 15.4%)
16.0%) 16.2%) 16.3%) 16.5%)17.0%) 17.1%) 17.3%)
19.2%)19.8%)
0.0%)
5.0%)
10.0%)
15.0%)
20.0%)
25.0%)
Average%DN
A%Ra
te%
Average%Outpa-ent%DNA%Rate%for%Māori%(2010/11%?%2012/13)%
Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
59

Aims)
1. Iden&fy)causes)of)DNAs)2. Iden&fy)evidenceMbased)solu&ons)to)DNAs)
Conclusions)
1. NZ)DNA)rates)are)comparable)to)similar)na&ons)
2. DNA)rates)for)Māori)are)2.5)x)nonMMāori)
3. There)are)mul&ple)reasons)for)DNA)events)
4. Mul&ple)solu&ons)are)required)
5. A)small)number)of)interven&ons)have)been)closely)evaluated)
6. Economic)evalua&on)data)is)sparse)
7. Determining)lead)DHBs)is)challenging)
60

Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
Recommenda&ons)
1. Determine)na&onal)DNA)direc&on)with)MoH)2. Standardise)terms)and)methodology)3. Develop)a)CQI)system)4. Collect)&)share)data)5. Iden&fy)relevant)interven&ons)6. Implement)7. Evaluate)8. Repeat)
61

Recommenda&ons)
1. Determine)na&onal)DNA)direc&on)with)MoH)2. Standardise)terms)and)methodology)3. Develop)a)CQI)system)4. Collect)&)share)data)5. Iden&fy)relevant)interven&ons)6. Implement)7. Evaluate)8. Repeat)
Topics)
1. Aims)
2. Methods)
3. Results)4. Conclusion)5. Recommenda&ons)
62

[Paper Ref]
[BOPHAC] [Hand Hygiene Plan]
[Julie Robinson Director of Nursing] February 2014 Page 1 of 2
http://docman/leadership/board/Meetings/BOPHAC/Open/7.1.1 - Hand Hygiene the way forward Cover Paper.doc
Hand Hygiene – the Way Forward
SUBMITTED TO: BOPHAC February 2014 Item No:
Submitted by: Julie Robinson Director of Nursing Endorsed by: Helen Mason Chief Operating Officer
For Information X For Discussion For Decision (Please ensure one of these options is marked)
RECOMMENDED RESOLUTION That the committee note the Hand Hygiene 2014 Improvement Plan.
ATTACHMENTS: Hand Hygiene Improvement Plan 2014.
BACKGROUND Auditing of hand hygiene compliance in District Health Boards (DHBs) throughout the country is a key component of the HHNZ (Hand Hygiene New Zealand) programme. Auditing takes place three times a year and data is submitted to HHNZ and the Health Quality & Safety Commission so it can be captured at a national level. The Hand Hygiene programme was placed under the Patient Safety Committee for monitoring and oversight in November 2012. A revised project plan with a range of initiatives culminating in the WHO International Hand Hygiene Day 5 May 2013 was supported through the Clinical Governance Committee For the period 1 July 2013 to 31 October 2013 BOPDHB did not manage to meet the national 70% compliance and was ranked 20 out of 20 DHBs. It is pleasing to note there has been an increase in the number of staff who have completed the on line learning module which is fundamental to understanding the “5 Moments of Hand Hygiene”. The Junior doctors have a very good uptake. The Hand Hygiene Steering group has developed an updated plan for 2014.
IMPACTS ON BAY OF PLENTY DHB GOALS AND OUTCOMES Given good hand hygiene is one of the most important measures in the fight against healthcare associated infections (HAIs) this makes it a key patient safety issue for us
64

[Paper Ref]
[BOPHAC] [Hand Hygiene Plan]
[Julie Robinson Director of Nursing] February 2014 Page 2 of 2
http://docman/leadership/board/Meetings/BOPHAC/Open/7.1.1 - Hand Hygiene the way forward Cover Paper.doc
all. In addition to posing a grave threat to patient safety, the economic burden for HAIs is significant across the globe, but high standards for hand hygiene represent a simple, cost-effective opportunity to minimize the impact of these potentially dangerous infections.
65

Plan to Improve Performance in the Hand Hygiene Target
February 2014
66

Plan to Improve the Performance of Bay of Plenty DHB in the five moments of hand hygiene 7 February 2014
Background
Hand hygiene prevents transmission of harmful microorganisms between patients or between anatomical sites on the individual patient that are prone to become infected.
It has been recognised internationally that the ‘5 moments for hand hygiene’ result in less hospital acquired infections
The five moments are:
• Before touching a patient.
• Before a procedure.
• After a procedure or body fluid exposure risk.
• After touching a patient.
• After touching a patient’s surroundings.
Hand hygiene is one of the three infection prevention and control projects coordinated by the Health Quality & Safety Commission along with surgical site infection and CLAB zero (Central line associated bacteraemia).
Results of audits
The national target is currently set at 70%.
In 2012, Bay of Plenty District Health Board ranked 20 of the 20 DHBs with an overall compliance of 43.4%. Nationally the compliance results ranged between 43.4% – 77%.
Following a communications campaign in early 2013 we increased our performance to 67%. Unfortunately our performance slipped in the last audit after we had the target in our sights from the previous audit period.
Hand Hygiene Clinical Lead Dr Joshua Freeman says an important part of education is not only to explain when hand hygiene is necessary but also why it is important.
“Our aim is to get to the point where every healthcare worker employed in a New Zealand hospital knows exactly when hand hygiene is necessary during patient care to interrupt the transmission of potentially harmful microorganisms,” he said.
“At its most basic level, hand hygiene prevents transmission of harmful microorganisms between anatomical sites on the individual patient that are prone to becoming infected. The driving reason to perform hand hygiene is, therefore, not for self-protection but for the protection of our patients.
67

“Medical staff and senior doctors are a vital ally in the fight to improve hand hygiene behaviour and reduce healthcare associated infections. They are generally regarded as opinion leaders, whose attitudes and beliefs help to shape the attitudes and beliefs of those around them. It is vitally important, therefore, to gain their support whenever possible.
“If our most influential healthcare workers genuinely believe hand hygiene is necessary to protect their patients, then more widespread improvements in practice will inevitably follow,” he say.
Dr Freeman came to Bay of Plenty District Health Board in November 2013, and addressed Grand Round on why staff need to improve their hand hygiene behaviour.
Unfortuantely, all though there was a lot of interest in his presentation, our doctors did not take up his challenge and subsequently their performance was disappointing.
As a DHB we are doing all the right things, but the messages are not resonating with some groups, so the hand Hygiene Steering Group is suggesting that we go back to the basics and putt emphasis on education for all hospital staff. Doctors need a targeted plan as their performance dropped from 55% to 33%.
Plan for 2014
The Hand Hygiene Steering Group agreed that themes for the 2014 year will be to:
• Develop a sustainable campaign.
• Put increased emphasis on education.
• Encourage front line ownership.
• Proactively involve the Hand Hygiene Champions across the organisation.
• Target smaller groups (professional or wards and units).
• Continue with the whole-of-hospitals awareness campaign using the cut-outs of staff.
• Introduce a patient empowerment campaign.
• And develop displays in the hospitals for International Hand Hygiene Day in May.
It is possible that some staff remain unaware of the five moments, therefore education must underpin our on-going campaigns and become our key priority.
If healthcare staff do not know when hand hygiene is necessary during patient care, they are unable to improve their practice.
Encouraging frontline ownership of the principles and practice of hand hygiene will result in a sustainable programme and increased performance in our target.
68

Action Plan Work led by Completion date
Education
Make e-moodle easier to access? Anne Stephens
Medical leaders, and other groups, hold collective e-moodle sessions in the Clinical School as part of their regular meetings.
Group leaders ie John Kyngdon
28 February 2014
Give incentives/prizes for groups who are getting the most staff to complete their e-moodle training.
Julie Robinson March 2014
Building on previous successes
Talk to Bella and Jill Van Walden about what they have done to maintain the sustained improvement in their ward and include in this action plan..
Julie Robinson 16 January 2014
Talk to Terry Jennings about what she is doing in the Renal Unit and incorporate activities in the Champions campaign.
Julie Robinson 16 January 2014
Make more cut-outs with additional staff. Change the 5 moment balloon to individual moments and description of what the moment is.
Diana Marriott May 2014
New ideas
Make bottles of hand sanitizer more obvious at the entrances to the hospitals. Diana Marriott mid-February 2014
Hold a Champions video conference to seek their input into new ideas and set out their new proactive role.
Julie Robinson Mid February 2014
Introduce league tables on Pacentral for the most staff completing e-moddle, and introducing the most original ideas for Hand Hygiene promotions and the best results.
Julie and Diana mid-February 2014
National Hand hygiene champion Dr Joshua Freeman writes a letter to every doctor in Diana / Joshua F mid-February
69
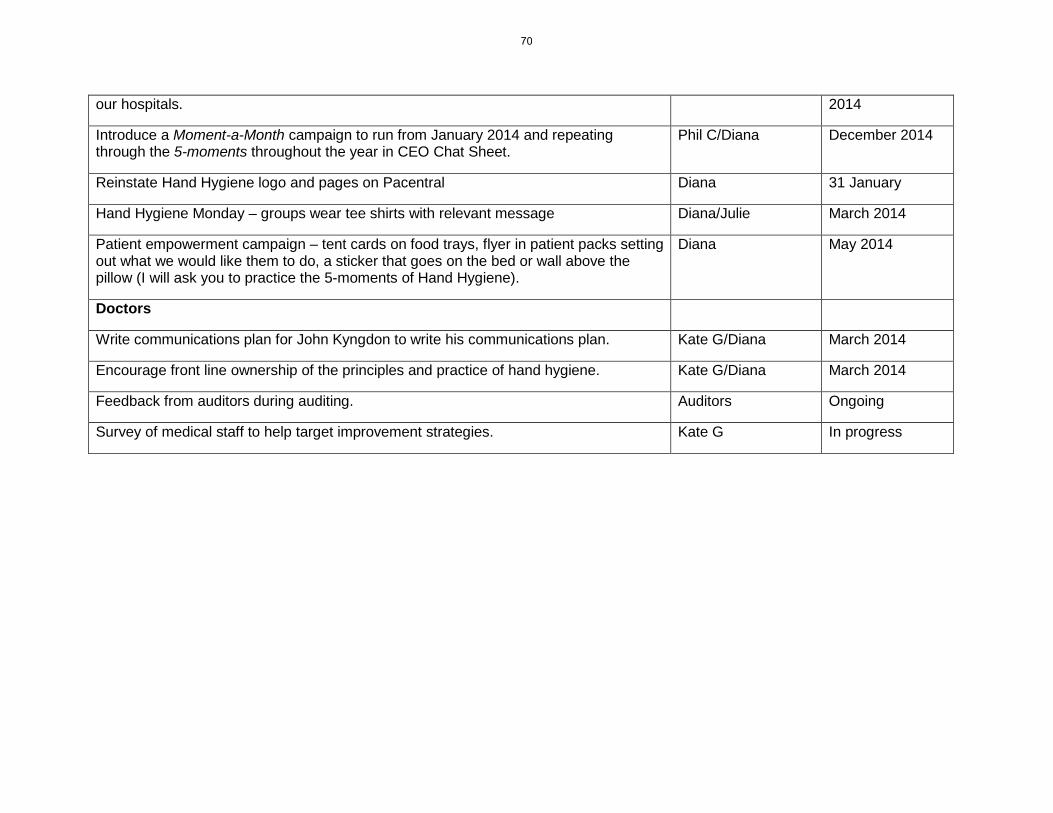
our hospitals. 2014
Introduce a Moment-a-Month campaign to run from January 2014 and repeating through the 5-moments throughout the year in CEO Chat Sheet.
Phil C/Diana December 2014
Reinstate Hand Hygiene logo and pages on Pacentral Diana 31 January
Hand Hygiene Monday – groups wear tee shirts with relevant message Diana/Julie March 2014
Patient empowerment campaign – tent cards on food trays, flyer in patient packs setting out what we would like them to do, a sticker that goes on the bed or wall above the pillow (I will ask you to practice the 5-moments of Hand Hygiene).
Diana May 2014
Doctors
Write communications plan for John Kyngdon to write his communications plan. Kate G/Diana March 2014
Encourage front line ownership of the principles and practice of hand hygiene. Kate G/Diana March 2014
Feedback from auditors during auditing. Auditors Ongoing
Survey of medical staff to help target improvement strategies. Kate G In progress
70

17/02/2014
1
SHARING OUR SUCCESS
NOT GERMS
B E L L A M A R K : G W E N D A R U E G G : J I L L V A N D E R W O U D E N
S U R G I C A L W A R D W H A K A T A N E H O S P I T A L
Fight Against Healthcare Associated Infections
• WHO• WHAT• WHEN• HOW
•HOW•WHEN•WHO•WHY
•HOW•WHEN•WHY•WHO
•WHO•WHEN•WHY
ACT PLAN
DOSTUDY
Clean Hands Save Lives
71

17/02/2014
2
STOP
Fight Against Healthcare Associated Infections
Increase and Sustain Good Hand Hygiene Practices Amongst Everyone
Our Very First Moment 2013
72

17/02/2014
3
Many of the 5 Moments Later 2014
It Only Takes 1 Moment To Practice 5 Moments
Ringa Mā Hunga Ora
Like HHNZ on Facebook!Like us on Facebook and join our informal community of passionate hand hygiene supporters. We share news,
information and interesting items about hand hygiene, while encouraging plenty of comments and discussion. The more people the better
73
17/02/2014
4
Proof Is In The Practice
BOPDHB MAY 2013
Business As Usual
It Only Takes 1 Moment To Practice 5 Moments
74

17/02/2014
5
Many Hands Make Light Work
Business As Usual
75
[Paper Ref]
[BOPHAC] [Falls Reduction in Harm]
[Julie Robinson Director of Nursing] February 2014 Page 1 of 2
http://docman/leadership/board/Meetings/BOPHAC/Open/7.2.1 - BOPHAC Falls Feb 2014 Cover paper.doc
Reducing Harm from Falls
SUBMITTED TO: BOPHAC February 2014 Item No:
Submitted by: Julie Robinson Director of Nursing Endorsed by: Helen Mason COO
For Information X For Discussion For Decision (Please ensure one of these options is marked)
RECOMMENDED RESOLUTION
• The committee notes the presentation and the Reducing Harm from Falls plan. ATTACHMENTS: Presentation
BACKGROUND Prior to the Health Quality & Safety Commission national patient safety campaign Open for better care BOPDHB had recognised the need to reduce serious harm from falls. An April 2010 Health Roundtable reported that the Bay of Plenty District Health Board (BOPDHB) was a high outlier for patient falls compared to similar size hospitals in Australasia.
Inpatient falls are the most reported safety incident and occur in all clinical areas. Internationally there is growing interest in prevention strategies and as part of this, in risk assessment tools. These may be useful if the aim is to flag up common risk factors or causes of falls and prompt interventions that are actually delivered. Tools that claim to predict patients’ risk of falling as ‘high’ or ‘low’ do not work well and often provide false reassurance that ‘something is being done’. Falls prevention should focus on a wider range of actions at the individual patient level and across organisations.
Falls in hospital lead to injury in about 30% of cases, with 1–5% leading to serious injury (Healey et al, 2008). As they occur predominantly in older people with frailty or multiple health problems, even minor injuries may lead to impaired rehabilitation, loss of confidence, fear of falling and a longer stay, and are a major factor in patients moving from living independently, to rest homes (Oliver, 2008b).
76

[Paper Ref]
[BOPHAC] [Falls Reduction in Harm]
[Julie Robinson Director of Nursing] February 2014 Page 2 of 2
http://docman/leadership/board/Meetings/BOPHAC/Open/7.2.1 - BOPHAC Falls Feb 2014 Cover paper.doc
Patients’ families often perceive falls as an indicator of a failure in the duty of care. In reality some falls cannot be prevented and are a feature of underlying medical problems or frailty. Falls are frequently cited in complaints (Oliver et al, 2008a).
HQSC Open for better care campaign has selected process measures which show whether the desired changes in practice have occurred at a local level eg, giving older patients a falls risk assessment and developing a care plan for them.
The markers chosen are processes that should be undertaken nearly all the time, so the threshold is set at 90 percent.
Outcomes to date Outcomes from the BOPDHB falls prevention strategy so far have resulted in an increase in falls reporting and correct detail, greater learning’s from any serious harm falls that occur, a reduction in serious harm falls, slowly but steadily, less recidivist fallers and a change in the nature of falls (less predictable falls and less confused patients falling).
After the first release of the Quality Safety Markers for BOPDHB initiated monthly audits by the Clinical Nurse Managers (CNM) to focus on completion of falls assessments and care plans. This has seen an increase from 43% to 67% in the second QSM release.
Lessons learned from other DHBS and part of the First, Do No Harm campaign are:
• Don’t present it solely as a nursing problem. • Don’t judge quality of care on crude falls rates, or panic if there is an increase in
one area over a month or two – falls data can be easily skewed. • Don’t focus on falls prevention at the expense of autonomy and rehabilitation. • Don’t panic if falls rates are slow to drop over the first few years – there are no
quick fixes for something this complex, and this often represents better reporting.
• Don’t forget real falls prevention interventions are what are important – not checklists and ‘box ticking’.
With the project group having completed their brief, expressions of interest have been called for to implement a Falls Steering group which is one of the recommended strategies from the literature for maintaining a focus on reducing harm from falls. There has been a high level of interest from all disciplines to be involved in this group. The group will have much more of an in depth focus on individual falls events to explore the root cause and implement learnings with direct feedback to the individuals caring for the patient at that time. This group will also help lead the April Falls campaign. Monthly auditing as a key accountability for the CNMs will continue as this has demonstrated improvement to date. What should be kept in mind is the overall goal which is reduction in serious harm from falls.
77

17/02/2014
1
Anamaria Watene, CNM 2a Kaupapa
Maurice Chamberlain, Nurse Leader (Falls clinical lead)
History ……..
Initial actions to reducing harm from fallskey points
2009 – 2010 8 serious harm falls including 2 deaths
2011 over 750 reported falls organisationally
BOPDHB Falls user group implemented
Organisational approach
Multi disciplinary
Whole of system
Patient focused
Benchmarked against Health Round Table
Following the health quality safety commissions National agenda to reduce harm from falls.
78

17/02/2014
2
What we did……
Reducing Harm from Falls ‐ OutcomesRecommendation Progress
Implement Intentional rounding organizationally Completed
Formal regular staff education Completed
Online education package be set up Completed
Patient footwear – non slip socks availability Completed
That Ultra low beds be made more available to the organisation
Implemented in the bed replacement programme
Implement a more formal, accurate, data set to measure incidents
HRT, RTTC, ongoing
Review the REF system so allow a drop down box (mandatory) post fall
In Progress
Review and update policies and protocols , A‐D planner, Care plan
Completed
Implement mobility cards at the bedside Completed
Implement a communication strategy Completed
Implement a sustainable working group to continue Reconvening
OUTCOME Moved from RED (HRT 2010) to ORANGE (HRT 2011) ‐ still plenty to do…
79
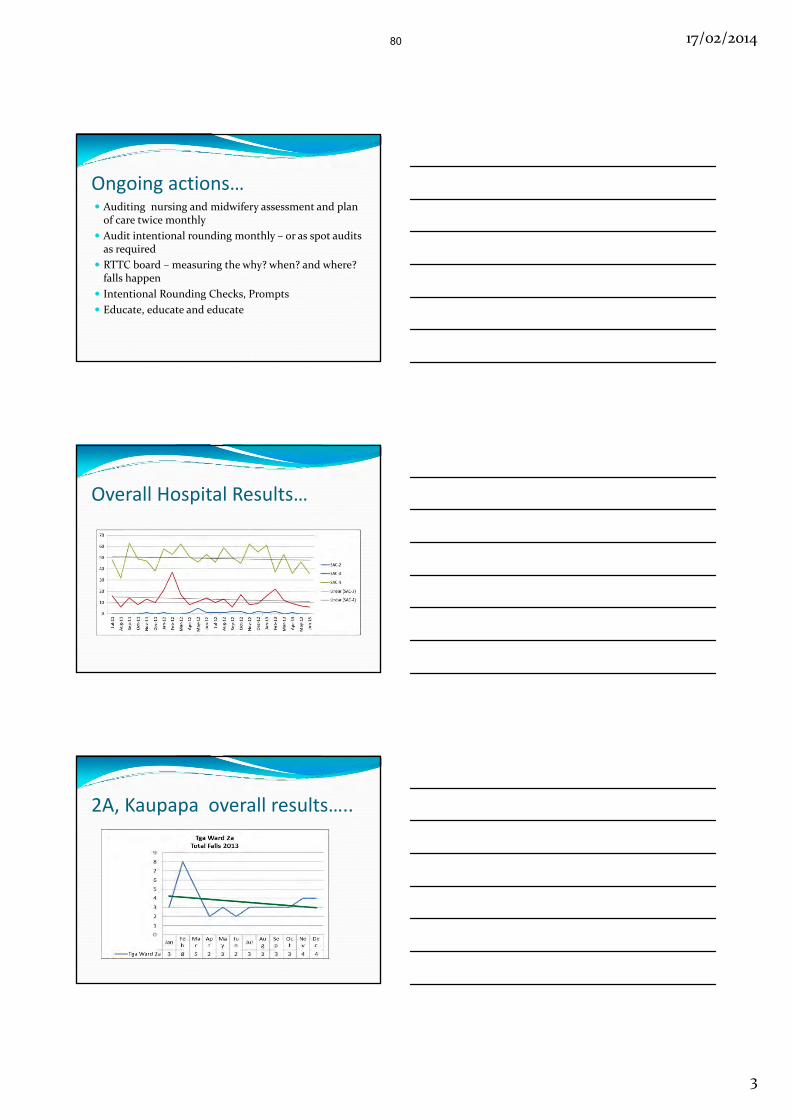
17/02/2014
3
Ongoing actions… Auditing nursing and midwifery assessment and plan of care twice monthly
Audit intentional rounding monthly – or as spot audits as required
RTTC board – measuring the why? when? and where? falls happen
Intentional Rounding Checks, Prompts
Educate, educate and educate
Overall Hospital Results…
2A, Kaupapa overall results…..
80
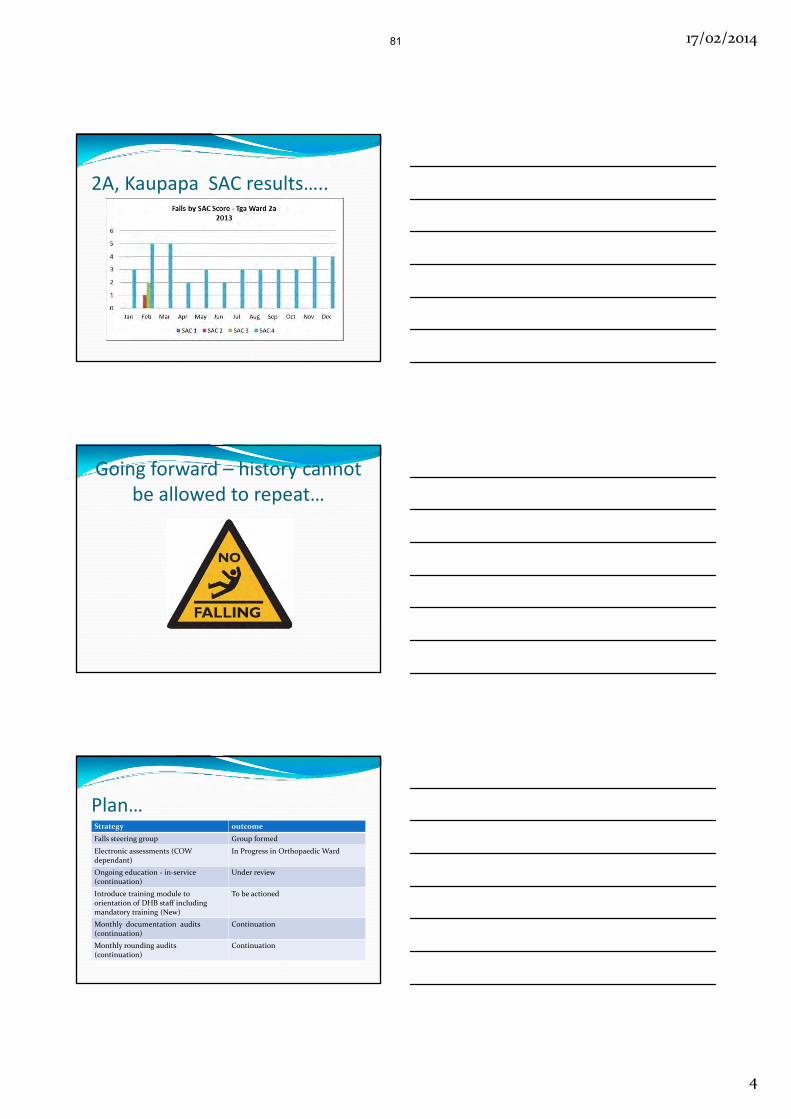
17/02/2014
4
2A, Kaupapa SAC results…..
Going forward – history cannot be allowed to repeat…
Plan…Strategy outcome
Falls steering group Group formed
Electronic assessments (COWdependant)
In Progress in Orthopaedic Ward
Ongoing education ‐ in‐service (continuation)
Under review
Introduce training module to orientation of DHB staff including mandatory training (New)
To be actioned
Monthly documentation audits (continuation)
Continuation
Monthly rounding audits (continuation)
Continuation
81

17/02/2014
5
Factors for Kaupapa success Leadership from CNM –role modelling, rounding, coaching and supporting.
Regular feedback to staff –empowerment and incentives
Staff understood why it was important for patients –we had buy in from the team.
Reinforced the practice of intentional rounding to become a habit for staff with each patient.
Consistency is the key message.
82