Embed Size (px)
Citation preview

Age, Race, Diagnosis, and Sodium Effects on thePressor Response to Infused Norepinephrine
JOEL E. DIMSDALE, ROBERT M. GRAHAM, MICHAEL G. ZIEGLER,
RANDALL M. ZUSMAN, AND CHARLES C. BERRY
SUMMARY We studied the blood pressure responses to infused norepinephrine in 34 normotensiveand 21 unmedicated subjects with essential hypertension. The two groups were similar in age, relativebody weight, and urinary electrolyte excretion. Patients were studied on two extremes of dietary salt(200 mEq Na and 10 mEq Na per day). The dose-response curves were highly linear (p<0.00001) forboth systolic and diastolic blood pressures. There was no evidence for an increased sensitivity toinfused norepinephrine among the hypertensive subjects. On the other hand, older subjects hadsteeper slopes ( p < 0.005). Subjects on a high salt diet had steeper slopes than those on low salt diets(p<0.0025); this trend was especially apparent among blacks (p<0.005). Black and white hyperten-sive subjects responded to the high salt diet in opposite fashion: The blacks showed an increasedpressor sensitivity (p<0.05), whereas the whites demonstrated a nonsignificant decreased pressorsensitivity. These results indicate that age, race, and salt effects must be meticulously controlled instudies of sympathetic nervous system physiology. (Hypertension 10: 564-569, 1987)
KEY WORDS • norepinephrine • sodium • hypertension • race • age • hostility
IN 1948, Goldenberg et al.1 made the intriguingobservation that hypertensive patients seemedunusually sensitive to the blood pressure (BP)-
elevating effects of infused norepinephrine (NE).Since then, many investigators have studied the slopeof this relationship, comparing hypertensive and nor-motensive subjects. Since BP is elevated in many es-sential hypertensive patients because of increased pe-ripheral resistance, many researchers have expectedthat hypertensive patients would demonstrate an in-creased vascular sensitivity (or steeper dose-responseslopes) to infused NE.2 Over the years, however, thishypothesized increased sensitivity has not been repli-cated consistently. Although no one has reported thathypertensive subjects are less sensitive than normoten-sive subjects to infused NE, the findings are mixed,
From the Departments of Psychiatry (J.E. Dimsdale), Medicine(M.G. Ziegler), and Community and Family Medicine (C.C. Ber-ry), University of California, San Diego, La Jolla, California; andthe Department of Medicine (R.M. Graham, R.M. Zusman), Mas-sachusetts General Hospital, Boston, Massachusetts.
Supported by Grants HL36005, HL350I8, and RROO827 fromthe National Institutes of Health.
Address for reprints: Joel E. Dimsdale, M.D., UCSD MedicalCenter, University of California, San Diego Medical Center, 225Dickinson Street, San Diego, CA 92103-9981.
Received January 12, 1987; accepted June 22, 1987.We are grateful to Dr. Stevo Julius for acting as guest editor in the
evaluation of this manuscript.
with some studies reporting increased sensitivityamong hypertensive subjects3"7 and other studies fail-ing to find such increased sensitivity.8"17
In reviewing these studies, we have been struck bytheir frequent reliance on small sample size and theirfailure to control for possibly confounding factors. Insome early studies, virtually all hypertensive subjectswere grouped together, regardless of subtype, for con-trast with normotensive subjects. Other differences inthe studies concern the severity of hypertension: Someinvestigators examined moderately hypertensive sub-jects, whereas others examined mildly hypertensivesubjects. Any of these differences may account for thedivergent findings. Finally, a sound, quantitative basisfor establishing a dose-response curve is absent inmany of the studies. Many studies infused only one ortwo doses of NE, and from these administrations in-ferred a linear relationship, despite the fact that theproposed difference in sensitivity could just as well becurvilinear (e.g., apparent principally at low doses ofinfused NE).
Curiously, many of these studies neglected to exam-ine age effects even though older subjects have de-creased clearance of NE from the circulation.18 Addi-tionally, differences in sodium intake were similarlyignored in many studies, although salt has major ac-tions on sympathetic nervous system activity. For in-stance, salt depletion shortens the prolonged half-life
564
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from

PRESSOR RESPONSE TO INFUSED NOREPlNEPHRINE/Dims^a/e et al. 565
of NE in hypertensive subjects." A number of otherfactors related to BP might confound studies contrast-ing normotensive and hypertensive subjects; for exam-ple, family history, obesity, and race are clearly relat-ed to BP. Two psychosocial factors — depression andhostility — have also been suggested as related togp 20.21 jf a n y of mese many factors were unequallyrepresented across hypertensive and normotensivesubjects, one would have reason to doubt the validityof attributed slope differences across the diagnosticgroups. We have examined this topic anew, trying totake into consideration these various methodologicalcriticisms.
Subjects and MethodsSubjects were recruited from community BP screen-
ing or by word of mouth. We studied 34 healthy menand 21 untreated hypertensive men. All subjects (hy-pertensive and normotensive) were free from anymedication for at least 3 weeks before participation inthe study. Subjects were classified as normotensive ifsystolic BP was below 140 mm Hg and diastolic BPwas below 90 mm Hg. Hypertensive subjects weredefined as having systolic BP above 140 mm Hg ordiastolic BP above 90 mm Hg. BPs were taken with amercury sphygmomanometer after the subject hadbeen seated quietly for at least 5 minutes. Three BPvalues were obtained, and subjects were classified onthe basis of the average of these readings. The subjectsreturned for a repeat BP screening approximately 1week later. Subjects were enrolled in the study only ifthey remained in the same BP group on repeat testing.The mean BPs for the normotensive and hypertensivegroups were 120/73 and 144/95 mm Hg, respectively.
Subjects' ratings on the Beck Depression Inven-tory22 and the Buss-Durkee Hostility Scale23 were ob-tained before the infusions. A family history was con-sidered positive for hypertension if the subjectindicated that a parent had high BP. Relative obesitywas calculated using Metropolitan Life Insurancetables.24
Subjects were admitted twice to the Clinical Re-search Center and randomized to either a high sodiumdiet (200 mEq/day) for 4 days or a low sodium diet (10mEq/day) for 5 days. The opposite diet was used dur-ing the second admission. Both diets were isocaloricand contained potassium, 100 mEq/day. An interval ofapproximately 1 week separated the hospitalizations.Four subjects completed only one hospitalization.Twenty-four-hour urine samples were obtained forelectrolytes.
The NE infusions were performed in the early after-noon of the final day of each hospitalization. All sub-jects had been caffeine-free for at least 16 hours beforethe infusion studies and had been asked to refrain fromcigarette smoking for at least 7 hours before the infu-sion studies.
The subjects were tested in the supine position. AD5W drip (5% dextrose in water) at the rate of 180ml/hr was administered in the subjects' nondominant
arm, and BPs were taken repeatedly during a half-hourperiod while the subject became acclimated to the infu-sion and the repeated BP measurements. At the end ofthe 30-minute interval, three more BPs were taken,and their average was used as the subject's baselineBP. After the baseline period, the NE solutions wereadded to the sustaining infusion. A freshly constitutedsolution of NE in D5W was infused at the rate of 0.01/Ltg/kg/min for 10 minutes. Subsequent doses were0.025, 0.05, and 0.10 pig/kg/min, each given for 10minutes. The infusion was stopped if systolic BP in-creased by 30 mm Hg, diastolic BP increased by 25mm Hg, or if premature ventricular contractions oc-curred. Throughout the infusion, BP was taken by amercury sphygmomanometer every minute after thestart of each infusing dose and continued until the BPplateaued for 3 successive minutes at that given dose.
The data were initially examined with a repeated-measures analysis of variance (ANOVA) and an ortho-gonal polynomials decomposition to determine wheth-er the increase of BP with increased amounts ofinfused NE was linear. The linear term was found to behighly significant (p< 0.00001) for both systolic anddiastolic BPs, while the higher order terms were notsignificant. Moreover, the higher order effects ac-counted for only a small portion of the total variance.Because of our safety precautions for stopping the NEinfusion (see the preceding paragraph), there weresome missing data; as a result, we could not rely on arepeated-measures ANOVA as the fundamental toolfor analysis. Rather, we used a least-squares analysisfor each subject to quantitate the slope of the linerelating infused NE and BP. Unpaired t tests were usedto contrast the hypertensive and normotensive subjectsin terms of the average slope and intercept of suchdose-response curves. We examined other variables toascertain whether they were significantly related to theslope of the dose-response curve. For continuous var-iables (age, relative obesity, depression, hostility), wecalculated Pearson correlation coefficients with slope.For categorical variables (race, family history of hy-pertension), we employed unpaired / tests to contrastthe slopes. Finally, we examined the effect of dietarysalt by employing a paired t test.
ResultsThe hypertensive and normotensive groups did not
differ in age or relative obesity. Analysis of 24-hoururine samples obtained the day before the study re-vealed no significant differences in urinary sodium orpotassium excretion (Table 1).
As a result of hospitalization, the BP in both groupsfell. Diastolic BP of most of the subjects who wereoriginally classified as hypertensive on two separateoccasions decreased below 90 mm Hg after 4 days ofhospitalization and rest, but overall BP in this groupremained 10/10 mm Hg higher than that of the controlgroup. There were no untoward effects of the NEinfusion.
Figure 1 portrays the relationship between infused
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from
566 HYPERTENSION VOL 10, No 6, DECEMBER 1987
TABLE 1. Characteristics of the Sample
Variable
Race (black/white)
Age (yr)
Relative body weight
High Na admission electrolytesUrinary Na (mEq/24 hr)Urinary K (mEq/24 hr)
Low Na admission electrolytesUrinary Na (mEq/24 hr)Urinary K (mEq/24 hr)
Normotensive(" = 34)
19:15
32±6
l. l±0.1
217±5266±17
29 ±2569 ±19
Hypertensive(i = 21)
8M3
35±7
1.1 ±0.2
214±8762 ±20
22 ±1057 ±22
Values, except for race, are means ± SD. There were no signifi-cant differences between groups.
60
50
140
130
120
no
100
90
80
70
60
SYSTOLIC
-
aASTOUC
-
— - — — — Hypertv&vtHormottmn*
0 025 05 075 10
N0REP1NEPHRIC INFUSED (>iQ/kg)
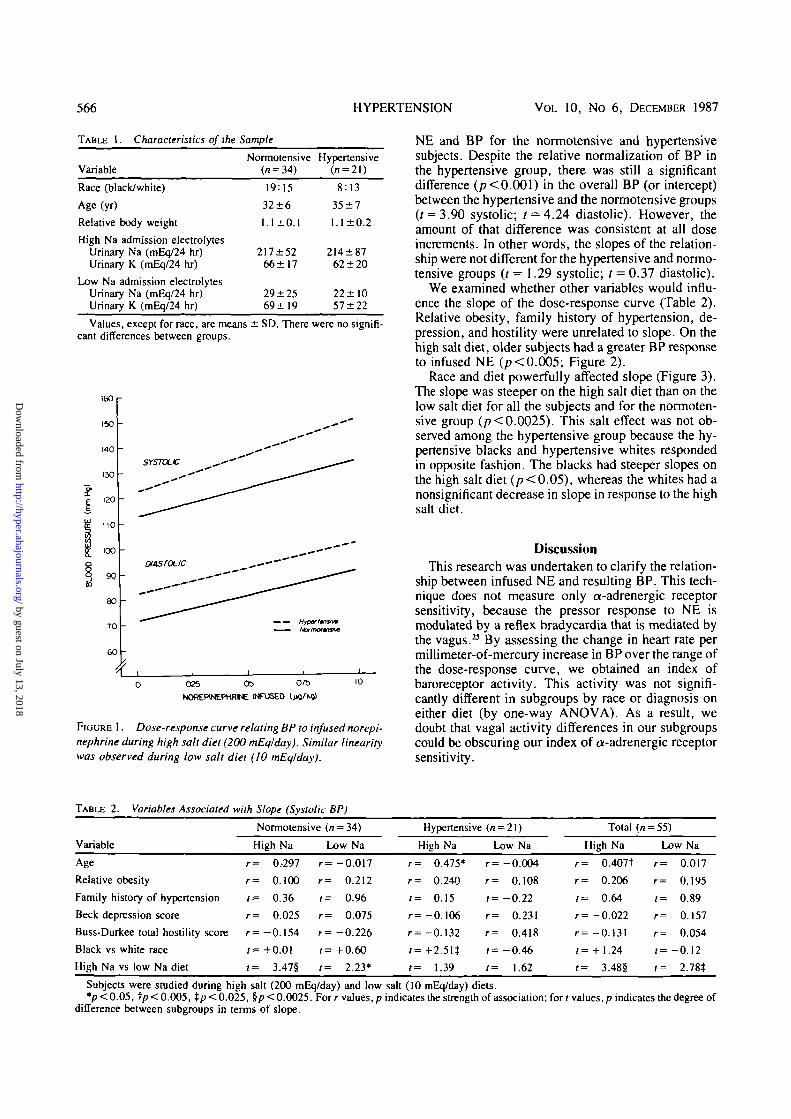
FIGURE 1. Dose-response curve relating BP to infused norepi-nephrine during high salt diet (200 mEqlday). Similar linearitywas observed during low salt diet (10 mEqlday).
NE and BP for the normotensive and hypertensivesubjects. Despite the relative normalization of BP inthe hypertensive group, there was still a significantdifference (/?<0.001) in the overall BP (or intercept)between the hypertensive and the normotensive groups0 = 3.90 systolic; f = 4.24 diastolic). However, theamount of that difference was consistent at all doseincrements. In other words, the slopes of the relation-ship were not different for the hypertensive and normo-tensive groups (t = 1.29 systolic; t = 0.37 diastolic).
We examined whether other variables would influ-ence the slope of the dose-response curve (Table 2).Relative obesity, family history of hypertension, de-pression, and hostility were unrelated to slope. On thehigh salt diet, older subjects had a greater BP responseto infused NE (p< 0.005; Figure 2).
Race and diet powerfully affected slope (Figure 3).The slope was steeper on the high salt diet than on thelow salt diet for all the subjects and for the normoten-sive group (p<0.0025). This salt effect was not ob-served among the hypertensive group because the hy-pertensive blacks and hypertensive whites respondedin opposite fashion. The blacks had steeper slopes onthe high salt diet (p<0.05), whereas the whites had anonsignificant decrease in slope in response to the highsalt diet.
DiscussionThis research was undertaken to clarify the relation-
ship between infused NE and resulting BP. This tech-nique does not measure only a-adrenergic receptorsensitivity, because the pressor response to NE ismodulated by a reflex bradycardia that is mediated bythe vagus.23 By assessing the change in heart rate permillimeter-of-mercury increase in BP over the range ofthe dose-response curve, we obtained an index ofbaroreceptor activity. This activity was not signifi-cantly different in subgroups by race or diagnosis oneither diet (by one-way ANOVA). As a result, wedoubt that vagal activity differences in our subgroupscould be obscuring our index of a-adrenergic receptorsensitivity.
TABLE 2. Variables Associated with Slope (Systolic BP)
Variable
Age
Relative obesity
Family history of hypertension
Beck depression score
Buss-Durkee total hostility score
Black vs white race
High Na vs low Na diet
Normotensive
High Na
r= 0,297
r= 0.100
/= 0.36
r= 0.025
r = - 0 . 1 5 4
/= +0.01
t= 3.47§
r
r
t
r
r
t
t
(« = 34)
Low Na
= -0.017
= 0.212
= 0.96
= 0.075
= -0.226
= +0.60
= 2.23*
Hypertensive
High Na
r= 0.475*
r= 0.240
/= 0.15
r= -0.106
r= -0.132
r= +2.51$
/= 1.39
(" = 21)
Low Na
r= -0.004
r= 0.108
r=-0 .2 2
r = 0.231
r= 0.418
/= -0.46
(= 1.62
Total (r
High Na
r= 0.407t
r= 0.206
t= 0.64
r=-0 .022
r= -0.131
/= + 1.24
t= 3.48§
, = 55)
Low Na
r= 0.017
r= 0.195
/= 0.89
r= 0.157
r= 0.054
»=-0.12
t= 2.78*
Subjects were studied during high salt (200 mEq/day) and low salt (10 mEq/day) diets.*p<0.05, t p < 0.005, tp< 0.025, §p< 0.0025. For r values, p indicates the strength of association; for rvalues,/? indicates the degree of
difference between subgroups in terms of slope.
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from

PRESSOR RESPONSE TO INFUSED NOREPINEPHRINE/D/mst/a/e et al. 567
IOOO
800
600J
400i
200
0
-200 15 20 25 30 35 40 45 50 55
AGE
FIGURE 2. Effect of age on systolic pressor sensitiv-ity during the high salt diet (200 mEqlday).
An additional issue concerns the variable rate ofclearance and half-life of plasma NE across individualsubjects.26-27 A dose-response calculation employingblood levels, as opposed to infused doses, would allowa more accurate estimation of receptor sensitivity andwould eliminate the confusing factor of different ratesof NE clearance in different subjects. We did draw abaseline plasma NE level before beginning the infu-sion and observed no significant overall correlationbetween resting NE and slope for systolic or diastolicBP on either diet. Future studies will examine NElevels at each step of the NE infusion. Predictably, NElevels increased in response to the low salt diet; how-ever, the degree of increase was unrelated to thechange in slope of the dose-response curve (r = 0.005for systolic slope, r = 0.195 for diastolic slope).
Despite these caveats, we believe these data lead to
ALL SUBJECTS NORMOTENSIVE HYPERTENSIVE
500 r
4 0 0
300
x 200p
100
<n 0
5100 -
200 -
3C0
rri
Wh
FIGURE 3. Effect of salt on pressor sensitivity. The slope of the BP dose-response curve to infused norepinephrinewas calculated, and the slope on the low salt diet was subtracted from the slope on high salt diet for each subject.The mean, SE, and individual points are portrayed for different groups according to race and diagnosis. Single(p < 0.05), double (p < 0.025), triple (p < 0.005), and quadruple (p < 0.0025) asterisks denote the significance ofthe salt effect in each group (obtained by paired t tests). All = all subjects; Bl = blacks; Wh = whites.
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from

568 HYPERTENSION VOL. 10, No 6, DECEMBER 1987
an important and clear conclusion. There is a disagree-ment in the literature about the relationship betweeninfused NE and the resulting BP in normotensive andhypertensive subjects. Our data argue against a differ-ence in sensitivity across the two groups. It is possiblethat subjects with moderate to severe hypertensioncould be more sensitive than normotensive subjects,but in comparing values for normotensive subjectswith those for mildly hypertensive subjects, there wasno difference in slope. Our methodology was designedexplicitly to control for factors that might influence thedose-response relationship. When we examined suchfactors, we found that they could have marked effectson slope, thus possibly confounding the relationshipbetween diagnosis and slope.
There is some evidence that older subjects have areduced clearance of NE from the circulation.l8 In ad-dition, there is some evidence that the pressor responseincreases with age6; however, not all groups have ob-served such an effect.28 Even across our modest agespan (19—48 years), we found that older subjects on thehigh salt diet had steeper slopes relating BP to infusedNE. If previous studies did not meticulously controlfor dietary salt and age differences, their comparisonsof hypertensive and normotensive subjects would thusbe of diminished value.
Since weight loss is associated with a decrease inadrenergic activity,29 it is possible that obese hyperten-sive persons have a steeper slope; however, Boeh-ringer et al.30 found no difference in NE sensitivityamong obese patients. In our study as well, relativeobesity was not related to slope. However, our obesityrange was quite circumscribed (91 -151 % of ideal bodyweight).
We could not reconfirm the observation by Bian-chetti et al.31 that a family history of hypertension wasrelated to slope. We relied on unverified self-report offamily history; thus, these data are subject to question.
There is a growing psychiatric literature about pos-sible sympathetic dysregulation in depressed pa-tients.3233 In addition, depression has long beenknown to increase BP.20 Our tool for depression was aself-reported demoralization measure that is related tobut not identical to a formal psychiatric diagnosis ofdepression. We found no association between slopeand the Beck Depression Inventory. If there is a slopeeffect, it may be evident only in clinically depressedpatients. Abnormalities in regulation of hostility havealso been related to hypertension,21 but they were unre-lated to slope in this study. Taken together, these twofindings suggest that no confounding of diagnosis andslope occurred because of these psychosocial factors.
We know of no study that has explicitly comparedblack and white dose-response curves. As race wasrarely discussed in previous studies, no informationwas available about possible differences in the racialcomposition of the hypertensive or control groups. Inour study we found a significant difference across theraces. On the high salt diet, black hypertensive sub-jects had steeper slopes than white hypertensive sub-jects (p < 0.025); there was no racial difference for thenormotensive subjects.
We reconfirmed the observation by Rankin et al.34
of a steeper dose-response curve on high salt diets.Rankin et al.M contrasted sodium diets of 800 and 10mEq/day; as our work demonstrates, the salt sensitiza-tion is apparent even at a dietary sodium intake of 200mEq/day (p<0.0025). In addition, we again found arace effect: In general, blacks were particularly sensi-tive to salt loading (p< 0.005); whereas whites had anonsignificant response to salt loading. However, inthe diagnostic subgroups, the pattern of sensitizationwas exactly opposite: There was salt sensitizationamong the normotensive whites and hypertensiveblacks (see Figure 3). Using diet as a within-subjectmeasure and race and diagnosis as between-subjectsmeasures, we employed a repeated-measures ANOVAto examine the role of salt, race, and diagnosis. Theanalysis revealed a significant three-way interactionamong salt, race, and diagnosis (p<0.02). These ra-cial and salt response differences are new observa-tions. However, they must be tempered by the smallsample size in the subgroups.
A final observation relates to our method of dataanalysis. We used each subject's total data to generatea dose-response curve rather than rely on only one ortwo points. At the doses infused, this relationship washighly linear, suggesting that elaborate data transfor-mations are not necessary.
At first glance, our findings may seem primarilynegative in nature. We are yet another research groupthat has failed to replicate observation of an increasedsensitivity to NE infusions among hypertensive sub-jects. However, the reasons for such confusion arenow clearer. Age, dietary salt intake, and race all im-pinge rather clearly on the sensitivity of the dose-re-sponse curve. Few reported studies controlled for oneof these factors, let alone three. Our findings point tothe importance of meticulous care in controlling forthese factors in studies of sympathetic nervous systemphysiology. These data also suggest a basic differencebetween black and white subjects' pressor sensitivityin the face of increased dietary salt.
References1. Goldenberg M, Pines K, Baldwin E, Greene D, Roh C. The
hemodynamic response of man to norepinephrine and epineph-rine and its relation to the problem of hypertension. Am J Med1948;5:792-8O6
2. Mendlowitz M, Naftchi N, Gitlow S, Wolf R. Vascular re-sponsiveness in hypertensive and hypotensive states. Geriat-rics 1965;20:797-807
3. PhillippT, Distler A, Cordes U, Wolff HP. Plasma noradrena-line and the pressor action of exogenous noradrenaline in nor-motensive subjects and patients with essential hypertension.Clin Sci Mol Med 1978;55:61s-63s
4. Vlachakis N. Blood pressure response to norepinephrine infu-sion in relationship to plasma catecholamines and renin activityin man. J Clin Pharmacol 1979;19:654-661
5. Henquet J, van Baak M, Schols M, Rahn K. Studies on theautonomic nervous system in borderline hypertension. Eur JClin Pharmacol 1982;22:285-288
6. Iimura O, Kikuchi K, Sato S. Plasma noradrenaline concentra-tion and pressor response to infused noradrenaline in patientswith borderline hypertension, and mild or moderate essentialhypertension. Jpn Circ J 1984;48:159-167
7. Bianchetti M, Beretta-Piccoli C, Weidmann P, FerrierC, LinkL, Gerber A. Correction of cardiovascular hypersensitivity to
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from

PRESSOR RESPONSE TO INFUSED NOREPINEPHRINE/DimsAz/e et al. 569
norepinephrine by potassium supplementation in normotensivemembers of hypertensive families and patients with essentialhypertension. J Hypertens 1984;2(suppl 3):445-448
8. Judson W, Epstein F, Wilkins R. The comparative effects ofsmall intravenous doses of /-norepinephrine upon arterial pres-sure and pulse rate in normotensive subjects and in hyperten-sive patients before and after thoracolumbar sympathectomy.J Clin Invest 1950;29:1414-1420
9. Gombus E, Hulet W, Bopp P, Goldring W, Baldwin D, ChasisH. Reactivity of renal and systemic circulations to vasocon-strictor agents in normotensive and hypertensive subjects.J Clin Invest 1962;41:203-217
10. Distler A, Barth C, Liebau H, Vecsei P, Wolff H. The effect oftyramine, noradrenaline, and angiotensin on the blood pressurein hypertensive patients with aldosteronism and low plasmarenin. Eur J Clin Invest 1970; 1:196-203
11. Manger W, Frohlich E, Gifford R, Dustan H. Norepinephrineinfusion in normal subjects and patients with essential or renalhypertension: effect on blood pressure, heart rate, and plasmacatecholamine concentrations. J Clin Pharmacol 1976;16:129-141
12. Beretta-Piccoli C, Weidmann P, Meier A, Grimm M, KeuschG, Gluck Z. Effects of short-term norepinephrine infusion onplasma catecholamines, renin, and aldosterone in normal andhypertensive man. Hypertension 1980;2:623-630
13. Grimm M, Weidmann P, Meier A, et al. Correction of alterednoradrenaline reactivity in essential hypertension by indapa-mide. Br Heart J 1981;46:404-409
14. Weidmann P, Beretta-Piccoli C, Meier A, Keusch G, Gluck Z,Ziegler W. Antihypertensive mechanism of diuretic treatmentwith chlorthalidone: complementary roles of sympathetic axisand sodium. Kidney Int 1983;23:320-326
15. Weidmann P, Beretta-Piccoli C, Link L, Bianchetti MG,Boehringer K, Morton JJ. Cardiovascular counterregulationduring sympathetic inhibition in normal subjects and patientswith mild hypertension. Hypertension 1983;5:873-88O
16. Gerber A, Weidmann P, Marone C, Uehlinger D, Riesen W.Cardiovascular and metabolic profile during intervention withurapidil in humans. Hypertension 1985;7:963-971
17. Bovy P, Juchmes J, Cession A. Metabolic clearance of norepi-nephrine in normotensive and borderline hypertensive sub-jects. Clin Exp Hypertens [A] 1984;6(3):709-715
18. EslerM, Skews H, Leonard P, Jackman G, Bobik A, Korner P.Age-dependence of noradrenaline kinetics in normal subjects.ClinSci 1981;60:217-219
19. Kimura S, Miura Y, Adachi M, et al. The effect of sodiumdepletion on plasma norepinephrine kinetics in patients withessential hypertension. Jpn Circ J 1983;47:1232-1241
20. Dimsdale J. The effect of depression on cardiovascular reactiv-
ity. In: Fields T, McCabe P, Schneiderman N, eds. Stress andcoping across development. Hillsdale, NJ: Lawrence ErlbaumAssociates, 1987:215-225
21. Dimsdale J, Pierce C, Schoenfeld D, Brown A, Zusman R,Graham R. Suppressed anger and blood pressure: the effects ofrace, sex, social class, obesity, and age. Psychosom Med1986;48:430-436
22. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. Aninventory for measuring depression. Arch Gen Psychiatry1961;4:561-571
23. Buss A, Durkee A. An inventory for assessing different kindsof hostility. J Consult Psychol 1957;21:343-349
24. Metropolitan Life Foundation. 1983 Metropolitan height andweight tables. Stat Bull Metrop Insur Co 1983;64:1
25. Pickering T, Sleight P. Quantitative index of baroreflex activ-ity in normal and hypertensive subjects using Valsalva's ma-noeuvre. Br Heart J 1969;31:392
26. Goldstein D, Horwitz D, Keiser H, Polinsky R. Plasma /-3Hnorepinephrine, d-]4C norepinephrine, and d,l-3H isoproter-enol kinetics in essential hypertension. J Clin Invest 1983;72:1748-1758
27. Esler M, Leonard P, Kelleher D, et al. Assessment of neuronaluptake of noradrenaline in humans: defective uptake in somepatients with essential hypertension. Clin Exp PharmacolPhysiol 1980;7:535-539
28. Meier A, Gubelin P, Weidmann P. Age-related profile of car-diovascular reactivity to norepinephrine and angiotensin innormal and hypertensive men. Klin Wochenschr 1980;58:1183-1188
29. Messerli F. Cardiovascular effects of obesity and hyperten-sion. Lancet 1982;1:1165—1168
30. Boehringer K, Beretta-Piccoli C, Weidmann P, Meier A,Ziegler W. Pressor factors and cardiovascular pressor respon-siveness in lean and overweight normal or hypertensive sub-jects. Hypertension 1982;4:697-702
31. Bianchetti M, Weidmann P, Beretta-Piccoli C, et al. Disturbednoradrenergic blood pressure control in normotensive mem-bers of hypertensive families. Br Heart J 1984;51:306-311
32. Siever L, Davis K. Overview: toward a dysregulation hypothe-sis of depression. Am J Psychiatry 1985;142:1017-1031
33. Esler M, Turbott J, Schwarz R, et al. Differing noradrenalinekinetics in essential hypertension and depressive illness, twodiseases in which the plasma concentration of noradrenaline issometimes elevated. Clin Exp Pharmacol Physiol 1981;8:525-530
34. Rankin LI, Luft FC, Henry DP, Gibbs PS, Weinberger MH.Sodium intake alters the effects of norepinephrine on bloodpressure. Hypertension 1981;3:650-656
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from

J E Dimsdale, R M Graham, M G Ziegler, R M Zusman and C C BerryAge, race, diagnosis, and sodium effects on the pressor response to infused norepinephrine.
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 1987 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/01.HYP.10.6.564
1987;10:564-569Hypertension.
http://hyper.ahajournals.org/content/10/6/564World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOffice. Once the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertension Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 13, 2018http://hyper.ahajournals.org/
Dow
nloaded from





























