Embed Size (px)
Citation preview

ARTICLE OPEN ACCESS
Age-dependent association of white matterabnormality with cognition after TIA or minorstrokeGiovanna Zamboni MD DPhil Ludovica Griffanti PhD Sara Mazzucco MD PhD
Sarah T Pendlebury MD DPhil FRCP and Peter M Rothwell MD PhD FMedSci
Neurologyreg 2019931-11 doi101212WNL0000000000007772
Correspondence
Dr Zamboni
Giovannazamboni
unimoreit
AbstractObjectiveTo investigate if the association between MRI-detectable white matter hyperintensity (WMH)and cognitive status reported in previous studies persists at older ages (gt80 years) when somewhite matter abnormality is almost universally reported in clinical practice
MethodsConsecutive eligible patients from a population-based cohort of all TIAnondisabling stroke(Oxford Vascular Study) underwent multimodal MRI including fluid-attenuated inversionrecovery and diffusion-weighted imaging allowing automated measurement of WMH volumemean diffusivity (MD) and fractional anisotropy (FA) in normal-appearing white matter usingFSL tools These measures were related to cognitive status (Montreal Cognitive Assessment) atage le80 vs gt80 years
ResultsOf 566 patients (mean [range] age 667 [20ndash102] years) 107 were aged gt80 years WMHvolumes and MDFA were strongly associated with cognitive status in patients aged le80 years(all p lt 0001 for WMH MD and FA) but not in patients aged gt80 years (not significant forWMH MD and FA) with age interactions for WMH volume (pinteraction = 0016) and MD(pinteraction = 0037) Voxel-wise analyses also showed that lower Montreal Cognitive Assess-ment scores were associated with frontal WMH in patients le80 years but not gt80 years
ConclusionMRI markers of white matter damage are strongly related to cognition in patients with TIAminor stroke at younger ages but not at age gt80 years Clinicians and patients should notoverinterpret the significance of these abnormalities at older ages
From the Centre for Prevention of Stroke and Dementia (GZ LG SM STP PMR) and Wellcome Centre for Integrative Neuroimaging FMRIB (GZ LG) Nuffield Department ofClinical Neurosciences John Radcliffe Hospital University of Oxford and Department of Biomedical Metabolic and Neural Sciences and Centre for Neurosciences and Neuro-technology (GZ) University of Modena and Reggio Emilia Italy
Go to NeurologyorgN for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article The Article ProcessingCharge was funded by the Wellcome Trust
This is an open access article distributed under the terms of the Creative Commons Attribution License 40 (CC BY) which permits unrestricted use distribution and reproduction in anymedium provided the original work is properly cited
Copyright copy 2019 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 1
Published Ahead of Print on June 14 2019 as 101212WNL0000000000007772
White matter hyperintensity (WMH) of presumed vascularorigin detectable on MRI is associated with cognitive impair-ment and dementia12 Associations between cognitive scoresand measures of WMH load have been shown in elderlyindividuals without dementia3ndash6 patients with manifested ar-terial disease7 and patients with TIA or minor stroke8 Meas-ures of white matter microstructural integrity estimated usingdiffusion tensor imaging (DTI) such as fractional anisotropy(FA) and mean diffusivity (MD) are also associated withcognitive deficits in elderly individuals without dementia9 in-cluding those with small vessel disease1011 Importantly it hasbeen shown that these DTI measures are abnormal not only inWMH regions but also in the surrounding normal-appearingwhite matter (NAWM) and that the level of DTI-detecteddeterioration of NAWM is associated with age and WMHburden in cognitively healthy adults1213 including those olderthan 9014 as well as poststroke patients1516 These findingssuggest that DTI modifications precede the occurrence ofWMH and better capture the true extent of pathophysiologicchanges underlying global white matter1718
The prevalence ofWMH increases with age particularly after age801920 and DTI estimates of white matter integrity also sharplydeteriorate with age21 However there are few data on the age-specific association between MRI-detectable white matterdamage and cognition with most studies reporting associationspooled across a broad range of ages (eg ge507 gt603 or gt6522)Yet some studies suggest that the association may attenuate atage gt802324 although to our knowledge no studies have directlycompared the association in older vs younger adults
Establishing the relevance of WMH to cognition in very oldpatients is increasingly important because individuals over 80years of age represent the most rapidly growing segment of thepopulation25 with the greatest concern about risk ofdementia26ndash28 Furthermore MRI is now very frequently per-formed as first-line brain imaging for a wide range of neurologicsymptoms such that someWMHare almost always reported inolder patients1929 The most common indication for suchimaging in routine practice is after TIA and stroke and patientsfrequently have evidence of small vessel disease inevitablyraising concern about vascular cognitive impairment30ndash32 Wetherefore studied MRI markers of white matter damage andcognitive status in a population-based cohort of patients withTIA or minor stroke comparing those aged le80 vs gt80 years
We also explored with voxel-wise analyses whatWMH locationis more strongly associated with cognitive impairment andwhether there would be differences between age groups
MethodsStudy populationConsecutive patients were recruited betweenMarch 2012 andJune 2016 from the Oxford Vascular Study (OXVASC)a prospective cohort study of all acute vascular events ina defined population of 92000 residents registered with 100primary care physicians in Oxfordshire and the onlypopulation-based study of all vascular disease that does notexclude very old patients After a suspected nondisabling ce-rebrovascular event (NIH Stroke Scale score lt4) OXVASCparticipants undergo brain MRI detailed clinical character-ization and cognitive assessment with face-to-face follow-upat 1 3 6 12 24 and 60 months In order to avoid anyselection bias particularly against older patients patients witha previous TIA or minor stroke prior to the imaging studyperiod were included Exclusion criteria specific for thepurposes of the present imaging study were (1) MRI con-traindication or known claustrophobia (2) intracranial space-occupying lesion (3) intracranial hemorrhage (4) braindefect due to previous neurosurgery or developmentalanomalies (4) large chronic subacute or acute infarcts(ie gt25 cm on T1-weighted T2-weighted or diffusion-weighted imaging sequences) (5) significant movementartefacts that would impair registration (6) inability to per-form cognitive testing (ie due to language barriers)
Standard protocol approvals registrationsand patient consentsWritten informed consent was obtained from all participantsOXVASC was approved by the local ethics committee (Re-search Ethics Committee reference number 05Q160470)
Data availabilityRequests for data from the OXVASC Study will be consideredby PMR in line with data protection laws The general policyis that as long as the proposed use of the data is scientificallyvalid and as long as ethics approval permits suitably anony-mized data can be shared with other researchers
GlossaryANOVA = analysis of variance BET = brain extraction tool BIANCA = brain intensity abnormality classification algorithmCI = confidence interval DTI = diffusion tensor imaging FA = fractional anisotropy FLAIR = fluid-attenuated inversionrecovery FNIRT = FMRIBrsquos nonlinear image registration tool FOV = field of view GRAPPA = generalized autocalibratingpartial parallel acquisition MD = mean diffusivity MildCI = mild cognitive impairment MNI = Montreal NeurologicalInstitute MoCA = Montreal Cognitive Assessment NAWM = normal-appearing white matter NoCI = no cognitiveimpairment OR = odds ratio OXVASC = Oxford Vascular Study SevereCI = severe cognitive impairment TE = echo timeTI = inversion time TR = repetition time WMH = white matter hyperintensity
2 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
Cognitive statusParticipants were divided into 3 groups according to theirMontreal Cognitive Assessment (MoCA) scores which hasbeen shown to be sensitive to detect vascular cognitiveimpairment33ndash35 no cognitive impairment (NoCI MoCAge26) mild cognitive impairment (MildCI 20 lt MoCA lt 26)or severe cognitive impairment (SevereCI MoCA le20)These cutoffs were chosen on the basis of previous workshowing that the MoCA has high sensitivity in identifyingpoststroke patients with mild but also severemultidomaincognitive impairment3436 For the purpose of the presentstudy we used MoCA scores from the 1-month follow-up asthese better reflect the cognitive status independent fromtransient cognitive variations related to the minor cerebro-vascular event37
Imaging acquisitionAll images were acquired on a 3T Verio (Orem UT) MRIscanner The imaging protocol used until December 2014included fluid-attenuated inversion recovery (FLAIR) (repe-tition time [TR]echo time [TE]inversion time [TI] 90009402500 ms flip angle 150deg field of view [FOV] 200 mmvoxel size 08 times 08 times 5 mm with 15 mm interslice gap) post-gadolinium T1-weighted imaging (TRTETI 1250463900 ms flip angle 16deg FOV 220 mm voxel size 11 times 11 times3 mm with 15 mm interslice gap) and diffusion-weightedimaging (TRTE 4000106 ms generalized autocalibratingpartial parallel acquisition [GRAPPA] factor 2 FOV 230 mmvoxel size 18 times 18 times 4 mm with 12 mm interslice gap 12directions b value 1000 smm2)
The protocol used from January 2015 included high-resolution T1 (TRTETI 2000194880 ms flip angle 8degFOV 256 mm voxel size 1 times 1 times 1 mm) FLAIR (TRTETI9000882500ms flip angle 150deg FOV 192mm voxel size 1times 1 times 3 mm) and diffusion-weighted imaging (TRTE =800086 ms GRAPPA factor 2 flip angle 16deg FOV 192 mmvoxel size 2 times 2 times 2 mm 32 directions b value 1500 smm2)
Measures of white matter damage (WMH volumes MD andFA in NAWM) obtained from the second protocol werestandardized on values obtained from the first protocol toallow statistical analyses across the whole sample In additionprotocol type was added as covariate of no interest on uni-variate and voxel-wise analyses
Presenceabsence of lacunar infarcts was rated by strokeneurologists and neuroradiologists who were blind to thecognitive scores Lacunar infarcts were defined as hypointenselesions on T1 imaging with corresponding hyperintense le-sion on FLAIR images with a diameter lt15 mm
WMH measurementWMHs were automatically segmented on FLAIR images withbrain intensity abnormality classification algorithm(BIANCA) a fully automated supervised method for WMHdetection which gives the probability per voxel of being
WMH38 The total WMH volume was calculated from thevoxels exceeding a probability of 09 (which gave the highestaccuracy on this dataset as tested in our previous work38) ofbeing WMH and located within a white matter maskObtained values were adjusted for the total brain and ven-tricles volume (ie the sum of the volumes of gray matterwhite matter and ventricles) calculated from the brain-extracted images using FSLrsquos brain extraction tool (BET)39
and log transformed40 as a proxy for intracranial volume thatcould be obtained from the available FLAIR images
For voxel-wise analyses the thresholded and masked WMHmaps were binarized and transformed into Montreal Neuro-logical Institute (MNI) standard space applying the nonlinearregistration (FMRIBrsquos nonlinear image registration tool[FNIRT])41 calculated from FLAIR to MNI (via high-resolution T1 if available) We further thresholded thetransformed maps at 05 binarized them and applied spatialsmoothing of full width at half maximum = 6 mm to com-pensate for registration errors (the size of the smoothingkernel was empirically decided to be the same as the maxi-mum voxel dimension) The resulting maps were entered intovoxel-wise WMH statistical analyses
WMH were also visually rated on the Fazekas WMH scaleallowing categorical measurement of periventricular and deepWMH in grades from 0 (absent) to 3 (severe)42
Measurements of microstructural whitematter integrity in NAWMDiffusion-weighted images were first corrected for head mo-tion and eddy currents DTI was then performed to createMD and FA maps by fitting a tensor model to the diffusion-weighted images using FMRIBrsquos Diffusion Toolbox43 Imageswere brain-extracted using FSLrsquos BET All participantsrsquo FAmaps were then nonlinearly registered to a common diffusionspace (FMRIB58_FA an FA template in MNI space) usingFNIRT and the same transformation was applied to MD dataFor each participant we calculated the linear transformationfrom FLAIR to diffusion data (b = 0 image used as reference)and combined it with the nonlinear transformation fromdiffusion data to the common space calculated before Theresulting transformation was then applied to WMH maps toregister them from FLAIR to diffusion common space MDand FA values from the NAWM were calculated as averagefrom voxels outside the WMH map within a mask includingall the main white matter tracts in the JHU-ICBM DTI atlas(figure 1) The evaluation of DTI-derived measures was re-stricted to the main white matter tracts and not performed inthe whole NAWM in order to focus on the tracts that aremore consistent across participants This also allows com-pensating for possible registration errors occurring in the restof the white matter In addition to exclude the possibility ofa bias in the results due to a systematic difference in regis-tration quality across age groups we calculated a cost metric(root mean square difference) between each participantrsquos FAimage registered to the template and the template itself and
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 3
verified that it was not significantly different between agegroups (estimated root mean square difference = 00420 plusmn00039 lt80 years only = 00418 plusmn 00039 gt80 years only =00426 plusmn 00041)
Statistical analysesPatients were grouped by age le80 vs gt80 years and cognitivestatus (NoCI MildCI SevereCI respectively) as definedabove Comparisons between age groups were performedwith Mann-Whitney or independent t test as appropriate forcontinuous variables and χ2 tests for dichotomous variablesusing SPSS version 220 (SPSS Inc Chicago IL) Age-relateddifferences in the associations between MRI markers of whitematter damage and cognitive status were studied with 2 times 3factorial analyses of variance (ANOVAs) Results were con-sidered significant at p lt 005
Sensitivity analyses were conducted to control for the effectsof potential confounders These analyses included MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risks factors (ie the sum of hyper-tension diabetes mellitus atrial fibrillation hyperlipidemiaand smoking) Furthermore to account for differences insample size between age groups the ANOVA was repeatedusing 4 random subsamples of young participants stratified oncognitive status to match the original large sample
Voxel-wise analysis of WMHWe performed the same 2 times 3 factorial ANOVA at the voxellevel on the maps of WMH obtained with BIANCA to studythe location in the brain of age-by-cognitive status interactionsWe then performed correlational voxel-wise analysis on the
samemaps to test the association between higher probability ofhavingWMH and lower MoCA score in patients aged le80 andin patients aged gt80 separately for the 2 groups
All the statistical analyses were performed with nonparametricpermutation tests using the randomise tool in FSL44 withprotocol as nuisance covariate and restricted to a whitematter mask Results were considered significant at p lt 005fully corrected for multiple comparisons using family-wiseerror correction at the voxel level44
ResultsAmong 570 consecutive eligible patients 4 were excluded dueto subsequently diagnosed WMHmimics (multiple sclerosis)and known other causes of dementia (cerebral autosomaldominant arteriopathy with subcortical infarcts and leu-koencephalopathy and Alzheimer disease) Table 1 reportsthe characteristics of the 566 patients included in the WMHanalyses also divided by age groups (ie le80 and gt80)Diffusion-weighted MRI allowing measurement of FA andMD were acquired from a subsample of 498 consecutiveparticipants (88) as this sequence was not initially includedin the protocol Sensitivity analyses on WMH volumes(available on 566 participants) were repeated in the sub-sample of 498 participants and gave similar results
Age-related associations between WMHvolume and cognitive statusA 2 times 3 factorial ANOVA on WMH volumes showed a maineffect of age (F = 3495 p lt 0001) a main effect of cognition
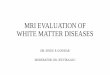
Figure 1 Diffusion tensor imaging (DTI) measurements in normal-appearing white matter (NAWM)
Examples of (A) fractional anisotropy (FA) and (B)mean diffusivity (MD) maps registered in Mon-treal Neurological Institute space from a singleparticipant Average FA and MD value within(NAWM) was calculated from the regions shownin yellow that is within a mask including all themain white matter tracts from the JHU-ICBM DTIatlas and excluding regions of white matterhyperintensity (WMH) obtained with brain in-tensity abnormality classification algorithm (red)
4 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(F = 661 p = 0001) and a significant interaction between ageand cognition (F = 416 pinteraction = 0016) The interactionsuggested that associations between WMH and cognitivestatus are different between the age groups (age le80 vs gt 80years figure 2) Follow-up one-way ANOVAs confirmed thatthere were WMH volume differences across cognitive groupsonly in patients aged le80 and not in patients aged gt80(table 2) even when correcting for within-group age (F =617 p = 0002 for age le80 F = 106 p = 0351 for age gt80)Sensitivity analyses showed that the interaction remainedsignificant (pinteraction = 0046) when adjusting for MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risk factors It also remained signifi-cant when repeated using groups of equal sample sizesobtained by randomly splitting the group of young partic-ipants in 4 subsets matched on cognition to the original one(table 3)
The association between highWMH load (above vs below the80th percentile) and dementia (SevereCI vs NoCI) wasstrong at age le80 (odds ratio [OR] 40 95 confidence in-terval [CI] 165ndash971 p = 0001) but absent at age gt80 (OR089 95 CI 026ndash303 p = 086) These associations were
unchanged when the analysis was repeated with the 80thpercentile cutoff determined separately in the 2 age groups(age le80 OR 39 95 CI 168ndash917 p = 0001 age gt80 OR16 95 CI 041ndash647 p = 0488)
A 2 times 3 factorial ANOVA with years of education as de-pendent variable showed no significant interaction betweenage and cognitive groups (p = 0693) nor did anotherANOVA with brain and ventricles volume as dependentvariable (p = 0159)
Age-relatedassociationsbetweenMDandFA inNAWM and cognitive statusA 2 times 3 factorial ANOVA on average MD values extractedfrom NAWM showed a main effect of age (F = 7358 p lt0001) a main effect of cognitive status (F = 1484 p lt 0001)and a significant interaction between age and cognitive status(F = 332 pinteraction = 0037) Sensitivity analyses showed thatthe interaction on MD from NAWM remained significantwhen adjusting for MRI protocol sex years of educationhead size presence of lacunes and number of vascular risksfactors (pinteraction = 0048) A similar 2 times 3 factorial ANOVAon average FA values extracted from NAWM showed a main
Table 1 Clinical and imaging features of total sample and age groups
Study Total Age le80 y Age gt80 y p Value
N 566 459 107
Age y mean plusmn SD 667 plusmn 143 625 plusmn 125 847 plusmn 37
Age range y 20ndash102 20ndash80 81ndash102
Age y median (IQR) 69 (205) 65 (179) 838 (49)
Female sex n () 280 (495) 228 (497) 52 (486) 0841
TIA other minor stroke n () 408 (721) 336 (734) 72 (679) 0259
Years of education mean plusmn SD 130 plusmn 35 133 plusmn 34 120 plusmn 37 0002
Hypertension n () 260 (459) 190 (415) 70 (654) lt0001
Diabetes n () 55 (97) 41 (90) 14 (131) 0168
Atrial fibrillation n () 60 (106) 40 (87) 20 (187) 0002
Hyperlipidemia n () 163 (288) 130 (284) 33 (308) 0538
Smoking n () 159 (281) 138 (301) 21 (196) 0040
Total Fazekas ge3 n () 174 (307) 117 (255) 57 (532) lt0001
Presence of lacunar infarcts n () 77 (136) 48 (105) 29 (274) lt0001
Brain volumea cm3 mean plusmn SD 10470 plusmn 1340 10738 plusmn 1298 9669 plusmn 1152 lt0001
WMH volume cm3 mean plusmn SD 117 plusmn 109 100 plusmn 89 191 plusmn 147 lt0001
Average FA (NAWM) mean plusmn SD 049 plusmn 003 050 plusmn 003 046 plusmn 003 lt0001
Average MD (NAWM) (times1023) mean plusmn SD 090 plusmn 009 088 plusmn 007 099 plusmn 008 lt0001
Abbreviations FA = fractional anisotropy IQR = interquartile range MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesTotal Fazekas calculated as sum of deep and periventricular scoresa Defined as the sum of gray and white matter volumes (ie not including the ventricles)
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 5
effect of age (F = 4174 p lt 0001) and a main effect ofcognitive status (F = 1367 p lt 0001) but no interaction (F =152 pinteraction = 0219)
One-way ANOVAs on average MD and FA values extractedfrom NAWM confirmed that there were differences acrosscognitive groups only in patients aged le80 but not inpatients aged gt80 (table 2) Adding age or WMH volume ascovariates (analyses of covariance) did not change theresults (table 4)
Localization of WMH relevant tocognitive statusThe voxel-wise 2 times 3 factorial ANOVA showed an interactionbetween cognitive status and age group in an area of the leftdeep frontal white matter (figure 3 bluendashlight blue) Thevoxel-wise correlational analysis performed in patients agedle80 showed that in this group the association between theprobability of having WMH and lower MoCA score was lo-calized in periventricular frontal and parietal white matterareas bilaterally more extended on the left hemisphere
Table 2 Clinical and imaging features of cognitive groups by age
No CI Mild CI Severe CI p Value
Age le80 y
NWMH (NDTI) 338 (295) 97 (83) 24 (20)
Age y mean plusmn SD 618 plusmn 25 620 plusmn 126 702 plusmn 87 0005
Female n () 165 (488) 45 (464) 18 (750) 0036
Event type TIA other minor stroke n () 254 (754) 71 (732) 11 (458) 0007
Hypertension n () 131 (389) 44 (454) 15 (625) 0161
Diabetes n () 26 (77) 7 (72) 8 (333) 0001
Atrial fibrillation n () 26 (77) 12 (124) 2 (83) 0561
Hyperlipidemia n () 93 (276) 28 (289) 9 (375) 0871
Smoking n () 107 (318) 24 (247) 7 (292) 0547
Presence of lacunar infarcts n () 33 (98) 12 (126) 3 (125) 0691
WMH volume cm3 mean plusmn SD 94 plusmn 79 101 plusmn 78 181 plusmn 184 lt0001a
Average FA (NAWM) mean plusmn SD 050 plusmn 003 049 plusmn 003 047 plusmn 003 lt0001a
Average MD (NAWM) (times1023) mean plusmn SD 086 plusmn 006 096 plusmn 007 096 plusmn 007 lt0001a
Age gt80 y
NWMH (NDTI) 44 (42) 46 (42) 17 (16)
Age y mean plusmn SD 839 plusmn 33 859 plusmn 42 834 plusmn 25 0009
Female sex n () 22 (500) 22 (478) 8 (471) 0970
Event type TIA other minor stroke n () 31 (721) 30 (652) 11 (647) 0749
Hypertension n () 26 (591) 32 (696) 12 (706) 0730
Diabetes n () 3 (68) 8 (174) 3 (176) 0575
Atrial fibrillation n () 6 (136) 12 (261) 2 (118) 0512
Hyperlipidemia n () 13 (295) 17 (370) 3 (176) 0637
Smoking n () 9 (205) 9 (196) 3 (176) 0901
Presence of lacunar infarcts n () 12 (279) 15 (326) 2 (118) 0256
WMH volume cm3 mean plusmn SD 159 plusmn 107 213 plusmn 146 214 plusmn 219 0166a
Average FA (NAWM) mean plusmn SD 047 plusmn 003 045 plusmn 003 045 plusmn 004 0110a
Average MD (NAWM) (times1023) mean plusmn SD 096 plusmn 007 101 plusmn 009 101 plusmn 010 0067a
Abbreviations CI = cognitive impairment FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesa Comparisons between cognitive groups that were significant for patients le80 but not for patients gt80
6 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

White matter hyperintensity (WMH) of presumed vascularorigin detectable on MRI is associated with cognitive impair-ment and dementia12 Associations between cognitive scoresand measures of WMH load have been shown in elderlyindividuals without dementia3ndash6 patients with manifested ar-terial disease7 and patients with TIA or minor stroke8 Meas-ures of white matter microstructural integrity estimated usingdiffusion tensor imaging (DTI) such as fractional anisotropy(FA) and mean diffusivity (MD) are also associated withcognitive deficits in elderly individuals without dementia9 in-cluding those with small vessel disease1011 Importantly it hasbeen shown that these DTI measures are abnormal not only inWMH regions but also in the surrounding normal-appearingwhite matter (NAWM) and that the level of DTI-detecteddeterioration of NAWM is associated with age and WMHburden in cognitively healthy adults1213 including those olderthan 9014 as well as poststroke patients1516 These findingssuggest that DTI modifications precede the occurrence ofWMH and better capture the true extent of pathophysiologicchanges underlying global white matter1718
The prevalence ofWMH increases with age particularly after age801920 and DTI estimates of white matter integrity also sharplydeteriorate with age21 However there are few data on the age-specific association between MRI-detectable white matterdamage and cognition with most studies reporting associationspooled across a broad range of ages (eg ge507 gt603 or gt6522)Yet some studies suggest that the association may attenuate atage gt802324 although to our knowledge no studies have directlycompared the association in older vs younger adults
Establishing the relevance of WMH to cognition in very oldpatients is increasingly important because individuals over 80years of age represent the most rapidly growing segment of thepopulation25 with the greatest concern about risk ofdementia26ndash28 Furthermore MRI is now very frequently per-formed as first-line brain imaging for a wide range of neurologicsymptoms such that someWMHare almost always reported inolder patients1929 The most common indication for suchimaging in routine practice is after TIA and stroke and patientsfrequently have evidence of small vessel disease inevitablyraising concern about vascular cognitive impairment30ndash32 Wetherefore studied MRI markers of white matter damage andcognitive status in a population-based cohort of patients withTIA or minor stroke comparing those aged le80 vs gt80 years
We also explored with voxel-wise analyses whatWMH locationis more strongly associated with cognitive impairment andwhether there would be differences between age groups
MethodsStudy populationConsecutive patients were recruited betweenMarch 2012 andJune 2016 from the Oxford Vascular Study (OXVASC)a prospective cohort study of all acute vascular events ina defined population of 92000 residents registered with 100primary care physicians in Oxfordshire and the onlypopulation-based study of all vascular disease that does notexclude very old patients After a suspected nondisabling ce-rebrovascular event (NIH Stroke Scale score lt4) OXVASCparticipants undergo brain MRI detailed clinical character-ization and cognitive assessment with face-to-face follow-upat 1 3 6 12 24 and 60 months In order to avoid anyselection bias particularly against older patients patients witha previous TIA or minor stroke prior to the imaging studyperiod were included Exclusion criteria specific for thepurposes of the present imaging study were (1) MRI con-traindication or known claustrophobia (2) intracranial space-occupying lesion (3) intracranial hemorrhage (4) braindefect due to previous neurosurgery or developmentalanomalies (4) large chronic subacute or acute infarcts(ie gt25 cm on T1-weighted T2-weighted or diffusion-weighted imaging sequences) (5) significant movementartefacts that would impair registration (6) inability to per-form cognitive testing (ie due to language barriers)
Standard protocol approvals registrationsand patient consentsWritten informed consent was obtained from all participantsOXVASC was approved by the local ethics committee (Re-search Ethics Committee reference number 05Q160470)
Data availabilityRequests for data from the OXVASC Study will be consideredby PMR in line with data protection laws The general policyis that as long as the proposed use of the data is scientificallyvalid and as long as ethics approval permits suitably anony-mized data can be shared with other researchers
GlossaryANOVA = analysis of variance BET = brain extraction tool BIANCA = brain intensity abnormality classification algorithmCI = confidence interval DTI = diffusion tensor imaging FA = fractional anisotropy FLAIR = fluid-attenuated inversionrecovery FNIRT = FMRIBrsquos nonlinear image registration tool FOV = field of view GRAPPA = generalized autocalibratingpartial parallel acquisition MD = mean diffusivity MildCI = mild cognitive impairment MNI = Montreal NeurologicalInstitute MoCA = Montreal Cognitive Assessment NAWM = normal-appearing white matter NoCI = no cognitiveimpairment OR = odds ratio OXVASC = Oxford Vascular Study SevereCI = severe cognitive impairment TE = echo timeTI = inversion time TR = repetition time WMH = white matter hyperintensity
2 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
Cognitive statusParticipants were divided into 3 groups according to theirMontreal Cognitive Assessment (MoCA) scores which hasbeen shown to be sensitive to detect vascular cognitiveimpairment33ndash35 no cognitive impairment (NoCI MoCAge26) mild cognitive impairment (MildCI 20 lt MoCA lt 26)or severe cognitive impairment (SevereCI MoCA le20)These cutoffs were chosen on the basis of previous workshowing that the MoCA has high sensitivity in identifyingpoststroke patients with mild but also severemultidomaincognitive impairment3436 For the purpose of the presentstudy we used MoCA scores from the 1-month follow-up asthese better reflect the cognitive status independent fromtransient cognitive variations related to the minor cerebro-vascular event37
Imaging acquisitionAll images were acquired on a 3T Verio (Orem UT) MRIscanner The imaging protocol used until December 2014included fluid-attenuated inversion recovery (FLAIR) (repe-tition time [TR]echo time [TE]inversion time [TI] 90009402500 ms flip angle 150deg field of view [FOV] 200 mmvoxel size 08 times 08 times 5 mm with 15 mm interslice gap) post-gadolinium T1-weighted imaging (TRTETI 1250463900 ms flip angle 16deg FOV 220 mm voxel size 11 times 11 times3 mm with 15 mm interslice gap) and diffusion-weightedimaging (TRTE 4000106 ms generalized autocalibratingpartial parallel acquisition [GRAPPA] factor 2 FOV 230 mmvoxel size 18 times 18 times 4 mm with 12 mm interslice gap 12directions b value 1000 smm2)
The protocol used from January 2015 included high-resolution T1 (TRTETI 2000194880 ms flip angle 8degFOV 256 mm voxel size 1 times 1 times 1 mm) FLAIR (TRTETI9000882500ms flip angle 150deg FOV 192mm voxel size 1times 1 times 3 mm) and diffusion-weighted imaging (TRTE =800086 ms GRAPPA factor 2 flip angle 16deg FOV 192 mmvoxel size 2 times 2 times 2 mm 32 directions b value 1500 smm2)
Measures of white matter damage (WMH volumes MD andFA in NAWM) obtained from the second protocol werestandardized on values obtained from the first protocol toallow statistical analyses across the whole sample In additionprotocol type was added as covariate of no interest on uni-variate and voxel-wise analyses
Presenceabsence of lacunar infarcts was rated by strokeneurologists and neuroradiologists who were blind to thecognitive scores Lacunar infarcts were defined as hypointenselesions on T1 imaging with corresponding hyperintense le-sion on FLAIR images with a diameter lt15 mm
WMH measurementWMHs were automatically segmented on FLAIR images withbrain intensity abnormality classification algorithm(BIANCA) a fully automated supervised method for WMHdetection which gives the probability per voxel of being
WMH38 The total WMH volume was calculated from thevoxels exceeding a probability of 09 (which gave the highestaccuracy on this dataset as tested in our previous work38) ofbeing WMH and located within a white matter maskObtained values were adjusted for the total brain and ven-tricles volume (ie the sum of the volumes of gray matterwhite matter and ventricles) calculated from the brain-extracted images using FSLrsquos brain extraction tool (BET)39
and log transformed40 as a proxy for intracranial volume thatcould be obtained from the available FLAIR images
For voxel-wise analyses the thresholded and masked WMHmaps were binarized and transformed into Montreal Neuro-logical Institute (MNI) standard space applying the nonlinearregistration (FMRIBrsquos nonlinear image registration tool[FNIRT])41 calculated from FLAIR to MNI (via high-resolution T1 if available) We further thresholded thetransformed maps at 05 binarized them and applied spatialsmoothing of full width at half maximum = 6 mm to com-pensate for registration errors (the size of the smoothingkernel was empirically decided to be the same as the maxi-mum voxel dimension) The resulting maps were entered intovoxel-wise WMH statistical analyses
WMH were also visually rated on the Fazekas WMH scaleallowing categorical measurement of periventricular and deepWMH in grades from 0 (absent) to 3 (severe)42
Measurements of microstructural whitematter integrity in NAWMDiffusion-weighted images were first corrected for head mo-tion and eddy currents DTI was then performed to createMD and FA maps by fitting a tensor model to the diffusion-weighted images using FMRIBrsquos Diffusion Toolbox43 Imageswere brain-extracted using FSLrsquos BET All participantsrsquo FAmaps were then nonlinearly registered to a common diffusionspace (FMRIB58_FA an FA template in MNI space) usingFNIRT and the same transformation was applied to MD dataFor each participant we calculated the linear transformationfrom FLAIR to diffusion data (b = 0 image used as reference)and combined it with the nonlinear transformation fromdiffusion data to the common space calculated before Theresulting transformation was then applied to WMH maps toregister them from FLAIR to diffusion common space MDand FA values from the NAWM were calculated as averagefrom voxels outside the WMH map within a mask includingall the main white matter tracts in the JHU-ICBM DTI atlas(figure 1) The evaluation of DTI-derived measures was re-stricted to the main white matter tracts and not performed inthe whole NAWM in order to focus on the tracts that aremore consistent across participants This also allows com-pensating for possible registration errors occurring in the restof the white matter In addition to exclude the possibility ofa bias in the results due to a systematic difference in regis-tration quality across age groups we calculated a cost metric(root mean square difference) between each participantrsquos FAimage registered to the template and the template itself and
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 3
verified that it was not significantly different between agegroups (estimated root mean square difference = 00420 plusmn00039 lt80 years only = 00418 plusmn 00039 gt80 years only =00426 plusmn 00041)
Statistical analysesPatients were grouped by age le80 vs gt80 years and cognitivestatus (NoCI MildCI SevereCI respectively) as definedabove Comparisons between age groups were performedwith Mann-Whitney or independent t test as appropriate forcontinuous variables and χ2 tests for dichotomous variablesusing SPSS version 220 (SPSS Inc Chicago IL) Age-relateddifferences in the associations between MRI markers of whitematter damage and cognitive status were studied with 2 times 3factorial analyses of variance (ANOVAs) Results were con-sidered significant at p lt 005
Sensitivity analyses were conducted to control for the effectsof potential confounders These analyses included MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risks factors (ie the sum of hyper-tension diabetes mellitus atrial fibrillation hyperlipidemiaand smoking) Furthermore to account for differences insample size between age groups the ANOVA was repeatedusing 4 random subsamples of young participants stratified oncognitive status to match the original large sample
Voxel-wise analysis of WMHWe performed the same 2 times 3 factorial ANOVA at the voxellevel on the maps of WMH obtained with BIANCA to studythe location in the brain of age-by-cognitive status interactionsWe then performed correlational voxel-wise analysis on the
samemaps to test the association between higher probability ofhavingWMH and lower MoCA score in patients aged le80 andin patients aged gt80 separately for the 2 groups
All the statistical analyses were performed with nonparametricpermutation tests using the randomise tool in FSL44 withprotocol as nuisance covariate and restricted to a whitematter mask Results were considered significant at p lt 005fully corrected for multiple comparisons using family-wiseerror correction at the voxel level44
ResultsAmong 570 consecutive eligible patients 4 were excluded dueto subsequently diagnosed WMHmimics (multiple sclerosis)and known other causes of dementia (cerebral autosomaldominant arteriopathy with subcortical infarcts and leu-koencephalopathy and Alzheimer disease) Table 1 reportsthe characteristics of the 566 patients included in the WMHanalyses also divided by age groups (ie le80 and gt80)Diffusion-weighted MRI allowing measurement of FA andMD were acquired from a subsample of 498 consecutiveparticipants (88) as this sequence was not initially includedin the protocol Sensitivity analyses on WMH volumes(available on 566 participants) were repeated in the sub-sample of 498 participants and gave similar results
Age-related associations between WMHvolume and cognitive statusA 2 times 3 factorial ANOVA on WMH volumes showed a maineffect of age (F = 3495 p lt 0001) a main effect of cognition
Figure 1 Diffusion tensor imaging (DTI) measurements in normal-appearing white matter (NAWM)
Examples of (A) fractional anisotropy (FA) and (B)mean diffusivity (MD) maps registered in Mon-treal Neurological Institute space from a singleparticipant Average FA and MD value within(NAWM) was calculated from the regions shownin yellow that is within a mask including all themain white matter tracts from the JHU-ICBM DTIatlas and excluding regions of white matterhyperintensity (WMH) obtained with brain in-tensity abnormality classification algorithm (red)
4 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(F = 661 p = 0001) and a significant interaction between ageand cognition (F = 416 pinteraction = 0016) The interactionsuggested that associations between WMH and cognitivestatus are different between the age groups (age le80 vs gt 80years figure 2) Follow-up one-way ANOVAs confirmed thatthere were WMH volume differences across cognitive groupsonly in patients aged le80 and not in patients aged gt80(table 2) even when correcting for within-group age (F =617 p = 0002 for age le80 F = 106 p = 0351 for age gt80)Sensitivity analyses showed that the interaction remainedsignificant (pinteraction = 0046) when adjusting for MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risk factors It also remained signifi-cant when repeated using groups of equal sample sizesobtained by randomly splitting the group of young partic-ipants in 4 subsets matched on cognition to the original one(table 3)
The association between highWMH load (above vs below the80th percentile) and dementia (SevereCI vs NoCI) wasstrong at age le80 (odds ratio [OR] 40 95 confidence in-terval [CI] 165ndash971 p = 0001) but absent at age gt80 (OR089 95 CI 026ndash303 p = 086) These associations were
unchanged when the analysis was repeated with the 80thpercentile cutoff determined separately in the 2 age groups(age le80 OR 39 95 CI 168ndash917 p = 0001 age gt80 OR16 95 CI 041ndash647 p = 0488)
A 2 times 3 factorial ANOVA with years of education as de-pendent variable showed no significant interaction betweenage and cognitive groups (p = 0693) nor did anotherANOVA with brain and ventricles volume as dependentvariable (p = 0159)
Age-relatedassociationsbetweenMDandFA inNAWM and cognitive statusA 2 times 3 factorial ANOVA on average MD values extractedfrom NAWM showed a main effect of age (F = 7358 p lt0001) a main effect of cognitive status (F = 1484 p lt 0001)and a significant interaction between age and cognitive status(F = 332 pinteraction = 0037) Sensitivity analyses showed thatthe interaction on MD from NAWM remained significantwhen adjusting for MRI protocol sex years of educationhead size presence of lacunes and number of vascular risksfactors (pinteraction = 0048) A similar 2 times 3 factorial ANOVAon average FA values extracted from NAWM showed a main
Table 1 Clinical and imaging features of total sample and age groups
Study Total Age le80 y Age gt80 y p Value
N 566 459 107
Age y mean plusmn SD 667 plusmn 143 625 plusmn 125 847 plusmn 37
Age range y 20ndash102 20ndash80 81ndash102
Age y median (IQR) 69 (205) 65 (179) 838 (49)
Female sex n () 280 (495) 228 (497) 52 (486) 0841
TIA other minor stroke n () 408 (721) 336 (734) 72 (679) 0259
Years of education mean plusmn SD 130 plusmn 35 133 plusmn 34 120 plusmn 37 0002
Hypertension n () 260 (459) 190 (415) 70 (654) lt0001
Diabetes n () 55 (97) 41 (90) 14 (131) 0168
Atrial fibrillation n () 60 (106) 40 (87) 20 (187) 0002
Hyperlipidemia n () 163 (288) 130 (284) 33 (308) 0538
Smoking n () 159 (281) 138 (301) 21 (196) 0040
Total Fazekas ge3 n () 174 (307) 117 (255) 57 (532) lt0001
Presence of lacunar infarcts n () 77 (136) 48 (105) 29 (274) lt0001
Brain volumea cm3 mean plusmn SD 10470 plusmn 1340 10738 plusmn 1298 9669 plusmn 1152 lt0001
WMH volume cm3 mean plusmn SD 117 plusmn 109 100 plusmn 89 191 plusmn 147 lt0001
Average FA (NAWM) mean plusmn SD 049 plusmn 003 050 plusmn 003 046 plusmn 003 lt0001
Average MD (NAWM) (times1023) mean plusmn SD 090 plusmn 009 088 plusmn 007 099 plusmn 008 lt0001
Abbreviations FA = fractional anisotropy IQR = interquartile range MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesTotal Fazekas calculated as sum of deep and periventricular scoresa Defined as the sum of gray and white matter volumes (ie not including the ventricles)
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 5
effect of age (F = 4174 p lt 0001) and a main effect ofcognitive status (F = 1367 p lt 0001) but no interaction (F =152 pinteraction = 0219)
One-way ANOVAs on average MD and FA values extractedfrom NAWM confirmed that there were differences acrosscognitive groups only in patients aged le80 but not inpatients aged gt80 (table 2) Adding age or WMH volume ascovariates (analyses of covariance) did not change theresults (table 4)
Localization of WMH relevant tocognitive statusThe voxel-wise 2 times 3 factorial ANOVA showed an interactionbetween cognitive status and age group in an area of the leftdeep frontal white matter (figure 3 bluendashlight blue) Thevoxel-wise correlational analysis performed in patients agedle80 showed that in this group the association between theprobability of having WMH and lower MoCA score was lo-calized in periventricular frontal and parietal white matterareas bilaterally more extended on the left hemisphere
Table 2 Clinical and imaging features of cognitive groups by age
No CI Mild CI Severe CI p Value
Age le80 y
NWMH (NDTI) 338 (295) 97 (83) 24 (20)
Age y mean plusmn SD 618 plusmn 25 620 plusmn 126 702 plusmn 87 0005
Female n () 165 (488) 45 (464) 18 (750) 0036
Event type TIA other minor stroke n () 254 (754) 71 (732) 11 (458) 0007
Hypertension n () 131 (389) 44 (454) 15 (625) 0161
Diabetes n () 26 (77) 7 (72) 8 (333) 0001
Atrial fibrillation n () 26 (77) 12 (124) 2 (83) 0561
Hyperlipidemia n () 93 (276) 28 (289) 9 (375) 0871
Smoking n () 107 (318) 24 (247) 7 (292) 0547
Presence of lacunar infarcts n () 33 (98) 12 (126) 3 (125) 0691
WMH volume cm3 mean plusmn SD 94 plusmn 79 101 plusmn 78 181 plusmn 184 lt0001a
Average FA (NAWM) mean plusmn SD 050 plusmn 003 049 plusmn 003 047 plusmn 003 lt0001a
Average MD (NAWM) (times1023) mean plusmn SD 086 plusmn 006 096 plusmn 007 096 plusmn 007 lt0001a
Age gt80 y
NWMH (NDTI) 44 (42) 46 (42) 17 (16)
Age y mean plusmn SD 839 plusmn 33 859 plusmn 42 834 plusmn 25 0009
Female sex n () 22 (500) 22 (478) 8 (471) 0970
Event type TIA other minor stroke n () 31 (721) 30 (652) 11 (647) 0749
Hypertension n () 26 (591) 32 (696) 12 (706) 0730
Diabetes n () 3 (68) 8 (174) 3 (176) 0575
Atrial fibrillation n () 6 (136) 12 (261) 2 (118) 0512
Hyperlipidemia n () 13 (295) 17 (370) 3 (176) 0637
Smoking n () 9 (205) 9 (196) 3 (176) 0901
Presence of lacunar infarcts n () 12 (279) 15 (326) 2 (118) 0256
WMH volume cm3 mean plusmn SD 159 plusmn 107 213 plusmn 146 214 plusmn 219 0166a
Average FA (NAWM) mean plusmn SD 047 plusmn 003 045 plusmn 003 045 plusmn 004 0110a
Average MD (NAWM) (times1023) mean plusmn SD 096 plusmn 007 101 plusmn 009 101 plusmn 010 0067a
Abbreviations CI = cognitive impairment FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesa Comparisons between cognitive groups that were significant for patients le80 but not for patients gt80
6 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

Cognitive statusParticipants were divided into 3 groups according to theirMontreal Cognitive Assessment (MoCA) scores which hasbeen shown to be sensitive to detect vascular cognitiveimpairment33ndash35 no cognitive impairment (NoCI MoCAge26) mild cognitive impairment (MildCI 20 lt MoCA lt 26)or severe cognitive impairment (SevereCI MoCA le20)These cutoffs were chosen on the basis of previous workshowing that the MoCA has high sensitivity in identifyingpoststroke patients with mild but also severemultidomaincognitive impairment3436 For the purpose of the presentstudy we used MoCA scores from the 1-month follow-up asthese better reflect the cognitive status independent fromtransient cognitive variations related to the minor cerebro-vascular event37
Imaging acquisitionAll images were acquired on a 3T Verio (Orem UT) MRIscanner The imaging protocol used until December 2014included fluid-attenuated inversion recovery (FLAIR) (repe-tition time [TR]echo time [TE]inversion time [TI] 90009402500 ms flip angle 150deg field of view [FOV] 200 mmvoxel size 08 times 08 times 5 mm with 15 mm interslice gap) post-gadolinium T1-weighted imaging (TRTETI 1250463900 ms flip angle 16deg FOV 220 mm voxel size 11 times 11 times3 mm with 15 mm interslice gap) and diffusion-weightedimaging (TRTE 4000106 ms generalized autocalibratingpartial parallel acquisition [GRAPPA] factor 2 FOV 230 mmvoxel size 18 times 18 times 4 mm with 12 mm interslice gap 12directions b value 1000 smm2)
The protocol used from January 2015 included high-resolution T1 (TRTETI 2000194880 ms flip angle 8degFOV 256 mm voxel size 1 times 1 times 1 mm) FLAIR (TRTETI9000882500ms flip angle 150deg FOV 192mm voxel size 1times 1 times 3 mm) and diffusion-weighted imaging (TRTE =800086 ms GRAPPA factor 2 flip angle 16deg FOV 192 mmvoxel size 2 times 2 times 2 mm 32 directions b value 1500 smm2)
Measures of white matter damage (WMH volumes MD andFA in NAWM) obtained from the second protocol werestandardized on values obtained from the first protocol toallow statistical analyses across the whole sample In additionprotocol type was added as covariate of no interest on uni-variate and voxel-wise analyses
Presenceabsence of lacunar infarcts was rated by strokeneurologists and neuroradiologists who were blind to thecognitive scores Lacunar infarcts were defined as hypointenselesions on T1 imaging with corresponding hyperintense le-sion on FLAIR images with a diameter lt15 mm
WMH measurementWMHs were automatically segmented on FLAIR images withbrain intensity abnormality classification algorithm(BIANCA) a fully automated supervised method for WMHdetection which gives the probability per voxel of being
WMH38 The total WMH volume was calculated from thevoxels exceeding a probability of 09 (which gave the highestaccuracy on this dataset as tested in our previous work38) ofbeing WMH and located within a white matter maskObtained values were adjusted for the total brain and ven-tricles volume (ie the sum of the volumes of gray matterwhite matter and ventricles) calculated from the brain-extracted images using FSLrsquos brain extraction tool (BET)39
and log transformed40 as a proxy for intracranial volume thatcould be obtained from the available FLAIR images
For voxel-wise analyses the thresholded and masked WMHmaps were binarized and transformed into Montreal Neuro-logical Institute (MNI) standard space applying the nonlinearregistration (FMRIBrsquos nonlinear image registration tool[FNIRT])41 calculated from FLAIR to MNI (via high-resolution T1 if available) We further thresholded thetransformed maps at 05 binarized them and applied spatialsmoothing of full width at half maximum = 6 mm to com-pensate for registration errors (the size of the smoothingkernel was empirically decided to be the same as the maxi-mum voxel dimension) The resulting maps were entered intovoxel-wise WMH statistical analyses
WMH were also visually rated on the Fazekas WMH scaleallowing categorical measurement of periventricular and deepWMH in grades from 0 (absent) to 3 (severe)42
Measurements of microstructural whitematter integrity in NAWMDiffusion-weighted images were first corrected for head mo-tion and eddy currents DTI was then performed to createMD and FA maps by fitting a tensor model to the diffusion-weighted images using FMRIBrsquos Diffusion Toolbox43 Imageswere brain-extracted using FSLrsquos BET All participantsrsquo FAmaps were then nonlinearly registered to a common diffusionspace (FMRIB58_FA an FA template in MNI space) usingFNIRT and the same transformation was applied to MD dataFor each participant we calculated the linear transformationfrom FLAIR to diffusion data (b = 0 image used as reference)and combined it with the nonlinear transformation fromdiffusion data to the common space calculated before Theresulting transformation was then applied to WMH maps toregister them from FLAIR to diffusion common space MDand FA values from the NAWM were calculated as averagefrom voxels outside the WMH map within a mask includingall the main white matter tracts in the JHU-ICBM DTI atlas(figure 1) The evaluation of DTI-derived measures was re-stricted to the main white matter tracts and not performed inthe whole NAWM in order to focus on the tracts that aremore consistent across participants This also allows com-pensating for possible registration errors occurring in the restof the white matter In addition to exclude the possibility ofa bias in the results due to a systematic difference in regis-tration quality across age groups we calculated a cost metric(root mean square difference) between each participantrsquos FAimage registered to the template and the template itself and
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 3
verified that it was not significantly different between agegroups (estimated root mean square difference = 00420 plusmn00039 lt80 years only = 00418 plusmn 00039 gt80 years only =00426 plusmn 00041)
Statistical analysesPatients were grouped by age le80 vs gt80 years and cognitivestatus (NoCI MildCI SevereCI respectively) as definedabove Comparisons between age groups were performedwith Mann-Whitney or independent t test as appropriate forcontinuous variables and χ2 tests for dichotomous variablesusing SPSS version 220 (SPSS Inc Chicago IL) Age-relateddifferences in the associations between MRI markers of whitematter damage and cognitive status were studied with 2 times 3factorial analyses of variance (ANOVAs) Results were con-sidered significant at p lt 005
Sensitivity analyses were conducted to control for the effectsof potential confounders These analyses included MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risks factors (ie the sum of hyper-tension diabetes mellitus atrial fibrillation hyperlipidemiaand smoking) Furthermore to account for differences insample size between age groups the ANOVA was repeatedusing 4 random subsamples of young participants stratified oncognitive status to match the original large sample
Voxel-wise analysis of WMHWe performed the same 2 times 3 factorial ANOVA at the voxellevel on the maps of WMH obtained with BIANCA to studythe location in the brain of age-by-cognitive status interactionsWe then performed correlational voxel-wise analysis on the
samemaps to test the association between higher probability ofhavingWMH and lower MoCA score in patients aged le80 andin patients aged gt80 separately for the 2 groups
All the statistical analyses were performed with nonparametricpermutation tests using the randomise tool in FSL44 withprotocol as nuisance covariate and restricted to a whitematter mask Results were considered significant at p lt 005fully corrected for multiple comparisons using family-wiseerror correction at the voxel level44
ResultsAmong 570 consecutive eligible patients 4 were excluded dueto subsequently diagnosed WMHmimics (multiple sclerosis)and known other causes of dementia (cerebral autosomaldominant arteriopathy with subcortical infarcts and leu-koencephalopathy and Alzheimer disease) Table 1 reportsthe characteristics of the 566 patients included in the WMHanalyses also divided by age groups (ie le80 and gt80)Diffusion-weighted MRI allowing measurement of FA andMD were acquired from a subsample of 498 consecutiveparticipants (88) as this sequence was not initially includedin the protocol Sensitivity analyses on WMH volumes(available on 566 participants) were repeated in the sub-sample of 498 participants and gave similar results
Age-related associations between WMHvolume and cognitive statusA 2 times 3 factorial ANOVA on WMH volumes showed a maineffect of age (F = 3495 p lt 0001) a main effect of cognition
Figure 1 Diffusion tensor imaging (DTI) measurements in normal-appearing white matter (NAWM)
Examples of (A) fractional anisotropy (FA) and (B)mean diffusivity (MD) maps registered in Mon-treal Neurological Institute space from a singleparticipant Average FA and MD value within(NAWM) was calculated from the regions shownin yellow that is within a mask including all themain white matter tracts from the JHU-ICBM DTIatlas and excluding regions of white matterhyperintensity (WMH) obtained with brain in-tensity abnormality classification algorithm (red)
4 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(F = 661 p = 0001) and a significant interaction between ageand cognition (F = 416 pinteraction = 0016) The interactionsuggested that associations between WMH and cognitivestatus are different between the age groups (age le80 vs gt 80years figure 2) Follow-up one-way ANOVAs confirmed thatthere were WMH volume differences across cognitive groupsonly in patients aged le80 and not in patients aged gt80(table 2) even when correcting for within-group age (F =617 p = 0002 for age le80 F = 106 p = 0351 for age gt80)Sensitivity analyses showed that the interaction remainedsignificant (pinteraction = 0046) when adjusting for MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risk factors It also remained signifi-cant when repeated using groups of equal sample sizesobtained by randomly splitting the group of young partic-ipants in 4 subsets matched on cognition to the original one(table 3)
The association between highWMH load (above vs below the80th percentile) and dementia (SevereCI vs NoCI) wasstrong at age le80 (odds ratio [OR] 40 95 confidence in-terval [CI] 165ndash971 p = 0001) but absent at age gt80 (OR089 95 CI 026ndash303 p = 086) These associations were
unchanged when the analysis was repeated with the 80thpercentile cutoff determined separately in the 2 age groups(age le80 OR 39 95 CI 168ndash917 p = 0001 age gt80 OR16 95 CI 041ndash647 p = 0488)
A 2 times 3 factorial ANOVA with years of education as de-pendent variable showed no significant interaction betweenage and cognitive groups (p = 0693) nor did anotherANOVA with brain and ventricles volume as dependentvariable (p = 0159)
Age-relatedassociationsbetweenMDandFA inNAWM and cognitive statusA 2 times 3 factorial ANOVA on average MD values extractedfrom NAWM showed a main effect of age (F = 7358 p lt0001) a main effect of cognitive status (F = 1484 p lt 0001)and a significant interaction between age and cognitive status(F = 332 pinteraction = 0037) Sensitivity analyses showed thatthe interaction on MD from NAWM remained significantwhen adjusting for MRI protocol sex years of educationhead size presence of lacunes and number of vascular risksfactors (pinteraction = 0048) A similar 2 times 3 factorial ANOVAon average FA values extracted from NAWM showed a main
Table 1 Clinical and imaging features of total sample and age groups
Study Total Age le80 y Age gt80 y p Value
N 566 459 107
Age y mean plusmn SD 667 plusmn 143 625 plusmn 125 847 plusmn 37
Age range y 20ndash102 20ndash80 81ndash102
Age y median (IQR) 69 (205) 65 (179) 838 (49)
Female sex n () 280 (495) 228 (497) 52 (486) 0841
TIA other minor stroke n () 408 (721) 336 (734) 72 (679) 0259
Years of education mean plusmn SD 130 plusmn 35 133 plusmn 34 120 plusmn 37 0002
Hypertension n () 260 (459) 190 (415) 70 (654) lt0001
Diabetes n () 55 (97) 41 (90) 14 (131) 0168
Atrial fibrillation n () 60 (106) 40 (87) 20 (187) 0002
Hyperlipidemia n () 163 (288) 130 (284) 33 (308) 0538
Smoking n () 159 (281) 138 (301) 21 (196) 0040
Total Fazekas ge3 n () 174 (307) 117 (255) 57 (532) lt0001
Presence of lacunar infarcts n () 77 (136) 48 (105) 29 (274) lt0001
Brain volumea cm3 mean plusmn SD 10470 plusmn 1340 10738 plusmn 1298 9669 plusmn 1152 lt0001
WMH volume cm3 mean plusmn SD 117 plusmn 109 100 plusmn 89 191 plusmn 147 lt0001
Average FA (NAWM) mean plusmn SD 049 plusmn 003 050 plusmn 003 046 plusmn 003 lt0001
Average MD (NAWM) (times1023) mean plusmn SD 090 plusmn 009 088 plusmn 007 099 plusmn 008 lt0001
Abbreviations FA = fractional anisotropy IQR = interquartile range MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesTotal Fazekas calculated as sum of deep and periventricular scoresa Defined as the sum of gray and white matter volumes (ie not including the ventricles)
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 5
effect of age (F = 4174 p lt 0001) and a main effect ofcognitive status (F = 1367 p lt 0001) but no interaction (F =152 pinteraction = 0219)
One-way ANOVAs on average MD and FA values extractedfrom NAWM confirmed that there were differences acrosscognitive groups only in patients aged le80 but not inpatients aged gt80 (table 2) Adding age or WMH volume ascovariates (analyses of covariance) did not change theresults (table 4)
Localization of WMH relevant tocognitive statusThe voxel-wise 2 times 3 factorial ANOVA showed an interactionbetween cognitive status and age group in an area of the leftdeep frontal white matter (figure 3 bluendashlight blue) Thevoxel-wise correlational analysis performed in patients agedle80 showed that in this group the association between theprobability of having WMH and lower MoCA score was lo-calized in periventricular frontal and parietal white matterareas bilaterally more extended on the left hemisphere
Table 2 Clinical and imaging features of cognitive groups by age
No CI Mild CI Severe CI p Value
Age le80 y
NWMH (NDTI) 338 (295) 97 (83) 24 (20)
Age y mean plusmn SD 618 plusmn 25 620 plusmn 126 702 plusmn 87 0005
Female n () 165 (488) 45 (464) 18 (750) 0036
Event type TIA other minor stroke n () 254 (754) 71 (732) 11 (458) 0007
Hypertension n () 131 (389) 44 (454) 15 (625) 0161
Diabetes n () 26 (77) 7 (72) 8 (333) 0001
Atrial fibrillation n () 26 (77) 12 (124) 2 (83) 0561
Hyperlipidemia n () 93 (276) 28 (289) 9 (375) 0871
Smoking n () 107 (318) 24 (247) 7 (292) 0547
Presence of lacunar infarcts n () 33 (98) 12 (126) 3 (125) 0691
WMH volume cm3 mean plusmn SD 94 plusmn 79 101 plusmn 78 181 plusmn 184 lt0001a
Average FA (NAWM) mean plusmn SD 050 plusmn 003 049 plusmn 003 047 plusmn 003 lt0001a
Average MD (NAWM) (times1023) mean plusmn SD 086 plusmn 006 096 plusmn 007 096 plusmn 007 lt0001a
Age gt80 y
NWMH (NDTI) 44 (42) 46 (42) 17 (16)
Age y mean plusmn SD 839 plusmn 33 859 plusmn 42 834 plusmn 25 0009
Female sex n () 22 (500) 22 (478) 8 (471) 0970
Event type TIA other minor stroke n () 31 (721) 30 (652) 11 (647) 0749
Hypertension n () 26 (591) 32 (696) 12 (706) 0730
Diabetes n () 3 (68) 8 (174) 3 (176) 0575
Atrial fibrillation n () 6 (136) 12 (261) 2 (118) 0512
Hyperlipidemia n () 13 (295) 17 (370) 3 (176) 0637
Smoking n () 9 (205) 9 (196) 3 (176) 0901
Presence of lacunar infarcts n () 12 (279) 15 (326) 2 (118) 0256
WMH volume cm3 mean plusmn SD 159 plusmn 107 213 plusmn 146 214 plusmn 219 0166a
Average FA (NAWM) mean plusmn SD 047 plusmn 003 045 plusmn 003 045 plusmn 004 0110a
Average MD (NAWM) (times1023) mean plusmn SD 096 plusmn 007 101 plusmn 009 101 plusmn 010 0067a
Abbreviations CI = cognitive impairment FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesa Comparisons between cognitive groups that were significant for patients le80 but not for patients gt80
6 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

verified that it was not significantly different between agegroups (estimated root mean square difference = 00420 plusmn00039 lt80 years only = 00418 plusmn 00039 gt80 years only =00426 plusmn 00041)
Statistical analysesPatients were grouped by age le80 vs gt80 years and cognitivestatus (NoCI MildCI SevereCI respectively) as definedabove Comparisons between age groups were performedwith Mann-Whitney or independent t test as appropriate forcontinuous variables and χ2 tests for dichotomous variablesusing SPSS version 220 (SPSS Inc Chicago IL) Age-relateddifferences in the associations between MRI markers of whitematter damage and cognitive status were studied with 2 times 3factorial analyses of variance (ANOVAs) Results were con-sidered significant at p lt 005
Sensitivity analyses were conducted to control for the effectsof potential confounders These analyses included MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risks factors (ie the sum of hyper-tension diabetes mellitus atrial fibrillation hyperlipidemiaand smoking) Furthermore to account for differences insample size between age groups the ANOVA was repeatedusing 4 random subsamples of young participants stratified oncognitive status to match the original large sample
Voxel-wise analysis of WMHWe performed the same 2 times 3 factorial ANOVA at the voxellevel on the maps of WMH obtained with BIANCA to studythe location in the brain of age-by-cognitive status interactionsWe then performed correlational voxel-wise analysis on the
samemaps to test the association between higher probability ofhavingWMH and lower MoCA score in patients aged le80 andin patients aged gt80 separately for the 2 groups
All the statistical analyses were performed with nonparametricpermutation tests using the randomise tool in FSL44 withprotocol as nuisance covariate and restricted to a whitematter mask Results were considered significant at p lt 005fully corrected for multiple comparisons using family-wiseerror correction at the voxel level44
ResultsAmong 570 consecutive eligible patients 4 were excluded dueto subsequently diagnosed WMHmimics (multiple sclerosis)and known other causes of dementia (cerebral autosomaldominant arteriopathy with subcortical infarcts and leu-koencephalopathy and Alzheimer disease) Table 1 reportsthe characteristics of the 566 patients included in the WMHanalyses also divided by age groups (ie le80 and gt80)Diffusion-weighted MRI allowing measurement of FA andMD were acquired from a subsample of 498 consecutiveparticipants (88) as this sequence was not initially includedin the protocol Sensitivity analyses on WMH volumes(available on 566 participants) were repeated in the sub-sample of 498 participants and gave similar results
Age-related associations between WMHvolume and cognitive statusA 2 times 3 factorial ANOVA on WMH volumes showed a maineffect of age (F = 3495 p lt 0001) a main effect of cognition
Figure 1 Diffusion tensor imaging (DTI) measurements in normal-appearing white matter (NAWM)
Examples of (A) fractional anisotropy (FA) and (B)mean diffusivity (MD) maps registered in Mon-treal Neurological Institute space from a singleparticipant Average FA and MD value within(NAWM) was calculated from the regions shownin yellow that is within a mask including all themain white matter tracts from the JHU-ICBM DTIatlas and excluding regions of white matterhyperintensity (WMH) obtained with brain in-tensity abnormality classification algorithm (red)
4 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(F = 661 p = 0001) and a significant interaction between ageand cognition (F = 416 pinteraction = 0016) The interactionsuggested that associations between WMH and cognitivestatus are different between the age groups (age le80 vs gt 80years figure 2) Follow-up one-way ANOVAs confirmed thatthere were WMH volume differences across cognitive groupsonly in patients aged le80 and not in patients aged gt80(table 2) even when correcting for within-group age (F =617 p = 0002 for age le80 F = 106 p = 0351 for age gt80)Sensitivity analyses showed that the interaction remainedsignificant (pinteraction = 0046) when adjusting for MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risk factors It also remained signifi-cant when repeated using groups of equal sample sizesobtained by randomly splitting the group of young partic-ipants in 4 subsets matched on cognition to the original one(table 3)
The association between highWMH load (above vs below the80th percentile) and dementia (SevereCI vs NoCI) wasstrong at age le80 (odds ratio [OR] 40 95 confidence in-terval [CI] 165ndash971 p = 0001) but absent at age gt80 (OR089 95 CI 026ndash303 p = 086) These associations were
unchanged when the analysis was repeated with the 80thpercentile cutoff determined separately in the 2 age groups(age le80 OR 39 95 CI 168ndash917 p = 0001 age gt80 OR16 95 CI 041ndash647 p = 0488)
A 2 times 3 factorial ANOVA with years of education as de-pendent variable showed no significant interaction betweenage and cognitive groups (p = 0693) nor did anotherANOVA with brain and ventricles volume as dependentvariable (p = 0159)
Age-relatedassociationsbetweenMDandFA inNAWM and cognitive statusA 2 times 3 factorial ANOVA on average MD values extractedfrom NAWM showed a main effect of age (F = 7358 p lt0001) a main effect of cognitive status (F = 1484 p lt 0001)and a significant interaction between age and cognitive status(F = 332 pinteraction = 0037) Sensitivity analyses showed thatthe interaction on MD from NAWM remained significantwhen adjusting for MRI protocol sex years of educationhead size presence of lacunes and number of vascular risksfactors (pinteraction = 0048) A similar 2 times 3 factorial ANOVAon average FA values extracted from NAWM showed a main
Table 1 Clinical and imaging features of total sample and age groups
Study Total Age le80 y Age gt80 y p Value
N 566 459 107
Age y mean plusmn SD 667 plusmn 143 625 plusmn 125 847 plusmn 37
Age range y 20ndash102 20ndash80 81ndash102
Age y median (IQR) 69 (205) 65 (179) 838 (49)
Female sex n () 280 (495) 228 (497) 52 (486) 0841
TIA other minor stroke n () 408 (721) 336 (734) 72 (679) 0259
Years of education mean plusmn SD 130 plusmn 35 133 plusmn 34 120 plusmn 37 0002
Hypertension n () 260 (459) 190 (415) 70 (654) lt0001
Diabetes n () 55 (97) 41 (90) 14 (131) 0168
Atrial fibrillation n () 60 (106) 40 (87) 20 (187) 0002
Hyperlipidemia n () 163 (288) 130 (284) 33 (308) 0538
Smoking n () 159 (281) 138 (301) 21 (196) 0040
Total Fazekas ge3 n () 174 (307) 117 (255) 57 (532) lt0001
Presence of lacunar infarcts n () 77 (136) 48 (105) 29 (274) lt0001
Brain volumea cm3 mean plusmn SD 10470 plusmn 1340 10738 plusmn 1298 9669 plusmn 1152 lt0001
WMH volume cm3 mean plusmn SD 117 plusmn 109 100 plusmn 89 191 plusmn 147 lt0001
Average FA (NAWM) mean plusmn SD 049 plusmn 003 050 plusmn 003 046 plusmn 003 lt0001
Average MD (NAWM) (times1023) mean plusmn SD 090 plusmn 009 088 plusmn 007 099 plusmn 008 lt0001
Abbreviations FA = fractional anisotropy IQR = interquartile range MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesTotal Fazekas calculated as sum of deep and periventricular scoresa Defined as the sum of gray and white matter volumes (ie not including the ventricles)
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 5
effect of age (F = 4174 p lt 0001) and a main effect ofcognitive status (F = 1367 p lt 0001) but no interaction (F =152 pinteraction = 0219)
One-way ANOVAs on average MD and FA values extractedfrom NAWM confirmed that there were differences acrosscognitive groups only in patients aged le80 but not inpatients aged gt80 (table 2) Adding age or WMH volume ascovariates (analyses of covariance) did not change theresults (table 4)
Localization of WMH relevant tocognitive statusThe voxel-wise 2 times 3 factorial ANOVA showed an interactionbetween cognitive status and age group in an area of the leftdeep frontal white matter (figure 3 bluendashlight blue) Thevoxel-wise correlational analysis performed in patients agedle80 showed that in this group the association between theprobability of having WMH and lower MoCA score was lo-calized in periventricular frontal and parietal white matterareas bilaterally more extended on the left hemisphere
Table 2 Clinical and imaging features of cognitive groups by age
No CI Mild CI Severe CI p Value
Age le80 y
NWMH (NDTI) 338 (295) 97 (83) 24 (20)
Age y mean plusmn SD 618 plusmn 25 620 plusmn 126 702 plusmn 87 0005
Female n () 165 (488) 45 (464) 18 (750) 0036
Event type TIA other minor stroke n () 254 (754) 71 (732) 11 (458) 0007
Hypertension n () 131 (389) 44 (454) 15 (625) 0161
Diabetes n () 26 (77) 7 (72) 8 (333) 0001
Atrial fibrillation n () 26 (77) 12 (124) 2 (83) 0561
Hyperlipidemia n () 93 (276) 28 (289) 9 (375) 0871
Smoking n () 107 (318) 24 (247) 7 (292) 0547
Presence of lacunar infarcts n () 33 (98) 12 (126) 3 (125) 0691
WMH volume cm3 mean plusmn SD 94 plusmn 79 101 plusmn 78 181 plusmn 184 lt0001a
Average FA (NAWM) mean plusmn SD 050 plusmn 003 049 plusmn 003 047 plusmn 003 lt0001a
Average MD (NAWM) (times1023) mean plusmn SD 086 plusmn 006 096 plusmn 007 096 plusmn 007 lt0001a
Age gt80 y
NWMH (NDTI) 44 (42) 46 (42) 17 (16)
Age y mean plusmn SD 839 plusmn 33 859 plusmn 42 834 plusmn 25 0009
Female sex n () 22 (500) 22 (478) 8 (471) 0970
Event type TIA other minor stroke n () 31 (721) 30 (652) 11 (647) 0749
Hypertension n () 26 (591) 32 (696) 12 (706) 0730
Diabetes n () 3 (68) 8 (174) 3 (176) 0575
Atrial fibrillation n () 6 (136) 12 (261) 2 (118) 0512
Hyperlipidemia n () 13 (295) 17 (370) 3 (176) 0637
Smoking n () 9 (205) 9 (196) 3 (176) 0901
Presence of lacunar infarcts n () 12 (279) 15 (326) 2 (118) 0256
WMH volume cm3 mean plusmn SD 159 plusmn 107 213 plusmn 146 214 plusmn 219 0166a
Average FA (NAWM) mean plusmn SD 047 plusmn 003 045 plusmn 003 045 plusmn 004 0110a
Average MD (NAWM) (times1023) mean plusmn SD 096 plusmn 007 101 plusmn 009 101 plusmn 010 0067a
Abbreviations CI = cognitive impairment FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesa Comparisons between cognitive groups that were significant for patients le80 but not for patients gt80
6 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

(F = 661 p = 0001) and a significant interaction between ageand cognition (F = 416 pinteraction = 0016) The interactionsuggested that associations between WMH and cognitivestatus are different between the age groups (age le80 vs gt 80years figure 2) Follow-up one-way ANOVAs confirmed thatthere were WMH volume differences across cognitive groupsonly in patients aged le80 and not in patients aged gt80(table 2) even when correcting for within-group age (F =617 p = 0002 for age le80 F = 106 p = 0351 for age gt80)Sensitivity analyses showed that the interaction remainedsignificant (pinteraction = 0046) when adjusting for MRI pro-tocol sex years of education head size presence of lacunesand number of vascular risk factors It also remained signifi-cant when repeated using groups of equal sample sizesobtained by randomly splitting the group of young partic-ipants in 4 subsets matched on cognition to the original one(table 3)
The association between highWMH load (above vs below the80th percentile) and dementia (SevereCI vs NoCI) wasstrong at age le80 (odds ratio [OR] 40 95 confidence in-terval [CI] 165ndash971 p = 0001) but absent at age gt80 (OR089 95 CI 026ndash303 p = 086) These associations were
unchanged when the analysis was repeated with the 80thpercentile cutoff determined separately in the 2 age groups(age le80 OR 39 95 CI 168ndash917 p = 0001 age gt80 OR16 95 CI 041ndash647 p = 0488)
A 2 times 3 factorial ANOVA with years of education as de-pendent variable showed no significant interaction betweenage and cognitive groups (p = 0693) nor did anotherANOVA with brain and ventricles volume as dependentvariable (p = 0159)
Age-relatedassociationsbetweenMDandFA inNAWM and cognitive statusA 2 times 3 factorial ANOVA on average MD values extractedfrom NAWM showed a main effect of age (F = 7358 p lt0001) a main effect of cognitive status (F = 1484 p lt 0001)and a significant interaction between age and cognitive status(F = 332 pinteraction = 0037) Sensitivity analyses showed thatthe interaction on MD from NAWM remained significantwhen adjusting for MRI protocol sex years of educationhead size presence of lacunes and number of vascular risksfactors (pinteraction = 0048) A similar 2 times 3 factorial ANOVAon average FA values extracted from NAWM showed a main
Table 1 Clinical and imaging features of total sample and age groups
Study Total Age le80 y Age gt80 y p Value
N 566 459 107
Age y mean plusmn SD 667 plusmn 143 625 plusmn 125 847 plusmn 37
Age range y 20ndash102 20ndash80 81ndash102
Age y median (IQR) 69 (205) 65 (179) 838 (49)
Female sex n () 280 (495) 228 (497) 52 (486) 0841
TIA other minor stroke n () 408 (721) 336 (734) 72 (679) 0259
Years of education mean plusmn SD 130 plusmn 35 133 plusmn 34 120 plusmn 37 0002
Hypertension n () 260 (459) 190 (415) 70 (654) lt0001
Diabetes n () 55 (97) 41 (90) 14 (131) 0168
Atrial fibrillation n () 60 (106) 40 (87) 20 (187) 0002
Hyperlipidemia n () 163 (288) 130 (284) 33 (308) 0538
Smoking n () 159 (281) 138 (301) 21 (196) 0040
Total Fazekas ge3 n () 174 (307) 117 (255) 57 (532) lt0001
Presence of lacunar infarcts n () 77 (136) 48 (105) 29 (274) lt0001
Brain volumea cm3 mean plusmn SD 10470 plusmn 1340 10738 plusmn 1298 9669 plusmn 1152 lt0001
WMH volume cm3 mean plusmn SD 117 plusmn 109 100 plusmn 89 191 plusmn 147 lt0001
Average FA (NAWM) mean plusmn SD 049 plusmn 003 050 plusmn 003 046 plusmn 003 lt0001
Average MD (NAWM) (times1023) mean plusmn SD 090 plusmn 009 088 plusmn 007 099 plusmn 008 lt0001
Abbreviations FA = fractional anisotropy IQR = interquartile range MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesTotal Fazekas calculated as sum of deep and periventricular scoresa Defined as the sum of gray and white matter volumes (ie not including the ventricles)
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 5
effect of age (F = 4174 p lt 0001) and a main effect ofcognitive status (F = 1367 p lt 0001) but no interaction (F =152 pinteraction = 0219)
One-way ANOVAs on average MD and FA values extractedfrom NAWM confirmed that there were differences acrosscognitive groups only in patients aged le80 but not inpatients aged gt80 (table 2) Adding age or WMH volume ascovariates (analyses of covariance) did not change theresults (table 4)
Localization of WMH relevant tocognitive statusThe voxel-wise 2 times 3 factorial ANOVA showed an interactionbetween cognitive status and age group in an area of the leftdeep frontal white matter (figure 3 bluendashlight blue) Thevoxel-wise correlational analysis performed in patients agedle80 showed that in this group the association between theprobability of having WMH and lower MoCA score was lo-calized in periventricular frontal and parietal white matterareas bilaterally more extended on the left hemisphere
Table 2 Clinical and imaging features of cognitive groups by age
No CI Mild CI Severe CI p Value
Age le80 y
NWMH (NDTI) 338 (295) 97 (83) 24 (20)
Age y mean plusmn SD 618 plusmn 25 620 plusmn 126 702 plusmn 87 0005
Female n () 165 (488) 45 (464) 18 (750) 0036
Event type TIA other minor stroke n () 254 (754) 71 (732) 11 (458) 0007
Hypertension n () 131 (389) 44 (454) 15 (625) 0161
Diabetes n () 26 (77) 7 (72) 8 (333) 0001
Atrial fibrillation n () 26 (77) 12 (124) 2 (83) 0561
Hyperlipidemia n () 93 (276) 28 (289) 9 (375) 0871
Smoking n () 107 (318) 24 (247) 7 (292) 0547
Presence of lacunar infarcts n () 33 (98) 12 (126) 3 (125) 0691
WMH volume cm3 mean plusmn SD 94 plusmn 79 101 plusmn 78 181 plusmn 184 lt0001a
Average FA (NAWM) mean plusmn SD 050 plusmn 003 049 plusmn 003 047 plusmn 003 lt0001a
Average MD (NAWM) (times1023) mean plusmn SD 086 plusmn 006 096 plusmn 007 096 plusmn 007 lt0001a
Age gt80 y
NWMH (NDTI) 44 (42) 46 (42) 17 (16)
Age y mean plusmn SD 839 plusmn 33 859 plusmn 42 834 plusmn 25 0009
Female sex n () 22 (500) 22 (478) 8 (471) 0970
Event type TIA other minor stroke n () 31 (721) 30 (652) 11 (647) 0749
Hypertension n () 26 (591) 32 (696) 12 (706) 0730
Diabetes n () 3 (68) 8 (174) 3 (176) 0575
Atrial fibrillation n () 6 (136) 12 (261) 2 (118) 0512
Hyperlipidemia n () 13 (295) 17 (370) 3 (176) 0637
Smoking n () 9 (205) 9 (196) 3 (176) 0901
Presence of lacunar infarcts n () 12 (279) 15 (326) 2 (118) 0256
WMH volume cm3 mean plusmn SD 159 plusmn 107 213 plusmn 146 214 plusmn 219 0166a
Average FA (NAWM) mean plusmn SD 047 plusmn 003 045 plusmn 003 045 plusmn 004 0110a
Average MD (NAWM) (times1023) mean plusmn SD 096 plusmn 007 101 plusmn 009 101 plusmn 010 0067a
Abbreviations CI = cognitive impairment FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesa Comparisons between cognitive groups that were significant for patients le80 but not for patients gt80
6 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

effect of age (F = 4174 p lt 0001) and a main effect ofcognitive status (F = 1367 p lt 0001) but no interaction (F =152 pinteraction = 0219)
One-way ANOVAs on average MD and FA values extractedfrom NAWM confirmed that there were differences acrosscognitive groups only in patients aged le80 but not inpatients aged gt80 (table 2) Adding age or WMH volume ascovariates (analyses of covariance) did not change theresults (table 4)
Localization of WMH relevant tocognitive statusThe voxel-wise 2 times 3 factorial ANOVA showed an interactionbetween cognitive status and age group in an area of the leftdeep frontal white matter (figure 3 bluendashlight blue) Thevoxel-wise correlational analysis performed in patients agedle80 showed that in this group the association between theprobability of having WMH and lower MoCA score was lo-calized in periventricular frontal and parietal white matterareas bilaterally more extended on the left hemisphere
Table 2 Clinical and imaging features of cognitive groups by age
No CI Mild CI Severe CI p Value
Age le80 y
NWMH (NDTI) 338 (295) 97 (83) 24 (20)
Age y mean plusmn SD 618 plusmn 25 620 plusmn 126 702 plusmn 87 0005
Female n () 165 (488) 45 (464) 18 (750) 0036
Event type TIA other minor stroke n () 254 (754) 71 (732) 11 (458) 0007
Hypertension n () 131 (389) 44 (454) 15 (625) 0161
Diabetes n () 26 (77) 7 (72) 8 (333) 0001
Atrial fibrillation n () 26 (77) 12 (124) 2 (83) 0561
Hyperlipidemia n () 93 (276) 28 (289) 9 (375) 0871
Smoking n () 107 (318) 24 (247) 7 (292) 0547
Presence of lacunar infarcts n () 33 (98) 12 (126) 3 (125) 0691
WMH volume cm3 mean plusmn SD 94 plusmn 79 101 plusmn 78 181 plusmn 184 lt0001a
Average FA (NAWM) mean plusmn SD 050 plusmn 003 049 plusmn 003 047 plusmn 003 lt0001a
Average MD (NAWM) (times1023) mean plusmn SD 086 plusmn 006 096 plusmn 007 096 plusmn 007 lt0001a
Age gt80 y
NWMH (NDTI) 44 (42) 46 (42) 17 (16)
Age y mean plusmn SD 839 plusmn 33 859 plusmn 42 834 plusmn 25 0009
Female sex n () 22 (500) 22 (478) 8 (471) 0970
Event type TIA other minor stroke n () 31 (721) 30 (652) 11 (647) 0749
Hypertension n () 26 (591) 32 (696) 12 (706) 0730
Diabetes n () 3 (68) 8 (174) 3 (176) 0575
Atrial fibrillation n () 6 (136) 12 (261) 2 (118) 0512
Hyperlipidemia n () 13 (295) 17 (370) 3 (176) 0637
Smoking n () 9 (205) 9 (196) 3 (176) 0901
Presence of lacunar infarcts n () 12 (279) 15 (326) 2 (118) 0256
WMH volume cm3 mean plusmn SD 159 plusmn 107 213 plusmn 146 214 plusmn 219 0166a
Average FA (NAWM) mean plusmn SD 047 plusmn 003 045 plusmn 003 045 plusmn 004 0110a
Average MD (NAWM) (times1023) mean plusmn SD 096 plusmn 007 101 plusmn 009 101 plusmn 010 0067a
Abbreviations CI = cognitive impairment FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matterhyperintensitiesa Comparisons between cognitive groups that were significant for patients le80 but not for patients gt80
6 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

(figure 3 redndashyellow) (see resulting maps on neurovaultorgcollections2763) The voxel-wise correlational analysis inpatients aged gt80 instead showed no voxel-wise associationsbetween WMH and MoCA score
Voxel-wise results did not significantly change when con-trolling for age within each group
DiscussionWe found high WMH load in patients with previous TIA orminor stroke aged gt80 but showed that in this age group itwas not significantly associated with cognitive impairmentHigh WMH load was strongly associated with cognition onlyin patients aged le80 who were 4 times more likely to havesevere impairment than patients aged le80 with low WMHload The lack of significant association between WMH andcognition in patients aged gt80 also persisted on voxel-wiseanalyses of WMH distribution which are expected to be moresensitive than the simple measure of total WMH volumeFinally we explored if DTI measures of microstructural in-tegrity in NAWM (ie outside WMH) would correlate betterwith cognitive status but again found no significant associa-tions at age gt80
This loss of association betweenWMH and cognition at olderages might seem at odds with many previous studies showingsignificant associations between white matter damage andcognition in the general population or in groups of patientsaged gt50 60 or 651ndash37 However 2 studies found no asso-ciations between WMH and cognition in community-dwelling elderly and stroke survivors older than 802324 Ourfindings taken together with these 2 previous studies haveimportant implications for interpretation of brain imaging atolder ages First MRI has become the recommended first-lineimaging investigation for several neurologic conditions af-fecting older people and some WMH are almost universallyreported in elderly patients Our results suggest that highWMH loads in patients aged gt80 may be considered notexcessively concerning by clinicians patients or their familiesHowever the presence of WMH at younger ages should
prompt further investigation of possible cognitive impair-ment Second MRI markers of white matter damage havebeen recommended for use as a proxy of vascular cognitiveimpairment114546 but interpretation may be more complexin patients aged gt80
Since WMH represents late-stage macroscopic damage of thewhite matter that occurs as a result of small vessel disease wealso studied microstructural markers of white matter integrityassociated with interstitial fluid mobility and water content(namely MD and FA) outside the WMH regions in macro-scopically normal-appearing white matter These measureshave been argued to be better markers of cognitive decline inpatients with symptomatic cerebrovascular disease and to bemore sensitive to change11 Yet we did not find a strong as-sociation between these measures and cognitive status inpatients gt80 suggesting that our findings are not due to in-trinsic limitations of the particular MRI marker adoptedNeuropathologic studies also showed that the associationbetween dementia and postmortem evidence of vascular pa-thology attenuates in the very old47
The lack of association between white matter abnormality andcognitive impairment in patients gt80 was mainly driven bypatients with substantial white matter disease and normalcognition Patients aged le80 with similar degree of damageinstead showed severe cognitive impairment This findinggoes against the hypothesis that a certain threshold of WMHis needed to affect cognition23 It also suggests that the lack ofcorrelation between WMH and cognition in patients agedgt80 could not simply be due to the fact that patients withsevere white matter damage might have already died by theage of 80 as if this were the case the group aged gt80 would beexpected to have little white matter abnormality HoweverWMH may have diverse underlying pathologies some notaffecting cognition or life expectancy others increasing sus-ceptibility to dementia and death (ie only patients whosewhite matter pathology caused dementia had died by the ageof 80) In addition since we studied all consecutive patientspresenting to a TIAstroke clinic we cannot exclude thepossibility of a sampling bias due to the fact that elderlypatients with severe cognitive impairment or dementia may
Table 3 Results of factorial analyses of variance (ANOVAs) repeated on 4 random subsamples of participants aged le80stratified according to cognition (ie same as the original group of 459)
Stratified random samples aged le80
N 2 times 3 factorial ANOVA
No CI Mild CI Severe CI Total Mean square F p Value
Random sample 1 84 24 6 114 0370 3098 0047
Random sample 2 84 24 6 114 0371 3271 0040
Random sample 3 85 24 6 115 0661 6307 0002
Random sample 4 85 25 6 116 0438 3559 0030
Abbreviation CI = cognitive impairment
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 7
not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

not present to medical attention for a suspected TIA How-ever previous studies on community-dwelling elderly notsubject to presentation bias similarly found no associationbetween white matter abnormalities and cognition1423 Yetthe clinical implications of our study (ie the lack of associ-ation between WMH and cognitive impairment in patientsaged gt80) remain irrespective of the mechanism asmdashultimatelymdashthe group of patients relevant to clinicians onlyincludes those who present to medical attention Of note thelack of correlation between WMH and cognition in patientsaged gt80 parallels the tendency for the associations betweenother risk factors and dementia to attenuate with advancingages48
One of the strengths of our study is that it addresses a majorlimiting factor in non-population-based studies by not ex-cluding very old patients In addition we imaged a relativelyhomogeneous population in that all patients had recentsymptomatic cerebrovascular disease such that confoundingby greater comorbidities or vascular risk factors in the olderage group is less likely as also shown by sensitivity analysesincluding potential confounders such as brain size educationnumber of vascular risks factors and presence of lacunarinfarcts as covariates
Several limitations should be highlighted First we lookedonly at the cross-sectional associations with cognitive status
Figure 2 Age-related associations between white matter hyperintensity (WMH) volume and cognitive status
(A) Violin plots of the adjusted log-transformed WMH volumesfor the 6 groups of interest obtained by dividing patientsaccording to cognitive status and age Error bars are plusmn 1 SD(B) Average maps of WMH distribution for each group Firstrow patients aged gt80 second row patients le80 Left Nocognitive impairment (CI) Middle Mild CI Right Severe CI(neurovaultorgcollections2763)
8 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

and cannot be certain that associations would be similar onlong-term follow-up Second we used only the MoCA asa screening tool for cognitive impairment and so we cannotexclude subtler cognitive deficits in older patients with severewhite matter disease which might have been evident on moredetailed neuropsychological assessment However we wereprimarily interested in clinically overt cognitive impairmentThird we did not adjust for the presence of subclinical
depression or other neuropsychiatric disorders which mayaffect cognitive performance However we would expect theeffect of stroke-related depression to be similar across the 2age groups49 as these did not differ in the severity of cere-brovascular event Finally we cannot exclude that the lack ofcorrelation between WMH and cognition in patients agedgt80 was merely due to differences in sample size Howeverwe believe this possibility to be extremely unlikely considering
Figure 3 Localization of white matter hyperintensity (WMH) relevant to cognitive status
In redndashyellow regions of significant correlation between higher probability of havingWMH and lowerMontreal Cognitive Assessment scores in patients agedle80 years The same correlational analyses in patients aged gt80 years did not lead to significant results In bluendashlight blue region of significant interactionbetween age and cognitive status resulting from the 2 times 3 voxel-wise analysis of variance (neurovaultorgcollections2763)
Table 4 Follow-up analyses of covariance performed adjusting for age and for other measures of white matterabnormalities as covariates
Cognitive group effect
Age le80 y Age gt 80
Meansquare F
pValue
Partialη2
Meansquare F
pValue
Partialη2
Dependent variable WMH no covariates (also reportedin table 2)
1358 11058 lt0001a 0046 0219 2070 0166a 0038
Dependent variable WMH covariate age 0574 6167 0002a 0026 0106 1056 0351a 0020
Dependent variable WMH covariate FA in NAWM 0312 3987 0019a 0020 0031 0394 0675a 0008
Dependent variable WMH covariate MD in NAWM 0113 1584 0206 0008 0013 0196 0822 0004
Dependent variable MD no covariates (also reported intable 2)
9578E-8 19487 lt0001a 0090 1985E-8 2782 0067a 0054
Dependent variable MD covariate age 4710E-8 14562 lt0001a 0069 1426E-8 2234 0113a 0044
Dependent variable MD covariate WMH 2031E-8 7144 0001a 0035 7015E-9 1568 0214a 0032
Dependent variable FA no covariates (also reported intable 2)
0015 18852 lt0001a 0087 0003 2256 0110a 0044
Dependent variable FA covariate age 0008 14282 lt0001a 0068 0002 1933 0150a 0039
Dependent variable FA covariate WMH 0005 9053 lt0001a 0044 0001 1262 0288a 0026
Abbreviations FA = fractional anisotropy MD = mean diffusivity NAWM = normal-appearing white matter WMH = white matter hyperintensitya Analyses of covariance in which the effect of the cognitive groups were significant for patients le80 but not for patients gt80
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 9
that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

that we found a significant interaction and that our resultsagree with other findings in the literature142350 Futurestudies with larger sample sizes in patients older than 80 arerequired to support the identified lack of clinical significanceof MRI markers
Our findings confirm the association between MRI markers ofwhite matter damage and cognitive impairment in patientsyounger than 80 They also suggest that the clinical significanceof MRI markers might not be overinterpreted in patients olderthan 80 or considered a good proxy of vascular cognitive im-pairment in trials or research studies on this age group
Author contributionsG Zamboni study design analysis and interpretation of datadraft and revision of the manuscript L Griffanti data analysisand interpretation draft and revision of the manuscript SMazzucco acquisition of data revision of the manuscript STPendlebury study design and concept revision of the man-uscript PM Rothwell study design and concept study su-pervision and funding analysis and interpretation of datacritical revision of the manuscript
AcknowledgmentThe authors thank Dr Matteo Paolucci and Dr RiccardoRicceri for their contribution to quality check of the imagesThe authors acknowledge the use of the facilities of theOxford Acute Vascular Imaging Centre (AVIC) Oxford Thiswork uses data provided by patients and collected by the NHSas part of their care and support and would not have beenpossible without access to this data The NIHR recognizesand values the role of patient data securely accessed andstored both in underpinning and leading to improvements inresearch and care
Study fundingThe Oxford Vascular Study is funded by the Wellcome TrustWolfson Foundation British Heart Foundation and theNIHR Biomedical Research Centre Oxford ProfessorPendlebury and Dr Griffanti were funded by the OxfordNIHR Biomedical Research Centre The views expressed arethose of the authors and not necessarily those of the NHS theNIHR or the Department of Health
DisclosureThe authors report no disclosures relevant to the manuscriptGo to NeurologyorgN for full disclosures
Publication historyReceived by Neurology October 25 2017 Accepted in final formMarch 4 2019
References1 Debette S Markus HS The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging systematic review and meta-analysis BMJ 2010341c3666
2 Mortamais M Artero S Ritchie K Cerebral white matter hyperintensities in theprediction of cognitive decline and incident dementia Int Rev Psychiatry 201325686ndash698
3 de Groot JC de Leeuw FE Oudkerk M et al Cerebral white matter lesions andcognitive function the Rotterdam Scan Study Ann Neurol 200047145ndash151
4 Dong C Nabizadeh N Caunca M et al Cognitive correlates of white matter lesionload and brain atrophy the Northern Manhattan Study Neurology 201585441ndash449
5 Arvanitakis Z Fleischman DA Arfanakis K Leurgans SE Barnes LL Bennett DA Asso-ciation of white matter hyperintensities and gray matter volume with cognition in olderindividuals without cognitive impairment Brain Struct Funct 20162212135ndash2146
6 Knopman DS Griswold ME Lirette ST et al Vascular imaging abnormalities andcognition mediation by cortical volume in nondemented individuals AtherosclerosisRisk in Communities neurocognitive study Stroke 201546433ndash440
7 Biesbroek JM Kuijf HJ van der Graaf Y et al Association between subcorticalvascular lesion location and cognition a voxel-based and tract-based lesion-symptommapping study The SMART-MR study PLoS One 20138e60541
8 Zamboni G Griffanti L Jenkinson M et al White matter imaging correlates of earlycognitive impairment detected by the Montreal Cognitive Assessment after transientischemic attack and minor stroke Stroke 2017481539ndash1547
9 Vernooij MW Ikram MA Vrooman HA et al White matter microstructural integrityand cognitive function in a general elderly population Arch Gen Psychiatry 200966545ndash553
10 Tuladhar AM Reid AT Shumskaya E et al Relationship between white matterhyperintensities cortical thickness and cognition Stroke 201546425ndash432
11 Nitkunan A Barrick TR Charlton RA Clark CA Markus HS Multimodal MRI incerebral small vessel disease its relationship with cognition and sensitivity to changeover time Stroke 2008391999ndash2005
12 Maniega SM Valdes Hernandez MC Clayden JD et al White matter hyperintensitiesand normal-appearing white matter integrity in the aging brain Neurobiol Aging201536909ndash918
13 Pelletier A Periot O Dilharreguy B et al Age-related modifications of diffusion tensorimaging parameters and white matter hyperintensities as inter-dependent processesFront Aging Neurosci 20157255
14 Bennett IJ Greenia DEMaillard P et al Age-related white matter integrity differencesin oldest-old without dementia Neurobiol Aging 201756108ndash114
15 Munoz Maniega S Chappell FM Valdes Hernandez MC et al Integrity of normal-appearing white matter influence of age visible lesion burden and hypertension inpatients with small-vessel disease J Cereb Blood flow Metab 201737644ndash656
16 Etherton MR Wu O Cougo P et al Integrity of normal-appearing white matter andfunctional outcomes after acute ischemic stroke Neurology 2017881701ndash1708
17 de Groot M Verhaaren BF de Boer R et al Changes in normal-appearing whitematter precede development of white matter lesions Stroke 2013441037ndash1042
18 Zhong G Lou M Multimodal imaging findings in normal-appearing white matter ofleucoaraiosis a review Stroke Vasc Neurol 2016159ndash63
19 de Leeuw FE de Groot JC Achten E et al Prevalence of cerebral white matter lesionsin elderly people a population based magnetic resonance imaging study The Rot-terdam Scan Study J Neurol Neurosurg Psychiatry 2001709ndash14
20 Yang Z Wen W Jiang J et al Age-associated differences on structural brain MRI innondemented individuals from 71 to 103 years Neurobiol Aging 20164086ndash97
21 Westlye LT Walhovd KB Dale AM et al Life-span changes of the human brain whitematter diffusion tensor imaging (DTI) and volumetry Cereb Cortex 2010202055ndash2068
22 Hajjar I Quach L Yang F et al Hypertension white matter hyperintensities andconcurrent impairments in mobility cognition and mood the Cardiovascular HealthStudy Circulation 2011123858ndash865
23 Piguet O Ridley L Grayson DA et al Are MRI white matter lesions clinicallysignificant in the rsquoold-oldrsquo Evidence from the Sydney Older Persons Study DemenGeriatr Cogn Disord 200315143ndash150
24 Firbank MJ Burton EJ Barber R et al Medial temporal atrophy rather than whitematter hyperintensities predict cognitive decline in stroke survivors Neurobiol Aging2007281664ndash1669
25 United Nations Department of International ES Affairs Population Division Worldpopulation prospects the 2015 revision Available at esaunorgunpdwpp2015Accessed June 7 2019
26 Yang Z Slavin MJ Sachdev PS Dementia in the oldest old Nat Rev Neurol 20139382ndash393
27 Lucca U Tettamanti M Logroscino G et al Prevalence of dementia in the oldest oldthe Monzino 80-plus population based study Alzheimers Dement 201511258ndash270e3
28 Fotuhi M Hachinski V Whitehouse PJ Changing perspectives regarding late-lifedementia Nat Rev Neurol 20095649ndash658
29 Skrobot OA OrsquoBrien J Black S et al The vascular impairment of cognition classifi-cation consensus study Alzheimers Dement 201713624ndash633
30 Jellinger KA Pathology and pathogenesis of vascular cognitive impairment a criticalupdate Front Aging Neurosci 2013517
31 Love S Miners JS White matter hypoperfusion and damage in dementia post-mortem assessment Brain Pathol 20152599ndash107
32 Jagust WJ Zheng L Harvey DJ et al Neuropathological basis of magnetic resonanceimages in aging and dementia Ann Neurol 20086372ndash80
33 Lees R Selvarajah J Fenton C et al Test accuracy of cognitive screening tests fordiagnosis of dementia and multidomain cognitive impairment in stroke Stroke 2014453008ndash3018
34 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM Impact of different opera-tional definitions on mild cognitive impairment rate and MMSE and MoCA perfor-mance in transient ischaemic attack and stroke Cerebrovasc Dis 201336355ndash362
10 Neurology | Volume 93 Number 3 | July 16 2019 NeurologyorgN
35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

35 Pendlebury ST Cuthbertson FC Welch SJ Mehta Z Rothwell PM Underestimationof cognitive impairment by Mini-Mental State Examination versus the MontrealCognitive Assessment in patients with transient ischemic attack and stroke a pop-ulation-based study Stroke 2010411290ndash1293
36 Pendlebury ST Mariz J Bull L Mehta Z Rothwell PM MoCA ACE-R and MMSEversus the National Institute of Neurological Disorders and StrokendashCanadian strokenetwork vascular cognitive impairment harmonization standards neuropsychologicalbattery after TIA and stroke Stroke 201243464ndash469
37 Pendlebury ST Wadling S Silver LE Mehta Z Rothwell PM Transient cognitiveimpairment in TIA and minor stroke Stroke 2011423116ndash3121
38 Griffanti L Zamboni G Khan A et al BIANCA (brain intensity abnormality classi-fication algorithm) a new tool for automated segmentation of white matter hyper-intensities Neuroimage 2016141191ndash205
39 Smith SM Fast robust automated brain extraction Hum Brain Mapp 200217143ndash155
40 Griffanti L Jenkinson M Suri S et al Classification and characterization of peri-ventricular and deep white matter hyperintensities on MRI a study in older adultsNeuroImage 2018170174ndash181
41 Andersson JLR Jenkinson M Smith S Non-linear optimisation FMRIB technicalreport TR07JA1 Available at wwwfmriboxacukdatasetstechreptr07ja2tr07ja2pdf Accessed June 7 2019
42 Fazekas F Chawluk JB Alavi A HurtigHI ZimmermanRAMR signal abnormalities at 15T in Alzheimerrsquos dementia and normal aging AJR Am J Roentgenol 1987149351ndash356
43 Behrens TE Woolrich MW Jenkinson M et al Characterization and propagation ofuncertainty in diffusion-weighted MR imaging Magn Reson Med 2003501077ndash1088
44 Winkler AM Ridgway GR Webster MA Smith SM Nichols TE Permutation in-ference for the general linear model Neuroimage 201492381ndash397
45 Wardlaw JM Smith EE Biessels GJ et al Neuroimaging standards for research intosmall vessel disease and its contribution to ageing and neurodegeneration LancetNeurol 201312822ndash838
46 Croall ID Lohner V Moynihan B et al Using DTI to assess white matter micro-structure in cerebral small vessel disease (SVD) in multicentre studies Clin Sci 20171311361ndash1373
47 Savva GM Wharton SB Ince PG Forster G Matthews FE Brayne C Age neuro-pathology and dementia N Engl J Med 20093602302ndash2309
48 Deckers K Kohler S van Boxtel M et al Lack of associations between modifiable riskfactors and dementia in the very old findings from the Cambridge City over-75scohort study Aging Ment Health 2018221272ndash1278
49 Wolfe CD Crichton SL Heuschmann PU et al Estimates of outcomes up to ten yearsafter stroke analysis from the prospective South London Stroke Register PLoS Med20118e1001033
50 Firbank MJ Wiseman RM Burton EJ Saxby BK OrsquoBrien JT Ford GA Brain atrophyand white matter hyperintensity change in older adults and relationship to bloodpressure brain atrophy WMH change and blood pressure J Neurol 2007254713ndash721
NeurologyorgN Neurology | Volume 93 Number 3 | July 16 2019 11
DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL0000000000007772 published online June 14 2019Neurology
Giovanna Zamboni Ludovica Griffanti Sara Mazzucco et al minor stroke
Age-dependent association of white matter abnormality with cognition after TIA or
This information is current as of June 14 2019
ServicesUpdated Information amp
772fullhttpnneurologyorgcontentearly20190614WNL0000000000007including high resolution figures can be found at
Citations
772fullotherarticleshttpnneurologyorgcontentearly20190614WNL0000000000007This article has been cited by 2 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectionvascular_dementiaVascular dementia
httpnneurologyorgcgicollectionmriMRI
httpnneurologyorgcgicollectioncognitive_agingCognitive aging e
httpnneurologyorgcgicollectionall_cerebrovascular_disease_strokAll Cerebrovascular diseaseStrokefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology









![[SfN] Agreement between the white matter connectivity via tensor-based morphometry and the volumetric white matter parcellations](https://img.pdfslide.us/doc/110x75/55ae666e1a28ab306b8b4655/sfn-agreement-between-the-white-matter-connectivity-via-tensor-based-morphometry-and-the-volumetric-white-matter-parcellations.jpg)